Embed Size (px)
Citation preview
THYROIDITIS &
HYPOTHYROIDISM
A PRESENTATION ON
CONTENTS OF PRESENTATION
I.THYROIDITIS
• ACUTE SUPPURATIVE THYROIDITIS• SUBACUTE THYROIDITIS
‐ Subacute granulomatous‐ Subacute lymphomatous
• CHRONIC THYROIDITIS‐ Hashimoto’s thyroiditis‐ Riedel’s thyroiditis
II.HYPOTHYROIDISM
CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s thyroiditis)
• Struma lymphomatosa – a transformation of thyroid tissue to lymphoid tissue
• First described autoimmune disease
• Commonest form of thyroiditis
Hashimoto’s thyroiditis is named after Hakaru Hashimoto (May 5, 1881 –January 9, 1934) , who described it first in 1912
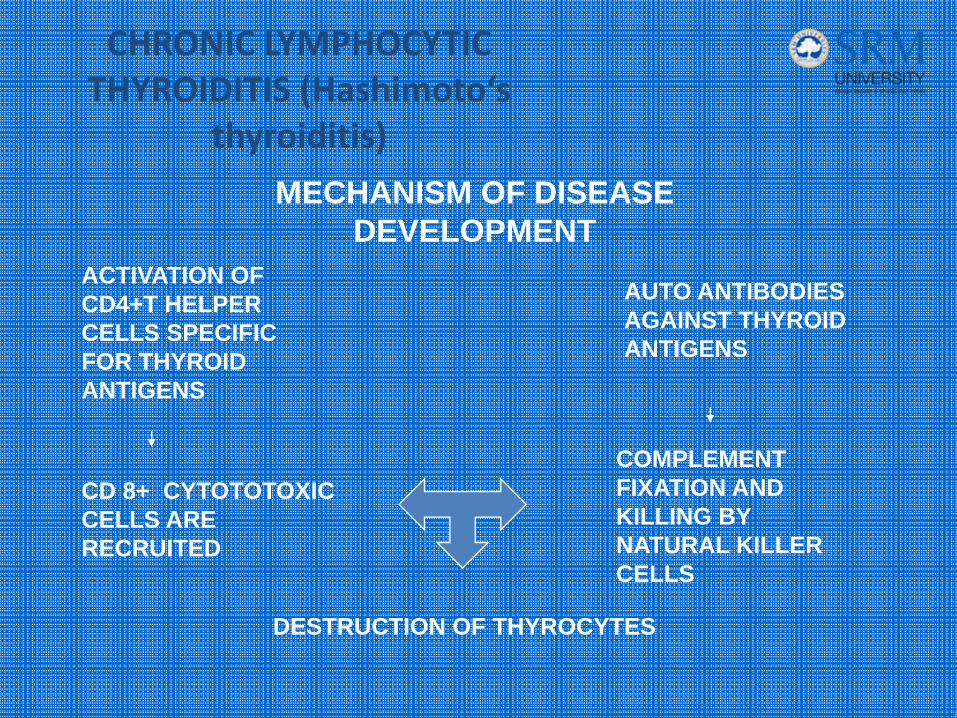
CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s
thyroiditis)
ACTIVATION OF CD4+T HELPER CELLS SPECIFIC FOR THYROID ANTIGENS
CD 8+ CYTOTOTOXIC CELLS ARE RECRUITED
AUTO ANTIBODIES AGAINST THYROID ANTIGENS
COMPLEMENT FIXATION AND KILLING BY NATURAL KILLER CELLS
DESTRUCTION OF THYROCYTES
MECHANISM OF DISEASE DEVELOPMENT
CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s
thyroiditis)
RISK FACTORS• Genetic predisposition
• Chromosomal abnormalities (eg. Turner’s, Down’s)
• HLA B8, DR5, DR3
CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s
thyroiditis)
PRESENTATION• Common in 30 – 50 yr old women
• Moderately enlarged, firm, nodular gland
• Symptoms of transient hyperthyroidism (HASHITOXICOSIS)
• Hypothyroidism
• Papillary carcinoma and malignant lymphoma ( non hodgkins type) are occasionally associated

CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s
thyroiditis)DIAGNOSIS
• Elevated TSH ( transiently reduced during Hashitoxicosis)
• Thyroid auto antibodies – antibodies against
‐Thyroid peroxidase
‐Thyroglobulin
‐TSH receptor
• USG – nodular enlarged thyroid
• FNAC
CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s
thyroiditis)
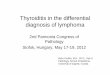
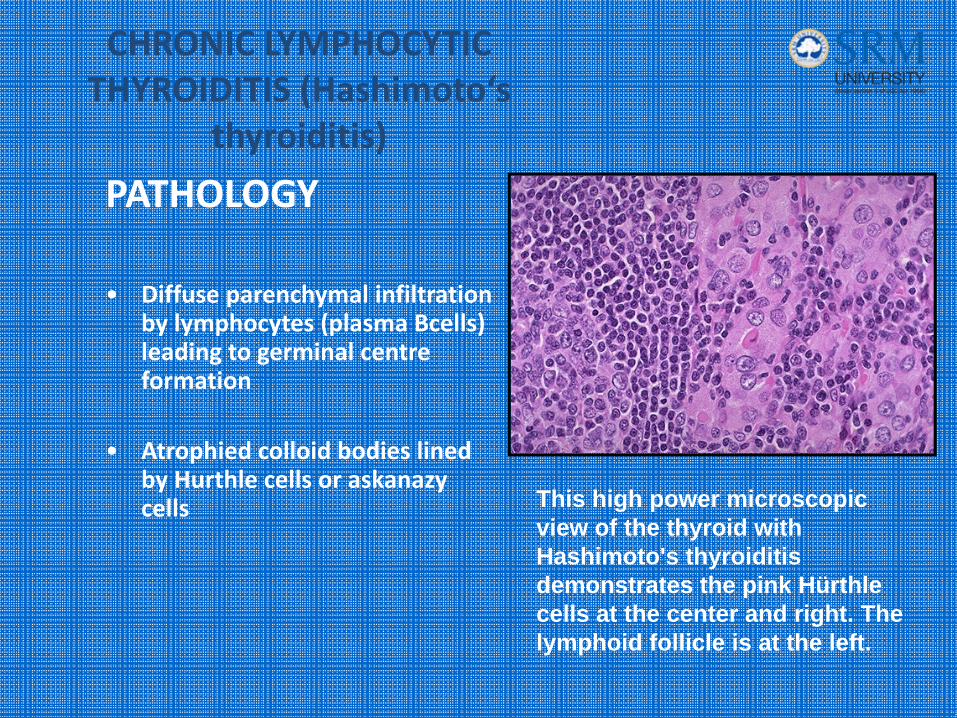
PATHOLOGY
• Diffuse parenchymal infiltration by lymphocytes (plasma Bcells) leading to germinal centre formation
• Atrophied colloid bodies lined by Hurthle cells or askanazy cells This high power microscopic
view of the thyroid with Hashimoto's thyroiditis demonstrates the pink Hürthle cells at the center and right. The lymphoid follicle is at the left.
CHRONIC LYMPHOCYTIC THYROIDITIS (Hashimoto‘s
thyroiditis)TREATMENT• Thyroid hormone replacement
• Maintenance of normal TSH LEVELS
• INDICATIONS FOR SURGERY
‐ Compressive symptoms
‐ Cosmetic deformity
RIEDEL’S THYROIDITIS(Riedel's struma )
• Chronic form of Autoimmune thyroiditis
• Replacement of the normal thyroid parenchyma by a dense fibrosis
• Invades adjacent structures of the neck and extends beyond the thyroid capsule.
• Associated with other focal sclerosing syndromes
RIEDEL’S THYROIDITIS(Riedel's struma )
PRESENTATION• Common in women 30 – 60 ys old• Painless , hard, enlarged thyroid gland• Compressive symptoms are common• Hypothyroidism and hypo parathyroidism
DIAGNOSIS• Pathological examination of tissue obtained from wedge biopsy of
isthmus• FNAC is not useful
RIEDEL’S THYROIDITIS(Riedel's struma )
TREATMENT• Tracheal decompression by wedge biopsy of isthmus
• Thyroid hormone replacement
• Corticosteroids
• Tamoxifen ( in steroid resistant cases)
ACUTE SUPPURATIVE THYROIDITIS
• Very rare, accounting for about 0.1‐0.7% of all thyroiditis
• More common among children
• Modes of infection
‐ Hematogenous spread‐ Lymphatic spread‐ Congenital pyriform sinus fistula‐ Penetrating trauma
ACUTE SUPPURATIVE THYROIDITIS
PATIENT PRESENTATION• Severe pain
• High grade fever with chills
• Odynophagia / dysphonia
INVESTIGATIONS• Leucocytosis
• USG – unilateral thyroid swelling
• FNAC – for gram stain / culture / cytology
• CT SCAN – extent of infection
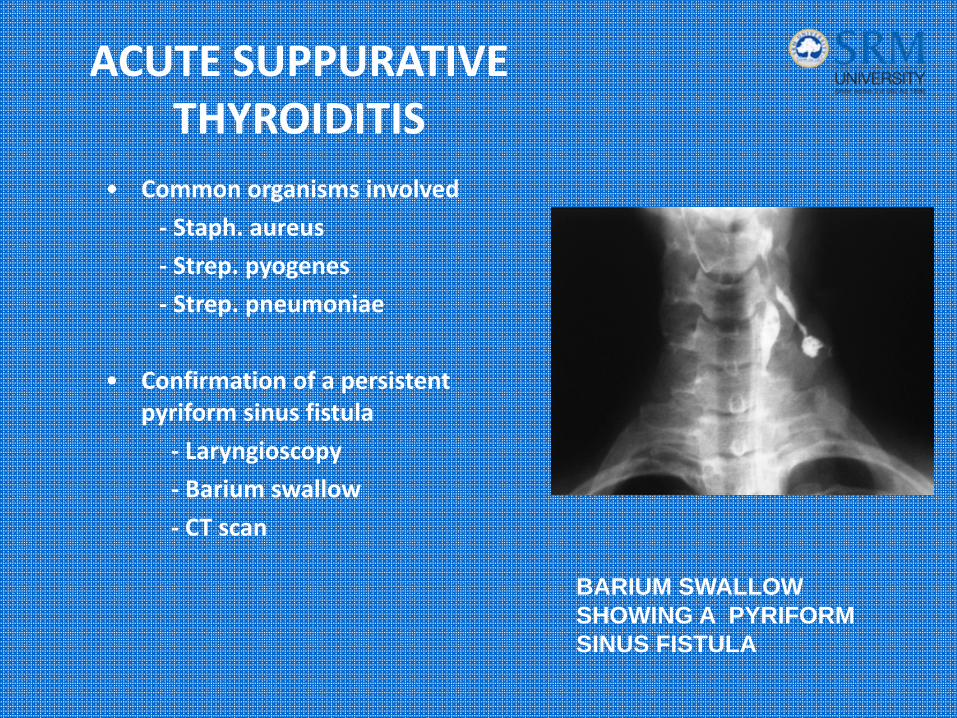
ACUTE SUPPURATIVE THYROIDITIS
• Common organisms involved
‐ Staph. aureus
‐ Strep. pyogenes
‐ Strep. pneumoniae
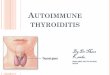
• Confirmation of a persistent pyriform sinus fistula
‐ Laryngioscopy
‐ Barium swallow
‐ CT scan
BARIUM SWALLOW SHOWING A PYRIFORM SINUS FISTULA
ACUTE SUPPURATIVE THYROIDITIS
TREATMENT • Appropriate parenteral antibiotics
• Surgical drainage of the abscess
• Resection of the sinus tract , including area of thyroid where the tract terminates
ACUTE SUPPURATIVE THYROIDITIS
COMPLICATIONS• Tracheal or esophageal rupture
• Systemic sepsis
• Jugular vein thrombosis
• Laryngeal chondritis
• Sympathetic trunk paralysis
SUBACUTE THYROIDITIS
SUBTYPES
I. Subacute granulomatous thyroiditis (painfull type)
II. Subacute lymphocytic thyroiditis (painless type)
SUBACUTE GRANULOMATOUS THYROIDITIS(Painfull thyroiditis)
• Also known as DE QUERVAIN’S THYROIDITIS
• Associated with post viral inflammatory response , leading to auto immune destruction of thyroid follicles
PRESENTATION• 30 – 40 yr old female with preceding history of viral illness
• Sudden / gradual onset neck pain
• Enlarged, tender, firm thyroid gland
• Painful dysphagia
SUBACUTE GRANULOMATOUS THYROIDITIS(Painfull thyroiditis)
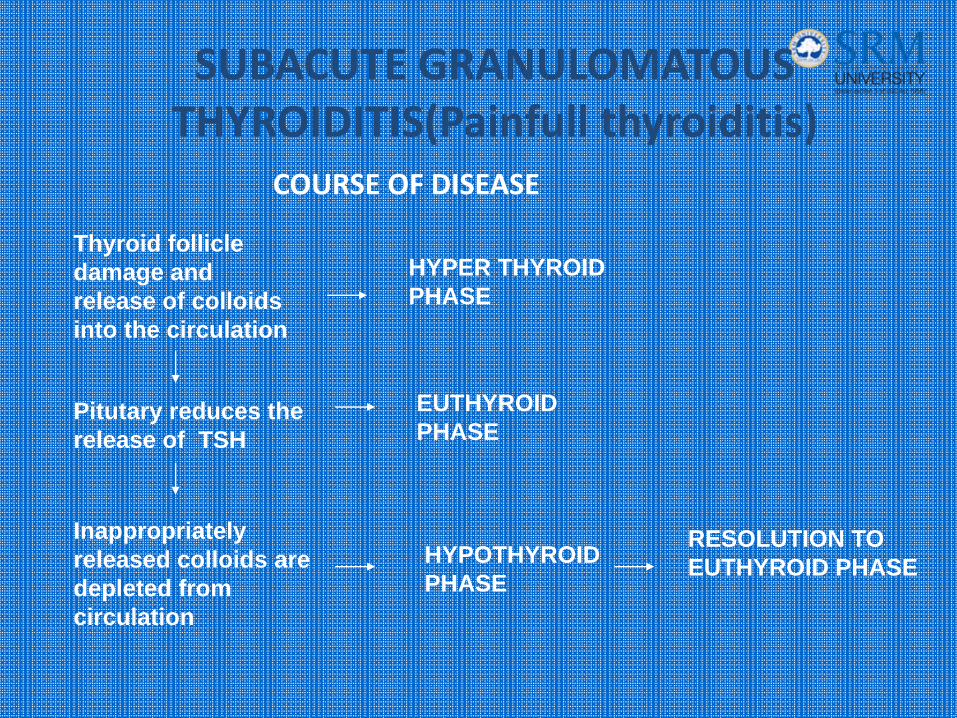
COURSE OF DISEASE
Thyroid follicle damage and release of colloids into the circulation
HYPER THYROID PHASE
Pitutary reduces the release of TSH
EUTHYROID PHASE
Inappropriately released colloids are depleted from circulation
HYPOTHYROID PHASE
RESOLUTION TO EUTHYROID PHASE
SUBACUTE GRANULOMATOUS THYROIDITIS(Painfull
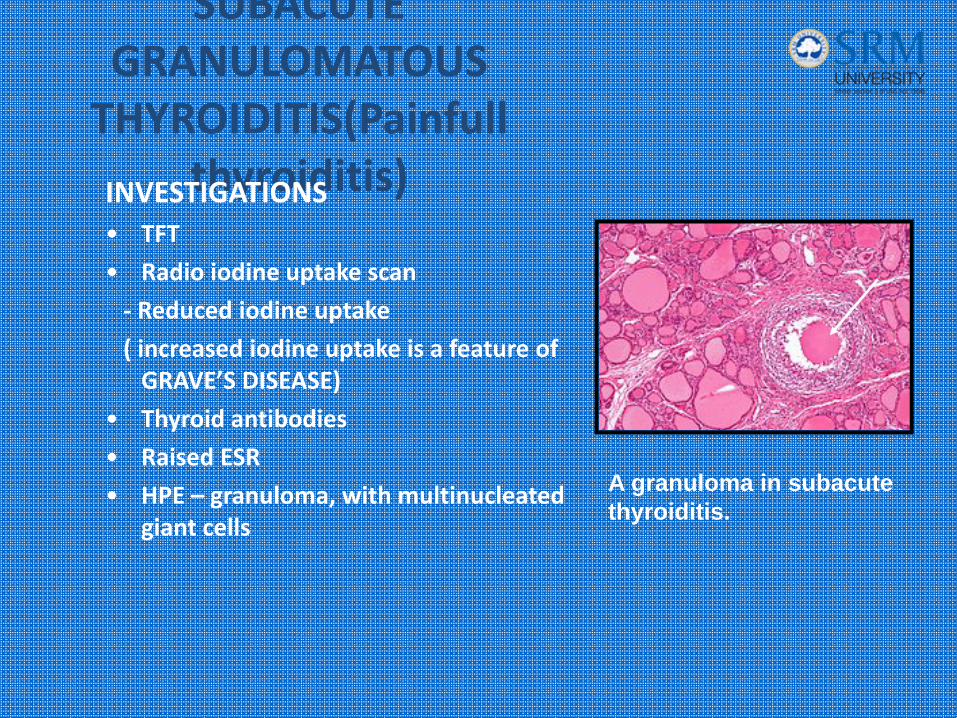
thyroiditis)INVESTIGATIONS• TFT
• Radio iodine uptake scan
‐ Reduced iodine uptake
( increased iodine uptake is a feature of GRAVE’S DISEASE)
• Thyroid antibodies
• Raised ESR
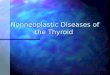
• HPE – granuloma, with multinucleated giant cells
A granuloma in subacute thyroiditis.
SUBACUTE GRANULOMATOUS THYROIDITIS(Painfull
thyroiditis)TREATMENT• Self limiting disease course
• NSAIDS
• Beta blockers for symptomatic releif
• Short term thyroid replacement
• Thyroidectomy – indicated only in prolonged , unresponsive disease
SUB ACUTE LYMPHOCYTIC THYROIDITIS(PAINLESS THYROIDITIS)
• Auto immune etiology
• Can occur in
‐ SPORADIC FORM
‐ POSTPARTUM FORM
• POSTPARTUM THYROIDITIS – caused due to immune system changes that occur during pregnancy
SUB ACUTE LYMPHOCYTIC
THYROIDITIS(PAINLESS THYROIDITIS)PRESENTATION
• Common in 30 – 60 yr old females• Normal or slightly enlarged, firm painless
thyroid gland• TSH , Tg fluctuations similar to PAINFULL
THYROIDITIS
INVESTIGATIONS• TFT• Normal ESR• RAIU – reduced• Thyroid antibodies
SUB ACUTE LYMPHOCYTIC
THYROIDITIS(PAINLESS THYROIDITIS)
TREATMENT• NSAIDS
• Beta blockers for symptomatic releif
• Thyroidectomy is reserved only for recurrent disabling disease
POST PARTUM THYROIDITIS
• Beta blockers in symptomatic hyperthyroid phase
• Short course of L – thyroxine in case of severe hypothyroidism
• Treatment usually upto one year postpartum
HYPOTHYROIDISM
DISCUSSION INCLUDES
I. ADULT HYPOTHYROIDISM
II. CRETINISM
ADULT HYPOTHYROIDISM
CLASSIFICATIONPrimary Primary defect in the function of thyroid gland
• Iodine deficiency • Hashimoto's thyroiditis,• Radioiodine therapy for hyperthyroidism• Subacute thyroiditis• Temporary hypothyroidism due to the Wolff‐
Chaikoff effect• Amiodarone ,lithium‐based mood stabilizers, usually
used to treat bipolar disorder interferon alpha, interleukin‐2, and thalidomide
ADULT HYPOTHYROIDISM
CLASSIFICATIONSecondary• Occurs if the pituitary gland does not
create enough thyroid‐stimulating hormone (TSH) to induce the thyroid gland to produce enough thyroxine and triiodothyronine.
Tertiary• Results when the hypothalamus fails
to produce sufficient thyrotropin‐releasing hormone (TRH).
Signs and symptoms
• CNS – impaired memory, impaired cognitive function, increased need to sleep, sluggish reflexes
• ANS – low basal body temperature, cold intolerance, decreased sweating
• PSYCHOLOGICAL – mood istability, irritability, depression
• CVS – bradycardia, conduction defects
• GIT – weight gain, constipation
• MUSCULOSKELETAL – muscle hypotonia, muscle cramps,joint pain
Signs and symptoms
• SENSORY – deafness, anosmia
• DERMATALOGICAL – dry itchy skin, brittle nails, yellowish discolouration of skin, loss of hair, thinning of lateral one thirds of eye brow(sign of Hertoghe)
• HEMATOLOGICAL – anemia
• HORMONAL – menstural abnormality, female infertility, loss of libido in male, gynecomastia
• OTHERS – hoarseness of voice, caused by Reinke's Edema.
MYXEDEMA
MYXEDEMA is used to describe the clinical syndrome secondary to severe
hypothyroidism.
SYMPTOMS• Supraclavicular puffiness, • Malar flush, • Yellow tinge to the skin • Depression , • Mental slowness, • Weakness , • Bradycardia , • Fatigue ,• Hypothermia ,• Alopecia
MYXEDEMA COMA
MYXEDEMA COMA• Represents the severest form of hypothyroidism and has an associated
mortality rate of 30 percent to 40 percent.
• It can occur due to ‐ long‐standing, untreated hypothyroidism, ‐ Precipitating factors ‐ eg .Acute infection, myocardial infarction, congestive heart failure, cerebral vascular accident, trauma,
• FEATURES ‐ Altered mental status , hypothermia. Hypoglycemia, hypotension, hyponatremia, bradycardia, and hypoventilation
INVESTIGATIONS
Thyroid function tests• High levels of TSH• Free triiodothyronine (fT3)• Free thyroxine (fT4)• Free T3 from 24‐hour urine catch
OTHER INVESTIGATIONS• Investigations to rule out THYROIDITIS• Testing for anemia • Serum cholesterol —may be elevated • Prolactin — test of pituitary function
TREATMENT
• Hypothyroidism is treated with the levorotatory forms of thyroxine (levothyroxine) (L‐T4) and triiodothyronine (liothyronine) (L‐T3).
• T4 only ‐ currently the standard treatment in mainstream medicine.
Myxoedema coma• Large intravenous bolus of levothyroxine should be administered (200 to
400 mcg), followed by daily doses of 50 to 100 mcg,
• combination of both T3 and T4.
CRETINISM
CAUSES• Endemic cretinism caused by iodine deficiency• Dysgenesis of the thyroid gland ‐ agenesis and ectopy • Inborn errors of thyroid hormone metabolism – eg.
‐ Dyshormonogenesis .‐ Thyroid‐stimulating hormone (TSH) unresponsiveness ‐ Impaired ability to uptake iodide‐ Peroxidase, or organification, defect ‐ Thyroid hormone resistance‐ TSH or thyrotropin‐releasing hormone (TRH) deficiencies
• Maternal autoimmune disease• Radioactive iodine therapy of pregnant women
CRETINISM
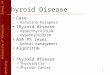
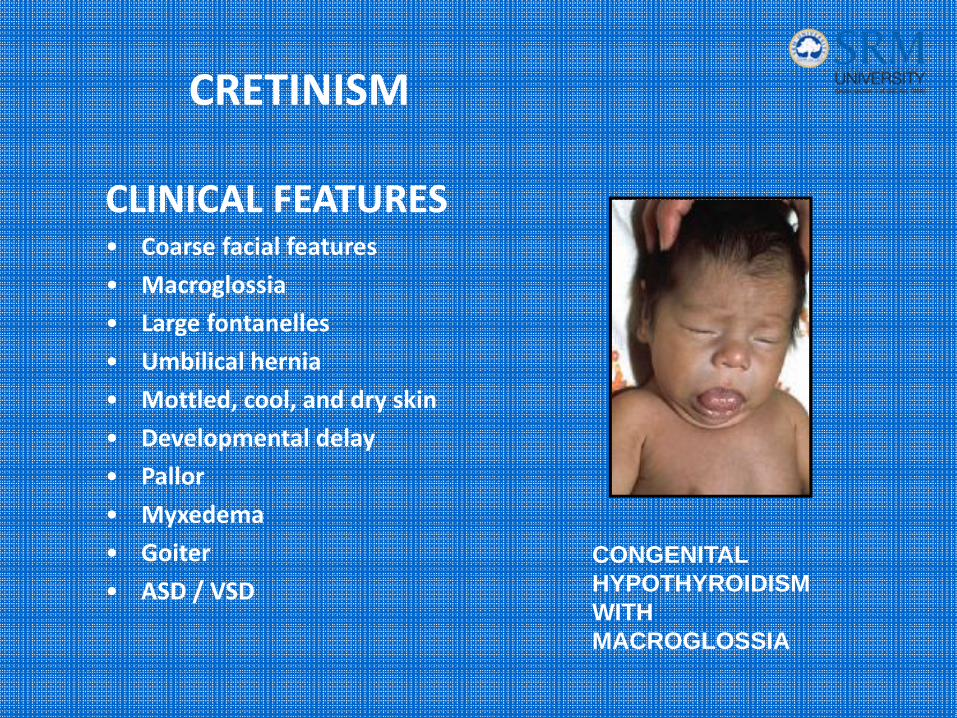
CLINICAL FEATURES• Coarse facial features
• Macroglossia
• Large fontanelles
• Umbilical hernia
• Mottled, cool, and dry skin
• Developmental delay
• Pallor
• Myxedema
• Goiter
• ASD / VSDCONGENITAL HYPOTHYROIDISM WITH MACROGLOSSIA
CRETINISM
DIAGNOSIS
• Diagnosis of primary hypothyroidism is confirmed by demonstrating decreased levels of serum thyroid hormone (total or free T4) and elevated levels of thyroid‐stimulating hormone (TSH).
• If maternal antibody–mediated hypothyroidism is suspected, maternal and neonatal antithyroid antibodies may confirm the diagnosis
TREATMENT
• The mainstay in the treatment of congenital hypothyroidism is early
diagnosis and thyroid hormone replacement.
Thank you for the patient listening…PRESENTED BY
R. VISHNU SUNDAR
POST GRADUATE
DEPARTMENT OF GENERAL SURGERY