Embed Size (px)
Citation preview

Graves’ DiseaseGraves’ Disease
Andrew G. Gianoukakis MD FACEAndrew G. Gianoukakis MD FACEAssociate Professor of MedicineAssociate Professor of Medicine
UCLA School of MedicineUCLA School of Medicine

DefinitionDefinition
• Graves’ Disease (GD) is an autoimmune Graves’ Disease (GD) is an autoimmune disease characterized by hyperthyroidism, disease characterized by hyperthyroidism, ophthalmopathy,and dermopathy. The ophthalmopathy,and dermopathy. The thyroidal component is driven by anti-thyroidal component is driven by anti-thyrotropin receptor (TSHR) antibodies.thyrotropin receptor (TSHR) antibodies.

Robert J. Graves’ 1797-1853
Caleb Hillier Parry 1755-1822
Karl Adolf von
Basedow
1799-1854

• Parry CH. Collections from the unpublished Parry CH. Collections from the unpublished medical writings. London: Underwoods, medical writings. London: Underwoods, 18251825:111:111
• Graves RJ. Clinical lectures delivered by Graves RJ. Clinical lectures delivered by Robert J. Graves, M.D. at the Mead Hospital Robert J. Graves, M.D. at the Mead Hospital during the session of 1834-5. London Med during the session of 1834-5. London Med Surg J Surg J 18351835; 7:516; 7:516
• Basedow CA. Exophthalmos durch Basedow CA. Exophthalmos durch hypertropie des Zellgewebes in der hypertropie des Zellgewebes in der Augenhohle. Wschr f d ges Heilkunde Augenhohle. Wschr f d ges Heilkunde 18401840;6:197-220;6:197-220

EpidemiologyEpidemiology
• Incidence- 30-200 new cases per Incidence- 30-200 new cases per 100,000 per year100,000 per year
• Prevalence- 2.5 % of women and 0.23% Prevalence- 2.5 % of women and 0.23% of menof men
• GD is distributed relatively equally GD is distributed relatively equally across races and around the globeacross races and around the globe
• Most common cause of hyperthyroidism Most common cause of hyperthyroidism in iodine sufficient areasin iodine sufficient areas
Tunbridge. Clin Endocrinol.1977Furszyfer J. Mayo Clin Proc.1970Vanderpump MPJ. Clinical Endocrinol 43:55-68, 1995

• Anxiety Anxiety • IrritabilityIrritability• A fine tremorA fine tremor• Sensitivity to heatSensitivity to heat• Weight loss Weight loss • A rapid heartbeatA rapid heartbeat• FatigueFatigue• Difficulty sleeping Difficulty sleeping • Perspiration Perspiration • Brittle hair Brittle hair • Light menstrual periods Light menstrual periods • Frequent bowel movementsFrequent bowel movements
Symptoms of thyrotoxicosis

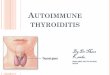
Diffuse hyperplasia
Lymphocytic infiltration
Thyroid Histology
NormalGraves’
Papillary structures

Risk FactorsRisk Factors
• GeneticGenetic• Monozygotic twins (35%) have a greater Monozygotic twins (35%) have a greater
concordance rate than dizygotic twins (3%)concordance rate than dizygotic twins (3%)• Susceptibility genes (CD40, CTLA-4, Susceptibility genes (CD40, CTLA-4,
PTPN22) have been associated with GDPTPN22) have been associated with GD• Increased frequency of HLA DR3 and Increased frequency of HLA DR3 and
DQA10501 haplotypes in GDDQA10501 haplotypes in GD
Brix TH. JCEM. 2001Jacobson EM et. al. J. Autoimmunity 2007. 28;85-98.

Risk FactorsRisk Factors• GenderGender
• Female to male ratio (8-10: 1)Female to male ratio (8-10: 1)• Age Age
• low incidence in childhoodlow incidence in childhood• Pregnancy Pregnancy • Environmental factors associated with GD Environmental factors associated with GD
• InfectionInfection• Stress (emotional or physical)Stress (emotional or physical)
• MedicationsMedications• IodineIodine• AmiodaroneAmiodarone
Prummel MF et. al. Eur J. Endocrinol 2004. 150;5:605-18.

PathogenesisPathogenesis• GD is an autoimmune disease in which host GD is an autoimmune disease in which host
susceptibility genes and environmental factors susceptibility genes and environmental factors interact to initiate cellular and humoral immune interact to initiate cellular and humoral immune responses against host antigensresponses against host antigens
• The TSH receptor (TSHR) is an autoantigen in The TSH receptor (TSHR) is an autoantigen in GD.GD.
• anti-TSHR antibodies (IgG class) stimulate the anti-TSHR antibodies (IgG class) stimulate the TSHR without modulation and cause TSHR without modulation and cause hyperthyroidismhyperthyroidism

DiagnosisDiagnosis• Clinical Clinical
• GoiterGoiter• ThyrotoxicosisThyrotoxicosis
• SymptomsSymptoms• OphthalmopathyOphthalmopathy• DermopathyDermopathy
• BiochemicalBiochemical• TSH, T3, T4, TSI (thyroid TSH, T3, T4, TSI (thyroid stimulating immunoglobulins)stimulating immunoglobulins)
• Nuclear MedicineNuclear Medicine• % Thyroidal Iodine uptake% Thyroidal Iodine uptake• Diffuse pattern of thyroidal uptake (scan)Diffuse pattern of thyroidal uptake (scan)
Weetman AP. N Engl J Med 2000. Oct 26;343(17):1236-48

Differential DiagnosisDifferential Diagnosis
• Other causes of hyperthyroidismOther causes of hyperthyroidism• Toxic uninodular or multinodular goiterToxic uninodular or multinodular goiter• Subacute thyroiditisSubacute thyroiditis• Silent thyroiditisSilent thyroiditis• Struma OvariiStruma Ovarii• Surreptitious Levothyroxine useSurreptitious Levothyroxine use• Toxic hyperplasiaToxic hyperplasia

Treatment of hyperthyroidismTreatment of hyperthyroidism
• ReversibleReversible• Thionamides* (PTU, Methimzole)Thionamides* (PTU, Methimzole)• B-blockers (Propranolol)B-blockers (Propranolol)• CorticoteroidsCorticoteroids• SSKISSKI
• DefinitiveDefinitive• Radioactive iodine therapyRadioactive iodine therapy• SurgerySurgery
*Cooper DS. JCEM 2003. 88 (8):3474-3481.Weetman AP. N Engl J Med 2000. Oct 26;343(17):1236-48

Remission of hyperthyroidismRemission of hyperthyroidism• Remission can occur after thionamide Remission can occur after thionamide
therapy (12-18 months). Long term therapy (12-18 months). Long term remission is rare with high % per year remission is rare with high % per year recurrence after discontinuation of recurrence after discontinuation of thionamide therapy.thionamide therapy.
• Severity of hyperthyroidism, goiter size, Severity of hyperthyroidism, goiter size, higher T3, higher TSI are poor prognostic higher T3, higher TSI are poor prognostic features for achieving remissionfeatures for achieving remission
Abraham et al. Cochrane Database Syst Rev 2004:2:CD003420Cooper DS. NEJM 2005;352:905-917

Graves’ DiseaseGraves’ DiseasePregnancyPregnancy
• Graves’ disease:Graves’ disease:• is uncommonly diagnosed during pregnancyis uncommonly diagnosed during pregnancy• thyrotoxicosis often improves and autoimmune phenomenon often thyrotoxicosis often improves and autoimmune phenomenon often
remit during pregnancyremit during pregnancy• commonly relapses or develops in the post-partum period in commonly relapses or develops in the post-partum period in
susceptible hostssusceptible hosts
• High maternal TSI levels after 25 weeks of gestation are High maternal TSI levels after 25 weeks of gestation are associated with increased risk of antibody transfer to fetus associated with increased risk of antibody transfer to fetus and the development of transient fetal thyroidal dysfunctionand the development of transient fetal thyroidal dysfunction
Chan GW. Nat Clin Pract Endocrinol 2007; 3:7; 470-78

Graves’ DiseaseGraves’ DiseaseChildren and the agedChildren and the aged
• ChildrenChildren• The most common form of hyperthyroidism in childrenThe most common form of hyperthyroidism in children• TAO is extremely rare in childrenTAO is extremely rare in children• Thionamide therapy is preferredThionamide therapy is preferred• RAI therapy is controversial in children RAI therapy is controversial in children
• AgedAged• Often lack hyperkinetic symptomatology and present Often lack hyperkinetic symptomatology and present
with myopathy, atrial fibrillation, heart failurewith myopathy, atrial fibrillation, heart failure• Apathetic hyperthyroidism (placid facies, withdrawn, Apathetic hyperthyroidism (placid facies, withdrawn,
depressed affect)depressed affect)
Rivkees SA. J Pediatr Endocrinol Metab 2006. 19;9:1095-111

GD Associated ManifestationsGD Associated ManifestationsThyroid Associated Ophthalmopathy (TAO)Thyroid Associated Ophthalmopathy (TAO)
• Pathogenesis* Pathogenesis* • TSHR and other antigens TSHR and other antigens
have been implicated have been implicated • Uniqueness of orbital Uniqueness of orbital
fibroblasts may underlie fibroblasts may underlie regional involvementregional involvement
• IncidenceIncidence• 20 % of patients with GD 20 % of patients with GD
develop clinically obvious develop clinically obvious opthalmopathyopthalmopathy
• SymptomsSymptoms• Gritty, sandy sensation, TearingGritty, sandy sensation, Tearing• Retrobulbar pain and discomfortRetrobulbar pain and discomfort• Diplopia Diplopia • PhotophobiaPhotophobia• Blurred visionBlurred vision
*Prabhakar BS et. al. Endocr Rev 2003. 24;6;802-25*Khoo TK et. al. Thyroid 2007.17(10);1013-18

Male SexMale Sex
Perros P, Kendall-Taylor P. Perros P, Kendall-Taylor P. J Intern Med J Intern Med 231:205.1992231:205.1992
Who develops TAOWho develops TAO ? ?
Bartalena L. et al. Bartalena L. et al. J Endocrinol Invest J Endocrinol Invest 12:733-737.198912:733-737.1989
SmokersSmokers

Burch HB, Wartofsky L. Burch HB, Wartofsky L. Endocrine reviewsEndocrine reviews 14:6.747-793. 1993 14:6.747-793. 1993
85% within 18months of
thyrotoxicosis
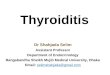
When?When?
Euthyroid Euthyroid Graves’Graves’

Dis
ease
Time
TAO-Disease Course
Immunomodulatory Therapy
Active Phase
Stable Phase
18-24m 5-7yrs
Surgery

Treatment of TAOTreatment of TAO
• GeneralGeneral• Local/ protective measuresLocal/ protective measures• Tinted spectacle lensesTinted spectacle lenses• Artificial tears/ointmentArtificial tears/ointment• Nighttime eye patch/taping lidsNighttime eye patch/taping lids• PrismsPrisms• Smoking cessation*Smoking cessation*
*Hegedius L, et al. J. Endocrinol Invest 2004. Mar:27 (3):265-71

Treatment of TAOTreatment of TAO• Treatment of coexistent hyperthyroidism• Immunomodulatory (most effective in active
phase)• Steroid Therapy
• PO, IV• Radiation Therapy
• Surgery (three step-reserved for stable disease)• Orbital decompression• Muscle surgery• Eyelid surgery
Wiersinga WM. Nat Clin Pract Endocrinol Metab. 2007. 3(5):396-404.

Bartelena L. et al. Bartelena L. et al. NEJM NEJM 338:2;73-78.1998338:2;73-78.1998
In a RCT, treatment with RAI alone led to development or worsening of: ophthalmopathy (15%) compared to methimazole (3%), RAI + prednisone (0%)
Treatment of co-existent hyperthyroidismTreatment of co-existent hyperthyroidism

• Steroid TherapySteroid Therapy• Never tested for efficacy Never tested for efficacy
against placebo.against placebo.• 60-90% response- Most 60-90% response- Most
efficacious early in disease efficacious early in disease process. process.
• Rapid improvement Rapid improvement (48hr) of inflammation, (48hr) of inflammation, soft tissue changes, optic soft tissue changes, optic neuropathy neuropathy ±±
• Proptosis, diplopia- less Proptosis, diplopia- less responsiveresponsive
• Relapse upon Relapse upon discontinuation-tapering/Side discontinuation-tapering/Side effecteffect
• Multiple routes (PO, IV, Local)Multiple routes (PO, IV, Local)• Can usually be safely with cautionCan usually be safely with caution
Bartalena et. al. Endocrine Reviews. 2000
Immunomodulatory therapy for Active Immunomodulatory therapy for Active TAOTAO

Immunomodulatory therapy for Active Immunomodulatory therapy for Active TAOTAO
• Retrobulbar irradiation-for active TAORetrobulbar irradiation-for active TAO• Rationale-Rationale-
• Non-specific anti-inflammatory effectsNon-specific anti-inflammatory effects• Radio-sensitivity of lymphocytesRadio-sensitivity of lymphocytes
• EfficacyEfficacy• Improvement occurs in 1-4 wks, continues 1yrImprovement occurs in 1-4 wks, continues 1yr• Equally as effective as oral steroids (~65%) (Double Equally as effective as oral steroids (~65%) (Double
blind, RCT, Prummel PF et al. Lancet. 1993) blind, RCT, Prummel PF et al. Lancet. 1993)

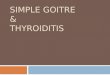
GD Associated ManifestationsGD Associated ManifestationsDermopathyDermopathy
• DiagnosisDiagnosis• Often associated with severe TAOOften associated with severe TAO• Non-pitting edemaNon-pitting edema• Peau d’orange texturePeau d’orange texture• Friable, weepy skinFriable, weepy skin(in the appropriate setting)(in the appropriate setting)
• TherapyTherapy• Local application of corticosteroidsLocal application of corticosteroids• Avoid trauma/biopsyAvoid trauma/biopsy• Does not improve with correction Does not improve with correction
of hyperthyroidismof hyperthyroidism
• PathogenesisPathogenesis• UnknownUnknown
• HistologyHistology• Glycosaminoglycan Glycosaminoglycan
(hyaluronan) deposition in (hyaluronan) deposition in dermisdermis
Fatourechi V. Am J Clin Derm. 2005; 6(5):295-309

Other manifestations of GDOther manifestations of GD
• AcropachyAcropachyTriad of:Triad of:• digital clubbingdigital clubbing• Soft tissue swelling of Soft tissue swelling of
hands and feethands and feet• Peri-osteal new bone Peri-osteal new bone
formationformation

Euthyroid Graves’ diseaseEuthyroid Graves’ disease• TAO consistent with GD in a patient with TAO consistent with GD in a patient with
normal thyroid functionnormal thyroid function• DDX includes orbital or retro-orbital tumor, DDX includes orbital or retro-orbital tumor,
lymphoma. Helpful clues include:lymphoma. Helpful clues include:• History suggestive of previous History suggestive of previous
hyperthyroidismhyperthyroidism• Measurement of TSIMeasurement of TSI• Orbital MRI to exclude involvement of orbital Orbital MRI to exclude involvement of orbital
muscle tendonsmuscle tendons• Orbital CTOrbital CT

TAOTAO TumorTumorEye Lid RetractionEye Lid Retraction CharacteristicCharacteristic UncharacteristicUncharacteristic
Eye Lid SwellingEye Lid Swelling DiffuseDiffuse NodularNodular
EOM Motility DeficitEOM Motility Deficit CommonCommon RareRare
TendonsTendons SparedSpared InvolvedInvolved
AgeAge YoungerYounger OlderOlder
Differential DiagnosisDifferential Diagnosis