Embed Size (px)
Citation preview

1
1
TITLE
Novice identification of melanoma: not quite as straightforward as the ABCDs.
Authors
R Benjamin Aldridge 1a
Matteo Zanotto 2
Lucia Ballerini 2a
Robert B Fisher 2
Jonathan L Rees 1
1 Department of Dermatology, University of Edinburgh, Lauriston Building, Lauriston
Place, Edinburgh, EH3 9HA
2 School of Informatics, University of Edinburgh, Informatics Forum, 10 Crichton Street,
Edinburgh, EH8 9AB
Funding from The Wellcome Trust (Reference 083928/Z/07/Z) and the Foundation for
Skin Research (Edinburgh) . RBAa and LBa supported by Wellcome Trust.
Corresponding author
Professor Jonathan Rees
Department of Dermatology, University of Edinburgh, Level 1 Lauriston Building,
Lauriston Place, Edinburgh, EH3 9HA
[email protected], Tel: 44-(0) 131 536 2041, Fax: 44-(0) 131 229 8769

2
2
ABSTRACT
The “ABCD” mnemonic to assist non-experts’ diagnosis of melanoma is widely
promoted, however, there are good reasons to be sceptical about public education
strategies based on analytical, rule-based approaches (such as ABCD). Evidence
suggests that accurate skin lesion diagnosis is predominately achieved through non-
analytical pattern recognition (via training examples) and not by rule-based algorithms.
If the ABCD are to function as a useful public education tool they must be used reliably
by untrained novices, with low inter-observer and intra-diagnosis variation, but with
maximal inter-diagnosis differences. The 3 subjective properties (the ABCs of the
ABCD) were investigated experimentally: 33 laypersons scored 40 randomly selected
lesions (10 lesions x 4 diagnoses: Benign naevi, Dysplastic naevi, Melanomas,
Seborrhoeic Keratoses) for the 3 properties on Visual-Analogue-Scales. Our results
(n=3960) suggest that novices cannot use the ABCs to reliably discern benign from
malignant lesions.
Keywords
ABCD, Non-analytical reasoning, Pattern recognition, Skin cancer, Melanoma,
Dermatology diagnosis
Principal Author
Professor Jonathan Rees
Department of Dermatology, University of Edinburgh, Level 1 Lauriston Building,
Lauriston Place, Edinburgh, EH3 9HA
[email protected], Tel: 44-(0) 131 536 2041, Fax: 44-(0) 131 229 8769

3
3
INTRODUCTION
The “ABCD” rule to aid in the diagnosis of early malignant melanoma has recently
celebrated its 25th Anniversary (1). This mnemonic was introduced in 1985 to aid non-
experts’ macroscopic diagnosis of pigmented lesions and over the years it has been
widely promoted in an attempt to facilitate the earlier detection of melanomas (2). In
the twenty-five years since its inception the use of the ABCD has transitioned from
assisting non-expert physicians’ diagnosis, through educating the public in intensive
clinician led programs, to now being used at the heart of most general public education
strategies; with the criteria described on the public websites of the American Academy
of Dermatology (AAD) (3), British Association of Dermatologists (4), Australasian
College of Dermatologists (5) and European Academy of Dermatology and Venereology
(6). Although the fundamental four-part ABCD mnemonic has received widespread
adoption, it is surprising that there has been little apparent validation of its utility as a
general public education strategy.
Given that lay individuals first identify the majority of melanomas and are also
responsible for the largest proportion of the delays in its diagnosis, reliable and
accurate information to assist them in early detection is essential (7-10). Recently the
importance of accurate patient information has been further highlighted as, thus far, the
numerous strategies initiated to improve screening and the early detection of melanoma
have not resulted in a substantial reduction in the proportion of tumours with
prognostically unfavourable thickness (11). There is now mounting evidence leading us
to question the use of the ABCD rule as a general public education strategy (12, 13).
The majority of studies that are cited as providing evidence for the mnemonics’

4
4
adoption have either involved clinician-performed assessments (14-18) or intensive lay
education (19, 20), and, as we detail below, there are methodological limitations with
extrapolating the findings from these studies to general public health promotion - the
roles of experience and prior examples.
The role of experience
Since the late 1980s the cognitive processes involved in dermatological diagnosis have
been under investigation, most notably in the laboratory of Geoff Norman and
colleagues (21-25). At the risk of some simplification, the processes involved in
diagnosis can be viewed as being either explicit and based on conscious analytical
reasoning or, alternatively, as being implicit and holistic, and hidden from the
conscious view of the diagnostician. Dermatologists appear to predominately use the
latter non-analytical reasoning, derived through experience of prior examples to
identify skin lesions. This overall pattern recognition cannot be unlearnt and thus has a
carry-over effect on any attempts at analytical rule application (26-30). In addition,
study designs where experts are asked to explain their diagnoses inherently over-
emphasize algorithmic reasoning by promoting intentional rather than incidental
analytical processing (31). It has even been suggested that experienced clinicians make
a diagnosis intuitively then alter their analytical assessment to fit in with their
preconceptions about the relation between these features (such as the ABCD) and the
diagnosis (such as melanoma) (31, 32). Certainly, the only prospective study of
dermatologists’ recognition patterns, confirmed that whilst analytical pattern
recognition (the ABCD rules) could be used to predict malignancy, it was not actually
5
5
how dermatologists arrived at the correct diagnosis; instead the experts seemed to use
overall or differential pattern recognition (“Ugly duckling sign (33)”) (23).
The role of prior examples
The exact number of prior examples that are required to significantly alter analytical
assessments is unknown, but we do know that these carry-over effects do not only
apply to seasoned clinicians; novices have been shown to exhibit this bias with only a
few prior examples (27, 28, 34). We do not fully understand how novices naturally
visually assess skin lesions, but unless it is significantly different to the rest of human
visual perception it is unlikely to be by analytical methods. If, as is likely, overall-
pattern recognition plays even a small role, the biasing effect of prior examples needs
to be controlled for when assessing the analytical ABCD criteria. In the few studies
where intensive ABCD education has been demonstrated to have a beneficial effect on
lay individuals, overall pattern recognition was not controlled for (19, 20). It is therefore
unclear how much of the positive effect can be attributed to the novices’ ability to
discriminate the true analytical ABCD criteria rather than their ability to use overall-
pattern recognition ‘learnt’ from the example lesions used to demonstrate the analytical
criteria during their patient education. Thus far the only randomized control trial testing
the ABCD in lay hands showed that it decreased diagnostic accuracy and was not as
effective as a pattern recognition education strategy (12).
In this particular context any screening or diagnostic tool would ideally have the
following three criteria: Inter-observer variability should be minimal; variation within a
diagnostic class should be small; and the inter-diagnosis differences should be
significant. In the present study we set out examine these three criteria experimentally

6
6
assessing the three subjective analytical properties (the ABCs) of the ABCD rule.

7
7
METHODS
Study Image selection
40 digital images of pigmented skin lesions were randomly selected from 878 relevant
images in the University of Edinburgh Department of Dermatology’s image database.
The Department's image library (now comprising over 3500 images) has been
prospectively collected for ongoing Dermato-informatics research investigating semi-
automated diagnostic systems and non-expert education. The 40 images selected for
this experiment were stratified so that there were 10 images from each of the following
4 diagnostic classes: benign naevi, dysplastic naevi (defined as lesions with histological
atypia), melanomas and seborrheic keratoses. All the images had been collected using
the same controlled fixed distance photographic setup; Canon (Canon, Japan) EOS
350D 8.1MP cameras, Sigma (SIGMA, Japan) 70mm f2.8 macro lens and Sigma EM-
140 DG Ring Flash at a distance of 50cms. The lesions were cropped from the original
digital photograph, each to the same resolution (600x450 pixels) and displayed in a 1:1
ratio (approximately equivalent to 7 times magnification from the original 50cm
capturing distance) in the custom built experimental software.
Software design & implementation
A purpose built program was created to allow the 3 subjective criteria of the ABCD rule
(Asymmetry, Border Irregularity and Colour Uniformity) to be tested remotely over the
Internet, to limit any investigator-related interaction bias. Diameter was felt not to be
suitable for assessment as the images were magnified and thus would have required the
placement of a relative 6mm marking scale next to each lesion before asking each

8
8
participant to comment which was longer; the lesion or the measuring scale, which
would not have been instructive. The program was written in JavaScript and PHP, and
after entering their demographics the participants were given a set of instructions stating
how to use the ABC criteria and the software. The instructions were based on the verbal
descriptors of the ABC criteria taken from the website of the AAD (3). After confirming
that they had read and understood the instructions the subjects assessed each of the 40
images in turn for Asymmetry, Border Irregularity and Colour Uniformity on a 10-point
visual analogue scale (VAS). A screen shot of the software can be seen in Figure 1. At
any stage the subjects could click on a “Help” button to redisplay the instructions and
verbal descriptors of the ABC.
To minimize any lead bias or fatigue effect, the software was programmed to
randomize the order in which the subjects undertook the 40-lesion assessment, so that
it was different for each participant. In addition to the verbal descriptions of the 3
properties assessed, to further reduce inter-rater differences visual anchor points were
integrated into the software at the mid point and either ends of the rating scale. These
anchor points were taken from the ABCDE patient guidelines on the SkinCancerNet
“Melanoma: What it Looks Like” webpage produced in conjunction with the AAD (35).
As we were interested in the lay public’s ability to discriminate analytically the three
properties and not their ability to use their innate non-analytical reasoning to match or
distinguish from real-life examples, only the caricatured diagrams from the
SkinCancerNet website were used as the high-end anchor points, rather than example
pictures of melanomas (Figure 2). The mid and low-end anchor points were computer
generated to complete the VAS.

9
9
Subjects
An open email request containing the URL link to the study was distributed to MSc
students of the University of Edinburgh’s School of Informatics, inviting them to
personally undertake the study and forward on to non-medical acquaintances who also
might be willing to participate. 33 lay subjects agreed to participate without
remuneration. Sex distribution was split with 21 males and 12 females (64% male).
Mean age was 34 years old (Range 17-62). None of the subjects had a personal history
of skin cancer.
Statistics
The subjects’ responses were automatically recorded by the program then exported into
‘R for MacOS’ for graphing and statistical analysis (36).
Ethics
NHS Lothian research ethics committee granted permission for the collection and use
of the images, and additional permission for the use of students in this research was
granted through the University of Edinburgh’s “Committee for the use of student
volunteers”.

10
10
RESULTS
The full results of all 3960 analytical VAS scores attributed in the study (33 subjects x
40 lesions x 3 ‘ABC’ properties) are graphically displayed in Figures 3a-c, with each
property presented in a separate plot. At first glance these plots may seem complicated
but they have the virtue that every data-point from the experiment is presented and the
variability in scoring can be instinctively assessed. In explanation: each horizontal
coloured bar represents an individual subject’s score for a specific lesion, with each of
the 40 lesions displayed in individual columns across the X-axis. These 40 lesions’
columns are grouped into different colours according to their diagnostic classes
(Green= the 10 Benign Naevi, Orange= the 10 Dysplastic Naevi, Red= the 10
Melanomas, Blue= the 10 Seborrheic Keratoses). The overall median score for each
diagnostic class is demonstrated by the large horizontal black bar, straddling each of
the 4 coloured series of 10 columns.
The inter-person variability in assessing each of the 3 ABC properties for any single
lesion is represented by a single column’s vertical spread across the Y-axis. Within a
specific diagnostic class the variability in scores is demonstrated by the differences in
vertical spread between the 10 uniform coloured columns. The variability between the
4 diagnostic classes is appreciated by the differences in the overall distributions
between the 4 coloured groups and further enforced by the differences in their median
scores indicated by the horizontal black bars.
The results are further summarised in Table 1.

11
11
Whilst it is possible to appreciate the small, albeit significant (Kruskal
Wallis=P<0.0001), difference between the 4 diagnostic groups’ scores what is far more
striking is the substantial spread in the scores attributed to the same lesion by the 33
subjects and the further variation in scoring between the 10 lesions within the same
diagnostic class for all 3 of the subjective ABC properties. Additional data analysis
demonstrates that a similar substantial variation exists within the 10 scores that each
individual attributed to the lesions within the same diagnostic class (data not shown).
The inter-person and intra-class variations can be better appreciated by specific
examples (see Figure 4, which is an enlarged view of the highlighted section of Figure
3b). In Figure 4 it can be seen that lesion 3 (blue arrow/highlights) which had the
largest inter-person variation (IQR= 4.86) of the 10 lesions within the melanoma class
had a range of ‘border irregularity’ scores attributed by the 33 subjects from 0.7 to 10
with a median score of 6.6, and lesion 7 (cyan arrow/highlights), which had the least
inter-person variance (IQR=1.93), had a range from 0 to 5.5 with a median score of
1.3.

12
12
DISCUSSION
Our principal motivation for the current work was the observation that the original
rationale and justification for the ABCD approach had slipped from the primary target
group of physicians to the lay public, with little supporting evidence to justify this
transfer. In the absence of empirical evidence of effectiveness, there are at least two
theoretical reasons to be suspicious of this approach. First, there is an increasing body
of evidence that experts are not necessarily able to explicitly state the basis of their own
expertise in a way that is simply transferable (31, 32). Second, that previous testing of
ABCD had not controlled for prior exposure (14-20), meaning that prior accounts of the
utility of the ABCD may have reflected prior experience and knowledge rather than the
implementation and use of the criteria themselves (26-30).
Other relevant considerations are that whereas experts may be able to use the criteria
on appropriate subclasses of lesions (i.e. melanocytic nevi and melanomas), available
evidence suggests that distinguishing primary melanocytic lesions from mimics (such as
seborrhoeic keratoses) requires considerable expertise (37-39). Finally, the only large
scale RCT in this area comparing ABCD approach with those based on pattern
recognition provided little support for the use of the ABCD criteria (12).
The approach we took was an experimental one attempting to delineate the
characteristics of the ABCD rules on a test series of lesions. Our rationale was that for
the ABCD system to be capable of guiding diagnosis, it would have to have certain
statistical properties: different diagnostic groups needed to score differently, and
variance between persons for the same lesion and within diagnostic groups needed to
be small. Within the limits of our test situation and the images randomly chosen it is
13
13
self evident that these criteria were not met. Different people judged the same lesion
very differently, and although the medians of different diagnostic groups differed, the
overlap was considerable. Looking at Figure 3, it is difficult to imagine being able to
choose any criteria based on ABCs that would usefully discriminate suspicious from
banal lesions.
There are limitations to our approach. Our subjects were not chosen at random, and
were highly educated, computer literate, and likely above average at abstract and
analytical reasoning. We doubt that this is a reason to doubt the generalisability of our
conclusions. Second, we included not just primary melanocytic lesions but mimics
such as seborrhoeic keratoses. The justification for this is simply that non-experts and
many physicians are not able to reliably distinguish between these classes of lesions. In
practice the ABCD criteria get applied (incorrectly) to various diagnostic classes: we
needed to account for this. Third, as the subjects undertook the experimental task
remotely over the Internet we were unable to assess the ‘effort’ they applied to their
scoring. However, because we randomized the order in which each subject assessed
the 40 lesions any fatigue effect would have been minimized. Indeed, close inspection
of the data demonstrates that whilst there is substantial overlap in scoring between (and
within) the diagnostic groups, the subjects’ scoring was not random; individual lesions
each had (to varying degrees) distinct scoring patterns.
We cannot say whether, if subjects had undergone intense education in the use of the
ABCD approach, the results might have been different. In practice, however, the
promulgation of the ABCD criteria via web sites and patient leaflets provides little
opportunity for such intense education. We also suggest that previous studies of the

14
14
ABCD approach have been methodologically compromised because of failure to
control for prior exposure during the teaching phase. Training persons in the use of the
ABCD inevitably means exposure to test images: during this, albeit minimal exposure,
pattern recognition skills will develop, and it is a mistake to believe that any change in
performance pre and post test is due to the ABCD system rather than other learning. To
make any other conclusion requires a degree of experimental control that has been
lacking in prior work.
We also acknowledge the multiple modifications to the basic ABCD mnemonic that
have been suggested over the years to “improve” its functionality (40-47), and accept it
is now commonplace to use the ABCDE criteria (although we note there is a wide
variety of ‘E’s suggested; evolving, enlarging, elevated, erythema, expert). However, in
light of the fact that there is now further evidence that untrained novices cannot use the
analytical ABC criteria effectively, should the public education message not be
simplified to only include Evolving (i.e. Change). Such a simplification has previously
been suggested by Weinstock (47, 48) and has independently been found to be the
most important predictor of melanoma in patient observed features (13).
Finally, given the changing epidemiology of malignant melanoma and the importance
of early presentation by patients and early diagnosis by physicians, our criticisms of the
ABCD approach are not meant to disparage attempts to develop alternative strategies.
In this respect we note the work of Grob who has used approaches based on fostering
pattern recognition skills for laypersons (12). Our own work has also suggested that use
of images and a structured database may enhance diagnostic skills of laypersons,
although in the context of malignant melanoma, such systems need far more testing

15
15
before being promoted as being clinically useful (49, 50).
16
16
ACKNOWLEDGMENTS
The work was supported by The Wellcome Trust (Reference 083928/Z/07/Z) and the
Foundation for Skin Research (Edinburgh). We are also grateful to the advice and
assistance given by Karen Roberston and Yvonne Bisset (Department of Dermatology,
University of Edinburgh) regarding the photographic capture and preparation of the
digital images. We also recognize the contribution of Nikolaos Laskaris (School of
Informatics, University of Edinburgh) who undertook some of the preliminary
programming as part of his MSc Thesis (51).

17
17
REFERENCES
1. Rigel DS, Russak J, Friedman R. The Evolution of Melanoma Diagnosis: 25 Years
Beyond the ABCDs. CA: A Cancer Journal for Clinicians. 2010;60:301-316.
2. Friedman RJ, Rigel DS, Kopf AW. Early detection of malignant melanoma: the role
of physician examination and self-examination of the skin. CA: A Cancer Journal
for Clinicians. 1985;35:130-151.
3. American Academy of Dermatology. ABCDs of Melanoma Detection [Internet].
2010 [Accessed 15/11/2010]. Available from:
http://www.aad.org/public/exams/abcde.html.
4. British Association of Dermatologists. Sun Awareness - mole checking [Internet].
2010 [Accessed 15/11/2010]. Available from:
http://www.bad.org.uk/site/719/default.aspx.
5. Australasian College of Dermatologists. A-Z of Skin- Moles & Melanoma
[Internet]. 2010 [Accessed 15/11/2010]. Available from:
http://www.dermcoll.asn.au/public/a-z_of_skin-moles_melanoma.asp.
6. European Academy of Dermatology and Venereology. Moles and Malignant
Melanoma Patient Information Leaflet. [Internet]. 2010 [Accessed 15/11/2010].
Available from: http://www.eadv.org/patient-corner/leaflets/eadv-leaflets/moles-
and-malignant-melanoma-patient-information-leaflet.
7. Koh HK, Miller DR, Geller AC, Clapp RW, Mercer MB, Lew RA. Who discovers
melanoma? Patterns from a population-based survey. Journal of the American
Academy of Dermatology. 1992;26:914-919.

18
18
8. Temoshok L, DiClemente RJ, Sweet DM, Blois MS, Sagebiel RW. Factors related to
patient delay in seeking medical attention for cutaneous malignant melanoma.
Cancer. 1984;54:3048-3053.
9. Richard MA, Grob JJ, Avril MF et al. Delays in diagnosis and melanoma prognosis
(I): the role of patients. Int J Cancer. 2000;89:271-279.
10. Richard MA, Grob JJ, Avril MF et al. Delays in diagnosis and melanoma prognosis
(II): the role of doctors. Int J Cancer. 2000;89:280-285.
11. Criscione VD, Weinstock MA. Melanoma thickness trends in the United States,
1988-2006. J Invest Dermatol. 2010;130:793-797.
12. Girardi S, Gaudy C, Gouvernet J, Teston J, Richard M, Grob J. Superiority of a
cognitive education with photographs over ABCD criteria in the education of the
general population to the early detection of melanoma: a randomized study. Int J
Cancer. 2006;118:2276-2280.
13. Liu W, Hill D, Gibbs AF et al. What features do patients notice that help to
distinguish between benign pigmented lesions and melanomas?: the ABCD(E) rule
versus the seven-point checklist. Melanoma Res. 2005;15:549-554.
14. McGovern TW, Litaker MS. Clinical predictors of malignant pigmented lesions. A
comparison of the Glasgow seven-point checklist and the American Cancer
Society’s ABCDs of pigmented lesions. J Dermatol Surg Oncol. 1992;18:22-26.
15. Healsmith MF, Bourke JF, Osborne JE, Graham-Brown RA. An evaluation of the
revised seven-point checklist for the early diagnosis of cutaneous malignant
melanoma. Br J Dermatol. 1994;130:48-50.

19
19
16. Thomas L, Tranchand P, Berard F, Secchi T, Colin C, Moulin G. Semiological
value of ABCDE criteria in the diagnosis of cutaneous pigmented tumors.
Dermatology. 1998;197:11-17.
17. Barnhill RL, Roush GC, Ernstoff MS, Kirkwood JM. Interclinician agreement on the
recognition of selected gross morphologic features of pigmented lesions. Studies of
melanocytic nevi V. Journal of the American Academy of Dermatology.
1992;26:185-190.
18. Gunasti S, Mulayim MK, Fettahloglu B et al. Interrater agreement in rating of
pigmented skin lesions for border irregularity. Melanoma Res. 2008;18:284-288.
19. Bränström R, Hedblad MA, Krakau I, Ullén H. Laypersons’ perceptual
discrimination of pigmented skin lesions. Journal of the American Academy of
Dermatology. 2002;46:667-673.
20. Robinson JK, Turrisi R. Skills training to learn discrimination of ABCDE criteria by
those at risk of developing melanoma. Arch Dermatol. 2006;142:447-452.
21. Norman GR, Rosenthal D, Brooks LR, Allen SW, Muzzin LJ. The development of
expertise in dermatology. Arch Dermatol. 1989;125:1063-1068.
22. Norman G, Brooks LR. The Non-Analytical Basis of Clinical Reasoning. Adv
Health Sci Educ Theory Pract. 1997;2:173-184.
23. Gachon J, Beaulieu P, Sei JF et al. First prospective study of the recognition
process of melanoma in dermatological practice. Arch Dermatol. 2005;141:434-
438.
24. Norman G, Young M, Brooks L. Non-analytical models of clinical reasoning: the
role of experience. Medical education. 2007;41:1140-1145.

20
20
25. Norman G. Dual processing and diagnostic errors. Adv in Health Sci Educ.
2009;14 Suppl 1:37-49.
26. Ross BH. Remindings and their effects in learning a cognitive skill. Cogn Psychol.
1984;16:371-416.
27. Allen SW, Brooks LR, Norman GR, Rosenthal D. Effect of prior examples on rule-
based diagnostic performance. Res Med Educ. 1988;27:9-14.
28. Allen SW, Norman GR, Brooks LR. Experimental studies of learning dermatologic
diagnosis: the impact of examples. Teaching and Learning in Medicine.
1992;4:35-44.
29. Regehr G, Cline J, Norman GR, Brooks L. Effect of processing strategy on
diagnostic skill in dermatology. Acad Med. 1994;69:S34-6.
30. Kulatunga-Moruzi C, Brooks LR, Norman G. Using comprehensive feature lists to
bias medical diagnosis. J Exp Psychol Learn Mem Cogn. 2004;30:563-572.
31. McLaughlin K, Rikers RM, Schmidt HG. Is analytic information processing a
feature of expertise in medicine? Adv Health Sci Educ Theory Pract. 2008;13:123-
128.
32. Norman G. Building on experience--the development of clinical reasoning. N Engl
J Med. 2006;355:2251-2252.
33. Grob JJ, Bonerandi JJ. The ‘ugly duckling’ sign: identification of the common
characteristics of nevi in an individual as a basis for melanoma screening. Arch
Dermatol. 1998;134:103-104.
34. Norman G, Brooks L, Colle C, Hatala R. The benefit of diagnostic hypotheses in
clinical reasoning: experimental study of an instructional intervention for forward
and backward reasoning. Cognition and Instruction. 1999;17:433-448.

21
21
35. SkinCancerNet (“A comprehensive online skin cancer information resource
developed by the AAD”). Melanoma-What it Looks Like [Internet]. 2010
[Accessed 15/11/2010]. Available from:
http://www.skincarephysicians.com/skincancernet/melanoma.html.
36. R Development Core Team (2009). R: A language and environment for statistical
computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-
900051-07-0, URL http://www.R-project.org.
37. MacKenzie-Wood AR, Milton GW, de Launey JW. Melanoma: accuracy of
clinical diagnosis. Australas J Dermatol. 1998;39:31-33.
38. Marks R, Jolley D, McCormack C, Dorevitch AP. Who removes pigmented skin
lesions? Journal of the American Academy of Dermatology. 1997;36:721-726.
39. Duque MI, Jordan JR, Fleischer AB et al. Frequency of seborrheic keratosis
biopsies in the United States: a benchmark of skin lesion care quality and cost
effectiveness. Dermatologic surgery. 2003;29:796-801.
40. Rigel DS, Friedman RJ. The rationale of the ABCDs of early melanoma. Journal of
the American Academy of Dermatology. 1993;29:1060-1061.
41. Abbasi NR, Shaw HM, Rigel DS et al. Early diagnosis of cutaneous melanoma:
revisiting the ABCD criteria. JAMA. 2004;292:2771-2776.
42. Rigel DS, Friedman RJ, Kopf AW, Polsky D. ABCDE--an evolving concept in the
early detection of melanoma. Arch Dermatol. 2005;141:1032-1034.
43. Zaharna M, Brodell RT. It’s time for a “change” in our approach to early detection
of malignant melanoma. Clin Dermatol. 2003;21:456-458.
44. Moynihan GD. The 3 Cs of melanoma: time for a change? Journal of the American
Academy of Dermatology. 1994;30:510-511.

22
22
45. Marghoob AA, Slade J, Kopf AW, Rigel DS, Friedman RJ, Perelman RO. The
ABCDs of melanoma: why change? Journal of the American Academy of
Dermatology. 1995;32:682-684.
46. Fox GN. ABCD-EFG for diagnosis of melanoma. Clin Exp Dermatol. 2005;30:707.
47. Weinstock MA. ABCD, ABCDE, and ABCCCDEEEEFNU. Arch Dermatol.
2006;142:528.
48. Weinstock MA. Cutaneous melanoma: public health approach to early detection.
Dermatologic therapy. 2006;19:26-31.
49. Brown N, Robertson K, Bisset Y, Rees J. Using a structured image database, how
well can novices assign skin lesion images to the correct diagnostic grouping? J
Invest Dermatol. 2009;129:2509-2512.
50. Aldridge RB, Glodzik D, Ballerini L, Fisher RB, Rees JL. The utility of non-rule
based visual matching as a strategy to allow novices to achieve skin lesion
diagnosis. Acta dermato-venereologica. In press
51. Laskaris N, Ballerini L, Fisher RB, Aldridge B, Rees J. Fuzzy description of skin
lesions. Medical Imaging 2010: Image Perception, Observer Performance, and
Technology Assessment, edited by David J Manning, Craig K Abbey, Proceedings
of SPIE Vol 7627 (SPIE, Bellingham, WA 2010) pp 762717-1 to 762717-10, San
Diego, CA, February 2010.

23
23
FIGURES
Figure 1 Legend
A screen “snap shot” of the purpose built software used to record the 33 subjects’
assessments of the 3 ABC properties. The subjects scored each of the 3 properties on
the 10-point Visual Analogue Scales that were displayed to the right of the image, by
moving the slider to the desired level.
Figure 1

24
24
Figure 2 Legend
A screen “snap-shot” taken from the SkinCancerNet website (35), demonstrating the
caricatured images which we used as the anchor points for the Visual Analogue Scales
in our software. The pictures on the right were used as they demonstrate the analytical
criteria of the ABC, but without facilitating any non-analytical pattern recognition that
could have developed if the “real-life” images had been used.
Figure 2

25
25
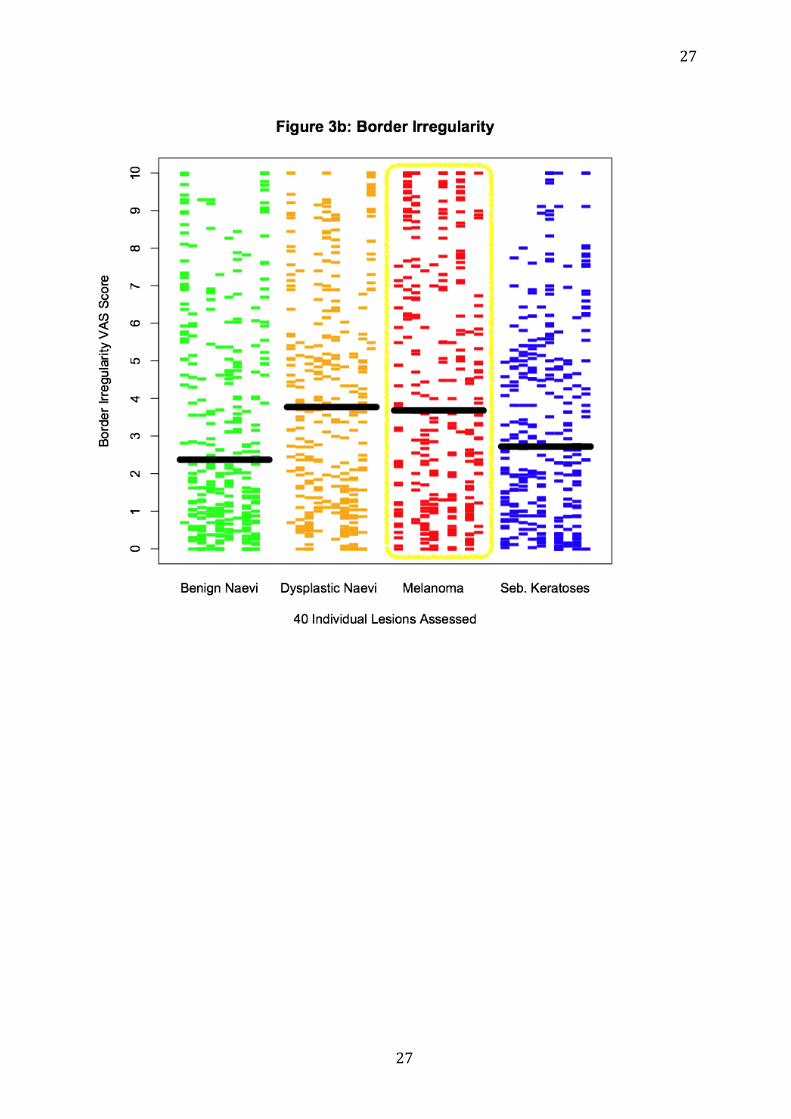
Figure 3 Legend
The full results of all 3960 comparisons undertaken are split according the ABC
properties assessed into 3 plots (Figure 3a- Asymmetry; 3b-Border Irregularity; 3c-
Colour Uniformity). Each horizontal bar represents an individual’s score. The 40 lesions
assessed are displayed in columns across the X-axis, grouped by their diagnostic classes
(Green= Benign Naevi, Orange=Dysplastic Naevi, Red=Melanomas, Blue=Seborrheic
Keratoses). The median score for each diagnostic class is demonstrated by the large
horizontal black bar.

26
26
27
27

28
28

29
29
Figure 4 Legend
An enlarged display of the highlighted section of Figure 3b, showing all the Border
Irregularity VAS scores for the 10 Melanoma lesions. The lesions with the highest
variation (lesion 3, IQR=4.86) and lowest variation (lesion 7, IQR=1.93) are further
highlighted, in blue and cyan respectively, to demonstrate the large spread of scores
attributed to lesions within the same diagnostic class. For lesion 3 it can be seen that
the range of scores attributed by the 33 subjects was 0.7 to 10 with a median of 6.6 and
for lesion 7 the range was 0 to 5.5 with a median of 1.3.
Figure 4

30
30
Table 1:
Lesion Class
Benign Naevi
Dysplastic Naevi
Melanomas Seborrheic Keratoses
Asymmetry VAS Scores (0= Symmetric, 10=Asymmetric)
Median 3.66 4.55 4.83 4.77
IQR 4.96 4.88 5.94 4.07
90th Percentile 8.93 8.97 9.52 8.09
Border Irregularity VAS Scores (0= Regular, 10=Irregular)
Median 2.37 3.77 3.68 2.72
IQR 4.61 5.05 6.46 4.08
90th Percentile 8.27 8.93 9.78 7.52
Colour Uniformity VAS Scores (0= Single uniform colour, 10= Multiple or non‐uniform colour distribution)
Median 3.92 4.83 5.63 4.92
IQR 5.00 4.88 5.59 4.23
90th Percentile 8.26 9 9.59 8.34





























