Embed Size (px)
Citation preview

La determinazione della HbA1C:
aspetti metodologici ed implicazioni cliniche
Roberto Scatena, Teresa De Michele, Francesca Annunziata, Giulia Canu
Dipartimento di Medicina di LaboratorioPoliclinico A. Gemelli - Università Cattolica
The Diagnosis of Diabetes Is Changing: How
Implementation of Hemoglobin A1c Will Impact
Clinical LaboratoriesDavid B. Sacks
Clinical Chemistry 2009, 55, 1612–1614.
HbA1c: how do we measure it and what does it mean?Randie R. Little and David B. Sacks
Current Opinion in Endocrinology, Diabetes & Obesity 2009, 16,113–118
International Expert Committee Report on
the Role of the A1C Assay in the Diagnosis
of Diabetes
An International Expert Committee with members appointed by the American Diabetes Association, the European Association for the Studyof Diabetes, and the International Diabetes Federation was convened in 2008 to consider the current and future means of diagnosing diabetesin nonpregnant individuals. The report of the International Expert Committee represents the consensus view of its members and notnecessarily the view of the organizations that appointed them. The International Expert Committee hopes that its report will serve as a stimulus to the international community and professional organizationsto consider the use of the A1C assay for the diagnosis of diabetes.
DIABETES CARE,32, 7, JULY 2009
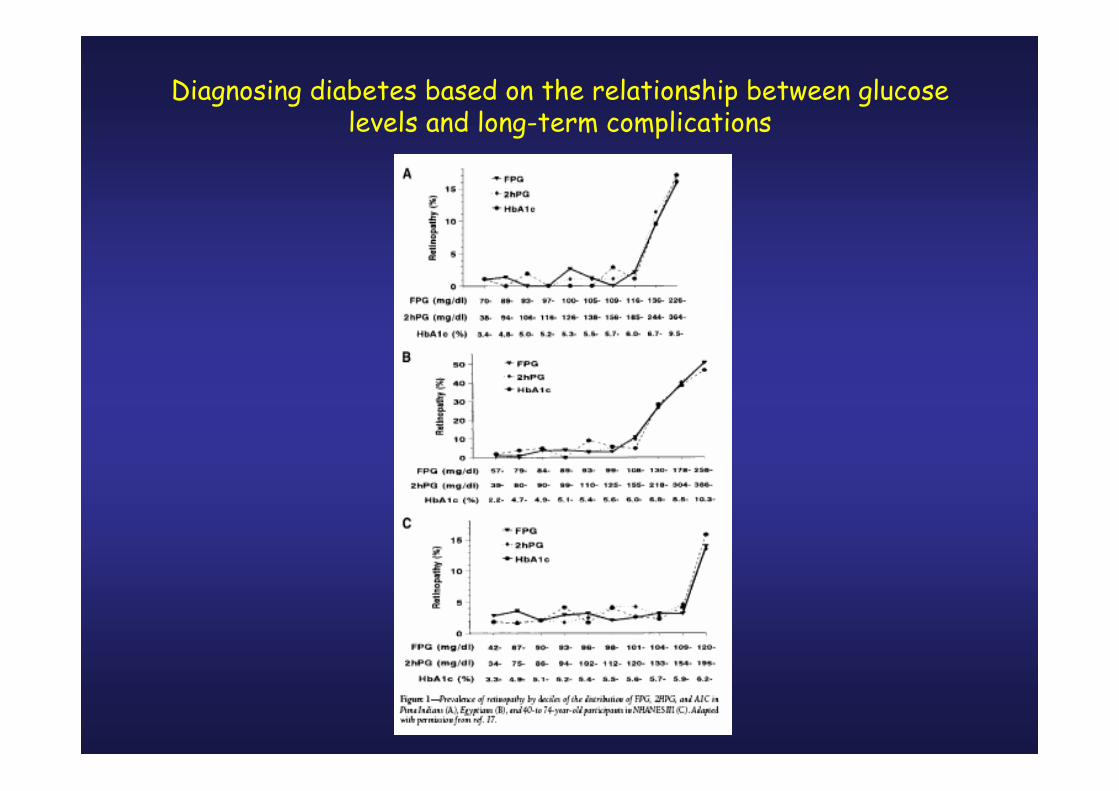
Diagnosing diabetes based on the relationship between glucoselevels and long-term complications
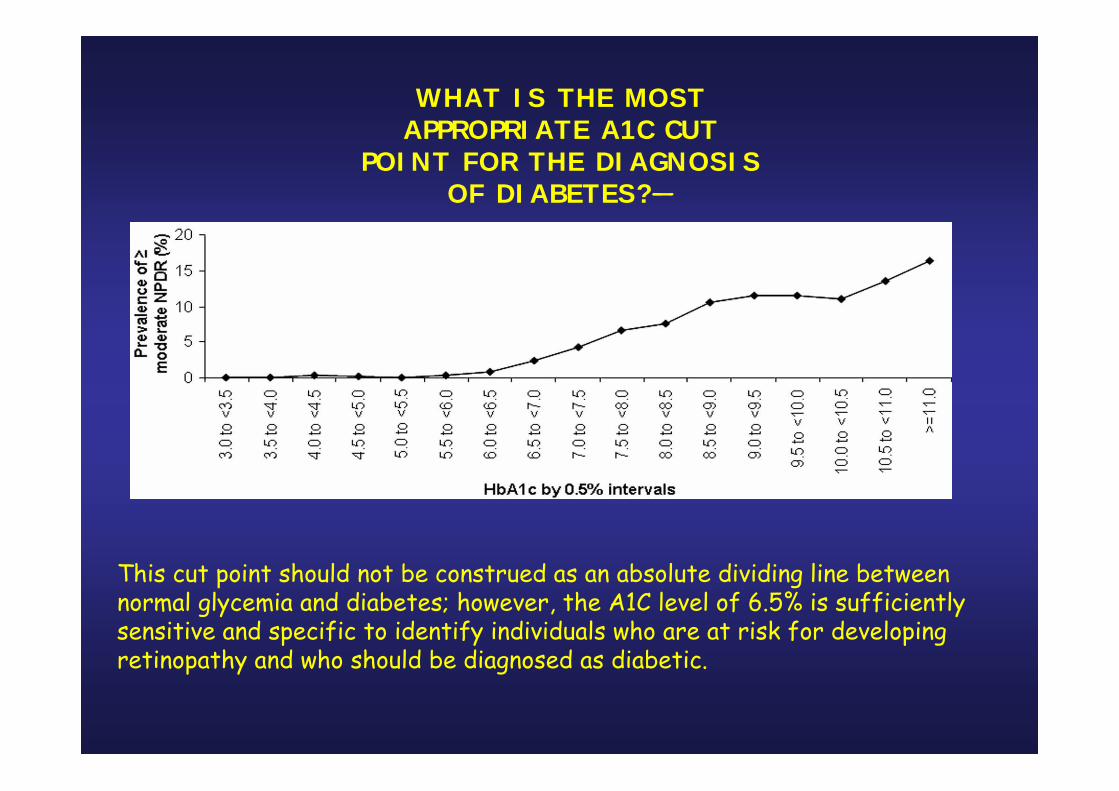
WHAT IS THE MOSTAPPROPRIATE A1C CUT
POINT FOR THE DIAGNOSISOF DIABETES?—
This cut point should not be construed as an absolute dividing line betweennormal glycemia and diabetes; however, the A1C level of 6.5% is sufficientlysensitive and specific to identify individuals who are at risk for developingretinopathy and who should be diagnosed as diabetic.
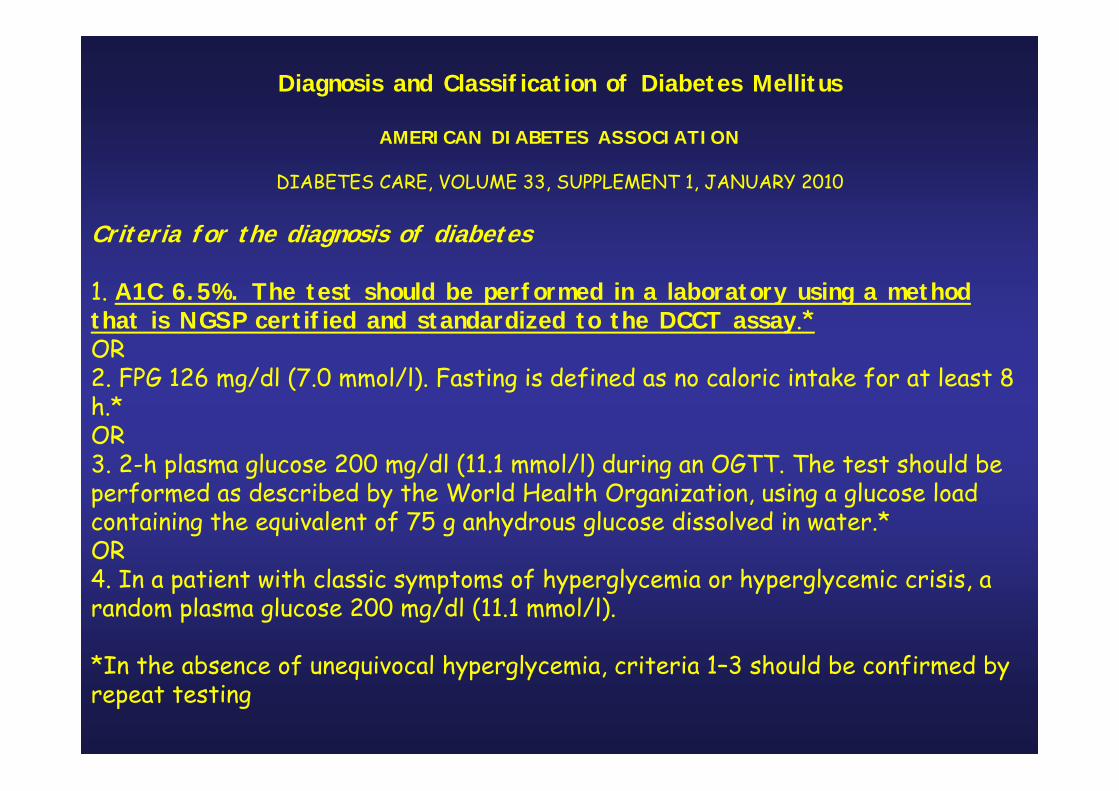
Diagnosis and Classification of Diabetes Mellitus
AMERICAN DIABETES ASSOCIATION
DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010
Criteria for the diagnosis of diabetes
1. A1C 6.5%. The test should be performed in a laboratory using a methodthat is NGSP certified and standardized to the DCCT assay.*OR2. FPG 126 mg/dl (7.0 mmol/l). Fasting is defined as no caloric intake for at least 8 h.*OR3. 2-h plasma glucose 200 mg/dl (11.1 mmol/l) during an OGTT. The test should beperformed as described by the World Health Organization, using a glucose loadcontaining the equivalent of 75 g anhydrous glucose dissolved in water.*OR4. In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose 200 mg/dl (11.1 mmol/l).
*In the absence of unequivocal hyperglycemia, criteria 1–3 should be confirmed byrepeat testing
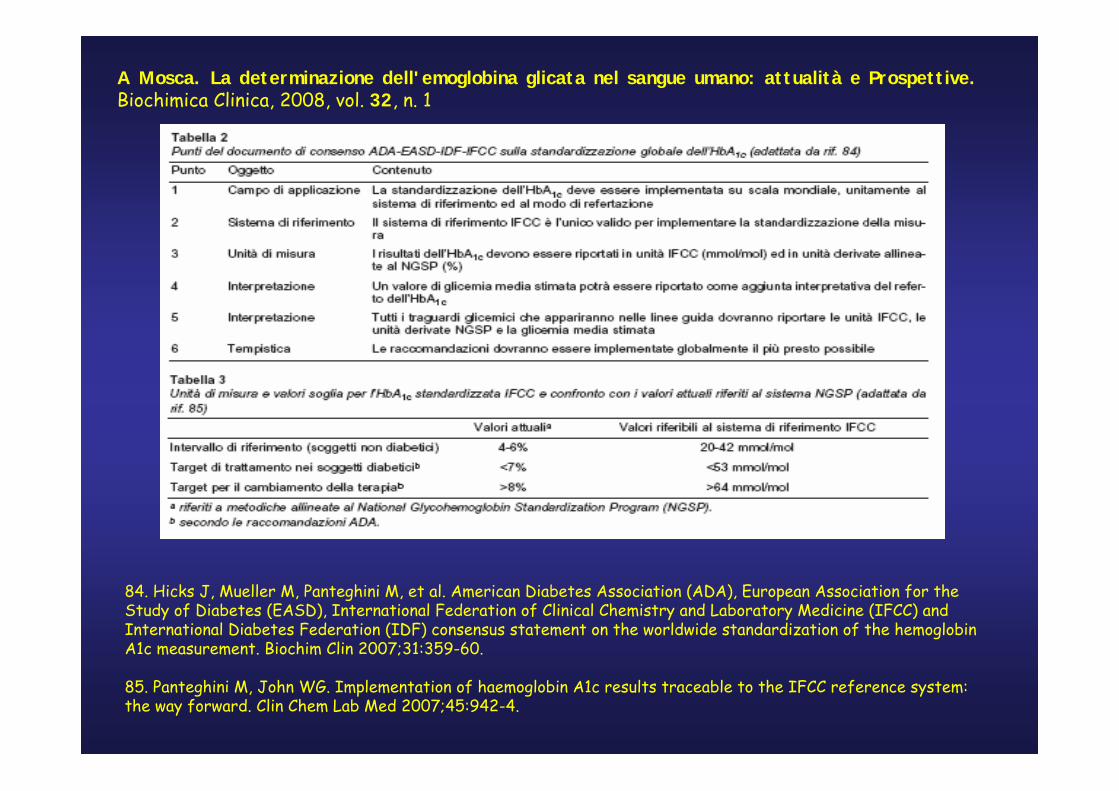
A Mosca. La determinazione dell'emoglobina glicata nel sangue umano: attualità e Prospettive. Biochimica Clinica, 2008, vol. 32, n. 1
84. Hicks J, Mueller M, Panteghini M, et al. American Diabetes Association (ADA), European Association for theStudy of Diabetes (EASD), International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) andInternational Diabetes Federation (IDF) consensus statement on the worldwide standardization of the hemoglobinA1c measurement. Biochim Clin 2007;31:359-60.
85. Panteghini M, John WG. Implementation of haemoglobin A1c results traceable to the IFCC reference system: the way forward. Clin Chem Lab Med 2007;45:942-4.
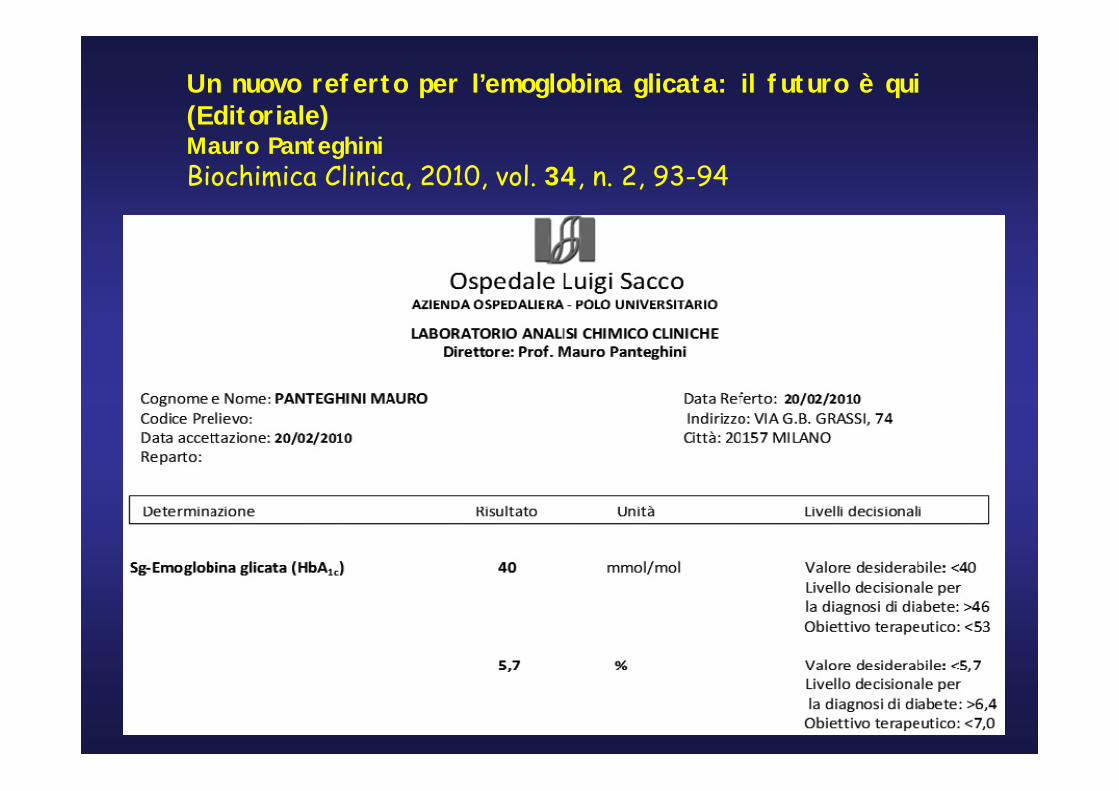
Un nuovo referto per l’emoglobina glicata: il futuro è qui (Editoriale)Mauro PanteghiniBiochimica Clinica, 2010, vol. 34, n. 2, 93-94
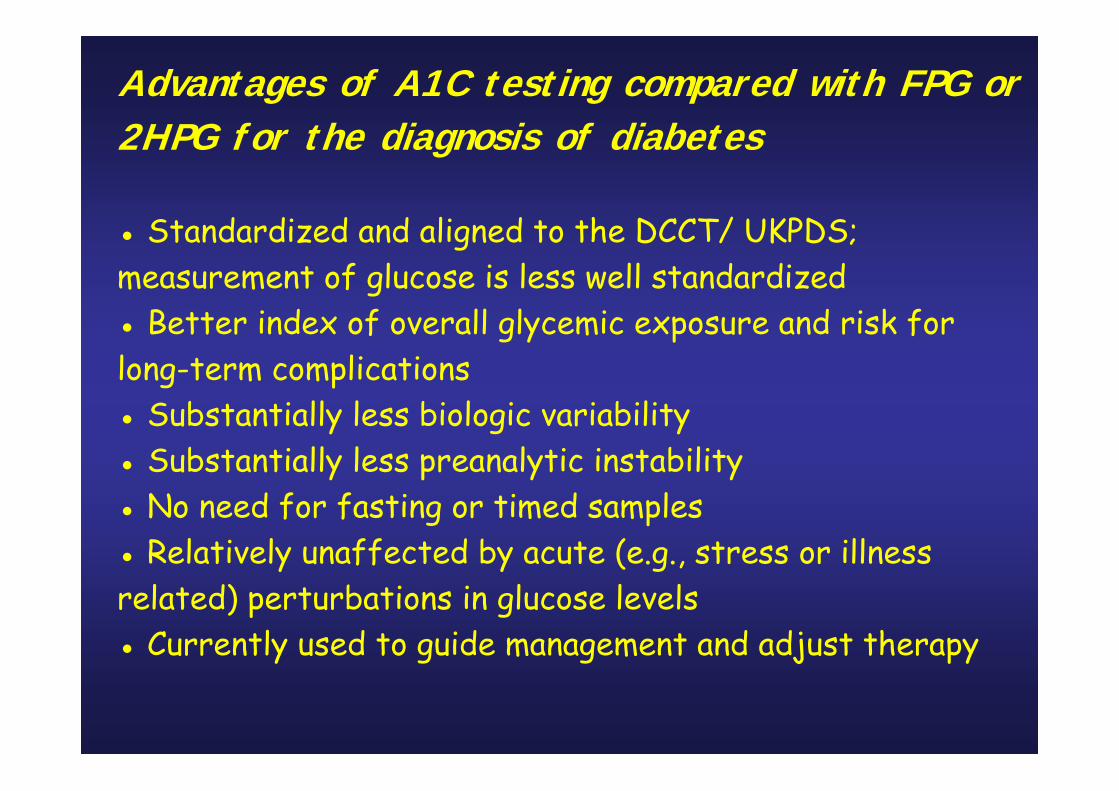
Advantages of A1C testing compared with FPG or 2HPG for the diagnosis of diabetes
● Standardized and aligned to the DCCT/ UKPDS; measurement of glucose is less well standardized● Better index of overall glycemic exposure and risk forlong-term complications● Substantially less biologic variability● Substantially less preanalytic instability● No need for fasting or timed samples● Relatively unaffected by acute (e.g., stress or illnessrelated) perturbations in glucose levels● Currently used to guide management and adjust therapy
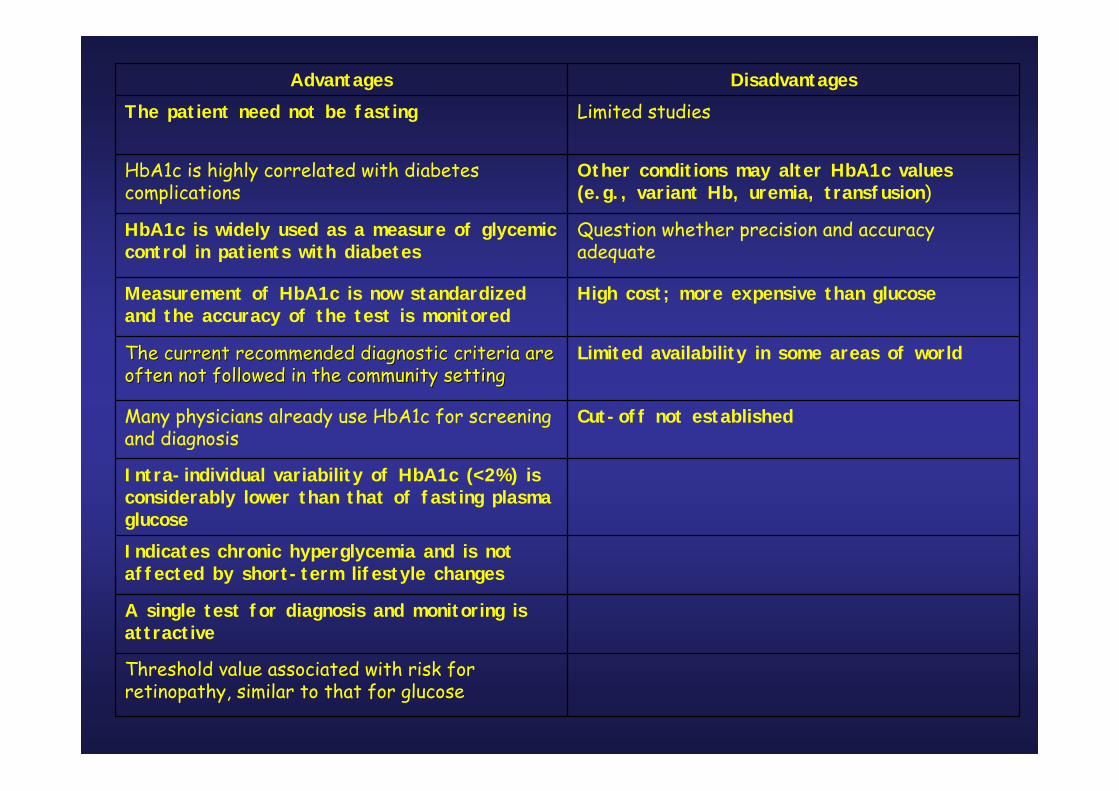
Threshold value associated with risk for retinopathy, similar to that for glucose
A single test for diagnosis and monitoring is attractive
Indicates chronic hyperglycemia and is not affected by short-term lifestyle changes
Intra-individual variability of HbA1c (<2%) is considerably lower than that of fasting plasma glucose
Cut-off not establishedMany physicians already use HbA1c for screening and diagnosis
Limited availability in some areas of worldThe current recommended diagnostic criteria are The current recommended diagnostic criteria are often not followed in the community settingoften not followed in the community setting
High cost; more expensive than glucoseMeasurement of HbA1c is now standardized and the accuracy of the test is monitored
Question whether precision and accuracy adequate
HbA1c is widely used as a measure of glycemiccontrol in patients with diabetes
Other conditions may alter HbA1c values (e.g., variant Hb, uremia, transfusion)
HbA1c is highly correlated with diabetes complications
Limited studiesThe patient need not be fastingDisadvantagesAdvantages
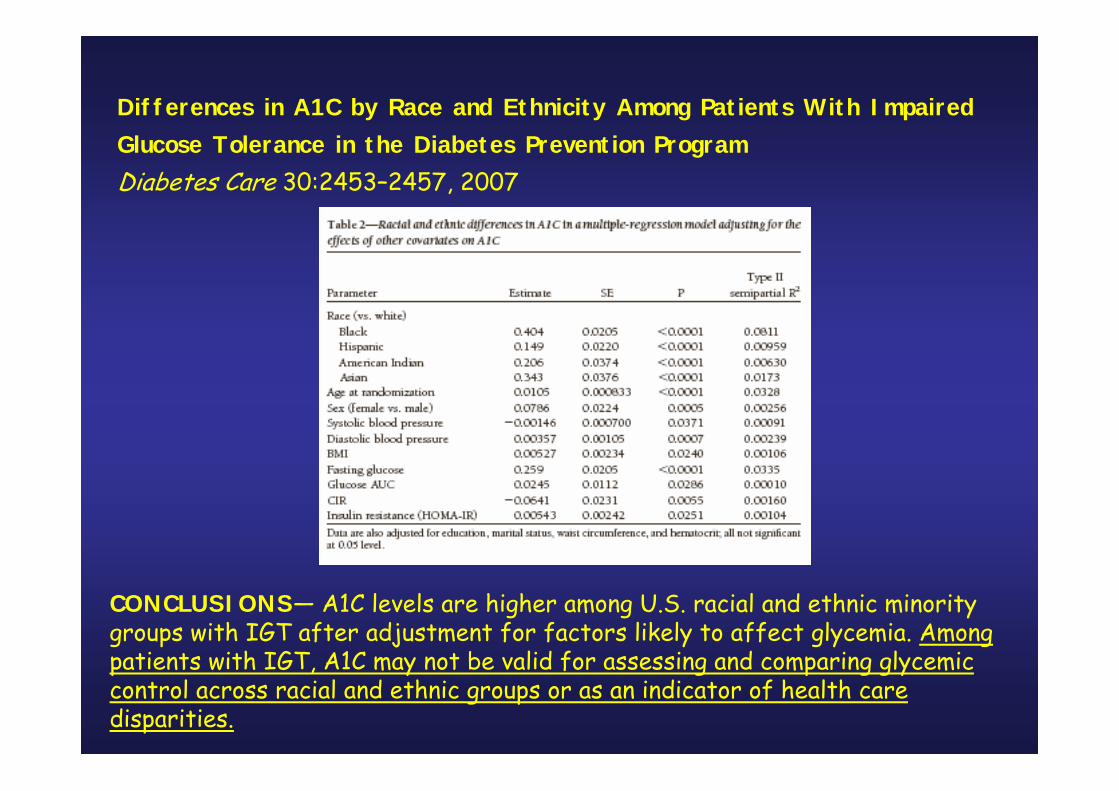
Differences in A1C by Race and Ethnicity Among Patients With ImpairedGlucose Tolerance in the Diabetes Prevention ProgramDiabetes Care 30:2453–2457, 2007
CONCLUSIONS— A1C levels are higher among U.S. racial and ethnic minoritygroups with IGT after adjustment for factors likely to affect glycemia. Amongpatients with IGT, A1C may not be valid for assessing and comparing glycemiccontrol across racial and ethnic groups or as an indicator of health care disparities.

Rahbar, S. (1968) An Abnormal hemoglobinin Red Cells of Diabetics. Clinica Chimica Acta 22(2): 296–298
Huisman TH, Martis EA, Dozy A (1958). "Chromatography ofhemoglobin types on carboxymethylcellulose". J. Lab. Clin. Med. 52(2): 312–27.
Bookchin RM, Gallop PM (1968). "Structure of hemoglobin A1c: nature of the N-terminal beta chain blocking group". Biochem. Biophys. Res. Commun. 32 (1): 86–93.
Bunn HF, Haney DN, Gabbay KH, Gallop PM (1975). "Furtheridentification of the nature and linkage of the carbohydrate in hemoglobin A1c". Biochem. Biophys. Res. Commun. 67 (1): 103–9.
Koenig RJ, Peterson CM, Jones RL, Saudek C, Lehrman M, Cerami A (1976). "Correlation of glucose regulation and hemoglobin AIc in diabetes mellitus". N. Engl. J. Med. 295 (8): 417–20

1978 – Assays commercially available
1988 – ADA recommends routine testing
Currently > numerous glycohemoglobin assay methods
- immunoassays
- ion-exchange HPLC
- boronate affinity HPLC
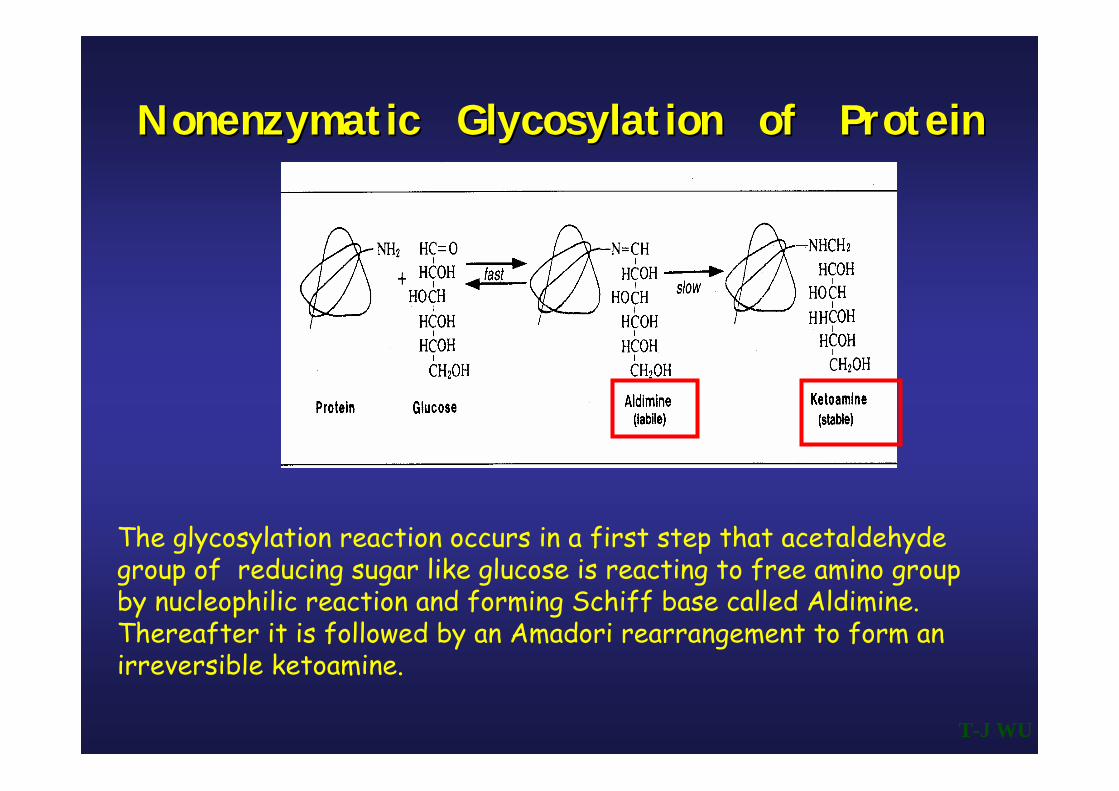
The glycosylation reaction occurs in a first step that acetaldehyde group of reducing sugar like glucose is reacting to free amino group by nucleophilic reaction and forming Schiff base called Aldimine. Thereafter it is followed by an Amadori rearrangement to form an irreversible ketoamine.
NonenzymaticNonenzymatic Glycosylation of ProteinGlycosylation of Protein
T-J WU

Da un punto di vista biochimico la reazione di glicazione dell’emoglobina ècomplessa, soprattutto per due motivi:
(a) perché più residui aminoacidici sono in grado di reagire col glucosio, principalmente le valine terminali delle catene β (Val 1β), ma anche diversi altri residui (Lys 66β, Lys 17β, Val 1α);
(b) perché la reazione ad ogni residuo avviene in più fasi, passando prima per una fase reversibile (formazione della aldimmina) e quindi per una fase lenta, praticamente irreversibile (ketoammina).
(c) Alcuni recenti dati di letteratura hanno provato che la glicazione ai residui N-terminali delle catene β rappresenta circa il 60% della glicazione totale della molecola, ma che esistono significative differenze tra individui a seconda del grado di scompenso glicometabolico
Mosca A., et al. La determinazione dell’emoglobina glicata (HbA1c) nel sangue: raccomandazioni. Biochimica Clinica, 2000, 24, 183
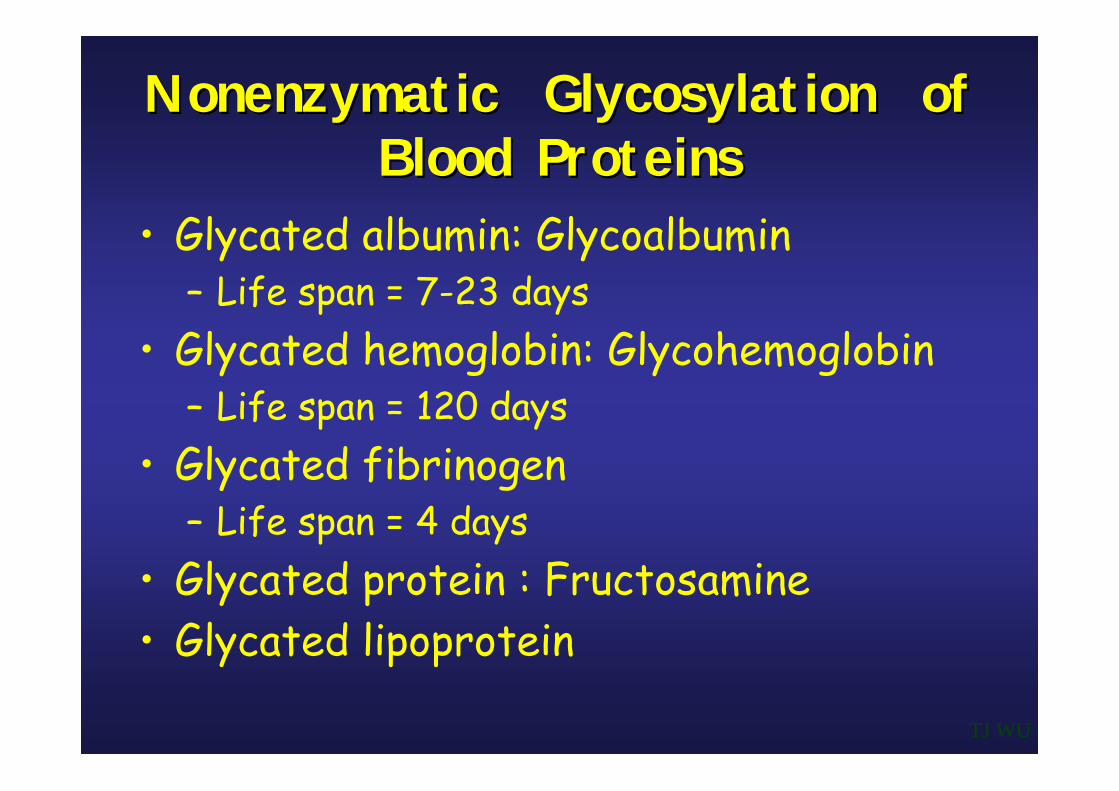
NonenzymaticNonenzymatic Glycosylation of Glycosylation of Blood ProteinsBlood Proteins
• Glycated albumin: Glycoalbumin– Life span = 7-23 days
• Glycated hemoglobin: Glycohemoglobin– Life span = 120 days
• Glycated fibrinogen– Life span = 4 days
• Glycated protein : Fructosamine• Glycated lipoprotein
TJ WU
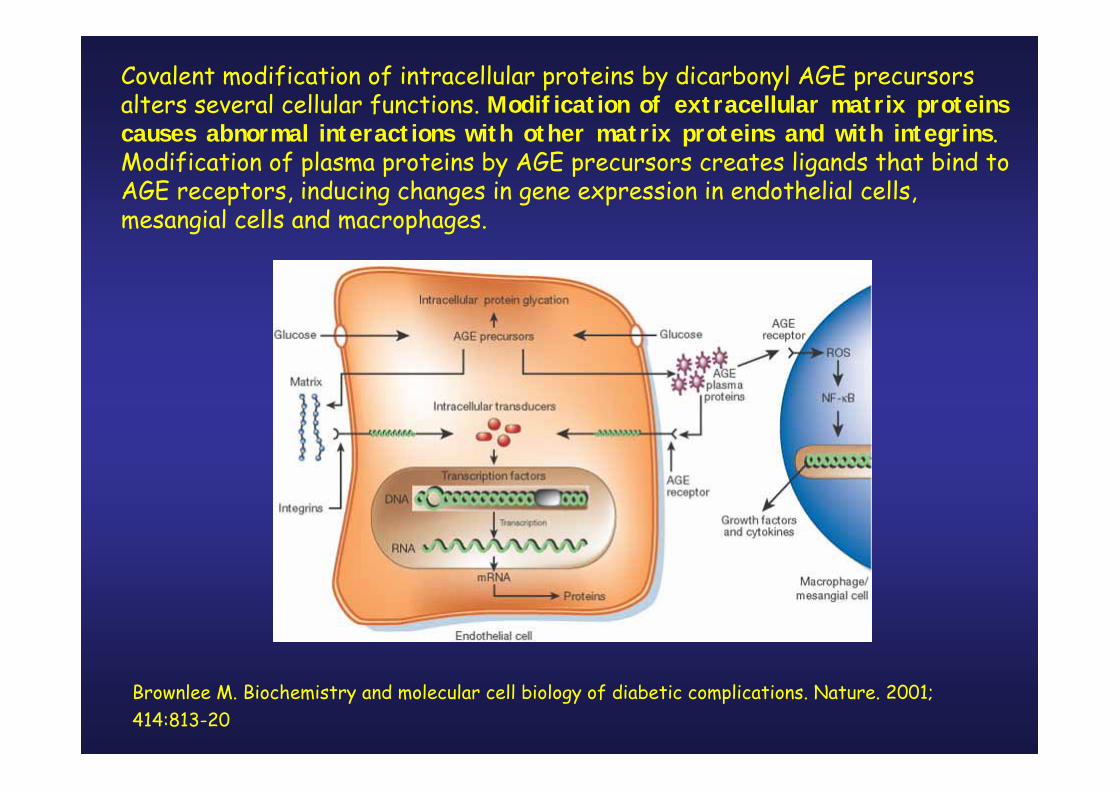
Covalent modification of intracellular proteins by dicarbonyl AGE precursorsalters several cellular functions. Modification of extracellular matrix proteinscauses abnormal interactions with other matrix proteins and with integrins. Modification of plasma proteins by AGE precursors creates ligands that bind toAGE receptors, inducing changes in gene expression in endothelial cells, mesangial cells and macrophages.
Brownlee M. Biochemistry and molecular cell biology of diabetic complications. Nature. 2001; 414:813-20

1: Semba RD, et al. Does Accumulation of Advanced Glycation End Products Contribute to the Aging Phenotype? J Gerontol A Biol Sci Med Sci. 2010
2: Jacobson J, et al. Biomarkers of aging in Drosophila. Aging Cell. 2010 Mar
3: Daroux M, et al. Advanced glycation end-products: implications for diabetic and non-diabetic nephropathies. Diabetes Metab. 2010 Feb;36(1):1-10
4: Vlassara H, et al. Identifying advanced glycation end products as a major source of oxidants in aging: implications for the management and/or prevention of reduced renal function in elderlypersons. Semin Nephrol. 2009 Nov;29(6):594-603.
5: Gugliucci A, et al. Short-term low calorie diet intervention reduces serum advanced glycation end products in healthy overweight or obese adults. Ann Nutr Metab. 2009;54(3):197-201
6:Srikanth V, et al. Advanced glycation endproducts and their receptor RAGE in Alzheimer's disease. Neurobiol Aging. 2009 May 21
7: Peppa M, et al. Advanced glycation end products and cardiovascular disease. Curr Diabetes Rev. 2008 May;4(2):92-100.
8: Takeuchi M, et al. Possible involvement of advanced glycation end-products (AGEs) in the pathogenesis of Alzheimer's disease. Curr Pharm Des 2008;14(10):973-8.
9: Abe R, et al. AGE-RAGE system and carcinogenesis. Curr Pharm Des. 2008;14(10):940-5.
10: Scatena R, et al. Impaired reactive oxygen metabolism of phagocytic leukocytes in NIDDMpatients. A role for non-enzymatic glycosylation of collagen. J Biolumin Chemilumin. 1998,13, 273.
11: Scatena R, et al. Monocyte oxygenation activities are significantly influenced by non-enzymatic glycosylation of collagen. J Biolumin Chemilumin. 1996, 11,207.

Hemoglobin A1c
The gold standard for more than 20 years for the measurement of chronic glycemia
Took many years for clinicians and patients to appreciate why the term ‘glycated hemoglobin’ or ‘hemoglobin A1c’ and its units
(4 – 6%) would be relevant in diabetes
Many patients still do not understand the relevance of the AMany patients still do not understand the relevance of the A11c c name and unitsname and units
Few people understand the biology of the assay
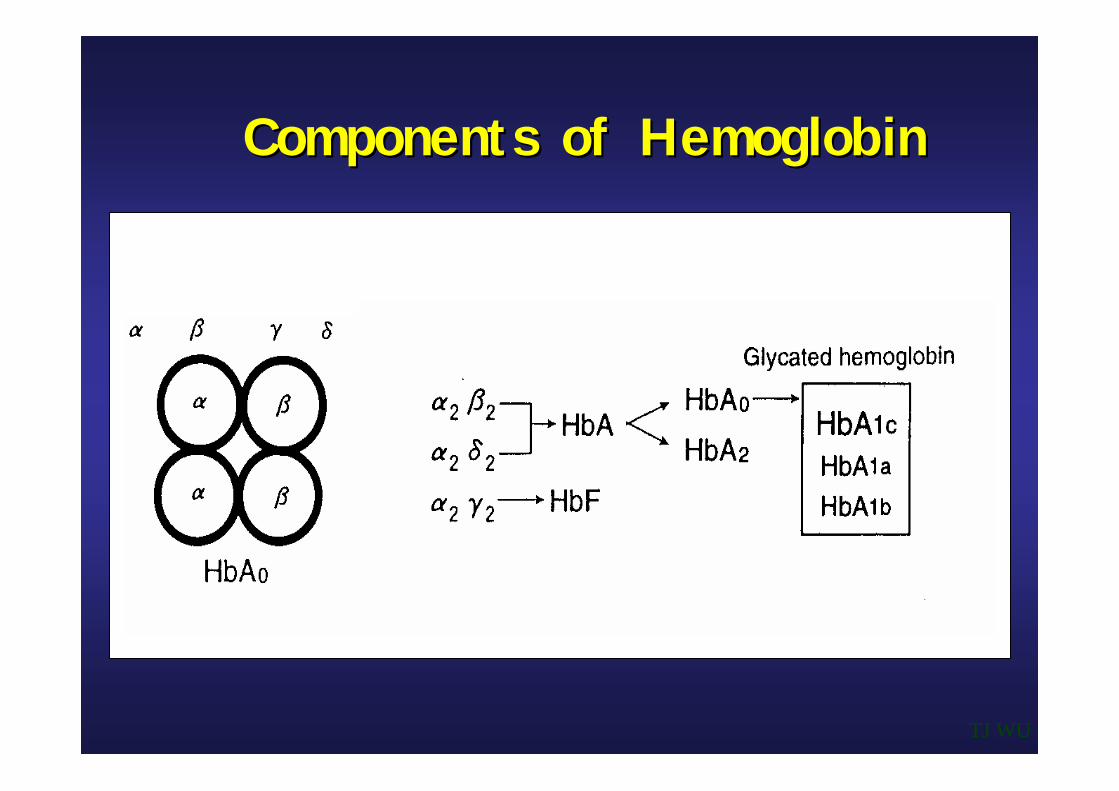
Components of HemoglobinComponents of Hemoglobin
TJ WU

IFCC recommends the name of the assay reflect what is actually being measured: N-[1deoxylfructose-1-yl] hemoglobin beta chain or DOF hemoglobin

Glycated Glycated HbHb Methods in Routine Laboratory Methods in Routine Laboratory UseUse
Kilpatrick ES, et al. Diabet Med 1997;14:819-31.TJ WU
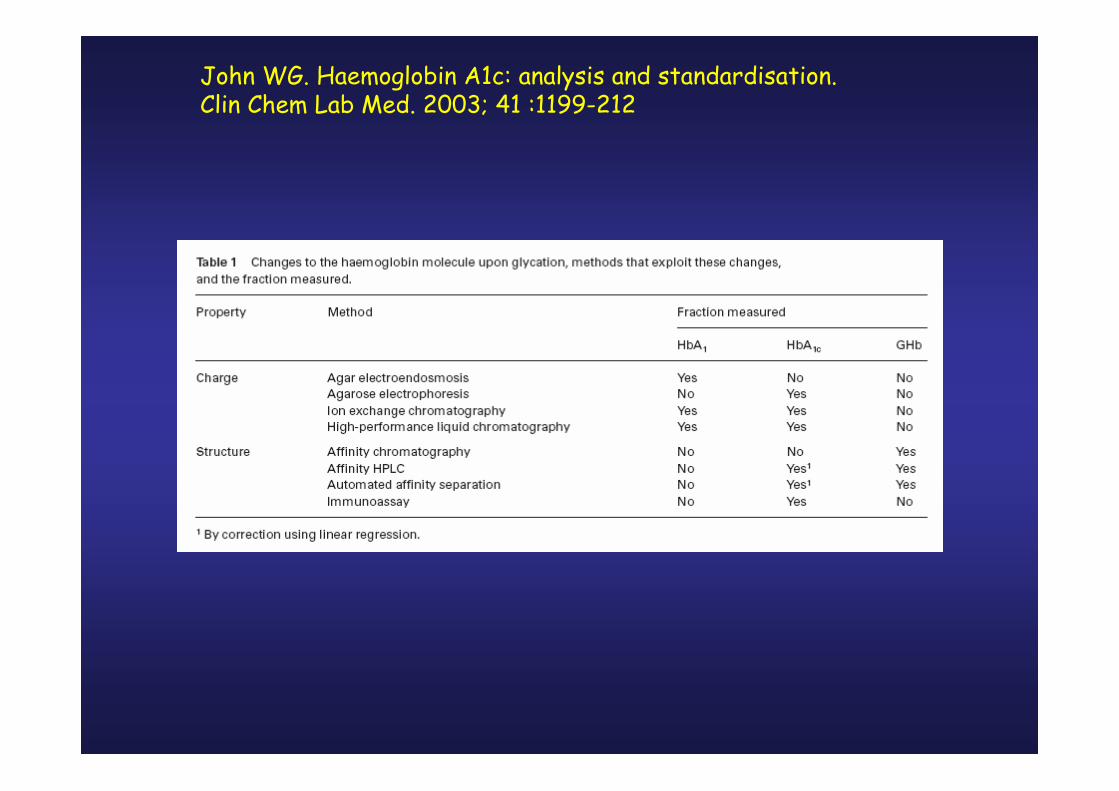
John WG. Haemoglobin A1c: analysis and standardisation. Clin Chem Lab Med. 2003; 41 :1199-212
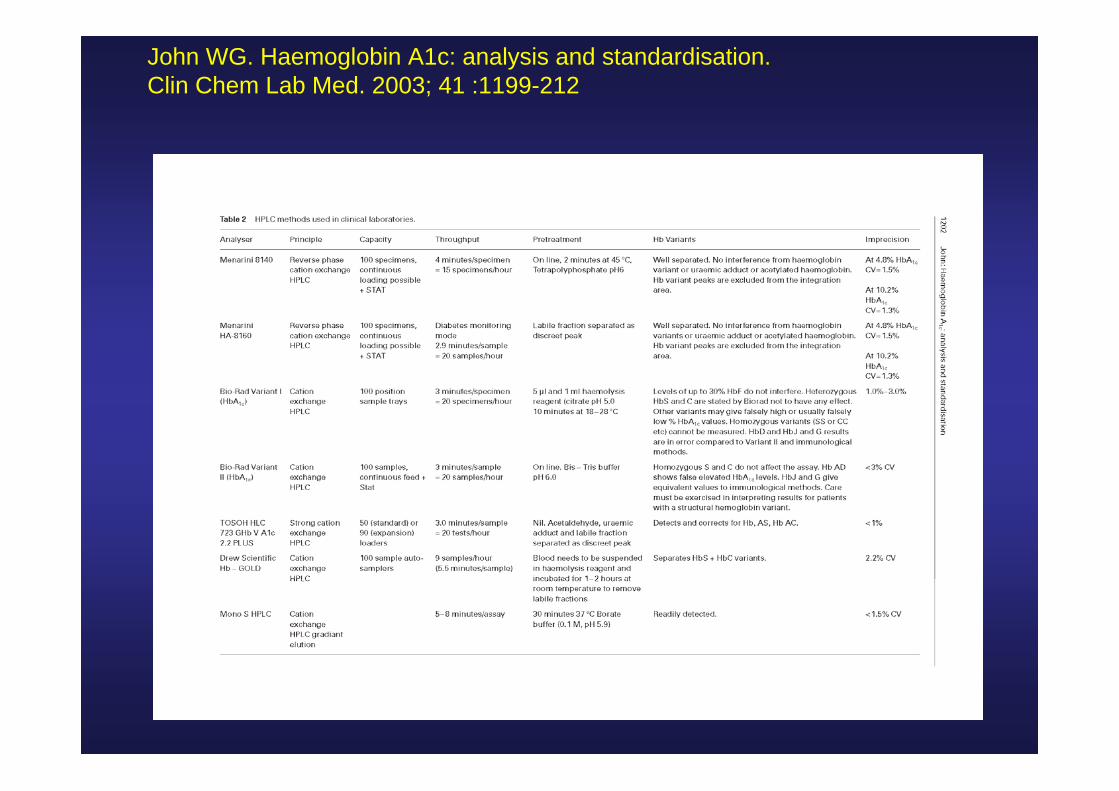
John WG. Haemoglobin A1c: analysis and standardisation. Clin Chem Lab Med. 2003; 41 :1199-212

Separation of Separation of GlycohemoglobinGlycohemoglobin by HPLCby HPLC
TJ WU
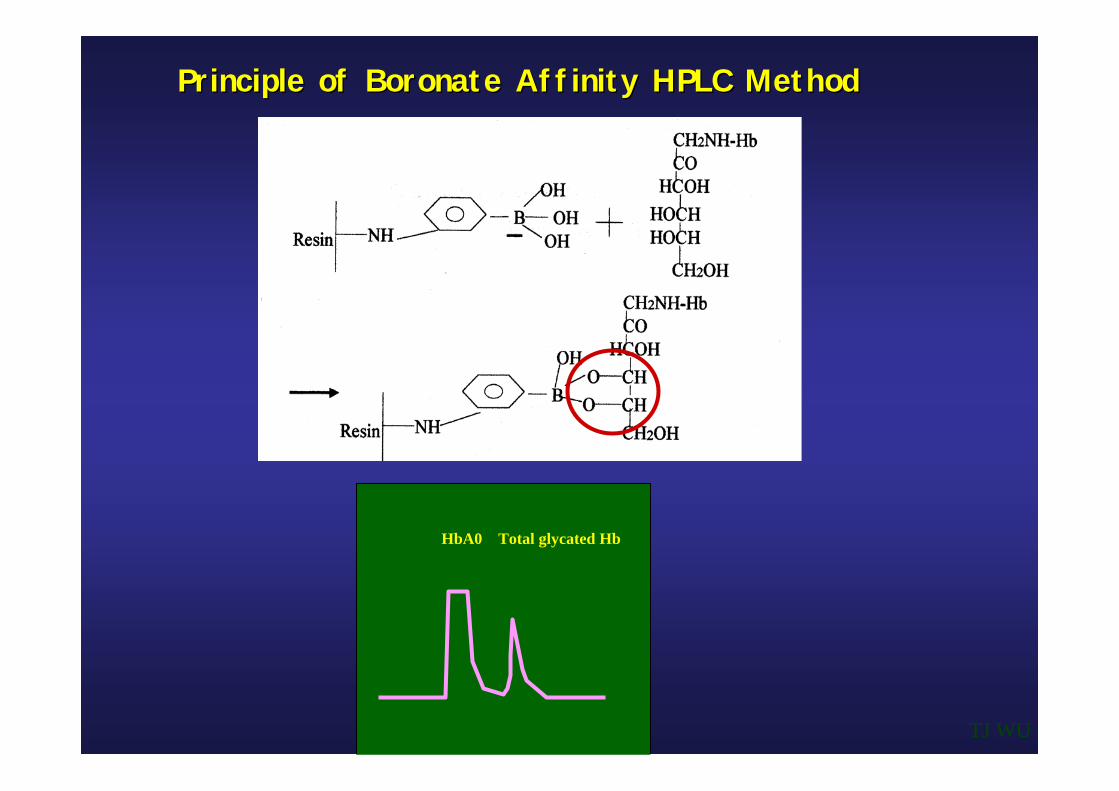
Principle of Principle of BoronateBoronate Affinity HPLC MethodAffinity HPLC Method
TJ WU
HbA0 Total glycated Hb

Latex enhanced Immunoassay method:
The latex enhanced immunoassay for HbA1c is based on interactionsbetween antigen molecules(HbA1c) and HbA1c specific antibodies coatedon latex beads. This cross-link reaction results in changes in the solutionturbidity which is proportional to the amount of the antigen in the samples as depicted in the scheme below
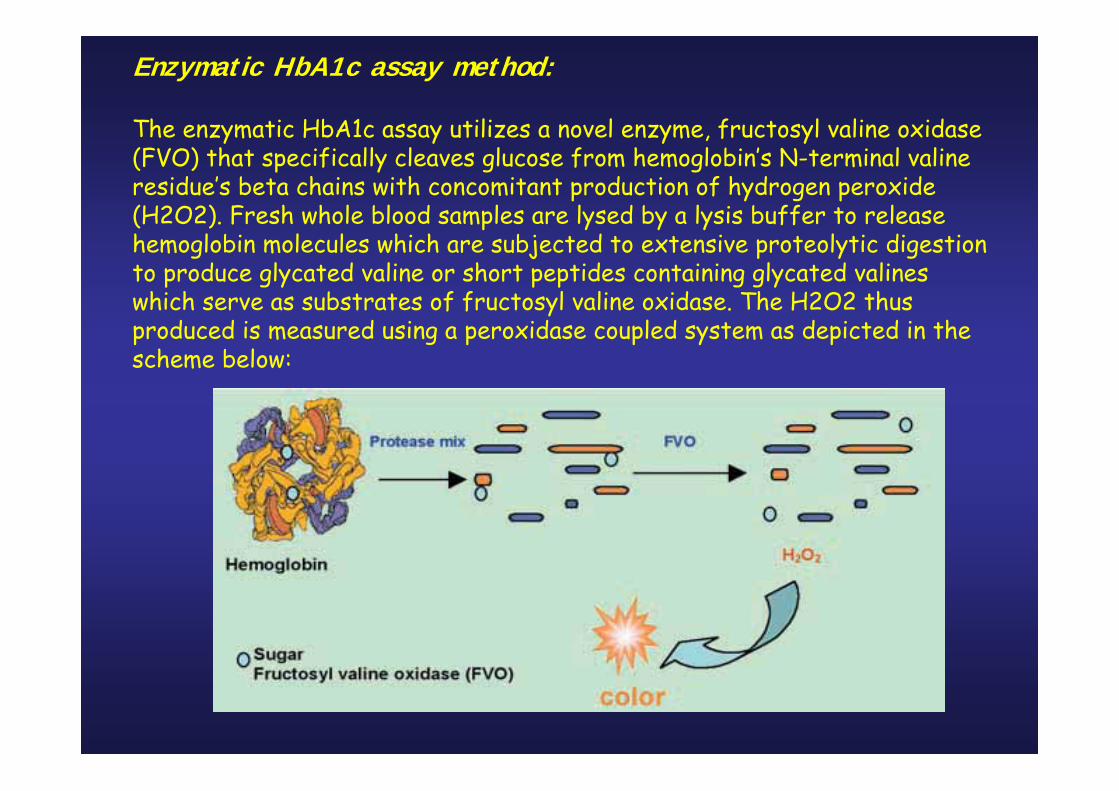
Enzymatic HbA1c assay method:
The enzymatic HbA1c assay utilizes a novel enzyme, fructosyl valine oxidase(FVO) that specifically cleaves glucose from hemoglobin’s N-terminal valineresidue’s beta chains with concomitant production of hydrogen peroxide(H2O2). Fresh whole blood samples are lysed by a lysis buffer to releasehemoglobin molecules which are subjected to extensive proteolytic digestionto produce glycated valine or short peptides containing glycated valineswhich serve as substrates of fructosyl valine oxidase. The H2O2 thusproduced is measured using a peroxidase coupled system as depicted in the scheme below:
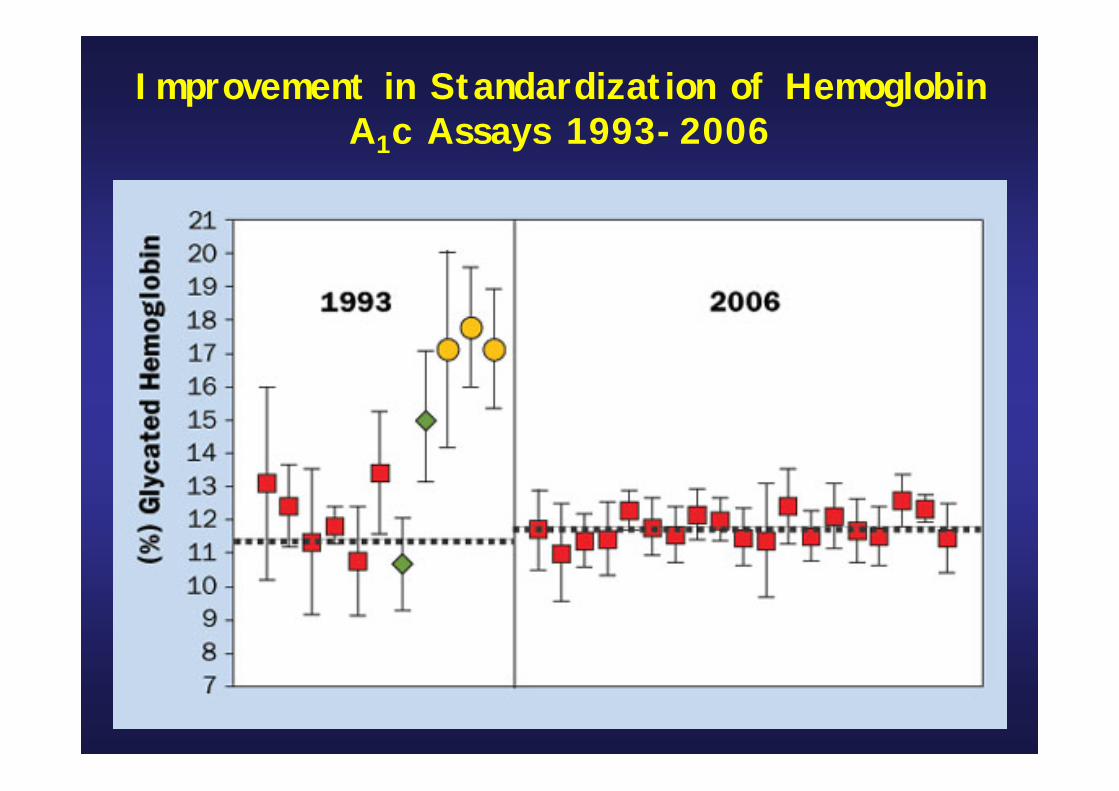
Improvement in Standardization of Hemoglobin A1c Assays 1993-2006


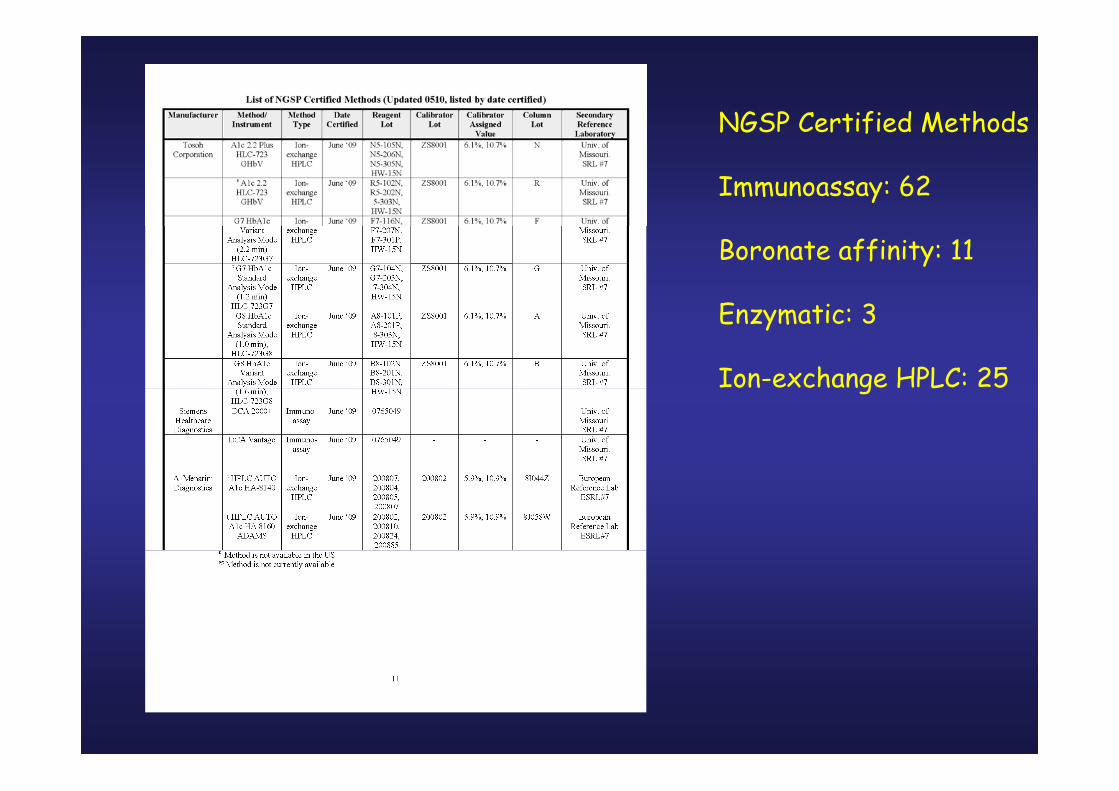
NGSP Certified Methods
Immunoassay: 62
Boronate affinity: 11
Enzymatic: 3
Ion-exchange HPLC: 25


Principali interferenti nella misura della HbA1c
Esistono variazioni post-traduzionali determinate dalegami con altri composti chimici presenti nell’eritrocita dovuti processi di
C a r b a m i l a z i o n e
A c e t i l a z i o n e

Mean Mean GlycohemoglobinGlycohemoglobin Percentages in Percentages in HemolysateHemolysateBefore and After In Vitro Before and After In Vitro
CarbamylationCarbamylation and and AcetylationAcetylation
Basal
5.5
5.7
4.6
3.2
Carbamylated
14.3*
12.9*
4.8
3.0
Acetylated
21.0*
6.7
4.9
3.6
Hemolysate Glycohemoglobin
HPLC
ElectrophoresisAffinity chromatographyEnzymes immunoassay
Methods
TJ WUWeykamp CW, et al. Clin Chem 1993;39:138-42.
Clinical Conditions That Affect Clinical Conditions That Affect GHbGHbMeasurementsMeasurements
• Conditions That Elevate GHb Values– Splenectomy, Thalassemia, HbF*#, Iron
deficiency anemia, Uremia*, Alcoholism*, Hyperbilirubinemia*, Hypertriglyceridemia*, Lead poisoning*, Large dose of salicylates*#, Opiate addiction*
• Conditions That Decrease GHb Values– Hemolytic anemia, Acute blood loss or
phlebotomy, HbC*, HbS*, Pregnancy, vitamin C and E.
*: ion-exchange ; #: electrophoreticmethod
TJ WU

NoYesNoNoTosoh G8
NoYesNoNoTosoh G7
NoYesNoNoTosoh A1c 2.2 Plus
--NoNoSiemens (Bayer) DCA 2000
--NoNoSiemens (Bayer) Advia A1c (new version)
--YesYesSiemens (Bayer) Advia HbA1c (original version)
NoNoNoNoRoche/Hitachi (Tina Quant II)
NoNoNoNoRoche Cobas Integra Gen.2
NoNoNoNoPrimus HPLC (affinity)
NoNoNoNoOrtho-Clinical Vitros
NoNoYesYesOlympus AU system
NoNoNoNoDade Dimension
YesYesNoNoBio-Rad Variant II Turbo A1c
NoNoNoNoBio-Rad Variant II A1c
YesNoNoNoBio-Rad Variant A1c
NoNoNoNoBio-Rad D-10
NoNoNoNoBeckman Synchron System
NoNoYesYesBayer (Metrika) A1cNOW
NoNoNoNoAxis-Shield Afinion
--YesYesAbbott Architect/Aeroset
HbADHbAEHbACHbASMethod
Interference from
HbA1c Assay Inteferences by NGSP

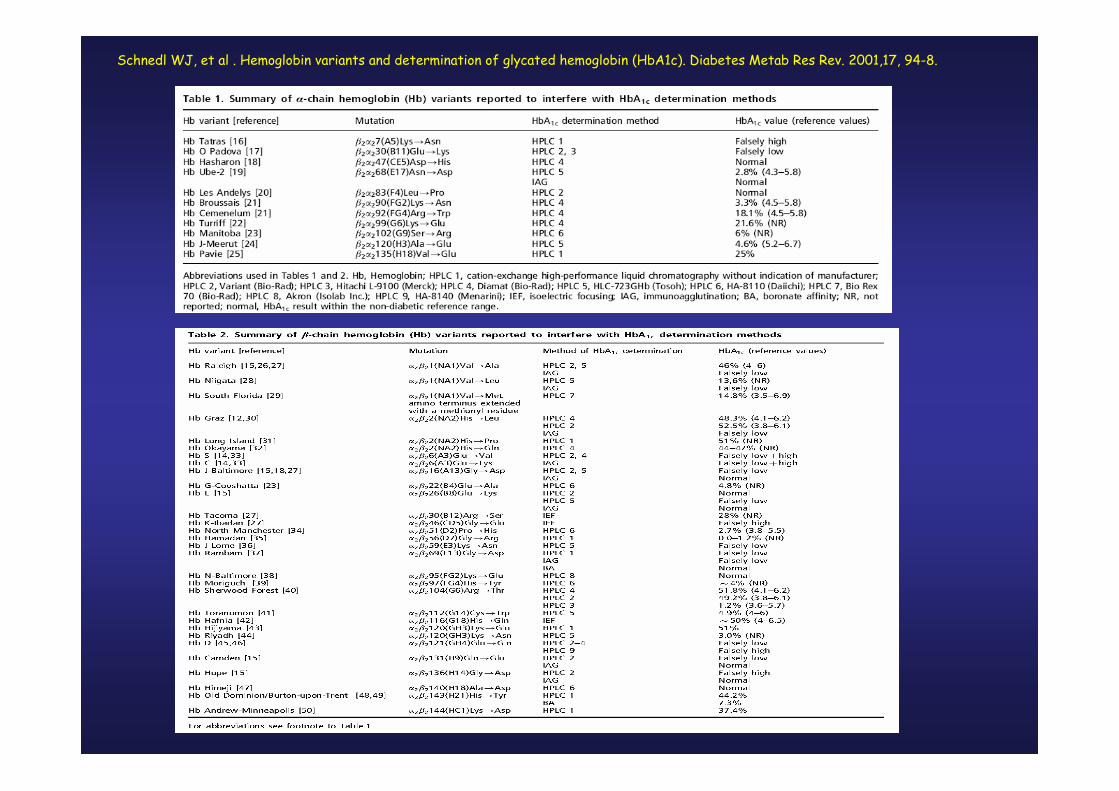
Schnedl WJ, et al . Hemoglobin variants and determination of glycated hemoglobin (HbA1c). Diabetes Metab Res Rev. 2001,17, 94-8.
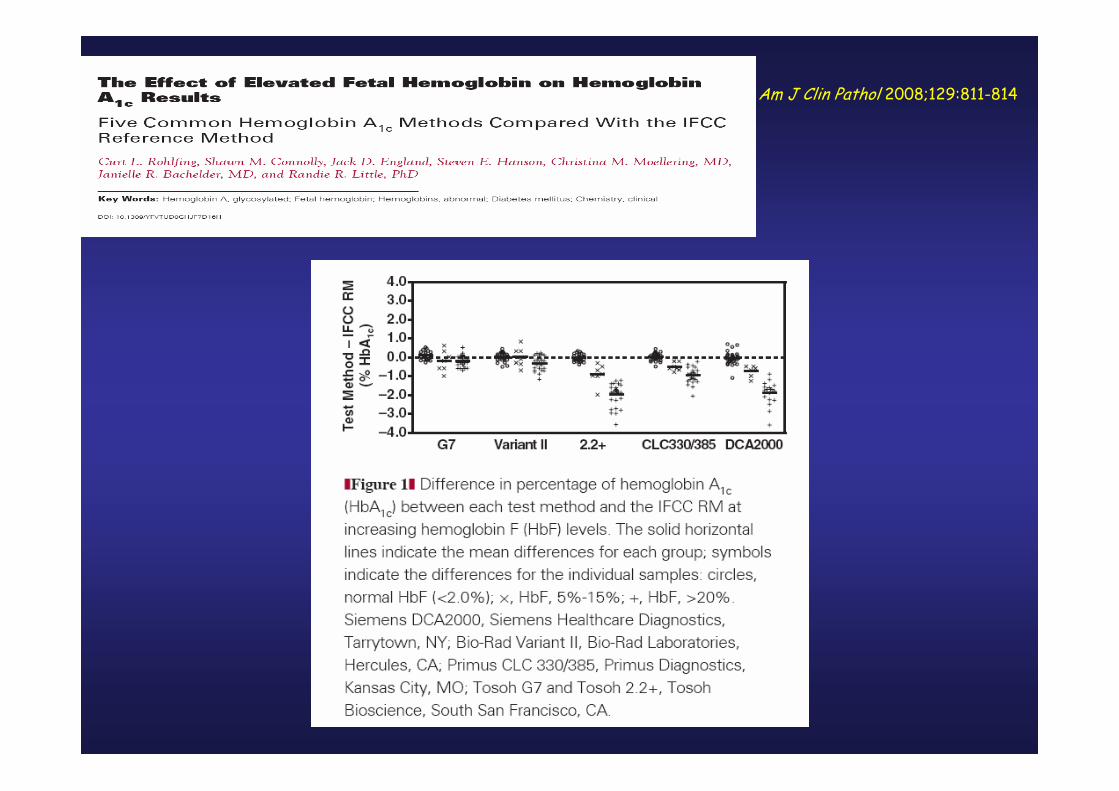
Am J Clin Pathol 2008;129:811-814
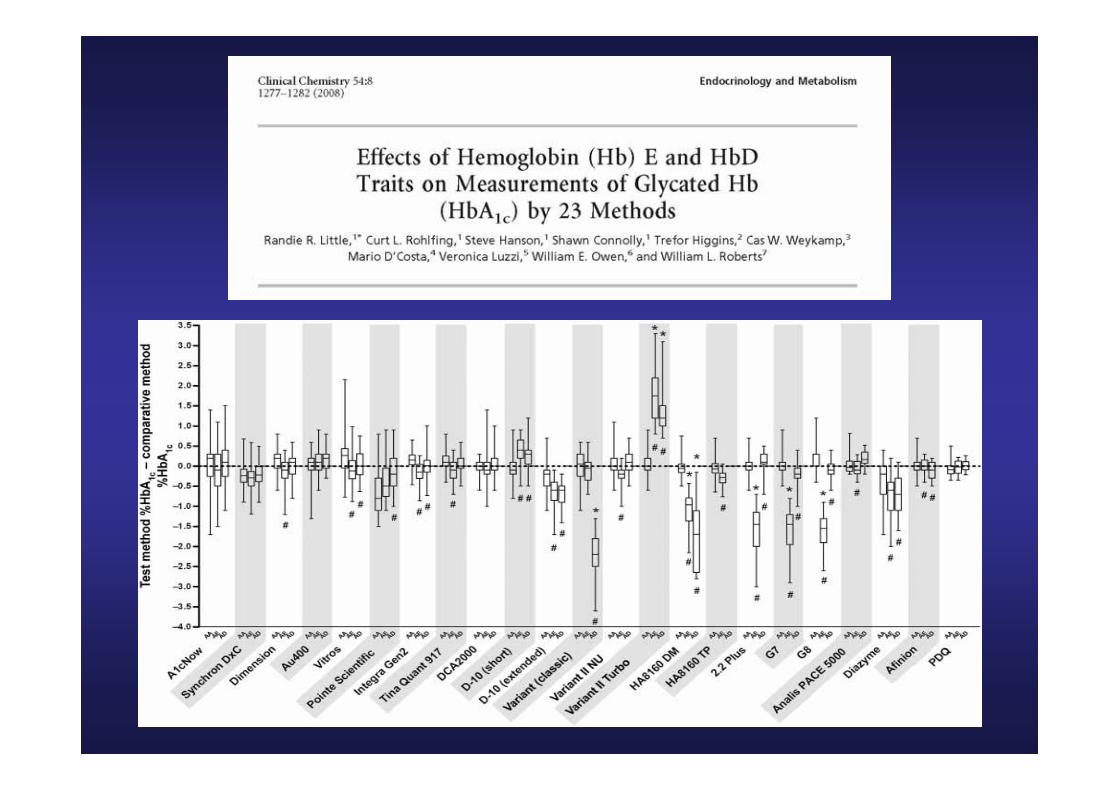
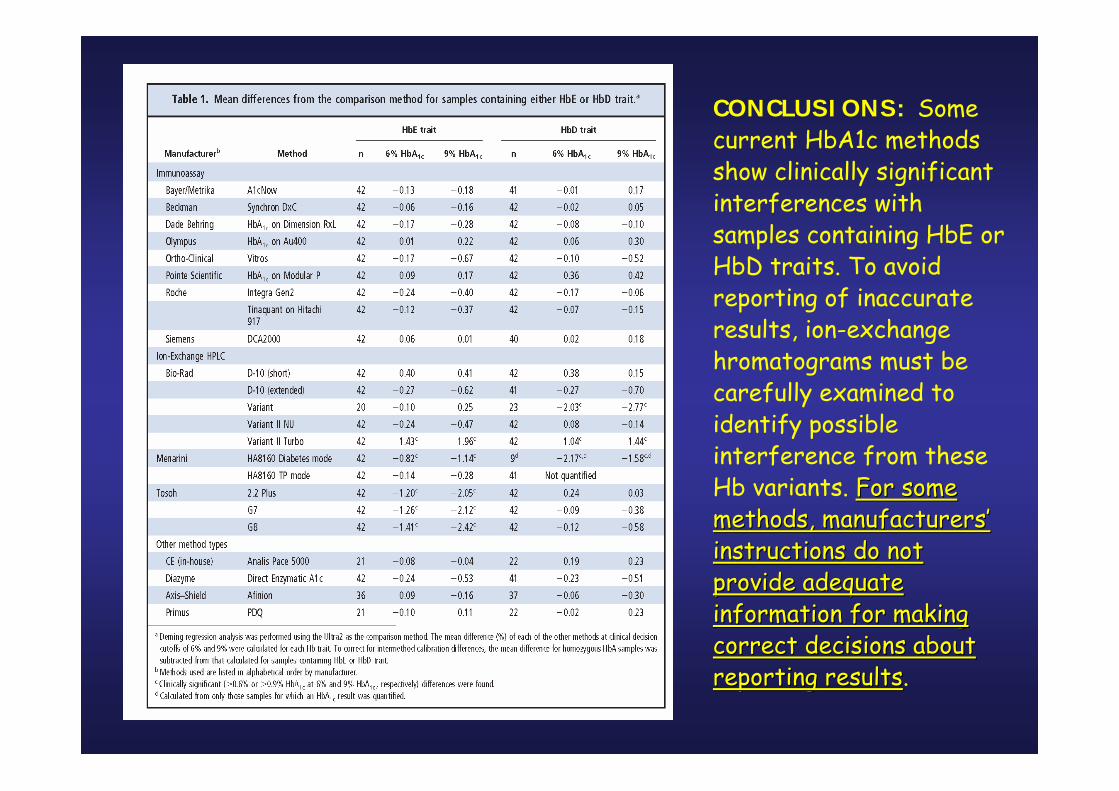
CONCLUSIONS: Some current HbA1c methodsshow clinically significantinterferences withsamples containing HbE or HbD traits. To avoidreporting of inaccurate results, ion-exchangehromatograms must becarefully examined toidentify possibleinterference from theseHb variants. ForFor some some methodsmethods, , manufacturersmanufacturers’’instructionsinstructions do do notnotprovideprovide adequateadequateinformation information forfor makingmakingcorrectcorrect decisionsdecisions aboutaboutreportingreporting resultsresults.
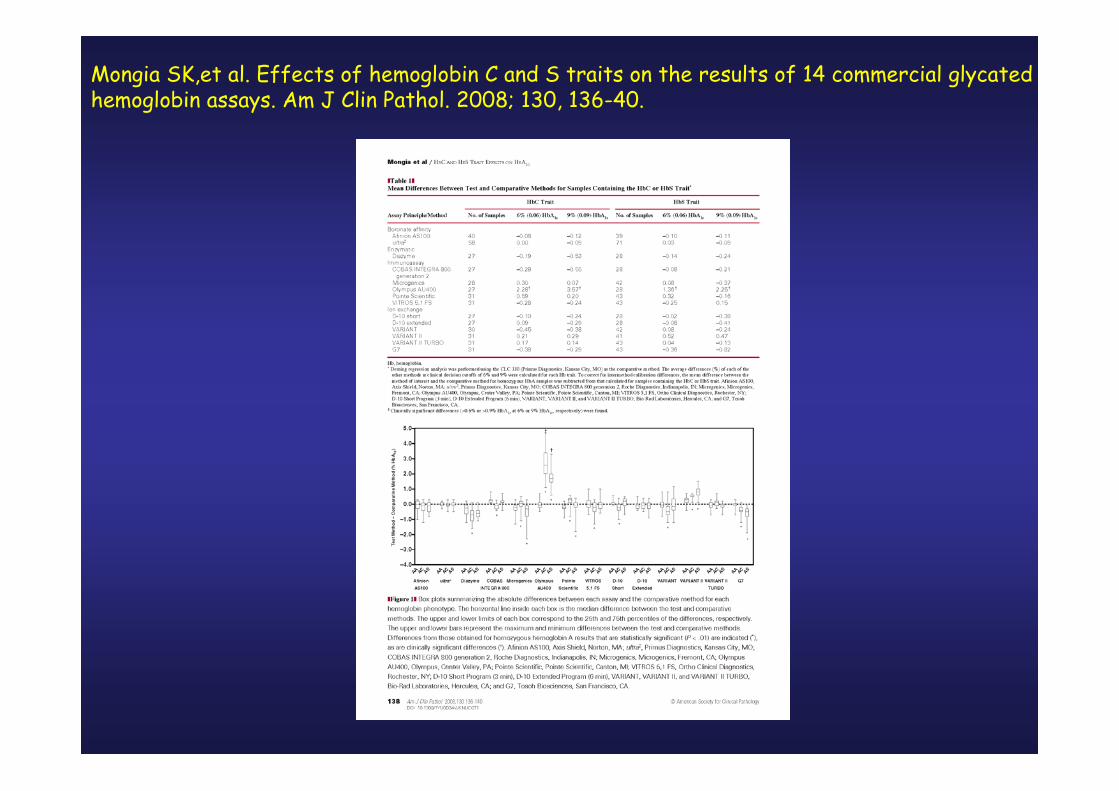
Mongia SK,et al. Effects of hemoglobin C and S traits on the results of 14 commercial glycatedhemoglobin assays. Am J Clin Pathol. 2008; 130, 136-40.



Prospective Diabetes Control and Complications Trial (DCCT)
• mean A1C values during the nine-year study: -7.2 percent with intensive therapy-- 155 mg/dL-9.1 percent with conventional therapy--235 mg/dL
• The DCCT provided conclusive evidence strict glycemic control
a) delay the onset of microvascular complications (primary prevention)
b) low the rate of progression of already present complications (secondary intervention)
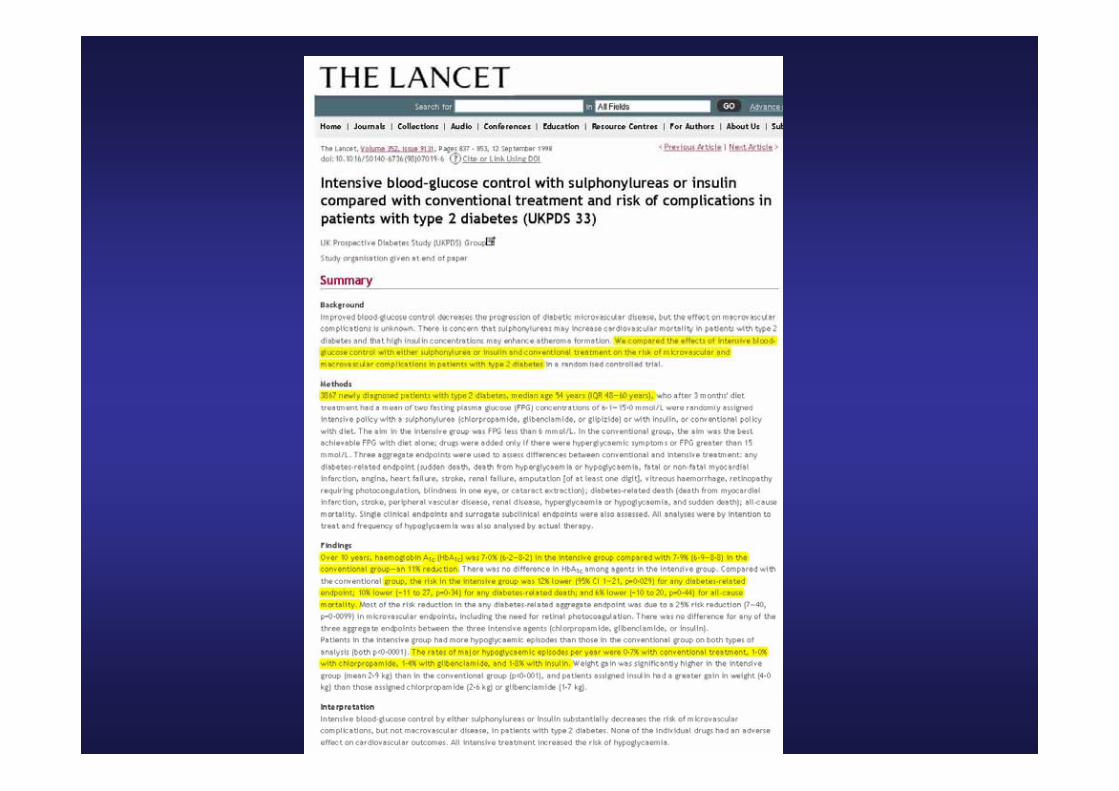

UKPDS Group. Lancet 1998;352:837-853.
UKPDS 10-Year Follow-up Results:Glycemic Control, Weight, and Plasma Insulin
Years from Randomization
0 1 2 3 4 5 6 7 8 9 10 11 12 0 1 2 3 4 5 6 7 8 9 10 11 12
Years from Randomization
Conventional
Conventional
Intensive
IntensiveConventional
Intensive
Intensive
Conventional
Fasting plasma glucose
Med
ian (
mm
ol/
L)
Hemoglobin A1c
Weight Plasma insulin
11
10
9
8
7
60
Med
ian (
%)
9
8
7
60
7.5
5
2.5
0
-2.5
Baseline = 75 kgMea
n C
han
ge
(kg)
40
30
20
10
0
-10
-20Med
ian C
han
ge
(pm
ol/
L)
Baseline = 89 pmol/L
UKPDS Group. Lancet. 1998;352:837-853.
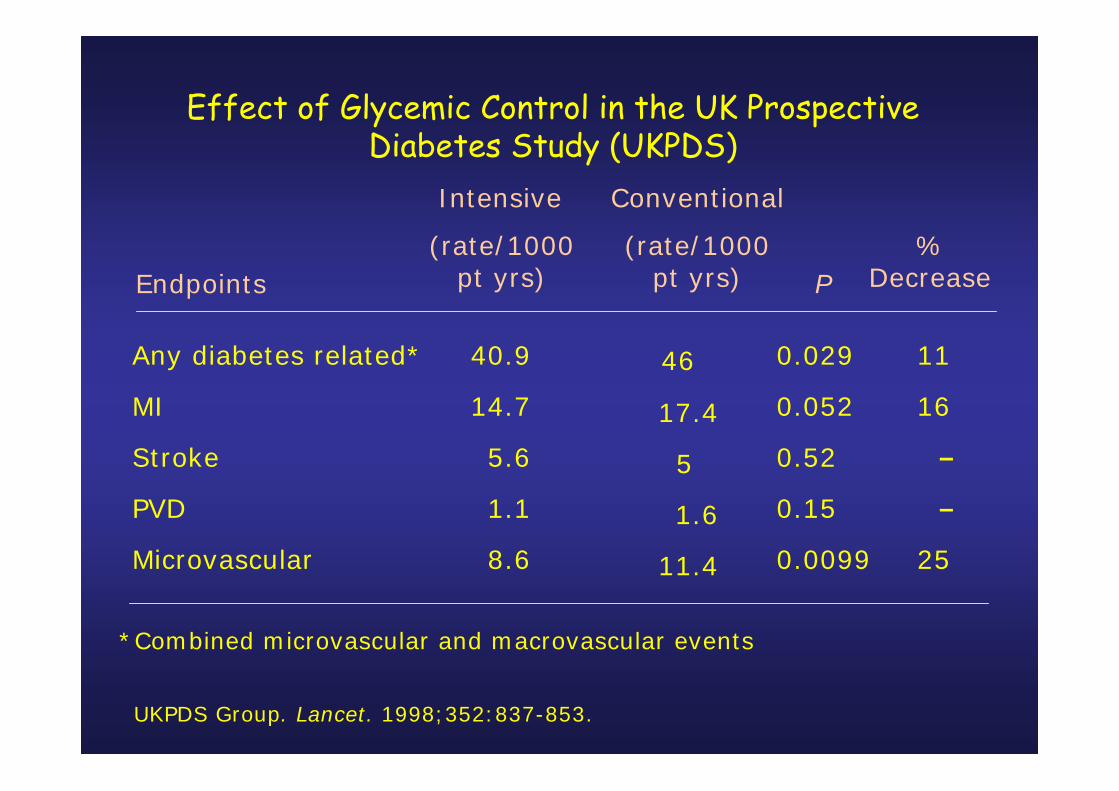
Effect of Glycemic Control in the UK Prospective Diabetes Study (UKPDS)
Any diabetes related*
MI
Stroke
PVD
Microvascular
40.9
14.7
5.6
1.1
8.6
46
17.4
5
1.6
11.4
0.029
0.052
0.52
0.15
0.0099
11
16
–
–
25
(rate/1000 pt yrs)
*Combined microvascular and macrovascular events
Intensive
%Decrease
(rate/1000 pt yrs) P
Conventional
Endpoints
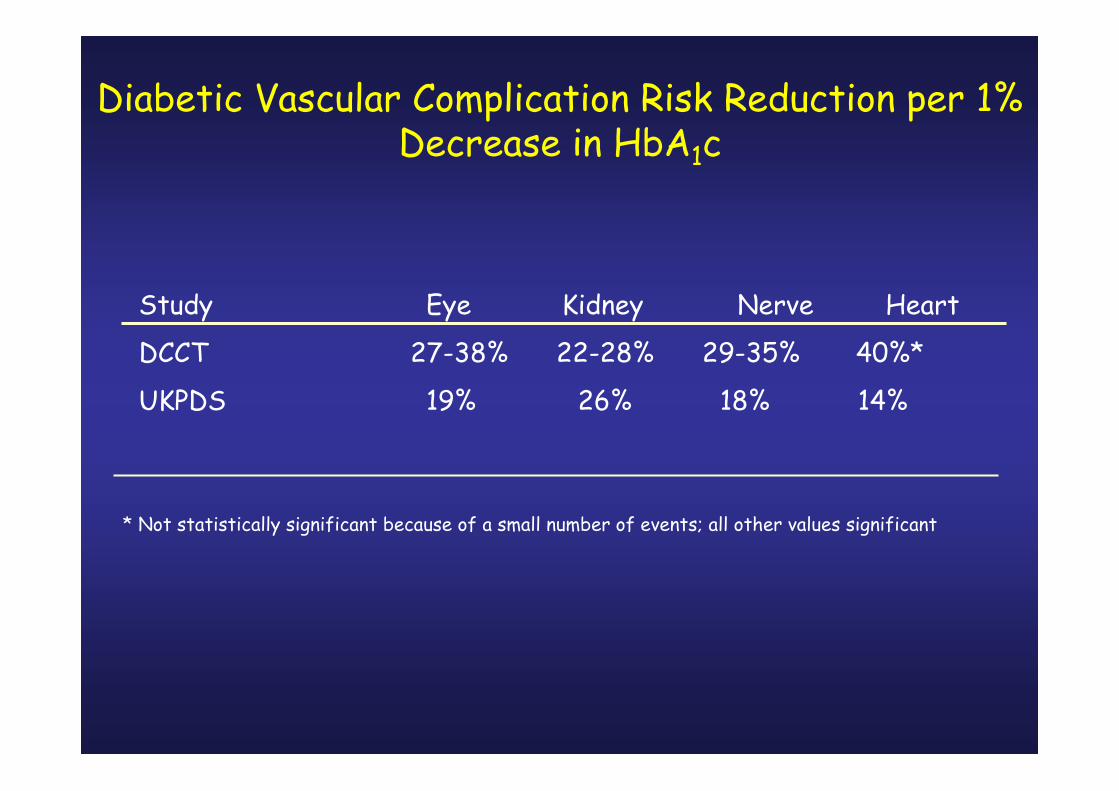
Diabetic Vascular Complication Risk Reduction per 1% Decrease in HbA1c
Study Eye Kidney Nerve Heart
DCCT 27-38% 22-28% 29-35% 40%*
UKPDS 19% 26% 18% 14%
* Not statistically significant because of a small number of events; all other values significant

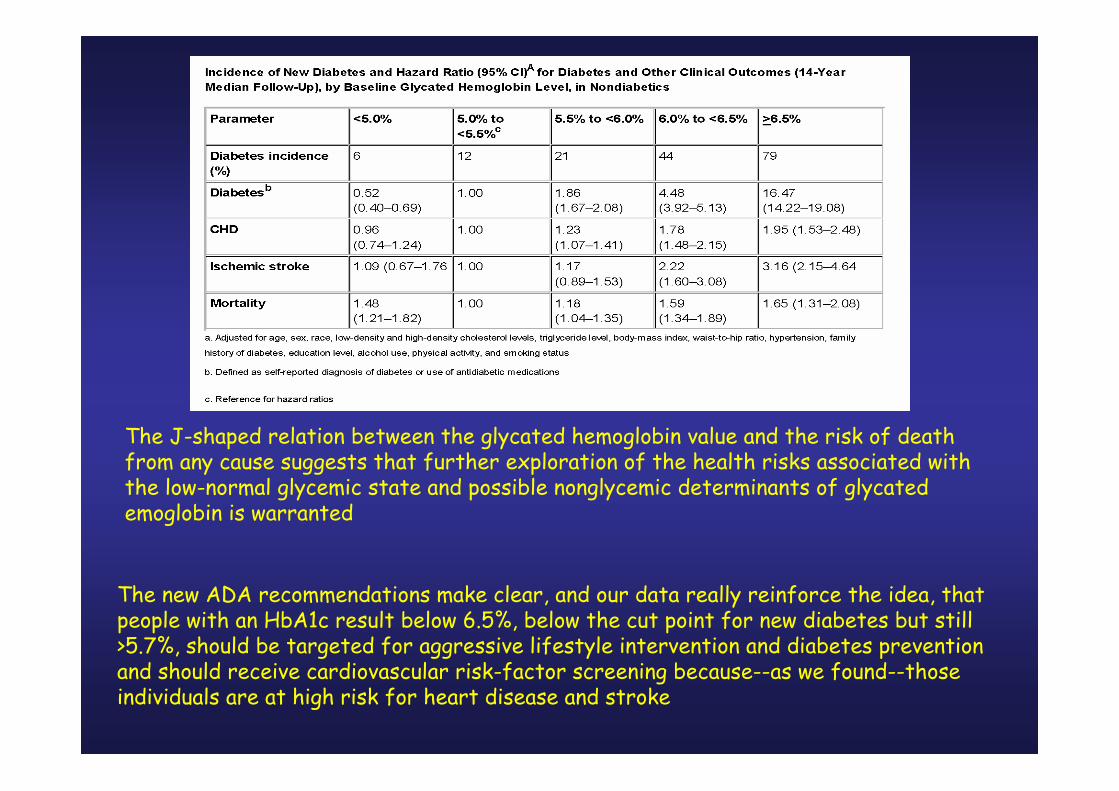
The J-shaped relation between the glycated hemoglobin value and the risk of deathfrom any cause suggests that further exploration of the health risks associated withthe low-normal glycemic state and possible nonglycemic determinants of glycatedemoglobin is warranted
The new ADA recommendations make clear, and our data really reinforce the idea, thatpeople with an HbA1c result below 6.5%, below the cut point for new diabetes but still>5.7%, should be targeted for aggressive lifestyle intervention and diabetes preventionand should receive cardiovascular risk-factor screening because--as we found--thoseindividuals are at high risk for heart disease and stroke





























