Embed Size (px)
Citation preview

Vol 6 Issue 2
December 2014
“Medication Safety Is Everyone’s Responsibility”
A Medication Safety Newsletter by the Pharmaceutical
Services Division, Ministry of Health Malaysia
This newsletter is for circulation
to healthcare providers only
Fixing the antics By Dr. Rizah Mazzuin RazaliGeriatrician, Kuala Lumpur Hospital
Another usual day at the ward and my geriatrician-
colleague was with me doing rounds together with
my medical officer and intern. We saw Pak cik MS
who was an elderly man with multiple comorbidities
(well, all our patients are elderly with multiple
comorbidities!) who is unable to ambulate because
of his low back pain that could have been attributed
by his previous fall five years ago which resulted in
a fractured spine. He was given regular
Paracetamol or in-short, PCM as analgesia. The
PCM does seem to help but it wasn’t enough to
control the pain as to allow him to mobilize better.
For the past few months, he has been dependent
on his equally elderly wife who has triple vessel
coronary disease to assist him in most of his
bADLs (Basic activities of daily living). As such, we
were quite desperate to get him up on his feet
again and we deliberated on what would be the
next best medication to alleviate the pain and at
the same time, avoiding complications. It took us
about 10 minutes before we finally made a
decision. As I turned to look at my MO and intern,
they looked amazed (perhaps not so much in a
positive way?) at how long it took for us to make a
decision of initiating another medication.
Many of us take for granted when it comes to
prescribing medications for patients. We like to
think that we are doing our patients favours,
however, what may then transpire is, with the lack
of knowledge and poor judgement, they are
exposed to harmful consequences especially the
vulnerable elderly patients. And I am not just
referring to highly toxic drugs like chemotherapy or
Dabigatran, which has no antidote…I am referring
to the usual simple medications like Calcium
lactate, L-thyroxine, Amitriptyline…
A geriatrician shares her experience……
>> Page 3
Speaking of Amitriptyline,
I have once encountered a
patient in a clinic who was
broken by good intentions of
her doctors but subsequently
rebuilt herself. She was a 79-
year-old lady, who looked good
and well for her age. As we
began to talk, I realized that
this lady had gone through a
period of difficulties, thanks to
what is called as prescription
cascade. She has been treated
by a physician for dyspepsia
and was given several types of
medications that unfortunately
did not help much.

NOTE
Page 2
AdvisorsYBhg. Dato’ Eisah A. RahmanDr. Salmah Binti Bahri
For enquiries kindly contact:
Medication Safety Section,Pharmaceutical Services Division, Ministry of Health Malaysia,P.O. Box 924, Jalan Sultan,46790 Petaling Jaya, Selangor.Tel: +603-78413200 / 3320Fax: +603-79682222 / 2268E-mail: [email protected]
Materials published in this newsletter may be reproduced with permission.
The Pharmaceutical Services Division (PSD) shall not be liable for any loss or damage caused by the use of any information obtained from this newsletter
Editorial MembersChe Pun Binti BujangWan Mohaina Binti Wan MohammadJohn C.P. ChangFaridah Binti Md. YusofSubasyini a/p SivasupramaniamTea Ming HuiErik Tan Xi YiYen Sze WheyOng Su HuaJuliana Binti Nazlim Lim
Medication Safety Newsletter Vol 6 Issue 2 December 2014
Editor’sEditor’sEditorial Board
High-Tech Pill Will Text When Swallowed
1) Proteus Digital Health has developed a pill which enables the caregivers and doctors to get alerts the momentpatients swallow their medications.
2) This system is already available for over-the-counter sale in a pilot program in the United Kingdom.3) It is intended for the growing number of aging people and is expected to be most in demand among those
recently discharged from a hospital stay who may face particular challenges adhering to a new medicationregimen.
• Each of the ‘texting pills’contains a tiny metal sensor,the size of a grain of sand, thatemits a signal when it gets wetin the stomach. It then passesharmlessly through the body.
• The pill’s signal is picked upby a patch on the arm, whichtransmits the message bywireless Bluetooth technologyto the patient’s mobile phone.
• The phone then texts thepatient’s contacts – such as aloved-one and their doctor ornurse – telling them it has beentaken.
Source: http://www.telegraph.co.uk/health/healthnews/10279007/The-pill-that-can-text-from-inside-the-body.html
By Tea Ming Hui Pharmacist, Sultanah Nora Ismail Hospital, Batu Pahat
What’s
New??
Our focus on Geriatrics is timely because Malaysian demographic profile is inching towards
older population where the above 60 years now stands at around 10% and expected to touch
15% by 2030. Rising living standard and health awareness with better healthcare have enabled
Malaysians to enjoy longer life. However, with life extension it also means having to endure
higher incidence of degenerative and other diseases requiring more medical attention and
medications, often lead to polypharmacy as well.
In the U.S., for example, 13% of the population are above 65 years but consume 30% of the
prescription medications. Over 46% of elderly patients hospitalised are taking at least 7
medications, and one can expect similar situation in Malaysia. More medications can result in
increasing risks of drug interactions that may lead to more complex drug regimens and medical
complications, serious enough for the US Department of Health and Human Services to
designate polypharmacy a principal medication issue in its Healthy People Report 2000.
Despite specialised need and care of older patients, healthcare providers and medical facilities
are still geared mainly towards mainstream younger population. It is timely we be reminded that
older persons today are living longer and want to stay active, healthy and independent. The last
they want is to suffer from medical and medicines mismanagement from callous attitude towards
their fragile body.
Dr. Rizah Mazzuin Razali, a geriatrician in Kuala Lumpur Hospital, in her article “Fixing the
antic”, shares her experience with a 79 year-old patient exemplifies situations that older people
could face as they seek medical attention for their endless aches and pain. This could have
been prevented earlier if geriatric conditions were given more attention especially with large
numbers of healthcare providers being churned out of our institutions, the younger practitioners
need to be reminded of special needs of such patients they would increasingly encounter.
To address situations where elderly patients often suffer from multiple co-morbidities that
require multiple and duplicative medicines, pharmacist Yen Sze Whey reminds us of simple yet
effective ways of ensuring care and minimising medication errors. Home Medication Review by
a multi-disciplinary team undertaken by the Ministry is another effort to optimise medication
therapy in geriatric patients, more importantly to ensure they do not become innocent victims of
malfunctioning system and neglect. Do take note of the "High-Tech" Pill that can be welcoming
to both patients and caregivers.
Finally, the Medication Safety Newsletter Editorial members would like to wish all our readers
“Happy New Year”. Hope you all enjoy reading this issue.

Page 3Medication Safety Newsletter Vol 6 Issue 2 December 2014
Are we doing it right??
Lack of information on the drugs side-effects and
identifying patients at risk are common causes of
elderly hospitalization. When prescribing medications
to the elderly, age and frailty are major determinants
for severe adverse drug reactions1. Hélène Peyriere
et al2 in her prospective study found that significant
hospital admissions among elderly secondary to
adverse drug reactions were actually avoidable. Cost
of care from iatrogenicities is expensive3, but to subject
patients to poor quality of life is even more! So, take
time to think thoroughly before you take that pen and
scribble down the prescription for your elderly patient.
So the questions now are: Does she need the
Amitriptyline in the first place? Does the possible side-
effects including dizziness were considered before she
was given the medication? Was the GP aware that
she developed dizziness as a side-effect of
Amitriptyline and that Prochloperazine can induce
postural hypotension especially in elderly?
After several visits, the persistent symptoms with
absence of significant physical examinations and
OGDS findings, she was deemed to be somewhat
anxious and was prescribed Amitriptyline. She was
then discharged from the clinic to be followed up at
outpatient department. After a few days, she developed
severe dizziness, especially in the morning. She
sought treatment from a GP who then prescribed her
Prochloperazine. The dizziness seems to become less
initially but several days later, the dizziness recurred
and got worse especially when she stood up to walk.
The story became tragic as she had a fall from the
dizziness and fractured her hip. She then underwent
hip surgery and was warded for weeks as she was
confused and contracted nosocomial infection. The
prolonged hospital stay had caused her to be
depressed and withdrawn. She became weak and
malnourished as she refused to eat, functionally
declined and became bed bound. The marked
deterioration of her condition has led her daughter
have her condition re-examined. She was given
Mirtazepine and was rehabilitated over a period of 14
months. At last, the robust lady recovered from the
complications and had become totally independent.
Reference
1) Graziano Onder et al, Adverse Drug Reactions as Cause of Hospital
Admissions: Results from the Italian Group of Pharmacoepidemiology in the
Elderly (GIFA), Journal of the American Geriatrics Society, December 2002,
vol 50, Issue 12, 1962–68,
2) Hélène Peyriere et al, Adverse Drug Events Associated with Hospital
Admission, The Annals of Pharmacotherapy, January 2003, vol. 37 no. 1 5-
11
3) Patrick Haentjens et al, The Economic Cost of Hip Fractures Among
Elderly Women : A One-Year, Prospective, Observational Cohort Study with
Matched-Pair Analysis, J Bone Joint Surg Am, 2001 Apr 01;83(4):493-493
>> from front page
Home Medication Review
The transformation of pharmacyservices over the years hasbroadened the scope ofpharmacists from being responsiblefor the supply of medicines to amore patient-centred care.Pharmacists involvement in patientcare has contributed towardsimproving health and economicoutcomes, enhancing quality of life,minimizing the incidence ofmedicines-related adverse eventsand reducing morbidity andmortality rates.
Home Medication Review (HMR)was introduced by the Ministry ofHealth in 2006. This service, whichfocuses mainly on stroke,psychiatric and geriatric patients,provides a platform for thehealthcare providers in managingchronic patients with complicatedpharmacotherapy issues. Patientswith these illnesses usually havedeteriorated functionalities and tendto encounter difficulties whenmanaging medications bythemselves.
The Geriatric Department, HospitalKuala Lumpur started home visitservices involving doctors, nurses,physiotherapists and occupationaltherapists since 2006. In 2009,pharmacists were also involved inthe geriatric multidisciplinary team.The pharmacist’s role is to identifymedication related problems (MRP),perform medication reconciliationsand educate patients and/orcaregivers on the Quality Use ofMedicines (QUM). Throughthorough medication reviewsconducted by pharmacists, drugtreatment received by patients canbe optimized.
By Hadijah Mohd Taib, Rosmaliah Alias & Jacqueline Wong Hui YiPharmacists, Kuala Lumpur Hospital
Ho
me
Vis
it P
roce
ss
Pre Visit – Identify case Visit day- Reconcile medications Post Visit – Discussion on MRP
Medication Related Problem (MRP)
(A) Management of medication
Stock
Storage
Administration
How?
Who?
(B) Use of medication
Polypharmacy
Adherence MMAS*
Knowledge DFIT*
ADR
Page 4 Medication Safety Newsletter Vol 6 Issue 2 December 2014
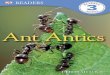
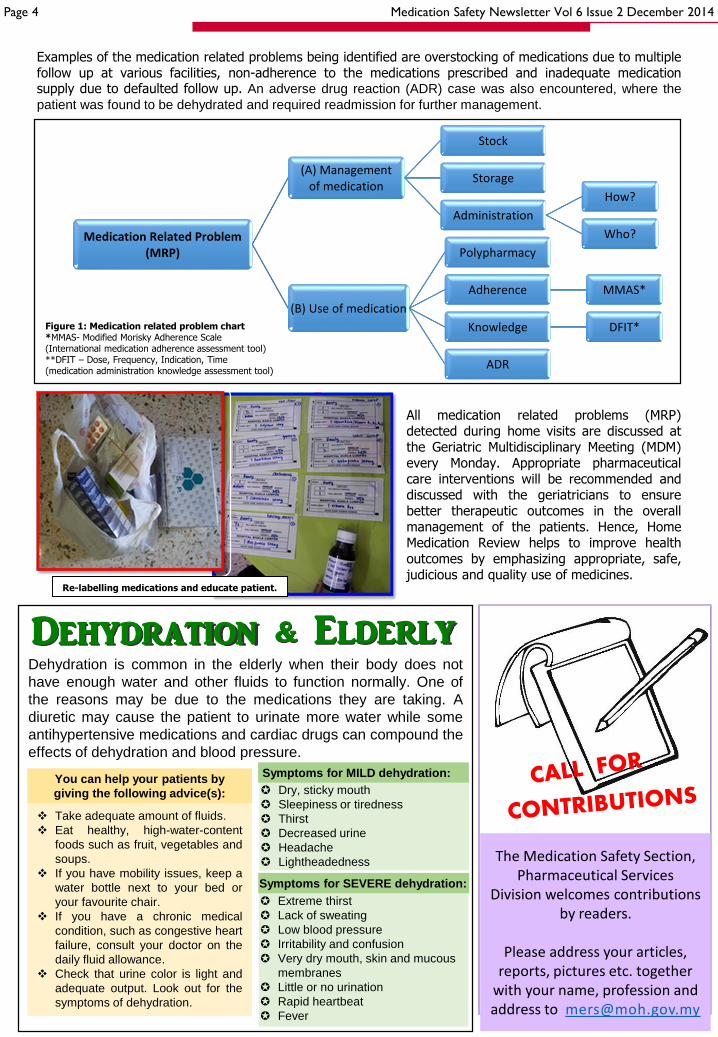
Examples of the medication related problems being identified are overstocking of medications due to multiplefollow up at various facilities, non-adherence to the medications prescribed and inadequate medicationsupply due to defaulted follow up. An adverse drug reaction (ADR) case was also encountered, where the
patient was found to be dehydrated and required readmission for further management.
Figure 1: Medication related problem chart*MMAS- Modified Morisky Adherence Scale (International medication adherence assessment tool)**DFIT – Dose, Frequency, Indication, Time (medication administration knowledge assessment tool)
All medication related problems (MRP)detected during home visits are discussed atthe Geriatric Multidisciplinary Meeting (MDM)every Monday. Appropriate pharmaceuticalcare interventions will be recommended anddiscussed with the geriatricians to ensurebetter therapeutic outcomes in the overallmanagement of the patients. Hence, HomeMedication Review helps to improve healthoutcomes by emphasizing appropriate, safe,judicious and quality use of medicines.
Re-labelling medications and educate patient.
The Medication Safety Section, Pharmaceutical Services
Division welcomes contributions by readers.
Please address your articles, reports, pictures etc. together
with your name, profession and address to [email protected]
Dehydration is common in the elderly when their body does not
have enough water and other fluids to function normally. One of
the reasons may be due to the medications they are taking. A
diuretic may cause the patient to urinate more water while some
antihypertensive medications and cardiac drugs can compound the
effects of dehydration and blood pressure.
Take adequate amount of fluids.
Eat healthy, high-water-content
foods such as fruit, vegetables and
soups.
If you have mobility issues, keep a
water bottle next to your bed or
your favourite chair.
If you have a chronic medical
condition, such as congestive heart
failure, consult your doctor on the
daily fluid allowance.
Check that urine color is light and
adequate output. Look out for the
symptoms of dehydration.
You can help your patients by
giving the following advice(s):
Extreme thirst
Lack of sweating
Low blood pressure
Irritability and confusion
Very dry mouth, skin and mucous
membranes
Little or no urination
Rapid heartbeat
Fever
Symptoms for SEVERE dehydration:
Dry, sticky mouth
Sleepiness or tiredness
Thirst
Decreased urine
Headache
Lightheadedness
Symptoms for MILD dehydration:
Dehydration & Elderly
Use of Tall Man lettering to reduce the confusionbetween similar drug names. Tall Man (uppercase)letters are used within a drug name to highlight itsprimary dissimilarities and help to differentiate look-alike names.1 Studies have shown that Tall Manlettering can draw the attention to the highlightingsections of the drug names making them less prone tomix-ups.2,3
Page 5Medication Safety Newsletter Vol 6 Issue 2 December 2014
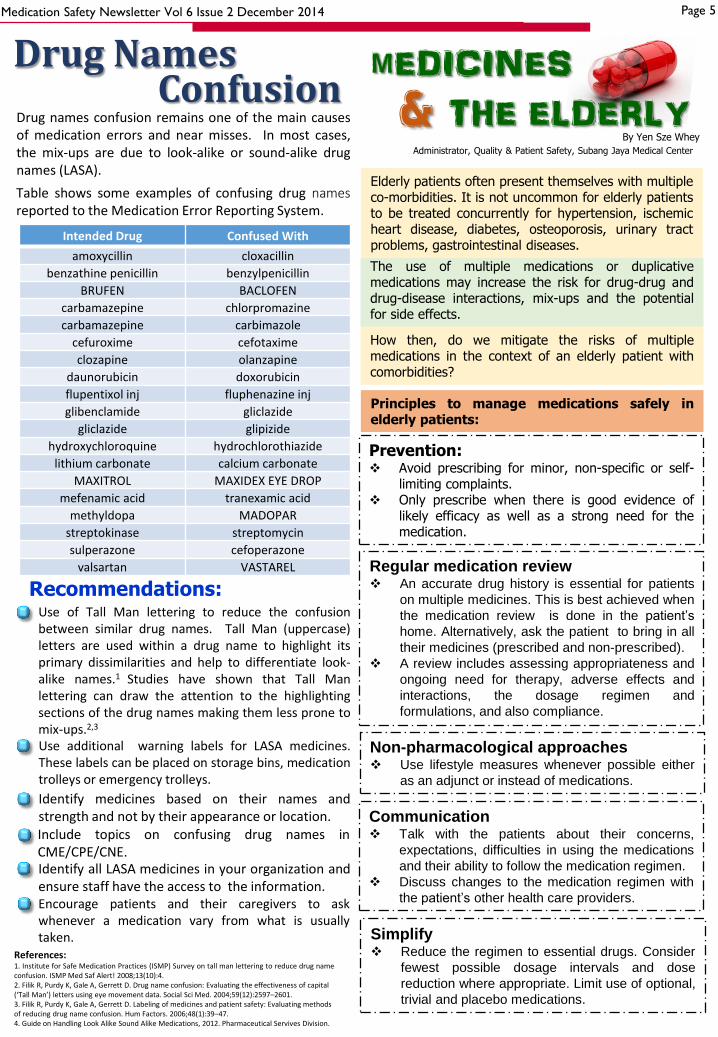
Drug names confusion remains one of the main causesof medication errors and near misses. In most cases,the mix-ups are due to look-alike or sound-alike drugnames (LASA).
Table shows some examples of confusing drug namesreported to the Medication Error Reporting System.
Intended Drug Confused With
amoxycillin cloxacillin
benzathine penicillin benzylpenicillin
BRUFEN BACLOFEN
carbamazepine chlorpromazine
carbamazepine carbimazole
cefuroxime cefotaxime
clozapine olanzapine
daunorubicin doxorubicin
flupentixol inj fluphenazine inj
glibenclamide gliclazide
gliclazide glipizide
hydroxychloroquine hydrochlorothiazide
lithium carbonate calcium carbonate
MAXITROL MAXIDEX EYE DROP
mefenamic acid tranexamic acid
methyldopa MADOPAR
streptokinase streptomycin
sulperazone cefoperazone
valsartan VASTAREL
Use additional warning labels for LASA medicines.These labels can be placed on storage bins, medicationtrolleys or emergency trolleys.
Identify medicines based on their names andstrength and not by their appearance or location.
Identify all LASA medicines in your organization andensure staff have the access to the information.
Include topics on confusing drug names inCME/CPE/CNE.
Encourage patients and their caregivers to askwhenever a medication vary from what is usuallytaken.
1. Institute for Safe Medication Practices (ISMP) Survey on tall man lettering to reduce drug nameconfusion. ISMP Med Saf Alert! 2008;13(10):4.2. Filik R, Purdy K, Gale A, Gerrett D. Drug name confusion: Evaluating the effectiveness of capital (‘Tall Man’) letters using eye movement data. Social Sci Med. 2004;59(12):2597–2601. 3. Filik R, Purdy K, Gale A, Gerrett D. Labeling of medicines and patient safety: Evaluating methods of reducing drug name confusion. Hum Factors. 2006;48(1):39–47. 4. Guide on Handling Look Alike Sound Alike Medications, 2012. Pharmaceutical Servives Division.
Recommendations:
References:
Drug NamesConfusion
The use of multiple medications or duplicativemedications may increase the risk for drug-drug anddrug-disease interactions, mix-ups and the potentialfor side effects.
Elderly patients often present themselves with multipleco-morbidities. It is not uncommon for elderly patientsto be treated concurrently for hypertension, ischemicheart disease, diabetes, osteoporosis, urinary tractproblems, gastrointestinal diseases.
mEDICINES& THE ELDERLY
By Yen Sze Whey
Administrator, Quality & Patient Safety, Subang Jaya Medical Center
How then, do we mitigate the risks of multiplemedications in the context of an elderly patient withcomorbidities?
Principles to manage medications safely inelderly patients:
Prevention: Avoid prescribing for minor, non-specific or self-
limiting complaints. Only prescribe when there is good evidence of
likely efficacy as well as a strong need for themedication.
Regular medication review An accurate drug history is essential for patients
on multiple medicines. This is best achieved when
the medication review is done in the patient’s
home. Alternatively, ask the patient to bring in all
their medicines (prescribed and non-prescribed).
A review includes assessing appropriateness and
ongoing need for therapy, adverse effects and
interactions, the dosage regimen and
formulations, and also compliance.
Non-pharmacological approaches Use lifestyle measures whenever possible either
as an adjunct or instead of medications.
Communication Talk with the patients about their concerns,
expectations, difficulties in using the medications
and their ability to follow the medication regimen.
Discuss changes to the medication regimen with
the patient’s other health care providers.
Simplify Reduce the regimen to essential drugs. Consider
fewest possible dosage intervals and dose
reduction where appropriate. Limit use of optional,
trivial and placebo medications.

Page 6 Medication Safety Newsletter Vol 6 Issue 2 December 2014
Training on MERS Online for StateMedication Safety Liaison Officers atComputer Lab, National PharmaceuticalControl Bureau on 8 April 2014.
A Medication Safety Course was held inBentong Hospital, Pahang on 18 April2014.
A talk on Medication Safety was held at SriKota Specialist Medical Centre on 27 August2014 in conjunction with the Safety MonthCampaign at the hospital.
The Kedah Pharmaceutical Services Division, MOH incollaboration with Malaysian Pharmaceutical Society,Kedah-Perlis Branch had organized a Medication SafetySeminar 2014 in Hotel Star City, Alor Setar on 8 June 2014.
The Root Cause Analysis Workshop 2014 was organized bythe Pharmaceutical Services Division, Ministry of Healthfrom 12 to 14 August 2014 in Concorde Inn, KLIA Sepang.
The Pharmaceutical Services Division, Penang State HealthDepartment had organized a Medication Safety Seminarwith the theme Considerations to Special Populations inPenang Hospital on 17 May 2014.
Medicat i on Safety