Embed Size (px)
Citation preview

EndocrinE
ThyrotoxicosisJohnathan Hubbard
AbstractThe presentation, causes, diagnosis and treatment strategies for patients
with thyrotoxicosis are reviewed, with particular emphasis on Graves’
disease.
Keywords hyperthyroid; Graves’ disease; thyroid opthalmopathy;
thionamide; radio-iodine; total thyroidectomy; subtotal thyroidectomy;
thyroid storm
Thyrotoxicosis represents the symptoms and signs of increased metabolic rate and sympathetic activity due to increased amounts of thyroid hormone in the circulation. It is usually associated with hyperthyroidism, which can be classified as primary or second-ary. Thyrotoxicosis can occur in the absence of hyperthyroidism, e.g. a short-term thyrotoxicosis can occur if stored hormones are released in a destructive thyroiditis.
The causes of thyrotoxicosis are listed in Table 1. Graves’ dis-ease, toxic multinodular goitre and solitary toxic nodule account for 95% of cases, and are commonly encountered in surgical practice. Other causes such as Hashimoto’s thyrotoxicosis or ami-oderone-related thyrotoxicosis are uncommon but may require surgical evaluation.
Presentation
The symptoms and signs of thyrotoxicosis (Table 2) are similar for all causes, with widespread effects due to the stimulation of metabolism, and sensitization of the sympathetic nervous sys-tem to catecholamines. The symptoms may be more subtle in the elderly than in younger patients. Apathetic thyrotoxicosis occurs in elderly patients if features of sympathetic reactivity are absent, and patients may present with severe depression, weight loss, slow atrial fibrillation and a small goitre. Graves’ disease has additional features due to the immunological nature of the condition (Table 3).
Diagnosis
The biochemical diagnosis of thyrotoxicosis is confirmed on blood tests showing increased concentrations of free thyroxine and/or free triiodothyronine. Thyroid-stimulating hormone is
Johnathan G H Hubbard FRCS(Gen) is a Consultant Endocrine Surgeon
at Guy’s and St Thomas’s Hospitals, London, UK. Conflicts of interest:
none declared.
SUrGErY 25:11 46
suppressed in most patients due to negative feedback of thy-roid hormones on the anterior pituitary, but can be normal or increased if a thyroid-stimulating hormone-secreting pitu-itary tumour is present, or due to thyroid hormone resistance. Subclinical thyrotoxicosis exists if thyroid-stimulating hor-mone is suppressed without overt elevation of free thyroxine/triiodothyronine.
The cause should be established once the diagnosis of thyrotoxi-cosis is confirmed. Extra-thyroidal signs and the size and shape of the goitre point to the likely cause. Thyroid antibodies should be
Causes of thyrotoxicosis
Primary hyperthyroidism
Graves’ disease
Toxic MnG
Toxic adenoma (Plummers disease)
drugs: lithium, iodine excess (e.g. contrast media, amioderone)
Secondary hyperthyroidism
Thyroid-stimulating hormone-secreting pituitary tumour
HcG secreting trophoblastic tumours (choriocarcinoma,
hydatidiform mole)
resistance to thyroid hormone
Without hyperthyroidism
Subacute thyroiditis
Silent/postpartum thyroiditis
Ectopic thyroid tissue (Struma ovarii)
Functioning thyroid carcinoma metastases
drugs (e.g. amiodarone)
Table 1
Signs and symptoms of thyrotoxicosis
Signs Symptoms
Sinus tachycardia Hyperactivity
Atrial fibrillation insomnia
Tremor Heat intolerance
Hyperreflexia Palpitations
Warm moist skin Sweating
Palmar erythema increased appetite and weight
loss (rarely weight gain can occur)
Muscle weakness and
proximal myopathy
Fatigue
Gynaecomasia increased bowel movements
Eyelid retraction oligomenorrhea
Goitre Amenorrhea
impaired fertility
reduced libido
Brittle nails
Hair loss
Table 2
9 © 2007 Elsevier Ltd. All rights reserved.

EndocrinE
evaluated. The pattern of thyroid uptake on a radioisotope scan (using 123I or 99mTc) can help to establish the cause, but is not nec-essary in all cases. Patients with a dominant nodule should have thyroid fine-needle aspiration to exclude malignancy.
Multidisciplinary teamworking involving endocrinologists, nuclear medicine physicians and thyroid/endocrine surgeons is required to tailor treatment to individual needs.
Graves’ disease
Basic conceptsName: in the English-speaking world, exopthalmic goitre is named after Robert James Graves, following his description of the disease in the early nineteenth century. It is known as Base-dow’s disease in mainland Europe.
Incidence: Graves’ disease is an autoimmune disease that can occur at any age; it typically affects young women 20–40 years of age. The female to male ratio is 5–10:1. It is more common in Caucasians and has been linked to certain HLA haplotypes (e.g. HLA DR3 and HLA B8 in Caucasian populations; HLA BW46 in Chinese populations). Other autoimmune conditions are associ-ated with Graves’ disease (Table 4).
The pathogenesis of Graves’ disease has not been fully eluci-dated. Stimulatory antibodies acting against the thyroid-stimulat-ing hormone receptor are crucial, and result in the unregulated overproduction of thyroid hormone. Antibodies to other thyroid antigens are frequently present (anti-thyroperoxidase, anti-thy-roglobulin). Inflammatory cells infiltrate the thyroid with the production of cytokines (e.g. interferon, tumour necrosis factor, interleukin-1). There is associated hyperplasia and hypertrophy of thyroid follicles, resulting in goitre formation. The combination of stimulatory and destructive thyroid antibodies may explain the variable course of Graves’ disease after medical treatment, which can cause remissions and hypothyroidism.
The diagnosis of Graves’ disease is confirmed clinically when thyrotoxicosis is present in a patient with a diffuse goitre, with
Features specific to Graves’ disease
Opthalmopathy
• Grittiness and periorbital oedema
• Proptosis
• involvement of extraocular muscles
• corneal involvement
• compression of the optic nerve
Dermopathy
• Violaceous, non-pitting induration of pretibial skin (pretibial
myxoedema)
Acropachy
• clubbing
Lymphoid hyperplasia
Table 3
SUrGErY 25:11 470
extra-thyroidal signs (e.g. opthalmopathy, dermopathy). Anti- thyroglobulin and anti-thyroid peroxidase antibodies are elevated in ≈80% of patients. Thyroid-stimulating antibodies are measured if the diagnosis is uncertain; their presence confirms the diagno-sis. A thyroid radioisotope scan shows diffuse uptake throughout the thyroid and can be used to distinguish between Graves’ dis-ease, toxic multinodular goitre and a toxic nodule (Table 5).
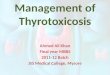
Thyroid opthalmopathyEyelid: although common, retraction (Figure 1a) and lag of the eyelid is not a specific eye sign in Graves’ disease and can occur
Autoimmune conditions associated with Graves’ disease
chronic lymphocytic thyroiditis
rheumatoid arthritis
Vitiligo
Myasthenia gravis
Type 1 diabetes
Systemic lupus erythematosus
Pernicious anaemia
Addison’s disease
immune-mediated thrombocytyopenia
Table 4
Features and pattern of radioiodine uptake in thyrotoxicosis (suppressed thyroid-stimulating hormone)
Low uptake
Silent/postpartum thyroiditis
• non-tender thyroid, postive antithyroid antibodies
Subacute/de Quervain’s
• recent viral infection of the upper respiratory tract, tender
thyroid, fever, high erythrocyte sedimentation rate
Struma ovarii
• Abdominal uptake
iodine-induced (e.g. radiological contrast (i.v.), amioderone)
• Usually on background of multinodular goitre
Thyrotoxicosis factitia
High uptake
Graves’ disease
• diffuse uptake
Toxic multinodular goitre
• nodular/patchy uptake
Toxic nodule
• Uptake in nodule with suppressed normal thyroid
Trophoblastic tumour
• raised β-chorionic gonadotrophin
Lymphocytic thyroiditis
• Postive thyroid autoantibodies
Table 5
© 2007 Elsevier Ltd. All rights reserved.

EndocrinE
Graves’ eye. a shows retraction of the eyelid and marked proptosis. b shows deviation of the right eye due to fibrosis of the right inferior
rectus muscle.
Figure 1
in other causes of thyrotoxicosis. It is due to the sensitization of sympathetic fibres (carried via the third cranial nerve) innervat-ing the smooth muscle fibres of levator palapabrae superioris.
The cause of Graves opthalmopathy is thought to be due to an immune response to antigens in retro-orbital tissues that are shared with the thyroid, or antigens that can crossreact with the thyroid-stimulating hormone receptor, and includes fibroblast acti-vation. The result is oedema, glycosaminoglycan deposition and fibrosis of retro-orbital tissue and extraocular muscles (Figure 1b). Opthalmopathy is more common in smokers, and the signs can be unilateral (10%). Eye signs and symptoms include: • discomfort and grittiness in ≈40% of patients • proptosis (Figure 1a) in 30% of patients• involvement of the extraocular muscles in <10% of patients.Involvement of the cornea and compression of the optic nerve are uncommon, but can threaten vision. Treatment options for opthalmopathy include: • reassurance and control of thyrotoxicosis • high-dose corticosteroids • orbital radiotherapy • surgical orbital decompression (rare) • tarrsorrhaphy (rare).
SUrGErY 25:11 47
TreatmentManagement is aimed at controlling hyperthyroidism.
Medical treatment is used to render the patient euthyroid and induce remission, or prepare the patient for definitive treatment (radioiodine or surgery).
Two thionamide antithyroid medications used in the UK are carbimazole and propylthiouracil. These agents interfere with the action of thyroid peroxidase, with consequent reduction in the synthesis of thyroid hormones. Propylthiouracil partially inhibits the conversion of thyroxine to triiodothyronine, poten-tially reducing the concentrations of the active triiodothyronine hormone more quickly than carbimazole. Propylthiouracil is pre-ferred in pregnancy because it is less likely to cross the placenta due to protein binding. Propranolol can be used to block the sympathetic effects of thyroid hormones while carbimazole or propylthiouracil take effect (about three weeks).
There are two widely used treatment strategies.In the titration regimen, a high starting dose of carbimazole
is gradually reduced to maintain a euthyroid state.In block and replace, a high dose (e.g. 40 mg carbimazole
daily) is continued to fully block endogenous production of thy-roid hormones and thyroxine (e.g. 100 μg daily) is added after
1 © 2007 Elsevier Ltd. All rights reserved.

EndocrinE
4–6 weeks to maintain a euthyroid state. Monitoring is required because the thyroxine dose may need adjustment. Treatment is continued for 6–24 months.
Remission is variable, but ≈20–40% of patients are euthyroid on stopping medication, although recurrence occurs in 40–80%, frequently within the first year.
Major side effects include agranulocytosis, hepatitis, and aplastic anaemia, and require the medication to be stopped. Patients should seek urgent medical advice if they develop a sore throat, mouth ulceration or fever during treatment; an advice card should be given on starting treatment. Minor side effects include skin rash, pruritis, urticaria, arthralgia, myalgia, and transient leucopenia; these effects may respond to dose reduc-tion or substitution of one thioamide for another, although there may be crossreactivity.
Radioiodine therapy: radioiodine is used as a definitive treat-ment as a first line or for recurrence after treatment with antithy-roid drugs or a subtotal thyroidectomy (see below). Radioiodine is the predominant choice of treatment for Graves’ disease in the USA; antithyroid drugs and surgery are more frequently used in Europe and Asia.
Radioiodine is most suitable for patients with a small goitre and in the absence of opthalmopathy. It is contraindicated: • in pregnancy • for those breastfeeding • for those planning to become pregnant within 4–6 months of
therapy.Radioiodine is often unacceptable to patients with contacts with children (e.g. parents, grandparents, nursery staff) due to the need to avoid close contacts for up to four weeks after treatment. Radioiodine is usually avoided in those with severe opthalmopa-thy because eye signs deteriorate in about 15% of patients after treatment. Patients with stable eye signs can be given a three-month course of corticosteroids starting at the time of therapy to prevent worsening of opthalmopathy.
Patients are medically treated until they are clinically euthy-roid before radioiodine treatment is started. Antithyroid drugs may be stopped several days before treatment to maximize uptake of radioiodine. Propylthiouracil has a longer radiopro-tective effect than carbimazole. Radioiodine is given orally as 131I, which emits β particles that destroy thyroid follicular cells. The effects of radioiodine are not immediate and continue for months after treatment. Symptomatic improvement takes about 6–8 weeks. The major consequence of radioiodine treatment is hypothyroidism and patients require lifelong follow-up to moni-tor thyroid status. Thyroid replacement therapy is started when thyroid-stimulating hormone concentrations start to rise above the normal range. Hypothyroidism occurs in ≈20% of patients at one year post-radioiodine treatment, and 80% of adequately treated patients eventually become hypothyroid. A second dose can be given 4–6 months later for persistent hyperthyroidism after initial radioiodine therapy.
Surgery is the first-line treatment: • for large goitres • if radioiodine is contraindicated • for opthalmopathy • if the patient prefers it.
SUrGErY 25:11 47
Unlike radioiodine therapy, surgery provides tissue for histologi-cal assessment.
Preparation for surgery – hyperthyroidism should be medi-cally controlled before surgery to reduce the risk of thyroid storm (see below) in the postoperative period. Lugol’s iodine (2–3 drops t.d.s.) can be given 7–10 days preoperatively to reduce the vas-cularity of the thyroid as an adjunct to antithyroid medications; this is not necessary for all patients. A team approach involving endocrinologists and anaesthetists is particularly important for patients with difficult-to-control thyrotoxicosis and those intol-erant of thioamide drugs; the HDU may be necessary for this patient group. Large doses of iodine can be given preoperatively to ‘stun’ the thyroid (Wolf–Chaikoff effect). This can be achieved using large doses of Lugol’s iodine or iodine containing radiologi-cal contrast agents (e.g. sodium ipodate). β-blockers should be used to control the adrenergic effects, although contraindications (e.g. asthma) must be considered.
Total and subtotal thyroidectomy – total thyroidectomy has become widely accepted as the first-line treatment in Graves’ dis-ease, although there are proponents of subtotal thyroidectomy.
In total thyroidectomy, the patient is rendered definitively hypothyroid, eliminating the risk of recurrence and necessitating lifelong thyroxine replacement.
The aim of a subtotal resection is to leave a remnant large enough to leave the patient euthyroid without medication, but small enough to avoid recurrent hyperthyroidism; this is not always straightforward. A remnant of size 2–4 g is recommended, carrying out a total thyroid lobectomy on one side and leaving a single remnant on the contralateral side, or leaving a remnant of 2 g on each side.
Proponents of a subtotal resection claim a lower risk of hypo-parathyroidism and recurrent laryngeal nerve injury, although this is not supported by many favouring total thyroidectomy. Patients undergoing subtotal resection require long-term moni-toring because many will become hypothyroid, and a small risk of recurrent hyperthyroidism remains.
Surgery has a beneficial effect on reducing thyroid-stimulat-ing hormone receptor antibody concentrations for many patients, which appears to be similar for both surgical procedures at twelve months, but which may be better maintained beyond 12 months in subjects undergoing total thyroidectomy. Surgery is preferred to radioiodine in patients with opthalmopathy, but the course of eye disease after surgery is unpredictable.
Thyroid storm
Thyroid storm is rare but potentially life-threatening. It is an acute exacerbation of thyrotoxicosis, with marked hypermetabo-lism and adrenergic response. It can be precipitated by defini-tive thyroid treatment (surgery or radioiodine) in a patient with inadequately controlled thyrotoxicosis, or in a subject with thy-rotoxicosis after parturition or a severe illness (e.g. uncontrolled diabetes, severe infection, myocardial infarction). Hyperpyrexia is the striking feature but tachycardia, atrial fibrillation, heart failure, agitation, confusion, vomiting, diarrhoea, coma and shock can occur. Patients should be cared for in the ICU.
Treatment is aimed at reducing secretion of thyroid hor-mones and the sympathetic response. Supportive therapy (e.g.
2 © 2007 Elsevier Ltd. All rights reserved.

EndocrinE
a Toxic left thyroid nodule. b corresponding radioisotope scan.
Figure 2
corticosteroids, external cooling, intravenous fluids) and treating the underlying cause is essential. Ensuring adequate preopera-tive preparation of surgical patients is the best way to prevent thyroid storm.
Toxic multinodular goitre and toxic nodule
Unlike Graves’ disease, medical control of thyrotoxicosis does not induce remission. Definitive treatment can be radioiodine for: • a non-compressive and cosmetically acceptable goitre • a small toxic nodule (Figure 2) • those wishing to avoid surgery.The risk of radioiodine-induced hypothyroidism for a toxic nodule is small because the toxic nodule inhibits uptake of radioiodine on the remaining thyroid. Total thyroidectomy is the first-line
SUrGErY 25:11 47
procedure for a large toxic multinodular goitre. This avoids possible regrowth of the goitre and recurrent thyrotoxicosis.
Thyroid lobectomy is the first-line procedure for a solitary toxic nodule because it provides tissue for histology; the nor-mal contralateral lobe means the patient is likely to be euthyroid postoperatively.
Amioderone
Amioderone is a widely used antiarrythmic drug that contains two atoms of iodine per molecule. It induces thyrotoxicosis, which can occur after years of treatment through two mechanisms: iodine-induced thyrotoxicity and amioderone-induced thyroiditis. Frequently, amioderone must be continued because of underly-ing heart disease and a total thyroidectomy may be indicated. ◆
3 © 2007 Elsevier Ltd. All rights reserved.






![kuliah hipertiroid.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000095-metabolism...Thyrotoxicosis and Hyperthyroidism Definitions • Thyrotoxicosis –The clinical syndrome of](https://img.pdfslide.us/doc/110x75/5b02f3bf7f8b9a89208b79b3/kuliah-read-onlyocwusuacidcoursedownload1110000095-metabolismthyrotoxicosis.jpg)