Embed Size (px)
Citation preview

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pathway to Patients Charting the Dynamics of the Global TB Drug Market
COMPENDIUM OF FINDINGS MAy 2007

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

Compendium |page�
may2007
PathwaytoPatientsChartingtheDynamicsoftheGlobalTBDrugMarket
Compendium of findings may2007
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

page�| TBallianCe
paThwayTopaTienTs
TableofContents
1. Preface ....................................................................................................... 4 1.1 IntroductiontotheProject. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.2 Methodology. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
2. GlobalProcurementServicesAgencies(PSAs). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 2.1 GlobalTBDrugFacility:BackgroundandRole. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.1.1 Customers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.1.2ProcurementAgentSelectionProcess. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2.1.3SupplierPre-QualificationandSelectionProcess. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2.1.4Pricing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2.1.5Suppliers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.1.6 QualityControl. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.1.7 TransportProcess. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.2 GreenLightCommittee:BackgroundandRole . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.1Customers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.2 ProcurementAgentSelectionProcess. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.3 Suppliers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.4 Pricing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.5 TransportPathway. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2.6QualityControl. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1
2.3 ConvergenceoftheGlobalTBDrugFacilityandtheGreenLightCommittee. . . . . . . . . . . . . . . . . . . 1 1
2.4 OtherGlobalPSAs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
3. CountryCaseStudies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 3.1 TBControlintheContextofNationalHealthcareSystems. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
3.1.1 HighBurdenCountries(HBCs). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.2HighIncomeCountries. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.2 OverviewofKeyTrendsImpactingTBFundingandTreatmentinHBCs. . . . . . . . . . . . . . . . . . . . . . . . .14
3.3 HBCNationalTBControlPrograms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14
3.3.1 Function. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14
3.3.2Financing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14
3.3.3Structure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.4 TreatmentofTBPatients. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.4.1HBCs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.4.2HighIncomeCountries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
3.4.3UseofFixed-DoseCombinationsinTreatmentRegimens. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
3.4.4 ServiceProvision. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
3.5 PublicSector:ReferralPathwayandSettingsofCare. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
3.5.1 HBCs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
3.5.2HighIncomeCountries. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.5.3PaymentforDrugsandServices. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.6 PrivateSector:ReferralPathwayandSettingsofCare. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.6.1 RoleofPublic-PrivateMixProgramsinTBTreatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
3.6.2 PaymentforDrugsandServicesinthePrivateSector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
3.7 MDR-TBControl . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19

Compendium |page�
may2007
4. ProcurementandDistributionofTBDrugsinHighBurdenCountries. . . . 20 4.1 FinancingforFirst-lineTBDrugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
4.1.1FinancingforSecond-lineTBDrugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
4.2 PublicDrugProcurement. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
4.2.1PublicTenderProcess . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
4.2.2DemandForecasting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22
4.2.3 DistributionPathways. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22
4.3 PrivateDrugProcurement:First-andSecond-lineDrugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
5. ProcurementandDistributionofTBDrugsinHighIncomeCountries.....25 5.1 FinancingofTBDrugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25
5.2 ProcurementofTBDrugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25
5.3 FlowofDrugs.............................................................................................25
6. CostofTreatmentofTBinBothHighBurdenandHighIncomeCountries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26
6.1 PricesofTBDrugRegimens. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
6.2 PublicandPrivatePricing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
7. ValueEstimatesForFirst-andSecond-LineTBDrugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28 7.1 OverviewofMethodology. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
7.2 Country-by-CountryEstimates. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
7.3 GlobalEstimates..........................................................................................32
8. AdditionalConsiderations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
9. PredictingFutureMarketDynamics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
10. Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
11. Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37 11.1 PartialListofAcronyms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
11.2 ListofManufacturers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
11.3 PricesofDrugsforSelectCountriesandPurchasers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
11.4 InterviewLists. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
12.Acknowledgements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46

page�| TBallianCe
paThwayTopaTienTs
1.Preface
MorethanacenturyafterthediscoveryofMycobacteriumtuberculosis(M.tb),thebacillusthatcausestuberculosis(TB),andahalf-centuryafterthediscoveryofantibioticstotreatthedisease,TBissecondonlytoHIVastheleadinginfectiouskillerofadultsworldwide.
TBkillssomeoneevery20seconds—about4,400peopleeveryday,orapproximately1.6millionin2005alone,accordingtothelatestestimatesfromtheWorldHealthOrganization(WHO).1Itaccountsformoredeathsamongwomenthanallothercausesofmaternalmortalitycombined2andistheleadinginfectiouscauseofdeathamongpeoplewithHIV/AIDS.3
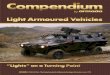
TheWHOestimatesthatonethirdoftheworld’spopulationisinfectedwithM.tb,whichcausesTB,withthegreatestburdenrelativetopopulationconcentratedinthedevelopingworld,withhighincidenceofinfectioninsub-SaharanAfrica,AsiaandSouthAmerica,asshowninFigure1.Further-more,today’sTBepidemicisfuelledbyasurgeinHIV-M.tbco-infectionandcompoundedbythegrowingemergenceofdrugresistantstrains.
Apartfromitsdevastatinghealthconsequences,theeconomicimpactofthediseaseisstaggering,makingTBasignificantcontributortoworldpoverty.TBisestimatedtoabsorbUS$12billionfromtheincomesoftheworld’spoorestcommunities.Insomecountries,lossofproductivityattributabletoTBisintheorderoffourtosevenpercentofgrossdomesticproduct.4
1 Global tuberculosis control: surveillance, planning, financing. WHO report 2007. Geneva, World Health Organization.2 Connolly M, Nunn P. Women and tuberculosis. World Health Stat Q. 1996;49:115-119.3 Frequently Asked Questions About TB and HIV. World Health Organization. http://www.who.int/tb/hiv/faq/en/. Accessed 2/27/07.4 HIV/AIDS, Tuberculosis and Malaria: The Status and Impact of the Three Diseases. The Global Fund to Fight AIDS, Tuberculosis
and Malaria, 2005.
Figure 1. Estimated Global TB Incidence (2005)
Source: Global tuberculosis control: surveillance, planning, financing. WHO report 2007. Geneva, World Health Organization.
l No Estimate
l 0-24
l 25-49l 50-99l 100-299l 300 or more

Compendium |page�
may2007
ThecurrentTBdrugregimen,aproductofthebestscientificadvancesofthe1960s,worksforactive,drug-susceptibleTB—aslongaspatientscompletethesix-tonine-monthtreatment.However,today’sfour-drugcombination,takenideallyunderdirectobservationbyahealthcareworkerorcommu-nitymember,isburdensomeforpatientsandcareprovidersalikeanddespitetheenormousadvancesinprovisionofservicesoverthepastfewyears,manypatientsdonotorcannotcompletetreatment.
Thepooradherenceandimproperadministrationofexistingantibioticshaveledtotheemergenceofmulti-andextensivelydrugresistantTBstrains,knownasMDR-TBandXDR-TB,respectively.Further,theglobalHIV/AIDSpandemicisfuellinganincreaseinTB,resultinginadramaticriseinthenumberofco-infectedindividuals.Anestimatedone-thirdofthe40millionpeoplelivingwithHIV/AIDSworldwideareco-infectedwithTB.PeoplewithHIVareupto50timesmorelikelytodevelopTBinagivenyearthanHIV-negativepeople,andTBisoneoftheleadingcausesofdeathinHIV-infectedpeople,particularlyinlowincomecountries.5Insub-SaharanAfrica,upto80percentoftuberculosispatientsarealsoHIVinfected.6Unfortunately,thecurrentTBdrugregimenisnotcompatiblewithcertaincommonantiretroviraltherapiesusedtotreatHIV/AIDS.
Criticaltofightingthisancientdiseaseisthedevelopment—andsubsequentadoption—ofaffordable,new,fasterandsimplerdrugregimens.Afteralmosthalfacenturyofvirtualinactivity,TBdrugdevelopmenthasresurged.Bolsteredbynewscientificinformationonthebacillus,transforminginternationalfundingfromphilanthropicsectorsandgovernmentdonors,andtheappearanceofinnovativebusinessmodelsdesignedtobreachthedrugdevelopmentgap,thecurrentglobalTBdrugpipelineisthelargestinhistory.
ExperiencehasdemonstratedthatattritionratesareveryhighindrugdevelopmentanditisexpectedthatTBdrugswillbenoexception.However,thestrengthoftheportfoliounderscoresthefactthatevenmorenewTBdrugcandidatesandnoveldrugregimensarelikelytobeforthcomingwithinthenextfivetotenyears.
Experiencehasalsodemonstratedthattheuptakeofinnovationisaprocessthatrequiresunderstanding
ofmarketforces,distributionchannels,purchasingpowerandmyriadotherconsiderations.ThepromisingnewTBcureswillbeineffectiveandtheresurgentmovementforTBdrugdevelopmentwillhavefailedifthenewtreatmentsdonotreachpatients.
In2006,theGlobalAllianceforTBDrugDevelopment(TBAlliance)commissionedPathway to Patients: Charting the Dynamics of the Global TB Drug Market.Thestudyisthefirstcomprehensiveanalysisofhowtoday’sTBdrugsreachpatientsonaglobalscale.Itincludesanassessmentoftenstrategicallyselectedcountries—Brazil,China,France,India,Indonesia,Japan,thePhilippines,SouthAfrica,theUKandtheUS—aswellasanappraisaloftoday’sworldwideTBdrugmarketvalue.
ThiscompendiumisadigestofinformationgatheredfromPathway to Patientsanddetailsthepricing,purchasing,procurementanddistributionmechanismsforfirst-andsecond-lineTBtreatmentsinthesecountries.Inaddition,thestudyupdatestheoriginalglobaldrugmarketassessmentcarriedoutbytheTBAlliancein2001inThe Economics of TB Drug Development .7
TheresearchforPathway to PatientswasconductedinpartnershipwithIMSHealth,Inc.,aglobalstrate-gicconsultinggroupfocusedonthepharmaceuticalandhealthcareindustries.TheprojectwasfinancedbyagrantfromtheNetherlandsMinistryofForeignAffairs’DepartmentofDevelopmentCooperation(DGIS)andwiththesupportoftheBill&MelindaGatesFoundation.Anabridgedoverviewofthesefindingsandaseparatemethodologydocumentareavailableonlineatwww.tballiance.org.
1.1 Introduction to the Project
Ofthetencountriesstudied,sixwerechosenfromamongthe22identifiedbytheWHOashighburdencountries(HBCs):Brazil,China,India,Indonesia,thePhilippines,andSouthAfrica.Together,thesecountriescarryapproximately50percentoftheworld’sTBburden.8Theprojectalsoencompassedfourhighincomecountries,France,Japan,theUKandUS.Althoughthelatterhavealowburdenofdisease,theyrepresentasignificantvalueoftheTBmarketbecauseofhighercostoftreatment.Thesecountriesareofparticularinteresttodrug
5 Frequently Asked Questions About TB and HIV. World Health Organization. http://www.who.int/tb/hiv/faq/en/. Accessed 2/27/07.6 Reid A, Scano F, Getahun H, et. al. Towards universal access to HIV prevention, treatment, care, and support: the role of tuberculosis/HIV
collaboration. Lancet 2006 ; 6: 483-495.7 The Economics of TB Drug Development. Global Alliance for TB Drug Development. October, 2001.8 Global tuberculosis control: surveillance, planning, financing. WHO report 2007. Geneva, World Health Organization.

page�| TBallianCe
paThwayTopaTienTs
manufacturersbecausetheyaccountfor61percentofthetotalglobalmarketforallpharmaceuticals.9Moreover,theywerechosenbecausetheyreflectdifferentgeographies,differentpricinganddifferenthealthsystemsstructures.
Forthestudy,researchonIndonesiaandJapanwaslimitedtodeterminingmarketvalueanddidnotexamineprocurementanddistribution.
1.2 Methodology10
Themethodologyusedinthestudyallowedforbothqualitativeandquantitativeanalyses.Qualita-tivecharacterizationoftheTBmarketincludedmappingtheflowofTBmedicinesfromthesuppliertothepatient,theselectionprocessforsuppliers,andtheroleofpublicandprivatepayersforfirst-andsecond-lineTBmedicines.Qualitativeanalysisalsoincludedthefollowingsteps:
1.Primaryresearchwasconductedthroughface-to-faceinterviewswithglobalandcountrystakehold-ersbytelephoneandinperson,includingstaffattheWHO,theStopTBPartnership,andnationalandlocalstafffromTBcontrolprogramsofthecountriesstudied
2.SecondarydatawerecollectedfromanumberofpubliclyavailablesourcesaccessedthroughsearchenginesanddirectlyfromtheWHOwebsite
3.Additionaldataandreportswerecollectedfromindividualstakeholdersfollowingdiscussions
Quantitativecharacterizationofthefirst-andsecond-linepublicTBdrugmarketsfocusedonmeasuringtheactualvalue(definedasmarketvalue)inthepublicandprivatesectors.Datawerecollectedfromseveralsecondarysources:
1.IMSHealthdatabasesprovidedinformationonvalueandunitssoldintheprivatemarketinallcountrieswhereaprivateTBmarketexists(China,India,Japan,thePhilippinesandtheUS)andthepublicmarketinsomecountries(France,SouthAfrica,theUKandtheUS)
2.Globalorganizationsprovideddataoncostsandsupplyofproductsbothgloballyandatthecountrylevel
3.ProductsuppliersprovideddataoncostsandsalesofTBproductssold
4.NationalTBcontrolprogramsinthecountriesstudiedprovideddataonthenumberofpatientstreatedinthepublicsector,fundingfordrugprocurement,andcostsperproductandregimeninthepublicsector
Fortheprivatefirst-andsecond-linemarkets,IMSHealthdatabaseswereusedwhereavailable(e.g.India)toestimatevalue.Valueestimatesarebasedontheactualvalueofdrugssoldintheprivatemarketplace.Recognizingthatmanysecond-linedrugsareusedforindicationsotherthanTB,prescriptiondatawereusedtoadjustthosefiguressothattheymorecloselyreflectedthevalueofsecond-linedrugsusedforTBspecifically.First-linedrugvaluefigureswereleftunadjustedbecausetheprescriptiondataindicatedthatonlyamarginalfractionofthosedrugsinthecountriesstudiedwerebeingusedforindicationsotherthanTB.
Estimatesofpatientvolumeintheprivatesectorcouldnotbeobtainedforeitherfirst-orsecond-linedrugsbecausepatientadherenceandtreatmentpractices,aswellasrecordkeeping,variedgreatlybetweenandwithincountries.Therefore,patientvolumesareonlyprovidedforpublic-sectorprograms.
Thepublic-sectordrugbudgetfiguresandthepricepertreatmentregimenestimatesdescribedinthisreportmaydifferslightlyfromthosereportedinthe2006WHOreportGlobal Tuberculosis: Surveillance, Planning, and Financing.ThisisbecauseresearchfortheWHOreportandforPathway to Patientsweregatheredatdifferenttimes.FiguresreportedtotheWHOmayhavebeenbasedonprojectionsfor2005,whereastheresearchinthisstudywasprimarilybasedonactualexpendituresfor2005.Moreover,where2005datawerenotavailableforthisreport,researchersreliedon2004datainstead.11Becausethefiguresaregatheredusingthesamemethodologyfromyeartoyear,thecombinationofdatafromconsecutiveyearswasdeterminedtobeappropriate.
ItshouldalsobenotedthatthestudydidnotseektorevieworaddressthequalityofTBtreatmentorthequalityofprocurementanddistributioninanyofthecountriesstudied.
9 IMS Knowledge Link. http://www.imsknowledgelink.com.10 For full information about the specific methodology used to determine the market estimates for each country and the global estimates, including
individual drug cost figures and a list of the countries included in the global extrapolation, a separate methodology document is available online at www.tballiance.org.
11 Discussions with Kathryn Floyd, WHO, October 2006.

Compendium |page�
may2007
2.GlobalProcurementServicesAgencies
Anumberoforganizationsknownasprocurementservicesagencies(PSAs)existatthegloballeveltoassistcountriesand/ororganizationsinsupplyingdrugstotheirrespectiveTBprograms.TheseincludeagenciesthatarededicatedspecificallytoTBdrugprocurement,suchastheStopTBPartnership’sGlobalTBDrugFacility(GDF)andGreenLightCommittee(GLC),orthosethatprocurearangeofproducts,suchasCrownAgentsortheIDAFoundation.Insomecountriesnon-governmentorganizations(NGOs)alsoprocureTBdrugs,eitherfortheirownprogramsorforthegeographicregioninwhichtheyoperate.Pathway to PatientsfocusedontwoofthePSAsengagedinprocurementinHBCs:TheGDFandtheGLC.12
2.1 Global TB Drug Facility: Background and Role
HousedattheWHOheadquartersinGeneva,SwitzerlandandmanagedbytheStopTBPartner-shipSecretariat,theGDFwasinitiatedin2001inresponsetothedifficultiesexperiencedbycountriesinfindingandfundingstableTBdrugsupplies.Itsstatedmissionis“toexpandaccessto,andavailabilityof,high-qualityTBdrugstofacilitateDOTSexpansion.”13
TheGDFseekstodirectlyaddressseveralproblemscountriesmayfaceintheprocurementofTBmedication,includinglackoffinancialresources,inefficientprocurementmechanisms,poorqualityassurancesystemsandinadequatein-countrymanagementandmonitoring.Forcountriesthatlacktheresourcestofunddrugprocurement,theGDFoffersin-kindgrantservices.Forcountriesthatcanaffordtopurchasedrugs,theGDFalsooffersdirectprocurementservices.Forallcountries,itofferspre-qualificationservicestoensureadequatequalitycontrolmechanismsandprovidesin-countrymonitoringandtechnicalsupporttoimproveandmaintainhigh-qualitydrugsupply,management,anddistributionprocesses.
Asdescribedinthissection,orderingTBmedicinesthroughtheGDFisamulti-stepprocess.ThepurchasermustapproachtheGDFwithrequestsfor
TBdrugs.TheGDFthenconfirmstheeligibilityofthepurchaserandforwardstheordertoaselectedprocurementagent.Theprocurementagentplacestheorderwithsuppliersthathavewonaninterna-tionalcompetitivebid.Finally,themajorityofordersareforwardedtotheprimarysuppliernamedinthebidand,ifnecessary,asecondarysupplierisusedtoprovideadditionalvolumes.
2.1.1 CustomersGDFcustomersfallintooneoftwocategories,purchasersorgrantees.
Purchasers (mostoftenhealthministries)obtaindrugsfromtheGDFthroughdirectprocurement.Incountrieswherethenationalgovernmentdoesnotplayacentralroleinprocurement,stateorprovincialhealthministriesorNGOssuchasPartnersinHealth(PIH)orMédecinsSansFrontières(MSF)mayserveasprimarypurchasers.
CountriesseekingtoprocuredrugsthroughtheGDF’sdirectprocurementprocessmustfirstbeapproved.Eligiblecountriesororganizationsinclude:
• CountriesthatimplementWHO-recommendedDOTSstrategyin90percentormoreofthepopulation
• NGOsthatsupportDOTSstrategyinthesecountries
• CountriesorNGOsapprovedbytheGDFforTBdruggrants
• CountriesorNGOsapprovedforagrantforTBcontrolbytheGlobalFundtoFightAIDS,TuberculosisandMalaria(GFATM)
• Organizations,donorsandtechnicalagenciessupportingthesecountriesorNGOs14
ThevaluetoclientsoftheGDF’sdirectprocure-mentservicesvariesdependingonthecapabilitiesandneedsofeachcountry.Forthemostpart,theGDF’svaluepropositionismeasuredinitsabilitytoassistcountriesthatdonothavesufficient,reliablequalitycontrol,and/orefficientinternalpurchasingorproductioncapabilities.Forsomecountries,priceandpackagingarealsoviewedasanattribute.
12 In early 2006, the GDF announced that it would converge with the GLC. Procurement functions of the GDF and GLC already have been combined. Plans to combine their application, review, monitoring, and evaluation functions are currently underway. For more information about the GDF/GLC convergence, see section 2.3 of this report.
13 Stop TB Partnership. http://www.stoptb.org/gdf/whatis/what_is.asp. Accessed 2/28/07.14 As per “Global Drug Facility: An Introduction”. Available in PDF format:
www.stoptb.org/gdf/documents/FS%20GDF%20An%20Introduction_June06.pdf.

page�| TBallianCe
paThwayTopaTienTs
GranteesincludecountriesthatlackfinancialresourcestoprocureTBmedicinesandinsteadreceivein-kindgrantsintheformoffreedrugs.Granteesreceivingdrugsmustmeetalleligibilityrequirementsfordirectprocurementaswellasthefollowingcriteria:
• Annualpercapitagrossnationalincome(GNI)underUS$3,000
• AnationalplanandbudgetallocationforDOTSexpansiontomeetglobalTBcontroltargets
• TechnicalguidelinesdemonstratingcommitmenttomeetglobalTBcontroltargets
• CompletionofanannualreportonDOTSperformance(WHOTBcollectionform)
• MusthavereceivedarecentexternalnationalTBprogramreview15
AsshowninFigure2,theGDFsuppliesfirst-lineTBdrugsto13ofthe22WHO-designatedhighburdencountries.However,ofthecountriesforwhichprocurementwasstudied,onlyIndiaandthePhilippinescurrentlyusetheGDF,andevenforthesecountries,first-linedrugsarealsosourcedthroughpublictenderprocesses.
2.1.2 Procurement Agent Selection ProcessTheGDFdoesnotprocureTBmedicinesonitsown.Instead,itservesasascreenerandbrokerbetweensuppliersandpurchasers.ItfirstidentifiesagenciesandorganizationsbestsuitedtoperformtheTBdrugprocurementanddistributionfunction.
Afterformingcontractualrelationshipswiththeseorganizations,theGDFseekstomatcheligiblecountrieswiththem.Indoingso,itfacilitatesaccesstoanuninterruptedsupplyofconcessionally-priced,high-qualityTBdrugs.
Figure3ontheoppositepagedescribestheprocessthroughwhichtheGDFselectsaprocurementagent.Theprocurementagentthenbecomesresponsibleforsub-contractingotherpartnersforqualitycontrolandfreight-forwardingfunctions.
SincetheinceptionoftheGDF,itsprimaryprocure-mentagenthasbeentheInter-AgencyProcurementServicesoftheUnitedNationsDevelopmentProgramme(UNDP-IAPSO).In2006,theservicewasre-bidandtheGermanAgencyforTechnicalCooperation(GTZ)wasselectedasthenewprocure-mentagent,contractedforaperiodoftwoyears.
2.1.3 Supplier Pre-Qualification and Selection Process InordertobeeligibletosupplydrugstotheGDF,suppliersmustbeassessedbytheWHO.ManufacturingsitesmustcomplywiththeWHO’sGoodManufacturingPractices(GMP)standards.TheymustthenmeetWHO/PSM16pre-qualificationrequirements.17Theselectionprocessforapprovedsuppliersisthencarriedoutbytheprocurementagentthroughanannualinternationalcompetitivebiddingprocess.
Typically,theprocurementagentselectstwosuppli-ersforeachproduct—aprimaryandasecondarysource.Theprimarysupplierisusuallyawarded65percentoftheannualsupplyandthesecondary,35percent.Pricesofferedbythesecondarysupplieraretypicallyhigher.TheawardperiodforeachproductistypicallyoneyearandisspecifiedinaLongTermAgreement(LTA).
2.1.4 PricingAnumberoffactorscancausethecostofGDF-sourcedtreatmentstofluctuate.Priceshaveincreasedinrecentyears,inpartbecausetheyarenotguaranteedorstabilizedduringthecompetitivebiddingprocess.18Also,thecostofgoodsofsomerawmaterialsrequiredtomanufactureTBdrugshasincreased.Furthermore,astheGDFincreasesthenumberofcountriesitserves,itexhauststhesupplyfromprimarysuppliers.Itmustthenrelyonthe
15 Stop TB Partnership Global Drug Facility: www.stoptb.org/gdf/applying/application_documents.asp.16 Medicines Policy and Standards (PSM).17 The specific prequalification standards for TB drugs are determined by the Procurement, Quality and Sourcing Project: Access to Anti-
Tuberculosis Drugs of Acceptable Quality (TB Prequalification Project). This project was initiated in 2002 by the WHO Department of Medicine and Policy Standards: Quality Assurance and Safety of Medicines (PSM/QSM) to facilitate access to anti-TB drugs of acceptable quality through the assessment of products and manufacturers for adherence with WHO-recommended standards.
18 Stakeholder discussions with GDF, UNDP-IAPSO, 2006; information also available online in PDF format: www.stoptb.org/gdf/documents/GDFFactBrief_April2005.pdf
* Do not purchase TB drugs or receive grants of drugs through the GDF
1. India
2. China*
3. Indonesia
4. Nigeria
5. Bangladesh
6. Pakistan
7. Ethiopia*
8. South Africa*
9. Phillipines
10. Kenya
11. DR Congo
12. Russian Federation*
13. Vietnam*
14. Tanzania
15. Brazil*
16. Uganda
17. Thailand*
18. Mozambique
19. Zimbabwe*
20. Myanmar
21. Afganistan
22. Cambodia*
Figure 2. WHO 22 High Burden Countries Based on GDF Supply

Compendium |page�
may2007
secondarysupplier,thusincreasingtheaveragepriceofthestandardfirst-lineregimen.
2.1.5 SuppliersInresponsetoincreasesinpricesanddecreasesinavailablesupply,theGDFissuedanewtenderforadditionalmanufacturersinMarch,2005.Theresultwasanincreaseinsuppliersfromthreecompaniestofour:Lupin,Cadila,Svizera,andStrides-Sandoz.19
2.1.6 Quality Control Beforeproductsareshippedtothepurchaser,ordersmustmeetspecificqualitycontrolstandardsdeterminedbytheGDF.Thequalitycontrolprocessincludespre-shipmentinspection(PSI)andlabora-torybatchtestingoftheproduct.Bothstepsaresub-contractedbytheprocurementagent.TheGDFappointsaqualitycontrolagentwhoisresponsibleforensuringthatanordermeetsGDFstandards.Thebatchtestisconductedbyasub-contractedqualitycontrollaboratory.
Beforeanorderisshipped,suppliersarerequiredtonotifyadesignatedagentthattheorderisready.ThesuppliermustthensubmitasampleoftheproducttotheGDFforqualitycontrol.Alocalagentissenttothesupplierfacilitytoevaluateproductpackagingandlabelingandreporttheresultstothequalitycontrolagent.Asampleofeachproductbatchisthensenttoalaboratoryfortesting.Thelaboratoryalsoreportsitsresultstothequalitycontrolagent.
OnceitisconfirmedthatanordermeetsalloftheGDF’sspecifications,thequalitycontrolagentnotifiestheprocurementagenttoreleasetheshipmenttoafreightforwarder.20
2.1.7 Transport ProcessOncethequalityoftheorderhasbeenassessed,afreightforwarderthathasbeencontractedbytheprocurementagentisnotifiedthattheorderisreadyforshipment.Thefreightforwarderpicksuptheorderfromthesupplierfacilityand,ifallproductsinthecountry’sorderarebeingsourcedfromonemanufacturer,theorderistransporteddirectlytothepurchaser.Iftheyarebeingsourcedfrommultiplemanufacturers,allproductsaretransportedtoaconsolidationpointwhereordersareassembledpriortobeingsenttothepurchaser.Oncetheorderhasbeentransported,thedistributionofdrugsbecomestheresponsibilityofthepurchaser.
Thequalitycontrolandtransportationprocessesarethesamewhentherecipientisagrantee.However,underthedirect-procurementmechanism,purchasershavetheoptionofspecifyingwheretheywouldliketheirordersshipped,andarebilledforthisservice.Conversely,whentheGDFisprocessingagrant,theorderisshippedtothecountry’sportofentryonly.Onceordershavebeenreceived,theGDFusuallyconductsafollow-upassessmentwithinfourtosixmonthstoensurethedrugsarebeingusedappropriately.
Figure 3: GDF Procurement Agent Selection Process
GDF invites expressions of interest
GDF issues an invitation for expressions of interest from potential procurement agents
Candidates submit preliminary application
Procurement agents outline the following:
• Experience in pharmaceutical procurement
• Experience in issuing international competitive bids
• Ability to maintain an Internet-based data collection and processing system
• Ability to manage buffer stock
GDF issues request for proposals/bids
Procurement agents who meet the minimum requirements are then asked to submit proposals to the GDF
Selection of Procurement Agent
GDF selects the procurement agent based on its capabilities and mark-up
19 Tender procedures and criteria can be found online in PDF format: www.stoptb.org/gdf/assets/documents/GDFFactBrief_April2005.pdf20 Stakeholder discussions with GDF, UNDP-IAPSO, 2006.

page�0| TBallianCe
paThwayTopaTienTs
2.2 Green Light Committee: Background and Role
Asnotedintheintroduction,casesofdrugresistantTBarebecomingincreasinglycommonacrosstheglobe.Becausethecostoftreatingthesepatientsisabarriertoreceivingcare,astrategyknownasDOTS-PluswaslaunchedbytheWHOin1998.Aspartofthisstrategy,theGLCwasformedin2000toservesasaglobalsupplierofsecond-linedrugstotreatMDR-TB.TheGLCmeetssixtimesayeartoassessapplicationsfromDOTS-Pluspilotprograms,determinesifaprogramisincompliancewiththeGuidelinesforEstablishingDOTS-PlusPilotProjectsfortheManagementofMDR-TB,andprovidesaccesstoaffordablypricedsecond-lineTBdrugstoapprovedprograms.2122
2.2.1 CustomersTheGLCacceptsapplicantsfromanyprogram,agencyororganizationthatfulfillsseveralcriteria.23Theymust:
•EnsurethattheDOTSstrategyisinplaceandisfunctioningwell
•Securegovernmentcommitmentandadequatefunding
• Developacoordinatedprojectmanagementplan• Demonstratethattheyhaveadequate
laboratoryresources• Devisearationaltreatmentstrategy•Developanadequateinformation
managementsystem•Confirmthatthedrugsrequestedareregistered
inthecountryoftheproject•Developadrugmanagementplanincluding
transportation,registration,customsprocedures,storage,distribution,monitoringandreporting
Eachapplicationmustbecompletedwiththefollowinginformation:
•Location•Sizeofpatientcohort•Anticipatedstartdateanddurationofprogram• Timescheduleforinclusionofpatientsduring
thepilotproject•Listofallorganizationsinvolved• JustificationoftheneedforaDOTS-Plus
pilotproject
Projectsmustalsofacilitateasitevisituponrequest.
Eachprogramisapprovedforasetnumberofpatients.Oncetheprogramhasmetitsquota,itmustreapplyforexpansion.Through2005,programsrepresentingapproximately9,000patientsworldwidewereapprovedbytheGLC.MorethanhalfofthosepatientswereinPerualone.24
2.2.2 Procurement Agent Selection ProcessTheprimaryprocurementagentservingtheGLCtodayistheIDAFoundation(IDA)25,whichhandlesdrugprocurement,qualitycontrol,andtransportation.IDA’sprimaryresponsibilityistoen-sureahigh-qualityandaffordablesupplyofsecond-linedrugsisavailablebynegotiatingpricesdirectlywithsuppliersfromalistofeligiblemanufacturersanddrugsthathavebeenassessedbytheWHOand/orGLC.IDAplaysakeyroleinqualitycontrolbyassessingpotentialmanufacturersandconduct-ingitsownqualitycontrolofprocureddrugs.Inaddition,IDAstandardizespacking,labelingandproductinformationspecificationsforgenericdrugs.Finally,IDAisresponsiblefortransportingdrugstopurchasers’portsofentryorairports.
2.2.3 Suppliers Becausemanysecond-linedrugsarepatent-protectedorareproducedbyalimitednumberofqualifiedsuppliers,neithertheGLCnorIDAcurrentlyusebidstoprocureitsdrugs.Instead,IDAapproachesmanufacturerswhoproducesecond-lineTBdrugsandformsagreementsdirectlywiththemforreducedpriceproducts.Duringitsinteractionswithpotentialsuppliers,IDAattemptstonegotiatethelowestpricepossibleforgenericdrugsor,inthecaseofbrandeddrugs,aconcessionalpricethatisaffordabletoitscustomers.ThemanufacturermayormaynotspecifyamaximumvolumeofreducedpricedrugsthatitwillprovidetotheGLC.
2.2.4 PricingTable1ontheoppositepagedescribesthepricesofsecond-lineTBdrugsofferedthroughtheGLCin2006,aswellasthecompaniesthatmanufacturethem.
2.2.5 Transport PathwayThefirststepofGLCprocurementisanapplicationprocessthatallpotentialpurchasersmustundergo.
21 Rajesh Gupta et al., Increasing transparency in partnerships for health – Introducing the Green Light Committee, Tropical Medicine and International Health, 2002; Stakeholder interviews, 2006.
22 As noted previously, the GLC recently converged with the GDF. Drugs procured on behalf of projects approved by the GLC will now be supplied through the the GDF procurement mechanism.
23 “Instructions for Applying to the Green Light Committee for Access to 2nd line Anti-tuberculosis Drugs”, 2002. whqlibdoc.who.int/hq/2006/WHO_HTM_TB_2006.369_eng.pdf
24 Data provided by the GLC, 2006.25 GLC’s most recent tender process was held in 2006. IDA, which already was serving as procurement agent, won that bid as well and new
contract is currently being finalized.

Compendium |page��
may2007
DOTS-PluspilotprojectsarerequiredtosubmitapplicationstotheGLC,whichreviewsthemanddecideswhethertograntaccesstoitsprice-negoti-atedsecond-lineTBdrugs.IftheGLCapprovestheapplication,anapprovalletterisissuedtotheapplicantoutliningthenumberofpatientsforwhomtheprogramhasbeenapproved.OnceGLCapprovalhasbeengranted,pilotprojectsarepermittedtoworkthroughIDA.PilotprojectsthensubmitorderstoIDA,andtheagentworkswithitsnetworkofsupplierstofillorders.Onceasupplierhasfilledanorder,drugsaresenttoanIDAwarehouse.
2.2.6 Quality Control Asnotedearlier,IDAconductsqualitycontrolassessmentstoensureproductsmeetGLCstandards.AfteranorderisplacedandbeforetheproductistransportedtoanIDAwarehouse,IDAevaluatesproductpackagingandlabelingandtestsbatchesofitsproductorders.Theproductisthenreleasedfortransport,andafreightforwardercontractedbyIDAprocessestheshipment.Ordersaresentdirectlytoacountry’sportofentry—mostcommonlyamajorairport.Oncetheorderreachesthatlocation,the
distributionofthedrugsbecomestheresponsibilityoftheprojectcoordinators.
2.3 Convergence of the Global TB Drug Facility and the Green Light Committee
In2006,theStopTBPartnershipmadeadecisiontocombinetheprocurementresponsibilitiesoftheGDFandGLC.27Underthisnewmodel,theGLCwillcontinuetoreviewapplicationsandgrantaccesstoitsnegotiatedratesforsecond-lineTBdrugs,andtheGDFwilltakeresponsibilityfortheselectionofsecond-linedrugprocurementagents.Thesameprocessesandpoliciesusedforfirst-linedrugsundertheGDFwillbefollowedfortheprocurementofsecond-linedrugs.IDAwillcontinueprocurementonbehalfofDOTS-PlusprojectsthathavealreadybeenapprovedbytheGLC,andanewprocurementagentwillpurchasedrugsonbehalfofallotherDOTS-Plusprojects.Movingforward,theGDFwillconductabid-and-tenderprocessforsecond-linedrugsthathavemultiplemanufacturers,andwillnegotiatedirectlywithmanufacturersofdrugsthatareproducedbyonlyonecompany.
Table 1. Prices of Second-Line Drugs Through the GLC26
UNITS PRICE (US$) SUPPLIER
Capreomycin, 1 gram powder for injection 1 vial $ 3.21 Eli Lilly
Cycloserine, 250 mg 100 cap $ 14.12 Eli Lilly
Cycloserine, 250 mg 100 cap bl $ 50.96 Macleods Daman Plant
Ethionamide, 250 mg 100 tab $ 10.21 Macleods Daman Plant
Amikacin 500 mg/2mL injection 100 amp $ 23.15 Gland Pharma Ltd. Pally Factory
Kanamycin, 1 gram powder for injection 50 vls $ 18.58 Panpharma
Ciprofloxacin, 250 mg 100 tab bl $ 2.12 Micro Labs Ltd. (Brown & Burke)
Ciprofloxacin, 500 mg 100 tab $ 3.81 Micro Labs Ltd. (Brown & Burke)
Ciprofloxacin, 500 mg 100 tab bl $ 3.80 Micro Labs Ltd. (Brown & Burke)
Ofloxacin, 200 mg 100 tab $ 3.49 Micro Labs Ltd. (Brown & Burke)
PAS acid sachet eq. to 4 gram aminosalicylic acid 30 sac $ 48.18 Jacobus Pharma Company Inc.
Prothionamide, 250 mg 100 tab $ 13.03 Fatol Arzneimitel
PAS sodium granules 60% (p-aminosalicylate sodium) 100 g $ 9.74 Macleods Daman Plant
Ofloxacin, 200 mg 60 tab $ 2.74 Macleods Daman Plant
26 Data provided by IDA, 2006.27 Discussions with GDF, GLC and procurement agents, 2006.

page��| TBallianCe
paThwayTopaTienTs
2.4 Other Global PSAs
InadditiontotheGDFandGLC,thereareanumberofPSAsthatplayaroleinglobalTBdrugprocurement.Forexample,whileIDAprocuressecond-linedrugsfortheGLConly,italsoprocuressomefirst-line.RoyalCrownAgentsisaPSAthatprocuresTBdrugsonbehalfofthestateofAndhraPradeshinIndiaandplayssomeroleinvariousregionsaroundtheworld.TheUnitedNationsChildren’sFund(UNICEF)hasaPSAdivisionthatprocurespediatricformulationsofTBmedicines.
Additionally,regionalprocurementmechanismsexistthatservetheCaribbeanandPersianGulf.ThismethodofprocurementisdemonstratedbythePanAmericanHealthOrganization(PAHO),whichwasonceresponsibleforthebiddingprocessformanu-facturersinBrazil.Finally,whiletheydonotplayasignificantroleinthecountriesincludedinthisstudy,anumberofNGOssuchasMSFfrequentlyprocureTBdrugsfortheirownprogramsand/ortheregionsinwhichtheyoperate.
3.CountryCaseStudies
Asnotedintheintroduction,atotaloftenstrategically-selectedcountrieswereincludedintheresearchforPathway to Patients.In-depthqualitativeanalysisofnationalandglobalprocurementanddistributionsystemsineightofthesecountrieswasconductedtoprovidethebasisforunderstandingthemarketdynamics.ResearchonIndonesiaandJapanwaslimitedtodeterminingmarketvalue.ThissectionprovidesanoverviewoftheroleofnationalhealthcaresystemsincontrollingTBinthefivehighburdenandthreehighincomecountriesstudiedforin-depthqualitativeanalysis.
Table2providesthepopulation,TBburden,andTBcasenotificationstatisticsforthetencountriesstudied.
3.1 TB Control in the Context of National Healthcare Systems
Allcountriesstudiedhaveanational,publicly-financedhealthcareprogramthroughwhichaportionoforalldrugsandmedicalservicesareprovidedfreeofchargetoatleastasegmentofindividualsandoftentoallcitizens.TBcontrolisoneofseveralcomponentsofthesenationalhealthcaresystems,andpatientsmaychoosetogotoapublicfacilityfortreatment.
28 As noted, Japan and Indonesia were included in the market sizing exercise, only. In depth analysis of procurement and distribution were not performed.
Table 2. Key Statistics for Focus Countries
PROJECTED TB PREVALENCE POPULATION NEW TB CASES (TOTAL) (TOTAL) TB CASE NOTIFICATION (TOTAL)
Brazil 184 million 109,672 141,115 86,881
China 1.3 billion 1,324,633 2,892,422 790,603
France 60 million 7,411 5,901 5,004
India 1.1 billion 1,824,395 3,394,040 1,136,506
Indonesia 220 million 539,189 605,759 210,229
Japan28 128 million 37,814 50,394 29,736
Philippines 82 million 239,459 378,094 130,530
South Africa 47 million 339,078 316,260 264,183
UK 59 million 7,101 5,497 7,039
US 295 million 13,877 14,517 14,517
Note: All data are 2004 numbers, as noted in WHO surveillance report released in 2006.

Compendium |page��
may2007
Theactualstructureofeachcountry’snationalhealthcaresystemdiffersinmanyways,includingwhichpatientshaveaccess,howpatientsenterthepublicsector,wherepatientsaretreatedandbywhom,whatdrugsandproceduresareprovidedinthepublicsector,andwhatcostspatientsincurinthepublicsystem.
Forexample,inBrazilallpatientshaveaccesstofreehealthcareacrossmultiplefacilities.Thismayincludelargepublichospitals,outpatientclinics,orevenprivatehospitalsthathavecontractswiththenationalpublichealthinsuranceprogram.Inthesefacilities,inpatientproceduresandpharmaceuticalsareprovidedforfree.Medicationforsomeoutpa-tienttreatmentiscovered,includingdrugsfortheoutpatienttreatmentofTB,HIVanddiabetes.
InSouthAfrica,clinicvisitsforthetreatmentofTBandsomeotherconditionsarefreeforallpatients,buthospitalstaysarebilledaccordingtoapatient’sincomelevel.Individualswhoareunabletopayforsuchservicesreceivecarefreeofcharge.
IntheUS,thereisnoseparateorcentralizedfundingforthetreatmentofeitherdrugsusceptibleorMDR-TB.Rather,TBtreatmentsarefundedbybothpublicandprivatepayers(e.g.Medicare,Medicaid,privatehealthinsurance.)Fortheuninsured,fundingmaybeprovidedthrougheitherthefederal,stateorlocalhealthsystemsorthroughpatientassistanceprogramssponsoredbypharmaceuticalcompanieswhomanufacturethedrugs.
Inaddition,treatmentandcarefornationalhealthpriorities(includingHIVandTB)areprovidedtopatientsthroughthepublicsectoratfederal-,state-,andcity-runhealthclinics.
3.1.1 High Burden CountriesManysimilaritiesanddifferencesexistacrossTBcontrolprogramsinHBCs,includingfunctionoftheprogram,structureoftheprogramanddivisionofresponsibilities,andsourceoffundingforTBcontrol.
AllHBCsstudiedhavenationalTBcontrolprogramswithintheirbroaderhealthcaresystems.TheseprogramsareresponsiblefordefiningTBcontrolstrategiesandpolicies.
Inhighburdencountries,TBcontrolistypicallyadministeredbyadedicateddepartmentwithintheMinistryofHealth(MOH)orequivalentagency,
althoughthestructureandreportingflowvariessignificantlybycountry.29Insomecountries,thenationalTBcontrolprogrammayreportdirectlytotheMOH,asisthecaseinBrazilandIndia.InothercountriestheTBcontrolprogramreportstoacommunicable-diseasesorinfectious-diseasesbranchofthehealthcareprogram.Forexample,inthePhilippines,TBcontrolispartofthecommunicable-diseasesdepartment,whichreportstothehealthministry.InSouthAfrica,theTBcontrolprogramfallsundertheTB,HIV/AIDSandSexuallyTransmittedInfectionsDepartment,whichisasubgroupoftheStrategicHealthPrograms,undertheMOH.InChina,thenationalTBcontrolprogramfallsdirectlyundertheChineseCenterforDiseaseControlandPreventionandreportstotheOfficeofTBAdministrationundertheMOH’sDepartmentofDiseaseControl.
3.1.2 High Income CountriesInthehighincomecountriesstudied,TBincidenceisrelativelylow.Forexample,in2004therewere6,242newcasesofTBinFrance30and6,837intheUK.31In2005intheUS,14,095casesofTBweredocumentedbytheUSCentersforDiseaseControlandPrevention(CDC).32
Inthesecountries,TBdiseasedisproportion-atelyaffectsspecificpopulations—particularlylowincomeandimmigrantcommunitiesinurbanareas.Forexample,intheUK,accordingtotheHealthProtectionAgency(HPA),in2004almost50percentoftheTBburdenwasconcentratedinLondon,andmostinfectedpatientswereimmigrantsfromSouthAsia.SimilartrendsexistinFrance,whereprevalenceishighestinPariswherethereisaconcentrationofhighriskgroups,includingimmigrantsfromendemiccountriesandpeoplelivinginpoverty.
InbothoftheEuropeancountriesstudied,TBcontrolisanintegratedfunctionofthepublichealth-caresystem.Forexample,intheUKtheNationalHealthService(NHS)providesuniversalcoveragetoallcitizens.Thereisnostand-aloneTBcontrolprogramintheUK.Instead,thecommunicable-diseasesbranchofthehealthministryisresponsibleforoverseeingthesurveillance,prevention,andcontrolofTB,aswellasotherinfectiousdiseases,includingCreutzfield-Jacobsdisease,diphtheria,hepatitis,flu,rubella,andpolio.InFrance,theDirectionsDépartementalesdesAffairesSanitairesetSociales(DDASS)—partoftheDepartmentof
29 Discussions with health ministries and national TB control programs in each country, 2006.30 Superior Council for Public Hygiene Guidelines; Bulletin Epidemiologique Hebdomadaire.31 Health Protection Agency; Office of National Statistics. www.hpa.org.uk/infections/topics_az/tb/menu.htm32 Trends in Tuberculosis – United States, 2005. MMWR. 2006;55(11):305-308. US Centers for Disease Control and Prevention (CDC)

page��| TBallianCe
paThwayTopaTienTs
HealthandSocialAffairs—actsasadefactoTBcontrolprogramandisresponsibleforsurveillanceandmonitoringofTBcases.IntheUS,TBcontrolispartoftheNationalCenterforHIV,STD,andTBPrevention,whichisaunitoftheCoordinatingCentersofInfectiousDiseaseswithintheCDC.
BecauseTBisconsideredapublichealththreat,additionalmeasuresexistinallcountriestoensurethatphysicianordrugcostsarenotabarriertotreatmentandthatallpatientshaveaccesstoTBmedicines.InFranceandtheUK,allpatientsmayreceiveTBtreatmentforfreeregardlessofimmigra-tionstatus.PaymentfordrugsandtreatmentismorecomplicatedintheUS,however.WhileitistheresponsibilityofeachstatetoprovidetreatmenttoeveryTBpatientregardlessofabilitytopay,onlypatientswithoutinsurancecoverageorwhocannotaffordtopayforphysicianofficeordrugco-paymentsareeligibleforassistance.Paymentassistanceisdeterminedusingaslidingscalebasedonapatient’sincome.Hospitalstypicallyreferpatientswhocannotaffordtreatmenttostatehealthdepartmentsorassisttheminapplyingforemer-gencyMedicaidcoverage,ifpotentiallyeligible.
3.2 Overview of Key Trends Impacting TB Funding and Treatment in HBCs
SeveralemergingtrendsmayaffecthowTBtreat-mentisfunded.First,somecountrieshavesignificantprivate-sectoractivityinthetreatmentofTB.Inthesecases,governmentsaremakingaclearefforttoshifttreatmentfromtheprivatetothepublicsectorsothattheycanincreasecontrolandmonitoringofpatientsandensureappropriateandsuccessfuldiag-nosis,tracking,andadherencetoTBtreatment(see Section 3.4.4).Second,asMDR-TBbecomesmoreprevalentanddiagnosismoreaccessible,countriesarebeginningtoincludetreatmentofdrugresistanceintheirnationalTBcontrolprograms.Currently,BrazilandSouthAfricaprovidesecond-linedrugs,andChina,IndiaandthePhilippineshaverecentlypilotedorwillbegintopilotsecond-linetreatmentprogramswithinthenextyear.33
3.3 HBC National TB Control Programs
3.3.1 FunctionInallHBCsstudied,nationalTBcontrolprogramswereestablishedtoprovideacentralorganizationtohelpcontrolTBthroughthepublicsector.Althoughthereareslightdifferencesbetweeneachcountry’s
program,theoverarchinggoalistoeffectivelytreat,monitor,andultimatelyeliminateTB.Fromanorganizationalstandpoint,thesenationalTBcontrolprogramstypicallyinclude:
•National,regional,orlocalbudgetlinesallocatedtoTBcontrol
•Establishedtreatmentguidelines•Mechanismsofmonitoringandevaluation•Drugprocurementanddistributionmechanisms•Treatmentimplementation,training,and
logisticalsupport
3.3.2 Financing InBrazil,China,IndiaandthePhilippines,financingandresource-allocationdecisionsforTBcontrolaresetatthenationallevelbyoneormoreindividualdepartments,includingacentralfinancingdepart-ment,MOH,and/ornationalTBcontrolprogram.
Additionally,inmanycountries(includingChinaandthePhilippines)thenationalTBcontrolprogramissupplementedbyregional(stateorprovincial)andlocalormunicipalresources,thoughthisisgenerallynotamandatedrequirement.Forexample,inthePhilippines,localgovernmentunitsareexpectedtosupplementnationalgovern-mentfundsbyprocuringsomeTBdrugs,providingresourcesforraisingawareness,andtrainingpharmacistsandphysicians.However,aspecificfundingthresholdisnotmandatedbythenationalgovernmentasaprerequisite.Instead,itisuptothelocalgovernmenttodeterminewhatpartofthebudgettoallocatetoTBcontrolversusotherhealthcare,education,orsocialinitiatives.
AsimilarmodelexistsinBrazil.Althoughfundingforthepublicsectorisgenerallydecentralized,BrazilianstatesandmunicipalitiesarenotrequiredtoallocatespecificfundingforTBcontrol.However,theydofrequentlyprovidefundstosupplementprograms.Forexample,officialsmaychoosetoimplementDOTSinmunicipalpublichospitalsorprovidefinancialincentivestopatientswhoadheretotheDOTSprogram.
InChina,localfundingismoreregulated.Theleveloffundingprovidedbythenationalgovern-mentisdeterminedbyaprovince’swealth,andallprovincesareexpectedtocontributeadditionalfunds.Withrespecttodrugprocurementspecifically,wealthierprovincesareexpectedtoprocuredrugsontheirown.
33 Stakeholder discussions with national TB control programs.

Compendium |page��
may2007
InSouthAfrica,thefinancingofTBcontroldiffersfromthatoftheotherHBCsincludedinthisstudy.Thenationalgovernmentallocatesan“equitableshareofresources”forprimaryhealthcaretoeachprovince,andtheprovinceisresponsiblefordetermininghowmuchofthisfundingisallocatedtoTBcontrolandhowthismoneyisused.
3.3.3 Structure IntheHBCsstudied,TBcontrolinthepublicsectoristypicallyadministeredthroughaverticallystructuredprogram,withresponsibilitiesdefinedatnational,stateorprovincial,andlocalormunicipallevels.34Figure4providesanoverviewoftherespon-sibilitiestypicallyassociatedwitheachsuchlevel.
3.4 Treatment of TB Patients
Thissectiondescribestypicalpatienttreatmentregimensinboththehighburdenandhighincomecountries.Amongtheissuesdiscussedaretheuseoffixed-dosecombinations(FDCs);theroleofpublicandprivatesectorsinserviceprovision,includingtypicalreferralpathways;andpublic-privatemix(PPM)programsinTBcontrol.
3.4.1 HBCsIneachoftheHBCsstudied,therearenationaldiagnosisandtreatmentguidelinesinplacetoinformtheclassificationandtreatmentofTBpatientsby
physiciansinthepublicsector.InIndiaandthePhil-ippines,wheremanypatientsreceivetreatmentintheprivatesector,prescribingpracticesvarywidely.35
Ingeneral,activeTBpatientsarecategorizedbasedontheirsputumtestresults,symptoms,andothercriteria,includingwhethertheirinfectionisextra-pulmonaryorpulmonaryandwhethertheyhavebeenpreviouslytreated.Thefirst-linetreatmentregimentypicallylastssixmonths,withanintensi-fiedtwo-monthphaseoftreatmentwithafour-doseregimenofrifampicin(RorRIF),isoniazid(HorINH),pyrazinamide(Z),andethambutol(E),andacontinuationphaseoftreatmentwithrifampicinandisoniazid.Insomecountriesstreptomycin(S)isalsoprescribedforre-treatmentcases.
Forexample,inIndia,first-lineTBpatientsarecategorizedasfollows:
• Category I:Newsmear-positive;seriouslyillsmear-negative;seriouslyillextra-pulmonary
• Category II:Previouslytreatedsmear-positive(relapse,failure,treatmentafterdefault)
• Category III:Newsmear-negative;andextra-pulmonary,notseriouslyill
Therearesomevariationsinnationalguidelinesandprotocolsfortreatment.OnekeyexampleisthedifferenceinregimensusedtotreatCategoryIandIIIpatients.Insomecountries,suchasIndia,
Figure 4. National TB Control Program Responsibilities
LEVEL OF NTP DESCRIPTION OF RESPONSIBILITIES
National • Defining the policy and strategy of the country’s TB control efforts • Allocating funding across TB control activities • Coordinating national level activities such as drug procurement • Overseeing regional TB control programs
Provincial/State • Implementing the TB program within a specific geographic region, which may Cinclude planning, training physicians and healthcare workers, supervising facilities, and monitoring program effectiveness • Prioritizing activities Cwithin a specific geographic region Cand allocating additional funds to carry out many of the implementation activities (e.g., training, public awareness programs, DOTS incentives programs for patients and physicians) • Tracking drug supply needs and reporting to national level • Aggregating TB/ MDR-TB patient case reporting and reporting to national level registry • Monitoring local level implementation activities within specific geographic regions
Local Office • Implementing on a local level, including public awareness, training, delivering e.g., city or drugs and equipment to facilities metropolitan area • Focusing on direct healthcare delivery, including diagnosing and treating patients
34 Stakeholder discussions with national, provincial/state and municipal/county level TB program administrators.35 NTP, pharmacist and physician discussions in India and the Philippines; discussions with PhilTIPS in the Philippines, 2006.

page��| TBallianCe
paThwayTopaTienTs
ethambutolmaynotbeusedforCategoryIIIpatientsasitisforCategoryIpatients,whereasinothercountries,suchasthePhilippinesandSouthAfrica,thesameregimenisusedforCategoryIandIIIpatients.InBrazil,ethambutolisnotapartoftheregimenforanynewTBpatients,whethersmear-positiveorsmear-negative,andisonlyprescribedforpreviouslytreatedsmear-positivepatients.
Variationalsoexistsbycountryindosingandadministration.InBrazil,ChinaandIndia,nationalguidelinesfollowthethree-times-weeklyorevery-other-dayapproach.InthePhilippinesandSouthAfrica,once-dailyregimensareused.
3.4.2 High Income CountriesInhighincomecountries,bothactiveandlatentTBpatientsareroutinelytreated.InFrance,theUKandtheUS,thefour-doseregimenofisoniazid,rifampicin,pyrazinamideandethambutol(HRZE)isusedintheintensivephaseandacombinationofrifampicinandisoniazidisadministeredinthecontinuationphase.Thesedrugsareoftenadminis-teredinfixed-dosecombinations(FDCs),whicharepopularinFranceandtheUKwheretheycompriseapproximately50percentand40percent,respec-tively,ofthevolumeoffirst-linedrugsbyunit.36
InbothEuropeancountriesstudied,patientswithlatentTBaremostcommonlytreatedwitharegimenofrifampicinandisoniazidforthreemonths37orsixmonthswithisoniazidalone.38IntheUS,thesepatientsaretreateddailywithisoniazidforninemonths.39
3.4.3 Use of Fixed-Dose Combinations in Treatment RegimensViewsandpracticesregardingtheuseofFDCsintreatmentdifferwidelybycountry.ThegovernmentsofBrazil,thePhilippines,andSouthAfricaactivelyprocureFDCsandincludethemasakeycomponentoftheirpublic-sectorTBprograms.PerceptionsaroundtheadvantagesofusingFDCsincludeeaseofadministration,easeofstockmanagement,andanincreaseinadherence.40Conversely,neitherChinanorIndiausesFDCsinthepublicsector—althoughtheyareadministeredintheIndianprivatesector.Similarly,FDCsarenotcommonlyusedintheUS,largelybecausephysiciansvaluetheirabilitytotitrateeachseparateagent.
3.4.4 Service Provision Allcountriesstudiedhaveapublicsectorinwhichpatientscanreceivediagnosticandtreatmentservices.InBrazilandSouthAfrica,mostTBtreatmentisprovidedbythegovernment.Insomecountries,TBcarecanbeobtainedthroughtheprivatesectorandPPMfacilities.
InBrazilandSouthAfrica,mostTBtreatmentisprovidedbythegovernment.Incontrast,inIndiaandthePhilippines,despitesignificantpublicsectorprograms,manypatientsprefertoseekdiagnosisandtreatmentintheprivatesectorforreasonsthatincludeperceivedqualityofcareandmaintenanceofanonymity.
PrivatesectorpracticesinTBposeanumberofchallengestothepublicsectorprogram.Forexample,patientsenteringtheprivatesectormaynotbereportedintotheNationalTBprogrammakingitdifficulttoestimatetheTBburdenandtracksuccessindiagnosingandtreatingpatients.Also,physicianregimensdifferfromnationalguidelinesandinmanyinstanceslesseffortisplacedontreatmentadherence.Toaddressqualityofcareintheprivatesector,IndiaandthePhilippineshavepilotedPPMprogramsinanefforttoreachmorepeoplewithappropriatetreatmentandhelpprovideanincentivetotheprivatesectortoadheretothenationallyapprovedregimen.Underthismodel,physicianswhosuspectapatientofhavingTBorinitiallydiagnoseapatientwithTBcanreferthepatienttothepublicsectorforfurtherdiagnosisandfreetreatment,ormaycontinuetotreatthepatienthimorherself,withdrugsprovidedatnocostorsubsidizedbythegovernment.(The PPM model is described in greater detail in Section3.6.1).
3.5 Public Sector: Referral Pathway and Settings of Care
Thissectiondetailsthegeneralreferralpathwayofapatientinthepublicsectoranddescribesspecificsettingsofcareforthehighburdenandhighincomecountriesstudied.Overall,therearethreemajorsectorsinwhichTBcareisadministered:thepublicsector,theprivate(forprofit)sector,andthroughNGOs.Inthecountriesstudied,NGOswerenotasignificantserviceproviderandthereforearenotcoveredindepthinthisreport.
36 IMS MIDAS data for 2005.37 France guidelines from Superior Council for Public Hygiene Guidelines; U.K. guidelines from National Institute for Health and Clinical
Excellence, British Thoracic Society.38 U.K. only guidelines from National Institute for Health and Clinical Excellence, British Thoracic Society.39 CDC Targeted TB Testing and Treatment of Latent TB Infection. Available online in PDF format at www.cdc.gov/mmwr/PDF/rr/rr4906.pdf40 Discussions with NTP and physicians in Brazil, the Philippines and South Africa, 2006.

Compendium |page��
may2007
3.5.1 HBCsGenerally,patientsenterthepublicsysteminoneoftwoways:ByvisitingapublichealthcareworkerandbeingreferredtoaTBspecialistorfacility,orbyvisitingaprivatephysicianandbeingreferredtothepublichealthcaresystem.
InmanyHBCs,patientssuspectedofhavingTBarereferredtoapublicoutpatientsettingfordiagnosisandtreatment.PatientswithTBaresubsequentlymanagedintheoutpatientsettingforthedurationoftreatment.IntherarecasethatapatienthasMDR-TB,HIVoranotherseriousconcomitantdisease,theymaybereferredtoaspecialcenteroradmittedtoahospital.FollowingaredescriptionsofpublicsectorreferralpathwaysandcaresettingsineachofthefiveHBCsstudied,followedbythethreehighincomecountriesstudied:
Brazil
InBrazil,patientswilltypicallypresentinapublichospitalambulatorysettingintheircommunity,andwillbereferredtothepulmonologydepartmentatthathospitalforsputumtesting.Oncediagnosed,patientswillbemanagedinthehospitaloutpatientdepartment.IfthefacilityhasbeendesignatedasaDOTShospitalbythemunicipal-orstate-levelauthorities,thepatientwillbeaskedtoreturndailyfortreatment.IfthefacilityisnotDOTS-designated,thepatienttypicallycomesinonaregularbasiseitheronceaweekoronceamonthforthenextsup-plyofpills.Patientswhoprefertoreceivetreatmentatafamilyhealthprogramintheircommunityorbyavisitinghealthcareworkermaychoosetodosoifsuchservicesareavailableintheirmunicipality.
China
InChina,patientstypicallypresentatacountyortownshiphospitalortoavillagehealthcareworker.PatientssuspectedofhavingTBarereferredtoaTBtreatmentdispensary—alocalChineseCDCunitorTBpreventioninstitute,forfreediagnosis,treatmentandmonitoring.Atthecountyortownshiphospitallevel,healthcareworkersmayconductX-raysandCTscans.Somefacilitiesmayhavecapabilitiestoconductsputummicroscopytestingaswell.Insuchcases,patientsarerequiredtopayaconsultationfeeinadditiontofeesforconductingX-rayandsputumtesting.OnceapatienthasbeendiagnosedwithTB,thefacilitywillrecordthepatientintoanInternet-basedreportingsystemandreferthepatienttothedispensary,wherethepatientisreportedagain.This
mayresultinduplicativecounting.Patientstypi-callyreturntotheCDCunitonceaweekoreverytwoweeksfortreatmentandmonitoring.InsomeruralareaspatientslivefarfromtheTBdispensary,avillageclinicphysicianwillreceivethemedicinesfromtheTBdispensaryandadministerdirectlytothepatientonceeveryonetotwoweeks.Theyareusuallypaidamonitoringfeetoperformthisservice.
india
InIndia,patientscanpresenttoanypublichealthfacility.IfapatientissuspectedofhavingTB,heorsheisreferredtooneofthemanydesignatedmicroscopycenterslocatedthroughoutthecountry.Oncediagnosed,anIDcardisfilledoutforthepatient,aTBhealthcareworkerconductsaninitialvisitwiththepatienttoinformhimorherofthetreatmentregimen,andthepatientisreferredbacktohisorheroriginalsiteofpresentationtobegintreatment.Ifthepatientlivesfarfromthistreatmentsite,theTBhealthcareworkerattemptstolocateaDOTSsitethatisclosertothepatient’sresidence.AvariationinthisreferralpathwayisthroughthePPMmodel,whichisviewedbygovernmentofficialsasanimportantwaytoleverageprivate-sectorcapacity.Throughthismodel,patientspresenttoprivateclinicsand/orhospitalsand,ifsuspectedofhavingTB,arereferredtopublic-sectormicroscopycenters.Afterdiagnosis,patientsmayopteithertoreceiveprivatelyfundedtreatment,astheywouldfromanyotherprivate-sectorphysician,orreceivefreedrugtreatmentthroughtheRevisedNationalTBControlProgram(RNTCP)underthesupervisionoftheirprivate-sectorphysician.Thisprogramhasbeenincreasingrapidlyinscope,althoughitstillinvolvesasmallfractionofprivate-sectorpractitioners.
PhiliPPines
InthePhilippines,patientsmayinitiallypresentatapublicorprivatehospitalorclinic.PatientsareusuallydiagnosedfirstbyX-rayandthenfollowingasputumtest,dependingonthefacility’scapabilitiesandresources.Inthepublicsetting,patientswhoarediagnosedsmear-positivearemanagedataDOTSclinicthatmaybelocatedatalargepublichospital,abarangay(ruralhealthunit),orevenaPPMclinicataprivatehospital.Thosepatientspreferringtobetreatedintheprivatesectoratnon-PPMsitesmaydoso,thoughtheyincurthecostofdrugsaswellasphysicianvisits.

page��| TBallianCe
paThwayTopaTienTs
south afriCa
AlthoughsomevariationexistswithinSouthAfrica,generalTBcontrolisamandateofthepublicsector,andprivate-sectorphysiciansarerequiredtoinformpatientsthattheycanreceivefreecareinpublicfacilities.Patientsmaythenchoosetoreceivecareintheprivatesectorattheirowncostorpresenttothepublicsector.Patientsinthepublicsectormostfrequentlypresenttoprimaryhealthcareclinics.IfsuspectedofhavingTB,patientsaregivenasputumsmeartestandtheresultsaresenttoamicroscopylabforconfirmation.IfdrugresistantTBisnotsuspectedandsymptomsarenottoosevere,thepatientbeginsDOTStreatmentattheclinic,inthecommunityunderthesupervisionofavolunteerDOTSsupporter,orinsomecases,athisorherworkplace.Inexceptionalcircumstances,suchasifthepatientismigrantormusttravelextremelylongdistancestohealthcarefacilities,heorshemaybeallowedtoself-administertreatment.
PatientswithseveresymptomsorthosewhoaresuspectedofhavingMDR-TBarereferredtospecialistcentersormajorhospitals,wheretheyundergoadrugsusceptibilitytest(DST)andaretreatedasaninpatientuntiltheyarenolongercontagious.Whereservicesareavailable,patientswhoareco-infectedwithHIVandTBarereferredtoaspecialHIVtreatmentsite,wheretheyreceivecarefromaspeciallytrainedhealthcareworker.
3.5.2 High Income Countries
franCe
InFrance,patientspresentmostcommonlyintheemergencyroomandalsotoageneralpractitioner.Inbothcases,theyarereferredtoahospitalforachestX-ray.IfapatientissuspectedofhavingTBaftertheX-ray,heorsheisreferredtoaspecialistforsputumtestingandsubsequenttreatment.
uK
PatientsintheUKpresenttoageneralpractitionerortheemergencyroomandarereferredtothehospitaloutpatientsettingfordiagnosisbyachestX-ray.PatientswhoaresuspectedofhavingTBaftertheinitialX-rayarereferredtoahospitalspecialistineitherthepublicorprivatesetting,dependingontheirpreference.Thatspecialistconfirmsdiagnosisthroughtheresultofasputumtestandsubsequentlymanagestreatment.ThegovernmentalsohasamandatoryscreeningpolicyforimmigrantsfromcountriesinwhichTBisendemicandwhoplanto
stayinthecountryformorethansixmonths.TheseindividualsmusthaveachestX-raywhentheyenterthecountry.
us
Similarly,patientsintheUStypicallypresentintheemergencyroomortotheirgeneralpractitionerandarereferredtoaspecialistforsputumanddrug-sensitivitytesting.ImmigrantsenteringthecountryarerequiredtoreceiveTBtestingpriortoobtainingavisaandanysuspectedcasesareimmediatelyreferredtothelocalhealthdepartmentuponentry.ThosewithlatentTBarerequiredtoundergoninemonthsofprophylactictherapywithisoniazid.
3.5.3 Payment for Drugs and Services InallHBCsstudied,TBdrugtreatmentinthepublicsectorisfreeofcharge.However,asprevi-ouslynoted,somepatientsmayincurfeesbeforebeingreferredtospecificfacilitiesfordiagnosisandtreatment.Forexample,inChina,patientsseekingdiagnosisinacountyhospitalorspecializedhospitalmaypayconsultationanddiagnosticfeesfortheadministrationofX-raysandsputumtests.OncetheyarereferredtoaTBdispensarydesignatedbytheChineseCDC,diagnosticproceduresandtreatmentarefree.InSouthAfrica,patientsreceiv-inginpatienttreatmentforTBwiththefinancialresourcestopayfortreatmentareaskedtopayaportionofthecosts,basedontheirincomelevel.
IntheUK,patientsinapublichospitalwillnotpayanythingiftreatmentisadministeredinaninpatientsetting.Inthehospitaloutpatientsettingorinaretailpharmacy,patientspaythestandardprescriptioncharge—£6.65(US$13)atthewritingofthisreport.InFrance,TBisclassifiedasanaffection de longue durée (ALD)andisthereforeexemptfromallconsultationfees,hospitalchargesanddrugco-payments,irrespectiveofsector.Alltreatmentanddrugsarealways100percentcoveredbysocialsecurityandarefreeofcharge.IntheUS,patientswhodonothaveinsuranceorcannotaffordco-paymentsarereferredtoapublicclinicandreceivetreatmentfreeofcharge.
3.6 Private Sector: Referral Pathway and Settings of Care
Basedonsalesfiguresandinformationfromprimaryandsecondarysources,asignificantportionofthepopulationinIndiaandthePhilippinesusesprivatehealthcarefacilitiesandsystemsforTBtreatment.

Compendium |page��
may2007
Inothercountries,private-sectorhealthcaremaybesignificant,butnotforthetreatmentofTB.41InthecaseofTB,patientsmaypresenttoanynumberoffacilitiesandmostlikelywillbediagnosedandtreatedonanoutpatientbasis.Asoutpatients,theywillreceiveprescriptionsfordrugtreatmentwhichtheymustself-administer.RegulationinHBCpri-vatesectorsislimited,andtreatmentpracticesvaryconsiderablyfromphysiciantophysician.Itisnotuncommonforpatientstoself-medicate,especiallyinareaswhereTBinfectioncarriesasocialstigma.
Thereasonsthatpatientsmaychoosetopayfortreatmentwhenfreetreatmentisavailablevarycon-siderably.Twoofthemostcommonlycitedreasonsarethatsomepatientsperceiveprivatetreatmentasbeingfasterandbetterandthatprivatetreatmentismorediscrete.
3.6.1 Role of Public-Private Mix Programs in TB TreatmentInIndiaandthePhilippinessignificantprivatemarketsforTBtreatmentexist.TheWHOpilotedthePPMmodelto:
• Increaseadherencebyensuringthatcostisnotanissueandbyrequiringthattreatmentisobserved
• Facilitatetheflowofpatientsbetweenthetwosectorsinorderto1)ensurethatpatientsdiagnosedwithTBarereportedintothenationalregistriesfortrackingandmonitoringpurposes;and2)facilitateproperdiagnosisandtreatmentbasedonthetreatmentguidelinesetinthatcountry,includingimplementationofdirectlyobservationaltherapy
APPMprogramwaslaunchedinIndiain1995inanefforttoextendthecapacityoftheRevisedNationalTBControlProgram(RNTCP)aswellasitsscopeofinfluenceintheprivatesector.Itwasinitiallypilotedin14citiesandwillsoonberolledoutnationwide.Throughtheprogram,patientsmayinitiallyconsultwithaprivateproviderandstillbeeligibleforfree,directly-observedtreatment.PatientswhoinitiallyvisitaprivatepractitionerhavetheoptionofbeingdiagnosedbytheirprivatephysicianorimmediatelybeingreferredtotheRNTCPfordiagnosis.Ifdiagnosedintheprivatesector,patientsmayremaininprivatecareormovetothepublicsector.ThoseunabletoaffordprivatetreatmentaregivenareferralformandsenttotheRNTCPfortreatment.Thosewhoprefertobetreatedintheprivatesectormaydo
so,howeverphysicianscanchoosewhetherornottowaivetheconsultationfee.
APPMprogramwaslaunchedinthePhilippinesin1993toaddressavarietyofchallengesthatexistedintheprivatesector.Private-sectorphysicianshadalackofknowledgeregardingTBcontrolchallengesanddevelopmentofdrug-resistance.Physiciansfrequentlyusedmanydifferenttreatments,oftennotfollowingtheregimensrecommendedbythenationalTBcontrolprogram.Furthermore,physiciansdidnotfollowupwithpatientsonaregularbasistoensureadherence.UnderthecurrentPPMmodel,aPPMfacilitycontractswithprivatephysiciansinthearea.PrivatephysiciansaffiliatedwiththePPMareaskedtoreferTBpatientstoapublichealthcenterunitwhentheyaresuspectedofhaving—orarediagnosedwith—TB.IfthediagnosisforTBisconfirmed,thepatientremainsinthepublicsectorfortreatmentbutmaychoosetoalsoreturntotheprivatesectorforperiodicfollow-upvisitsduringtreatment.
3.6.2 Payment for Drugs and Services in the Private SectorAsnotedpreviously,asizeableprivatemarketforfirst-lineTBmedicinesexistsinIndia,thePhilip-pinesandtheUS.Intheprivatesector,patientsareresponsibleforpayingforconsultationanddiagnos-ticfeesatthephysician’sofficeorhospitalandareresponsibleforthecostofdrugsatthepharmacy.Asanexceptiontothis,patientswhoarecoveredbyprivateorpublichealthinsurancemaynotincurallfeesassociatedwithTBtreatment.ForexampleintheUS,manypatientshaveprivateinsuranceandthuspayanofficeco-paymentandadrugco-pay-mentratherthanthefullcostofservicesanddrugs.However,thecostvariesbecausethereisamixofpublicandprivateinsurancecoverage.
3.7 MDR-TB Control
BrazilandSouthAfricacurrentlyhavenationalpublic-sectorprogramsfortreatmentofMDR-TBandutilizedomesticfundingandin-countryprocurementmechanisms.ChinaandIndiaplantoimplementand/orexpandDOTS-Pluspilotprojectsasearlyas2007.Meanwhile,patientswhoneedtoreceivetreatmentforMDR-TBmustdosointheprivatesectorattheirownexpense.ThePhilippinesreceivesfundingfortreatmentofMDR-TBthroughGFATMgrantsanddrugsthroughtheGLC.In
41 In China, village doctors may provide TB care but they receive a payment from the government to do so and drugs are free to patients.

page�0| TBallianCe
paThwayTopaTienTs
2005,treatmentwasprovidedfor250patientsandthecountryisnowintheprocessofexpandingtreatmentforupto2,500MDR-TBpatients(seesection4.1.1).42
MDR-TBpatientstypicallystarttoflowintonationalTBcontrolprogramsmuchastheywouldforregularTB.However,oncetheyarediagnosedwithMDR-TB,theyarereferredtoaspecializedsitethatmayormaynotfunctionexclusivelyforthetreatmentofTB.InSouthAfrica,patientsareusuallysenttoaspecialistatadistrictorregionalfacility,andinthePhilippines,patientsaresenttoeitherMakatiMedicalCenterinManilaoranothertertiarycarecenterfortreatment.Brazil’sMDR-TBpatientsaresenttospecializedTBreferencecenters.
ThetreatmentofMDR-TBisaregularfeatureofTBcontrolinhighincomecountries,and—likethe
treatmentofdrug-susceptibleTB—isfullyinte-gratedintothegeneralhealthcaresystem.InFranceandtheUK,thetreatmentofsuchpatientsisprimar-ily,ifnotexclusively,publicallyfunded.IntheUSthefundingofMDR-TBtreatmentdependsonthepatient’sinsurancecoverageandwhetherheorsheiseligibletoreceiveassistancefromthegovernment.Inthethreehighincomecountriesstudied,theprimarydifferencebetweenthetreatmentofdrug-susceptibleandMDR-TBpatientsisinthesettingofcare.InFranceandtheUK,patientsgenerallyreceivetreat-mentonaninpatientbasisatahospitaluntiltheyarenolongerconsideredcontagiousandarehealthyenoughtofinishtreatmentontheirown.IntheUS,patientsmayalsobetreatedonaninpatientbasisatanyhospital,ortheymayalsobereferredtooneoftheTB“CentersofExcellence”fundedbytheCDC.
4.ProcurementandDistributionofTBDrugsinHighBurdenCountries
Thissectionfocusesonthefinancingoffirst-andsecond-linedrugsaswellasthepublictenderingprocess,akeyprocurementmechanismintheHBCsstudied.DiscussionofthepublicsectorincludesthedemandforecastingprocessanddistributionpathwaysofTBdrugs.Finally,thissectionprovidesanoverviewofprocurementintheprivatesectorsofIndiaandthePhilappines,thetwoHBCsevaluatedinPathway to PatientsinwhichtheprivatesectorplaysalargeroleinTBcontrol.
4.1 Financing for First-line TB Drugs
InallHBCsstudied,thepurchaseofTBdrugsisatleastpartiallyfundedbythenationalgovern-ment(seeFigure5).InBrazil,allfundingfordrugpurchasescomesfromthenationaltreasury.InIndia,
donorfundsfromGFATM,theUKDepartmentforInternationalDevelopment(DFID),theUSAgencyforInternationalDevelopment(USAID),andotheragenciesarepaidtothecentralTBdivisionandcombinedwithdomesticfunding,aswellasWorldBankloans,topayforTBdrugs.
InChina,themajorityoffundingcomesfromthenationalgovernment.However,thegovernmentsofwealthierprovinces—mostlylocatedonthecoast—arealsoresponsibleforprovidingfundingfordrugssuppliedintheirlocalities.
InthePhilippines,nationalandregionallevelsofgovernmentsharethecostofdrugpurchases.ThenationalgovernmenthascommittedtopurchasingCategoryIandIIpatientkitsfortheentireTB
Figure 5. Level of Centralization of Drug Funding in the Public Sector, HBCs
Centralized
42 Discussions with national TB control officials in each country.
DecentralizedMix of Centralized and
Decentralizaed
India, Brazil China Philippines South Africa

Compendium |page��
may2007
controlprogramandlocalgovernmentsgenerallyfunddrugpurchasesforCategoryIIIpatients.
InSouthAfrica,provincialgovernmentsholdprimaryhealthcarebudgets,aportionofwhichareallocatedtodrugpurchasesforthepublicsector.Althoughdrugsaretenderedatthenationallevel,theactualamountthatissetasideforTBdrugpurchaseisdeterminedattheprovinciallevel.
4.1.1 Financing for Second-line TB DrugsSystemsthatsupportsecond-lineTBdrugfinancingareintheirinfancyinmanycountries.However,astheincidenceofMDR-andXDR-TBbecomesagrowingconcern,anefforthasemergedtoincludesecond-linecoverageaspartofnationalTBcontrolprograms.Atthewritingofthisreport,onlyBrazilandSouthAfricahadestablishedfundingforsecond-linemedicinesundertheirnationalTBcontrolprograms.Theremainingcountriesstudiedhaveonlyrecentlybegunpilotprogramsorhaveplanstoinitiatethemoverthenextyear.
InIndia,theRNTCPhasbegunapilotprogramtoincludesecond-linedrugs.Theprogram,whichfundedtreatmentfor100patientsfor2006,43isexpectedtogrowrapidly—althoughfundingsourcesareintheprocessofbeingconfirmed.
ThePhilippineshasreceivedGFATMfundingforitspilotMDR-TBprogram.In2005,theGFATMRound2grantprovidedfundstotreat250patientsthroughtheGLC.Another2,500patientsareexpectedtobetreatedbetween2007and2011withfundsprovidedintheGFATMRound5grant.
FundsfromaGFATMRound5grantwillallowChinatolaunchtwopilotprogramstotreatap-proximately4,000patients,withplanstoexpandthenumberofprojectstoinclude115countiesinsixprovincesby2011.
4.2 Public Drug Procurement
4.2.1 Public Tender ProcessTable3illustratesthemodesofprocurementinthepublicsectorforeachHBCincludedinthestudy.
MostofthepublicmarketsintheHBCsstudiedprocuredrugsthroughabidandtenderprocess.Forsecond-lineproducts,theremayalsobeadirectnegotiationbetweenthegovernmentsandsuppliers.ThenationalTBcontrolprogram(orarelatedagencywithinthegovernment)determinestheapproximatevolumeofdrugsthatareneededbythepublicsectorfortheperiodofthetendercontract,requestsbidsfromdrugmanufacturersandselectssupplierswhoagreetoprovidedrugsforapresetperiodoftime,atapricedeterminedinthebiddingprocess.WiththeexceptionofSouthAfrica,44allten-dercontractsintheHBCsstudiedarebidannually.
Althoughtendersareopentobothnationalandinternationalsuppliers,nearlyallofthecountriesincludedinthestudyprefertosourcetheirdrugsfromlocally-basedcompanieswhenpossible.Onlytwoofthecountriesstudied,IndiaandthePhilip-pines,usetheGDF.InIndia,theGDFsuppliesapproximatelyhalfofthedrugsusedbythepublicsectorandinthePhilippines,theGDFsuppliesalltreatmentsforsmearpositiveandre-treatmentcases.
Moreover,withtheexceptionofChina,tendersinthefiveHBCsstudiedareadministeredatanationallevel,evenifthefinancingfordrugscomesfromprovincialbudgets.InChinathetenderingsystemissplitbetweenthenationalandtheprovinciallevels,dependingontheoriginoffunds.IftheChinesegovernmentorexternalfundersareprovidingtheresources,thetenderisadministeredbythenationalgovernment.Whenprovincesareprovidingthefunding,tendersareissuedbytheprovincialhealthministry.
Inmostcases,beforeadrugmanufacturercanparticipateinabidandtenderprocess,itmustbepre-qualifiedormeetanumberofcriteriasetbythetenderadministrator.Onecommonlyusedcriterioniswhetheramanufacturerislocaltothecountryissuingthetender.Mostofthecountriesstudiedpreferredtosourcetheirdrugsfromlocalcompanieswhenpossible.ProcuringdrugsdirectlyfromlocalsuppliersoftenoffersnationalTBcontrolprogramsandgovernmentsthebenefitoflowerprices,asisthecaseinChinaandIndia.
Table 3. Procurement Mechanisms in HBCs
PUBLIC COUNTRy TENDER45 GDF GLC
Brazil46 l
China l
India l l
Philippines l l l
South Africa l
43 The program is administered in the states of Gujarat and Maharashtra with the first cohort scheduled to begin in early 2007. The LRS Institute in Delhi also has had a small self-funded program with approximately 150 patients.
44 South Africa bids on a bi-annual basis. 45 For some second-line drugs, procurement is done through direct negotiation with suppliers rather than through a tender process.46 In 2005 due to internal manufacturing problems, Brazilian national suppliers were unable to meet the total demand for first-line TB drugs,
and were assisted by PAHO. Generally, Brazil produces 100 percent of its national drug supply.

page��| TBallianCe
paThwayTopaTienTs
However,procuringdrugslocallydoesnotalwaysresultincost-savings.ThepubliclysanctionedTBtreatmentregimensinothercountriesstudied,notablyBrazil,thePhilippinesandSouthAfrica,actuallycostmorethansimilarregimensofferedontheglobalmarketorthroughtheGDF.Thecitedrationaleforprocuringdrugsatthesehigherpriceswasadesiretosupportlocalindustryaswellasensurethequalityandsafetyofproducts.SomeoftheHBCsstudiedhaveturnedtointernationalcompetitivebidsortheGDFfortheirdrugprocurementneedswhenqualityorsufficientvolumescouldnotbeassuredbylocalsuppliers,orbecauseofdonorpreference.
Whilesomeelementsofthepre-qualificationofsuppliersweresimilaramongtheHBCsstudied,othercriteriausedinmanufacturerpre-qualificationvariedwidely.Forexample,inIndia,potentialsuppliersmusthaveWHO-GMPcertification,meetaminimumthresholdofannualrevenues,anddemonstratepriorexperienceinmanufacturinglargequantitiesofTBdrugs.47InChina,manufactur-ersmustbecertifiedbytheStateFoodandDrugAdministrationbeforetheycansubmitbidsinthepublictender.InBrazil,theinvitationforbidsinthepublictenderisissuedonlytostateandmilitarylaboratories.
4.2.2 Demand ForecastingEnsuringacontinuoussupplyofdrugsforpatientsisanimportantaspectofTBcontrol.EachoftheHBCsstudiedhasdevelopeddifferentstrategiestoensurethatsufficientsupplieswillbeonhandforpatientsevenintheeventofmanufacturingdelaysoremergencies.ThesestrategiestypicallyrequireanassessmentoftherateofTBdrugutilization,antici-pationofneedsfortheupcomingtenderperiod,andthemaintenanceofa“bufferstock”ateachlevelofthesupplychain.Thisdemandforecastingisusuallyconductedatthelevelatwhichthetenderisbeingadministered.
DemandforecastingisusuallyperformedbyapersonordivisionwithinthenationalTBcontrolprogram,asisthecaseinBrazil.48Everyyear,theBrazilianMinistryofHealthforecaststheneedsoftheprogramforthefollowingyearusingfiguresfromstatereportsthatarebasedonprojectionsbyeachmunicipality.Theministrythenaugmentsthesefigureswithabufferstockof25percent.Similarly,inChina,forecastingisconductedbytheStatistics
andSurveillanceOfficewithintheNationalCenterforTBControlandPrevention.TheTBpreventioninstitutesatthecounty,prefectureandprovinciallev-elsreportthesupplyanddistributionofdrugs—aswellasthenumberofnewpatientsdetected—tothenationalgovernment,whichusesthosefigurestoforecastthedemandfortheentireprogramandallocationsofdrugsforeachprovince.InIndia,forecastingisconductedbytheCentralTBDivisionandtheMinistryofHealthandFamilyWelfarewiththeassistanceofaprivateagencycalledStrategicAlliance.AlllevelsoftheTBcontrolprogramarerequiredtosubmitstandardizedreportsthatindicatepatientnumbers,inventorylevels,anddrug-utiliza-tionrates.Thesereportsfeedintotheforecastingprocess,whichdeterminesthedrugsupplyneedsoftheprogramatnational,regional,andlocallevels.
InSouthAfrica,bycontrast,forecastingisnotperformedbyapersonoragencydedicatedsolelytoTBcontrol.49BecauseTBcontrolinSouthAfricaisintegratedintothegeneralprimarycaresystem,adivisionwithintheMinistryofHealthcalledPhar-maceuticalPlanningandPolicyforecastsdemandfornearlyalldrugsusedinthepublichealthcaresystem.Thisdivisionalsonegotiatessuppliesofcertainsecond-lineTBdrugswhosevolumesdonotwarrantapublictender.Usinghistoricalutilizationreportsfromprovincialgovernmentdepots,thisagencydeterminestheannualneedfortheentirehealthcaresystemandinsertsthesefiguresintothepublictender.However,theactualorderingofthedrugsduringthetendercontractperiodisperformedbytheprovincialdepotsthatserveasthefirstpointofdelivery.Oncethepriceissetbythenationaltender,theresponsibilityforprocurementfallsattheprovincialdepotlevel,whichisresponsibleforcontactingmanufacturerstoplaceordersandprovidingpayment.
InthePhilippines,trackingpatientsandforecastingsupplyaredonethroughabottom-upapproach.Localhealthsitesreporttoruralhealthunits,whichreporttotheprovincialandregionallevels.Dataarecollectedatthenationallevel,analyzedattheDOH,andusedforfundingallocation,futureplanningandpolicydevelopment.
4.2.3 Distribution PathwaysPublicdistributionsystemsfordrugswithinthecountriesstudiedarequitediverse.However,qualityassurancewasidentifiedasachallengefacedbyall
47 As noted in Section 2.1.3 GMP refers to Good Manufacturing Practices. Additional information available on the WHO website at www.who.int/medi-cines/areas/quality_safety/quality_assurance/gmp/en/index.html.
48 Stakeholder discussions with Brazil MOH and NTP, 2006.49 Stakeholder discussions with South Africa MOH and NTP, 2006.

Compendium |page��
may2007
programs.Accordingly,eachcountryhasaseriesofcheckpointstotestthequalityofdrugordersbeforetheyarereleasedtootherpartsofthesupplychain.
Inthecountriesstudied,qualitytestingisusuallyfirstconductedattheproductionsite.Onceanorderhasbeenmanufacturedandisreadyfordeliv-ery,theagencythathasplacedtheorderisnotified.Asampleofthebatchissenttoalaboratory—eitheragovernmentlaboratoryoraprivatelaboratorythathasbeencontractedbythegovernment—andistestedbeforetheorderisshipped.Iftheresultsofthebatchtestindicatethattheorderisnotofsufficientquality,follow-uptestsareconductedtoconfirmtheresultsoftheinitialtest.Duringthistime,theorderisheldatthemanufacturingsite.Ifnegativeresultsareconfirmed,anorderisfrozenandmanufacturersarerequiredtoreplacetheproduct.Iftheresultsofasecondarybatchtestaresatisfactory,theorderisreleasedfordistributionanddeliveredtoaninitialpointofdelivery—usuallyagovernmentdepot—wherethefinalpackagingofdrugsisconductedifnecessary.Anadditionalbatchtestmaybeconductedatthislevelbeforetheorderisshipped,eithertootherdepotsorthevarioushealthcarefacilitieswhereproductsaredistributed.
TBdrugspurchasedbythepublicsectortendtoflowthroughaseriesofpublicdepotsorwarehousesbeforereachingthefacilitiesthatadministerthemtopatients.Thefrequencywithwhichdrugordersaresubmittedandshippedvariesbycountry.Thecountriesstudiedfollowoneoftwomodelsofdistri-bution:thepushsystemorthepullsystem.Figure6representshowdrugsareorderedanddistributedinthepublicsectorthoughthepushandpullsystems.
Underthepushsystem,drugsareorderedbyonecentralagencyordivisionandthen“pushed”ordeliveredatregularintervalstootherpartsofthesupplychain.ThispushsystemisfoundinmostprovincesinChina.TBmedicinesflowtofacilitiesatpre-specifiedsupplylevelsandarriveatfacilitiesatregularintervals,typicallyfourtimesayear.
InthePhilippines,drugstotreatCategoryIandIIpatientsflowthroughapushsystemandaredeliveredtwiceayeartoaportofentry,withsuppliessenttoregionalwarehousesoneitheramonthlyorquarterlybasis.Second-linedrugsarealsoorderedonanintermittentbasisbytheTropicalDiseaseFoundationfordistributioninitsfacility.
Underthepullsystem,theflowofdrugsisdrivenprimarilybyordersfromdepotsand/orfacilitiesfurtheralongthesupplychain.CountriesoperatingonsuchamodelincludeBrazil,thePhilippines(forCategoryIIIdrugs)andSouthAfrica.Throughthissystem,bulksuppliesofdrugsareorderedbyandheldinregionaldepotsuntiltheyarerequestedbyfacilities.Ordersmayvarywidelyinsizeandfrequency,dependingontheneedsofthefacilityordepot.
Indiahasahybridsystemthroughwhichthecentralunitprocuresdrugsanddeterminesannualrequire-mentsforthecountryasawhole.Theamountsuppliedtostatesanddistrictsisdeterminedbasedonmonitoringofdrugstocks.
4.3 Private Drug Procurement: First- and Second-line Drugs
InBrazil,ChinaandSouthAfrica,thedistributionofTBdrugsinprivatefacilitiesorpharmaciesiseitherdiscouragedorprohibitedforqualitycontrolreasons.
InIndiaandthePhilippinestreatmentintheprivatesectorisutilizedbyabroadersegmentofthepopulation.Inthesecountries,theprivatesectorplaysasignificantroleintheprocurementanddistributionofTBdrugs.
Figure 6. Flow of Drugs Through the Public Pull vs. Push Systems in High Burden Countries
Push-Through Public Sector Channels
SuPPLIERS
HEALTHCARE FACILITIES
PATIENT
GOVERNMENT DEPOTS
Pull-Through Public Sector Channels
SuPPLIERS
HEALTHCARE FACILITIES
PATIENT
GOVERNMENT DEPOTS
Flow of Drugs:
Flow of ordering Flow of drugs

page��| TBallianCe
paThwayTopaTienTs
Theflowofdrugsintheprivatesectorisquitedifferentfromthatofthepublicsector.InIndia,forexample,treatmentintheprivatesectorisnotfreeofcharge,thoughpricesarerelativelylowandoftencontrolled.Patientsintheprivatesectoraremorelikelytoreceiveaprescriptionsorareadvisedtopur-chasecertainTBdrugsratherthanbeadministeredmedicationinafacility.Ifthisisthecase,apatientmustobtaindrugsfromaretailpharmacy,wheretheyarepaidforeitherout-of-pocketorthroughfundsfromaninsuranceplan,ifthepatienthasone.AsinIndia,inthePhilippines,patientsmayapproachapharmacydirectlyandpurchaseTBmedicineswithoutaprescription.Patientsmayalsovisitadoctorwhoprovidesaninitialsupplyofmedica-tionandaprescriptiontoobtaindrugsfromaretailpharmacy,wheretheyarepaidforout-of-pocket.
Anotherdifferencebetweentheprivateandpublicsectorsisinthedecentralizationofdistribution.Forexample,intheprivatesectorsinIndiaandthePhilippines,manufacturersoftenselltheirproductstoseveralwholesalerswhoresellthosedrugstothemanyretailersthroughoutthecountry.Mostprocurementanddistributionisperformedeitherbylargeandcomplexnetworksofmassivepharmacychainsorby“mom-and-pop”pharmaciesthatservespecificregions.
AnothersignificantdifferencebetweentheprivateandpublicsectorsinIndiaandthePhilippinesisthemannerinwhichdrugsarepricedandprocured.Ratherthanusingabidandtenderprocessforpricesetting,manufacturerssetapriceatthelaunchandnegotiatevolumediscountsorrebatesonanindivid-ualclientbasis.Wholesalersordistributorspurchasedrugsfrommanufacturersatan“ex-manufacturing”price.Theythenselltheirdrugstoretailpharmaciesorfacilitiesatamarked-upprice.ThesefacilitiessubsequentlyselldrugstopatientsataCmargin.Asanexample,Figure7describeshowdrugsmostcommonlyflowfrommanufacturertopatientinIndia’sprivatesector.
Althoughthestructureofprivate-sectorprocure-mentanddistributionwasfairlysimilaramongthecountriesstudied,thenumberof“middle-men”whoprocessdrugorders,andthepricemark-upstheseintermediariescharge,varywidely.Private-sectorpricesandmark-upsinIndiaandSouthAfricaarehighlyregulated,althoughadditionalmarginsmaysometimesbenegotiatedthroughvolumediscountsandrebates.Figure7describestheprivatesectorpricemark-upstructureinIndiaandtheaveragemark-upateachstageofthedrug-flowprocess.Inothercountries,notablyChina,themark-upstruc-tureissounpredictablethatitwouldbemisleadingtostatedefinitenumbers.
Figure 7. India Private-Sector Mark-up Structure
*Bears the risk-burden of procurement
First Point of Sale: Manufacturers work with a series of wholesalers who sell drugs at the ex-manufacturing price to private secondary stockists (distributors) or directly to certain healthcare facilities.
Secondary Stockist Sale: Stockists sell drugs to retail pharmacies, clinics, etc., at a marked-up price that has been predetermined (usually 8%).
Retail Sale: Retail pharmacies and/or providers then sell drugs to patients–again at a marked-up price that has been predetermined (usually 16%). This price to the patient is known as the maximum retail price (MRP).
PRIVATE CLINICS/HOSPITALS*
MANuFACTuRERS
WHOLESALERS
STOCKISTS*
PATIENT
NGOS/ CORPORATE-RUN
FACILITIES*
RETAIL PHARMACIES*
Drug Flow:
Private Sector Channels

Compendium |page��
may2007
5.ProcurementandDistributionofTBDrugsinHighIncomeCountries
5.1 Financing of TB Drugs
AsnotedinSection3.1.2,TBcontrolinthehighincomecountriesstudiedisnotaseparateprogrambutratheranextensionoftheexistinghealthcaresystem.FinancingofTBdrugtreatmentfollowsthesamefinancingpatternsasthatofotherdrugs.
5.2 Procurement of TB Drugs
WhileprocurementofTBdrugsinthepublicsectorsoftheHBCsstudiedismostlycentralized,itisdecentralizedinthepublicsectorsofhighincomemarkets.Insomecases,drugsarepricedthroughapublictendersystem.Forexample,intheUK,anyordersvaluedatorabove£100,000(US$197,000)mustbepricedthoughpublictenderbytheprimarycaretrusts.50InFrance,eachindi-vidualhospitalnegotiatespriceandordersuppliesdirectlywiththewholesaler.TheonlyexceptiontothisisforhospitalbuyinggroupsinLyonandParis,thetwolargestcities,whichmayusepurchasingcollectivestonegotiatevolumediscounts.However,mostfrequently,thepricesofdrugsaredirectlynegotiatedbyfunders(e.g.,privateinsuranceplans
intheUS)and/orwholesalersthatsupplyhealthcarefacilitiesandretailpharmacies.
ThedistributionofTBdrugsinhighincomecountriesoperatesalmostentirelybythepullsystem.51ThisislikelybecausethevolumeofTBdrugsneededissmallandtheprocurementanddistributionsystemsareoftendecentralized.Inthesemarkets,thevolumeandfrequencyofdrugordersaredeterminedonareal-timebasisandbufferstocksarekeptatsmalllevels,ifatall.Furthermore,thepullsystemiseasilysupportedbytheinfrastructuresinhighincomemarkets.Facilitiesandretailpharmaciesoftenhaveelectronicstockmaintenanceprogramsthatprovidealertswhennewproductsneedtobeordered.Thesmallsizeofordersandtheeaseoftransportationallowfacilitiesandretailpharmaciestoquicklyreplenishtheirstocks,ifnecessary.
5.3 Flow of Drugs
ThedistributionofdrugsinhighincomecountriesalsodifferssignificantlyfromthatinHBCs.UnliketheHBCsstudied,whichmaintaincompletely
Drug Flow:
Figure 8. Comparison of Typical Drug Flow in High Income Countries
MANuFACTuRERS
WHOLESALERS/DISTRIBuTORS
PATIENT
HEALTHCAREFACILITIES
RETAIL PHARMACIES
MANuFACTuRERS
CENTRALIZED WAREHOuSE
PATIENT
HOSPITALPHARMACIES
Private Sector Channels
Public Hospitals (Buying Group)
50 Primary care trusts are responsible for setting healthcare budgets for all NHS Hospital Trusts and general practitioners (GPs) in their area and allocating resources across settings.
51 In the US, some states also use a push system, with the state providing free supply and distribution of drugs to regional or local health units.

page��| TBallianCe
paThwayTopaTienTs
separatedistributionroutesforthepublicandprivatesectors,TBdrugsinthehighincomemarketsstudiedflowthroughoverlappingdistributionroutes,regardlessofhowthedrugsarefunded.Ratherthanpassingthroughaseriesofgovernmentdepots,TBdrugsinthehighincomemarketsflowthroughthesamechannelsasanyotherlegalmedicines—frommanufacturerstowholesalers,tofacilitiesorretailpharmacies,andfinallytopatients.Insomecases,
drugsmayflowthroughacentralizedwarehousethatservesaregionorpurchasinggroup.Forexample,inPariscertainhospitalretailpharmaciesarepermittedtoconsolidatetheirorders.Figure8onthepreviouspageprovidesacomparisonofthetypicalflowofTBdrugsthroughcentralizedwarehousesvs.wholesalersinhighincomecountries.
6.CostofTreatmentofTBinBothHighBurdenandHighIncomeCountries
6.1 Prices of TB Drug Regimens
TBdrugpricesinthepublicsectorcanvarysignifi-cantlybycountrybasedonsupplysourcesusedandtheprocessthroughwhichdrugsareprocured.IntheHBCsstudied,andinsomecasesFranceandtheUK,procurementofdrugsinthepublicsectorisadministeredthroughapublicbiddingprocessinwhichmanufacturersbidtosupplyTBmedicines.Priceisthusdeterminedaspartofthebiddingprocess.Inothercountries,pricesmaybenegotiatedbyeachfacility,eitherwithwholesalersordirectlywithmanufacturers.
Pricesalsovarybecausesupplysourcesdifferbycountry.Forinstance,inChinaandSouthAfrica,localmanufacturersareutilizedasaresultofthebiddingprocess.InBrazil,rawmaterialsareprocuredthroughabiddingprocessanddrugsareproducedbystatelaboratories.InthePhilippines,theNTPprocuresfromtheGDFandpricesareestablishedduringtheGDF/manufacturerbiddingprocess.AdditionaldrugsupplyinthePhilippinesisprocuredbylocalgovernmentunitsfromlocalandmultina-tionalmanufacturers,throughwhichdrugpricesaresignificantlyhigher.InIndia,theNTPprocuresfromacombinationoflocalsuppliersandtheGDF.Ex-amplesofhowpricesforvariousTBdrugregimenscanvarybetweenthecountriesstudiedareillustratedinTables4and5onthefollowingpage.
6.2 Public and Private Pricing
Pricesofdrugsalsodiffersignificantlybetweentheprivateandpublicsectorsinbothburdenandhighincomecountries.IntheHBCsstudiedthathavesizeablepublicandprivateTBsectors(i.e.,IndiaandthePhilippines),drugprocurementintheprivatesectorismoreexpensivethaninthepublicsector.Thisislikelyduetosupplysources—forexample,whetherdrugsareprocuredfromtheGDF,fromlocalmanufacturers,orfrommultinationaldrugmanufacturers.Differencesindrugprocure-mentcostsbetweenthepublicandprivatesectorsalsostemfromthevaryingprocurementprocesses.Theseincludenationalbidding,localbidding,ordirectnegotiationswithmanufacturers.Moreover,pricemark-upsoccurregularlyalongthesupplychaininprivate-sectors.
Tables6and7onthefollowingpageprovideexamplesofthecostsofvariousTBdrugregimensinthepublicvs.privatesectorsinIndiaandPhilip-pines.InthePhilippines,pricesdifferbecausethepublicsectorisabletoutilizetheGDFandobtaindirectsupplyatalownegotiatedprice.Privatesectordrugprocurementoperatesthroughthetraditionalpharmaceuticalpathwayandfacesadditionalmark-upsthatoccuralongthesupplychain.
InthepublicsectorinIndia,drugsareprocuredthroughtwomajorpathways,theRNTCPandthenon-RNTCP.TheRNTCPutilizestheGDFforabout50percentofpatients.Fortheotherhalf,theRNTCPobtainsdrugsthroughacentrally-adminis-teredbidandtenderprocesstochoosemanufacturersanddrivedowncosts.Thefewpublicfacilitiesthat

Compendium |page��
may2007
52 Prices refer to cost of full drug treatment regimen. 53 Prices refer to cost of full drug treatment regimen.
Table 5. National TB Control Programs Public Sector Prices in Studied High-Income Countries53
ACTIVE SOURCE
France $270.92 Local and Multi-national manufacturers
UK $489.83 Local and Multi-national manufacturers
USA $409.79 Local and Multi-national manufacturers
Table 4. Select Public-Sector Prices in HBCs52
CATEGORy I CATEGORy II CATEGORy III SOURCE
Brazil $41 $69 $62 Drugs traditionally produced internally (Scheme 1) (Scheme 1R) (Scheme 2) through state, military or national laboratories.
China $8-17 $14-27 $8-11 Sourced from national manufacturers. Procured through competitive bidding process. Prices differ based on bid (central, JICA or WB funds).
India $10 $18 $8 GDF (loose drugs)
Philippines $18 $33 $18 Categories I and III procured by the national TB program from GDF (patient kits and FDCs); Category II procured from local government units and patients from local manufacturers.
South Africa $47 $127 $47 Sourced from multinational manufacturers with production facilities in South Africa (Sanofi-aventis and Sandoz).
Note: In South Africa, smear negative and extrapulmonary are treated as Category I.
Table 6. Private vs. Public Costs of a Full Course Treatment in the Philippines (Drugs Only)
TREATMENT COST OF DRUGS IN COST OF THERAPy CATEGORy THE PRIVATE SECTOR ($) USING GDF PRODUCTS ($)
Philippines Category I $135.36 $17.89
Category II $315.84 $32.50
Category III $135.36 $17.89
Table 7. Private vs Public Cost of Full Course of Category I Treatment in India (Drugs Only)
Note: All amounts in US$.
TREATMENT COST OF DRUGS IN COST OF THERAPy CATEGORy THE PRIVATE SECTOR ($) USING GDF PRODUCTS ($)
India Category I $135.36 $17.89

page��| TBallianCe
paThwayTopaTienTs
Figure 9. Prices in the uS Across Different Settings54
0% 20% 40% 60% 80% 100%
Patient Assistance Programs
340B
Federal Supply Schedule Service
Wholesale Acquisition Cost (WAC)-Market Price
Average Wholesale Price (AWP)
20%
46%
50%
57%
100%
Veterans Affairs Price
Discount
Market Price
54 States, and the 340B Drug Pricing Program, 2006 edition. Average Wholesale Price (AWP) defines the list price published in RedBook, currently used only as a reference to negotiate discounts. Wholesaler Acquisition Cost (WAC) is typically at 20 percent below AWP; usually referred to as the market price. Federal Supply Schedule Price, VA Price, and 340B are all set discounted prices calculated based on Medicaid best price available for all federally covered entities.
arenotprocuringtheirdrugsthroughtheRNTCPnegotiatedirectlywithmanufacturerstoobtainthelowestpricepossible,orthroughabidandtenderprocesssimilartothatusedbytheRNTCP.Privatemarketdrugsarepurchasedthroughwholesalers,stockistsandretailersandfacehighmark-upsateachlevel.
PricesforTBdrugsintheUS—theonlyhighincomecountrystudiedwithasizableprivateTBmarket—differbasedonwhetherpayersareprivateinsurancecompaniesorapubliclyadministered
programsuchasMedicaid.Intheprivatesector,manufacturerssetalistpriceandinsuranceplansnegotiatewithmanufacturersforrebates.However,inthepublicsectorpricesarepartiallysetbythefederalgovernment.Thegovernment’spricelevelisrequiredtobesetatorbelowthebestpriceofferedtocommercialplanswhichistypicallyatorbelowtheWholesaleAcquisitionCost(WAC)price,andmanufacturersbidatthatpriceorlessforgovernmentbusiness.Asaresult,pricesdifferacrossdifferentsettings,asshowninFigure9.
7.ValueEstimatesForFirst-andSecond-LineTBDrugs
AkeyobjectiveofPathway to Patientswastocollectsufficientdatatoprojectaglobalestimateofthemarketforfirst-lineTBdrugs,basedonthevalueoftheTBdrugmarketineachofthecountriesstudied.
Thissectiondescribesthefirst-andsecond-lineTBdrugmarketvalueestimatescalculatedforeachofthetencountriesstudiedandonaglobalaggregatelevel.Abriefdescriptionofthemethodologyusedtodetermineboththecountryandglobalestimatesisprovided,aswellasinformationoneachhighburdenandhighincomecountry.Valueestimatesforfirst-andsecond-linedrugmarketsareprovidedbycountryand,whereavailable,patientvolumenumbersarealsoincluded.Finally,basedonanextrapolation,thestudyestimatestheglobalmarket
valueforfirst-lineTBdrugs.BecauseMDR-TBpatientregimensvarysignificantly,itwasimpossibletoquantifytreatedMDR-TBpatientsandestimateaglobalmarketvalueforsecond-lineTBdrugs.
7.1 Overview of Methodology
ThemethodologyusedtodeterminethevalueoftheTBdrugmarketineachcountryincludedinPathway to Patientsvariedaccordingtothedataavailable.Thevalueofthepublicmarketswasinmostcasessourceddirectlyfromdiscussionswithstakeholders—usuallygovernmentofficialsorkeyfunders—orfromfinancialreportsissuedbyNTPs.ForSouthAfrica,figuresforthepublicsectorweresourcedfromthetwosupplierschosenthroughthegovernmenttender.Whenreliablepatientfiguresand
0% 20% 40% 60% 80% 100%
Patient Assistance Programs
340B
Federal Supply Schedule Service
Wholesale Acquisition Cost (WAC)-Market Price
Average Wholesale Price (AWP)
20%
46%
50%
57%
100%
Veterans Affairs Price
Discount
Market Price
0% 20% 40% 60% 80% 100%
Patient Assistance Programs
340B
Federal Supply Schedule Service
Wholesale Acquisition Cost (WAC)-Market Price
Average Wholesale Price (AWP)
20%
46%
50%
57%
100%
Veterans Affairs Price
Discount
Market Price

Compendium |page��
may2007
drugpriceswereavailable,abottom-upcalculationwasconductedtovalidatetop-linefigures.
Private-sectorfiguresweresourcedfromIMSHealthdatabasesandsegmentedbyproductintothefirst-andsecond-linemarket.Becauseprelimi-naryanalysisoffirst-lineprescriptiondataindicatedthatalmostallfirst-linedrugsforTBwereusedexclusivelyforTBtreatment,figuresforthesedrugswereleftunadjusted.However,prescriptiondata—availableformostcountriesinthestudy—wereusedtoadjustsecond-linefigures.55ThepercentageofprescriptionswrittenforTBforeachdrugwasmultipliedbythetop-linesalesfigureforthedrugtocalculatethesecond-lineTBdrugmarketvalue.
Formoreinformationaboutthespecificmethodol-ogyusedtodeterminethemarketestimatesforeachcountryandtheglobalestimates,includingindividualdrugcostfiguresandalistofthecountriesincludedintheglobalextrapolation,aseparatemethodologydocumentisavailableonlineatwww.tballiance.org.
7.2 Country-by-Country Estimates
Forthetencountriesstudied,publicandprivatesectorvaluedataforfirst-andsecond-linedrugsweredeterminedusingIMSandprogramdata(seeTable8).First-linevalueisdefinedasthetotalvalueofthefirst-lineregimen(rifampicin,isoniazid,ethambutol,andpyrazinamide).Volumeisdefinedbythenumberofpatients,ratherthanunits,sinceregimensmayvarybycountryandactualadherencemaydifferaswell.
Estimatingpatientvolumeintheprivatesectorisextremelychallengingbecausetreatmentregimensofferedmayvarysignificantlyandactualadherenceisunknown.Therefore,estimatesonprivate-sectorvolumewerenotconsideredreliableenoughtoincludeinthisreport.
However,thetotalvalueofthesecond-linemarketinthepublicandprivatesectorsinthecountriesstudiedwascalculated.Intheinstanceswherevolumedataarecollectedforsecond-linepatientsinthepublicsector(e.g.,BrazilandthePhilip-pines),volumecalculationsweredevelopedforthesecond-linemarket.Fortheprivatesector,volumewasnotcalculatedbecauseofsignificantvariationintreatmentregimensandadherence.Suchvariationrenderedestimatestoouncertaintoyieldaconfident
Table 8. First- and Second-Line Market Values in Each Country Studied
* China first-line private market sales could not entirely be extricated from public sales, so exact figures are not available at this time.** Some of India’s public-sector facilities may procure second-line drugs directly, but figures for such sales were not available.
Interviews suggest that such purchases are unusual.*** Figure does not include Category III drugs, which are procured primarily by Local Government Units.
The estimated value of Category III drugs is US$908,865.
Note: All figures in US$. NA = not available
FIRST-LINE PUBLIC FIRST-LINE PRIVATE SECOND-LINE PUBLIC SECOND-LINE PRIVATE
Brazil $4.9 million NA $5.0 million NA
China $20 million Unknown* NA $25 million
India $24.25 million $61.2 million Unknown** $8.4 million
Indonesia $5.75 million $8.96 million NA $2.7 million
Philippines*** $2.16 million $28.9 million $58,600 $13,100
South Africa $18.31 million $940,000 $1.71 million $850,000
France $3.6 million NA $4.0 million NA
Japan $11.3 million NA $1.99 million NA
UK $4 million NA $4.5 million NA
US $16.2 million $4.01 million
55 Not available for China or the Philippines.

page�0| TBallianCe
paThwayTopaTienTs
globalsecond-linevalueprojection.FollowingareTBdrugmarketvalueestimatesforthetencountriesstudied(SeeFigure10).
Brazil
TheBrazilianTBdrugmarketisvaluedatapproxi-matelyUS$10million,allofwhichisaccountedforinthepublicsector.Thevalueofthetotalmarketisnearlyevenlysplitbetweenfirst-linedrugs(US$4.9million)andsecond-linedrugs(US$5million).However,duetothemuchhighercostofsecond-linetreatment,thefirst-linemarketismuchlargerintermsofpatientvolume.Thereareapproximately115,000first-lineTBdrugrecipientsinBrazilandonly5,000patientswhoreceivesecond-linedrugs.
China
Thecombinedfirst-andsecond-lineTBdrugmarketinChinaisvaluedatUS$45million.Thefirst-linemarketispredominantlyapublicmarket.
Public-sectorreportsfrom2005indicatethat789,189patientsweretreatedandapproximatelyUS$20millionwasspentonfirst-linedrugs.Thetotalvalueforfirst-linedrugsprocuredthroughnationaltenderswasapproximatelyUS$10.8million.AnadditionalUS$8.9millionaccountsfordrugsfundedlocally.Thisincludesexpendituresbyboththeprivateandpublicsectors,thoughresearchindicatesthatthemajorityof“locallyprocured”drugsarefinancedbythepublicsector.
Unlikethefirst-linemarket,thesecond-linemarketinChinaisexclusivelyprivate.ItsvalueisapproximatelyUS$25million.
india
ThetotalTBdrugmarketinIndiaisvaluedatapproximatelyUS$94million,about74percentofwhichisrepresentedintheprivatesector.India’smarketispredominantlyfirst-line,valued
Figure 10. First- and Second-line TB Drug Market Value by Country
l First-line Drug (Public Market) l First-line Drug (Private Market) l Second-line Drug (Public Market) l Second-line Drug (Private Market)
(USD millions)
$0 $10 $20 $30 $40 $50 $60 $70 $80 $90 $100
Brazil
China*
India
Indonesia
Phillipines
South Africa
France
Japan
UK
US*
4.9 5.0
20.0 25.0
5.75 8.96 2.7
2.16 0.0130.05928.9
24.25 61.2 8.4
11.3 2.0
18.3 1.7
3.6 4.0
4.0 4.5
16.2 4.0
0.94 0.85
high Burden
high inCome
(USD millions)
$0 $10 $20 $30 $40 $50 $60 $70 $80 $90 $100
Brazil
China*
India
Indonesia
Phillipines
South Africa
France
Japan
UK
US*
4.9 5.0
20.0 25.0
5.75 8.96 2.7
2.16 0.0130.05928.9
24.25 61.2 8.4
11.3 2.0
18.3 1.7
3.6 4.0
4.0 4.5
16.2 4.0
0.94 0.85
* Although exact figures are unknown, the majority of first-line treatment is financed by the public sector. In the US, this is also true for second-line treatments.
(USD millions)
$0 $10 $20 $30 $40 $50 $60 $70 $80 $90 $100
Brazil
China*
India
Indonesia
Phillipines
South Africa
France
Japan
UK
US*
4.9 5.0
20.0 25.0
5.75 8.96 2.7
2.16 0.0130.05928.9
24.25 61.2 8.4
11.3 2.0
18.3 1.7
3.6 4.0
4.0 4.5
16.2 4.0
0.94 0.85

Compendium |page��
may2007
atUS$85.45million,withbothpublicandprivatepayers.Payersrepresentingthepublicsector,whichinitiatestreatmentin1.5millionpatientsperyear,purchaseapproximatelyUS$24.3millioninTBdrugs.Theprivatesector,whosepatientnumberscannotbeestimatedwithaccuracy,accountsfortheremainingUS$61.2million.
AsisthecaseinChina,thesecond-linemarketinIndiaisfoundonlyintheprivatesector,thoughspendingbythepublicsectorinthisareawillbegintoincreaseinthenextthreetofiveyearsasDOTS-Pluspilotprojectsareimplemented.Thesecond-linemarketiscurrentlyvaluedatUS$8.4million.
indonesia
ThetotalIndonesianTBdrugmarketisvaluedatUS$17.4million,abouttwothirdsofwhichisspentintheprivatesector(US$11.7million),andathirdofwhichisspentinthepublicsector(US$5.75million).AsinotherHBCs,first-linedrugsaccountformostofthemarket,withsalesfiguresatapproximatelyUS$14.7million,or85percentofthetotal.Thefirst-linemarketissplit61percentand39percentbetweentheprivateandpublicsectors,respectively.
Indonesia’spublicprogramdoesnotdistributesecond-linedrugsatthistime.Thesecond-linemarketisentirelyprivateandhasanestimatedvalueofUS$2.7million.
PhiliPPines
AsinIndia,thevalueoftheTBdrugmarketinthePhilippinesispredominantlyprivate.Thevalueofthecombinedfirst-andsecond-linemarketisapproximatelyUS$31.13million,93percentofwhichisaccountedforintheprivatesector.Thefirst-linemarket,valuedatUS$31.1million,isalmostentirelyprivate.Thepublicsector,inwhichabout135,000patientsaretreatedperyear,accountsforUS$2.16millionperyear.ThisfiguredoesnotincludeCategoryIIIdrugs,whichareprocuredprimarilyviapublictenderbyLocalGovernmentUnits(LGUS).TheestimatedvalueofCategoryIIIdrugsisUS$908,865.Thesecond-linemarket,whichaccountsforlessthanUS$100,000peryear,isdominatedbypublic-sectorexpenditures(approximatelyUS$58,600).Presently,theprivatesectoronlyspendsapproximatelyUS$13,100peryearonsecond-linedrugs.However,treatmentofMDR-TBisexpectedtogrowoverthenextfiveyears.
south afriCa
ThevalueoftheSouthAfricanTBdrugmarketisestimatedatapproximatelyUS$21.8million,nearlyallofwhichisspentinthepublicsectoronfirst-linedrugs.OftheUS$19.25millionfirst-linemarketinSouthAfrica,almost95percent(US$18.31million),ispurchasedinthepublicsector.Proportionally,theprivatesectorplaysalargerroleinthesecond-linemarket,representingaboutonethird,orUS$850,000,oftheUS$2.56millionmarket.
high inCome marKets
SalesandpatientfiguresforthehighincomemarketsstudiedinPathway to PatientsweremoreeasilyaccessedthandataforHBCs.However,pricingoftreatmentregimenswasdifficulttoascertain,whichmadeitdifficulttovalidatethroughbottom-upcalculations.
Ofthehighincomecountriesstudied,JapanhadthehighestincidenceofTBinfection.In2004,therewereapproximately30,000newlyregisteredcasesandthepercentageofpatientswithMDR-TBwaslessthanonepercent.ThevalueoftheJapanesedrugmarket,whichisentirelypublic,isestimatedatUS$13.3million,withUS$11.3millionrepresentingthefirst-linemarket.
TheFrenchandBritishTBdrugmarketsarealsoentirelypublicandarevaluedatapproximatelyUS$7.6millionandUS$8.5million,respectively.ThemarketvalueinFranceissplitbetweenfirst-linetreatment(US$3.6million)andsecond-linetreatment(US$4million).AsinFrance,thetotalBritishTBdrugmarketissplitbetweenfirst-linetreatment(US$4million)andsecond-linetreatment(US$4.5million).
TheUSreportedapproximately14,000newcasesofTBin2005,lessthanonepercentofwhichwereMDR-TB.ThetotalUSmarketvalueforTBdrugsisapproximatelyUS$20.21million,82percentofwhichisrepresentedbyfirst-linetreatment(US$16.2million)withtheremainingUS$4.01millionrepresentingsecond-linetreatment.

page��| TBallianCe
paThwayTopaTienTs
7.3 Global Estimates
First-line treatmentAsnotedearlier,thesixhighburdencountriesstudiedrepresentapproximately60percentofTBdiseaseinthe22highburdencountriesandalltencountriesstudiedaccountforapproximately50percentofthetotalglobalTBburden.
Researcherswereabletoextrapolatethefirst-everestimateoftheglobalmarketbasedonoriginalresearchbyusingthedataofthecountriesstudiedtoyieldthefollowingprojectionsonaworldwidescale:
1)Alowendestimate,basedonDOTSnotificationrates(actualnumberofcasesreportedeachyear)andarangeofactualandaveragepriceperpatientregimencosts,suggeststhatthevalueoftheglobalfirst-linemarketisbetweenUS$261M–316M.
2)Ahighendestimate,basedontheWHO’sglobalincidencefigures(totalprojectednumberofnewcases)andarangeofactualandaveragepriceperpatientregimencosts,suggeststhatthevalueoftheglobalfirst-linemarketisbetweenUS$310M–418M.
Assumingthatcurrentcasenotificationratesdonotalwaysreflectthefullnumberofpatientsbeingtreated,andthatincidenceratesreflecttheabsolutemaximumnumberofpatientsthatcanbetreated,
theoverlapofthetworangesistheclosestestimateoftheactualfirst-linemarket,indicatingthatthetotalvalueoftheglobalmarketforfirst-lineTBdrugsisapproximatelyUS$315M(seeFigure11).
Second-line TreatmentThestudyfoundthatanumberoffactorspreventmakingasimilar,globalestimateofthesecond-lineTBdrugmarket.AccordingtotheStopTBPartnership’sGlobalPlantoStopTB2006-2015,lessthantwopercentofestimatedculturepositiveMDR-TBpatientsaretreatedappropriately.CasesofMDR-TBarenotconsistentlyreported,particularlyiftheyarenottreatedinthepublicsector.Thereareanumberofpotentialtreatmentsincludedinsecond-lineregimens,andthereisvarianceinprescribingpractices,lengthofregimenaswellasadherencerates.Similarly,costsalsovarydramaticallyacrosscountriesandthereisnorealistic“averagecost”forsecond-lineregimens.Therefore,researchersfeltitisinappropriatetoapplythemethodologyusedtoprojectthefirst-lineglobalestimatetoasecond-lineworldwideestimate.
However,lookingonlyatthetencountriesstudied,theresearchfoundthattheestimatedvalueofthesecond-lineTBdrugmarketinthosecountriesisapproximatelyUS$54M.
Figure 11. Global Estimate Ranges of First-Line TB Drug Market
(US
D m
illio
ns)
250
300
350
400
450
Low End Range High End Range Estimated Actual Market Value
US$261M
OverlapUS$310M–316M
US$418M
Low end range defined based on case notification approach; High end range based on incidence.

Compendium |page��
may2007
8.AdditionalConsiderations
Pathway to Patientsprovidesin-depthinsightintoissuesthataffectthedynamicsoftoday’sTBdrugmarket.Thesefindingshelpmapfactorsthatwillhavedirectandindirectimpactonmarketdynamicsbetweennowandthetimenoveldrugregimensareapprovedandreadyforintroductionintotheglobalmarketplace.However,thisanalysisalsosuggeststheneedforadditionalresearchorexplanation.
Quality of TB services, programs and processesAsmentionedintheintroduction,thisresearchdidnotrevieworaddressthequalityofTBservicesortheprocurementanddistributioninthecountriesstudied.Instead,itsoughtonlytodescribethem.Issuesrelatedtothedegreetowhichthosesystemsfunctioneffectively—suchaswhetherthequalityofcareiseffective,whetherpatientsarereceivingDOTS,whetherdemandforecastingisaccurate,orwhetheradequatelevelsofbufferstocksarealwaysonhand—werenotaddressed.
TB control programs in decentralized systems ThecharacterizationoftheTBcontrolprogramsofhighlydecentralizedhealthcaresystems,suchasthosefoundinChinaandSouthAfrica,wouldbenefitfromadditionalstudy.Inthosecountries,theimplementationofTBcontrolvarieswidelyfromprovincetoprovinceandamorerobustanalysisofeachprogram,includingaregion-by-regionstudy,wasnotpossiblewithinthetimeconstraintsofthisproject.Futurestudiesofsuchprogramsshouldincludeacomprehensiveregionalanalysistoensurethatthenuancesoflocalvariationarecaptured.
Data discrepancies regarding value and volume estimates Inmostcases,thedifferentdatasourcesfromwhichfigureswerepulledeithercorroboratedwithoneanotherorcouldbecheckedwithanalternativecalculation.However,inafewinstances,suchasinChina,stakeholderdiscussionsyieldednumbersthatdidnotalign,and/orresearcherswereunabletotriangulateontheactualfiguresthroughabottom-upcalculation.Asystematicauditofeachofthesourcesusedwouldhelptofurtherrefineestimatesinfuturemarketsizingattempts.
Market segmentation of private-sector data Thesegmentationofprivate-sectordataintofirst-lineandsecond-linemarketsalsoposedachallenge.Inmostcountries,IMSHealthprivate-sectordatabasesareaggregatedbyproductandnotindication,sothefirst-linemarketincludesdrugsthatareusedinsecond-linetreatmentandviceversa.Therefore,availableprescriptiondatadidnotalwaysallowresearcherstodistinguishbetweenthefirst-andsec-ond-lineuseofanygivendrug.Improvedabilitytoallocateeachdrug’ssalesandvolumetoitsrespectiveusemightchangethecharacterizationofthemarket.
Lack of estimates for private-sector patient volumeEstimatingthepatientvolumeintheprivatesectorwasnotpossible.Thereasonsstemmedfromvariationsintreatmentregimens,lackofinformationaboutadherence,andlackofdataavailableregardingflowofpatientsbetweenprivateandpublicsectors.AsurveyofprescribingpracticesandadherenceinHBCswithasignificantprivatesectorwouldallowforthedevelopmentofarelativelyreliablevolumeestimateforeachcountry.
Inherent imprecision in extrapolatingFinally,whilethemarketestimatesofthecountriesincludedinthescopeoftheresearchprovidedthebasisforextrapolationtoothercountries,itisclearthatsuchcomparisonsarenotaperfectproxy.Forinstance,Russia’sgroupingintotheHBCswasbasedonitsTBincidence,butthepricesofitsTBdrugsaresignificantlyhigherthaninotherHBCs.The“restofworld”extrapolationalsohasadegreeofuncertainty.Drugpricesforcountriesinthe“restofworld”categorywerealsodeterminedbasedoninformationfromHBCsstudied.Thus,morespecificpricingandutilizationinformationfromthesecountrieswouldallowforamoreexactestimate.

page��| TBallianCe
paThwayTopaTienTs
9.PredictingFutureMarketDynamics
UnderstandingthestructureoftheTBdrugmarket,includingprocurementanddistributionsystemsinhighburdencountries,isessentialforplanningtheintroductionofnewTBdrugregimens.
Potential Market ChangesThisstudyprovidesin-depthinsightsintoissuesthataffectthedynamicsoftheTBdrugmarkettodayandhelpsmapfactorsthatwillhavedirectandindirectimpactonthesedynamicsbetweennowandthetimenoveldrugregimensareapprovedandreadyforintroductionintotheglobalmarketplace.TheanalysisalsosuggeststheneedforadditionalresearchintoanumberofevolvingfactorsthatmayaltertheflowofTBdrugs,highlightingthatabetterunderstandingofallofthisclosertothenewproductsroll-outwouldfacilitateadoptionofandaccesstonewTBdrugswhentheybecomeavailable.
TheGlobalPlancallsforexpanded,equitableaccessforalltoqualityTBdiagnosisandtreatmentby2015.Therefore,effortsundertakenoverthenextdecadetoachievetheGlobalPlan,includingtheintroductionofnewtoolstodiagnose,treatandpreventthedisease,alongwithpolicyandfundingconsiderations,areexpectedtoincreasesignificantlythenumberofpatientsbeingtreatedforTB.
New DiagnosticsNew,fasterandmorereliablediagnostictoolsforTBareinthepipeline,andshouldbegintoenterthemarketoverthenextseveralyears.TheGlobalPlancallsforpointofcarediagnosticsby2010thatwillallowrapid,sensitiveandinexpensivedetectionofactiveTB.Twoyearslater,StopTBenvisionsadiagnostictoolboxthatwillaccuratelyidentifypeoplewithlatentTBinfectionandthoseathighriskofprogressiontodisease.Newdiagnostics,oncedeveloped,shouldleadtoincreasesincasefindingthatwillresultinanincreaseindemandfortreatment.
New DrugsThegoaloftheGlobalPlanistohaveanewshort(one–twomonths)TBregimen(s)by2015.Anumberoftrialsarecurrentlyunderwaythatcould,by2010,potentiallyshortentheregimentothree–fourmonths.Shortenedtreatmentwithnoveldrugsoffersthepotentialtoenhancepatientadherence,decrease
defaultrates,curtailcoststothehealthcaresystemandpatients,andsubstantiallyimproveoutcomesforthoseinfected,especiallyforpatientsco-infectedwithHIVandTB.Ifrealized,theseadvantagesareexpectedtoincreasetheneedanddemandfornewTBdrugs.
TheexpansionofdrugresistantTBworldwideisaf-fectingmarketdynamics.ThisisexpectedtoincreasebecausecountriesarebeginningtoincludetreatmentofMDR-TBandXDR-TBaspartoftheirnationalTBcontrolprograms.Expandingthecoverageofdrug-resistantTBwillincreasethemarketdemandforsecond-linedrugs.
Patientaccesstonoveltherapieswillrequirenationalandinternationaladoptionofnewtreatmentsandextensive“retooling”ofTBprogramstoaccommo-datechangesintheregimen.Anumberofelements,includingcost,availabilityandeaseofadministra-tionwillhaveadirectimpactonadoptionofnewtherapies.Fullyunderstandingtheseandotherfactorswillbecriticalforimplementationofnewshorterregimensworldwide.
New VaccineWhilenumerousfactorsleadtothepotentialofincreasednumbersofpatientsbeingtreated,resultinginlargerdemandforTBdrugs,otherscouldleadtoalonger-termdecreaseinmarketdemand.Specifically,theGlobalPlancallsforanew,safe,effectiveandaffordablevaccinetobeavailableby2015.Thecurrentvaccineis85yearsold,worksonlyinchildren,andisnotalwayseffective.Anewpreventivevaccinethatworkstoprotectallagegroupshasthepotential,ifwidelyadoptedandused,toprovideapositiveimpactonTBcontroland,inthelong-term,asignificantreductioninthenumberofthoserequiringtreatment.
ItwillbeimportanttounderstandthepotentialeffectsofasuccessfulvaccineonTBdrugdemandandthemarket.Furtherstudyofthisinterfacewillbepossiblewhenmoreisknownabouttheprofileofanewvaccine.
Policy InfluencesPolicychangeshavethepotentialtoincreasethenumberofpatientstreated,therebyaffectingthemarketdynamicsandhighlightingtheneedfor

Compendium |page��
may2007
closemonitoringofthesechangesintheyearsahead.AnexampleisChina’srecentdecisiontoincludetreatmentofsmearnegativepatientsasapartofitsnationalTBcontrolprogram,whichaddspatientsandincreasestheamountofdrugsneededbythepublicprogram.Similarly,theexpansionofpublicsectorfundingfortreatmentofdrugresistantTBinmarketslikeIndia,ChinaandthePhilippines,albeitslow,willincreasethenumberofpatientsreceivingsecond-linedrugsand,overtime,willchangethevaluedynamicsofthatmarket.
Inthepast15years,publicsectorTBprogramshavedramaticallyexpandedinmanyhighburdencountries.Inthosecountrieswithlargeprivatesectormarkets,likeIndiaandthePhilippines,thereisaslowtrendofpatientsmovingfromprivatetopublicsectortreatment,largelyduetogovernmentimplementationofWHO-recommended“public-privatemix”programs.Thiscouldresultinadecreaseinthevalueoftheprivatemarket,butanincreaseinvalueofthepublictendermarket.
Funding InfluencesWithwidespreadcommitmenttotheGlobalPlanandtheintroductionofnewfinancingmechanismsandcommitmentsbytheUN,G8,anddonorandhighburdencountries,itisexpectedthatTBcontrolprogramswillcontinuetoexpandandstrengthenoverthenexttenyears.However,theextenttowhichthedrugmarketrespondstothisexpansionwilldependonanumberofvariables.
Inthecountriesstudied,mostfundingusedforTBdrugs,whetherfromthepublicorprivatesectors,comesfromdomesticsources.Somehighburdencountries,however,aredependentonexternaldonorfundingtoenhancetheirnationalcommitment,especiallyforsecond-linedrugsandpediatricTBmedication.Newfundingschemes,suchastheGlobalFundforAIDS,TBandMalaria(GFATM)andUNITAID,aninternationaldruganddiagnos-ticspurchasefacility,mayofferincreasedaccesstosecond-lineTBmedicationsovertime.Thus,markets—especiallyforsecond-linedrugs—willcontinuetobesusceptibletotrendsandchangesinfunding.
�0.Conclusions
Pathway to PatientsstudiedtheTBdrugmarketplaceintencountries,providingacomprehensiveunder-standingofcountry-specificdataandananalysisofprocurementanddistributionsystemsineightofthesecountriesandatthegloballevel.Thestudypointstothevariabilityofthemarketdynamicsamongthecountriesstudied,thecomplexitiesoftheissuesfaced,andthefragmentednatureofthemarket.
The MarketThestudy’scurrentglobalestimateforfirst-lineTBdrugsisapproximatelyUS$315Mperyear,includ-inghighincomecountrysales.Thisprojectionisconsistentwiththatofferedinthe2001studyThe Economics of TB Drug Development56which,usingadifferentmethodology,estimatedthefirst-linemarketin2001atapproximatelyUS$350M.
Whilethetotalmarketestimateisnotinconsider-able,theTBmarketplaceishighlyfragmentedbecauseitissharedbymorethanfourdrugsandamultiplicityofsuppliers.Thisfragmentationisnotlikelytochange.First,successfultreatmentof
TBwillmostlikelyrequireacombinationtherapy.Second,asthestudysuggests,domesticdrugproductionfacilitiesmaybeintegraltomarketentryfornewTBdrugsinmostcountriesstudiedandlikelyinothers.
Atpresent,thereisalsoalimitedcommercialmarketforsecond-lineTBdrugs.WhiletheMDRandXDR-TBmarketshaverevenue-generatingpotential,currentaccessinmostcountriesisprimarilyrestrictedtotheprivatesector,withpricesthatseverelylimitaccessformostpatientswithdrugresistantTB.Tappingthismarketwouldrequireasignificantexpansionofpublicsectortreatmentprograms,aswellasgovernment-ordonor-sponsoredpurchaseandprocurement.
Inthehighincomecountriesstudied,thetotalTBmarketisrelativelysmall,withpricingandprocure-mentfollowingthesamepricingsystemsasotherpharmaceuticals.France,Japan,theUKandtheUScombined—accountingfor61percentofthetotalglobalpharmaceuticalmarket57—purchaselessthanUS$50MworthofTBdrugs.
56 Executive Summary for The Economics of TB Drug Development. Global Alliance for TB Drug Development. October, 2001.57 IMS Knowledge Link. http://www.imsknowledgelink.com.

page��| TBallianCe
paThwayTopaTienTs
Lessons Learned from High Burden CountriesThestudysuggeststhatcarefulplanningwillbeneededtoacceleratetheadoptionofanynewTBdrugregimeninthehighburdencountries.ResearchconfirmsthepreferenceofmanycountriestopurchaseTBdrugsdirectlyfromlocalsuppliersandnotfromtheglobalmarketplace.AlthoughtheGDFservicesanumberofcountries,especiallythosethatlacklocalmanufacturersorqualityassurancecapacity,mostpurchasersforthepublicsectormarketsstudiedshowastrongpreferenceforprocurementfromdomesticmanufacturers.Itwillbeessentialtoresearchthisissuefurther,includingotherhighburdencountries,beforedevelopingroll-outplansfornewTBdrugs.
Thestudyalsosuggeststhatthelaunchofanynewdrugregimenwillrequireaphasedroll-outinhighburdencountries.Drugapprovalbyregulatoryauthoritiesisonlythefirststeptowardadoption.ThenationalTBprogrammustthendecideifitwillincludethenewtherapyaspartofthetreatmentregimen.Thus,accesstopublicsectormarketswillrequireanunderstandingoftheprocessesbywhichnewregimensareadoptedbynationalTBprogramsaswellasthepublictendersystemsandtheirrequirements.
Evenafteradoption,nationalroll-outleadingtoactualpatientaccesswilltaketimebecausecountrieswillneedtounderstandtheimpactofanewregimenonservicedeliveryandexistingsupply.Also,bufferstocksofexistingmedicationsmustbeexhaustedfromboththeGDFandnationalstores.Planningforappropriateproductionwillrequireanunderstandingofhowlongitwouldtakepost-approvalforhighburdencountriestoimplementachangeintherapy.Collaborationwithdiseasecontrolprogramsanddonoragencieswhichhaveworkedonsupplychainissuesinotherareas,suchasmalariaandHIV,wouldbehelpfulinsuchplanning.
Lessons Learned from High Income CountriesTBisdetectedthroughoutthehighincomecountriesstudied,althoughmostdiagnosedandtreatedcasesareconcentratedinthemajorcities.Intheseeconomies,anumberofmedicalspecialtiesandsubspecialtiestreatTB,withphysiciansdecidingwhichtreatmentregimenstouse.Combinedwithotherfactors,thisdynamicsuggeststhatnewTBdrugsandregimenswillrequireanawarenessbuildingcampaignand/orsubstantialmarketingeffortstoreachthesedoctors.
Summary ObservationsAlthoughthisstudyfoundsomesimilaritiesacrossmarkets,thecriticalfindingwiththesupplychainforTBdrugswasthevariabilitybycountry.Therehasbeenarecentcallforaglobal“infomediary”togatherandorganizemarketdataforlowandmiddleincomecountries,acrossdiseaseareas,andactasanintermediarybetweenthosewhosupplytheinformation,suchasnationalTBcontrolprograms,andthosewhowanttheinformationtoassistsupplierswithdemandforecasting,reducedelaysandensureconsistentsupply.58Thisresearchsuggeststhataglobal“infomediary”couldbeextremelyhelpfultothedevelopmentandroll-outofnewTBdrugs,byprovidingefficientandcost-effectiveinformationsharing.
Thisstudyprovidesuniqueinsightintothecomplexityoftoday’sglobalTBmarket.Justasresearchanddevelopmentintonewcompoundsrequiresmanystagesbeforeadrugisreadyforregulatoryapprovalanduse,preparingtheworldforrapiduniversaladoptionanduseofnewTBtreatmentswillrequiretheunderstandingofmarketdynamics,perceivedbenefitsofthenewregimens,manufacturingandsupplychainissues,operationalchangesnecessitatedbynewtherapies,donorpolicies,priceelasticityofdemandandotherattributesthatwouldjustifythechangeintreatmentregimen.
Giventhemarketintricaciesrevealedinthisresearch,itissafetoconcludethatprovidingtheproperpath-wayforanewgenerationoffasterandeasier-to-useTBdrugstoreachthepatientwillrequireatargetedandinformedcountry-levelandglobalstrategy.
58 Center for Global Development, Global Health Policy Research Network. Consultation Report of the Global Health Forecasting Working Group. February, 2007.

Compendium |page��
may2007
11.Appendices
11.1 Partial List of Acronyms
APHA AmericanPublicHealthAssociation
ARVs antiretrovirals
AWP averagewholesaleprice
BMGF Bill&MelindaGatesFoundation
CDC U.S.CentersforDiseaseControlandPrevention
ChinaCDC ChineseCenterforDiseaseControl andPrevention
CIDA CanadianInternationalDevelopmentAgency
DFID U.K.DepartmentforInternationalDevelopment
DGIS Directorate-GeneralforInternationalCooperation(oftheNetherlandsMinis-tryofForeignAffairs)
DOH DepartmentofHealth
DOTS directlyobservedtherapy,shortcourse
EMB ethambutol
EU EuropeanUnion
FDC fixed-dosecombination
GDF GlobalDrugFacility
GFATM GlobalFundtoFightAIDS,TBandMalaria
GLC GreenLightCommittee
HBC highburdencountry
HR isoniazid,rifampicin
HRE isoniazid,rifampicin,ethambutol
HRZE isoniazid,rifampicin,pyrazinamide,ethambutol
IAPSO Inter-AgencyProcurementServicesOrganization
IBEF IndiaBrandEquityFoundation
IDA InternationalDispensaryAssociation
INH isoniazid
JICA JapanInternationalCooperationAgency
JSI JohnSnowInternational
KNCV RoyalNetherlandsChemicalSociety
MDR-TB multi-drugresistanttuberculosis
MRC MedicalResearchCouncil
MRP maximumretailprice
MSH ManagementSciencesforHealth
NCTB NationalTBControlProgram(China)
NDTI NationalDiseaseandTherapeuticIndex
NGO non-governmentalorganization
NPA IMSHealth’sNational PrescriptionAudit
NSP IMSHealth’sNationalSalesPerspective
NTP nationalTBcontrolprogram
OPPI OrganisationofPharmaceuticalProducersofIndia
PAHO PanAmericanHealthOrganization
PDI PharmacyDOTSInitiative
PhilCAT PhilippinesCoalitionAgainstTuberculosis
PhilTIPS PhilippinesTBInitiativesinthePrivateSector
PIH PartnersInHealth
PPM public-privatemixprograms
PZA pyrazinamide
RIF rifampicin
RNTCP RevisedNationalTBControlProgram(India)
TAC TreatmentActionCampaign
TB tuberculosis
ICD-10 InternationalClassificationofDiseases
UNICEF UnitedNationsChildren’sFund
UNDP UnitedNations DevelopmentProgramme
USAID U.S.AgencyforInternationalDevelopment
WAC wholesaleracquisitioncost
WB WorldBank
WHO WorldHealthOrganization

page��| TBallianCe
paThwayTopaTienTs
11.2 List of Manufacturers (By Country)
BrazilThemajorityofdrugsareproducedbyNationalandStateLaboratories
National:• Farmanguinhos(underFiocruz)
Military:• Army(LQFEX)• AirForce(LQFAE)• Navy(LFM)
State:• FURP(SaoPaulo)• Iquego(Goias)• LAFEPE(Pernambuco)• Nuplan(RioGrandedeNorte)
ChinaManufacturersawardednationaltender:• ShenyangHongqiLuoshanSanjiu• GuoyaoGuorui
Hospitalscanprocurefromanyapprovedmanufacturer.
FranceManufacturersoffirst-linedrugs:• Ethambutol(GenoPharm;SERP;GSK)• Isoniazid(Laphal)• Pyrazinamide(Sanofi-aventis)• Rifampicin(Sandoz;Sanofi-aventis)• Rifampicin+isoniazid(Sanofi-aventis)• Rifampicin+isoniazid+pyrazinamide
(Sanofi-aventis)
Manufacturersofsecond-linedrugs:• Ciprofloxacin(Sandoz)• Clavulanicacid(Sandoz)• Levofloxacin(Sanofi-aventis)• Ofloxacin(Sanofi-aventis,Sandoz)
India• CadilaPharma• ConceptPharma• Lupin• Macleods• OverseasHealthcare• Sandoz-Novartis• ShreyaLifeScience• ThemisMedicare• Wockhardt
Japan• Cycloserine(MeijiMeuiseka)• Ebutol(KakenSeiyaku)• Ethambutol(SandozJapan)• Iscotin(Daiichiseiyaku)• Pyramide(Sankyo)• Rifampicin(SandozJapan,NiproPharma)• Rifandin(Daiichiseiyaku)• Rimactane(NovartisPharmaJapan)• StreptomycinSulfmei(Meuiseka)• Tubermin(Meuiseka)
Philippines• Biomedis• DuncanPharmPhil• Medichem• Natrapharm• PascualLabs• PatriotPharma• PediatricaLab• Sandoz• TerramedicInc.• UnitedAmerican• Westmont• Wyeth
South AfricaManufacturersawardednationaltenders:• Sandoz• Sanofi-aventis
Manufacturersofsecond-linedrugs:• Be-tabsPharmaceuticals• BiotechLaboratories*• BizshelfPharmaceuticals• CapsPharmaceuticals*• PfizerLaboratories*• Sandoz• Sanofi-aventis• InternationalSuppliers
* Suppliers of streptomycin, which is also used in first-line treatment of relapse patients

Compendium |page��
may2007
11.3 Prices of Drugs for Select Countries and Purchasers
China
INTENSIFIED CONTINUATION
PER PER UNIT # PER # OF UNIT # PER # OF TOTAL TOTAL REGIMEN RMB WEEK MONTH RMB WEEK MONTH COST RMB COST USD
CAT I HRZE HR 1.57 3 3 0.62 3 4 86 $ 10.79
CAT II HRZE HRE 1.57 3 3 1.14 3 6 139 $ 17.33
INTENSIFIED CONTINUATION
PER PER UNIT # PER # OF UNIT # PER # OF TOTAL TOTAL REGIMEN RMB WEEK MONTH RMB WEEK MONTH COST RMB COST USD
CAT I HRZE HR 2.10 3 2 0.82 3 4 81 $ 10.13
CAT II HRZE HRE 2.10 3 2 1.52 3 6 138 $ 17.26
CAT III HRZ HR 1.25 3 2 0.82 3 4 66 $ 8.65
Price per regimen for centrally financed drugs (2005)
INTENSIFIED CONTINUATION
PER PER UNIT # PER # OF UNIT # PER # OF TOTAL TOTAL REGIMEN RMB WEEK MONTH RMB WEEK MONTH COST RMB COST USD
CAT I HRZE HR 2.10 3 3 0.82 3 4 115 $ 14.37
CAT II HRZE HRE 2.10 3 3 1.52 3 6 185 $ 23.13
CAT III HRZ HR 1.25 3 3 0.82 3 4 84 $ 10.55
COST PER REGIMEN (ASSUMING 3 MONTHS INTENSIFIED PHASE)
Price per regimen for JICA funded centrally procured drugs (2005)
INTENSIFIED CONTINUATION
PER PER UNIT # PER # OF UNIT # PER # OF TOTAL TOTAL REGIMEN RMB WEEK MONTH RMB WEEK MONTH COST RMB COST USD
CAT I HRZE HR 1.57 3 2 0.62 3 4 67 $ 8.41
CAT II HRZE HRE 1.57 3 2 1.14 3 6 120 $ 14.94
COST PER REGIMEN (ASSUMING 3 MONTHS INTENSIFIED PHASE)
Price per regimen for DFID/WB funded centrally procured drugs (2005)
INTENSIFIED CONTINUATION
PER PER UNIT # PER # OF UNIT # PER # OF TOTAL TOTAL REGIMEN RMB WEEK MONTH RMB WEEK MONTH COST RMB COST USD
CAT I HRZE HR 2.44 3 2 0.93 3 4 103 $ 12.88
CAT II HRZE HRE 2.44 3 2 1.76 3 6 185 $ 23.12
INTENSIFIED CONTINUATION
PER PER UNIT # PER # OF UNIT # PER # OF TOTAL TOTAL REGIMEN RMB WEEK MONTH RMB WEEK MONTH COST RMB COST USD
CAT I HRZE HR 2.44 3 3 0.93 3 4 133 $ 16.56
CAT II HRZE HRE 2.44 3 3 1.76 3 6 215 $ 26.82
COST PER REGIMEN (ASSUMING 3 MONTHS INTENSIFIED PHASE)

page�0| TBallianCe
paThwayTopaTienTs
Philippines
FIRST LINE DRUGS
The cost of First- and Second-Line TB drugs in the private sector
SECOND LINE DRUGS
DRUG MANUFACTURER DOSE COST PER PILL
Myrin P Wyeth HRZE $ 0.23
Myrin Wyeth HRE 0.18
Tritab Unilab HRE 0.20
Quadtab Unilab HRZE 0.18
Ciprofloxacin Local 300 mg $ 0.34 -1.50
Clarithromycin Local 300 mg 1.88
South Africa
Sandoz private-sector prices (uS$)
Sanofi-aventis private-sector prices (uS$)
SANDOZ TRADE NAME PACK SIZE SEP PRICES (VAT ExCLUDED) SEP PRICES (VAT INCLUDED)
Rimactane 150 100 $ 16.50 $ 18.81
Rimactane 300 Vials 1 17.29 19.71
Rimactane 450 100 29.03 33.09
Rimactane 600 100 54.15 61.73
Rimactazid 150/75 60 7.00 7.98
Rimactazid 300/150 40 6.20 7.07
Rimactazid 60/30 40 5.27 6.00
Rimactazid Paed 60/60 80 11.92 13.59
120 17.88 20.38
Rimcure Paed 3-FDC 80 15.93 18.16
120 23.90 27.24
500 99.57 113.51
Rimstar 4-FDC 40 4.60 5.24
60 6.90 7.87
80 9.20 10.49
100 11.50 13.11
500 57.50 65.55
Sandoz Ethambutol HCl 400 100 12.67 14.44
Sandoz Pyrazinamide 500 100 14.72 16.78
SANOFI-AVENTIS TRADE NAME PACK SIZE SEP PRICES (VAT ExCLUDED) SEP PRICES (VAT INCLUDED)
Rifafour e-275 40 $ 4.43 $ 5.05
60 6.64 7.57
80 8.86 10.10
100 11.65 13.29
500 55.35 63.10
Rifinah 300 mg 40 5.83 6.65
Rifater Junior 40 7.00 7.98
40 5.78 6.58

Compendium |page��
may2007
11.4 Interview Lists
GLOBAL STAKEHOLDERS
Marcos Espinal ExecutiveSecretary,StopTBPartnershipSecretariat
Peter Evans Consultant,IndependentconsultanttoGDF
Kathryn FloydActingHeadofTBMonitoringandEvaluation,WHO
Christina FoleyTBAdvisor,CIDA
Ernesto JaramilloMDR-TBWorkingGroupSecretariat,WHO/GLC
Fabienne JoubertonProcurementOfficer(second-line),GDF/GLC
Kathryn Kempton DirectorofDrugProcurement,PIH
Marieke Korsten AreaManager,IDA
Robert Matiru ManagerofOperations,Procurement,GDF/GLC
Elisabetta Molari Procurement,SupplyPolicy&ManagementTeamLeader,GFATM
Poul MullerAccountManager,ProcurementServicesHealthCommodities,UNDP-IAPSO
Sue PerezDonorCountryProjectManager,GlobalTBCampaign,ResultsInternational
Ralph RackPharmaceuticalandLogisticsAdvisor,JohnSnowInc.(JSI)
Jim Rankin Director,CentreforPharmaceuticalManagement,ManagementSciencesforHealth
Mario RaviglioneDirector,StopTBDepartment,WHO
Doris RouseDirector,GlobalHealth,RTIInternational
Jereon van GorkomSeniorConsultant,KNCV
Hilary VaughanSeniorHealthAdvisor,RoyalCrownAgents
Hugo VrakkingProcurementAdvisor,GDF/GLC
Diana WeilSeniorPublicHealthSpecialist,StopTBDepartment,WHO
BRAZIL
Miguel Aiub Hijjar Director,NationalReferenceLab(HelioFraga)
Paulo Alburquerque Physician,PoliclinicaAmaralPeixoto
Joao Batista Oliveira MOHconsultanttoFarmanguinhosFarmanguinhos
Solange CavalacanteRiodeJaneiroMunicipalTBProgram
Joseney dos SantosNationalTBProgramManager,NationalTBProgram
Betina Durovni MunicipalTBProgramManager,RiodeJaneiroMunicipalTBProgram
Paiva Edilson StateTBProgramManager,MinasGeraisStateTBProgram
Fernando Fiuza Mello DirectorandPhysician,InstitutoClementeFerreiraTBReferenceCenter,SãoPauloTBReferenceCenter
Lisia FreitasStateTBProgramManager,RiodeJaneiroStateTBProgram
Vera Galesi StateTBProgramManager,SaoPauloStateTBProgram
Germano Gerhardt-Filho DirectorandformerPNCT,ProgramManagerFundaçãoAtaulfodePaiva-R.J.

page��| TBallianCe
paThwayTopaTienTs
Gustavo Bastos, Luis MSH/practicingphysician
Joel Keravec Director,MSH/RPMPlus
Naomi Komatsu MunicipalTBProgramManager,SaoPauloMunicipalTBProgram
Afranio Kritski DirectorofAcademicTBProgram, UniversidadeFederaldoRiodeJaneiro
Ana Regina Physician,CentroMunicipaldeSaúdePíndarodeCarvalhoRodrigues(DOTS)
Jorge Rocha Practicingphysician,MSH/RPMPlus
Dr. Rosangela StateTBProgramManager, BahiaStateTBProgram
Waldir Silva MOH,NationalTBProgram
Andrea Sousa de Ataide Pharmacyservices,MOH/NationalTBProgram
Marcio Thome DirectorofLogisticsandSupply, BEMFAM(NGO)
EzioTavora dos Santos Filho GrupoPelaVidda
Marilene Vinhas Pharmacistatwarehouse,BEMFAM(NGO)
CHINA
Yanbing ChenAssistantofGuangdongCDCDirector,GuangdongCDC
Sun Chenguang DirectorofShanghaiChangningDistrictCDC,ShanghaiCDC
Daniel Chin MedicalOfficer,StopTBDepartment,WHO
Vimal Dias MSHProject-RPMPlus,ManagementSciencesforHealth
Xiao Fan Physician&DirectorofInternalMedicine,GuangzhouThoracicHospital
Lin Fen HainanCDCDirector,HainanCDC
Cornelia M. Hennig MedicalOfficer,StopTBDepartment,WHO
Dr. Li PhysicianatHainanCDC,HainanDongChuangCountyCDC
Hongdi LiDoctorinCharge,ManagerofTBPreventionSection,ShanghaiChangningCDC
Jianjun LiuDirector,NCTB,ChinaCDC
Jian Mei DirectorofTBPreventionDepartment,ShanghaiCDC
Shen MeiAssociateDirectorofTBPreventionDepartment,ShanghaiCDC
Vice General ManagerFirst-LineSupplier
Sales and Marketing DirectorSecond-LineSupplier
Vice General Manager NationalDistributor
Tao Tao DirectorofPharmacy,GuangzhouThoracicHospital
Lin Wang AssociateResearcher,Director,Dept.forHealthPromotion,Director,Dept.ofDrugandFacilityResources,NCTB,ChinaCDC
Ni Wang DepartmentofDrugandFacilityResources,NCTB,ChinaCDC
Xiaomei Wang ProgramOfficer,GFATMChinaTBProgram
Zhao Wang FormerDirector,ChinaCDC

Compendium |page��
may2007
Ying Xu DirectorofPharmacy,GuangdongPanyuCountyChronicDiseasesHospital
Fu Yu Director,TBClinicalCenter;President,BeijingThoracicTumorandTBHospital
Qiang Zhang SurgeonandDeputyDirector,GuangzhouThoracicHospital
Shuo Zhang HealthOperationsOfficer,HumanDevelopmentSector,WorldBank
Xi Zhang ManagerofPharmacy,BeijingThoracicTumorandTBHospital
Yu Wen Zhang PhysicianatHainanCDC,HainanDongChuangCountyCDC
FRANCE
PharmacistChiefPharmacist,Hospital
Specialist Pulmonologist,Hospital
INDIA
Two DirectorsRKMissionClinicandGTBChestClinic
Three PPM Providers
Rajiv Alex Sandoz GeneralManager,GlobalTBBusinessandExports
Dr. ChauduryStateTBOfficerforMaharashtra,StateTBDivision
LS Chauhan DeputyDirectorGeneral(TB),CentralTBDivision
Mandar Deo MarketingManager,GlobalTB,Sandoz
Vijay K. Dhiman PPMCoordinator,Delhi,WHO-RNTCPDepartment
Ritu GuptaAdditionalGeneralManager,RITES
Rajesh KabuVicePresident,SalesandMarketing,Macleods
Ritu Khushu ProjectLeader,CentralTBDivision-StrategicAlliance
Alok Malik Sr.GeneralManager,Marketing,Macleods
Jayanti Patel Chairman,ManagingDirector, MaheshwarDistributorsPrivateLtd.
RK Pradham Representative,DrugControllerOffice
Suvanand Sahu NationalProfessionalOfficer,TB,WHO-RNTCPDepartment
VS Salhotra ChiefMedicalOfficer,CentralTBDivision
Vinay SapteManagingDirector,ManeeshPharma-Svizera
Pradeep Saxena ChiefMedicalOfficer,CentralTBDivision
Tariq ShahMedicalOfficer,CentralTBDivision
Preetish ToraskarGeneralManager,SalesandMarketing,Lupin
RP VashistStateTBOfficerforDelhi,StateTBDivision
D. Fraser WaresMedicalOfficer,WHO-RNTCPDepartment
INDONESIA
Andy Barraclough PrincipalProgramAssociate,ManagementSciencesforHealth
Petra Heitkamp StopTBPartnership
Jan Voskens SeniorConsultant,KNCV

page��| TBallianCe
paThwayTopaTienTs
JAPAN
Hajime Inoue Director,MinistryofHealth,LaborandWelfare–InternationalAffairsDivision
PharmacistHospital
PHILIPPINES
Asuncion Anden Director,DOHCenterforHealthDevelopment,MetroManila
Michael Arabit Pharmacist,MakatiMedicalCenter
Eduardo Banzon VicePresident,HealthFinancePolicy&ServicesSectorandOIC,BenefitsDevelopmentOffice,PhilHealth
Victoria Basa-Dalay ChairmanTBResearchUnit,DeLaSalleUniversity(PrivateDOTSProgram)
Jubert Benedicto Chairman,PhilCAT
Marilou Costello HealthSystemsAdvisor,PhilTIPS
Ruben Escarda PhysicianandDepartmentChairmanofInternalMedicine,VisayaCommunityMedicalCenter(PrivateHospital)
Nereza S. Javier ProvincialCoordinatorforTBProgram,ProvincialTBProgram,Cavite
Dory C. Loquias ProvincialCoordinatorforTBProgram,ProvincialTBProgram,Cebu
Amelia Medina RegionalCoordinatorforTBProgram,NationalCapitalRegion(MetroManila),DOHRegionalOffice,MetroManila
Jose Hesron D. Morfe PhysicianandDOTSProgramManager,PhilTIPS;UniversityofStThomasHospital(PrivateDOTSProgram)
DOTS Nurse Coordinator UniversityofStThomasHospital(PrivateDOTSProgram)
Individual DOTS-PlusCommitteeofStopTB
Pharmacy ManagerPhilippinesGeneralHospital
Pharmacist; Purchasing ManagerNationalPharmacyChain(PDI)
Marketing Coordinator; General ManagerSupplier
Marilyn Noval-Gorra PolicyandFinanceAdvisor,PhilTIPS
Erlinda Pascual President,DrugstoresAssociationofthePhilippines
Earl Stanley Perez Comptroller-MerchandizingDivision,WatsonsPersonalCareStores
Fulgencia Ricero RHP,DOH,BatangasCity
Leticia Rivera ProvincialCoordinatorforTBProgram,ProvincialTBProgram,BatangasCity
Marilyn Tiu PurchasingManager,MedExpress
Thelma Tupasi PresidentofTDF,ChairmanofDOTS-PlusCommittee,TropicalDiseaseFoundation(TDF),MakatiMedicalCenter
Rosalind VianzonNationalTBProgramManager,DOH,OfficeofInfectiousDiseases
Sergio Villahermosa SupplyOfficer,ProvincialTBProgram,Cebu
Andre Daniel Villanueva PharmacyDOTSInitiative-ProgramManager,PhilTIPS
John Wong SpecialistforDrugManagementandFinance,PhilTIPS;AsianDevelopmentBankHealthSectorDevelopmentProgram
Charles Y. Yu SeniorAdvisor,PhilTIPS

Compendium |page��
may2007
SOUTH AFRICA
Shabir Banoo SeniorProgramAssociate,MSH
Alan Beattie NationalSalesManager(PublicSector),AspenPharmacare
Gavin Churchyard CEO,AurumInstitute
Elaine Cross HeadofTBSupplies,Sandoz
Virginia de Azeveda Sub-districtNTPDirector(Kylitscha),Sub-districtTBControlProgram(Kylitscha)
Deon Du Plessis MedicalDirector,Netcare
Bernard Fourie ResearchAssociate/ClinicalTrialsAdvisortotheMRC;ChiefScientificOfficer/Director,SouthAfricanOperationsofMEND,MedicalResearchCouncil(MRC)
Ria Grant Director,TBCareAssociation
John Heinrich CEO,SANTA
Mandisa Hela DirectorofPharmacyServices,PharmacyPlanningandPolicy
James Kruger DistrictNTPDirector(Boland,Overberg),DistrictTBControlProgram(BolandOverberg)
Liezel Channing PharmacistARVProgram,ProvincialTBControlProgram,WestCape
M. Makhetha TBProgramCoordinator/NPO–TB,WHO
Ethel Makoena Chairman,SANTA
Reuben Mawela DistrictSalesManager,TB Sanofi-aventis
Penny Mkalipe MedicalOfficer,ESKOM
Tumi Molongoana SeniorProgramAssociate,MSH
Sipho Mthathi GeneralSecretary,TreatmentActionCampaign(TAC)
Lindiwe Mvusi NTPDirector,NationalTBControlProgram
Ann Preller ProvincialNTPCoordinator,ProvincialTBControlProgram,NorthWest
Jean-Pierre Sallet RegionalTechnicalAdvisor,MSH
Mandisa Swartz ProvincialNTPCoordinator,AssistantDirector,TBControl,ProvincialTBControlProgram,WestCape
UK
Pharmacist ChiefPharmacist,Hospital
Pharmacist Ownerofasmallchainofretailpharmacies,Retail
SpecialistConsultantinRespiratoryDiseases,Hospital
US
Muhammad Anwar Pulmonologist,St.Joseph’sHospital
Kenneth Castro MedicalDirector,DivisionofTuberculosisElimination,U.S.CDC
MikeEhren Pharmacist,FloridaStateHealthDept.,BrowardCountyTuberculosisControlClinic
Sonal S. Munsiff MedicalOfficer,BureauofTuberculosisControl,U.S.CDC,NYCDepartmentofHealthandMentalHygiene
MaryAnn O’Brien Pharmacist,QuincyMedicalCenter
Lee Reichman ExecutiveDirector,NewJerseyMedicalSchool,NationalTuberculosisCenter
Susan Spieldenner PublicHealthAdvisor,TBControlBranch–CaliforniaDepartmentofHealthServices
Charles Wallace ProgramManager,TBControlBranch–TexasDepartmentofStateHealthServices

page��| TBallianCe
paThwayTopaTienTs
12.Acknowledgements
TheTBAlliancewouldliketoacknowledgethemanypeoplewhosetime,effortandenthusiasm,madethisunprecedentedresearchprojectpossible.
Weareverygratefultoourprojectadvisors:MonaAshiya,SarahEwart,JordanLewis,MariekeKorsten,RobertMatiru,JimRankinandDorisRouse,andthemembersofourresearchteam:NinaSchwalbeandHeatherIgnatiusfromtheTBAlliance,andAlyseForellina,AlexisGeaneotes,MichelleLee,LaurenDiCola,TarekRaafat,andClareWalkerfromIMSHealth.
ThePathway to PatientsresearchteamwouldliketoacknowledgethecontinuoussupportofTBAllianceofficersMariaFreire,MelSpigelman,KarenWright,AlHinmanandBradleyJensen;theresearch&developmentteam’sAnnGinsberg,ZhenkunMa,ChristovanNiekerk,andKhisiMdluli;andthecommunicationsandpolicyteams’CuylerMayer,DerekAmbrosino,StephanieSeidel,andAsmitaBarvefortheirreview,writingandpublicationsupport.
TheTBAlliancewouldalsoliketothankthefollowingfortheircontribution:KenCastro,LSChauhan,DanielChin,GavinChurchyard,KatherineFloyd,PetraHeitkampp,MandisaHela,JeffHoover,MichaelHowley,HajimeInoue,FabienneJouberton,JoelKeravec,HannahKettler,AfranioKritski,ElisabettaMolari,SonalMunsiff,LindiweMvusi,Pierre-YvesNorval,AntonioRuffinoNetto,IkushiOnozaki,NitinPatel,SuvanandSahu,VSSalhotra,ThelmaTupasi,RosalindG.Vianzon,JanVosken,DianaWeil,FraserWares,WangXiaomei,andCharlesYu.
Finally,thisprojectwouldnothavebeenpossiblewithoutthegenerousfinancialsupportofTheNetherlandsMinistryofForeignAffairs’DepartmentofDevelopmentCooperation(DGIS)andtheBill&MelindaGatesFoundation.
de
sig
n:
ide
as
on
Pu
rP
os
e,
ne
w Y
or
K,
nY
Ph
oto
gr
aP
hY:
Co
ve
r (
far
le
ft
), C
ov
er
(s
eC
on
d f
ro
m r
igh
t),
Jo
hn
-miC
ha
el
ma
as
; C
ov
er
(s
eC
on
d a
nd
th
ird
fr
om
le
ft
),
Ba
CK
Co
ve
r (
se
Co
nd
fr
om
rig
ht
), g
ar
Y h
am
Pto
n;
Co
ve
r (
far
rig
ht
), B
aC
K C
ov
er
(f
irs
t t
wo
fr
om
le
ft
), a
tu
l l
oK
e

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
About the Global Alliance for TB Drug Development
The Global Alliance for TB Drug Development (TB Alliance) is a not-for-profit, product
development partnership accelerating the discovery and/or development of new TB
drugs that will shorten treatment, be effective against susceptible and resistant strains,
be compatible with antiretroviral therapies for those HIV-TB patients currently on such
therapies, and improve treatment of latent infection.
Working with public and private partners worldwide, the TB Alliance is leading the
development of the most comprehensive portfolio of TB drug candidates in history,
and is committed to ensuring that approved new regimens are affordable, accessible
and adopted.
The TB Alliance operates with the support of the Bill & Melinda Gates Foundation,
Irish Aid, the Netherlands Ministry of Foreign Affairs (DGIS), the United Kingdom
Department for International Development (DFID), and the United States Agency for
International Development (USAID).
For more information on TB drug development and the TB Alliance, please visit
www.tballiance.org.

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
80 Broad Street
31St Floor
New York, NY 10004
USa
tel: +1 212 227 7540
Fax: +1 212 227 7541
www.tballiance.org