Embed Size (px)
Citation preview

Thyroid Disorders in the Elderly: Does it Matter
Don Bodenner MD-PhDAssociate Professor
Central Arkansas VAMC, Geriatric Research Education and Clinical Center
Department of Geriatrics
Reynolds Institute on Aging
Chief, Endocrine Oncology
Director, Thyroid Center

TSH
T4
T3
BrainKidneyMuscleLiverSkinHeart thyroid
pituitary
T4
T3
TSH moves opposite of thyroid hormone levels

Changes with Aging
Some decrease in pituitary/hypothalamic response
Most elderly not clinically significant. The incidence of hypothyroidism
increases with age The incidence of hyperthyroidism
increases with age (nodules)
Subclinical Thyroid Disease: Difficult Cases
Thyroid levels in the normal range TSH levels abnormally high or low No overt clinical signs or symptoms of
thyroid dysfunction ATA prefers “mild thyroid failure or
dysfunction”
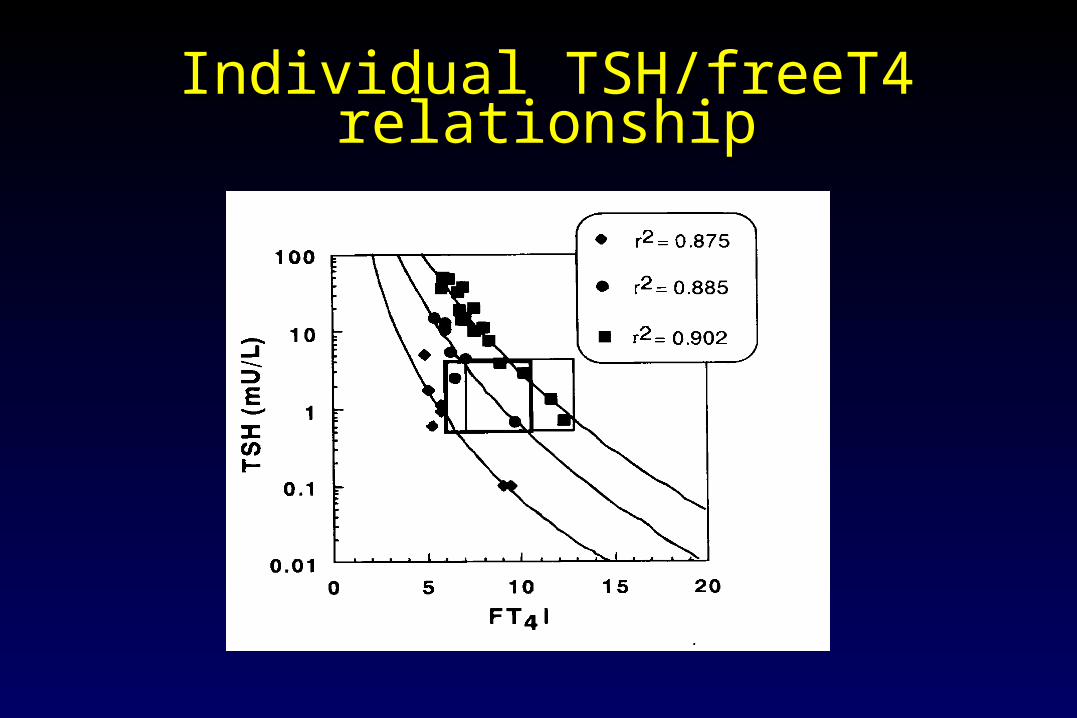
Individual TSH/freeT4 relationship

Normal Ranges:Individual vs. Group
individual <<groupe.g. free T4
individual groupe.g. TSH (?)

Clinical Presentation of Hypothyroidism (all patients)
Scoring system established in 1969.
Review of utility of these measures in 1997 (average age 55 years)
Zulewski JCEM (1997) 82:771

Subclinical Hypothyroidism: prevalence
Geriatric Clinic US 15 %
Community England 17 % Senior Citizen Center US 14 % Community US 14 % Community New Zealand 4 % Senior Citizen Center Italy 0.6 %
Highly dependent upon screening norms in community and Iodine intake

Subclinical hypothyroidism: Is it important
Homocysteine decreased
Diekman, Clin Endo (2001) 54: 197-204
subclinical hypothyroidism 2-3 times more frequent in people with elevated cholesterol
Tanis, Clin Endo (1996) 44: 643-649

Subclinical hypothyroidism: Cardiac effects
Rotterdam Study Population based study
studying chronic disease in the aging population (>55 at entry
3105 men, 4878 women TSH > 4.0 with normal free
thyroxine

Rotterdam Study
Hak, A. E. et. al. Ann Intern Med 2000;132:270-278
1.7 1.9
2.3 2.3

Rotterdam Study

Japan: Ischemic Heart Disease and SCH
2,856 subjects screened for thyroid dysfunction
257 with subclinical hyothyroidism TSH > 5 Prior thyroid disease or thyroid hormone
therapy excluded Initial screening 1984 to 1987 10 year follow-up
Japan: Ischemic Heart Disease and SCH
Ischemic heart disease: EKG changes consistent with
MI Enzyme elevation Positive exercise test
Death as second endpoint

Japan: Ischemic Heart Disease and SCH
Controls (%) Subclinical Hypothyroidism (%)
OR (95% CI)
All subjects 1.3 3.5 2.5
males 1.6 6.8 3.8
females 1.1 1.8 1.8

Japan: Ischemic Heart Disease and SCH
Men had significant increase in all cause mortality
Increase trend for women
Men had increase in non-neoplastic related deaths
men
women

Basel Thyroid Study 66 women with SCH, Randomized to
placebo and titration with T4 until TSH normalized
Age 57 years (18-75), TSH greater than 5 on two tests
Total and LDL reduced after T4 Apo B-100 decreased (p<.03) Billewicz scores improved (p=.02)
Subclinical hypothyroidism: natural history
30 patients (24 men, 6 women) referred with subclinical hypothyroidism
Kabadi, Arch Intern Med (1993) 153: 957-961
16/30 progressed to frank hypothyroidism
14/30 remained stably elevated

Pathogenic factors leading to hypothyroidism
Previous iodine 131 or subtotal thyroidectomy for hyperthyroidism7
Hashimoto’s (autoimmune thyroiditis)4
Radical neck dissection or neck radiation therapy2
for malignancy Long-term lithium therapy
1 idiopathic
2
Cause Patients
Kabadi, Arch Intern Med (1993) 153: 957-961

Hashimoto’s and development of hypothyroidism
30% at five years, 60% at 10 years with positive antibodies
Jcem 87:3221

Who to treat with mild TSH elevations?
Measure anti-TPO aby, if positive, then treat. If negative, follow every 6 months
Monitor patients closely every 6 months, with history of neck irradiation, lithium exposure, radioactive iodine treatment

Evaluation and treatment of hypothyroidism
All patients over the age of 50, screening TSH Repeat every 5 years with family history. Sooner
with symptoms. If 5-10, repeat TSH on at least two occasions Treat for even mild elevations in TSH if indicated
(antibodies, I131, radical neck, radiation Any hint of CAD, start at 25 mcg/day, increase
every month with TSH measured to normal

Sublcinical Hyperthyroidism
Very poorly understood TSH must be suppressed (< .1), not
lower than normal Common in elderly with multinodular
goiter Treatment controversial

Hyperthyroidism:Signs and Symptoms
Nervousness Fatigue/weakness Heat Intolerance Hyperdefecation Palpitations Weight
loss/Increase appetite
Tremor
Hyperactivity Lid retraction Hyperreflexia Goiter Opthalmopathy Localized edema Menstrual
disturbances

Elderly: Apathetic Thyrotoxicosis
-may present as depression
-apathy, lethargy, pseudo-dementia, extreme weight loss, are common
-pulse can be minimally elevated
-goiter, heat intolerance, eye signs often absent
-scan and uptake can be normal
Subacute thyroiditis Viral induced, self-limiting, hyperthyroidism
followed by hypothyrodism. Uptake very low. ESR elevated
Exogenous thyroid hormone Iodine exposure (IV contrast, kelp, amiodarone) Graves’ Autonomous nodule or toxic multinodular goiter
Causes of Subclinical hyperthyroidism

TSH vs number of nodules

Cardiovascular disease and subclinical hyperthryoidism
All cause mortality increased 1.8 fold after 5 years of followup
Cardiovascular events increased 2.2 fold
Cerebrovascular events incresed 2.8 fold
Lancet 358:861

24 Hour Holter Monitoring after therapy Increase in atrial premature beats
(p<.001) Increase in premature ventricular beats
(p<.003)
Cardiovascular disease and subclinical hyperthryoidism
JCEM 88: 1672
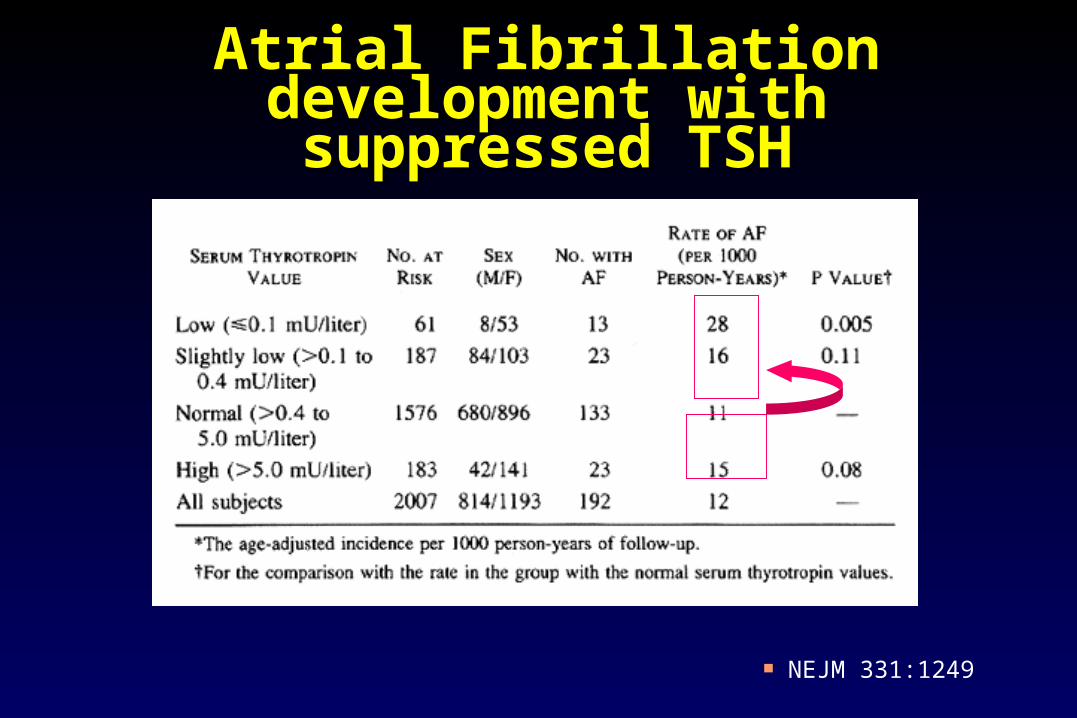
Atrial Fibrillation development with suppressed TSH
NEJM 331:1249

Atrial Fibrillation with suppressed TSH
NEJM 331:1249

Subclinical hyperthyroidism and bone
Increase in markers of bone resorption Postmenopausal women
Loss of up to 1.8% of bone mass per year in femoral neck and lumbar spine
Fracture risk unknown Treatment increased BMD at hip and
spine by 1 to 2 % vs a drop of 2 to 5% in untreated patients

Rotterdam study 1843 participants over age 55 2 years of follow-up TSH level <.4 Dementia assessed by
MMSE < 26, Cambridge examination for disorder of elderly Examination by neurologist and neyropsychologist
Exclusions: prior dementia, antithyroid medications, amiodarone,
Dementia and subclinical hyperthyroidism

Dementia and subclinical hyperthyroidism (RR, 95% CI)
Total dementia Alzheimer’s disease
TSH < .4 3.5 3.5
TSH < .4 with positive antibodies 23.7 14.3
TSH > 4.0 .5 .6

Evaluation and treatment of subclinical hyperthyroidism
Repeat TSH on at least 2 occasions 24 hour radioactive iodine uptake Thyroid ultrasound Exclude medications (amiodarone) and
recent IV contrast

Evaluation and treatment of subclinical hyperthyroidism
No signs, symptoms, depression or weight loss Monitor TSH, free T4 and T3
Signs, symptoms, weight loss or depression Trial of antithyroid medications or I131 ablative therapy Surgery rarely required

Thyroid Nodules in the Elderly
• Nodules are very common• Prevalence: 5% palpation, 50%
autopsy and ultrasound• By middle age, half of the
population will have a nodule.• The prevalence is much higher
in women

Davies, L. et al. JAMA 2006;295:2164-2167.
Trends in Incidence of Thyroid Cancer (1973-2002) and Papillary Tumors by Size (1988-2002) in the United States

On the other hand…..
Thyroid cancer “uncommon” In 2001, ACS estimates thyroid cancer 1.5
% of all new cancers SEER (NCI) estimates prevalence 0.1% of
all Americans Death even more uncommon, 0.23% of all
cancer deaths, IN THE YOUNG

Everyone does well with thryoid CA
recurrence
death
Age 70 at dx, 40% mortality

Thyroid Cancer:
1. Papillary most common, (> 70%) a.) Local invasion b.) Good prognosis (10 year survival >90%)
2. Follicular (15%) a.) Invasion into vessels, metastasis more likely b.) Good prognosis (10 year survival 65-85%)

Thyroid Cancer:
Medullary a.) Associated with MEN syndromes b.) Fair prognosis
Anaplastic a.) Local invasion and distant metastasis b.) Fast growing c.) Poor prognosis

Ionizing radiation and thyroid cancer
No threshold dose cancers develop 20-30 years later 50% of patients develop thyroid
abnormalities 15-30% will develop thyroid cancer earlier the exposure, higher risk of cancer.

Thyroid “Facts”
Cancer is unlikely in a gland with Hashimoto’s thyroiditis.
Cancer is less likely in a multinodular goiter. Its only a cyst. Bigger nodule, more likely cancer
……The risk of cancer is almost the same in any
thyroid nodule …. 4 - 6 %
Simple Cyst is always benign
Uncommon, 1% of all cysts Complex cysts
septations intracystic cells or sedimentation Risk of thyroid cancer identical to
nodule in a multinodular gland

Size and Malignancy
NO CORRELATION BETWEEN SIZE AND PRESENCE OF THYROID CA
Prevalence of thyroid cancer in sub-centimeter lesions greater than in those over one centimeter 1
Prevalence the same (app 6%) as in clinically apparent solitary thyroid nodules. 2
1 Leenhardt JCEM 84:24 2 Hagag Thyroid 8:989

Frequency of Malignancy in MNG
Belfiore A et al. Am J Med 1992. 93:363
4.7 % vs 4.1%

Thyroid Scan
Malignant nodules are cold Benign nodules are cold
Benign colloid nodules Hashimotos Cysts
Hot nodules rare in the US (app 1%)
Very limited role for scan and uptake in initial evaluation of thyroid nodule

Author PET scans
Incidentaloma Biopsy Malignancy
Cohen 4525 102 (2.3%) 15 7 (47%)
Kim 4136 45 (1.1%) 32 16 (50%)
Chu 6241 76 (1.2%) 14 4(28%)
Yi 140 7 (4.3%) 7 4 (57%)
Davis 1285 - 5 5 (100%)
Van den Bruel - 8 7 5 (71%)
Very useful in staging many cancers including thyroid cancer
Initial reports had incidence of thyroid ca as high as 75%
thyroid cancer in incidental PET positive thyroid nodules


FNA: the procedure 4-8 passes of a 22 or usually 25 gauge needle to
obtain the specimen 20 minutes start to finish no local anesthetic (expect ice in a plastic bag) neck tenderness for about 24 hrs afterwards Among >11000 FNA procedures over 12 years at Mayo
Clinic: no infections, one patient required surgery for acute tracheal compression after bleeding into the nodule

FNA: the results
92-98% predictive values for a result either of a malignancy or a benign lesion
35-75% reduction on patients undergoing thyroidectomy
suspicious lesions referred for surgery about 15-20% of all aspirations yield inadequate
material for diagnosis -- more in MNG (degenerated or hemorrhagic nodules)
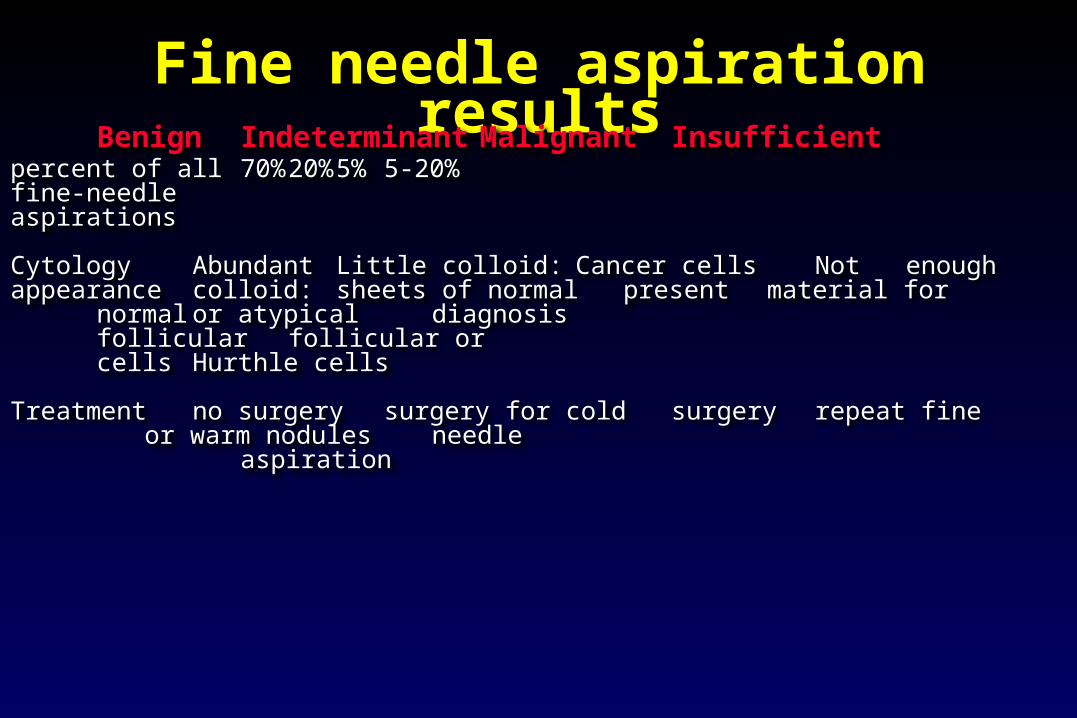
Fine needle aspiration resultsBenign Indeterminant Malignant Insufficient
percent of all 70% 20% 5% 5-20%fine-needle aspirations
Cytology Abundant Little colloid: Cancer cells Not enough appearancecolloid: sheets of normal present material for
normal or atypical diagnosisfollicular follicular orcells Hurthle cells
Treatment no surgery surgery for cold surgery repeat fineor warm nodules needle
aspiration

Ultrasound features Indicative of Cancer
Papini JCEM 87:1941
% occurrence RR specificity
Blurred margin 77 16 87
Intranodal vascularity 74 14 85
Microcalcifications 29 4.9 96

Insufficient Samples
Take time to read the cytopath report carefully “negative for cancer” is often used for insufficient
samples 10-15% of nodules with repeatedly insufficient
samples will be malignant “three strikes and your out”. Incidence
approximates 20 %

The Conundrum…..

Contact InformationContact Information
For any questions about this audio conference please contact Dr. David Bodenner at [email protected]
For any questions about the monthly GRECC Audio Conference Series please contact Tim Foley at [email protected] or call (734) 222-4328
To evaluate this conference for CE credit please obtain a ‘Satellite Registration’ form and a ‘Faculty Evaluation’ form from the Satellite Coordinator at you facility. The forms must be mailed to EES within 2 weeks of the broadcast
For any questions about this audio conference please contact Dr. David Bodenner at [email protected]
For any questions about the monthly GRECC Audio Conference Series please contact Tim Foley at [email protected] or call (734) 222-4328
To evaluate this conference for CE credit please obtain a ‘Satellite Registration’ form and a ‘Faculty Evaluation’ form from the Satellite Coordinator at you facility. The forms must be mailed to EES within 2 weeks of the broadcast