Embed Size (px)
Citation preview

- ARTICLES
Tissue Engineering
Robert Langer* and Joseph P. Vacanti
The loss or failure of an organ or tissue is one of the most frequent, devastating, and costlyproblems in human health care. A new field, tissue engineering, applies the principles ofbiology and engineering to the development of functional substitutes for damaged tissue.This article discusses the foundations and challenges of this interdisciplinary field and itsattempts to provide solutions to tissue creation and repair.
Every year, millions of Americans suffertissue loss or end-stage organ failure (Table1). The total national health care cost forthese patients exceeds $400 billion per year(1, 2). Approximately 8 million surgicalprocedures are performed annually in theUnited States to treat these disorders and40 to 90 million hospital days are required(2). Physicians treat organ or tissue loss bytransplanting organs from one individualinto another, performing surgical recon-struction, or using mechanical devices suchas kidney dialyzers (3). Although thesetherapies have saved and improved count-less lives, they remain imperfect solutions.Transplantation is severely limited by acritical donor shortage. For example, fewerthan 3,000 donors are available annuallyfor the approximately 30,000 patients whodie from liver failure (4). Donor shortagesworsen every year and increasing numbersof patients die while on waiting lists forneeded organs (5). Surgical reconstructioncan result in long-term problems. For ex-ample, colon cancers often develop aftersurgical treatment of incontinence that di-rects urine into the colon (6). Mechanicaldevices cannot perform all of the functionsof a single organ and therefore cannotprevent progressive patient deterioration.
Tissue engineering is an interdiscipli-nary field that applies the principles ofengineering and the life sciences toward thedevelopment of biological substitutes thatrestore, maintain, or improve tissue func-tion (7). Three general strategies have beenadopted for the creation of new tissue:
1) Isolated cells or cell substitutes. Thisapproach avoids the complications of surgery,allows replacement of only those cells thatsupply the needed function, and permits ma-nipulation of cells before infusion. Its poten-
R. Langer is in the Department of Chemical Engineer-ing and the Harvard-M.I.T. Division of Health, Scienc-es and Technology, Massachusetts Institute of Tech-nology, E25-342, Cambridge, MA 02319 and the De-partment of Surgery, Children's Hospital, Boston, MA02115. J. P. Vacanti is in the Department of Surgery,Harvard Medical School and Children's Hospital, Bos-ton, MA 02115.
*To whom correspondence should be addressed atMassachusetts Institute of Technology, E25-342.
920
tial limitations include failure of the infusedcells to maintain their function in the recipi-ent, and immunological rejection.
2) Tissue-inducing substances. The suc-
cess of this approach depends on the puri-fication and large-scale production of ap-
propriate signal molecules, such as growthfactors, and, in many cases, the develop-ment of methods to deliver these moleculesto their targets.
3) Cells placed on or within matrices.In closed systems, the cells are isolated fromthe body by a membrane that allows perme-
ation of nutrients and wastes but preventslarge entities such as antibodies or immunecells from destroying the transplant. Thesesystems can be implanted or used as extra-corporeal devices (Fig. 1). In open systems,cells attached to matrices are implanted andbecome incorporated into the body (Fig.2). The matrices are fashioned from naturalmaterials such as collagen or from syntheticpolymers. Immunological rejection may beprevented by immunosuppressive drugs or
by using autologous cells.Investigators have attempted to engi-
neer virtually every mammalian tissue. Inthe following summary, we discuss replace-ment of ectodermal, endodermal, and me-
sodermal-derived tissue.
Ectoderm
Nervous system. Brain diseases such as Par-kinson's disease, where there is a loss ofdopamine production, represent an impor-tant target for tissue engineering. Trans-plantation of normal fetal dopamine-pro-ducing cells by stereotaxically guided injec-tion into the brain has produced significantreversal of debilitating symptoms in humans(8). Alternative methods have been testedin animal models. PC12 cells, an immortal-ized cell line derived from rat pheochromo-cytoma, have been encapsulated in polymermembranes and implanted in the guinea pigstriatum (Fig. 3A). Dopamine release fromthe capsules was detectable for 6 months (9).Similarly, encapsulated bovine adrenal chro-maffin cells have been implanted into thesubarachnoid space in rats, where through
SCIENCE * VOL. 260 * 14 MAY 1993
their continuous production of enkephalinsand cathecholamines they appeared to re-lieve chronic intractable pain (10).
Nerve regeneration has also been studied.Peripheral nerves are capable of regenerationafter transection injury. Transected nervescan sometimes be clinically repaired by end-to-end approximation of the stumps withfine sutures. When nerve injury results ingaps that are too wide for healing, autolo-gous nerve grafts are used as a bridge. Syn-thetic nerve guides (conduits) could help inthese cases by protecting the regeneratingnerve from infiltrating scar tissue or by di-recting new axons toward their target. Sev-eral laboratories have shown in animal mod-els that synthetic guides composed of naturalpolymers (laminin, collagen, chondroitinsulfate) or synthetic polymers can enhancenerve regeneration (11). Initial results sug-gest that this process can be aided by placingSchwann cells derived from sciatic nerves inMatrigel® seeded in polymer membranes(12). In addition, polymers can be designedso that they slowly release growth factors,which may allow regrowth of the damagednerve over a greater distance (13).
Cornea. More than 10 million peopleworldwide suffer from bilateral comeal blind-ness. Not only are transplant donors limited,but there is a risk of infectious agent trans-mission. Ideally, an artificial cornea wouldconsist of materials that support adhesionand proliferation of comeal epithelial cellsso that an intact continuous epithelial layerforms. These materials should also haveappropriate nutrient and fluid permeability,light transparency, and no toxicity. Comealepithelial cells have been preseeded on poly-vinyl alcohol hydrogels and transplantedinto rabbit comeas, where they remainedadherent and proliferated for 1 to 2 weeks(14). Long-term studies of such materials arewarranted; safe and effective methods ofattaching these materials to the cornea mustalso be developed.
Skin. Approximately 150,000 individu-als are hospitalized and 10,000 die eachyear in the United States because of bums.Several new types of tissue transplants arebeing studied for the treatment of bums,skin ulcers, deep wounds, and other inju-ries. In some cases, patients are implantedwith a composite material whose upperlayer consists of silicone (which preventsfluid loss) and whose lower layer consists ofchondroitin-sulfate and collagen (which in-duces new blood vessels and connectivetissue ingrowth). In essence, the patients
p, pp, pp RP pp RP RP PP -m PR pp RP, PP RP RP PR RR 1-1 RP ----------1------------------- :1 x R :l :M

7 --I .
receive a new dermis. After 3 weeks, theupper layer is replaced with an extremelythin epidermal graft. Clinical studies haveshown good graft acceptance with minimalscarring (15). In a refinement of the proce-dure, the second skin graft was eliminatedby seeding epidermal cells obtained from asmall skin graft (0.003 inch thick) onto thelower layer prior to placement on the pa-tient (16).
Table 1. Incidence of organ and tissue defi-ciencies, or the number of surgical proceduresrelated to these deficiencies, in the UnitedStates. This is a partial list compiled from sourc-es that include the American Diabetes Associ-ation, American Liver Foundation, MuscularDystrophy Association, American Red Cross,American Kidney Foundation, The WilkersonGroup, Cowen and Co., American Academy ofOrthopedic Surgery, American Heart Associa-tion, National Institute of Neurological Disordersand Stroke, Source Book of Health Insurance(Health Assurance Association of America),1991, Federal Register, and Department ofHealth and Human Services (Medicare-basedinformation).
ProceduresIndication or patients
per year
SkinBurns* 2,150,000Pressure sores 1,500,000Venous stasis ulcers 500,000Diabetic ulcers 600,000
Neuromuscular disorders 200,000Spinal cord and nerves 40,000Bone
Joint replacement 558,200Bone graft 275,000Internal fixation 480,000Facial reconstruction 30,000
CartilagePatella resurfacing 216,000Chondromalacia patellae 103,400Meniscal repair 250,000Arthritis (knee) 149,900Arthritis (hip) 219,300Fingers and small joints 179,000Osteochondritis dissecans 14,500
Tendon repair 33,000Ligament repair 90,000Blood vessels
Heart 754,000Large and small vessels 606,000
LiverMetabolic disorders 5,000Liver cirrhosis 175,000Liver cancer 25,000
Pancreas (diabetes) 728,000Intestine 100,000Kidney 600,000Bladder 57,200Ureter 30,000Urethra 51,900Hernia 290,000Breast 261,000Blood transfusions 18,000,000Dental 10,000,000
A second approach to skin grafts involvesthe in vitro culture of epidermal cells (kera-tinocytes). Small skin biopsies (1 cm2) are
harvested from bum patients and expanded10,000-fold-a size comparable to an adult'sbody surface area. This expansion has beenachieved by cultivating keratinocytes on a
feeder layer of irradiated NIH 3T3 fibro-blasts, which, in conjunction with certainadded media components, stimulates rapidcell growth. An advantage of this approachis the ability of the grafts to cover extremelylarge wounds; a disadvantage is the 3- to4-week period required for cell expansion,which may be too long for a severely burnedpatient. Cryopreserved allografts may helpto circumvent the problem (17).
Another promising approach uses humanneonatal dermal fibroblasts grown on degrad-able polyglycolic acid mesh (Fig. 3B). Be-cause fibroblasts are easy to cryopreserve andgrow, a uniform stock of cells can be main-tained for these grafts. In deep injuries in-volving all layers of skin, the grafts are
placed onto the wound bed and a skin graftis placed on top. The graft then vascularizes,resulting in the formation of organized tissueresembling dermis. Clinical trials haveshown good graft acceptance with no evi-dence of immune rejection (18). Fibroblastshave also been placed on a hydrated collagengel. Upon implantation, the cells migratethrough the gel by enzymatic digestion ofcollagen, which results in reorganization ofcollagen fibrils (19). This approach has un-
dergone limited clinical testing.
Endoderm
Liver. Most liver support systems remove
toxins normally metabolized by the liverthrough dialysis, charcoal hemoperfusion,immobilized enzymes, or exchange transfu-sion (20). None of these systems, however,can offer the full spectrum of functionsperformed by a healthy liver. Investigatorsare now endeavoring to achieve liver re-
placement with isolated hepatocytes. Thehepatocytes have been placed in suspen-
sions, encapsulated in microcapsules or hol-low fibers, placed on substrates such as
microcarriers coated with extracellular ma-
trix proteins, or attached to polymer net-works (20, 21). In animal models, thetransplanted hepatocytes have produced al-bumin and other liver function markers,and have cleared products of bilirubin andurea metabolism.
Hepatocyte systems are being studied forboth extracorporeal and implantable appli-cations. Extracorporeal systems, whichwould be used when a patient's own liver isrecovering or as a bridge to transplant, offerseveral advantages: (i) better control of themedium surrounding the cell system (forexample, the ability to achieve improvedtransport of oxygen, nutrients, and wastes);(ii) better control of the timing and dura-tion of use; and (iii) a decreased chance ofimmune rejection because the patient'swhite cells can be separated from hepato-cytes by plasmapheresis. Implantable hepa-tocyte systems, on the other hand, offer the
Fig. 1. There are three commonclosed-system configurations forcell transplant devices (69, 70) IIII[figure adapted with permission Blood - Extravascularfrom (70)]. In vascular devices, flow cormpartmsntsthe cells are placed in an extra- t t t t t tcellular compartment surroundinga tubular membrane (i.d. -1 mm) ,through which blood can flow. Inmacrocapsule systems, the cellsare placed in sheaths, rods, ordisks (diameter >0.5 to 1.0 mm).In microcapsule systems, the
tMacrocapsu.
cells are placed in injectable - ','4'e' sheaths,rods,dscs
spherical beads (diameter <0.5 tmm). Device biocompatibility iscritical because tissue reactioncan block the flow of nutrients and ,wastes to and from the capsule. ( MirocapsuesMicrocapsules are commonly sphecalmade of hydrogels-in particular, 'pe*ortsthe polysaccharide alginate-be- Pormcause of the extremely mild con-ditions required for gel formation. The alginate can be further coated with polyanions, such aspolylysine, and again with alginate if desired. Such coatings can affect the flow of nutrients andwastes, mechanical strength, and biocompatibility. Results of in vivo studies with alginate are notalways consistent, possibly because of variations in alginate purity (71). Macrocapsules and vasculardevices often consist of acrylonitrile-vinyl chloride copolymers (69, 70). Microcapsules haveadvantages over macrocapsules in that they impose fewer limitations on diffusional flow of nutrientsand wastes and they can be administered by injection. Macrocapsules, on the other hand, are easierto retrieve should complications occur and are physically more stable than microcapsules.
SCIENCE * VOL. 260 * 14 MAY 1993
*Approximately 150,000 of these individuals are hos-pitalized and 10,000 die annually.
921

possibility of permanent liver replacementif properly integrated into the patient. Fur-thermore, the vascular access required forextracorporeal use, which is sometimes as-sociated with thromboembolic complica-tions, may not be necessary with an im-plantable system (20).
Successful hepatocyte transplantationdepends on a number of critical steps. First,the hepatocytes must be cultured in vitroprior to transplantation. Hepatocyte mor-phology can be maintained by sandwichingthe cells between two hydrated collagenlayers. Under these conditions, the hepato-cytes secrete functional markers at physio-logical levels for at least 6 weeks (22).Second, the hepatocytes must be attachedto the polymer substrata so that they main-tain their differentiated function. By con-trolling the density of the extracellular ma-trix substrate used to coat microcarriers orpolymer films, both the extent of differen-tiated function and cell proliferation can beregulated (23). Third, the viability of thetransplanted hepatocytes must be main-tained. This step can be accomplished byvascularizing the cell transplant region toprovide oxygen and nutritional factors(24). Fourth, a sufficient mass of hepato-cytes must become engrafted and functionalto achieve metabolic replacement. For im-plantable systems, this problem has beenaddressed in animal models in which largenumbers of hepatocytes are placed intovascularized areas of the body and suppliedwith hepatotrophic factors from the portalcirculation (25). Finally, hepatocyte trans-plantation per se does not provide all celltypes nor the delicate and complex struc-tural features of the liver. For example,products normally excreted through bilemay accumulate because of the difficulty inreconstructing the biliary tree solely fromhepatocytes. This problem is not life-threatening, however, and resins that bindsuch products could be incorporated into anartificial liver (20). Hepatocytes placed onappropriate polymers can form tissue struc-tures resembling those in the natural organ(Fig. 2) and have shown evidence of bileducts and bilirubin removal (25).
Pancreas. Each year, over 728,000 newcases of diabetes are diagnosed and 150,000Americans die from the disease and itscomplications; the total yearly cost in theUnited States is over $20 billion. Diabetesis characterized by pancreatic islet destruc-tion, leading to loss of glucose control.Tissue-engineering approaches to treatmenthave focused on transplanting healthy pan-creatic islets, usually encapsulated in amembrane to avoid immune rejection.Three general approaches (Fig. 1) havebeen tested in animal models. In the first, atubular membrane was coiled in a housingthat contained islets. The membrane was
connected to a polymer graft that in turnconnected the device to blood vessels. Themembrane had a 50-kD molecular masscutoff, which allowed free diffusion of glu-cose and insulin but blocked passage ofantibodies and lymphocytes. In pancreatec-tomized dogs treated with this device, nor-moglycemia was maintained for more than150 days (26). In a second approach, hollowfibers containing rat islets were immobilizedin the polysaccharide alginate. When thedevice was placed intraperitoneally in dia-betic mice, blood glucose levels were low-ered for more than 60 days and good tissuebiocompatibility was observed (27). Finally,islets have been placed in microcapsulescomposed of alginate or polyacrylates. Insome cases, rodents treated with these mi-crocapsules maintained normoglycemia forover 2 years (28). All of these transplanta-tion strategies require a large, reliable sourceof donor islets. Porcine islets are used inmany studies, although genetically engi-neered cells that overproduce insulin are alsobeing examined.
Tubular structures. The current practiceof using parts of other organs for reconstruc-tion of the ureter, bladder, and urethraoften leads to urinary reflux, infection, and
dilation of the upper urinary tract, and, insome instances, electrolyte disturbance.Polymer or metal implants have been usedto replace ureters but have generally failedbecause of poor biocompatibility, lack ofperistaltic activity, and accumulation of saltdeposits. Because the ureter has a goodregenerative capacity, cell-polymer im-plants have also been explored as replace-ment therapy. In an initial study, cellsderived from a bladder cell carcinoma werecultured on collagen sponges and implantedin rats and dogs for over 3 months. Al-though the rat implants showed substantialsalt deposits on the sponge surface, the dogimplants showed extensive urothelial cellregeneration on the collagen graft innersurface (29). More recently, urothelial cellswere seeded onto degradable polyglycolicacid tubes and implanted in rats and rab-bits. After 20 days, two to three layers ofurothelial cells lined the polymers (30).
The concept of using tubular structuresis being studied for other tissues such as thetrachea, esophagus, intestine, and kidney.A diseased esophagus, for example, can betreated clinically with autografts from thecolon, stomach, skin, or jejunal segments.However, such procedures may result in
Flg. 2. In one approach to open- Biodegradablsystem implants, three-dimen- polymer scfoldsional highly porous scaffoldscomposed of synthetic polymersserve as cell transplant devices.These devices may facilitate for-mation of structural and functionaltissue units by the transplantedcells. This approach is based on In vkro tlsue culturethe following observations: (i) Ev-ery tissue undergoes remodeling- Octobh~seS4'(ii) Isolated cells tend to reform ethe appropriate tissue structure Chondoyte. eunder appropriate experimental Hepatocyte econditions. For example, when Enter~**capillary endothelial cells are erocyt..placed on the proper substrate in Urohelia c In vhvo mpantationvitro, they form tubular structures.(iii) Although isolated cells have Newthe capacity to form the appropri-ate tissue structure, they do so Boneonly to a limited degree when carwageplaced as a suspension into tis- Uversue. Such cells begin without any Intestineintrinsic organization and have notemplate to guide restructuring. Ureter(iv) Tissue cannot be implanted inlarge volumes-cells will not sur-vive if they are located more thana few hundred micrometers fromthe nearest capillary. Thus, theopen-system implants are de-signed so that the polymer scaf-fold guides cell organization and growth and allows diffusion of nutrients to the transplanted cells(32). Ideally, the cell-polymer matrix is prevascularized or would become vascularized as the cellmass expands after implantation. Vascularization could be a natural host response to the implant orcould be artificially induced by slow release of angiogenic factors. The polymer could bedegradable or nondegradable. Materials that disappear from the body after they perform theirfunction obviate concerns about long-term biocompatibility.
SCIENCE * VOL. 260 * 14 MAY 1993922

graft necrosis, inadequate blood supply, andother complications. Copolymer tubes con-sisting of lactic and glycolic acid have beensutured into dogs after removal of 5-cmesophageal segments. Over time, connec-tive tissue and epithelium covered the poly-mer graft (which had begun degrading) andthe dogs were able to drink freely and eatsemisolid food (31). In a similar approach,fetal intestinal cells have been placed ontothese copolymer tubes and implanted inrats. Histologic examination several weekslater revealed that some animals had well-differentiated intestinal epithelium liningthe tubes, and this epithelium appeared tosecrete mucous (32). Tubular structureshave also been used in kidney replacementstudies. Current treatments for end-stagerenal failure are based solely on nonphysi-ological driving forces and are not able tomimic active molecular transport accom-plished by renal tubular cells. As a first steptoward creating a bioartificial kidney, renaltubular cells have been grown on acryloni-trile-vinyl chloride copolymers or micro-porous cellulose nitrate membranes. In vi-tro, these cells transported insulin, glucoseand tetraethylammonium in the presence ofa hemofiltrate from a uremic patient (33).This approach has not yet, to our knowl-edge, been explored in vivo.
Mesoderm
Cartilage, bone, and muscle. Over 1 millionsurgical procedures in the United Stateseach year involve cartilage replacement.Current therapies include transplantation(removing healthy cartilage, carving it intodesired shapes, and reimplanting it whereneeded in the same patient) and implanta-
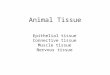
Fig. 3. Histologic sections of engi-neered tissues. (A) Dopamine-pro-ducing cells in a polymer capsulein the guinea pig striatum 12 weeksafter transplant. Cells were visual-ized (orange color) by immuno-staining for tyrosine hydroxylase[reprinted with permission from(9)]. (B) New dermis producedfrom neonatal fibroblasts that wereplaced on degradable polymerswith a thin overlying skin graft andtransplanted into a mouse. Photowas taken 10 days after the trans-plant. (C) New cartilage producedfrom chondrocytes seeded ontodegradable polymers 7 weeks af-ter transplant into a nude mouse.(B) and (C) are stained with hema-toxylin and eosin.
tion of artificial polymer or metal prosthe-ses. Problems arise, however, in that donortissue for transplantation is limited, and it isextremely difficult to form delicate three-dimensional implants from host cartilage.Artificial prostheses may result in infectionand adhesive breakdown at the host-pros-thesis interface. A prosthesis also cannotadapt in response to environmental stressesas does cartilage (34).
The need for improved treatments hasmotivated research aimed at creating newcartilage that is based on collagen-glycos-aminoglycan templates (35), isolated chon-drocytes (36), and chondrocytes attachedto natural (37) or synthetic (38, 39) poly-mers (Fig. 3C). In mice chondrocytesgrown for 1 to 6 months on highly porousscaffolds of polyglycolic or polylactic acidmaintained the scaffold's original three-dimensional shape, appeared glisteningwhite macroscopically, contained sulfatedglycosaminoglycans and type II collagen,and closely resembled cartilage histological-ly (39). It is critical that cartilage trans-plants of appropriate thickness be mechan-ically functional. Recently, chondrocytesgrown in agarose gel culture have beenshown to produce tissue with stiffness andcompressibility similar to articular cartilage(40). The use of well-stirred bioreactors forcultivating chondrocytes on polymer scaf-folds in vitro may enable nutrients to pen-etrate the center of this nonvascularizedtissue, leading to relatively strong and thick(up to 0.5 cm) implants (41).
Over 1 million operations annually in-volve bone repair. Conventionally, boneingrowth is accelerated through the use ofautogenous bone grafts or allogenic bone.The former can be a successful procedure
SCIENCE * VOL. 260 * 14 MAY 1993
but is often material limited and causesdonor site morbidity and contour irregular-ities (42). The latter can also be a successfulprocedure, but cell-mediated immune re-sponses to transplantation alloantigens andpathogens can be problematic.
Metals and ceramics are also used inseveral forms: bioinert (for example, alumi-na), resorbable (for example, tricalciumphosphate), porous (for example, hydroxy-apatite-coated metals), and bioactive (forexample, hydroxyapatites and certain glass-es). Bioactive materials form a bond withthe surrounding tissue upon implantation.Such materials are currently being used inmiddle ear surgery, vertebral surgery, andother applications. Alumina prostheseshave been used in a variety of dental andorthopedic procedures because of their min-imal interaction with surrounding tissueand low coefficients of friction and wearrates. Porous materials (pore size > 100 gum)allow bone to grow into the pores, whichstrengthens the union between the implantand bone. In practice, it may be desirablefor these materials to degrade over timebecause they lose strength as they age. Acritical aspect of ceramic design is deter-mining the appropriate composition, mi-crostructure, pore size, porosity, and surfacechemistry to match the specific biologic andmetabolic requirements of tissues and dis-ease states (43).
Synthetic and natural polymers havebeen explored for bone repair, but it hasbeen difficult to create a polymer displayingoptimal strength and degradation proper-ties. Another approach involves implanta-tion of demineralized bone powder (DBP),which is effective in stimulating bonegrowth in animals and humans; however,DBP cannot induce sufficient bone forma-tion in most non-bony sites. Bone morpho-genic proteins (BMP), now produced bygenetic engineering but originally derivedfrom DBP, or growth factors such as trans-forming growth factor-1 (TGF-P), are oth-er promising strategies. The former induceformation of both cartilage and bone (in-cluding marrow) and the latter augmentbone growth (44). Such molecules havetheoretically unlimited availability; effec-tive delivery systems for such agents will beimportant. Bone growth can also be in-duced when cells are grown on syntheticpolymers or ceramics. For example, whenmarrow cells are grown on porous calciumphosphates in mice, bone forms inside thepores within 3 weeks (45).
The ability to generate muscle fibers maybe useful in the treatment of muscle injury,cardiac disease, disorders involving smoothmuscle of the intestine or urinary tract, andin patients with muscular dystrophy. It hasbeen difficult to find drug therapies to treatsuch diseases; however, gene therapy or
923

cell-based therapies may provide a means oftreating diseases such as Duchenne muscu-lar dystrophy (DMD) (46). Normal myo-blasts from unaffected relatives have beentransplanted into patients with DMD andshown to produce dystrophin for 1 to 6months after transplant, although the effi-ciency of myoblast transfer was low. Myo-blasts can migrate from one healthy musclefiber to another (47); thus, if the efficiencyof transfer can be increased, cell-based ther-apies may be useful in treating DMD andother muscle atrophies.
Heart disease is the single greatest killerin the United States. Once patients be-come symptomatic, their life expectancy isusually markedly shortened. This decline isgenerally attributed to the inability of car-diac cells to regenerate after injury. Incontrast, skeletal muscle has the capacityfor tissue repair, presumably because ofsatellite cells that have regenerative capa-bility. Recently, the feasibility of usingautotransplanted skeletal muscle satellitecells multiplied in vitro and placed intodamaged heart muscle was explored in acanine model. Preliminary results showedthat muscle formation occurred at 8 weeks,but not at 14 weeks after transplant (48).
Blood vessels and cells. The design ofartificial blood vessels and vascular grafts isan active research area. Although large-diameter [>5 mm internal diameter (i.d.)]vascular grafts have been successfully devel-oped with polymers such as Dacron orexpanded polytetrafluoroethylene, it hasbeen difficult to develop vascular grafts of<5 mm i.d. because of biological reactionsat the blood-material and tissue-materialinterface. These reactions lead to strictur-ing and total occlusion from clotting andscarring. To circumvent these problems,grafts have been made from relatively inertmaterials (with either heparin coatings orpolyethylene oxide surfaces) or from mate-rials that interact in a desirable way withblood cells (49). One idea has been to linepolymers in vitro with endothelial cells topromote hemocompatibility (50). Suchgrafts have allowed these blood vessels tostay open in short-term clinical studies.Endothelialization in vivo can be inducedby the healing responses of host tissue,which leads to coverage of grafts with endo-thelial and smooth muscle cells (51). Poly-mer surface modification by chemical means(for example, plasma discharge) or proteinadsorption may also be desirable. The latterapproach may be useful in designing materi-als that interact appropriately with cells, butit may be difficult to design materials thatselectively support endothelial cell adhe-sion. Materials that promote endothelial cellattachment unfortunately often simultane-ously promote attachment of platelets andsmooth muscle cells, with the attendant
924
adverse effects of clotting and pseudointimalthickening. Polymers have recently beendesigned that contain a cell adhesion ligandspecific for endothelial cells (52).
There are 18 million human blood trans-fusions in the United States annually. Be-cause donor blood suffers from problems oflimited storage time, donor shortage, re-quirements for typing and cross-matching,and infectious disease transmission, there isa critical need for blood cell substitutes.Red blood cells provide a number of func-tions, one of which is oxygen transport.Oxygen-containing fluids or materials offerenormous applications for use in emergencyresuscitation, angioplasty, shock, tumortherapy, exchange transfusion, and organpreservation. Several oxygen transportersare under development. A primary candi-date is hemoglobin, which not only servesas the natural oxygen transporter in bloodbut also functions in carbon dioxide trans-port, as a buffer, and in regulating osmoticpressure. Early clinical trials of cell-freehemoglobin were complicated by its lack ofpurity, instability, and high oxygen affinity,but these problems have subsequently beenaddressed by various chemical modifications(53). One remaining problem is the limitedsource of hemoglobin. It is unlikely thatthere will be sufficient outdated humanblood to prepare practical quantities of he-moglobin for widespread clinical use. Ge-netically engineered human hemoglobin orhemoglobin from bovine sources could bean alternative to human hemoglobin if notoxic effects are associated with their use.
Solutions of perfluorocarbons (PFCs;large organic molecules in which hydrogensare replaced by fluorines) dissolve 40 to70% oxygen per unit volume, nearly threetimes the oxygen-carrying capacity ofblood. PFCs are not metabolized and areimmiscible with blood. They must be emul-sified with dispersing agents such asnonionic detergents or phospholipids. Crit-ical factors in the choice of PFCs includetheir emulsifying ability, emulsion stability,tissue retention time, vapor pressure, safe-ty, and the effectiveness and safety of theemulsifying agent required. Although PFCshave advantages in terms of unlimited sup-ply and oxygen-carrying capacity, they alsohave a number of disadvantages, includingcomplement activation, toxicity, and re-tention by the reticuloendothelial system(RES), which then reduces the body's abil-ity to clear waste products (53).
Clinical trials of both modified hemoglo-bins and PFCs have been conducted. Theresults of the hemoglobin trials have varieddepending on the protocol and the specifichemoglobin preparation tested. Some stud-ies have shown allergic or toxic responses,and others have shown good tolerance andclinical improvement (for example, in a
SCIENCE * VOL. 260 * 14 MAY 1993
study of patients with sickle cell anemia).No single preparation has demonstratedclear superiority, and further study is re-quired. Clinical trials with PFCs haveshown efficacy, but toxic effects have lim-ited the current allowable dose in humans.
Research to create functional substitutesfor platelets (by encapsulating platelet pro-teins in lipid vesicles) has also been con-ducted (54). The success of this researchwill depend on the identification of themembrane proteins critical to platelet func-tion and the ability to minimize RES uptakeand toxicity.
Finally, it is possible that bone marrowstem cells could be maintained in cultureand induced to multiply and differentiateinto the various cellular elements of blood.Several culture systems are under develop-ment to foster cell division (55-57). Forexample, a combination of rapid mediumexchange and use of appropriate growthfactors has allowed up to a sixfold expan-sion of stem cells in 2 weeks (55). Mainte-nance of low oxygen concentrations (56)and the addition of stem cell factor may alsofacilitate in vitro cell expansion (58).
Future Research
Numerous research areas are critical for thesuccess of tissue engineering. Much must belearned from cell biology, such as whatcontrols cellular differentiation and growthand how extracellular matrix componentsaffect cell function (59). Immunology andmolecular genetics will contribute to thedesign of cells (for example, by gene ther-apy) or cell transplant systems that are notrejected by the immune system (60).
Cell source and cell preservation areother important issues. The transplantedcells may come from cell lines or primarytissues-from the patients themselves, oth-er human donors, animal sources, or fetaltissue. In choosing the cell source, a bal-ance must be struck between ethical issues,safety issues, and efficacy. Cryopreservationhas been used successfully for certain cells(61), but procedures need to be broadenedso that cell banks can be created for manydifferent tissues. Large-scale cell culturesystems are also important to ensure prolif-eration of needed cells in vitro prior totransplantation and to solve nutrient trans-port issues (62). Sterilization of the trans-plants is also critical.
The materials used in tissue engineeringrepresent a major area of study. Naturalmaterials are advantageous in that theycontain information (for example, particu-lar amino acid sequences) that facilitatescell attachment or maintenance of differen-tiated function. Countering this advantageis the fact that many natural materials sufferbatch-to-batch variations or scale-up diffi-

culties. Synthetic polymers, on the otherhand, allow precise control over molecularweight, degradation time, hydrophobicity,and other attributes, yet they may not inter-act with cells in a desired manner. Recently,the advantages of both natural and syntheticpolymers have been combined in strategieswhereby critical amino acid sequences fromnatural polymers are grafted onto syntheticpolymers (63). Polymer processing is anoth-er key issue. Many implants are made ofcomposite materials or highly porous struc-tures; methods of manufacturing such im-plants reproducibly may be crucial to theirsuccess (64). The development of controlledrelease systems, which deliver moleculesover long time periods, will be important inadministering numerous tissue-inducing fac-tors, growth factors, and angiogenesis stim-ulators (65). Finally, it will be useful todevelop methods of surface analysis forstudying interfaces between cell and materi-als (66) and mathematical models (67) andin vitro systems (68) that can predict in vivocellular events.
Current methods of transplantation andreconstruction are among the most costlytherapies available today. Tissue engineeringoffers the possibility of substantial future sav-ings by providing substitutes that are lessexpensive than donor organs and by providinga means of intervention before patients arecritically ill. In addition, cell transplant sys-tems may complement gene therapy ap-proaches in facilitating transfer of large popu-lations of cells expressing a desired phenotype.Few areas of technology will require moreinterdisciplinary research than tissue engi-neering or have the potential to affect morepositively the quality and length of life.
REFERENCES AND NOTES
1. Data derived from American Heart Association,American Diabetes Association, American LiverFoundation, American Lung Foundation, Ameri-can Kidney Foundation, Muscular Dystrophy As-sociation, Industry sources, National Institute ofNeurological Disorders and Stroke, and AmericanAcademy of Orthopedic Surgeons.
2. Procedure number: National Inpatient Profile 1991Data, Hospital Discharge Survey; length of stay:1991 Diagnostic Related Groupings, FederalRegister, Department of Health and Human Ser-vices (Medicare-based information).
3. W. J. Kolf' and H. T. S. Berk, Acta Med. Scand.177, 121 (1944); J. E. Murray, J. P. Merrill, J. H.Harrison, Surg. Forum 6, 432 (1955); E. D. Tho-mas et al., N. Engl. J. Med. 292, 832 (1975).
4. American Liver Foundation, Vital Statistics of theUnited States, 1988, vol. II, part A.
5. Annual Report of the U.S. Scientific Registry forOrgan Transplantation and The Organ Procure-ment and Transplant Network, 1990, United Net-work for Organ Sharing, Richmond, VA; and TheDivision of Organ Transplantation, Health Re-sources and Services Administration, Bethesda,MD, pp. ES9 and 19.
6. K. Kusama, W. I. Donegan, T. G. Samter, Dis.Colon Rectum 32, 694 (1989).
7. R. Skalak and C. F. Fox, Eds., Tissue Engineering(Liss, New York, 1988); R. M. Nerem, Ann.Biomed. Eng. 19, 529 (1991).
8. 0. Lindvall et al., Prog. Brain Res. 82, 729 (1990).9. P. Aebischer, P. A. Tresco, S. R. Winn, L. A.
Greene, C. B. Jaeger, Exp. Neurol. 111, 269(1991).
10. J. Sagen, ASAIO J. 38, 24 (1992).11. R. Madison, Exp. Neurol. 88, 767 (1985); R. F.
Valentini, T. G. Vargo, J. A. Gardella, Jr., P.Aebischer, Biomaterials 13, 183 (1992); A. S.Chang and 1. V. Yannas, in Neuroscience Year, B.Smith and G. Adelman, Eds. (Birkhauser, Boston,1992), pp. 125-126.
12. V. Gudnard, N. Kleitman, T. K. Morrissey, R. P.Bunge, P. Aebischer, J. Neurosci. 12, 3310(1992).
13. P. Aebischer, A. N. Salessiotis, S. R. Winn, J.Neurosci. Res. 23, 282 (1989); C. E. Beaty and W.M. Saltzman, J. Controlled Release, in press.
14. H. Kobayashi, Y. Ikada, T. Moritera, Y. Ogura, Y.Honda, J. Appl. Biomater. 2, 261 (1991); V.Trinkaus-Randall et al., Invest. Opthalmol. Vis.Sci. 29, 393 (1988); K. P. Thompson etal., Refrac-tive Corneal Surg. 7, 240 (1991); R. Sipehia, A.Garfinkle, W. B. Jackson, T. M. S. Chang, Biom-ater. Artif. Cells Artif. Organs 18, 643 (1990).
15. I. V. Yannas, J. F. Burke, D. P. Orgill, E. M.Skrabut, Science 215, 174 (1982); D. Heimbachetal., Ann. Surg. 208, 313 (1988); D. Michaeli andM. McPherson, J. Burn Care Rehabil. 11, 21(1990); R. Stern, M. McPherson, M. T. Longaker,ibid., p. 7.
16. G. F. Murphy, D. P. Orgill, I. V. Yannas, Lab.Invest. 63, 305 (1990).
17. H. Green, 0. Kehinde, J. Thomas, Proc. Nati.Acad. Sci. U.S.A. 76, 5665 (1979); C. C. Comptonetal., Lab. Invest. 60, 60 (1989); M. Nave, J. BurnCare Rehabil. 13, 130 (1992).
18. J. F. Hansbrough et al., Surgery 1 1 1, 438 (1992).19. E. Bell, B. lversson, C. Merrill, Proc. Nati. Acad.
Sci. U.S.A. 76, 1274 (1979).20. M. L. Yarmush, J. C. Y. Dunn, R. G. Tompkins, Cell
Transplant. 1, 323 (1992).21. J. C. Hager et al., Trans. Am. Soc. Artif. Intern.
Organs 24, 250 (1978); Z. Cai, Z. Sni, M. Sher-man, A. M. Sun, Hepatology 10, 855 (1989); G. D.M. Wells, M. M. Fisher, M. V. Sefton, Biomaterials,in press; D. E. R. Sutherland, M. Numata, A. J.Matas, R. L. Simmons, J. S. Najarian, Surgery 82,124 (1977); A. A. Demetriou et al., Science 233,1 190 (1986); A. A. Demetriou et al., Hepatology8,1006 (1988); J. A. Thompson et al., Proc. Nati.Acad. Sci. U.S.A. 86, 7928 (1989); J. A. Thomp-son et al., ibid. 87, 1625 (1990); L. G. Cima et al.,J. Biomech. Eng. 113,145 (1991).
22. J. C. Y. Dunn, R. G. Tompkins, M. L. Yarmush,Biotechnol. Prog. 7, 237 (1991).
23. D. J. Mooney et al., J. Cell Physiol. 151, 497(1992).
24. A. G. Mikos etal., Biotechnol. Bioeng., in press; A.Rotem, M. Toner, R. A. Tompkins, M. C. Yarmush,ibid. 40,1286 (1992).
25. S. Uyama, P.-M. Kaufmann, T. Takeda, J. P.Vacanti, Transplantation, in press.
26. S. J. Sullivan et al., Science 252, 718 (1991).27. P. E. Lacy, 0. D. Hegre, A. Gerasimidi-Vazeou, F.
T. Gentile, K. E. Dionne, ibid. 254, 1782 (1991).28. F. Lim and A. M. Sun, ibid. 210, 908 (1980); G. M.
O'Shea, G. M. F. Goosen, A. M. Sun, Biochim.Biophys. Acta 804, 133 (1984); M. E. Sugamoriand M. V. Sefton, Trans. Am. Soc. Artif. Intern.Organs 35, 791 (1989); L. Levesque, P. L.Brubaker, A. M. Sun, Endocrinology 130, 644(1992); Z.-P. Lum, M. Krestow, I. T. Tai, I. Vacek,A. M. Sun, Transplantation 53, 1180 (1992).
29. M. Tachibana, G. R. Nagamatsu, J. C. Addonizio,J. Urol. 133, 866 (1988).
30. A. Atala et al., ibid. 148, 658 (1992).31. M. F. Grower, E. A. Russell, Jr., D. E. Cutright,
Biomater. Artif. Cells Artif. Organs 17, 291 (1989).32. J. P. Vacanti et al., J. Pediatr. Surg. 23, 3 (1988).33. H. Uludag, T. K. Ip, P. Aebischer, Int. J. Artif.
Organs 13, 93 (1990).34. V. C. Mow, A. Ratcliffe, A. R. Poole, Biomaterials
13, 67 (1992).35. K. R. Stone, W. G. Rodkey, R. J. Webber, L.
McKinney, J. R. Steadman, Clin. Orthop. Relat.Res. 252, 129 (1990).
36. D. A. Grande, M. I. Pitman, L. Peterson, D.Menche, M. Klein, J. Orthop. Res. 7, 208 (1989);M. Takigawa et al., Bone Miner. 2, 449 (1987).
37. S. Wakitani et al., J. Bone Jt. Surg. 71 B, 74 (1989).38. C. Vacanti, R. Langer, B. Schloo, J. P. Vacanti,
Plast. Reconstr. Surg. 88, 753 (1991); H. P. vonSchroeder, M. Kwan, D. Arniel, R. D. Coutts, J.Biomed. Mater. Res. 25, 329 (1991).
39. L. Freed et al., J. Biomed. Mater. Res. 27, 11(1993).
40. M. D. Buschmann, Y. A. Gluzband, A. J. Grodzin-sky, J. H. Kimura, E. B. Hunziker, J. Orthop. Res.10, 745 (1992).
41. L. Freed, G. Vunjak-Novakovic, R. Langer, J. Cell.Biochem. 51, 257 (1993).
42. D. E. Mark, Plast. Reconstr. Surg. 86, 623 (1990).43. L. L. Hench, J. Am. Ceram. Soc. 74,1487 (1991);
M. Spector, in Non-Cemented Total Hip Arthro-plasty, R. Fitzgerald, Jr., Ed. (Raven Press, NewYork, 1988), pp. 69-85.
44. D. M. Toriumi, H. S. Kotler, D. P. Luxenberg, M. E.Holtrop, E. A. Wang, Arch. Otolaryngol. HeadNeck Surg. 1 17,1101 (1991); A. W. Yasko et al., J.Bone Jt. Surg. 74A, 659 (1992). M. Noda and J. J.Camilliere, Endocrinology 124, 2991 (1989).
45. J. Goshima, V. M. Goldberg, A. I. Caplan, Clin.Orthop. Relat. Res. 269, 274 (1991); S. E. Haynes-worth, J. Goshima, V. M. Goldberg, A. I. Caplan,Bone13,81 (1992).
46. C. Webster and H. M. Blau, Somatic Cell Mol.Genet. 16, 557 (1990); T. A. Partridge, J. E.Morgan, G. R. Coulton, E. P. Hoffman, L. M.Kunkel, Nature 337, 176 (1989); G. Acsadi et al.,ibid. 352, 815 (1991).
47. E. Gussoni et al., Nature 356, 435 (1992); S. M.Hughes and H. M. Blau, ibid. 345, 350 (1990).
48. D. Marelli, C. Desrosiers, M. El-Alfy, R. C. Kao, R.C. J. Chiu, Cell Transplant. 1, 383 (1992).
49. P. Galletti, P. Aebischer, H. F. Sashen, M. B.Goddard, T.-M. Chiu, Surgery 103, 231 (1988); M.A. Golden, S. R. Hanson, T. R. Kirkman, P. A.Schneider, A. W. Clowes, J. Vasc. Surg. 11, 838(1990); H. P. Griesler et al., ibid. 9, 588 (1989).
50. B. E. Jarrell and S. K. Williams, J. Vasc. Surg. 13,733 (1991); J. M. Wilson etal., Science 244, 1344(1989); E. G. Nabel, G. Plautz, F. M. Boyce, J. C.Stanley, G. J. Nabel, ibid., p. 1342.
51. A. W. Clowes and T. Kohler, J. Vasc. Surg. 13, 734(1991).
52. J. A. Hubbell, S. P. Massia, N. P. Desai, P. D.Drumheller, Biotechnology 9, 586 (1991).
53. T. M. S. Chang, in Blood Substitutes, T. M. S.Chang and R. P. Geyer, Eds. (Dekker, New York,1989), pp. 11-29; R. A. Kahn, R. W. Allen, J.Baldassare, Blood 66, 1 (1985); R. P. Geyer, inBlood Substitutes, T. M. S. Chang and R. P.Geyer, Eds. (Dekker, New York, 1989), pp. 31-49;F. DeVenuto, Biomater. Artif. Cells Artif. Organs16, 77 (1988); L. R. Manning et al., Proc. Nati.Acad. Sci. U.S.A. 88, 3329 (1991).
54. J. J. Baldassare, R. A. Kahn, M. A. Knipp, P. J.Newman, J. Clin. Invest. 15, 35 (1985); P. Sie etal., Biochem. Biophys. Res. Commun. 97, 133(1980); L. V. Parise and D. R. Phillips, J. Biol.Chem. 260,1750 (1985).
55. R. M. Schwartz, B. 0. Pallson, S. G. Emerson,Proc. Nati. Acad. Sci. U.S.A. 88, 6760 (1991); R.M. Schwartz, S. G. Emerson, M. F. Clarke, B. 0.Pallson, Blood 78, 3155 (1991).
56. M. R. Koller, J. G. Bender, E. T. Papoutsakis, W.M. Miller, Blood 80, 403 (1992).
57. B. A. Naughton, A. Tjota, B. Sibanda, G. K.Naughton, J. Biomech. Eng. 113, 172 (1991).
58. K. M. Zsebo et al., Cell 63, 195 (1990).59. N. Le Douarin, Nature 280, 663 (1980); R. 0.
Hynes, Cell 48, 549 (1987); A. W. Stoker, C. M.Streulig, M. Martins-Green, M. J. Bissell, Curr.Opin. Cell Biol. 2, 864 (1990); I. V. Yannas,Angew. Chem. 29, 20 (1990).
60. F. P. Sullivan et al., Transplantation 44, 465(1987); C. Ricordi, D. W. Scharp, P. E. Lacy, ibid.45, 994 (1988); A. M. Posselt et al., Science 249,1293 (1990); M. Sykes et al., Transplantation 55,197 (1993).
61. I. H. M. B. Rinkes, M. Toner, S. J. Sheehan, R. G.
SCIENCE * VOL. 260 * 14 MAY 1993
EMI-Em-
925

Tompkins, M. L. Yarmush, Cell Transplant. 1, 281(1992).
62. W.-S. Hu and M. V. Peshway, Can. J. Chem. Eng.69, 409 (1991).
63. J. A. Hubbell, S. P. Massia, P. P. Drumheller, Ann.N.Y Acad. Sci. 665, 253 (1992); H.-B. Lin et al.,Biomaterials 13, 905 (1992); D. Barrera, A. Adri-anov, R. Langer, paper presented at the Annualmeeting of the American Institute of ChemicalEngineers, Miami, FL, 5 November 1992.
64. A. G. Mikos et al., J. Biomed. Mater. Res. 27,183(1993).
65. R. Langer, Science 249, 1527 (1990).66. B. D. Ratner et al., J. Vacuum Sci. Technol. A8,
2306 (1990).67. D. A. Lauffenberger, Annu. Rev. Biophys. Chem.
20, 387 (1991).68. H.-E. Hsieh, N.-Q. Li, J. A. Frangos, J. Cell Phys-
iol. 154,143 (1993); R. M. Nerem and P. R. Girard,Toxicol. Pathol. 18, 572 (1990); M. R. Parkhurstand W. M. Saltzman, Biophys. J. 61, 306 (1992);S. Guido and R. T. Tranquillo, J. Cell Sci., in press.
69. L. Christenson, K. E. Dionne, M. J. Lysaght, inFundamentals ofAnimal Cell Encapsulation andImmobilization, M. F. A. Goosen, Ed. (CRCPress, Boca Raton, FL, 1993), pp. 7-41.
70. R. P. Lanza, S. J. Sullivan, W. L. Chick, Diabetes41, 1503 (1992).
71. To address this problem, several approaches are
under study: (i) purifying alginates [A. M. Sun, I.Vacek, I. Tai, in Microcapsules and Nanoparticlesin Medicine and Pharmacy, M. Donbrow, Ed.(CRC Press, Boca Raton, FL, 1992), pp. 315-322]; (ii) synthesizing hydrogels with polyethyleneoxide chains (which are relatively resistant toprotein and cell adsorption) on their surface [A. S.Sawhney and J. A. Hubbell, Biomaterials 13, 863(1992)]; (iii) encapsulating cells with syntheticpolymers that have good biocompatibility, suchas polyacrylates-interestingly, procedures forusing polyacrylates expose cells to organic sol-vents, yet viability and function of a number ofmammalian cell types are retained [M. V. Sefton,L. Kharlip, V. Marvath, T. Roberts, J. ControlledRelease 19, 289 (1992); H. Uludag and M. V.Sefton, Biotech. Bioeng. 39, 672 (1992)]; and (iv)synthesizing polymers that form gels upon expo-sure to ions in water (for example, certain poly-phosphazenes) [S. Cohen et al., J. Am. Chem.Soc. 119, 7832 (1990)].
72. We thank J. Stoudemire and L. Blankstein forassistance, and J. Hubbell, G. Naughton, S. Wein-stock, H. Blau, R. Tompkins, R. Pops, and C.Mullon for reviewing the manuscript. Supportedby Advanced Tissue Sciences, Inc., La Jolla, CA,NSF, NIH, the Thomas Anthony Pappas Charita-ble Foundation, Inc., and the Holly Ann SoulardResearch Fund.
The Basic Science ofGene Therapy
Richard C. MulliganThe development over the past decade of methods for delivering genes to mammalian cellshas stimulated great interest in the possibility of treating human disease by gene-basedtherapies. However, despite substantial progress, a number of key technical issues needto be resolved before gene therapy can be safely and effectively applied in the clinic. Futuretechnological developments, particularly in the areas of gene delivery and cell transplan-tation, will be critical for the successful practice of gene therapy.
Ever since the development of recombi-nant DNA technology, the promise of thetechnology for dramatically improving thepractice of medicine has been vigorouslychampioned. Most of the advances affect-ing the clinical management of patientshave involved either the development ofnew molecular techniques for the diagnosisof specific inherited and acquired diseases orthe development of new therapeutic prod-ucts made possible by the ability to engineerthe overexpression of specific genes. Re-combinant DNA technology has also pro-duced the means for defining the roles ofspecific gene products in the pathogenesisof human disease. The ability to character-ize disease in such molecular terms hasalready led to more precise and effectiveclinical interventions.
However, the idea underlying gene ther-apy-that human disease might be treatedThe author is at the Whitehead Institute for BiomedicalResearch and Department of Biology, MassachusettsInstitute of Technology, Cambridge, MA 02142.
926
by transfer of genetic material into specificcells of a patient, rather than by conven-tional drugs-has yet to make its mark inmedicine. Although the concept may ap-pear to be elegantly straightforward and themost direct application of recombinantDNA technology, research has indicatedthat successful implementation of genetransfer in the clinic will require the coor-dinated development of a variety of newtechnologies and the establishment ofunique interactions between investigatorsfrom divergent medical and basic sciencedisciplines.
Although several reviews of gene thera-py research have been published (1), fewhave focused on the technical issues thatcontinue to impede the translation of pre-clinical studies of gene therapy into effec-tive clinical protocols. In this review andcommentary, I have attempted to definethose issues and to suggest new areas ofinvestigation that may help to resolvethem.
Development of Methods forGene Delivery
The transduction of appropriate target cellsrepresents the critical first step in gene
therapy; consequently, the development ofmethods of gene transfer suitable for differ-ent forms of therapy has been a major focusof research (Table 1). The single commonfeature of these methods is the efficientdelivery of genes into cells. In the case ofretroviral vectors and adeno-associated vi-rus vectors, the transferred DNA sequences
are stably integrated into the chromosomalDNA of the target cell. These vectors havebeen considered most often for ex vivo gene
therapy, which involves removal of therelevant target cells from the body, trans-duction of the cells in vitro, and subsequentreintroduction of the modified cells into thepatient. All of the other methods of gene
transfer result primarily in the introductionof DNA sequences into the nucleus in an
unintegrated form. Those methods, whichresult in high, but transient, gene expres-
sion, have predominantly been consideredfor use in in vivo gene therapies, in whichgenetic material is directly transferred intocells and tissues of the patient. As discussedbelow, little is known about the fate andproperties of DNA delivered to cells bythese other methods.
Retroviral vectors. Interest in retrovirus-mediated gene transfer stems primarily fromthe ability of some vectors to stably trans-duce close to 100% of target cells.
Although retrovirally mediated gene
transfer is ideal for many ex vivo applica-tions of gene therapy, several features of thegene transfer method may limit its applica-bility, particularly with regard to in vivotherapies. First, retrovirus entry into cells isabsolutely dependent on the existence ofthe appropriate viral receptor on the targetcell. To provide a means of infecting mostcells of interest, researchers have developedpackaging cell lines capable of generatingviruses Qf a variety of host ranges (2).Because the identities of most retroviralreceptors are unknown, however, it has notbeen possible to determine the distributionof receptors in different cell types. Problemsencountered in transducing specific celltypes (such as hematopoietic stem cells)may be due, in part, to the lack of expres-sion of appropriate viral receptors. Second,replication of the target cells is necessary forproviral integration to occur. Althoughpreviously it had been assumed that thisrequirement reflected the necessity forDNA synthesis, recent studies suggest thatviral integration may depend on mitosis(3). Thus, successful gene transfer dependson the ability to induce proliferation of the
target cell, at least for short periods of time.Another problem is that the retroviral
SCIENCE * VOL. 260 * 14 MAY 1993
11In
- -1 ll-1'IS. 1111 ---M ..... ......l 'I'M