Embed Size (px)
Citation preview

Title page
HbA1c values calculated from blood glucose levels using truncated Fourier series and implementation
in standard SQL database language WWIILLHHEELLMM TTEEMMSSCCHH,,11 AANNTTOONN LLUUGGEERR,,22 MMIICCHHAAEELLAA RRIIEEDDLL33
1Section of Medical Information and Retrieval Systems Core Unit for Medical Statistics and Informatics
Medical University of Vienna, Austria 2Division of Endocrinology and Metabolism
General Hospital of Vienna, Austria 3Department of Medicine III
General Hospital of Vienna, Austria
Corresponding author:
Wilhelm Temsch
Core Unit for Medical Statistics and Informatics Section of Medical Information and Retrieval Systems Medical University of Vienna Spitalgasse 23, BT88, room 88.04.807 1090 Vienna, Austria
Postal address:
Besondere Einrichtung für Medizinische Statistik und Informatik An der Medizinischen Universität Wien Bauteil 88, Ebene 4 Zimmer 807 Spitalgasse 23 1090 Vienna, Austria
+43 1 40400 6691 (Phone) +43 1 40400 6697 (Fax) +43 676 5429863 (Mobile)
Email: [email protected]

Summary Objectives: This article presents a mathematical model to calculate HbA1c values based on self-measured blood glucose and past HbA1c levels, thereby enabling patients to monitor dia-betes therapy between scheduled checkups. This method could help physicians to make treat-ment decisions if implemented in a system where glucose data are transferred to a remote server. Systems of this type would yield results without involving any additional cost or ef-fort. The proposed model is both faster and more reliable than chemical analysis, and there is no need for extra measurements because available values are used exclusively. The method, however, cannot replace HbA1c measurements; past HbA1c values are needed to gauge the method. But it provides a useful complement to actual measurement for the trend between checkups.
Methods: The mathematical model of HbA1c formation was developed based on biochemical principles. Unlike an existing HbA1c formula [1], the new model respects the decreasing con-tribution of older glucose levels to current HbA1c values. Convolution is the mathematical operation by which glucose profiles are transformed to HbA1c profiles. This requires Fourier series. A php program with embedded SQL statements was written to perform Fourier trans-form, convolution and inverse Fourier transform. Regression analysis was used to gauge re-sults with previous HbA1c values. Trigonometric, time-cast and sum functions were used ex-clusively in a total of merely 12 SQL statements, such that the method can be readily imple-mented in any SQL database.
Results: The predicted HbA1c values thus obtained were in accordance with measured val-ues. They also matched the results of the HbA1c formula in the elevated range. By contrast, the formula was too “optimistic” in the range of better glycemic control. Individual analysis of two subjects improved the accuracy of values and reflected the bias introduced by different glucometers and individual measurement habits.
Conclusions: Individual analysis has some advantages but requires a substantial body of data, which can be best obtained by implementing the mathematical model such that glucose values are transferred to a remote server [2].
Key words: diabetes mellitus · glycosylated hemoglobin A · Fourier analysis · SQL database · regression analysis

3
Introduction Diabetes therapy is mainly about restoring natural glycemic control [3-8] to avoid long-term consequences such as impaired vision, kidney failure or angiopathy. Ways to prevent these vascular diseases include dietary measures, oral drugs or insulin substitution. The objective is always to keep blood glucose levels essentially within the normal range. HbA1c values give an indication of mean blood glucose levels over the previous 2 or 3 months and therefore are a suitable parameter to monitor the success of self-performed glycemic control.
HbA1c has been an established parameter in diabetes therapy for over 25 years [9-12]. The designation indicates hemoglobin molecules that have formed a permanent chemical bond with glucose molecules. HbA1c values reflect the percentage of hemoglobin having under-gone this type of reaction, which is so significant that HbA1c constitutes the backbone of dia-betes checkups alongside risk factors such as body weight, blood pressure or blood glucose values.
Several theories have been presented to explain how hyperglycemia induces the late compli-cations typically associated with diabetes. One of them is the hypothesis of advanced glyca-tion and product formation [13]. According to this theory, glucose molecules react with an amino group included in all protein molecules to form what is known as aldimine or Schiff base. Enzymes are not required for this fast reaction. The resultant aldamine is very unstable and never reaches significant concentrations. Chemical equilibrium will quickly develop. The bulk of newly formed aldimine will quickly decay back into glucose and protein and is very slowly but irreversibly rearranged to form stable fructoseamine. Defense mechanisms identify the protein molecule as being damaged and will attack it by oxidation. This will very slowly lead up to a configuration in which other bindings sites for protein molecule develop, thereby giving rise to unwanted cross-linking of different protein molecules.
Collagen affected in this way could result in the formation of new chemical bonds between collagen molecules. Thus the collagen would lose its elasticity and keep blood vessels, being a major constituent of their inner surface, in a contracted state. Unwanted bonds of this type could form while vessels are contracted and prevent their re-expansion. Cross-links could also form between collagen and complement, which is part of the immune system and destroys bacteria by binding to them with the help of antibodies under physiological conditions. Erro-neous binding and activation of complement at the surface of blood vessels will result in in-flammation and contraction. Vessels are thereby reduced in diameter and will no longer be able to supply oxygen to tissues, such that the tissue is deprived and eventually dies. Eyesight deteriorates if this happens to the retina, and affected limbs may sooner or later require ampu-tation [13].
The first stable intermediate of this chain is fructoseamine. Hemoglobin is also subject to aldimine condensation. HbA1c is the fructoseamine emerging from this aldimine [14] and therefore does not just supply information on blood glucose levels of the previos 2 or 3 months but indeed reflects the destructive action of elevated blood glucose levels.

4
Objectives Self-management is becoming increasingly important in diabetes therapy. This is a positive development because greater flexibility will improve quality of life and hence patient accep-tance. In addition, personal responsibility contributes to the success of therapy. [5, 8, 15-18].
Conventional insulin therapy (CT) involves a defined regimen of insulin and food intake to be strictly observed by the patient. A matching regimen is found heuristically in hospital but is usually no longer adequate on disease progression. In that case, the existing regimen needs to be replaced by a new one offering greater flexibility while also requiring a higher degree of personal responsibility.
Patients on functional insulin therapy (FIT) are allowed to eat as much as they like anytime but have to adjust their insulin doses based on individually derived algorithms. They need to measure their blood glucose values several times a day and adjust them with short-acting in-sulin if required. Pump therapy offers a similar degree of flexibility to FIT. Patients have a certain leeway to adjust therapy on noticing disease progression. Both treatment modalities (FIT and pump) can only work with responsible patients. Being responsible also means being interested in the success of therapy and in the development of HbA1c values between sched-uled checkups. This interest is also reflected by commercially available HbA1c kits for home use.
HbA1c values estimated on the basis of current blood glucose and past HbA1c levels are not actually identical to the HbA1c values present in erythrocytes. However, a good approxima-tion supplied by an appropriate mathematical model would have some advantages over true measurement. There would be no need for taking additional blood samples as blood glucose values are measured to determine the required insulin doses anyhow. Values could thus be calculated at the push of a button. This would be more convenient than performing measure-ments based on a kit. It would also eliminate the cost and hassle of acquiring the kit. In addi-tion, it may not be possible to ensure the required level of quality control when chemical tests are performed at home.
The main objective of this article is to provide a mathematical model for HbA1c estimation (or, more general, risk estimation, like [19, 20]) based on data available to the patient. The model we have developed is an inexpensive, convenient and reliable tool providing valuable information for self-management that would enable diabetics to consult a physician earlier than the scheduled checkup if appropriate.
As a nice spin-off, the HbA1c values obtained through this model will reflect average blood glucose levels of the previous 2 or 3 months as a logical consequence of the erythrocyte life span (around 4 months). The model also demonstrates that recent blood glucose values are overemphasized compared to older ones.
It is also demonstrated that the data collected by diabetics contains a large amount of valuable information. For example, insulin demand varies with daytime, which is partially due to cir-cadian rhythms of hormone secretion [21, 22]. Mathematical tools can help to extract such hidden information, thereby enabling patients to further optimize their therapy and lifestyle. Fourier transform has figured prominently in previous articles [23, 24].

5
Financial implications also play an important role. Complications of diabetes will involve substantial costs for hemodialysis and patient care. Some of these costs could be avoided by tools offering more effective self-management.
Methods In this section we present a mathematical model of HbA1c formation based on biochemistry, convolution and a triangle-shaped convolution kernel. First intermediate result is an appropri-ately weighted mean of the glucose values of the recent 4 months. Fourier transform is adapted to the specific requirements of the problem and implemented in SQL language. Re-gression analysis was performed with SAS 9.1 software.
Model of HbA1c formation: HbA1c as such indicates a value that has been measured rather than mathematically derived (or predicted) from blood glucose values. One formula to calcu-late HbA1c from blood glucose values does already exist [1]. A mean blood glucose level of 130 mg per 100 ml (= 7.2 mmol/l) would be equivalent to 6.5% HbA1c. Any additional 10 mg per 100 ml (= 0.56 mmol/l) translate to an additional 0.3% HbA1c. Lower glucose val-ues will reduce the HbA1c. These considerations result in the following formula:
HbA1c=2.6+0.03*G[mg/100ml] and 2,6+0.54*G[mmol/l]
HbA1c levels change slowly. Even radical changes in glycemic control would take several weeks to show. Therefore it suffices perfectly to obtain blood glucose values daily or even weekly for HbA1c estimation. The above formula is fairly useable especially in well-controlled diabetes involving constant HbA1c levels over several years. Some glucometers and software tools for diabetes management rely on this formula to predict HbA1c values.
Despite being a valuable tool, the formula is liable to create a wrong impression. While dia-betics who actively maintain glycemic control will manage to keep their HbA1c constant, they are more likely to keep track of these values in the first place, no matter if they are calcu-lated or measured. Newly diagnosed patients are, however, concerned with many other things and may therefore not be able to focus on models as abstract as predicting HbA1c values in this early phase. Some of them will only become interested in such models after their HbA1c values have stabilized.
Unlike the HbA1c formula, the model presented below respects the gradually decreasing con-tribution of older glucose values. For this purpose, a triangle-shaped function is used that reaches zero 120 days in the past, corresponding to the life span of erythrocytes. The HbA1c formula, by contrast, utilizes a moving mean value derived from the previous 2 to 3 months.
Complexity of the model is not a valid argument. Only about 12 SQL queries were needed to perform the required Fourier analysis for this project. Once the program has been written and implemented in a database, it can be executed as conveniently and inexpensively as a simple query. The model also respects the underlying biochemistry and thus would outperform the formula in the presence of variable HbA1c levels.
The processes on which the mathematical model is based are described in detail elsewhere [14]. HbA1c formation starts out by condensation of hemoglobin (H) and glucose (G) to aldimine (denoted G = H). A double bond between those protein and glucose molecules forms quickly. Equilibrium between formation and decay will soon develop since G = H will also decay quickly. The law of mass action applies:

6
const==
]H][G[]HG[
For details on the law of mass action, the reader is referred to appropriate textbooks of chem-istry [25]. The letters in brackets indicate glucose, hemoglobin and aldimine concentrations. The initial fraction will ideally yield a constant value under identical conditions (e.g. pH or temperature). This is the equation converted to give [G = H]:
[G = H] = const. × [H] × [G]
Strictly speaking, [G = H] forms at the expense of [H]. In other words, total hemoglobin is re-duced by the amount of aldimine forming. The percentage of hemoglobin bound in aldimine condensed state is roughly 0.5% under normal (non-diabetic) conditions. Therefore the fol-lowing rule applies if [H0] denotes the whole of hemoglobin:
[H] = 0.995 [H0]
In a seriously hyperglycaemic situation with 540 mg/100 ml (30 mmol/l) glucose, the aldi-mine level would rise to 3% of total hemoglobin:
[H] = 0.97 [H0]
[H] is still fairly close to [H0] even in this situation. Glucose values that are significantly higher cannot contribute to HbA1c for long because immediate glucose-lowering treatment will be required once ketoacidosis develops. Thus [H] will not fall below 97% of total hemo-globin under physiological conditions.
Large amounts of already glycosylated hemoglobin will imply a decrease in [H]. Old erythro-cytes can have 10% HbA1c or even more, but they only account for a small fraction of all erythrocytes present. Their effect is therefore negligible, and we can assume that [H] still ap-plies except for a constant not exceeding a few percent. A good approximation is obtained by stating that aldimine levels are proportional to glucose concentrations:
[G = H] ~ [G]
The second step in HbA1c formation is that the newly formed aldimine is rearranged to form stable fructoseamine, which is identical to the HbA1c molecule. The kinetics involved here differ greatly from the kinetics of aldimine condensation. Conversion is so slow that equilib-rium will never develop since erythrocytes will die before that point is reached. This process is almost irreversible.
Speed of chemical reaction equals change of concentration per time unit expressed by time derivative:
.]HG[]HbA1c[ constt
×==∂
∂
Thus the reaction speed of HbA1c formation is proportional to the concentration of its imme-diate precursor aldimine. Since we found that [G = H] was proportional to glucose level [G] by defining [H] as constant, it follows that:
]G[~]HbA1c[t∂
∂

7
Thus the speed of HbA1c formation is proportional to glucose concentration by a constant yet to be determined. A single erythrocyte born with no HbA1c is exposed to blood glucose, such that HbA1c will increase:
∫∫ ×=T
0
T
0
]G(t)[~]G(t)[.])HbA1c([ dtdtconstT
where [HbA1c(T)] is the HbA1c content of an erythrocyte with age T. [G(t)] indicates blood glucose values at time t, taking all values between 0 and T. Erythrocytes have an average life span of 120 days, such that erythrocytes with T > 120 days become increasingly rare. If the survival function of erythrocytes is defined as g, then the number of cells surviving after time span T will be 1,000,000*g(T) if the initial number was 1 million cells. There are two possi-ble ways of reading this—either as N0g(T) indicating the number of newly formed erythro-cytes (N0) left after time span T, or as the number of erythrocytes with age T in a blood sam-ple being proportional to g(T). The latter view is required for the model at hand. Let T1 be the time of blood sampling and T a point of time preceding T1. Erythrocytes built at T had a time span T1−T to accumulate the HbA1c level observed in the sample. Since the age of this frac-tion of erythrocytes is T1−T, their number is proportional to g(T1−T). This is the contribution to total HbA1c:
∫−1
)()(~ 1
T
T
dttGTTg
Total HbA1c is the integral starting from an appropriately selected time T0:
( ) ( ) dTdttGTTgT
T
T
T∫ ∫−1
0
1
1~
Conversion rules for double integrals are applied, assuming that ∫=T
dssgTH0
)(:)( (then
H(0)=0):
dtTTHtGdTdtTTgtGdtdTtGTTgT
T
tTT
T
T
t
TTtTT
T
T
T
T∫∫ ∫∫∫ ∫ =
≤≤≤
−=−==−⇒1
0
0
1
0 010
1
0
1
|)()()()()()( 111 Κ
)()(|)( 0111 0TTHtTHTTH t
TT −−−=− =
H(T) is the integral of erythrocyte life spans up to T, indicating the fraction of erythrocytes not older than T in blood samples containing erythrocytes of all ages (in portions determined by the age curve g). H becomes constant if T significantly exceeds 120 days, meaning that no erythrocytes of that age are detectable in the sample. In mathematical terms, this is expressed as H(T) equaling H(∞). The point of T0 should be selected far enough in the past for H(T1−T0) to equal H(∞). If K(T1−t) equals H(T1−t)−H(∞), then K equals 0 for t (the interval from the se-lected time in the past to the present) because H(T1−t) equals H(∞) too. K(T) indicates the fraction of erythrocytes older than T. This is the resultant double integral:
∫ −1
0
)()( 1
T
T
dttTKtG

8
The next step is to extend the integral from − to + infinity:
∫∫∫ ∫∞+∞
∞− ∞−
++=1
1
0
0
T
T
T
T
ΚΚ
The first one of the three integrals occurs in a range where K(T) is consistently zero. The third integral reflects the contribution of erythrocytes (and glucose values) not yet formed. An ef-fect of such future values must be ruled out for the model to be meaningful. Therefore the first and third integrals must be zero:
( )∫ ∫∞
∞−
∗=−=−1
0
111 :)()()()(T
T
TKGdttTKtGdttTKtG
This expression is the convolution of G with K. Note that K is not the erythrocyte age curve. From the viewpoint of HbA1c formation, K overemphasizes recent blood glucose levels, such that today’s glucose level would affect virtually all erythrocytes present. A glucose value of 1 month previously has left its mark on roughly one-quarter fewer erythrocytes—i.e. those not yet built. We think of each erythrocyte as featuring a calendar, each sheet giving a day’s mean blood glucose level. Total HbA1c is the integral over all sheets of all erythrocytes. If an eryth-rocyte dies, all of its sheets are lost as well. Erythrocytes in a uniformly distributed mix are 2 months old on average. This explains a phenomenon of which experienced diabetics are well aware, namely that HbA1c values are essentially in accordance with the blood glucose values of the previous 2 months even though the average life span of erythrocytes is 4 months.
Fourier transform and convolution theorem: Calculation of predicted HbA1c values is done in two steps: First, an appropriately weighted mean of glucose, denoted GΔ, is calcu-lated. This is the mean of the recent four months with decreasing importance (weight) of older values in a triangle shaped weighing function. This step requires convolution. In the second step regression analysis of GΔ plotted against HbA1c values from the laboratory will give the predicted HbA1c values.
GΔ values are the convolution of glucose profiles with a convolution kernel K. The convolu-tion theorem is a very convenient tool to obtain G * K:
GΔ = )ˆˆ(1 KGFKG •=∗ − Thus the Fourier coefficients of G and K are simply multiplied for each frequency and subse-quently for each inversion of the Fourier transform (reconstruction). Proof of the convolution theorem can be found in any textbook of analysis [26]. The reader is also referred to section 3.1, No. 30, of a relevant thesis [27]. From the convolution theorem it follows that G*K = K*G. Fourier transform of a glucose profile is a typical irregular sampling problem; the intervals of blood glucose sampling are not always strictly periodic. Relevant tools and solutions to ad-dress this problem are described in detail elsewhere [28, 29]. Since Discrete Fourier Trans-form (DFT), the most popular tool for Fourier transform in information technology, requires constant sampling intervals, the author decided for an approach based on Fourier series. As opposed to DFT, which simply maps a vector with N values to another N-vector, Fourier se-ries is a mapping form a continuous function defined on a compact (i.e. finite length) interval to an infinite series of Fourier coefficients. The time interval from diabetes onset to now is a compact interval and sampling points are connected by appropriate interpolation. Fourier se-ries actually decomposes the profile into slowly to fast changing profiles. HbA1c is a slowly

9
changing parameter, so fast changes are suppressed in HbA1c formation. A resolution of weekly intervals is sufficiently fine if we are only interested in HbA1c. This corresponds to a maximum frequency in the range of 0.5 week–1 according to Shannon’s theorem [27], chapter 5.3. Corresponding Fourier coefficients can be neglected for this purpose and the series can be truncated. Linear interpolation of sampling points will generate frequencies above an hour−1 due to the corners, but these can be neglected, too in case of HbA1c formation. But if, for example, cir-cadian phenomena are explored by Fourier series, the corners play a role and the author should consider spline or polynomial interpolation rather than linear. As opposed to DFT the analytic integration is needed. The kth coefficient is calculated
∫ −=now
onset
iktk dtetGC )( . For the linear interpolated glucose profile with N sampling points Gn (at
time Tn) ( )∫ ∑ ∫−
=
−−+
+=1
1
1
)(N
n
T
T
iktnn
iktn
n
dtetBAdtetG (An,Bn are the parameters for G between Tn and
Tn+1). The antiderivative of te −ikt is ⇒⎟⎠⎞
⎜⎝⎛ += −−∫ e iktikt
kit
kdtte 2
1
( ) =+== ∫ ∑ ∫−
=
−−+1
1
1
)(N
n
T
T
iktnn
iktk
n
n
dtetBAdtetGC1
2
1 +
=
−∑ ⎟⎟⎠
⎞⎜⎜⎝
⎛⎟⎠⎞
⎜⎝⎛ ++
n
n
T
Tt
iktnn ek
itk
BkiA
Fourier transform is intended for complex numbers. Blood glucose profile and erythrocyte age curve are real-valued functions. This can reduce the amount of calculation required for the Fourier transform by 50%. Real-valued functions will transform to conjugate complexes [27], chapter 2.2, No. 20. Functions with N samples will map to Fourier transforms with N entries, indexed −½N…+½N if N is an even number or −½(N-1)…0…+½(N-1) if N is an odd number. For a real-valued function, the Fourier transform at −k can be derived from the value at +k as follows:
)(ˆ)(ˆ kfkf =−
Only real values should be returned because HbA1c is also real valued. This is the Fourier co-efficient for the kth frequency:
kk ibakH +=)(ˆ ( ))(ˆ)(ˆ)(ˆ kGkKkH =
The Fourier coefficients are complex numbers. Note that iktekH −− )(ˆ is exactly the conjugate complex of iktekH )(ˆ . The following equation is for inverse transform and for indices k and –k:
))(ˆRe(2)sincos(2)(ˆ)(ˆ iktkk
iktikt ekHktbktaekHekH =−=−+ −
The next step is to completely reconstruct and evaluate the processed profile H(t) at time t:
{ }
∑
∑∑
+=
=−++===
−−=
))(ˆRe(12
)0(ˆ
))(ˆ)(ˆ()0(ˆ21)(ˆ
21)( 2/
1
2/
2/
ikt
N
kiktiktN
Nkikt
ekHH
ekHekHHekHtH
ππ
ππ
Fourier series are based on periodic functions. The time over which the blood glucose profile has been monitored is treated as one period of a periodic function. Some effects can only be understood if we think of the blood glucose profile as a periodic function and perform convo-

10
lution on it. The average life span of erythrocytes is 120 days. Thus current blood glucose va-lues contribute to calculated HbA1c values from the first 4 months of the observation interval even those 4 months were several years ago. A similar problem exists in principle for current values, as the documented interval ends at the present moment. If it is considered a periodic function, then the value of the next time unit (whether the next day, hour or even second) is identical to the value measured at baseline several years ago.
Even if we knew those glucose values of the next time unit, they obviously could not contrib-ute to any physiological parameters yet. Since the erythrocyte age curve does not extend into the future, it is irrelevant for a calculated HbA1c value reflecting the current situation how blood glucose levels will develop in the future. However, at least 120 days need to be antici-pated in the early phase of the observation interval. Any HbA1c values calculated in that phase must be discarded as nonsensical. Finally regression analysis of the GΔ−values obtained by this procedure and recent HbA1c val-ues will lead to predicted HbA1c values. This method compensates constant bias, like measur-ing habits or glucometer bias. A separate regression analysis is recommended in case of a glu-cometer change. Programmers, that want to use DFT of their favourite software package, have to build daily means of the glucose profile. Alternatively an approach based on (daily) fasting glucose values can be made, but changes in medication with long acting insulin could modify the relation between fasting and mean glucose and should be treated like a glucometer change. Daily values provide the equidistant step width needed for DFT. For HbA1c formation even weekly means are sufficient.
Results Glucose data of 11 diabetic subjects were available for analysis. All timestamps of a specific individual were shifted by a defined period to avoid secondary identification attributes. It has been noted that this model requires glucose values over at least 120 days (4 months) for each newly calculated HbA1c value. Other HbA1c values are ignored. Each HbA1c record ana-lyzed was based on a mean of 582 glucose records.
Table 1: Patient IDs, observation intervals and glucose/HbA1c records
ID Observation interval Number of records
(MM/DD/YYYY) Glucose HbA1c
1 03/12/2002 04/30/2004 2520 5
2 06/25/2003 08/29/2004 2493 4
3 01/19/2004 08/01/2004 1008 1
4 11/24/2003 09/08/2004 2514 2
5 04/19/2004 08/08/2004 446 1
6 12/22/2003 09/19/2004 1316 2
7 04/05/2004 08/08/2004 966 1
8 05/09/2003 05/13/2004 2276 3

11
9 01/12/2004 07/11/2004 1062 1
10 04/30/2000 05/05/2004 4414 8
11 12/26/2001 04/26/2004 5529 11
Table 2: An appropriate mean glucose value (GΔ) was calculated for each of the 39 HbA1c re-cords by convolution with the triangle-shaped weight function.
ID Date HbA1c G∆ ID Date HbA1c G∆
1 09/25/2002 6.7 123
9 07/11/2004 8.3 136
1 02/03/2003 6.3 120
10 10/11/2000 6.9 109
1 06/02/2003 6.6 129
10 06/13/2001 7.1 116
1 10/06/2003 7.1 132
10 12/05/2001 7.4 127
1 02/16/2004 6.6 123
10 11/27/2002 7.4 121
2 12/17/2003 7.1 129
10 05/07/2003 7.5 120
2 03/09/2004 7.7 127
10 09/17/2003 6.9 119
2 07/21/2004 7.4 132 10 01/14/2004 7.4 118
2 08/29/2004 7.2 134
10 04/21/2004 7.4 114
3 08/05/2004 7.1 124
11 08/08/2002 7.9 157
4 04/15/2004 7.1 114
11 09/05/2002 7.9 167
4 09/08/2004 6.7 104
11 10/22/2002 7.7 156
5 08/19/2004 6.3 127
11 11/28/2002 7.2 150
6 06/17/2004 7.5 143
11 01/29/2003 6.8 134
6 09/19/2004 7.7 142
11 03/19/2003 6.4 126
7 08/08/2004 8.4 195
11 05/14/2003 7.1 127
8 10/06/2003 6.2 102
11 06/23/2003 6.4 117
8 01/19/2004 6.5 104
11 09/03/2003 6.4 121
8 04/19/2004 6.2 111
11 01/14/2004 7.1 129
11 03/05/2004 6.6 138
The overall correlation coefficient between calculated and measured HbA1c values was 0.6645 (39 pairs; p < 0.0001). One patient had to be excluded because of a significant mis-match between HbA1c (9.4) and GΔ (134).
The regression line of this analysis can be read as a linear relationship between GΔ and HbA1c, its parameters being 4.4 (intercept) and 0.0209 (slope). The established HbA1c for-

12
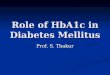
mula [1] also has a linear context, the corresponding values being 2.6 and 0.03. Comparison between both models yielded a difference in the range of better glycemic control. While GΔ = 130mg/100ml (7.2 mmol/l) is equivalent to 7.11% HbA1c in our own model, the for-mula yields 6.5% HbA1c [1]. The two lines meet at 8.53% HbA1c and 198 mg/100 ml (10.99 mmol/l), meaning that both approaches will produce the same HbA1c values in this range.
For a constant profile, an effect of convolution with K is not expected. A (weighted) mean of equal values will always give the same number regardless of how they are weighted. This was verified by substituting a value of 100 for all 5529 glucose values of subject 11 based on all timestamps available.
Table 3: Test with timestamp data from subject 11 and a constant blood glucose value
08/08/2002 100
09/05/2002 100
10/22/2002 99.999999999999
11/28/2002 100
01/29/2003 100
03/19/2003 100
05/14/2003 99.999999999999
06/23/2003 100
09/03/2003 99.999999999999
01/14/2004 100
03/05/2004 99.999999999998
The results are summarized in table 3. The differences on the order of 10–12 are due to the fact that the computer ran up against its limits of numerical precision. These figures may vary de-pending on which computer or database system is used.
The next question concerned the reliability of HbA1c values thus predicted. The value from the regression line is the mean of a Gaussian-like distribution. Due to statistical fluctuation, the result is a range of values and probabilities (i.e. 95% CL intervals) rather than a singular value. Based on regression analysis a value from the “smoothened” glucose profile GΔ yields an interval carrying a 95% probability that it covers the actual HbA1c. The confidence range of a value thus predicted depends on its position on the regression line [30]. The confidence interval is narrower in the cluster of points than in areas where points are isolated or absent.
There is a difference between CL and CLI intervals in regression analysis. CLI refers to an individual predicted value while CL refers to a point along the regression line. The regression line is subject to statistical fluctuation as a whole. CL becomes smaller than CLI as more points are available, since this will increasingly enhance the precision of the regression line.

13
Table 4: Compressed overview of CL and CLI intervals for HbA1c values ranging from 6.5 to 8.5. The CL intervals are narrower in this overview as 27 of 40 HbA1c values are around 7.
HbA1c CL lower CL upper CLI lower CLI upper Points
6.5 6.25 6.75 5.59 7.41 5
7 6.86 7.14 6.12 7.88 27
7.5 7.28 7.72 6.60 8.40 6
8 7.67 8.33 7.07 8.93 1
8.5 7.96 9.04 7.48 9.52 1
The SAS output only returned CL and CLI for measured (i.e. actually present) HbA1c values. Since these values were not straightforward integers or half-integers, the figures in table 4 we-re obtained by intrapolation.
In some individuals, the relationship between blood glucose profile and HbA1c may be dis-torted due to physiological conditions or specific habits in glucose measuring. Thus better re-sults may be obtained via individual correlations for all subjects than by blanket analysis.
Table 5: Regression lines and estimates for subjects 10 and 11 based on predicted HbA1c. Regression lines are almost parallel to those obtained with the HbA1c formula from G∆
Subject 10 Subject 11
G∆ Predicted Formula G∆ Predicted Formula
109 7.03 5.87 157 7.63 7.31
116 7.20 6.08 167 7.95 7.61
127 7.47 6.41 156 7.60 7.28
121 7.32 6.23 150 7.41 7.10
120 7.30 6.20 134 6.91 6.62
119 7.27 6.17 126 6.66 6.38
118 7.25 6.14 127 6.69 6.41
114 7.15 6.02 117 6.37 6.11
121 6.50 6.23
129 6.75 6.47
138 7.03 6.74
All blood glucose data of subject 11 were electronically downloaded from the glucometer and stored in a database, such that any bias related to selective logging is excluded. The logs of all other subjects in this article were manually written. The results of CL and CLI analysis for subject 11 do not significantly differ from the overall picture even though the intervals are slightly larger due to a smaller number of regression points. Remarkably, the regression line for predicted HbA1c is almost parallel to the line for the HbA1c formula [1], the latter being

14
0,25% HbA1c lower than the former. The overall difference is two to three times that value in the range of better glycemic control.
The CL figures obtained for subject 10 do not significantly differ from the overall picture ei-ther. Again, the regression line and the line obtained for the HbA1c formula were almost par-allel. Both were 1.11% HbA1c apart, which was a larger distance than in subject 11. Again the lower values were obtained with the formula. The values available for other subjects were too scanty for individual analysis.
Discussion The convolution kernel for HbA1c prediction is derived from integration of the erythrocyte age curve, which would have to be rectangular for a perfect triangle, meaning that all erythro-cyte would have to die precisely after 120 days. Integration does succeed in rendering the fi-nal segment of the age curve less critical. A significant fraction of erythrocytes dying in month 4 would imply that an equal fraction will become older than 4 months. The kernel would then be deformed within a range contributing the 16th part of the entire integral.
Extension: The question arises how values calculated in the past can simplify a system that is based on continuously collected data. It is certainly not useful to store the Fourier coefficients because the base frequencies will change over extended observation intervals. It may be pos-sible to reuse some values when new intervals happen to be an integral multiple of the old ones. If the observation interval is doubled, odd-numbered frequencies need to be calculated from scratch and even-numbered ones for half the new interval, such that the computation load is only reduced by 25%. Extending the observation interval by a factor of “k” will allow 1/k² of the total calculation to be reused. Everything else needs to be recalculated.
Considerable machine power can be saved by recalculating not the entire observation interval. Convolution does not depend on the set of frequencies contained in the Fourier series. Thus the old results for GΔ should not change. To avoid unwanted effects of periodization, the de-parture point of the new observation interval should precede the oldest one of the new HbA1c values by 4 months. Only the immediate result of convolution (i.e. the smoothened profile GΔ) is invariant. Used in regression analysis, the new values can change predicted HbA1c values in the past as well. Therefore all HbA1c values need to undergo regression analysis, although this will not affect the glucose records, which outnumber them by a factor of 800.
Routine application: On first sight, this approach to obtaining HbA1c values may seem im-practical for routine application. Manual editing of glucose data as performed in this project is obviously a laborious task (Table 1). In addition, most glucose records are not archived for the 120 days needed to calculate a predicted HbA1c value. More than ten HbA1c measurements were available for only one patient analyzed in this article. However, projects exist in which records of diabetics are being transferred to servers and remain stored there as part of a life-long health record. Predicted HbA1c values can be obtained at virtually no cost by utilizing systems of this kind. Some projects focus on transmission technology [31-33] and may even supply feedback to the patient [31]. The Austrian ELGA project [34] deals with diabetes as a representative example of a life-long disease and therefore includes private data on glucose, insulin and diet.

15
Predicted HbA1c values in diabetes care: Implementing the presented model in diabetes ca-res would first require diabetics to transmit their blood glucose values to a server. HbA1c val-ues would then be routinely calculated on a daily or weekly basis. If they deteriorate, a mes-sage to the effect that HbA1c is increasing would be sent to the patient by SMS or e-mail, in-cluding a recommendation to consult a physician. Care should be taken about ethical aspects [35] .
A similar approach is indicated for mathematical models analyzing the circadian rhythm of insulin therapy. The patient could be given relatively safe advice, such as to apply base insulin 2 hours earlier.
Another useful application of the mathematical model would be to anticipate critical situa-tions. Cases that need attention would be filtered out by automated routines and be brought to the attention of diabetologists who would then advise those patients by e-mail or call them for a visit if necessary.
In the long term, automated routines of this type should be beneficial for the healthcare sys-tem because some level of monitoring between scheduled check-ups will surely reduce costs by requiring fewer visits to the ward. However, this phase must be preceded by a test period to verify the reliability of the system.
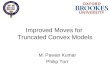
Linear regression analysis: The CL and CLI intervals compiled in Table 4 illustrate the great reliability of predicted HbA1c values by ”compressed“ statistics using groups of indi-vidual pairs. Figure 1 is a graphical representation including all 39 records.
Figure1: CL and CLI corridors with predicted values (of regression analysis) plotted against measured values (asterisks) for all individual pairs.

16
6,86
CL lower7,14
CL upper
6,12
CLI lower
7,88
CLI upper
7,00
6,5
7,5
8,0
5
6
7
8
9
10
6 7 8
The CL interval in Figure 1 is significantly narrower where observation points are densely clustered and opens trumpet-style as the frequency of observations decreases in the presence of increasing HbA1c values.
The CLI interval in Figure 1 simply indicates what we get by calculating a HbA1c value with the proposed method. Figure 1 shows that 1 of 39 points is outside of the CLI corridor, re-flecting a 95% probability (i.e. in 19 out of 20 cases) that the value returned from the labora-tory for a simultaneously obtained blood sample will be inside this CLI interval.
As already noted, the CL corridor is the area covered by 95% of all regression lines. Thus there is a 95% probability that the true regression line will be inside the CL corridor. The true regression line is reflected more closely as more points along its course are available. The CL corridor will then become narrower and ultimately (if a large number of points are available) form a straight line rather than a band with flaring ends. While personal glucometer meas-urements will normally involve 20% fluctuation, a mean number of 582 glucose values as processed to single GΔ values in the present study is very likely to compensate for this fluctua-tion. A constant mean level of deviation will naturally remain and will cause parallel transla-tion of regression lines when individual analysis is performed (Table 5). In blanket analysis, both the deviations introduced by different glucometers and the bias introduced by individual measurement habits will cause some fluctuation of GΔ values. However, any fluctuation of glucose values is not expected to be significant in individual analysis.
Lack of a linear association between mean glucose (GΔ) and HbA1c values might conceivably be a source of fluctuation in linear regression. The HbA1c content of erythrocytes is linearly proportional to speed of HbA1c formation and duration of exposure to the glycosylating envi-ronment. This duration is constant as the life span of erythrocytes is essentially constant. It is reasonable to infer from the above model of HbA1c formation that its speed is almost linearly proportional to glucose concentrations. Therefore, since GΔ is a mean glucose level respecting

17
the model of HbA1c formation, a linear association between HbA1c content and GΔ does exist through formation speed.
Ultimately, the HbA1c values coming from the laboratory are the main source of fluctuation. In blanket analysis, some fluctuation will also be present on the glucose side as different glu-cometers and measuring habits enter the equation. For a small number of pairs, the regression line itself is only obtained within the probability limits of a 95% CL corridor. In a sense, the difference between CL and CLI is essentially due to statistical fluctuation of HbA1c meas-urements. The figures would suggest inaccuracies in the range of 0.5% for HbA1c values coming from the laboratory.
Figure 2: Regression line and line produced by the HbA1c formula. The formula seems too “optimistic” in the range of better glycemic control. According to the CL corridor, this devia-tion can be due to statistical fluctuation only for HbA1c > 7.5%.
HbA1c Formula
CL lower
CL upper
5
6
7
8
9
10
100 120 140 160 180 200 220 240
Since the mathematical model is naturally based on glucose values from the logbook, Figure 2 could be read as indicating that true glucose levels are higher than would appear from the log-book. However, this does not imply that the true situation has been intentionally misrepre-sented. Both functional insulin therapy (FIT) and conventional therapy (CT) usually require patients to measure their blood glucose levels before meals to adjust insulin doses or food in-take. Glucose levels will then remain elevated for a few hours after meals, but these levels are not normally measured or logged, simply because there are no appropriate columns in the logbook. In addition, some diabetics may avoid measuring when they know the values will be high. The reason why better matches are obtained at higher HbA1c levels could be that the glucose profile may be less stable. Low glucose values before meals would then be less spe-cific due to a higher degree of general variability, as would be increased values after meals.

18
The data for two subjects analyzed individually yielded regression lines that were remarkably parallel to the lines obtained with the established HbA1c formula. This suggests that the in-herent bias in glucose profiles, while varying from one diabetic to the next, is fairly constant for the same individual over a range of HbA1c values.
Conclusions The model is best implemented in a system that will collect glucose data of patients and allow them to be transferred to a database. Today a high level of automation is required as health-care systems are becoming inordinately expensive. Predicted HbA1c values and other modes of analyzing blood glucose profiles are no exception but should be automated as well. Feed-back supplied to the patients should also be automated unless glucose values exceed a prede-fined range continuously or repeatedly. A diabetologist should be alerted if a critical situation occurs, which the proposed system can help to identify [36]. The system cannot prescribe or change therapy [35] but it can give recommendations involving little risk such as to see a dia-betologist.
To some extent, the CL corridor is better suited for monitoring requirements than CLI. Pre-dicted HbA1c values would only be regarded as undergoing change in diabetes care if the CL limits are exceeded. Some physicians may want to have a safety margin in making statements. Depending on the specific clinical situation, it may be appropriate to base statements of this kind not on predicted values along the regression line but on the (upper or lower) CL.
Additional information could be obtained by performing regression analysis for each diabetic individually. If the proposed system of calculated HbA1c has been implemented in a database system and enough HbA1c/GΔ pairs of a patient have been collected, then the current status of glycemic control is indicated by maximum clustering of points. Incipient change can be de-tected more readily because it is reasonable that predicted values located within that cluster should be more accurate. Values located outside of the cluster may still indicate change, even tough with less precision. By reflecting deterioration or improvement, the mathematical model can be a valuable aid in clinical decision-making.
CL intervals can thus help to distinguish change from mere fluctuation. As a practical exam-ple, diabetics with good glycemic control might want to notice incipient change to take ap-propriate measures. Patients with poor control might want to try different regimens and may identify the most appropriate strategy by the greater accuracy of predicted HbA1c values in the higher range.
Individual habits of glucose measurement appear to have a significant effect by introducing bias. A way to conserve values that would not normally be logged is by automated data trans-fer from the glucometer to a remote server. In this way, enough data could be accumulated to obtain meaningful results by individual regression analysis and to eliminate some bias-related fluctuation.
Theoretical implications of the present study include the triangle-shaped convolution kernel and the fact that a Fourier transform and Fourier series were implemented in standard SQL language with trigonometric functions.

19
Acknowledgements
Special thanks are due to Harald Heinzl for his very useful and informative discussion of sta-tistical data analysis. I am indebted to Julian Eigenbauer for manually typing most of the glu-cose data from hardcopy prints.

20
References 1. Thomas, L., Labor und Diagnose, 5.Auflage. 1998. 5.
2. Larizza, C., et al., The M2DM Project--the experience of two Italian clinical sites with clinical evaluation of a multi-access service for the management of diabetes mellitus patients. Methods Inf Med, 2006. 45(1): p. 79-84.
3. DeVries, J.H., et al., Improved glycaemic control in type 1 diabetes patients following participation per se in a clinical trial--mechanisms and implications. Diabetes Metab Res Rev, 2003. 19(5): p. 357-62.
4. Nomura, D.M., Importance of using and understanding self-monitoring of blood glu-cose (SMBG) data in assessing ambient and long-term glycaemic control. J Indian Med Assoc, 2002. 100(7): p. 448, 450-1.
5. Marre, M. and J.P. Sauvanet, [What allows a type 1 diabetic to be well controlled]. Diabetes Metab, 2002. 28(4 Pt 2): p. 2S7-2S14.
6. Rodgers, J. and R. Walker, Glycaemic control in type 2 diabetes. Nurs Times, 2002. 98(19): p. 56-7.
7. Rahlenbeck, S.I., Monitoring diabetic control in developing countries: a review of glycated haemoglobin and fructosamine assays. Trop Doct, 1998. 28(1): p. 9-15.
8. Dworacka, M., et al., 1,5-anhydro-D-glucitol: a novel marker of glucose excursions. Int J Clin Pract Suppl, 2002(129): p. 40-4.
9. Jeffcoate, S.L., Diabetes control and complications: the role of glycated haemoglobin, 25 years on. Diabet Med, 2004. 21(7): p. 657-65.
10. Bunn, H.F., K.H. Gabbay, and P.M. Gallop, The glycosylation of hemoglobin: rele-vance to diabetes mellitus. Science, 1978. 200(4337): p. 21-7.
11. Schernthaner, G., et al., [The clinical importance of glycohaemoglobin (HbA1) (au-thor's transl)]. Wien Klin Wochenschr Suppl, 1980. 115: p. 1-11.
12. Kasezawa, N., et al., Criteria for screening diabetes mellitus using serum fructosa-mine level and fasting plasma glucose level. The Japanese Society of Multiphasic Health Testing and Services (JMHT), Fructosamine Working Committee. Methods Inf Med, 1993. 32(3): p. 237-40.
13. Gugliucci, A., Glycation as the glucose link to diabetic complications. J Am Osteo-path Assoc, 2000. 100(10): p. 621-34.
14. Higgins, P.J. and H.F. Bunn, Kinetic analysis of the nonenzymatic glycosylation of hemoglobin. J Biol Chem, 1981. 256(10): p. 5204-8.
15. Kilpatrick, E.S., Problems in the assessment of glycaemic control in diabetes mellitus. Diabet Med, 1997. 14(10): p. 819-31.
16. Kildegaard, J., et al., A study of trained clinicians' blood glucose predictions based on diaries of people with type 1 diabetes. Methods Inf Med, 2007. 46(5): p. 553-7.
17. Hyysalo, S. and J. Lehenkari, An activity-theoretical method for studying user partici-pation in IS design. Methods Inf Med, 2003. 42(4): p. 398-404.
18. Goldwyn, A.J. and G. Ember, DIAPAS: A "personalized alerting service" for diabetes. Methods Inf Med, 1967. 6(3): p. 130-5.

21
19. Park, J. and D.W. Edington, Application of a prediction model for identification of in-dividuals at diabetic risk. Methods Inf Med, 2004. 43(3): p. 273-81.
20. Armengol, E., A. Palaudaries, and E. Plaza, Individual prognosis of diabetes long-term risks: a CBR approach. Methods Inf Med, 2001. 40(1): p. 46-51.
21. Chakravarty, S. and Y. Shahar, Acquisition and analysis of repeating patterns in time-oriented clinical data. Methods Inf Med, 2001. 40(5): p. 410-20.
22. Achtmeyer, C.E., T.H. Payne, and B.D. Anawalt, Computer order entry system de-creased use of sliding scale insulin regimens. Methods Inf Med, 2002. 41(4): p. 277-81.
23. Miller, J.D., et al., Spontaneous and stimulated growth hormone release in adoles-cents with type I diabetes mellitus: effects of metabolic control. J Clin Endocrinol Me-tab, 1992. 75(4): p. 1087-91.
24. Derr, R., et al., Is HbA(1c) affected by glycemic instability? Diabetes Care, 2003. 26(10): p. 2728-33.
25. Näser, K.-H., Physikalische Chemie. 1960, Leipzig: VEB Deutscher Verlag für Grundstoffindustrie.
26. Heuser, H., Lehrbuch der Analysis Teil 1. Vol. 1. 1986, Stuttgart: B.G.Teubner.
27. Temsch, W., Discrete Fourier Analysis, Diploma Thesis. 12/1996: Vienna. 28. Feichtinger, H.G. and K. Gröchenig, Theory and practice of irregular sampling.
29. Strohmer, T., Irregular Sampling, Frames and Pseudoinverse. 1991.
30. Sachs, L., Angewandte Statistik. 6 ed. 1984, Berlin, Heidelberg, New York, Tokyo: Springer Verlag.
31. Kastner, P., et al., Diab-Memory: Ein mobilfunk-gestütztes Datenservice zur Unter-stützung der funktionellen Insulintherapie. 2003.
32. Andersson, N., Prototype for Transmission of Glucometer Data by Wireless Technol-ogy. http://www.csd.uu.se/datalogi/cmtrl/xjobb/docs-reports/Niklas_Andersson-2003.pdf.
33. Adlaßnig, A., Mobiltelefone als Blutzuckermeßgeräte. www.diabetes-news.de.
34. Dorda, W., et al., Introducing the electronic health record in austria. Stud Health Technol Inform, 2005. 116: p. 119-24.
35. Collste, G., N. Shahsavar, and H. Gill, A decision support system for diabetes care: ethical aspects. Methods Inf Med, 1999. 38(4-5): p. 313-6.
36. Biermann, E., et al., Semi-automatic generation of medical tele-expert opinion for primary care physician. Methods Inf Med, 2003. 42(3): p. 212-9.

22
Table 1: Patient IDs, observation intervals and glucose/HbA1c records
ID Observation interval Number of records
(MM/DD/YYYY) Glucose HbA1c
1 03/12/2002 04/30/2004 2520 5
2 06/25/2003 08/29/2004 2493 4
3 01/19/2004 08/01/2004 1008 1
4 11/24/2003 09/08/2004 2514 2
5 04/19/2004 08/08/2004 446 1
6 12/22/2003 09/19/2004 1316 2
7 04/05/2004 08/08/2004 966 1
8 05/09/2003 05/13/2004 2276 3
9 01/12/2004 07/11/2004 1062 1
10 04/30/2000 05/05/2004 4414 8
11 12/26/2001 04/26/2004 5529 11

23
Table 2: An appropriate mean glucose value (GΔ) was calculated for each of the 39 HbA1c re-
cords by convolution with the triangle-shaped weight function.
ID Date HbA1c G∆ ID Date HbA1c G∆
1 09/25/2002 6.7 123 9 07/11/2004 8.3 136
1 02/03/2003 6.3 120 10 10/11/2000 6.9 109
1 06/02/2003 6.6 129 10 06/13/2001 7.1 116
1 10/06/2003 7.1 132 10 12/05/2001 7.4 127
1 02/16/2004 6.6 123 10 11/27/2002 7.4 121
2 12/17/2003 7.1 129 10 05/07/2003 7.5 120
2 03/09/2004 7.7 127 10 09/17/2003 6.9 119
2 07/21/2004 7.4 132 10 01/14/2004 7.4 118
2 08/29/2004 7.2 134 10 04/21/2004 7.4 114
3 08/05/2004 7.1 124 11 08/08/2002 7.9 157
4 04/15/2004 7.1 114 11 09/05/2002 7.9 167
4 09/08/2004 6.7 104 11 10/22/2002 7.7 156
5 08/19/2004 6.3 127 11 11/28/2002 7.2 150
6 06/17/2004 7.5 143 11 01/29/2003 6.8 134
6 09/19/2004 7.7 142 11 03/19/2003 6.4 126
7 08/08/2004 8.4 195 11 05/14/2003 7.1 127
8 10/06/2003 6.2 102 11 06/23/2003 6.4 117
8 01/19/2004 6.5 104 11 09/03/2003 6.4 121
8 04/19/2004 6.2 111 11 01/14/2004 7.1 129
11 03/05/2004 6.6 138

24
Table 3: Test with timestamp data from subject 11 and a constant blood glucose value
08/08/2002 100
09/05/2002 100
10/22/2002 99.999999999999
11/28/2002 100
01/29/2003 100
03/19/2003 100
05/14/2003 99.999999999999
06/23/2003 100
09/03/2003 99.999999999999
01/14/2004 100
03/05/2004 99.999999999998

25
Table 4: Compressed overview of CL and CLI intervals for HbA1c values ranging from 6.5 to
8.5. The CL intervals are narrower in this overview as 27 of 40 HbA1c values are around 7.
HbA1c CL lower CL upper CLI lower CLI upper Points
6.5 6.25 6.75 5.59 7.41 5
7 6.86 7.14 6.12 7.88 27
7.5 7.28 7.72 6.60 8.40 6
8 7.67 8.33 7.07 8.93 1
8.5 7.96 9.04 7.48 9.52 1

26
Table 5: Regression lines and estimates for subjects 10 and 11 based on predicted HbA1c.
Regression lines are almost parallel to those obtained with the HbA1c formula from G∆
Subject 10 Subject 11
G∆ Predicted Formula G∆ Predicted Formula
109 7.03 5.87 157 7.63 7.31
116 7.20 6.08 167 7.95 7.61
127 7.47 6.41 156 7.60 7.28
121 7.32 6.23 150 7.41 7.10
120 7.30 6.20 134 6.91 6.62
119 7.27 6.17 126 6.66 6.38
118 7.25 6.14 127 6.69 6.41
114 7.15 6.02 117 6.37 6.11
121 6.50 6.23
129 6.75 6.47
138 7.03 6.74

27
Figure1: CL and CLI corridors with predicted values (of regression analysis) plotted against
measured values (asterisks) for all individual pairs.

28
Figure 2: Regression line and line produced by the HbA1c formula. The formula seems too
“optimistic” in the range of better glycemic control. According to the CL corridor, this devia-
tion can be due to statistical fluctuation only for HbA1c > 7.5%.