Embed Size (px)
DESCRIPTION
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master’s P rogrammes at the University of Pécs and at the University of Debrecen Identification number : TÁMOP-4.1.2-08/1/A-2009-0011. - PowerPoint PPT Presentation
Citation preview

Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat the University of Pécs and at the University of DebrecenIdentification number: TÁMOP-4.1.2-08/1/A-2009-0011

TISSUE REPAIR (3)
Dr. Judit PongráczThree dimensional tissue cultures and tissue engineering – Lecture 19
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat the University of Pécs and at the University of DebrecenIdentification number: TÁMOP-4.1.2-08/1/A-2009-0011

TÁMOP-4.1.2-08/1/A-2009-0011
Heart failure• One of the most frequent conditions• Major cause of morbidity and mortality in
developed countries• Causes:
– Congenital malformations– Hypertension– Myocardial infarction– Toxic– Infectious

TÁMOP-4.1.2-08/1/A-2009-0011
Heart regenerative therapiesHeart regenerative therapies are in focus of investigation:• The occurence of heart failure (HF) is
increasing with age• Population of developed countries are
increasingly aged• Number of patients surviving myocardial
infarction (MI) is increasing• Most of them have chronic HF (CHF)

TÁMOP-4.1.2-08/1/A-2009-0011
Left ventricle assist device (LVAD)• Aids the pumping function
of the (left) ventricle• Pulsatile pumping or• Continous pumping• Longest bearing of an
implanted LVAD was 7 years

TÁMOP-4.1.2-08/1/A-2009-0011
Ventricular assist devicesIn targets of heart transplantation:• Bridges the time until a donor is found• In itself enhances the regeneration of the damaged heart
muscle• Improves life qualityIn patients not fitting for transplantation:• Palliative therapy• Improves life qualityComplications may involve:• Risk of infection• Risk of clotting disorders• Risk of embolization

TÁMOP-4.1.2-08/1/A-2009-0011
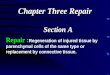
Bone marrow cells in cardiac repair
Blood vesselEndothelial
progenitor cells (hemangioblasts)
HeartSP cellsKit+ cells
Sca-1+ cells
Bone marrowMesenchymal stem
cellsHematopoietic stem
cellsSP cells
Skeletal muscleSatellite cells
SP cells
Fusion-dependent andfusion-independent
differentation

TÁMOP-4.1.2-08/1/A-2009-0011
Cellular therapies in cardiac repair I• Bone marrow cells (BMC)• Hemopoetic stem cells may contribute to
heart repair• Extensively studied in animal models with
variously labelled BMC• Sex-mismatched human heart transplant
patients• After injury, homing to the injured region can
be detected• GCSF mobilisation of BMC does not reproduce
the results with injection

TÁMOP-4.1.2-08/1/A-2009-0011
Cellular therapy of cardiac musclesIntravenous infusionSelective intracoronary infusionDirect intramyocardial injection
↓Cardiomyocyte apoptosisRecruitment of resident stem
cellsCardiomyocyte proliferation
Matrix:Scar
compositionGranulation
tissue
Pro-angiogenic cytokinesAngiogenic ligands
↑Cardiac performance
↑Number of functional
cardiomyocytes↑Perfusion
Secretion of paracrine factors
Differentiation to components of vascular wall
Differentiation to a cardiac phenotype
Fusion with resident
cardiomyocytesPerivascular incorporation

TÁMOP-4.1.2-08/1/A-2009-0011
Cellular therapies in cardiac repair II• No direct evidence of BMC
transdifferentiation to cardiomyocytes• If it occurs, it is a rare event• Maybe the obviously present benefit is the
increased vascularization of the injured heart muscle which enhances intrinsic regeneration capacity

TÁMOP-4.1.2-08/1/A-2009-0011
Cellular therapies in cardiac repair III• Evidence for dividing cardiomyocytes in the
human heart• Multyple types of proliferating cells in the
myocardium was observed bearing both SC markers (Sca-1, CD31) and cardiomyocyte markers upon triggered injury (5-azacytidine)
• Present in rodents and humans• Marked proliferative capacity

TÁMOP-4.1.2-08/1/A-2009-0011
Cellular therapy of cardiac muscle
Cardiomyocite• Single nuclei (central)• Gap junction (+)• Cx43 expression (+)
Myotube• Multinucleated• Gap junction (-)• Cx43 expression (-)
Skeletal muscle• Multinucleated (peripheral)• Gap junction (-)• Cx43 expression (-)
Myoblast (satellite cell)• Single nucleus• Gap junction (+)• Cx43 expression (+)• Proliferation (+)
Fusion and differentiation
???

TÁMOP-4.1.2-08/1/A-2009-0011
Skeletal myoblasts• Early studies used cultured SMBs from muscle
biopsies• Improvement of cardiac performance and life quality:
– Reduced NO consumption– Improvement in NYHA class– Better excercise tolerance
• Patients showed ventricular arhyithmias• Sometimes ICD use was necessary• However, the number of patients treated was low• No untreated control group was used in these studies

TÁMOP-4.1.2-08/1/A-2009-0011
Embryonic stem cells• Cardiogenic potential is assured• Injury repair: hESC needed to be differentiated
before application• Injury itself is not enough to trigger growth and
functional replacement, moreover, inflammatory citokines damage the grafted cells
• Anti-inflammatory treatment and protective agents needed for graft support (IGF-1, pan-caspase inhibitors and NO blockers)
• Differentiated cardiomyocytes trigger an immunoresponse in immunocompetent mice
• Problem: teratoma risk! Translation to the clinic is recently questionable

TÁMOP-4.1.2-08/1/A-2009-0011
Tissue engineering in tooth regeneration/replacement• Dentition is important for feeding in
vertebrates• Aberrations in dentition or poor dental care is
not life-threatening in developed countries• But damage and loss of teeth may
substantially affect quality of life

TÁMOP-4.1.2-08/1/A-2009-0011
Tooth development• Reciprocal signaling events
between the epithelium and underlying mesenchyme
• Initiation, morphogenesis and terminal differentiation
1.Bud stage2.Epithelial cup (Encloses
the mesenchyme)3.Bell stage4.Crown stage
Dentin
Odontoblast
Root
Periodontalmembrane
Cementum
Enamel
Crown
Blood vessel
Sharpey fiber
Gingival fiberPulp
Alveolarbone
Neural fiber

TÁMOP-4.1.2-08/1/A-2009-0011
Dental pulp stem cells (DPSC)• DPSC are multipotent cells in the dental pulp• Regeneration of dentin after tooth injury• Odontoblasts emerge close to the site of
injury• Undifferentiated mesenchymal cells are
constantly migrating from deeper tooth layers to the dentin differentiating into odontoblasts
• Evidence suggest that these are DPSC

TÁMOP-4.1.2-08/1/A-2009-0011
Differentiation capacity of DPSC• Human DPSC cultured under mineralization-
enhancing conditions • Cells form odontoblast-like cells producing
dentin and expressing nestin• DPSCs phenotypically resembles to MSC but
its capacity to produce dentin is unique

TÁMOP-4.1.2-08/1/A-2009-0011
Bioengineered tooth conceptsScreening of
tooth-forming cells3D manipulation of
single cellsTransplantation of a
bioengineered tooth germ
Patient derivedstem cells
Epithelial cells
Mesenchymal cells
Transplantation
Bioengineered tooth,prepared by in vitro culture
Bioengineered toothgerm development
Bioengineeredtooth germ

TÁMOP-4.1.2-08/1/A-2009-0011
De novo tooth engineering IScaffold-based roots:• Bio-artificial root implant that supports an
artificial (porcelain) crown• Cells grow inside the scaffold thus serving as
a proper anchor• Animal (porcine) model proved the
applicability of this solution

TÁMOP-4.1.2-08/1/A-2009-0011
De novo tooth engineering IIReproduction of embryonic tooth germs:• Fully functional tooth by reproducing the
embryonic tooth development• Both roots and crown are formed• Rodent experiments were successful• Not only embryonic or newborn cells but also
adult cells were able to recreate tooth• Both scaffold and scaffoldless experiments

TISSUE REPAIR (4)
Dr. Judit PongráczThree dimensional tissue cultures and tissue engineering – Lecture 20
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat the University of Pécs and at the University of DebrecenIdentification number: TÁMOP-4.1.2-08/1/A-2009-0011

TÁMOP-4.1.2-08/1/A-2009-0011
Major causes of urogenital injuriesInjuries or loss of function of the urogenital organs:• Congenital malformations• Trauma• Infection, inflammation• Iatrogenic injury

TÁMOP-4.1.2-08/1/A-2009-0011
Repair possibilities of the urogenital organsAutologous non-urogenital tissues• Skin• Gastrointestinal
segments• Mucosa from multiple
body sitesAllogen• Kidney graft for
transplantation (cadaver or living)
• Cadaver fascia
Xenogenic materials• Bovine collagenArteficial materials• Silicone• Polyurethane• Teflon

TÁMOP-4.1.2-08/1/A-2009-0011
Obtaining cells for tissue regeneration• Autologous or allogenic• End stage organ damage restricts cell
availability for tissue repair• In vitro culturing results are different
– In vitro cultured bladder SMC: lower contractility
• Low cell number may hinder possibilities• Stem cells can be the solution• Therapeutic cloning is also might be feasible

TÁMOP-4.1.2-08/1/A-2009-0011
Biomaterials for genitourinary reconstruction I• Arteficial materials• Replacement of ECM functions:
– Providing 3D structure of tissue formation– Regulation and stimulation of cell
differentiation via the storage and release of bioactive factors
– Injecting cells without scaffold support is not effective

TÁMOP-4.1.2-08/1/A-2009-0011
Biomaterials for genitourinary reconstruction IINaturally derived biomaterials:• Collagen• Alginate• Acellular tissue matrices:
– Bladder submucosa– Small intestinal submucosa (SIS)
Synthetic polymers:• PLA, PGA, PLGA

TÁMOP-4.1.2-08/1/A-2009-0011
Uroepithel – unique features• Excretion not absorption• Recent methods favor intestinal autografts
for urethra, ureter or bladder repair• The different structure and function of
uroepithel and intestinal epithel often lead to complications which may be severe

TÁMOP-4.1.2-08/1/A-2009-0011
Urethra reconstruction I Strictures, injuries, trauma, congenital abnormalities (hypospadiasis)Most often, buccal mucosa grafts are used for reconstruction:
• Graft tissue is taken from the inner surface of the cheek or lips
• The epithelium is thick and the submucosa is highly vascular
• This graft is resistant for infections

TÁMOP-4.1.2-08/1/A-2009-0011
Urethra reconstruction II Bladder-derived urothelium:
• Suitable for reconstruction in rabbits• No human tests have been conducted
Decellularized collagen matrices:• The material is available on-demand• Good results in „only” reconstructive
surgery• Results in strictures when tubularized
reconstruction is needed

TÁMOP-4.1.2-08/1/A-2009-0011
Urethra reconstruction III Decellularized and tubularized matrices seeded with autologous urothelium:
• Good results in animal models• Constructs seeded with cells developed
similar histological structure to that of uroepithelium
• Collagen matrices without cell seeding resulted in strictures

TÁMOP-4.1.2-08/1/A-2009-0011
Bladder reconstruction IMost commonly intestinal-derived mucosal sheets are used for reconstruction:
• Intestinal epithelium is different from urothelium
• Designed to absorb and secrete mucus• Complications: infection, urolithiasis, metabolic
disorders, perforation, increased mucus production, malignancies
Because of disappointing results, attempts for alternative treatments are performed

TÁMOP-4.1.2-08/1/A-2009-0011
Bladder reconstruction IIAugmentation of bladder:• Progressive dilatation of native bladder tissue
in animal experiments• Augmentation cystoplasty in animals and
humans with dilated urethral segments• Better than the usage of GIT-derived
segments

TÁMOP-4.1.2-08/1/A-2009-0011
Bladder reconstruction IIINon-seeded acellular matrices:• Xenogenic SIS → decellularized collagen-based
tissue matrix → no musclular layer• Epithelization of the graft construct did occur• Non-compliance because of the lack of
muscularis layer
Matrices seeded with epithel and SMC:• Successful muscular layer formed, compliance is
fair• Scaffolds: combination of PGA and collagen

TÁMOP-4.1.2-08/1/A-2009-0011
Ureter reconstructionAnimal studies for urether reconstruction:• Non-seeded matrices facilitated the re-
growth of the urethral wall components in rats
• Stiff tubes like teflon were un-successful in dogs
• Non-seeded acellular matrices proved to be un-successful to replace a 3cm long urethral segment in dogs
• Cell seeded biodegradable scaffolds gave more satisfying results in dogs

TÁMOP-4.1.2-08/1/A-2009-0011
Kidney replacement therapyCurrently two options are available for the treatment of end-stage renal failure (ESRF):• Dialysis • Kidney transplantation

TÁMOP-4.1.2-08/1/A-2009-0011
Dialysis• Hemodialysis, hemofiltration
– Extracorporeal dialyzer unit: hollow fiber dialyzers are most commonly used
– Anticoagulated venous blood is let through the dialyzer, countercurrent of dialysis solution is applied
• Peritoneal dialysis– Dialysis solution is applied in the peritoneal cavity
• Toxic metabolites and excessive water are removed from the patient via osmotic differences between the blood and dialysis solution
• Cardiovascular, metabolic and musculoskeletal complications are frequent

TÁMOP-4.1.2-08/1/A-2009-0011
Kidney transplantation• Most often transplanted parenchymal organ• Cadaver or live donor• Offers an improvement in the life quality of
dialyzed patients• Implantation of allogenic grafts needs
immunosuppressive treatment • Side effects of immunosuppressive agents
involve increased risk of infections and malignancies, kidney and hepatotoxicity, cardiovascular and metabolic side effects

TÁMOP-4.1.2-08/1/A-2009-0011
Tissue engineered kidneyBioartificial approach:• Replace dialysis machines with bioartificial
kidney• Extracorporeal devices/intracorporeal devices• Preclinical trials on dogs with porcine TE renal
tubules: successful BUN and K control• However, the patient is still tied to an
extracorporeal machine

TÁMOP-4.1.2-08/1/A-2009-0011
Bioartificial kidney
Pump 370-80 ml/min
Ultrafiltratereservoir
Heatexchanger
Heatexchanger
Ultrafiltrate(into RAD luminal space)
Hem
ofilte
r
Pressure monitor
Post hemofilter blood(into RAD ECS)
Replacementfluid
RAD cartridge
Processedultrafiltrate
(urine)
Pump 25-7 ml/min
Pump 180 ml/min
5-10mm Hg
10-25 mm Hg
Venous blood
Post RADblood
Luminal spaceProximal tubule cells
Extracapillary spaceFiber wall

TÁMOP-4.1.2-08/1/A-2009-0011
Tissue engineered kidneyIn vivo approach:• Human kidney cells were seeded onto a
polycarbonate tubular construct• Upon implantation in nude mice the construct
was extensively vascularized• Urine-like fluid production: urea and
creatinine content• Epithelial cells showed signs of tubular
differentiation

TÁMOP-4.1.2-08/1/A-2009-0011
In vitro engineered murine kidney
Wolff duct
Metanephricmesenchyme
4-6 days
Bud
Cells
Cells
Bud