-
Thyroid DiseaseAnd OsteoporosisLisa Hays, MDEndocrinology
Fellow
-
OutlineSigns and symptoms of hyperthyroidismDiagnostic studies
for hyperthyroidismCauses and treatments of hyperthyroidismGeneral
overview of hypothyroidismEvaluation of thyroid nodulesOverview of
osteoporosis
-
Cellular effects of thyroid
-
Hyperthyroidism
SymptomsAnxiety/irritabilityWeaknessTremorsDifficulty
sleepingPalpitationsIncreased bowel movementsFatigueWeight loss
Hyperkinetic movementsHeat intolerance
-
Case Presentation37 yo male presented to PCP w/ complaint of
feeling poorly for past monthAlso complained of weakness,
difficulty sleeping, increased heart rate. 10 stools per day.What
else do we need to know before examining?
-
Case PresentationT 99.1, HR 92 irregular, RR 20, BP
153/75Physical examinationMild proptosisNontender goiter with
thyroid bruit presentCV: Irregularly irregular rhythmExt: Brisk
DTRs, mild resting tremorWhat labs or studies do we need?
-
Laboratory StudiesTSH 6 ng/dl (nl 0.71-1.85)Total T3 >600
ng/dl (nl 72-170)Thyroid Stimulating Antibody 130% (nl
0-125%)Negative Thyroid peroxidase and thyroglobulin antibodies
-
Case PresentationPatient was diagnosed with Graves
DiseaseStarted on Methimazole 10 mg TIDPropranolol for symptom
managementAnticoagulation for atrial fibrillation
-
Thyroid AntibodiesTSH receptor antibodiesCan be stimulating or
inhibitoryThyroglobulin antibodiesThyroid peroxidase antibodies
(formerly known as microsomal)
-
Anything else?Radioactive Iodine UptakeMeasures the amount of
iodine taken up by the thyroid in 24 hoursNormal 15-30%Thyroid
ScanGives an anatomic view of the thyroidTechnetium used to
image
-
Differential DiagnosisHigh uptakeGraves DiseaseMultinodular
GoiterToxic solitary NoduleTRH secreting Pituitary TumorHCG
secreting tumorLow uptakeSubacute ThyroiditisSilent
ThyroiditisIodine induced Exogenous L-ThyroxineStruma
ovariiAmiodarone
-
Graves DiseaseMost common cause of hyperthyroidism60-80% of
casesAutoimmune diseaseCaused by thyroid stimulating
immunoglobulinsBind to TSH receptors on thyroidCause
hypersecrection of thyroid hormoneCause hypertrophy &
hyperplasia of thyroid follicles
-
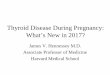
Weetman, A. P. N Engl J Med 2000;343:1236-1248Pathogenesis of
Graves' Disease
-
Clinical ManifestationsSymptoms and signs of
hyperthyroidismOphthalmopathyPresent in 50% of patientsEyelid
retractionPeriorbital edemaProptosis
(exopthalmos)DiplopliaDermopathy (myxedema)
-
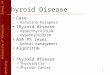
Weetman, A. P. N Engl J Med 2000;343:1236-1248Clinical
Manifestations of Graves' Disease
-
Graves DiseaseAssociated ConditionsType I Diabetes
MellitusAddisons DiseaseVitiligoPernicious anemiaAlopecia
AreataMyasthenia GravisCeliac Disease
-
Graves TreatmentAntithyroid drugs (Thionamides)Proplythiouracil
(PTU) 300-400 mg dailyMethimazole 30-40 mg dailyDecrease synthesis
of hormone, PTU also decreases conversion of T4 to T3Permanent
remission in 40-50% of treated patientsRisk of agranulocytosisPTU
used in pregnancyBeta-Blockers for symptoms
-
Graves TreatmentThyroidectomyRapid cure but requires thyroid
replacementRadioactive Iodine Iodine (131I) is givenEffect is
typically seen in 3-6 monthsHypothyroidism often develops
-
Multinodular GoiterLess common than Graves and effects older
individualsDiscrete nodules become autonomous and
hyperfunctionTreatment with thyroidectomy (often poor surgical
candidates) or iodine, thionamides
-
Subacute ThyroiditisEtiology is typically viralKnown as De
Quervains thyroiditis or granulomatous thyroiditisThyroid is often
enlarged, tender, painfulVery low radioactive iodine
uptakeSelf-resolving within weeks to monthsTreatment with NSAIDS,
steroids, Beta-blockers
-
Silent ThyroiditisAlso called painless or lymphocytic
thyroiditisNot painful like subacuteTransientLow iodine uptake
-
HypothyroidismWeaknessFatigueLethargy, sleepinessSlowness of
speech and thoughtPuffy appearanceDry skin, coarse hairCold
intoleranceConstipation
-
Physical FindingsPuffy featuresDry skinNonpitting
edemaHypothermiaBradycardiaSlow return of deep tendon reflexesLoss
of lateral portion of eyebrows
-
Causes of HypothyroidismPrimary HypothyroidismIodine
deficiencyIatrogenic-surgery, radioablationAutoimmune thyroid
destructionDrugs interfering with hormone synthesisInfiltrative
diseasehemochromotosis, sarcoidosis, neoplastic diseaseCongenital
thyroid agensis or defects in hormone synthesis
-
Hashimotos ThyroiditisMost common type of thyroid
diseaseAutoimmune damageLymphocytic infiltrate, fibrosis, decreased
thyroid hormone productionAutoantibodies (thyroglobulin and
peroxidase)Can also be associated with polyglandular autoimmune
diseaseAdrenal insufficiency, ovarian failure, vitiligo,
diabetes
-
Thyroid ReplacementSynthetic levothyroxine (T4)Converted to T3
in the bodyStudies vary on utility of using T3 Typical replacement
dose is 1.6 micrograms/kg (100-150 mcg typical)Start with reduced
dose in elderly and patients with history of heart disease
-
Myxedema ComaSevere untreated hypothyroidismHypothermia,
hypoglycemia, shock, hypoventilation, ileus50% mortalityTreat with
IV levothyroxine, steroids
-
Thyroid Nodule21 yo male w/ no past medical history presents to
his PCP complaining of gradually enlarging knot in his neckWhat
questions do you have?Examination reveals a firm 3 cm nodule in
right lobe of thyroidWhat is the next step?
-
Thyroid NodulesLifetime risk of palpable nodule 5-10%50% of the
population has a nodule on autopsy or ultrasoundOnly 1 in 20 is
malignant
-
Differential
DiagnosisMalignancyPapillaryFollicularMedullaryAnaplasticMetastasisBenign
follicular adenomaCystColloid Nodule
-
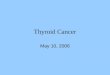
Hegedus, L. N Engl J Med 2004;351:1764-1771Algorithm for the
Cost-Effective Evaluation and Treatment of a Clinically Detectable
Solitary Thyroid Nodule
-
Hegedus, L. N Engl J Med 2004;351:1764-1771Clinical Findings
Suggesting the Diagnosis of Thyroid Carcinoma in a Euthyroid
Patient with a Solitary Nodule, According to the Degree of
Suspicion
-
Evaluation of NoduleMeasure TSHIf Hyperthyroid (low TSH), do
uptake and scanTreat with surgery or I-131 ablationIf normal
thyroid function, next step is fine needle aspiration (FNA)Check
Calcitonin level if family history of MEN2 or medullary carcinoma
exists.
-
Hegedus, L. N Engl J Med 2004;351:1764-1771Algorithm for the
Cost-Effective Evaluation and Treatment of a Clinically Detectable
Solitary Thyroid Nodule
-
Fine Needle AspirationFNA is most effective way to distinguish
between benign and malignant nodulesInexpensive, performed as
outpatientUltrasound guided FNA if not palpable or less than 1.5 cm
in diameterWhat results will I see?Benign-75% of the
timeMalignant-4% of casesSuspicious or inadequate-22%
-
Hegedus, L. N Engl J Med 2004;351:1764-1771Algorithm for the
Cost-Effective Evaluation and Treatment of a Clinically Detectable
Solitary Thyroid Nodule
-
Management of NodulesMalignantTotal
thyroidectomySuspiciousThyroidectomyBenignDiscuss with the
patientUltrasound surveillanceSurgeryConsider levothyroxine
suppression (varying results)
-
Case PresentationFNA revealed papillary thyroid carcinomaPatient
underwent total thyroidectomyTreatment with I-131 ablation after
surgery
-
Osteoporosis
-
Case Presentation70 year old female asks her PCP if she should
have a bone density done.What questions should her PCP ask?No
history of fracturesMenopause was surgical at age of 55Mother
fractured her hip at 74
-
OsteoporosisDefinitionMicroarchitectural deterioration of bone
tissue leading to decreased bone massBone fragilitySusceptibility
to fractureA problem of decreased peak bone mass and accelerated
bone lossAffects 10 million in the United States
-
1. Consensus Development Conference. Am J Med.
1993;94:646-650.2. Riggs BL, Melton LJ III. Bone.
1995;17:505S511S.3. Ray NF et al. J Bone Miner Res.
1997;12(1):2435.4. Cummings SR et al. Arch Intern Med.
1989;149:24452448.Hip Fractures Can Lead to Disability, Loss of
Independence, and Even DeathHip fracture is associated with
increased risk of:Disability: 50% never fully recover1,2 Long-term
nursing home care required: 25%2Increased mortality within 1 year
due to complications: up to 24%3Lifetime risk of death: comparable
to that of breast cancer4
-
OsteoporosisPrimary osteoporosisUnrelated to chronic
illnessRelated to aging and decreased gonadal functionSecondary
osteoporosisSecondary to chronic illnesses that cause accelerated
bone lossExamples: Glucocorticoid use, celiac sprue,
hyperthyroidism
-
Risk Factors for Osteoporotic FractureNonmodifiablePotentially
ModifiableGold color denotes risk factors that are key factors for
risk of hip fracture, independent of bone density.National
Osteoporosis Foundation, Physicians Guide to Prevention and
Treatment of Osteoporosis. Belle Mead, NJ: Excerpta Medica, Inc.;
1998.
-
Diagnosis of OsteoporosisHistory and physical examination to
exclude secondary osteoporosisLaboratory studies if suspect
secondary osteoporosisMeasurement of Bone Mineral Density (BMD)Dual
X-ray Absorptiometry (DEXA scan)Provides most reproducible values
of bone densityg/cm2
-
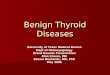
6070809010030405060708090AgeRelative BMD (%)ForearmSpineHip and
Heel0100020003000400035-3985+Colles'VertebraeHipAgeAnnual Fracture
IncidenceCooper C. Baillires Clin Rheumatol. 1993;7:459477.Faulkner
KG. J Clin Densitom. 1998;1:279285.BMD and Fracture Risk Are
Inversely Related
-
Central DXA MeasurementMeasures multiple skeletal
sitesSpineProximal femurForearmTotal bodyOffice basedConsidered the
clinical standard
- National Osteoporosis Foundation, Physicians Guide to
Prevention and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta
Medica, Inc.; 1998.National Osteoporosis Foundation GuidelinesWho
Should Be Considered for BMD Testing?Women 65 years of age
regardless of additional risk factorsPostmenopausal women
-
Other Populations To Consider for Assessment of
OsteoporosisMenPatients on long-term high-dose glucocorticoids
-
T-Score Is KeyInterpreting BMD Measurement ReportsA clinically
relevant value on the BMD reportDescribes bone mass compared with
the mean peak bone mass of healthy young adult women in terms of
Standard Deviation (SD)Can help confirm the diagnosis of low bone
mass or osteoporosisFor every SD below the young adult normal, the
risk of fracture approximately doubles
1. National Osteoporosis Foundation, Physicians Guide to
Prevention and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta
Medica, Inc.; 1998. 2. Marshall D. Johnell O, Wedel H.
Meta-analysis of how well measures of bone mineral density predict
occurrence of osteoporotic fractures. BMJ. 1996;312:12541259.
-
SDAge (years)21012345620 30 40 50 60 70 80 90T-score = 3.0Peak
Bone MassVisualizing a Patients T-ScoreT-score = Number of standard
deviations (SDs) by which the patients bone mass falls above or
below the mean peak bone mass for normal young adult women =
T-score for patient, a 60-year-old woman; here, T = 3.0Light line:
Change in mean bone mass over time in womenHeavy line: Mean peak
bone mass for young normal adult women National Osteoporosis
Foundation, Physicians Guide to Prevention and Treatment of
Osteoporosis. Belle Mead, NJ: Excerpta Medica, Inc.; 1998.
-
National Osteoporosis Foundation, Physicians Guide to Prevention
and Treatment of Osteoporosis. Belle Mead, NJ: Excerpta Medica,
Inc.; 1998.T-SCOREACTION
< 2.0Initiate therapy
< 1.5Initiate therapy(with at least 1 additional risk
factor)National Osteoporosis Foundation Guidelines for
postmenopausal WomenRecommendations for Treatment Based on BMD
Testing Results
-
Treatment of OsteoporosisAdequate Calcium (1200 mg
elemental)Adequate Vitamin D (at least 400 IU)Weight-bearing
exercise
-
Pharmacologic AgentsBisphosphonatesInhibit osteoclastic bone
resorptionIncreased BMD and decreased fracturesEx: alendronate,
risedronateCalcitoninNasal spray or injectionDecreased vertebral
fracturesNo hip fracture dataRaloxifenSERMDecreased vertebral
fracture
- Osteoporosis SummaryOsteoporosis is a disease with serious
consequences.Bone loss associated with osteoporosis increases
fracture risk, which may lead to disability, loss of independence,
and death.Patients at risk for osteoporotic fracture should be
considered for BMD testing.T-score is the most clinically relevant
measure of fracture risk.According to NOF guidelines, consider
therapy in patients with a T-score of