Embed Size (px)
Citation preview

Esophageal DisordersEsophageal Disorders
Dr. Salem M. Bazarah, Dr. Salem M. Bazarah, MD, M.Ed, FACP, FRCPC, FRCPC(GI) & PhDMD, M.Ed, FACP, FRCPC, FRCPC(GI) & PhD
Ass. Prof. & Consultant Gastroenterologist, Ass. Prof. & Consultant Gastroenterologist, Hepatologist & Interventional Endoscopist Hepatologist & Interventional Endoscopist
King Abdul Aziz UniversityKing Abdul Aziz UniversityDirector, Liver Transplant Program & Department of Director, Liver Transplant Program & Department of
Internal Medicine DSFHInternal Medicine DSFH

Esophageal DisordersEsophageal Disorders
MotilityMotilityAnatomic & Anatomic &
StructuralStructuralRefluxRefluxInfectiousInfectiousNeoplasticNeoplasticMiscellaneousMiscellaneous

Esophageal AnatomyEsophageal Anatomy
Upper EsophagealSphincter (UES)
Lower EsophagealSphincter (LES)
Esophageal Body(cervical & thoracic)
18 to 24 cm

Normal Phases of SwallowingNormal Phases of Swallowing
VoluntaryVoluntaryoropharyngeal phase – bolus is voluntarily oropharyngeal phase – bolus is voluntarily
moved into the pharynxmoved into the pharynx InvoluntaryInvoluntary
UES relaxationUES relaxationperistalsis (aboral movement)peristalsis (aboral movement)LES relaxationLES relaxation

Normal Phases of SwallowingNormal Phases of Swallowing
Between swallowsBetween swallowsUES prevents air entering the esophagus UES prevents air entering the esophagus
during inspiration and prevents during inspiration and prevents esophagopharyngeal refluxesophagopharyngeal reflux
LES prevents gastroesophageal refluxLES prevents gastroesophageal refluxperistaltic and non-peristaltic contractions in peristaltic and non-peristaltic contractions in
response to stimuliresponse to stimulicapacity for retrograde movement (belch, capacity for retrograde movement (belch,
vomiting) and decompressionvomiting) and decompression

Normal SwallowingNormal Swallowing
Cortical Swallowing Areas
Swallowing Center
Motor Nuclei
Oropharynx & Esophagus
Frontal cortex
Brainstem

Esophageal Motility Esophageal Motility DisordersDisorders

Motility DisordersMotility Disorders upper esophagealupper esophageal
UES disordersUES disorders neuromuscular disordersneuromuscular disorders
esophageal bodyesophageal body achalasiaachalasia diffuse esophageal spasmdiffuse esophageal spasm nutcracker esophagusnutcracker esophagus nonspecific esophageal nonspecific esophageal
dysmotilitydysmotility LESLES
achalasiaachalasia hypertensive LEShypertensive LES
primary disordersprimary disorders achalasiaachalasia diffuse esophageal spasmdiffuse esophageal spasm nutcracker esophagusnutcracker esophagus nonspecific esophageal nonspecific esophageal
dysmotilitydysmotility secondary disorderssecondary disorders
severe esophagitissevere esophagitis sclerodermascleroderma diabetesdiabetes Parkinson’sParkinson’s strokestroke

Diagnostic ToolsDiagnostic Tools
cineradiology or cineradiology or videofluoroscopy (MBS)videofluoroscopy (MBS)
barium esophagrambarium esophagramesophageal manometryesophageal manometryendoscopyendoscopy

Normal ManometryNormal Manometry

Motility DisordersMotility DisordersBased on ManometryBased on Manometry
AchalasiaAchalasia – – Inadequate LES relaxationInadequate LES relaxationDiffuse Esophageal SpasmDiffuse Esophageal Spasm – – Uncoordinated contractionUncoordinated contractionNutcracker EsophagusNutcracker Esophagus – – HypercontractionHypercontraction Ineffective Esophageal MotilityIneffective Esophageal Motility – – HypocontractionHypocontraction

AchalasiaAchalasia

AchalasiaAchalasia first clinically recognized esophageal first clinically recognized esophageal
motility disordermotility disorder described in 1672, treated with described in 1672, treated with
whale bone bougiewhale bone bougie term coined in 1929term coined in 1929 epidemiologyepidemiology
1-2 per 200,000 population1-2 per 200,000 population usually presents between ages usually presents between ages
25 to 6025 to 60 male=femalemale=female Caucasians > othersCaucasians > others average symptom duration at average symptom duration at
diagnosis: 2-5 yearsdiagnosis: 2-5 years

PathophysiologyPathophysiology
Degeneration of NO producing inhibitory neuronsDegeneration of NO producing inhibitory neurons loss of ganglionic cells in the myenteric plexus (distal loss of ganglionic cells in the myenteric plexus (distal
to proximal)to proximal) vagal fiber degenerationvagal fiber degeneration underlying cause: unknownunderlying cause: unknown
autoimmune? (antibodies to myenteric neurons in autoimmune? (antibodies to myenteric neurons in 50% of patients)50% of patients)
that affect relaxation of LESthat affect relaxation of LES Basal LES pressure risesBasal LES pressure rises

Mechanical End ResultMechanical End Result
dual disorderdual disorderLES fails to appropriately relaxLES fails to appropriately relax
resistance to flow into stomachresistance to flow into stomachnot spasm of LES not spasm of LES but an increased basal but an increased basal
LES pressure often seen (55-90%)LES pressure often seen (55-90%) loss of peristalsis in distal 2/3 esophagusloss of peristalsis in distal 2/3 esophagus

Clinical PresentationClinical Presentation
clinical presentationclinical presentationsolid dysphagia 90-100% (75% also with solid dysphagia 90-100% (75% also with
dysphagia to liquids)dysphagia to liquids)post-prandial regurgitation 60-90%post-prandial regurgitation 60-90%chest pain 33-50%chest pain 33-50%pyrosis 25-45%pyrosis 25-45%weight lossweight lossnocturnal cough and recurrent aspirationnocturnal cough and recurrent aspiration

Diagnostic Work UpDiagnostic Work Up
plain film (air-fluid level, wide mediastinum, plain film (air-fluid level, wide mediastinum, absent gastric bubble, pulmonary infiltrates)absent gastric bubble, pulmonary infiltrates)
barium esophagram (dilated esophagus with barium esophagram (dilated esophagus with taper at LES) taper at LES) Bird peak Bird peak good screening test (95% accurate)good screening test (95% accurate)
endoscopy (rule out GE junction tumors, esp. endoscopy (rule out GE junction tumors, esp. age>60)age>60)
esophageal manometry (absent peristalsis, esophageal manometry (absent peristalsis, LES relaxation, & resting LES >45 mmHg)LES relaxation, & resting LES >45 mmHg)


Manometric FeaturesManometric Features
Incomplete LES Incomplete LES relaxationrelaxation
Elevated resting Elevated resting pressure (>45 pressure (>45 mmHg)mmHg)
Aperistalsis of Aperistalsis of esophageal bodyesophageal body

Treatment of Achalasia Treatment of Achalasia

GoalsGoals
reduce LES pressure and reduce LES pressure and increase emptyingincrease emptying

Nitrates and Calcium Channel Nitrates and Calcium Channel BlockersBlockers
Isosorbide dinitrateIsosorbide dinitrate
Reduces LES Pressure 66% for 90 minReduces LES Pressure 66% for 90 min NifedipineNifedipine
Reduces LES pressure 30-40% for > 60 minutesReduces LES pressure 30-40% for > 60 minutes
50-70% initial response; <50% at 1 year50-70% initial response; <50% at 1 yearlimitations: tachyphylaxis and side-effectslimitations: tachyphylaxis and side-effects

Botulinum ToxinBotulinum Toxin
prevents ACH release at NM junction prevents ACH release at NM junction 90% initial response; 60% at 1 year90% initial response; 60% at 1 yearNeeds repetitive sessions Needs repetitive sessions

Pneumatic DilatationPneumatic Dilatation
Balloon dilatation to 300 psi Balloon dilatation to 300 psi disrupt circular muscle disrupt circular muscle 60-95% initial success; 60% at 5 years 60-95% initial success; 60% at 5 years recent series suggest 20-40% will require recent series suggest 20-40% will require
re-dilation re-dilation Success increases with repeat dilatationsSuccess increases with repeat dilatations risk of perforation 1-13% (usually 3-5%); risk of perforation 1-13% (usually 3-5%);
death 0.2-0.4%death 0.2-0.4%

Surgical TreatmentSurgical Treatment
surgical myotomy surgical myotomy (open or minimally-(open or minimally-invasive)invasive)
>90% initial response; >90% initial response; 85% at 10 years; 70% 85% at 10 years; 70% at 20 years (85% at 5 at 20 years (85% at 5 years with min. inv. years with min. inv. techniques)techniques)
<1% mortality; <10% <1% mortality; <10% major morbiditymajor morbidity
10-25% acutely 10-25% acutely develop reflux, up to develop reflux, up to 52% develop late reflux52% develop late reflux

Spastic Motility Disorders of the Spastic Motility Disorders of the EsophagusEsophagus

Spastic Motility Disorders of the Spastic Motility Disorders of the EsophagusEsophagus
Diffuse Esophageal Spasm Diffuse Esophageal Spasm Nutcracker EsophagusNutcracker EsophagusHypertensive LESHypertensive LESNonspecific Esophageal DysmotilityNonspecific Esophageal Dysmotility

EpidemiologyEpidemiology
Any age (mean 40 yrs)Any age (mean 40 yrs)Female > MaleFemale > Male

Clinical PresentationClinical Presentation
Dysphagia to solids and liquidsDysphagia to solids and liquids intermittent and non-progressiveintermittent and non-progressive present in 30-60%, more prevalent in DES (in most studies)present in 30-60%, more prevalent in DES (in most studies)
Chest Pain Chest Pain constant % across the different disorders (80-90%)constant % across the different disorders (80-90%) swallowing is not necessarily impairedswallowing is not necessarily impaired can mimic cardiac chest paincan mimic cardiac chest pain
Pyrosis (20%) and IBS symptoms (>50%)Pyrosis (20%) and IBS symptoms (>50%)Symptoms and Manometry correlate Symptoms and Manometry correlate
poorlypoorly

Diffuse Esophageal SpasmDiffuse Esophageal Spasm
frequent non-peristaltic frequent non-peristaltic contractionscontractions simultaneous onset (or simultaneous onset (or
too rapid propagation) too rapid propagation) of contractions in two of contractions in two or more recording or more recording leadsleads
occur with >30% of wet occur with >30% of wet swallows (up to 10% swallows (up to 10% may be seen in may be seen in “normals”)“normals”)

Nutcracker EsophagusNutcracker Esophagus
high pressure peristaltic high pressure peristaltic contractionscontractions avg pressure in 10 avg pressure in 10
wet swallows is >180 wet swallows is >180 mm Hgmm Hg
33% have long duration 33% have long duration contractions (>6 sec)contractions (>6 sec)
may inter-convert with may inter-convert with DESDES

Hypertensive Hypertensive LESLES
Nonspecific Nonspecific Esophageal Esophageal DysmotilityDysmotility
high LES high LES pressurepressure>45 mm Hg>45 mm Hg
normal normal peristalsisperistalsis
often overlaps often overlaps with other with other motility disordersmotility disorders
abnormal motility patternabnormal motility pattern fits in no other categoryfits in no other category
non-peristalsis in 20-non-peristalsis in 20-30% of wet swallows30% of wet swallows
low pressure waves low pressure waves (<30 mm Hg)(<30 mm Hg)
prolonged prolonged contractionscontractions

Diagnosis of Spastic Motility Diagnosis of Spastic Motility Disorders of the EsophagusDisorders of the Esophagus
ManometryManometryBarium Esophagram Barium Esophagram EndoscopyEndoscopyPH monitoring PH monitoring

Spastic Motility Disorders Spastic Motility Disorders of the Esophagusof the Esophagus
treatmenttreatment reassurancereassurance nitrates, anticholinergics, hydralazine - nitrates, anticholinergics, hydralazine - all all
unprovenunproven calcium channel blockers - calcium channel blockers - too few data with too few data with
negative controlled studies in chest painnegative controlled studies in chest pain psychotropic drugs – psychotropic drugs – trazodone, imipramine and trazodone, imipramine and
setraline effective in controlled studiessetraline effective in controlled studies dilation -dilation - anecdotal reports, probable placebo anecdotal reports, probable placebo
effecteffect

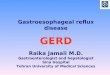
Manometry in Esophageal Manometry in Esophageal SymptomsSymptoms
Non-Cardiac Chest Pain Dysphagia
JE Richter, Ann Int Med, 1987

Hypomotilty DisordersHypomotilty Disorders
primary (idiopathic)primary (idiopathic) aging produces gradual decrease in contraction aging produces gradual decrease in contraction
strengthstrength reflux patients have varying degrees of hypomotilityreflux patients have varying degrees of hypomotility
more common in patients with atypical reflux more common in patients with atypical reflux symptomssymptoms
usually persists after reflux therapyusually persists after reflux therapy defined asdefined as
low contraction wave pressures (<30 mm Hg)low contraction wave pressures (<30 mm Hg)incomplete peristalsis in 30% or > of wet incomplete peristalsis in 30% or > of wet
swallowsswallows

Hypomotilty DisordersHypomotilty Disorders secondarysecondary
sclerodermascleroderma in >75% of patientsin >75% of patients progressive, resulting in aperistalsis in smooth-muscle regionprogressive, resulting in aperistalsis in smooth-muscle region incompetent LES with refluxincompetent LES with reflux
other “connective tissue diseases”other “connective tissue diseases” CRESTCREST polymyositis & dermatomyositispolymyositis & dermatomyositis
diabetesdiabetes 60% with neuropathy have abnormal motility on testing (most 60% with neuropathy have abnormal motility on testing (most
asx)asx) otherother
hypothyroidism, alcoholism, amyloidosishypothyroidism, alcoholism, amyloidosis

Non ischemic Chest PainNon ischemic Chest Pain remains poorly understood (remains poorly understood (functional chest pain)functional chest pain) enthusiasticenthusiastic investigation finds numerous investigation finds numerous
associations in studiesassociations in studies psychiatric disorders (depression, panic or anxiety psychiatric disorders (depression, panic or anxiety
disorder…)disorder…) esophageal disorders (GERD, motility disorders…)esophageal disorders (GERD, motility disorders…) musculoskeletal disordersmusculoskeletal disorders cardiac disease (microvascular, MVP, tachyarrhythmias…)cardiac disease (microvascular, MVP, tachyarrhythmias…)

Non ischemic Chest PainNon ischemic Chest Pain GERD is by far the most common, diagnosable, GERD is by far the most common, diagnosable,
esophagealesophageal cause cause 50-60% of patients have heartburn or acid regurgitation 50-60% of patients have heartburn or acid regurgitation
symptomssymptoms 50% have abnormal esophageal pH studies (not always 50% have abnormal esophageal pH studies (not always
correlating to sxs)correlating to sxs) veryvery low incidence of endoscopic findings low incidence of endoscopic findings ““PPI Test” may be best and most cost-effective approachPPI Test” may be best and most cost-effective approach
a small subset of patients with non-GERD NCCP display a small subset of patients with non-GERD NCCP display a variety of esophageal motility disordersa variety of esophageal motility disorders symptoms and motility findings correlate poorlysymptoms and motility findings correlate poorly esophageal hypersensitivity/hyperalgesia may explain the esophageal hypersensitivity/hyperalgesia may explain the
symptomssymptoms

GERDGERD
36-77% of all Americans experience36-77% of all Americans experience GERDGERD – – 7% have daily GERD symptoms7% have daily GERD symptoms – – 14-20% weekly symptoms14-20% weekly symptoms – – 15-50% monthly15-50% monthly Symptoms include: heartburn, acidSymptoms include: heartburn, acid regurgitation, water brash, dysphagia,regurgitation, water brash, dysphagia, atypical symptoms (asthma, globus,atypical symptoms (asthma, globus, laryngitis, cough, throat clearing)laryngitis, cough, throat clearing)

PathophysiologyPathophysiology
Lower esophageal sphincter dysfunctionLower esophageal sphincter dysfunctionDelayed gastric emptyingDelayed gastric emptyingEsophageal dysmotilityEsophageal dysmotility+/- hiatal hernia+/- hiatal herniaRepetitive mucosal injury / esophagitisRepetitive mucosal injury / esophagitisBarrett’s EsophagusBarrett’s Esophagus

Medical TreatmentMedical Treatment
Lifestyle modificationsLifestyle modifications
– – avoid coffee, fatty foods, smoking; avoid coffee, fatty foods, smoking; lose weight, raise head of bed, lose weight, raise head of bed, eliminate late night mealseliminate late night meals
Acid suppressin via PPI’sAcid suppressin via PPI’s

Indications for SurgeryIndications for Surgery
Failed medical managementFailed medical managementNeed for lifelong medical therapyNeed for lifelong medical therapyHiatal herniaHiatal herniaAtypical symptoms with (+) pH probeAtypical symptoms with (+) pH probeComplicationsComplications– – Barrett’s esophagus (5-15% develop BE)Barrett’s esophagus (5-15% develop BE)– – Erosive esophagitisErosive esophagitis

Surgical TreatmentSurgical Treatment
Pre-operative evaluationPre-operative evaluation– – EsophagramEsophagram– – EGDEGD– – Manometry (resting LES >5, length Manometry (resting LES >5, length
>2cm)>2cm)– – 24-hr esophageal pH monitoring24-hr esophageal pH monitoring

Surgical TreatmentSurgical Treatment
Laparoscopic Nissen FundoplicationLaparoscopic Nissen Fundoplication Goals of antireflux surgery:Goals of antireflux surgery: – – Recreate Angle of HisRecreate Angle of His – – Reconstitute LES with wrapReconstitute LES with wrap Predictors of good surgical outcome:Predictors of good surgical outcome: – – typical symptoms (heartburn, regurg)typical symptoms (heartburn, regurg) – – abnormal pH score, but NML motilityabnormal pH score, but NML motility – – clinical response to acid suppressionclinical response to acid suppression therapytherapy

Other New TreatmentsOther New Treatments
Stretta...radiofrequecy ablation of LESStretta...radiofrequecy ablation of LESEnteryx, Gatekeeper...implantedEnteryx, Gatekeeper...implantedbiopolymer into LESbiopolymer into LESEndocinch, Plicator...endoscopic suturingEndocinch, Plicator...endoscopic suturing to recreate LESto recreate LES

GERD Controversies GERD Controversies
Are meds better than antireflux surgery?Are meds better than antireflux surgery?Does antireflux surgery allow regression ofDoes antireflux surgery allow regression of Barrett’s esophageal better than meds?Barrett’s esophageal better than meds?Which is more cost effective?Which is more cost effective?Does symptom relief correlate withDoes symptom relief correlate with esophageal acid exposure?esophageal acid exposure?Where do the newer endoscopic therapiesWhere do the newer endoscopic therapies stand?stand?

Quiz?Quiz?
51 yrs old lady presented with chest pain , 51 yrs old lady presented with chest pain , difficulty to swallow, post prandial vomitingdifficulty to swallow, post prandial vomiting
Endoscopy failed to intubate the Endoscopy failed to intubate the esophagusesophagus
PPI givenPPI givenSymptoms improveSymptoms improve

04/19/2304/19/23 LDLT 5th caseLDLT 5th case 4949

GERD Medical Vs Surgical GERD Medical Vs Surgical TherapyTherapy
In 1992, VA Cooperative study found In 1992, VA Cooperative study found open open NissenNissen fundoplication better than fundoplication better than antacids, H2 blockers antacids, H2 blockers inin controlling GERDcontrolling GERD In 2001, VA Coop study follow-up at 10 years showedIn 2001, VA Coop study follow-up at 10 years showed 62% of surgical arm used acid suppression meds for62% of surgical arm used acid suppression meds for symptom controlsymptom control Few deaths due to esoph cancer, but study wasFew deaths due to esoph cancer, but study was underpowered to detect differenceunderpowered to detect difference

GERD Medical Vs Surgical GERD Medical Vs Surgical TherapyTherapy
A multicenter Nordic study evaluated treatmentA multicenter Nordic study evaluated treatment failures of Omeprazole to Nissen fundoplicationfailures of Omeprazole to Nissen fundoplication – – failure defined as: mod/severe heartburn,failure defined as: mod/severe heartburn, dysphagia or regurg; grade 2 esophagitis; > 8 wksdysphagia or regurg; grade 2 esophagitis; > 8 wks post-op requiring PPIpost-op requiring PPI At 12 months surgery was favoredAt 12 months surgery was favored But at five year follow-up, open surgery appearedBut at five year follow-up, open surgery appeared superior, but when allowing for escalating doses ofsuperior, but when allowing for escalating doses of PPI, each strategy was similar for symptom controlPPI, each strategy was similar for symptom control Lundell et al. Gastroenterology 114:A207, 1998.Lundell et al. Gastroenterology 114:A207, 1998. Lundell et al. JACS 192:172-179, 2001Lundell et al. JACS 192:172-179, 2001

GERD Medical Vs Surgical GERD Medical Vs Surgical TherapyTherapy
UK study evaluated UK study evaluated laparoscopic laparoscopic Nissen toNissen to PPI therapy in 217 randomized patients withPPI therapy in 217 randomized patients with chronic GERDchronic GERD At three months, LNF group had improvedAt three months, LNF group had improved LES pressure, DeMeester acid eposureLES pressure, DeMeester acid eposure score, GI symptom and general well-beingscore, GI symptom and general well-being score as compared to PPI group, and lastedscore as compared to PPI group, and lasted to twelve monthsto twelve months Mahon et al. Brit Journ Surg 92:695-699, 2005.Mahon et al. Brit Journ Surg 92:695-699, 2005.

Regression Of Barrett’s Regression Of Barrett’s
PPI compared to LNF in 35 non-randomizedPPI compared to LNF in 35 non-randomized pts with low-grade dyspasia detected onpts with low-grade dyspasia detected on surveillance EGDsurveillance EGD 12 of 19 (63%) in PPI group had regression of12 of 19 (63%) in PPI group had regression of LGD to Barrett’s compared to 15 of 16 (93%)LGD to Barrett’s compared to 15 of 16 (93%) of LNF pts at 12 and 18 monthsof LNF pts at 12 and 18 months Is biliopacreatic reflux to blame for BE?Is biliopacreatic reflux to blame for BE? Rossi et al. Annals of Surgery 243:58-63, 2006.Rossi et al. Annals of Surgery 243:58-63, 2006.

DO Symptoms Correlate with DO Symptoms Correlate with Treatment Treatment (Success/Failure)(Success/Failure)
24 hr pH and DeMeester acid scores24 hr pH and DeMeester acid scores compared in 70 pts on no meds, on PPIs, orcompared in 70 pts on no meds, on PPIs, or after antireflux surgeryafter antireflux surgery LES pH decreased most by LNFLES pH decreased most by LNF 18 of 30 PPI pts asymptomatic but had18 of 30 PPI pts asymptomatic but had pathologic pH probe testingpathologic pH probe testing 19 LNF pts complained of heartburn/regurg,19 LNF pts complained of heartburn/regurg, only two had positive pH probeonly two had positive pH probe Jenkinson et al. Brit Jour Surg 91:1460-1465, Jenkinson et al. Brit Jour Surg 91:1460-1465,
2004.2004.

Hiatal HerniaHiatal Hernia

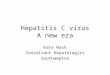
Pathophysiology & ClassificationPathophysiology & Classification
Type I - slidingType I - sliding Type II - Type II -
paraesophagealparaesophageal Type III - para and Type III - para and
sliding componentsliding component Type IV - other Type IV - other
viscera involvedviscera involved

Clinical PresentationClinical Presentation
postprandial fullness (63%),postprandial fullness (63%),Reflux (31%), Reflux (31%), Dysphagia (34%), Dysphagia (34%), Bleeding (24%)Bleeding (24%)Regurgitation/vomiting (36%)Regurgitation/vomiting (36%)Dyspnea (11%)Dyspnea (11%)

Work UpWork Up

Surgical TreatmentSurgical Treatment
Effective repair includes:Effective repair includes:
– – Excision of hernia sacExcision of hernia sac
– – Reduction of hernia contentsReduction of hernia contents
– – Repair of crural defectRepair of crural defect– – Fundoplication, gastropexy, PEG,Fundoplication, gastropexy, PEG,
esophageal lengthening (Collisesophageal lengthening (Collis
gastroplasty)gastroplasty)

Upper Esophageal Motility Upper Esophageal Motility DisordersDisorders

OverviewOverview cause oropharyngeal dysphagia (transfer dysphagia)cause oropharyngeal dysphagia (transfer dysphagia)
patients complain of patients complain of difficulty swallowingdifficulty swallowing tracheal aspiration may cause symptomstracheal aspiration may cause symptoms
pharyngoesophageal neuromuscular disorderspharyngoesophageal neuromuscular disorders strokestroke Parkinson’sParkinson’s poliomyelitispoliomyelitis ALSALS multiple sclerosismultiple sclerosis diabetesdiabetes myasthenia gravismyasthenia gravis dermatomyositis and polymyositisdermatomyositis and polymyositis
upper esophageal sphincter (cricopharyngeal) dysfunctionupper esophageal sphincter (cricopharyngeal) dysfunction

OverviewOverview cricopharyngeal hypertensioncricopharyngeal hypertension
elevated UES resting toneelevated UES resting tone poorly understood (reflex due to acid reflux or distension)poorly understood (reflex due to acid reflux or distension)
cricopharyngeal achalasiacricopharyngeal achalasia incomplete UES relaxation during swallowincomplete UES relaxation during swallow may be related to Zenker’s diverticula in some patientsmay be related to Zenker’s diverticula in some patients
clinical manifestationsclinical manifestations localizes as upper (cervical) dysphagialocalizes as upper (cervical) dysphagia within seconds of swallowingwithin seconds of swallowing coughing, choking, immediate regurgitation, orcoughing, choking, immediate regurgitation, or
nasal regurgitationnasal regurgitation diagnosis: swallow evaluation & modified barium swallowdiagnosis: swallow evaluation & modified barium swallow