Embed Size (px)
Citation preview
Tony Goddard MRCP FRCR
Consultant Interventional Neuroradiologist
Trust Members Meeting
Wed 28th Jan 2015
Overview:
Differences between the ‘stroke’ types
Why urgent treatment matters
Standard treatment available
Development of non-invasive treatments
Major trials and major shift in approach
Future directions and challenges


Uncommon type of ‘stroke’
Bleeding onto the surface of the brain
Cause usually an aneurysm:
Brain aneurysms rarely cause symptoms until they bleed/rupture
Very characteristic headache:
1. Back of the head
2. Thunderclap
Sickness
Light makes headache worse (photophobia)
Stiff neck
Affects 11,000 patients per year
Incidence 9 per 100,000 population
45-70 yrs of age most common
Average age is 55 yrs
65-70% women
50% mortality from a ruptured aneurysm

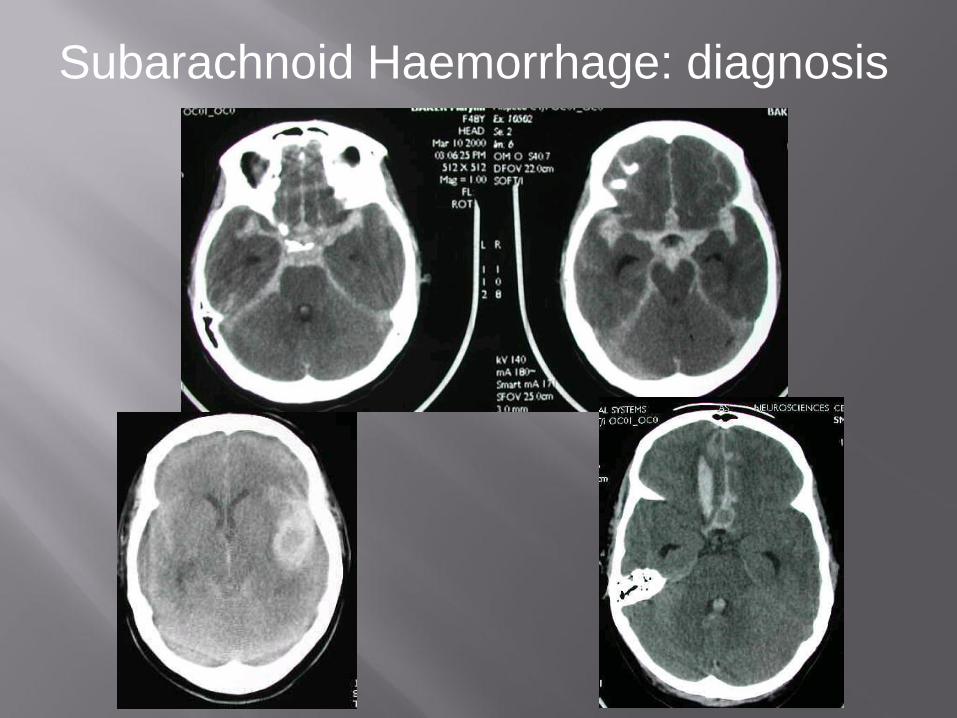
Subarachnoid Haemorrhage: diagnosis
• Brain scan (CT scan) ASAP
• If negative and clinical suspicion is high- a lumbar
puncture (spinal tap) is carried out to sample fluid
around the brain and test for blood
• If CT scan is positive the patient should be transferred
to a hospital that specialises in dealing with brain
haemorrhages.
• In Yorkshire this is Leeds General Infirmary
Subarachnoid Haemorrhage: diagnosis

• If aneurysm is not secured quickly it could burst again
• Risk is 50% in first 3-4 weeks
• If aneurysm is not treated most survivors will die of re-bleeding
within a year
• Risk is highest in first 1-3 days after initial bleed
• Minimum 50% immediate mortality with re-bleeding
• NCEPOD guidelines are to treat within 48 hours
• Most centres aim to treat within 24 hours 5/7 and
7/7 if enough operators
• Some patients cannot be saved due to very rapid re-bleeding
within hours
Natural History of Ruptured Brain Aneurysms


• Open surgery has been available for over 50 years
• Very effective treatment
• Evidence-based
PROS:
• Actual treatment risk similar to endovascular treatment
• Aneurysm is ‘cured’
• No imaging follow up for the aneurysm or re-treatment required
BUT:
• Requires craniotomy
• Long recovery
• Risk of seizures and infection
• Cannot drive for minimum 6 months
• Cosmetic deformity
Neurosurgical Treatment

So, if surgery is so good, why were coils developed?

Some aneurysms inaccessible, very high risk

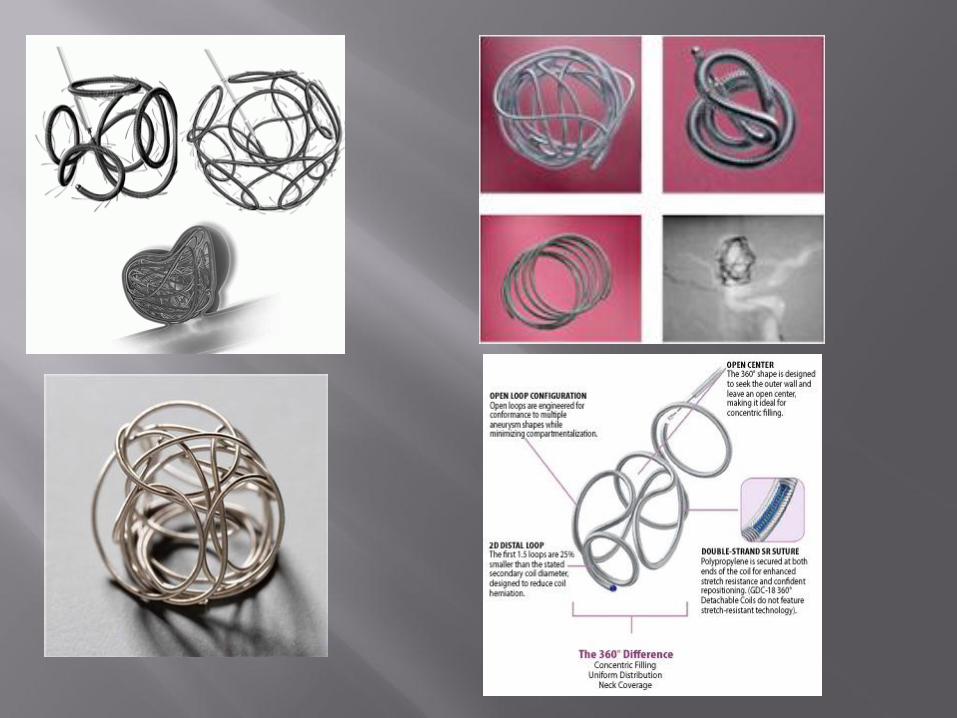
Development of Electrolytically detachable coils
Guglielmi G, Viñuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach. Part 1: Electrochemical basis, technique and experimental results. J Neurosurg 1991;75:1-7 Guglielmi G, Viñuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach. Part 2: Preliminary clinical experience. J Neurosurg 1991;75:8-14
15 patients, all awake Aneurysms 70-100% occluded 1 transient aphasia
FDA Multicentre study

Development of Electrolytically detachable coils
- Stainless steel delivery wire
- Electrolytic detachment
- Platinum Coils


Aim
To compare the safety and efficacy of an endovascular treatment policy of ruptured intracranial aneurysms with a conventional neurosurgical treatment policy in an eligible population.

To determine whether an endovascular treatment policy compared with a neurosurgical treatment policy, reduces the proportion of patients with a moderate or poor outcome (Rankin 3 or worse) by 25% at one year.

To determine whether endovascular coil treatment is:
• As effective as surgery at preventing re-bleeding
• Results in a better quality of life
• Is more cost effective
• Improves neuropsychological outcome

•ISAT Terminated by steering committee by fax to neuroscience
centres 03/05/02
• Relative reduction in adverse outcome at 1 yr (mGOS 3-5 )
of 22.6%
• Absolute reduction = 6.9%
• Endpoint of trial reached, “unethical” to continue randomisation
• Full 1yr f/u data presented AANS/CNS Feb 2003:
relative risk reduction 26.8%
absolute risk reduction: 8.7%
Immediate shift of significant workload to radiology in a Disorganised, ad hoc fashion without shift in finances or
personnel (ODAs, anaesthetists)

rebleed coil clip
<30 days 20 8
<1 yr 45 39
>1yr 7 2
0.2% p.a. >1yr for coiling
0.15% p.a. >1yr for clipping

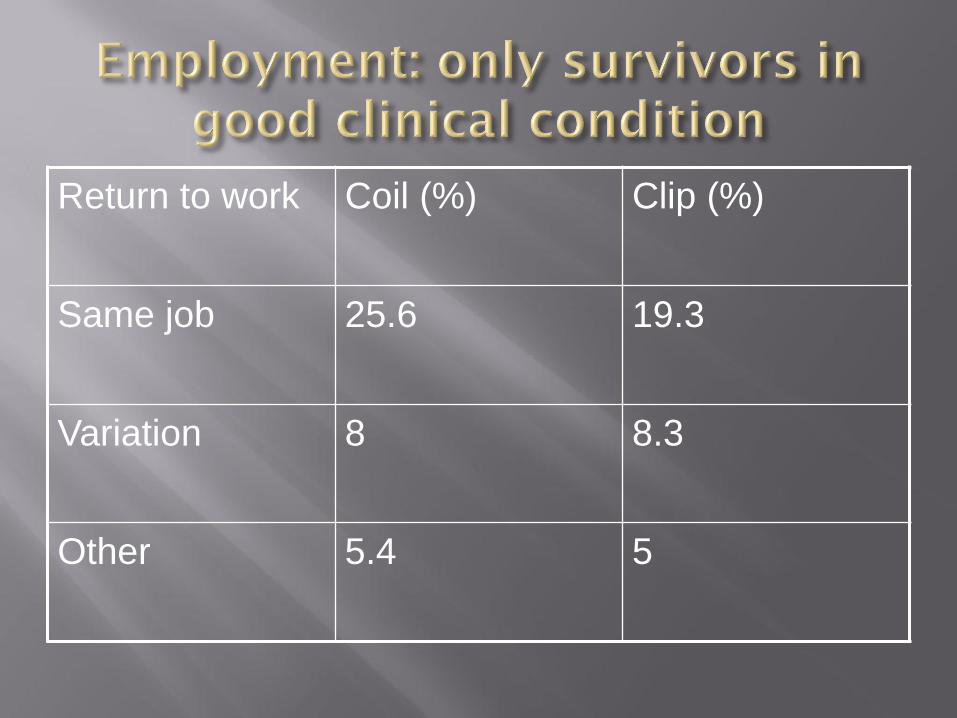
Return to work Coil (%) Clip (%)
Same job 25.6 19.3
Variation 8 8.3
Other 5.4 5


Basic Coiling Procedure

Expensive radiology equipment…

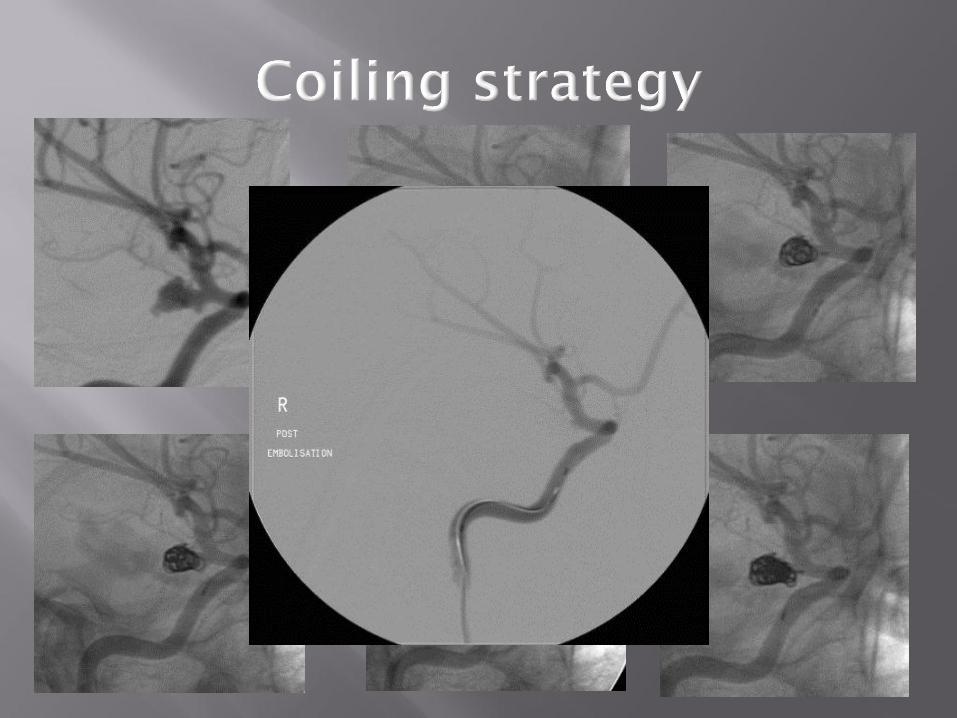

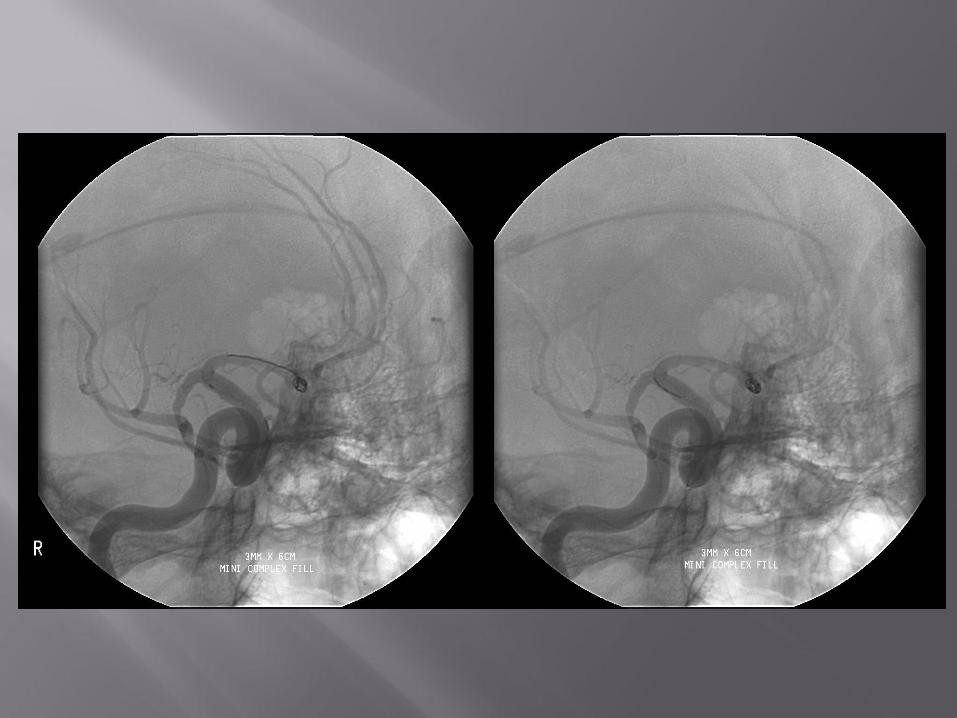


6/12 f/u
Small
SAH

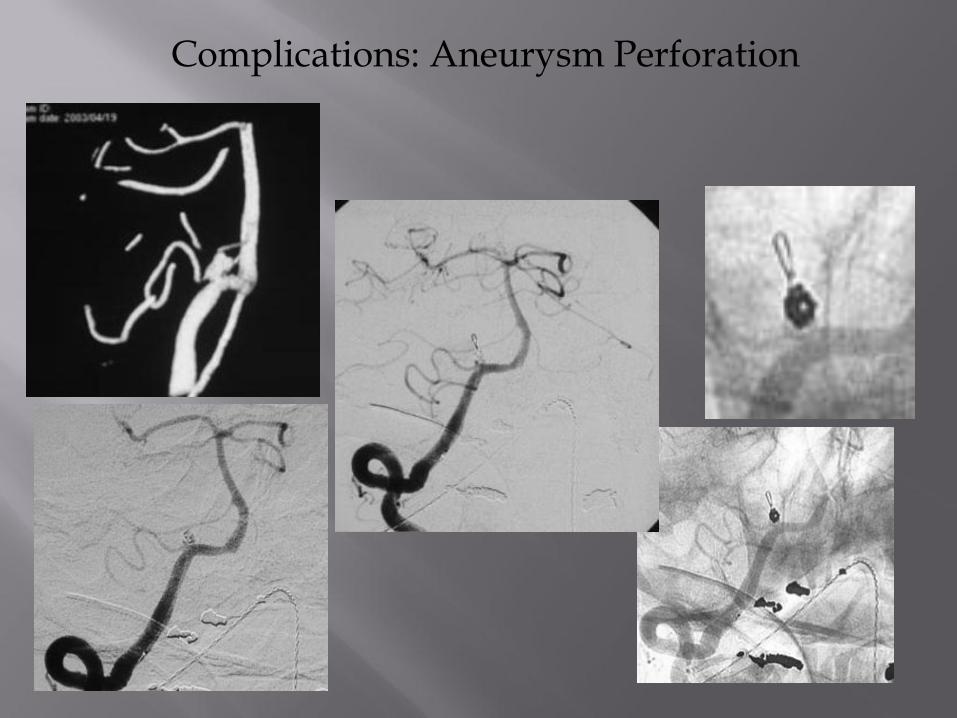
Complications: Aneurysm Perforation


New and Emerging Technologies
* Please read full “Instructions for Use” prior to use of the product.
** Fluoroscopy may be used up this point at the physician’s discretion .
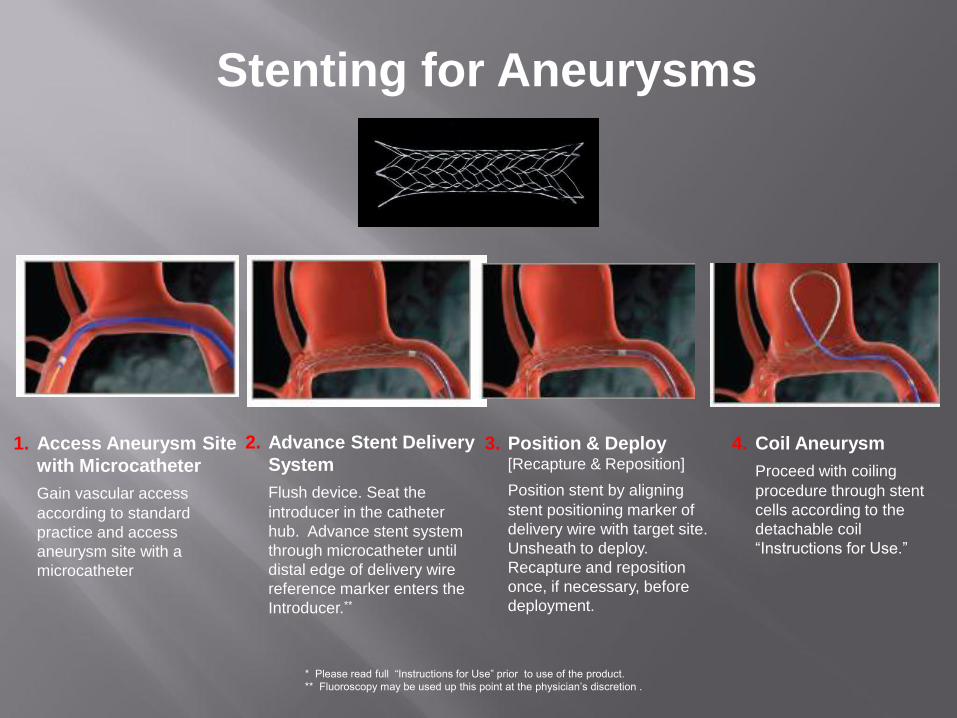
1. Access Aneurysm Site
with Microcatheter
Gain vascular access
according to standard
practice and access
aneurysm site with a
microcatheter
2. Advance Stent Delivery
System
Flush device. Seat the
introducer in the catheter
hub. Advance stent system
through microcatheter until
distal edge of delivery wire
reference marker enters the
Introducer.**
3. Position & Deploy [Recapture & Reposition]
Position stent by aligning
stent positioning marker of
delivery wire with target site.
Unsheath to deploy.
Recapture and reposition
once, if necessary, before
deployment.
4. Coil Aneurysm
Proceed with coiling
procedure through stent
cells according to the
detachable coil
“Instructions for Use.”
Stenting for Aneurysms

Stent is a permanent implant.
Patient requires Aspirin and
Clopidogrel beforehand, otherwise
high risk of acute thrombosis with
c 50% mortality.
Always causes groin problems!!!!
• Game-changing technology
PROS:
• Simplifies procedure as aneurysm does not have to be entered at all
• Large aneurysms treated with coils tend to come back and need
re-treatment or at the very least long-term surveillance
• Allow more difficult aneurysms to be treated without surgery
CONS:
• Expensive: £10,000 per device
• Need antiplatelet therapy therefore risk of ulcers and bleeding
(like cardiac stents)
• Can be difficult to deploy
• Strong evidence for their efficacy is lacking, despite more than 25,000
Worldwide being treated this way to date
• As procedure is simpler, wider variety of physicians (esp in U.S.) are
treating aneurysms this way: neurosurgeons, neurologist, cardiologists etc


LEO 5.5mm x 7.5cm
5.5mm x 40cm
5.5mmx 30mm




• Career longevity: stressful
• Not enough trainees
• Lack of opportunities to train in more than one centre
• Providing a seven day service
• De-skilling of neurosurgeons:
- aneurysm clipping is no longer a core requirement for trainees
- 95% of all ruptured aneurysm were treated by endovascular
means in 2014
Link:
Leeds
Hull
Sheffield
Networking!

Ischaemic Stroke

Pathogenesis of Acute Ischemic Stroke
What is Stroke ?
Definition:
It is a term used for acute focal or diffuse
neurological deficit lasting for more than
24 hours and caused by a focal or
diffuse insult to the brain that is of a
vascular origin (WHO).
Pathogenesis of Acute Ischemic Stroke
What is Stroke ?
Stroke involves a blockage of blood vessels
(temporary or permanent) and damage to brain
substance as a result.
CLINICAL BURDEN:
• About 150,000 strokes occur in the UK each ear
• Stroke accounts for 53,000 deaths in the UK /yr
• Third biggest killer after coronary artery disease and cancer
• Leading cause of disability in the UK
• 300,000 living with disability in the UK
• 25% occur in those younger than 65 yrs of age
• 20,000 younger than 45
ECONOMIC BURDEN:
• Average patient cost: £15,000-£30,000
• £2.8 billion per annum in 2003-2004
• £1.8 billion in indirect costs (loss of earnings etc)
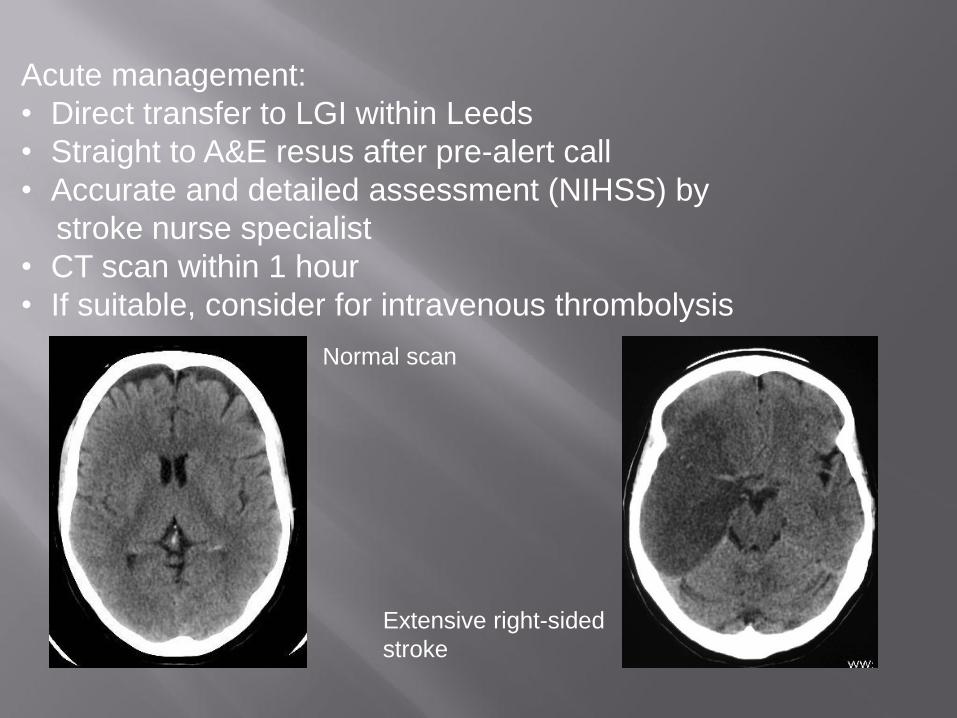
Acute management:
• Direct transfer to LGI within Leeds
• Straight to A&E resus after pre-alert call
• Accurate and detailed assessment (NIHSS) by
stroke nurse specialist
• CT scan within 1 hour
• If suitable, consider for intravenous thrombolysis
Normal scan
Extensive right-sided
stroke

Why time matters:
- Central area of infarcted brain
- Surrounding area where there is not enough blood to maintain normal
brain function
- This area will recover if blood flow is restored (PENUMBRA)
- If blood flow is not restored, the area of irreversibly dead brain will increase
in size until there is no penumbra left and no treatment will help,
and may actually cause further harm
- This process occurs within 3-6 hours
Pathophysiology of stroke

For each minute of occlusion/infarction the following are lost: 1.9 million neurons 14 billion synapses 12km of nerve fibres

The aim of
pharmacological or
neuro-intervention is to
restore anterograde
perfusion, thus salvaging
ischaemic brain

First Thrombolysis in 1958
• Sussman BJ, Fitch TSP
Thrombolysis with Fibronolysin in cerebral
arterial occlusion.
JAMA 1958; 167:1705-1709
• 3 patients: 1 ICA, 1 MCS and 1 ACA
occlusion
• 2 no change, 1 improved

“Early recanalisation is strongly associated with improved
functional outcome and reduced mortality”
Stroke, 2007; 38:967-973
“Recanalisation within 6 hours of onset increase the odds of a
non-disabled outcome 6 fold”
It has taken 49 years to prove that rapidly opening a
blocked blood vessel in the brain
benefits patients in clinical trials!
Neurovascular Revascularization
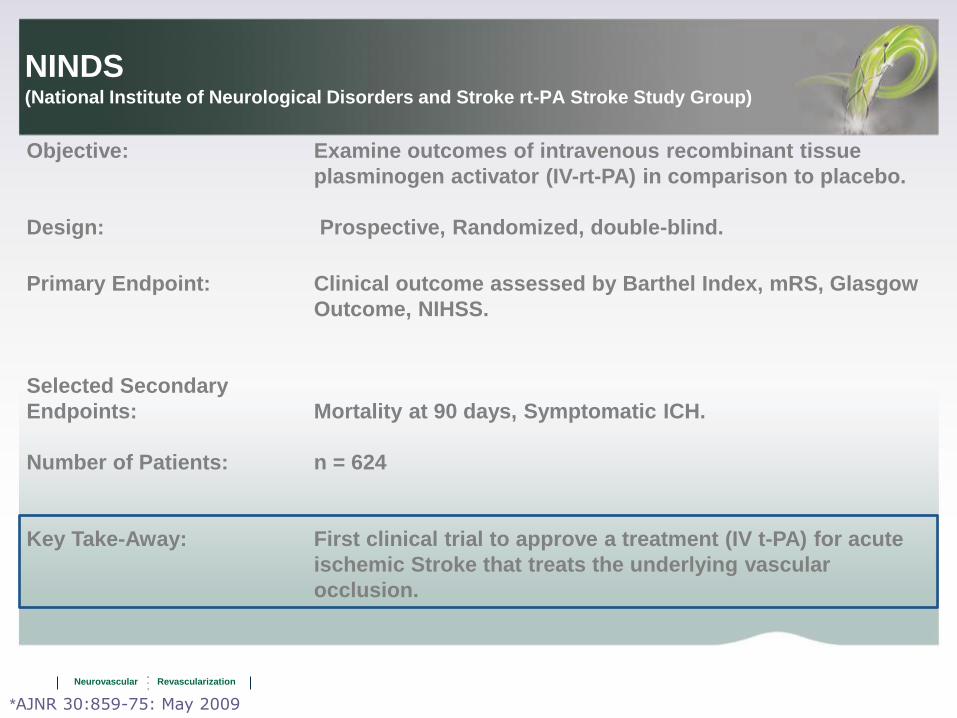
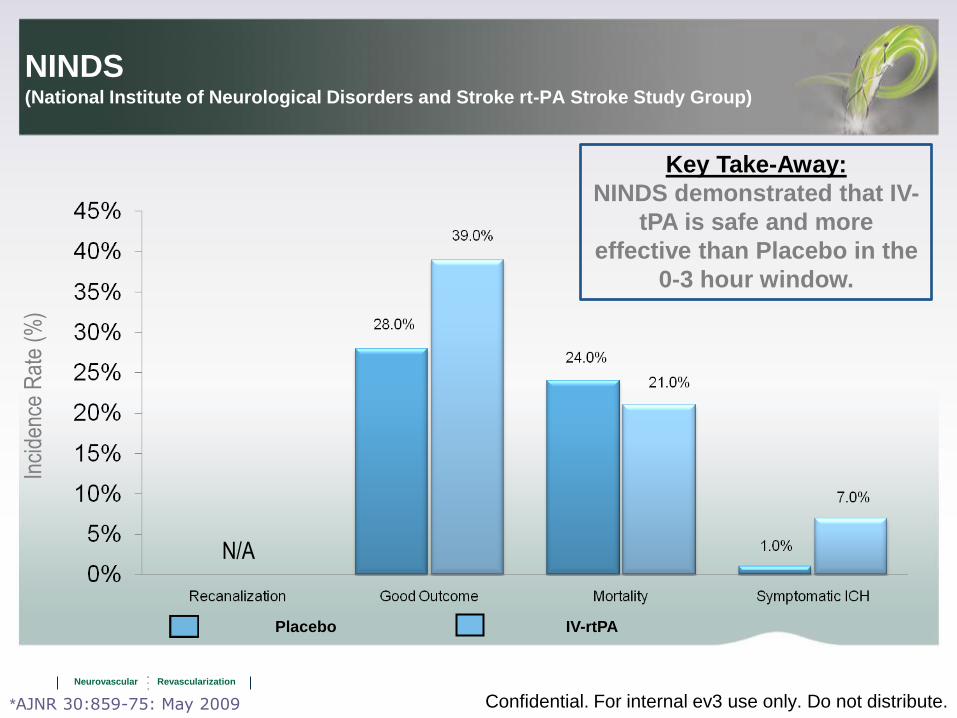
NINDS (National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group)
Objective: Examine outcomes of intravenous recombinant tissue
plasminogen activator (IV-rt-PA) in comparison to placebo.
Design: Prospective, Randomized, double-blind.
Primary Endpoint: Clinical outcome assessed by Barthel Index, mRS, Glasgow
Outcome, NIHSS.
Selected Secondary
Endpoints: Mortality at 90 days, Symptomatic ICH.
Number of Patients: n = 624
Key Take-Away: First clinical trial to approve a treatment (IV t-PA) for acute
ischemic Stroke that treats the underlying vascular
occlusion.
*AJNR 30:859-75: May 2009
Neurovascular Revascularization
Confidential. For internal ev3 use only. Do not distribute.
N/A
Inci
denc
e R
ate
(%)
IV-rtPA Placebo
NINDS (National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group)
*AJNR 30:859-75: May 2009
Key Take-Away:
NINDS demonstrated that IV-
tPA is safe and more
effective than Placebo in the
0-3 hour window.

“21.25% of patients had acute vessel re-opening of a proximal
occlusion following IV rTPA (thrombolysis)”
Stroke, 2010; 41:2254-2258
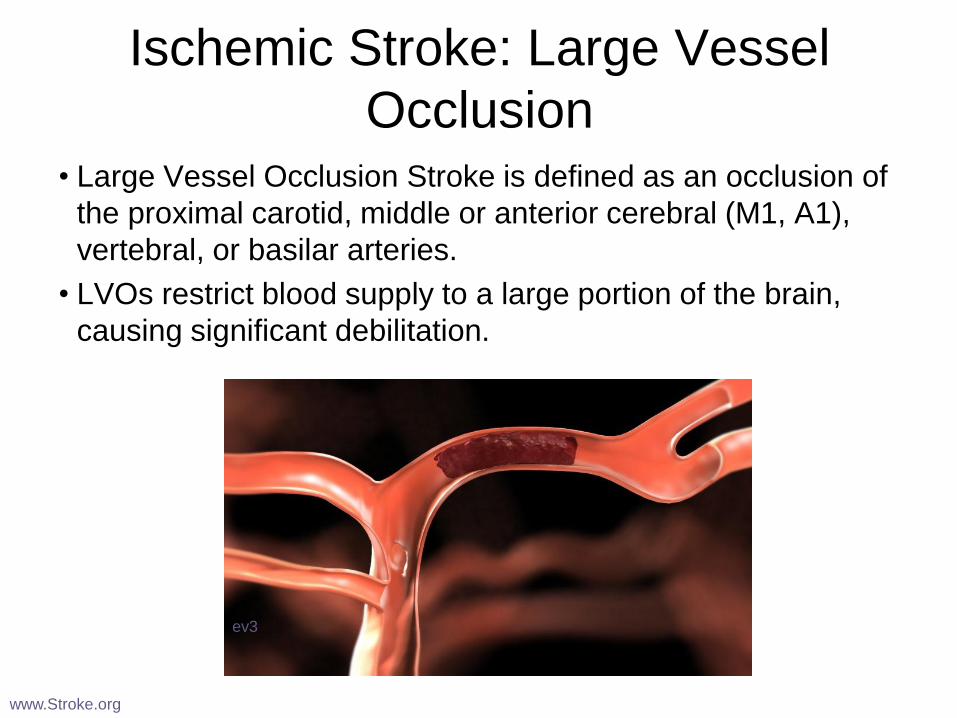
Ischemic Stroke: Large Vessel
Occlusion • Large Vessel Occlusion Stroke is defined as an occlusion of
the proximal carotid, middle or anterior cerebral (M1, A1),
vertebral, or basilar arteries.
• LVOs restrict blood supply to a large portion of the brain,
causing significant debilitation.
www.Stroke.org
ev3

“68% final recanalisation rate”
BUT
Only 36% patient were
independent 90 days
Stroke, 2008; 39:1205-1212

81.6% of the treated vessels were successfully
revascularised”
BUT
Only 29% of patients
were independent at
90 days”
Stroke, 2009, 40: 2761-2768

Successful re-opening in 90.9%
50% independent
Stroke, 2010; 41:2559-2567
First IA stroke treatment 1982
• Zeumer H, Hacke W, Kolman HL,
Poeck K.
Fibrinolysetherapie bei
Basilaristhrombose.
Dtsch Med Wschr 1982; 107: 728-31
• Successful treatment of a 27 y o woman
with basilar artery occlusion treated with
intra-arterial streptokinase
Experience in Leeds, UK
• Gradual increase in numbers of IA treatments
• Several ‘high-profile’ treatments
• National press coverage
• Increased public awareness of what is available

Boy, 5, is saved
by stroke op
A STROKE victim aged five has
become the youngest person to
undergo a new stent operation.
At hospital in Leeds he then threaded a stent
through the paient’s thigh to remove a clot
blocking an artery to his brain, allowing blood
to flow again.
The 20-minute op saved Saad’s life and —
after further surgery to reduce brain swelling —
he is now recovering at home in Bradford,
West Yorks.
Dad Safdar, 44, said: “It’s a miracle. All the
doctors and nurses have done such a great
job.”
22nd February 2012
BBC2: “Keeping Britain Alive”
Dr Tufail ‘Jazz Hands’ Patankar
With Dr Hannah Stockley
Dr Sapna Puppala offering moral support
18th October 2012

Stroke ‘live on TV’
• 19 yr old leaving lecture
• Stroke in front of camera
• Arrival 15 minute
• IV lysis
• Long MCA clot
• Not improving
• Successful thrombectomy and complete
recovery

It felt like a firework in my brain': Mother receives
life-saving treatment that cured stroke in two hours
Jacqueline had a stroke that left her paralysed and
unable to talk
She was cured after surgeons removed the blood
clot using a tube containing a tiny mesh basket
'It almost felt like fireworks in my head,' the mother
said
She is now fully recovered
By DAILY MAIL REPORTER
PUBLISHED: 13:26 GMT, 4 December
2012 | UPDATED: 13:27 GMT, 4 December 2012
Read more: http://www.dailymail.co.uk/health/article-
2242746/It-felt-like-firework-brain-Mother-receives-life-
saving-hour-stroke-cure.html#ixzz2wKl1hUaQ
Follow us: @MailOnline on Twitter | DailyMail on

Anecdote not evidence…
But it DOES work!

UK Status
• 33 Neuroscience centers
• Population 65 million
• 91 Interventional neuroradiologists
• Non-funded gradual increase in numbers

The region....
Heart attack
Hypertension
Stroke
Obesity

• A&E
• Radiology
• HASU
• Neurology
• Neurosurgery
• Neuro ITU
• Neuro HDU
• Paediatric neurology
• Paed neurosurgery
The place......

The people....
• 2 interventional neuroradiologists
• 8 stroke physicians working 24 hours on call
• 9 surrounding hospitals
• 8 Brain Attack team (BAT) nurses; on call 24/7
• On call radiographers
• On call nurse x 2
• Anaesthesia available 24/7

A&E
CT
Angiography

Clinical criteria:
• Clinically significant stroke
• <4.5 hours from stroke onset
• Patient less than 80 yrs of age (probably…)
• Patients who cannot have thrombolysis (e.g. on Warfarin)
• CT shows absence of large infarct
• No haemorrhage
Stroke Infrastructure in Leeds: Decision for IA lysis
Make a decision quickly and stick to it.
Don’t wait for IV lysis to work
Stroke Infrastructure in Leeds:
Decision for IA lysis

• Place stent across occlusion: leave in position for 10-20 min
• Reperfuse brain
• ‘Relax’ and plan your strategy
• Most clot will lyse naturally or improves efficacy of IV tPA
• Withdraw stent slowly

Procedural Details I • Requires simultaneous and immediate availability of :
- Neuroanaesthesia team
- Neuroradiology team
- Neurology team
• Local anaesthesia versus general still debated
• Team member to talk to family
• Arrange for a HASU or HDU bed to go afterwards

You have to be the conductor!
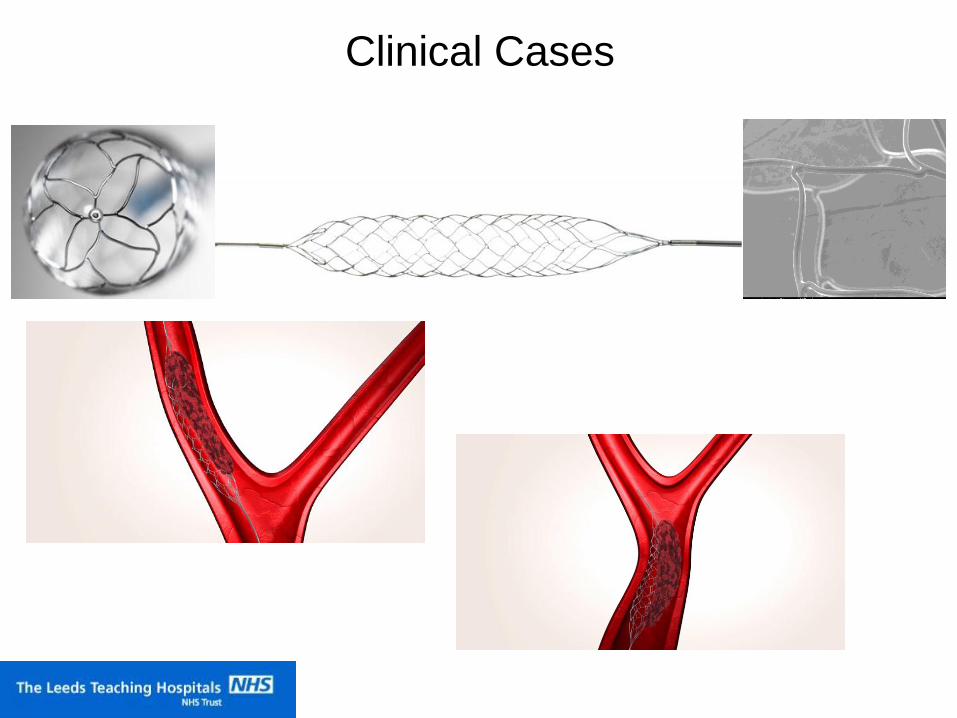
Clinical Cases

First Leeds Thrombectomy 16 yr old
Previously fit and well
Facial droop whilst having tea
Mum had seen F.A.S.T. posters
Straight to A&E Huddersfield
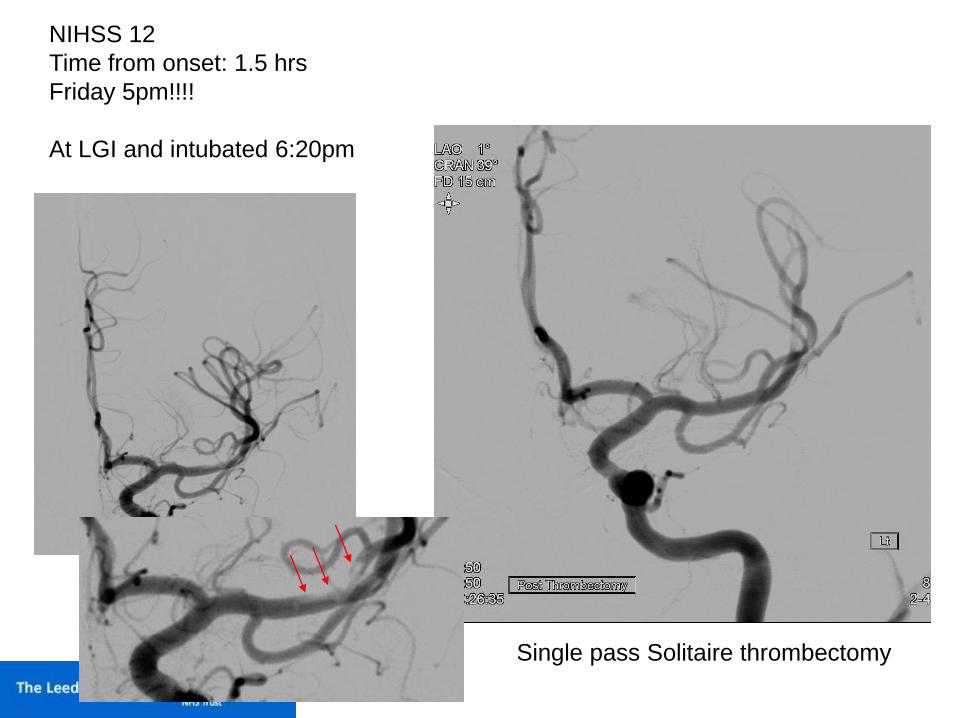
NIHSS 12
Time from onset: 1.5 hrs
Friday 5pm!!!!
At LGI and intubated 6:20pm
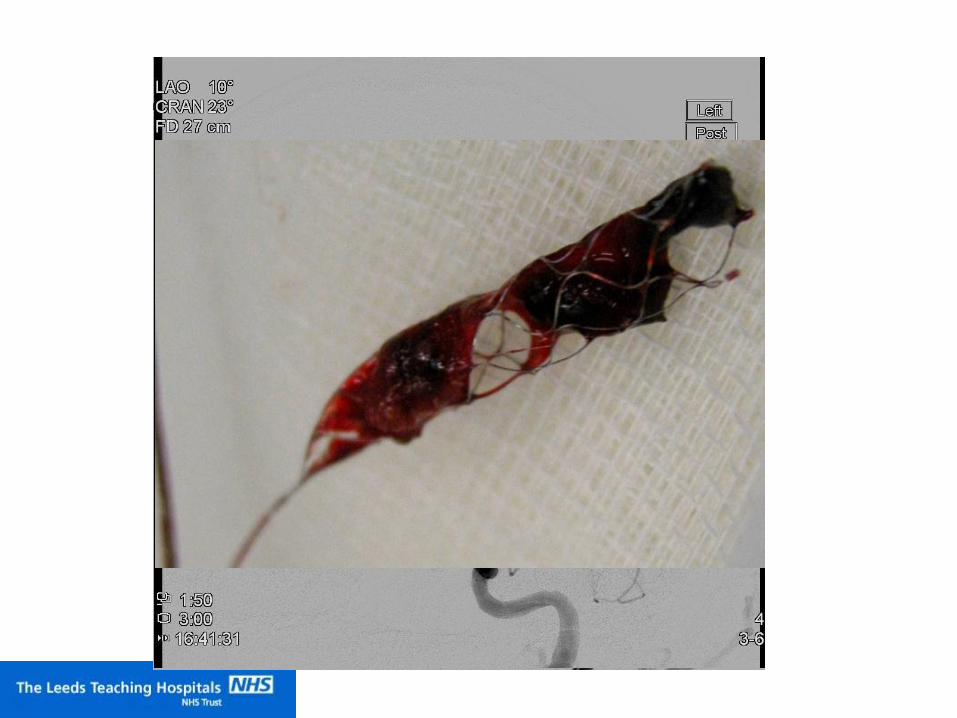
Single pass Solitaire thrombectomy
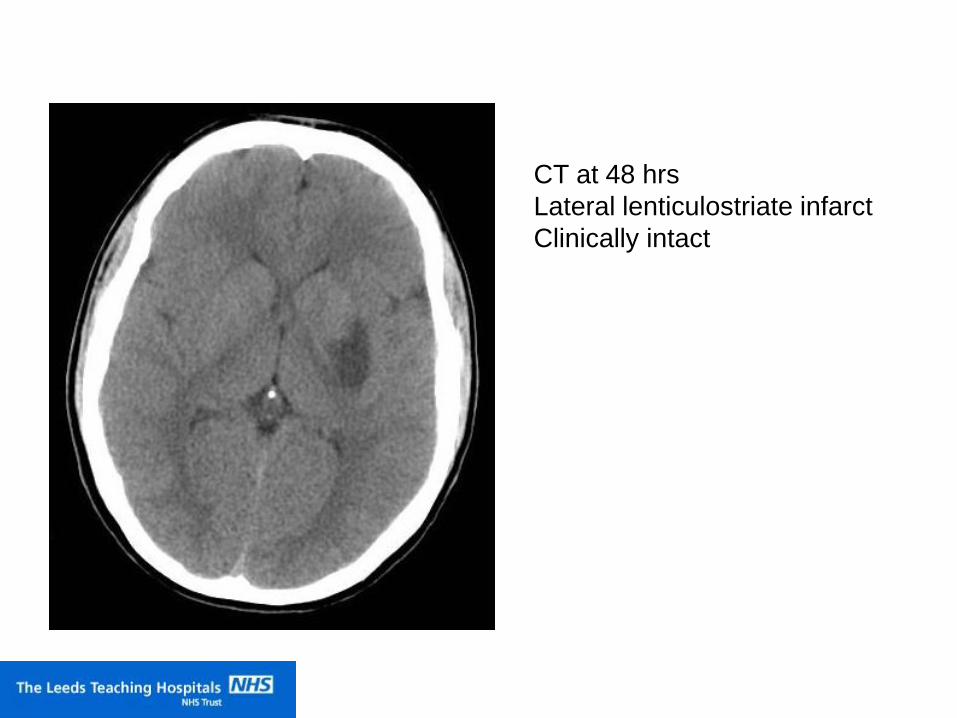
CT at 48 hrs
Lateral lenticulostriate infarct
Clinically intact

CTA: Acute MCA bifurcation
occlusion
Anaesthesia mobilised
GA 4pm
Case 2

Case 3
• M 10 yr old
• Prev F&W
• Onset dysphagia, dysarthria
• CT: 10pm 26/1/12 hyperdense BA (missed)
• MRI: 11am 27/1/12 BA thrombosis
• 2pm GCS 15/15 to 7/15
• Transfer to Leeds

Case 3

Revive 5 passes
Procedure terminated
Patient heparinised
I hoped clot would dissolve....

Clinical deterioration 3/7 later:
Locked in. Moving eyes only.
CT day 3: worsening central ischaemia

2nd attempt
Revive 4 passes


Patient Ages
0
1
2
3
4
5
6
7
8
<10 11 to 20 21-30 31-40 41-50 51-60 61-70 >70

MRS at 90 days
MRS 0-2 = 48%
5 deaths were in basilars that failed to recanalise
Poorer outcomes in patients over 70 years
0
1
2
3
4
5
6
7
8
0 1 2 3 4 5 6
Tips on improving case load:
• Don’t just be a technician
• Take credit for your success
• Audit results – especially those cases where
NO other treatment can be offered
• Present your cases
• Analyse cases with poor outcome
• Realise that some are ‘no lose’ situations and
occasional poor outcomes are inevitable
• PISTE



ORIGINAL ARTICLE A Trial of Imaging Selection and Endovascular Treatment for Ischemic Stroke
Chelsea S. Kidwell, M.D., Reza Jahan, M.D., Jeffrey Gornbein, Dr.P.H., Jeffry R. Alger, Ph.D., Val Nenov, Ph.D.,
Zahra Ajani, M.D., Lei Feng, M.D., Ph.D., Brett C. Meyer, M.D., Scott Olson, M.D., Lee H. Schwamm, M.D.,
Albert J. Yoo, M.D., Randolph S. Marshall, M.D., Philip M. Meyers, M.D., Dileep R. Yavagal, M.D., Max
Wintermark, M.D., Judy Guzy, R.N., Sidney Starkman, M.D., and Jeffrey L. Saver, M.D. for the MR RESCUE
Investigators
N Engl J Med 2013; 368:914-923March 7, 2013DOI: 10.1056/NEJMoa1212793
CONCLUSIONS
A favorable penumbral pattern on neuroimaging did not identify patients who would differentially benefit
from endovascular therapy for acute ischemic stroke, nor was embolectomy shown to be superior to
standard care.
(Funded by the National Institute of Neurological Disorders and Stroke; MR RESCUE
ClinicalTrials.gov number,
METHODS
In this study, we randomly assigned patients within 8 hours after the onset of large-vessel, anterior-circulation
strokes to undergo mechanical embolectomy (Merci Retriever or Penumbra System) or receive standard care.
All patients underwent pretreatment computed tomography or magnetic resonance imaging of the brain.
Randomization was stratified according to whether the patient had a favorable penumbral pattern
(substantial salvageable tissue and small infarct core) or a nonpenumbral pattern (large core or small or
absent penumbra). We assessed outcomes using the 90-day modified Rankin scale, ranging from 0
(no symptoms) to 6 (dead).

But: in the last 2 months…
RESULTS
We enrolled 500 patients at 16 medical centers in the Netherlands
(233 assigned to intra-arterial treatment and 267 to usual care alone).
The mean age was 65 years (range, 23 to 96),
and 445 patients (89.0%) were treated with intravenous alteplase before randomization.
Retrievable stents were used in 190 of the 233 patients (81.5%) assigned to
intraarterial treatment.
The adjusted common odds ratio was 1.67 (95% confidence interval [CI], 1.21 to 2.30).
There was an absolute difference of 13.5 percentage points (95% CI, 5.9 to 21.2)
in the rate of functional independence (modified Rankin score, 0 to 2)
in favor of the intervention (32.6% vs. 19.1%).
There were no significant differences in mortality or the occurrence of symptomatic
intracerebral hemorrhage.
MR CLEAN: A Randomized Trial of Intraarterial Treatment for
Acute Ischemic Stroke

Since MR CLEAN reported, three other trials evaluating endovascular
interventions:
- ESCAPE (Endovascular Treatment for Small Core and Proximal
Occlusion Ischemic Stroke)
- EXTEND IA (Extending the Time for Thrombolysis in Emergency
Neurological Deficits - Intra-Arterial)
- SWIFT PRIME (Solitaire FR as Primary Treatment for Acute
Ischemic Stroke)
Have been stopped after early interim analyses showed benefit in the
intervention group.
i.e. unethical to continue randomisation.

So what next….?
• IA therapy probably ought to be offered to patients 24/7 across the UK
• 2 people cannot do this in Yorkshire
• 4 maybe?
• Need to improve speed of diagnosis and hospital transfer
• Look to Germany……

Thank you for your attention