Embed Size (px)
Citation preview

5/23/2014
1
Marshall Dahl MD PhD FRCPC cert Endo
Clinical Professor, University of British [email protected]
Tel 604 875 5577Fax 604 875 5188
• Faculty: Marshall Dahl
• Relationships with commercial interests:– None– Nada– Nil

5/23/2014
2
• None
CFPC CoI Templates: Slide 2
Not applicable

5/23/2014
3
Review endocrine physiology ofthyroid gland
Five selected types of thyrotoxicosis-understand: Pathophysiology Clinical presentation Investigations Treatment

5/23/2014
4
Multiple Etiologies 5 are common Diagnosis needed for
appropriatemanagement
Differentiation canoften be made throughhistory and physicalexamination
23 woman presents for care Chief Complaint: “I went to the fitness club and a guy came up to
me and said that I should get my thyroidchecked!”
“I looked on the internet- I think that it’soveractive!”

5/23/2014
5
Some findings ofthyrotoxicosis are presentregardless of the etiology
What symptoms? What physical findings?

5/23/2014
6
She wants you to know thather mother and sister have“overactive thyroids”.
She has noticed that hereyes have become moreprominent
She’s pretty sure from herreading that she hasGraves’ disease
What findings are specificto this condition?

5/23/2014
7
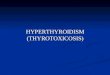
Weetman, A. P. N Engl J Med 2000;343:1236-1248
Clinical Manifestations of Graves' Disease
Pathogenesis of Graves' Disease.
Weetman AP. N Engl J Med 2000;343:1236-1248.

5/23/2014
8
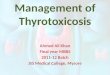
Weetman, A. P. N Engl J Med 2000;343:1236-1248
Bahn, R. S. et al. N Engl J Med 1993;329:1468-1475
Computed Tomographic Scans of the Orbits (Axial Views) in a Patient with Graves' Ophthalmopathy(Panel A) and a Normal Subject (Panel B)

5/23/2014
9
>60% of cases of thyrotoxicosis HLA-DR, CTLA-4, but 20% concordance
monozygotic twins Women in North America: 0.5/1000 (20 year
incidence) Women:Men 10:1 Peak: age 40-60, but any age possible
Disease Etiology SpecificSymptoms
Signs Lab Tests Other tests
Graves’ TSI Orbitopathy,Dermopathy
Firm, rubberygland +/-orbitpathy
↓ TSH↑ Free T4TSH receptorantibody*
Third generation assay sens 97%, spec 99%. JCEM 98, 6, June 2013, Barbesino

5/23/2014
10
Radioiodine Two day procedure Isotope limited: Tuesday, Wednesday
Good for etiology Good for structure Good if planning
iodine therapy
Pertechnetate Same day procedure Short notice Quick result Good for high uptake Not good for structure

5/23/2014
11
Disease Etiology SpecificSymptoms
Signs Lab Tests Uptake #Pattern
Graves’ TSI Orbitopathy,Dermopathy
Firm, rubberygland +/-orbitpathy
↓ TSH↑ Free T4+ve TSHrAb
HighDiffuse

5/23/2014
12
Contra-indicated in pregnancy and breast-feeding
Can’t be performed in the face of recent radio-contrast dye: IVP CT Angiography
Tracer can’t compete with large exogenousiodine dose for uptake Kelp pills
57 year old woman Chief Complaint:
“It’s the worst flu I’veever had! I’ve got afever, I ache all overand I’ve got the worstsore throat andearache!”
“Can I get someantibiotics?”

5/23/2014
13
“Flu” started withrunny nose and cough
Progressed to fever,generalized myalgia,ear pain, pain withswallowing
Thyroid is enlarged,tender, firm, no nodes
Pearce, E. N. et al. N Engl J Med 2003;348:2646-2655

5/23/2014
14
Pearce, E. N. et al. N Engl J Med 2003;348:2646-2655

5/23/2014
15
Disease Etiology SpecificSymptom
s
Signs Lab Tests Uptake #Pattern
Graves’Disease
TSI Orbitopathy,Dermopathy
Rubberygland +/-orbitpathy
↓ TSH↑ Free T4
HighDiffuse
Sub-acuteThyroiditis
Auto-immune+/-viral
Pain,tenderness
Firm,tendergland
↓ TSH↑ Free T4
NoneNone
58 year old woman Symptoms of
thyrotoxicosis Enlarged neck for
many years 2010:
TSH 0.1 (0.5-5.5), Free T4 20 (11-22)
2014: TSH < 0.01, Free T4 35

5/23/2014
16
General Appearance: thyrotoxic HR 100, BP 150/80 Lid-lag, stare, no proptosis Thyroid asymmetrically enlarged It is quite firm, irregular, non-tender with no
adenopathy

5/23/2014
17
Worldwide: iodine deficiency Developed world: genetic and non-immune Early: diffuse goitre Later: nodularity Slow growth with gradual functional
“autonomy”- dropping TSH with normal T4 Minority: biochemical and clinical
thyrotoxicosis Some may have local obstructive signs
Avoid exogenous iodine Jod-Basedow phenomenon Iodine causes autonomous nodules to overproduce
thyroxine
Often older patients Weight loss, atrial fibrillation, palpitations
No increased risk of malignancy Biopsy if dominant nodule or increasing size

5/23/2014
18
Disease Etiology SpecificSymptoms
Signs Lab Tests Uptake #Pattern
Graves’Disease
TSI Orbitopathy,Dermopathy
Rubbery gland+/- orbitpathy
↓ TSH↑ Free T4
HighDiffuse
Sub-acuteThyroiditis
Auto-immune+/-viral
Pain,tenderness
Firm, tendergland
↓ TSH↑ Free T4
NoneNone
Toxic Multi-nodularGoitre
“Autonomy” Slow goitregrowth
Asymmetric,nodular
↓ TSH↑ Free T4
HighPatchy

5/23/2014
19
Disease Etiology SpecificSymptoms
Signs Lab Tests Uptake #Pattern
Graves’Disease
TSI Orbitopathy,Dermopathy
Rubbery gland+/- orbitpathy
↓ TSH↑ Free T4
HighDiffuse
Sub-acuteThyroiditis
Auto-immune+/-viral
Pain,tenderness
Firm, tendergland
↓ TSH↑ Free T4
NoneNone
Toxic Multi-nodular Goitre
“Autonomy”Multifactorial
Slow goitregrowth
Asymmetric,nodular
↓ TSH↑ Free T4
HighPatchy
Toxic Nodule TSH receptormutation
Singlenodule?
Nodule,remainder ofthyroid small
↓ TSH↑ Free T4
HighNodule

5/23/2014
20
49 year old man withhistory majordepression treatedwith medication
Improved mood, butweight loss,tachycardia,diaphoresis, tremour
TSH < 0.01
Sertraline Cytomel TSH <0.01 Free T4 8 (11-22) Free T3 9.3 (3.5-6.5)

5/23/2014
21
Disease Etiology SpecificSymptoms
Signs Lab Tests Uptake #Pattern
Graves’Disease
TSI Orbitopathy,Dermopathy
Rubbery gland+/- orbitpathy
↓ TSH↑ Free T4
HighDiffuse
Sub-acuteThyroiditis
Auto-immune+/-viral
Pain,tenderness
Firm, tendergland
↓ TSH↑ Free T4
NoneNone
Toxic Multi-nodular Goitre
“Autonomy”Multifactorial
Slow goitregrowth
Asymmetric,nodular
↓ TSH↑ Free T4
HighPatchy
Toxic Nodule TSH receptormutation
Single nodule? Nodule,remainder ofthyroid small
↓ TSH↑ Free T4
HighNodule
Factitious,Iatrogenic
Exogenousthyroidhormone
History maynot beobvious
Thyroid notpalpable
↓ TSH↑ Free T4 or T3
NoneNone
Surgery Sub-total
thyroidectomy Rarely performed Special cases: Pregnancy and
intolerance of anti-thyroid drugs
<2% recurrence rate Hypothyroidism
common

5/23/2014
22
Thionamides: propylthiouracil, carbimazole and active
metabolite methimazole(Tapazole)
Inhibit TPO: reducingoxidation andorganification of iodide
This image cannot currently be displayed.
Methimazole Propylthiouracil
Serum Half-life 4-6 hrs 75 minutes
Tissue concentration 100X serum (gives 20 hrduration of action)
Dosing Single daily 3X/day
Time to normalizationT3,T4
5.8 weeks 16.8 weeks

5/23/2014
23
Measure Free T4monthly (TSHunreliable)
Titrate dose down tomaintenance
Maximum remissionrate by 18-24 months Discontinue and monitor
for relapse
Methimazole starting dose: 20-40 mg
daily Maintenance: 2.5-10
PTU Starting dose: 100-200
TID Maintenance: 50-100
daily in divided doses
~4%: rash, urticaria <3:1,000 agranulocytosis
“Sore throat, high fever- notify physician” Less common with low dose methimazole
Rarer: PTU: hepatocellular necrosis Methimazole: reversible cholestatic jaundice PTU: vasculitis Methimazole: scalp defect in neonates

5/23/2014
24
Either as initial treatment or second-line afterrelapse following drugs
Progressive destruction of thyroid cells Calculated dose based on uptake value and
size of gland Hypothyroidism common Time to normalization 4- 8 weeks Worsen orbitopathy?
Radioiodine is treatment of choice Concentrates within toxic nodule Remainder of thyroid is suppressed and unaffected Normal thyroid tissue recovers
Surgical resection is also effective Some centres use repeat injection of ethanol
solutions

5/23/2014
25
During acute inflammation: If marked local or systemic symptoms: Prednisone 40-60 mg daily tapered over 6-8 weeks
If less symptomatic: NSAIDs or ASA
If hypothyroid phase is prolonged andsymptomatic: Thyroxine at modest dose 50-100 ug daily 2-3
months
Three additional references?