Embed Size (px)
Citation preview
Applying Human Factors to Healthcare Systems Safety
A. Zach Hettinger, MD MS
Medical Director National Center for Human Factors in Healthcare
MedStar Institute for Innovation (MI2), MedStar Health Research Institute
Assistant Professor of Emergency Medicine Georgetown University School of Medicine
April 29th, 2014
To Better is HumanTM
1
Disclosures
• Root Cause Analysis – Emergency Medicine Patient Safety Foundation – Latham Foundation – American Society for Healthcare Risk Mgt (ASHRM)
• Other Funding – Agency for Healthcare Research & Quality – Office of the National Coordinator – National Institutes of Health
2

Agenda
• Case • What is Human Factors? • Concepts in Human Factors
• Effective & Sustainable Solutions • Skill/Rule/Knowledge Based Errors • Just Culture
• Conclusion
3

CASE It starts with a
4
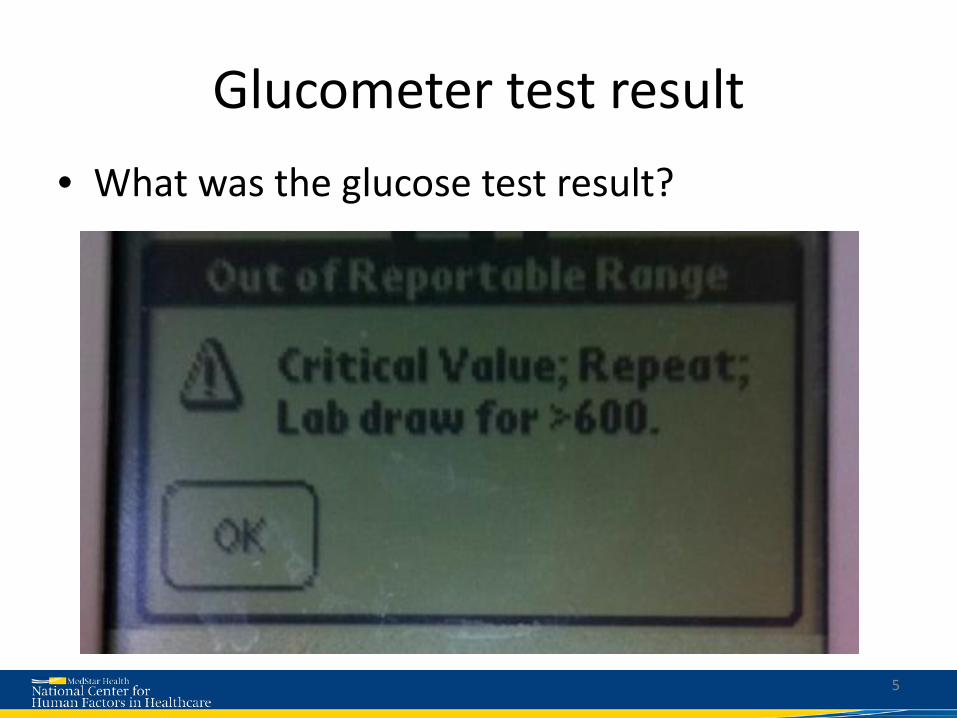
Glucometer test result • What was the glucose test result? HIGH or LOW?
5

6

How could you miss it?
7

Critical Low: 0.1% of results (119/80,000)
8

Who is the expert?
Hospital Text of ‘Out of Reportable Range’ message popup
A Critical value; Repeat; Lab Draw for > 600.
B RR Lo = result <40; RR Hi = result >600
C Out of range: repeat test to confirm
D Critical value; repeat within 15 mins; notification required; lab draw for >600
E Critical value; you must repeat immediately; STAT glucose Lab draw for RR HI
F Repeat test
9
CRITICAL VALUE; REPEAT TEST: NOTIFY MD/RN

HUMAN FACTORS What is
10

What is Human Factors Engineering?
Designing….. systems, process, and devices ….with regards to what humans do well….
11
What is Human Factors Engineering?
and what we do with variability…..
12

Human Factors Engineering
“We don’t redesign humans; We redesign the system within which humans work”
13

Human Factors Engineering (HFE)
• “Designing for human use” – Human-Machine Interface (display, control)
• Optimizes the relationship between technology and the human user
• Designs the system to match abilities • Data-driven, evidence based • Normal in aviation, nuclear, military
14

15

16

17

18
19

20
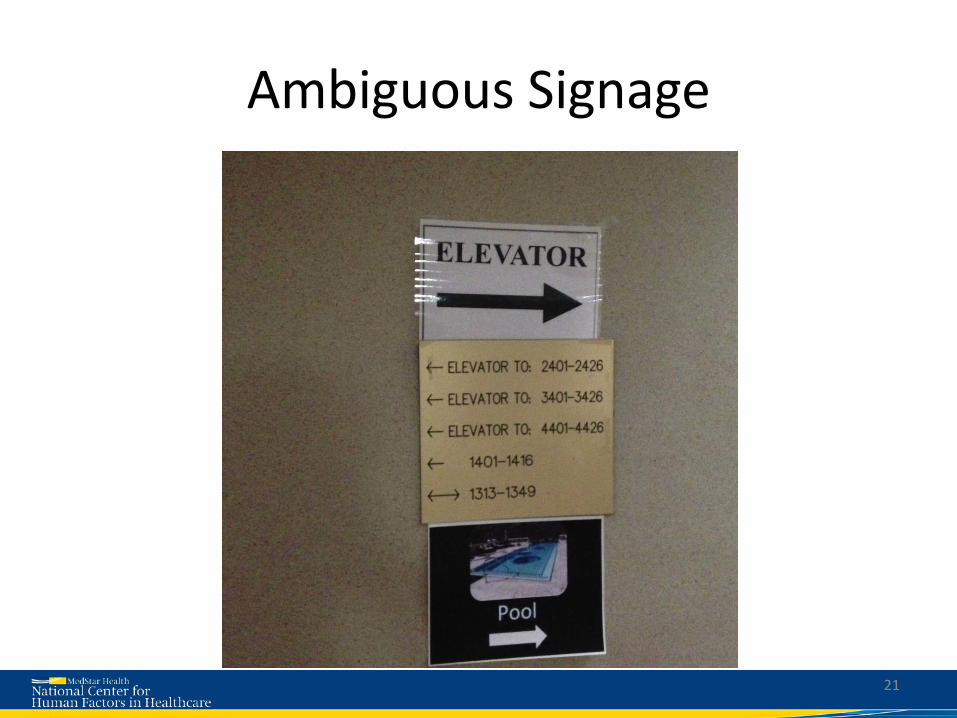
Ambiguous Signage
21
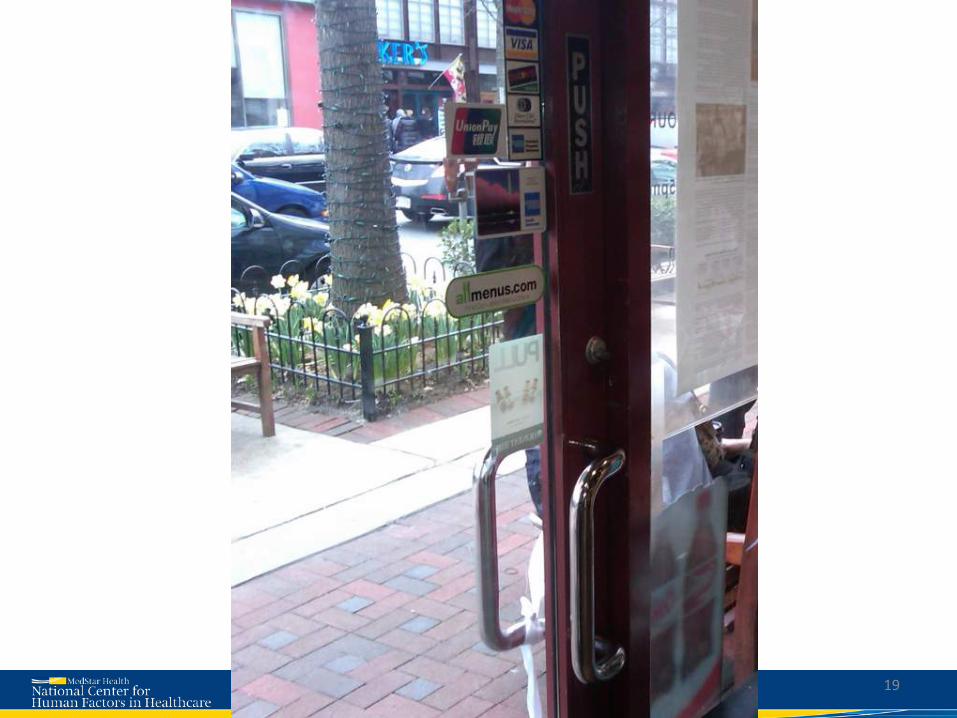
Even Door Design has Real World Consequences
22

CONCEPTS Human Factors
23

Reckless Behavior
Conscious disregard of unreasonable risk
Manage through: • Remedial action • Punitive action
At-Risk Behavior
A choice: risk not recognized or believed justified
Manage through:
• Removing incentives for At-Risk Behaviors
• Creating incentives for healthy behaviors
• Increasing situational awareness
• Re-examining environment
Normal Error
Inadvertent action: slip, lapse,
mistake
Manage through changes in: • Processes • Procedures • Recurrent training • Design • Environment
Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: www.JustCulture.org See also, Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008)
Just Culture: The Three Behaviors
24
ROOT CAUSE ANALYSIS Applying Human Factors to
25

Study Overview
26

27
Definition: Facility wide change that requires a large capital investment Solution: New bariatric accesible imaging equipment
28
Example: Medical image delayed secondary to morbid obesity and lack of access to adequate in-house imaging.
Institutional

Definition: Changing features of EHR/Health IT system to change functionality Solution: Ability to track aspiration precautions through EHR
29
Example: A patient aspirated despite being clinically identified as high risk for aspiration by staff members
Information Technology Structure

30
31
32
Definition: Changes to the physical environment within which medical staff work Solution: Patient care environments stocked with 1:1000 epinephrine
33
Example Case: A patient with anaphylaxis is given 0.5 mg of 1:10,000 epinephrine, instead of 0.3mg of 1:1,000 because the later was not available.
Physical Environment

Defibrillator Case
• VF cardiac arrest • nurse with patient • charges unit… • clears patient… • presses “on” button • Machine powers down
– 2-3 minute delay in shock
34
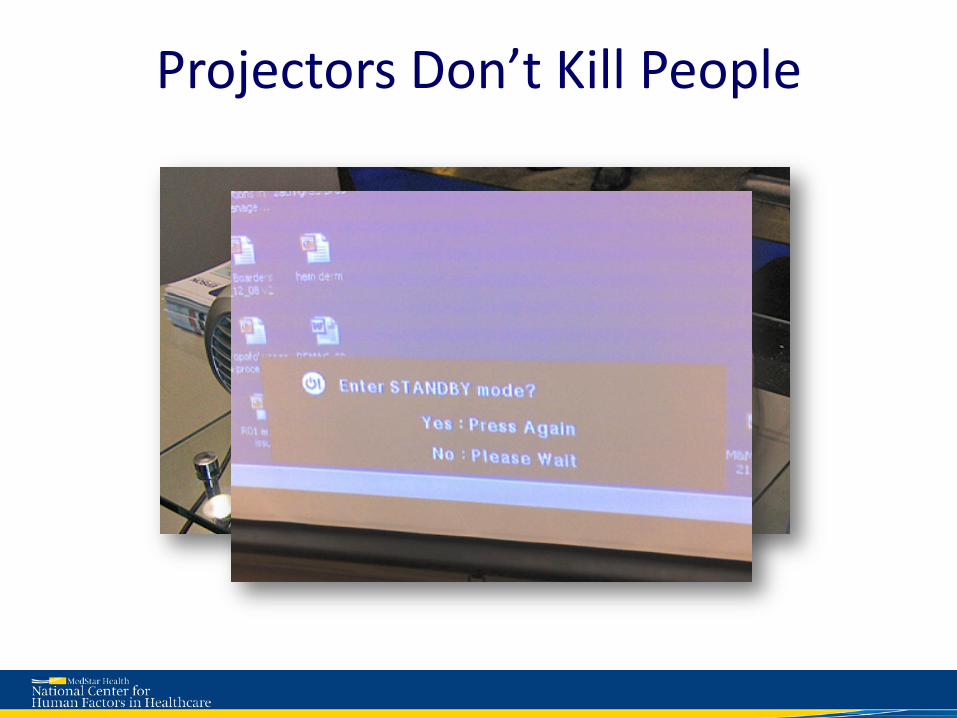
Projectors Don’t Kill People
Definition: Changing the work process and flow of the healthcare workers in an attempt to reduce hazards Solution: A standard process/protocol developed to implement aspiration precautions. Aspiration precautions should be the standard of care for all patients with difficulty swallowing. Swallowing study can be done seven days a week
36
Example: A post surgical patient aspirates and dies without a swallow evaluation, despite recognition as an aspiration risk by staff.
Process
Definition: New forms or changes to documentation templates and procedures. Solution: All lab specimens required to have a requisition/order for testing
37
Example: A critically lab value repeated per protocol, but paper requisition never filed and test not performed.
Forms & Paperwork
38

Definition: An assessment of a particular system/process Solution: Implement regular RRT case review with staff within 24 hours to provide a feedback loop to identify points in care where interventions could have prevented RRT
39
Example: A patient with sepsis (RRT evaluated the day before) was transported to radiology where she died while awaiting transport.
Review

Definition: Education is the primary goal of the solution, either of individuals or groups. Solution: Dialysis staff to provide written and a verbal report to home unit of any changes in patient status.
40
Example: Critical labs from a dialysis session and a hypotensive episode were not communicated to floor team, leading to a delayed response to a patient’s critical lab values.
Training

Knowledge-Based
Rule-Based
Skill-Based
Improvisation in unfamiliar environments No routines or rules available to help handle
Protocolized behavior Process, Procedure
Automated Routines Require little conscious attention
Figure adapted from: Embrey D. Understanding Human Behaviour and Error, Human Reliability Associates Based on Rasmussen’s SRK Model of cognitive control, adapted to explain error by Reason (1990, 2008)
41

Policies, Inservices,
Discipline, Training, Vigilance Encouraging “Mindfulness”
Slips and Lapses: Common
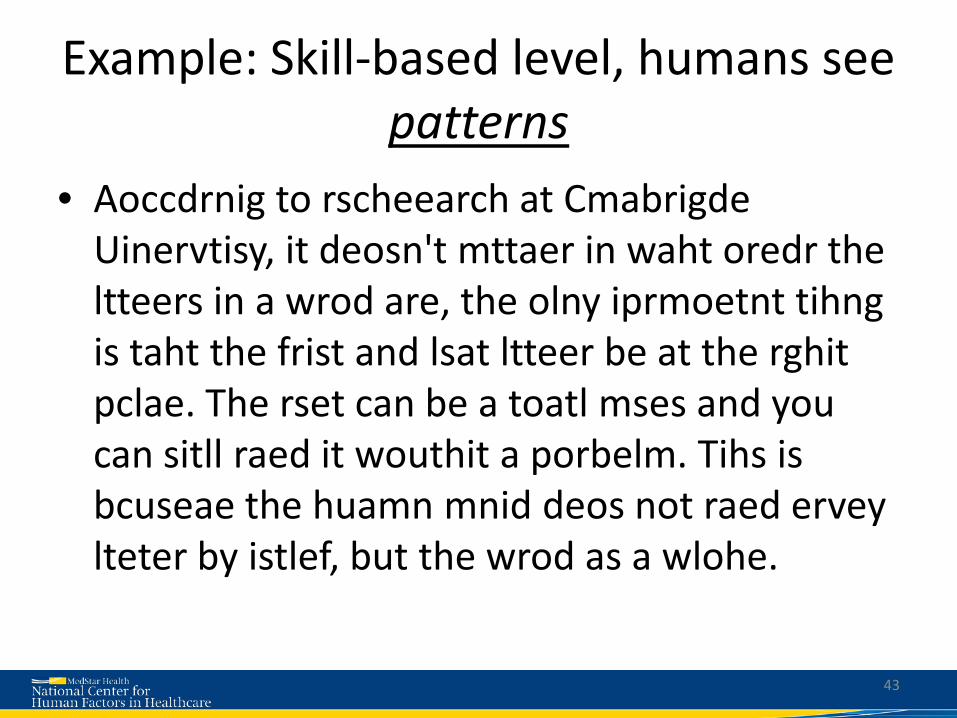
Example: Skill-based level, humans see patterns
• Aoccdrnig to rscheearch at Cmabrigde Uinervtisy, it deosn't mttaer in waht oredr the ltteers in a wrod are, the olny iprmoetnt tihng is taht the frist and lsat ltteer be at the rghit pclae. The rset can be a toatl mses and you can sitll raed it wouthit a porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe.
43
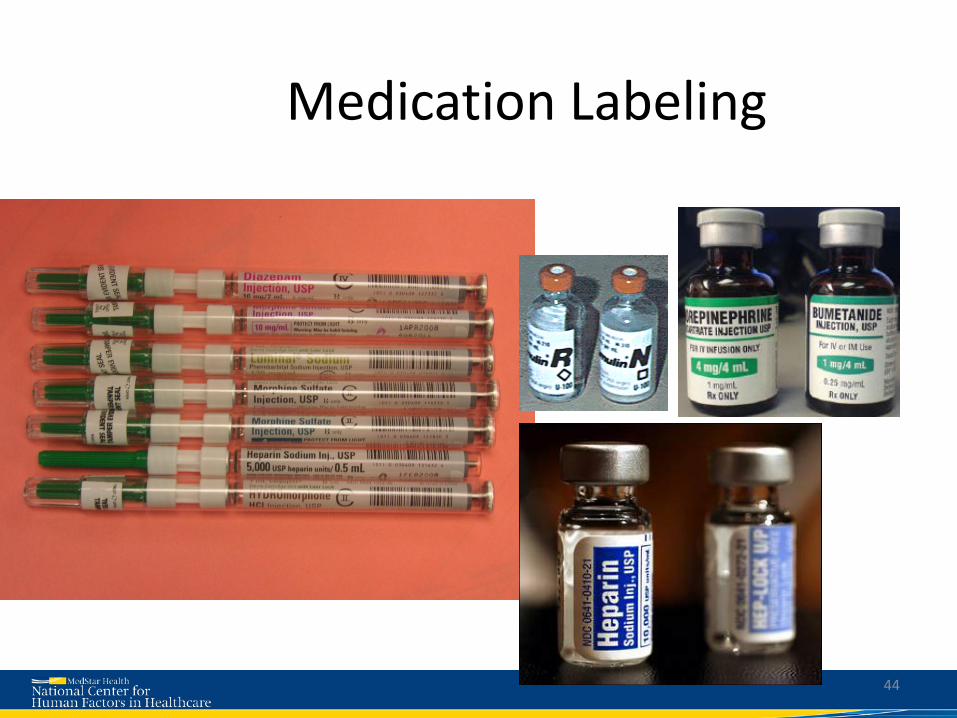
Medication Labeling
44

45
Definition: These solutions are focused on reviews of charts or processes for the purpose of monitoring or regulating a particular process. Solution: Incorporate hourly rounding into concurrent auditing.
46
Case: An elderly woman fell out of bed and broke her hip.
Compliance Checks
Definition: Changes that are limited to creating, changing or reinforcing a policy. Solution: The nurse and the transporter must jointly ID the patient prior to the patient leaving the unit.
47
Case: Due to a patient mix up, a hearing impaired patient received an unnecessary procedure.
Policy
48
Definition: The creation of development plan, feedback or referral to practice committee for individuals.
49
Counseling
Contact Third Parties
Definition: The involvement of third parties includes bringing in manufacturers representatives, motivational speakers and other consultants.

Definition: These solutions focus only on the involvement of Risk Management
50
Risk Management
Definition: These solutions focus disciplinary actions taken towards involved staff members.
Disciplinary

Reckless Behavior
Conscious disregard of unreasonable risk
Manage through: • Remedial action • Punitive action
At-Risk Behavior
A choice: risk not recognized or believed justified
Manage through:
• Removing incentives for At-Risk Behaviors
• Creating incentives for healthy behaviors
• Increasing situational awareness
• Re-examining environment
Normal Error
Inadvertent action: slip, lapse,
mistake
Manage through changes in: • Processes • Procedures • Recurrent training • Design • Environment
Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: www.JustCulture.org See also, Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008)
Just Culture: The Three Behaviors
51

CONCLUSION
53

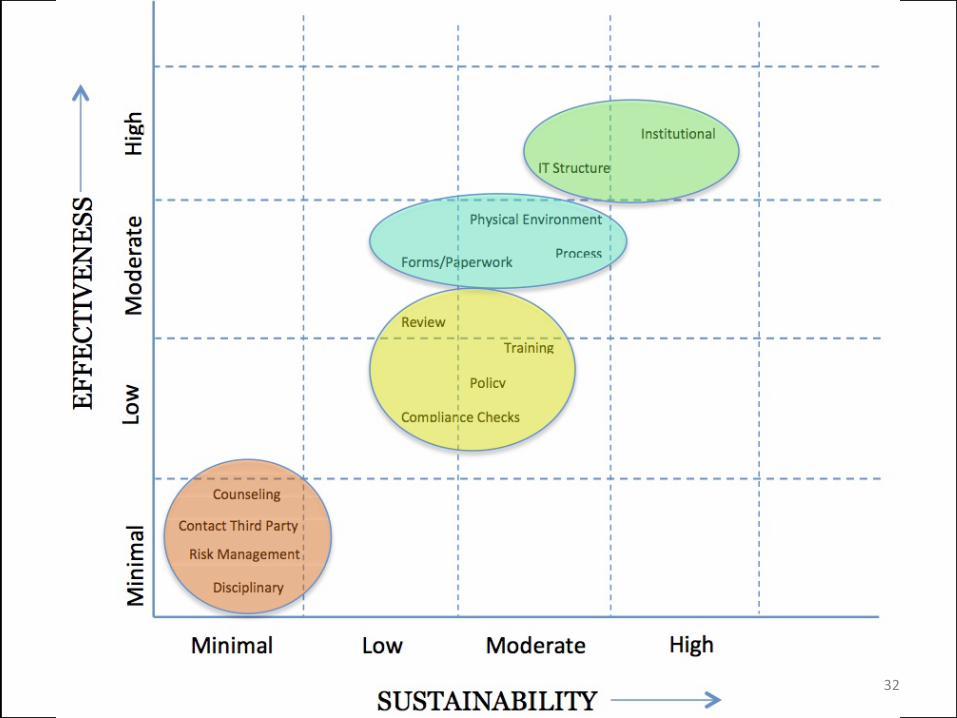
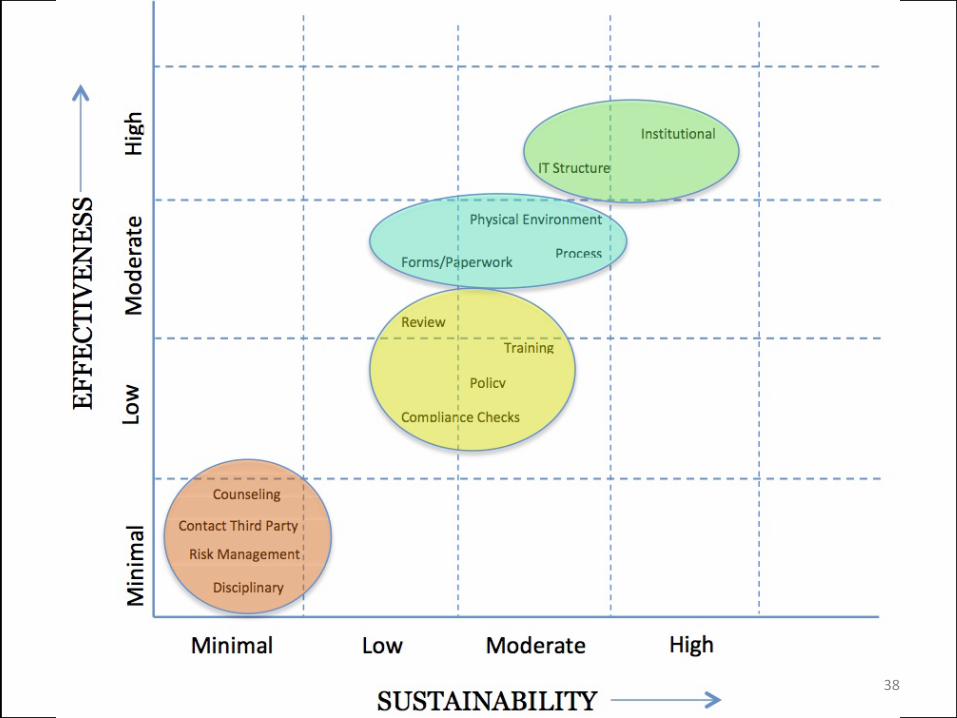
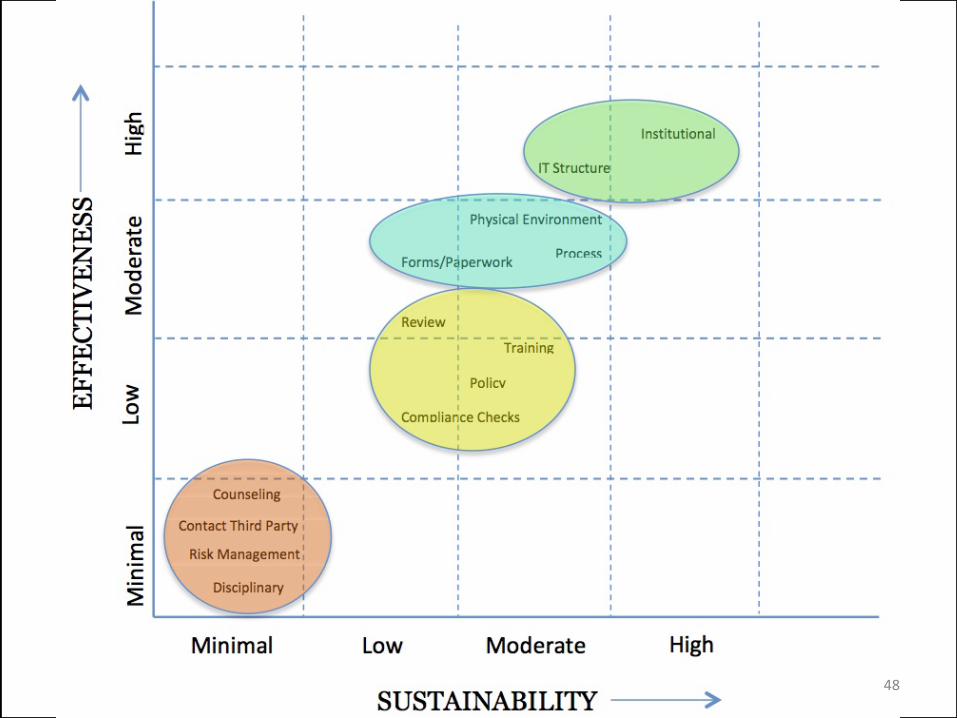
Staged Sustainability Approach
54
Effe
ctiv
enes
s
Sustainability
Take Home Points
• Staged Approach • Generalizability • Limiting individual focused solutions • Classify the contributing factors and create
solution appropriate to the error • Consider Implementation of Just Culture
55
Be Optimistic
56
• https://www.youtube.com/watch?v=xtxd27jlZ_g&feature=youtu.be

Thank you
• Terry Fairbanks, MD, MS • Amy Bisantz, PhD • Vicki Lewis, PhD • Robert Wears, MD, PhD • John Wreathall, MS • Sudeep Hegde, MS • Alex Rackoff, MD • Kate Kellogg, MD
57
Questions?
www.MedicalHumanFactors.net
58
TABLETOP EXCERCISE
59

Skill/Rule/Knowledge Based Errors • Case 1: A new physician is admitting a patient from the emergency
department, and places the patient with chest pain on a non-telemetry unit. While waiting to move to the correct floor, the patient has an arrhythmia that is not initially detected and the patient has a poor outcome.
• Case 2: While performing triage on a patient with “stomach pain” in the emergency department a nurse uses the standing abdominal pain orders to request lab and urine tests. An hour later the patient is seen by the physician who immediately orders an EKG which shows a STEMI (heart attack) and the patient is rushed to the cardiac catheterization lab.
• Case 3: A nurse receives an order for clindamycin 300mg PO, obtains the medication from the automated medication system and administers it to the patient after performing the safety checks. Thirty minutes after receiving the medication the patient has an anaphylactic reaction requiring a stay in the ICU. It was later determined that the patient was given Pen VK to which they have a known allergy, and that the medications were stocked in the system incorrectly.
60

Knowledge-Based
Rule-Based
Skill-Based
Improvisation in unfamiliar environments No routines or rules available to help handle
Protocolized behavior Process, Procedure
Automated Routines Require little conscious attention
Figure adapted from: Embrey D. Understanding Human Behaviour and Error, Human Reliability Associates Based on Rasmussen’s SRK Model of cognitive control, adapted to explain error by Reason (1990, 2008)
61
Just Culture • Case 1: In an effort to perform all of the patient care duties and
documentation, a patient care tech uses • barcodes taped to a desk instead of the patient’s wrist bands to
improve efficiency. • Case 2: A medical staff member is known by other members to be
disrespectful; when asked about some medical decisions that lead to hazardous situations and patient harm he states “I don’t care” and “I’ve always done it this way.”
• Case 3: After opening the chart to write an order for antibiotics for a patient with low blood pressure and sepsis (blood infection), a physician is approached by a nurse and asked for pain medications for a different patient. The physician writes the order for Dilaudid 1mg IV for the patient with sepsis that results in a further lowering of their blood pressure and requires additional IV fluids and monitoring.
62
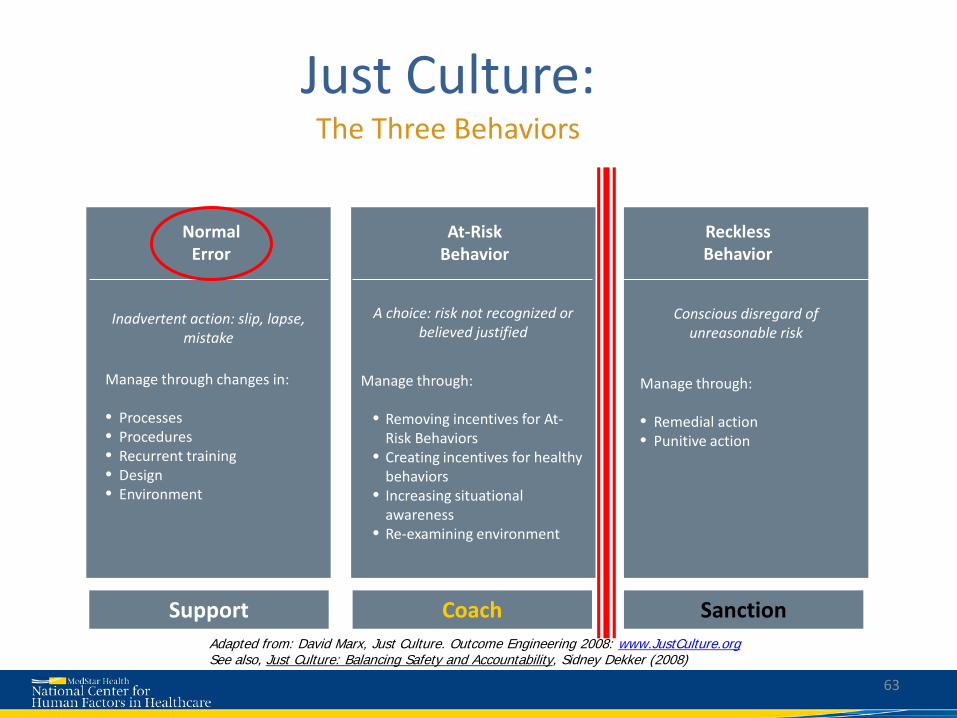
Reckless Behavior
Conscious disregard of unreasonable risk
Manage through: • Remedial action • Punitive action
At-Risk Behavior
A choice: risk not recognized or believed justified
Manage through:
• Removing incentives for At-Risk Behaviors
• Creating incentives for healthy behaviors
• Increasing situational awareness
• Re-examining environment
Normal Error
Inadvertent action: slip, lapse,
mistake
Manage through changes in: • Processes • Procedures • Recurrent training • Design • Environment
Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: www.JustCulture.org See also, Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008)
Just Culture: The Three Behaviors
63

Sustainable System Solutions
• Case 1: After an adverse event all staff members are given an in-service on the Patient Controlled Analgesia (PCA) pump (medical device) that has been involved in multiple medication overdoses.
• Case 2: After multiple observation sessions where medical staff is observed not washing their hands, the team decides to add alcohol-based hand sanitizers outside each patient room.
• Case 3: A physician is fired after performing a procedure on the wrong side of the patient.
64