Embed Size (px)
Citation preview

Occupational and Environmental Medicine 1997;54:289-295
METHODOLOGY Series editors: T C Aw, A Cockcroft, R McNamee
Time to pregnancy: a measure of reproductivefunction in either sex
Michael Joffe, Asclepios project (appendix)
AbstractIntroduction-Growing evidence ofreproductive effects associated with occu-pational and environmental agents hascreated the need for research with sensi-tive and well validated methods. There isa complex relation between manifesteffects and underlying pathogenicprocesses. Conceptions will on averagetend to be delayed in a populationexposed to an agent that causes embry-onic damage, an increase in germ cellmutations, or decreased fertility.Studying time to pregnancy-Time topregnancy can be used to measure thedegree of delay in conceiving, across thewhole continuum of biological fertility, ineither men or women. The distribution oftime to pregnancy largely reflects a sort-ing process, as the more fertile couplesbecome progressively less well repre-sented with the passage of time. The basicresearch strategy is comparison of thetime to pregnancy within groups definedby their exposures, allowing for potentialconfounding factors relating not only tothe study subject but also to his or herpartner.Measurement and validity-Prospectiveand retrospective methods are available,and each has strengths and weaknesses.Prospective studies have some theoreticaladvantages, but have unrepresentativepopulations and problems of feasibilityand cost. Retrospective assessment oftime to pregnancy is feasible with a shortquestionnaire, without intruding into sen-sitive areas of respondents' lives, withgood validity at the group level, and with-out the necessity of large populations.Potential biases have been identified thatcan be minimised by careful design andanalysis; the principal remaining problemis difficulty in obtaining exposure dataretrospectively.
(Occup Environ Med 1997;54:289-295)
the effect could be recognised relatively easilybecause the particular defect, phocomelia, wasvanishingly rare in the absence of the drug. Itwould be far more difficult to recognise anincrease in a common abnormality, even if thiswere responsible for many cases.
Congenital malformations have enormousemotional and practical implications for thoseaffected. However, there are many other waysin which reproductive processes can be dis-rupted.
There is growing evidence that occupationalfactors can adversely affect reproductiveprocesses. This is relevant both because manywomen have now joined the workforce, andbecause of the possibility of male mediatedeffects. Much exploratory work has been done,with linkage of routine data sets in those coun-tries where these exist, case control studies,and relatively insensitive indicators such asdemographic fertility (number and timing ofbirths).
At present, evidence for or against repro-ductive or genetic toxicity of specific agentsstill exists only for a few of those in commonuse-for example, ionising radiation, lead, andthe soil fumigant dibromochloropropane(DBCP). There is also epidemiological evi-dence which refers to groups of agents or tobroad occupational categories, such as expo-sure to organic solvents or work in the elec-tronics industry. In general, the informationavailable is seriously incomplete, and the lackof satisfactory evidence cannot be taken toindicate lack of effect.
Research is now urgently needed, with themore sensitive methods that have been devel-oped in recent years. The purpose of thispaper is to describe the use of the time takento conceive, time to pregnancy, to assessreproductive function in either sex. The focus ismainly on short questionnaires for use in ret-rospective cohort studies. Before describingthe method and outlining what is known aboutits validity, it is necessary to understand howtime to pregnancy relates to other reproduc-tive end points, and to the underlying biology.
Department ofEpidemiology andPublic Health,Imperial CollegeSchool of Medicine atSt Mary's, NorfolkPlace, London W2 lPGM JoffeAccepted 3 September 1996
Keywords: research methods; questionnaires; time topregnancy
Why study time to pregnancy?Over 30 years ago, the thalidomide tragedyshowed that a chemical agent can cause devas-tating reproductive damage. In that instance,
Biological dysfunction and manifest effectSeveral biological processes are involved inreproductive and genetic damage, and thereare also several possible outcomes that couldbe found among those affected. The interrela-tion of these is not one to one: figure 1 showsan overview of the links between them. I
289
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from

290
Figure 1 Overview ofpossible relations betweenbiological dysfunction andmanifestation inreproductive outcomes(adapted withpermission).
Biological dysfunction
Endocrine dysfunction
Gonadal damage
Gametotoxicity
Oocyte maturation dysfunction
Germ cell mutation
Gamete transport dysfunction
Implantation dysfunction
Embryotoxicity
Fetotoxicity
Breast milk toxicants-
Effect
Reduced libido
Menstrual dysfunction
Reduced fertility
Miscarriage
Malformation
Perinatal death
,-Low birthweight
WPreterm birth
Altered sex ratio
Organ dysfunction
Cancer or disease in child
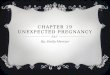
A given pathogenic process can result in dif-ferent manifestations. For example, anincrease in germ cell mutations can cause vari-ous types of adverse health effects (fig 2):manifest genetic disease; increased frequencyof heterozygous (carrier) status of recessivedisorders; cancer, especially that occurring inchildhood; and those congenital defects whichhave an important genetic component. Withineach of these categories, many different clini-
cal conditions would be included. For exam-ple, a range of genetic diseases would occur,each one being rare; it would therefore be diffi-cult to detect an increased risk in a particularpopulation. Also, one would expect dominanteffects causing fetal death, manifest as perinataldeath or miscarriage, or embryonic death,which would be apparent only as a cycle dur-ing which conception did not occur, so that aclinically manifest pregnancy takes longer to
Figure 2 Possibleconsequences ofgernm cellmutation (adapted withpermission).'
Biological dysfunction
Germ cell mutation
Effect
Reduced fertility, (apparent non-conception)
Embryonic lossMiscarriage
* Malformation
Perinatal death
Altered sex ratioo
Cancer or leukaemia in child
Other disease of child (genetic)
'Recessive genes - carrier
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from

Time to pregnancy: a measure of reproductive function in either sex
Figure 3 Possibleantecedents of delayedconception (adapted withpermission). '
Biological dysfunction Effect
Endocrine dysfunction
Gonadal damageGametotoxicity
Oocyte maturation dysfunction * Reduced fertility
Germ cell mutation
Gamete transport dysfunction
Implantation dysfunctionEmbryotoxicity
conceive. At a group level, it would be mani-fest as a tendency for delay in conception in anexposed population.On the other hand, a given manifestation
can result from several types of biological dys-function. For example, delay in conceptionmay result not only from germ cell mutationbut also from embryotoxicity (some embry-otoxic agents are teratogens), as well asreduced biological fertility in a more literalsense, which can be due to toxic effects on thegamete, or gonad, or both, or to endocrineeffects (fig 3); in some cases, a decrease inlibido can also occur as a result of exposure tochemical agents. Most of these biologicalmechanisms can affect either sex.
The concept of time to pregnancyThe phrase "delay in conception" has beenused to indicate that on average, the couples ina particular population take longer to produce aclinically recognizable pregnancy. This isalways relative, a matter of comparing exposedand non-exposed conceptions, as there is noabsolute standard.
It has long been recognised that humanpopulations have a wide range of reproductivecapacity: whereas some couples have a highprobability of conception in a particular men-strual cycle, other couples have fertility that islow, or even zero (sterility). It is important torecognise that there is a smooth continuumbetween these extremes, and that categorisa-tion into fertile and subfertile or infertile isnecessarily arbitrary. As very fertile coupleshave a higher probability of conception within afew months of beginning unprotected inter-course, they are relatively unrepresentedamong couples who take a long time to con-ceive: thus, time to pregnancy measures aprocess that is partly a matter of sorting cou-ples according to their degree of fertility, andpartly a probabilistic occurrence for each cou-ple, given their degree of fertility.The most convenient way of representing
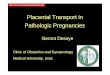
time to pregnancy is as a cumulative percent-age curve (fig 4).2 The probability of concep-tion in the first month is typically around 0 3,and gradually diminishes throughout the dis-tribution; 50% of couples conceive within twomonths, and over 80% in six months; evenafter at least five years of non-conception haveelapsed, the probability of conception is
greater than zero, so that the curve goes onsingg'The practical importance of these findings
is that it is much more statistically efficient tocompare the time to pregnancy distributionsof exposed and non-exposed populations thanto compare proportions of those defined asclinically subfertile (no conception within forexample, 12 months). Also, just one part ofthe curve may be affected, the classic casebeing recent use of the oral contraceptive pillwhich tends to delay conception in the earlymonths, but does not affect the probability ofconception in the long term.4
Study designThe natural design for studying time to preg-nancy is a cohort study, populations beingdefined in terms of exposure status. The basicstrategy is the comparison of the time topregnancy distributions of exposed and non-exposed populations, or better, of subpopula-tions with differing degrees of exposure.
Research is typically aimed at studying onlymale mediated or female mediated effects, butthe degree of fertility is a property of the couple,so potential confounding factors for both part-ners are needed. As in any epidemiological
100
>.a)
E0
-3 0 3 6 9 12 15 18 21 2
Time to pregnancy (months)
Figure 4 Comparison of time to pregnancy distributionsrecorded concurrently in the Oxford Family PlanningAssociation study database and reported in a short sealcompletion questionnaire, for 1392 matched pregnancies(taken with permission).2
I
291
24
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from

2Joffe
study, every effort should be made to measureall variables that could be associated both withthe outcome (time to pregnancy) and with theexposures of interest.
However, because the comparison is ofpopulations, it is not essential to include infor-mation on every factor that could affect fertility.For example, in an individual case, conceptioncould be delayed because illness or travel leadto an interruption in the sexual life of a couple.At the population level, this would only beimportant if an exposure group was especiallypredisposed to such events. The assumptioncan often be made that such factors are equallybalanced between groups, or that their effect issmall at the population level. The practicalimportance is that one does not have toacquire information at this level of detail,which is fortunate, as intimate questioning ofthis nature would not be appropriate for theoccupational situation.
Similarly, although the frequency of inter-course is associated with the probability ofconception, it is not essential to collect suchdata: it can often be assumed that its distribu-tion is similar in the different exposure groups.In the special case of an agent that affects thelibido, adjustment for frequency of intercoursewould even obscure the adverse effect of theagent.
Measuring time to pregnancyTime to pregnancy is a functional measure,corresponding not to any specific biologicalprocess, but rather to the final common pathof conception. There are two approaches to itsmeasurement, prospective and retrospective,corresponding to prospective and retrospectivecohort study designs.
Conceptions that occurred in the presenceof a normally effective method of contracep-tion are excluded from consideration, so thattime to pregnancy is only measured for thatcategory of pregnancies that were conceivedby couples who had embarked upon a periodof unprotected intercourse. In principle, it isessential to base this distinction on actualbehaviour and its biological implications,rather than on subjective aspects such aswhether the couple was planning a pregnancyor trying to conceive.
In practice, this is especially problematic forprospective studies, as it affects recruitment:participating couples are likely to be those whoare actively planning, so that those who have amore relaxed approach will be underrepre-sented. Retrospective studies have less of aproblem in this respect, as the research popula-tion initially includes all pregnancies, and thedecision is then which to exclude from theanalysis, based on reported contraceptivebehaviour; including knowledge of the expo-sure status of those excluded, any resultingbias can be evaluated. Also, the inherentlyblurred definitions involved can be exploredstatistically by carrying out a sensitivity analysis(described later).The prospective method uses either a mani-
fest biological outcome (birth of a baby),4 or a
pregnancy test.5 In the pregnancy test, a uri-nary human chorionic gonadotrophin (HCG)assay detects pregnancy within a few days afterimplantation of the fertilised ovum. Selectionbias can arise, not only because those whotend to plan their pregnancies are favoured, asalready mentioned, but also due to the needfor participants to declare their intention toconceive, which they may be reluctant to do,especially in an occupational context. An addi-tional problem, which is more fundamental, isthat a sampling frame may not exist; however,this does not apply to occupational studies.Finally, problems of feasibility and cost limitthe use of this approach, as large populationsare required to generate enough pregnanciesfor study.An early example of a prospective study was
from the Oxford Family Planning Associationcontraceptive study, which showed that recentuse of oral contraceptives was associated withan increased time to birth;4 a subsequentreport showed the effect of maternal smoking.6A more recent study in an occupational con-text, with a urinary pregnancy test, was con-cerned with physical activity.7
Retrospective questionnaire based studieshave two important advantages. Firstly, manypregnancies are readily obtained (althoughonly some of these are exposed pregnancies).Secondly, it is possible to study a historicalperiod when exposures were considerablyhigher than at present; companies which havemade improvements may be more motivatedto take part in the research. A limitation is thatexposure data may be difficult to obtain forearlier periods, and information on potentialconfounding factors is likely to be less accu-rate.Some studies have been carried out with
comparatively long duration of recall, of theorder of 10 years or more. Others focus onlyon pregnancies conceived within a few yearsbefore the research, and so have advantages-such as the use of more detailed questioning,based on discrete menstrual cycles, and eventssuch as illness or separation that occurred at aparticular time; information on exposures andconfounding can be expected to be more reli-able than with longer recall. On the otherhand, the advantages listed in the previousparagraph increase with the duration of recall.An example of an occupational study that
used relatively short recall is that of nitrousoxide exposure among dental assistants;8 astudy of pharmacy assistants focused on preg-nancies occurring up to seven years previ-ously;9 and a study of exposure to pesticidesamong fruit growers used a 12 year period.10
In designing the questionnaire, it is advis-able to focus on a single pregnancy, for tworeasons: it is not statistically justifiable toinclude more than one pregnancy per couple,as these are not independent; and the moredefined focus allows detailed questioning onpotential confounding factors.
In the questionnaire that is being used inthe Asclepios project, a major European col-laborative study of male fertility in the occupa-tional context, the most recent birth has been
292
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from

Time to pregnancy: a measure of reproductive function in either sex
chosen as the pregnancy of interest. The rea-son for restriction to births is that ascertain-ment of the occurrence and timing of births isclearer than in the case of miscarriages thatavoid pregnancy recognition bias;" further-more, the recall of time to pregnancy is almostcertainly better when an actual child isinvolved. The most recent one is studiedbecause the man is more likely to be in thesame industry if this is chosen; in other words,it is the one most likely to be an exposed preg-nancy.
Restriction of data collection to births raisesthe possibility previously mentioned, that anexposure may affect both fertility and the riskof miscarriage; pregnancies that miscarry tendto take slightly longer to conceive.'2 Summarydata on all pregnancies is therefore also col-lected so that the miscarriage rate can also beestimated, as an additional outcome variable.
In the Asclepios questionnaire, exposureinformation is focused on the time 12 monthsbefore the baby was born, thus allowing ninemonths for the pregnancy and up to threemonths for spermatogenesis and spermiogene-sis. This is not ideal, as exposures (and con-founding factors) can vary during the waitingtime before conception occurs. However, thiswill predominantly affect the relatively fewcouples with a long time to pregnancy, not thebulk of the population in each exposure groupwhich is where the statistical power lies.Information on any other phases of infertilityis also collected, which is important for thosewho have never conceived.
Potential confounding factors include age,smoking habit, and educational level of bothparents, maternal occupation (for possiblechemical exposures and occupational class),the last method of contraception (includingbreast feeding), and relevant medical condi-tions such as pelvic inflammatory disease.Maternal parity is another potential confound-ing factor, but it should not be automaticallycontrolled for, as it reflects earlier fertility,which may be related to the exposure of inter-est.From the practical point of view in an occu-
pational context, it is vital to avoid questionsabout intimate or possibly stigmatised aspectsof respondents' lives. Fortunately this is easyin time to pregnancy studies: asking about theduration of time before conception occurredhas been found to be acceptable in a wide vari-ety of different cultural settings. Frequency ofintercourse as a possible confounding factorhas been already discussed; no other informa-tion about sexual behaviour is relevant. Theperiods of respondents' lives that are not con-nected with a birth are irrelevant, as are con-traceptive histories, casual or illicit sexualactivity, deliberate termination of pregnancy,and any period of celibacy they may have had.
Validity of retrospective questionnairedataIn reproductive studies generally, it has beenfound that recall of characteristics relating to apregnancy (and especially to an actual baby),
such as birthweight and gestational age, isremarkably accurate and durable.' This sec-tion outlines the evidence on recall of time topregnancy.
In a 1987 study, male factory workers werefound to be able to answer a questionnaireitem on time to pregnancy, in the context ofan interview study of reproductive effects ofoccupation, and the resulting distributionclosely resembled that expected from prospec-tive studies.'4 In the case of female workers,the predicted infertile worker effect' wasfound, that workplaces contain a relativelyhigh proportion of women who have not pro-duced a live birth. Apparently reasonable datawere obtained with 10 or even 20 years ofrecall.
In an American study, the validity of recallobtained with a short, self completed ques-tionnaire was compared with that from adetailed telephone interview, among 523 pre-dominantly white dental assistants.'6 All thepregnancies had occurred within four yearsbefore the study. For most covariates, discrep-ancies were non-differential, the main effect ofmisclassification thus being to reduce statisti-cal power. Accuracy was unrelated to durationof recall. Although menstrual cycles were usedin the questioning, there was some evidencethat women found it easier to think in months.
In a Dutch validity study, 132 participantsin a previous prospective study of pregnancyfailures were asked about the time to preg-nancy; duration of recall was three to 20months.'7 No systematic errors were found,but random errors were fewer with personalinterview format than with telephone interviewor self completed questionnaire. Reliability(test-retest) showed great stability of responseafter three to five weeks, in all formats. Aquestion on phases of subfertility not relatedto a pregnancy was poorly understood.A further validation study compared the
values of time to pregnancy recorded essen-tially prospectively in the Oxford FamilyPlanning Association contraceptive study withthose reported several years later when mem-bers of that study were sent a short self com-pletion questionnaire.2 18 Figure 4 shows thefindings, as a comparison at the group level.The curves are almost superimposed for mostof the distribution, with a small degree of digitpreference evident at 3, 6, 12, and 24 months.
At the individual level, considerable mis-classification was found. This was greater forlonger waiting times to pregnancy, confirmingthe view that research is best carried out as acomparison of whole distributions of time topregnancy between population groups definedin terms of exposure characteristics, ratherthan as a comparison of the proportion ofthose defined as having clinical infertility.The findings at group level are all the more
remarkable, as the median recall time was 14
years (interquartile range 11 to 16 years); asimilar graph confined to duration of recallabove the median surprisingly showed an evencloser correspondence between the twocurves.2The concept of time to pregnancy is thus
293
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from

24offe
well understood by the general population;indeed it seems to form part of lay thinking.Typically a value for time to pregnancy can beobtained from over 90% of female respon-dents, and over 80% of male respondents.'9 It isbest to ask the number of months as an openended question, rather than to group thevalues-for example, 0-3, 4-6, etc.
If interviews are being used, it seems to beuseful to provide potential respondents withadvance warning of the topics that they will beasked about. If questionnaires are to be selfcompleted in a male population, it is anadvantage if the men can take the question-naires home and complete them with theirwives.
Biases, analysis, and statistical powerThere are several potential pitfalls in thedesign, statistical analysis, and interpretationof time to pregnancy studies." Detailed dis-cussion is beyond the scope of this paper. Oneexample, pregnancy recognition bias, hasalready been mentioned. Another one, timetrend bias, resulted in a spurious protectiveeffect among dental assistants who woregloves: time to pregnancy was apparentlylonger among assistants who did not weargloves, because these women started trying toconceive before awareness of HIV was wide-spread.8 Its occurrence depended on the studypregnancies being clustered in time, andwould be much less of a problem in studieswith long duration of recall.
Survival methods are appropriate for analy-sis, including cumulative percentage graphs(similar to fig 4, equivalent to Kaplan-Meiercurves), log rank tests for bivariate analysis,and Cox regression for multivariate analysis.The Cox regression is ideal for comparingtime to pregnancy distributions between pop-ulations with different exposures, allowing forpotential confounding effects.The criterion for including pregnancies in
the basic analysis is that no effective form ofcontraception was used. In terms of the ques-tionnaire, categories of birth control in use are:(a) not at all, (b) only sometimes, (c) nearly allthe time, and (d) all the time; this meansrestricting analysis to (a) and (b). Also, toallow for the problem of blurred definitionsalready mentioned, a sensitivity analysis isneeded, restricted to only (a).
Populations do not have to be very large. Ithas previously been estimated that to detect a50% fall in the probability of conception with80% power at the 5% level of significancewould require only 55 exposed and 55 non-exposed pregnancies;20 however, this assumedperfect information and no confounding. Thedegree of misclassification at the individuallevel in retrospective data means that stableestimates probably require more like 300exposed pregnancies.
ConclusionTime to pregnancy is a sensitive measure offertility in either sex, which can be measured
prospectively or retrospectively. Eligible preg-nancies are defined in terms of objective crite-ria, relating to the use of contraception, not interms of whether the couple was wanting,intending, or trying to conceive. Time to preg-nancy is measured in menstrual cycles ormonths, and grouping into categories shouldbe avoided, as should dichotomous analysis interms of clinical infertility.
In retrospective cohort studies, with a suit-ably designed questionnaire, information canbe obtained that is valid at the group level, andsample size requirements are such that manyoccupational and environmental exposurescan be studied.
AppendixThe Asclepios project is a European Union concertedaction research project coordinated by The StenoInstitute of Public Health, University of Aarhus,Denmark, with the following participants: Belgium,Gent (P Kiss, A Mahmoud, M Vanhoorne, HVerstraclen); Denmark, Aarhus (A Abell, JP Bonde, SBrixen Larsen, G Danscher, E Ernst, H Kolstad),Copenhagen (A Giwercman); England, London (ADale, M Joffe, N Shah); Finland, Helsinki (M-LLindbohm, H Taskinen, M Sallmen), Turku (JLhhdetie); France, Paris (P Jouannet, P Thonneau);Strasbourg (A Clavert); Germany, Erlangen (KHSchaller, W Zschiesche); Italy, Brescia (P Apostoli, SPorru), Milano (L Bisanti), Pietrasanta (L Lastrucci),Rome (M Span6); Netherlands, Nijmegen (NRocleveld, H Thuis, GA Zielhuis), Zeist (W de Kort);Poland, Lodz (K Sitarek). The Asclepios project isfunded by the BIOMED programme of the EuropeanUnion, and by several complementary national sourcesof funding. The questionnaire was developed andtranslated with the aid of a grant from the Health andSafety Executive. We thank an anonymous reviewer forhelpful comments on an earlier draft.
1 Joffe M. Epidemiology of occupational reproductive haz-ards: methodological aspects. Rev Epidemiol SantePublique 1992;40:S17-25.
2 Joffe M, Villard L, Li Z, Plowman R, Vessey M. A time topregnancy questionnaire designed for long term recall:validity in Oxford, England. Jf Epidemiol CommunityHealth 1995;49:314-9.
3 Spira A. Epidemiology of human reproduction. HumReprod 1986;1: 111-5.
4 Vessey MP, Wright NH, McPherson K, Wiggins P.Fertility after stopping different methods of contracep-tion. BMJ 1978;i:265-7.
5 Canfield RE, O'Connor JF, Birken S, Krichevshy A,Wilcox AJ. Development of an assay for a biomarker ofpregnancy and early fetal loss. Environ Health Perspect1987;74:57-66.
6 Howe G, Westhoff C, Vessey M, Yeates D. Effects of age,cigarette smoking, and other factors on fertility: findings ina large prospective study. BMJ 1985;290: 1697-700.
7 Florack EI, Zielhuis GA, Rolland R. The influence of occu-pational physical activity on the menstrual cycle andfecundability. Epidemiology 1994;5:14-8.
8 Rowland A, Baird DD, Weinberg CR, Shore DL, Shy CM,Wilcox AJ. Reduced fertility among women employed asdental assistants exposed to high levels of nitrous oxide.NEnglJMed 1992;327:993-7.
9 Schaumburg I, Olsen J. Time to pregnancy among Danishpharmacy assistants. Scand J Work Environ Health 1989;15:222-6.
10 de Cock J, Westveer K, Heederick D, te Velde E, van KooijR. Time to pregnancy and occupational exposure topesticides in fruit growers in The Netherlands. OccupEnviron Med 1994;51:693-9.
11 Weinberg CR, Baird DD, Wilcox AJ. Sources of bias instudies of time to pregnancy. Stat Med 1994;13:671-81.
12 Joffe M, Li Z. Association of time to pregnancy and theoutcome of pregnancy. Fertil Steril 1994;62:71-5.
13 Joffe M. Male- and female-mediated reproductive effectson occupation: the use of questionnaire methods. Y OccupMed 1989;31:974-9.
14 Joffe M. Feasibility of studying subfertility using retrospec-tive self reports. Jf Epidemiol Community Health 1989;43:268-74.
15 Joffe M. Biases in research on reproduction and women'swork. Int_3Epidemiol 1985;14:118-23.
294
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from

Time to pregnancy: a measure of reproductive function in either sex
16 Baird DD, Weinberg CR, Rowland AS. Reporting errors intime-to-pregnancy data collected with a short question-naire: impact on power and estimate of fecundabilityratios. Am j Epidemiol 199 1;133:1282-90.
17 Zielhuis GA, Hulscher MEJL, Florack EIM. Validity andreliability of a questionnaire on fecundability. Imtt JEpidemiol 1992;21:1151 -6.
18 Joffe M, Villard L, Li Z, Plowman R, Vessey M. Long-termrecall of time-to-pregnancy. Fertil Steril 1993;60, 99-104.
19 Joffe M, Li Z. Male and female factors in fertility. Am JEpidemiol 1994;140:921-9.
20 Baird DD, Wilcox AJ, Weinberg CR. Use of time to preg-nancy to study environmental exposures. Am J Epidemiol1986;124:470-80.
Vancouver styleAll manuscripts submitted to Occup EnvironMed should conform to the uniformrequirements for manuscripts submitted tobiomedical journals (known as theVancouver style.)
Occup Environ Med, together with many
other international biomedical journals, hasagreed to accept articles prepared in accor-
dance with the Vancouver style. The style(described in full in the JAMA1) is intendedto standardise requirements for authors,and is the same as in this issue.
References should be numbered consec-
utively in the order in which they are firstmentioned in the text by Arabic numeralson the line in square brackets on each occa-
sion the reference is cited (Manson[l] con-
firmed other reports . . . [2] [3] [4] [5] . .).In future references to papers submitted to
Occup Environ Med should include: thenames of all authors if there are seven orless or, if there are more, the first six fol-lowed by et al; the title of journal articles orbook chapters; the titles of journals abbrevi-ated according to the style of Index Medicus;and the first and final page numbers of thearticle or chapter. Titles not in IndexMedics should be given in full.
Examples of common forms of refer-ences are:
1 International Committee of Medical Journal Editors.Uniform requirements for manuscripts submitted tobiomed journals. JAMA 1993;269:2282-6.
2 Soter NA, Wasserman SI, Austen KF. Cold urticaria:release into the circulation of histamine and eosino-phil chemotactic factor of anaphylaxis during coldchallenge. N Engl J Med 1976;294:687-90.
3 Weinstein L, Swartz MN. Pathogenic properties ofinvading micro-organisms. In: Sodeman WA Jr,Sodeman WA, eds. Pathologic physiology, mechanismsof disease. Philadelphia: W B Saunders, 1974:457-72.
295
on April 8, 2020 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.54.5.289 on 1 M
ay 1997. Dow
nloaded from