Embed Size (px)
Citation preview

A.Arputha Selvaraj APMP IIM Calcutta
2
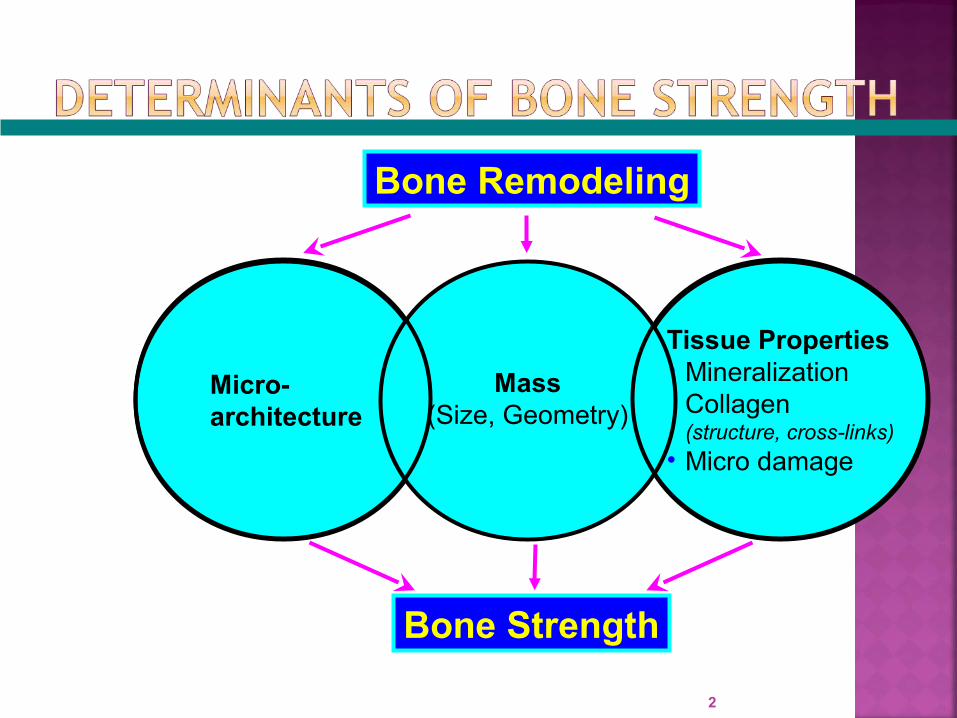
Bone Remodeling
Bone Strength
Tissue Properties• Mineralization• Collagen
(structure, cross-links)• Micro damage
Micro-architecture
Mass(Size, Geometry)
3
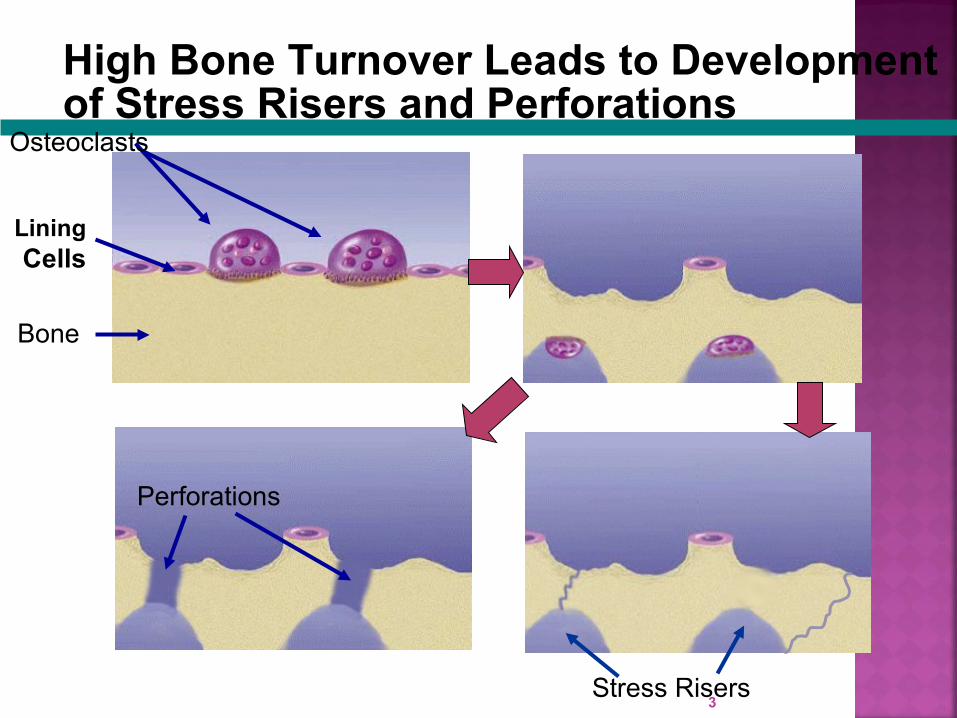
High Bone Turnover Leads to Development of Stress Risers and Perforations
Lining Cells
Bone
Osteoclasts
Stress Risers
Perforations

4 4
NormalNormal22 OsteoporosisOsteoporosis22
““Osteoporosis is a skeletal disorder characterized by Osteoporosis is a skeletal disorder characterized by compromised bone compromised bone strengthstrength predisposing a person to an predisposing a person to an increased risk of fractureincreased risk of fracture.”.”11
1. Consensus Development Conference, JAMA 2001; 285: 785-95; 2. Dempster DW et al, JBMR 1986; 1: 15-21.
Increased mineralization in existing bone Increased bone tissue per unit of bone volume:
Filling in resorption spaceWidening existing trabeculaeCreating new trabeculae
Increased bone size
5

Reflected in DXA Measurements:Bone sizeTrabecular volume and cortical thicknessAmount of mineralization in bone and surrounding
tissuesNot Reflected in DXA Measurements:
Trabecular connectivity and number Collagen quality Microscopic damage (e.g. microcracks) Bone geometry
6

According to the National Osteoporosis Foundation (NOF):
“Osteoporosis (porous bone) is a disease characterized by low bone
mass and structural deterioration of bone tissue, leading to bone
fragility and an increased susceptibility to fractures of the hip,
spine, and wrist.”
In common practice osteoporosis is seen as disease of compromised
bone strength.
BONE STRENGTH= Bone Quality + Bone Mineral
Density
7
The most common type of fractures in men and women is vertebral, followed by hip fractures.Vertebral fractures are associated with
Acute and chronic pain Height loss and spinal deformity Decreased mobility and work capacity Diminished self confidence.
Vertebral, hip and forearm fractures are strong signals for increased risk of additional osteoporotic fractures.
8
9
Factors that can affect the rate of bone loss: thinness. inactivity. calcium intake. vitamin D. smoking. alcohol. corticosteroids.
10

Lumbar spine region most prone to osteoporosis
11

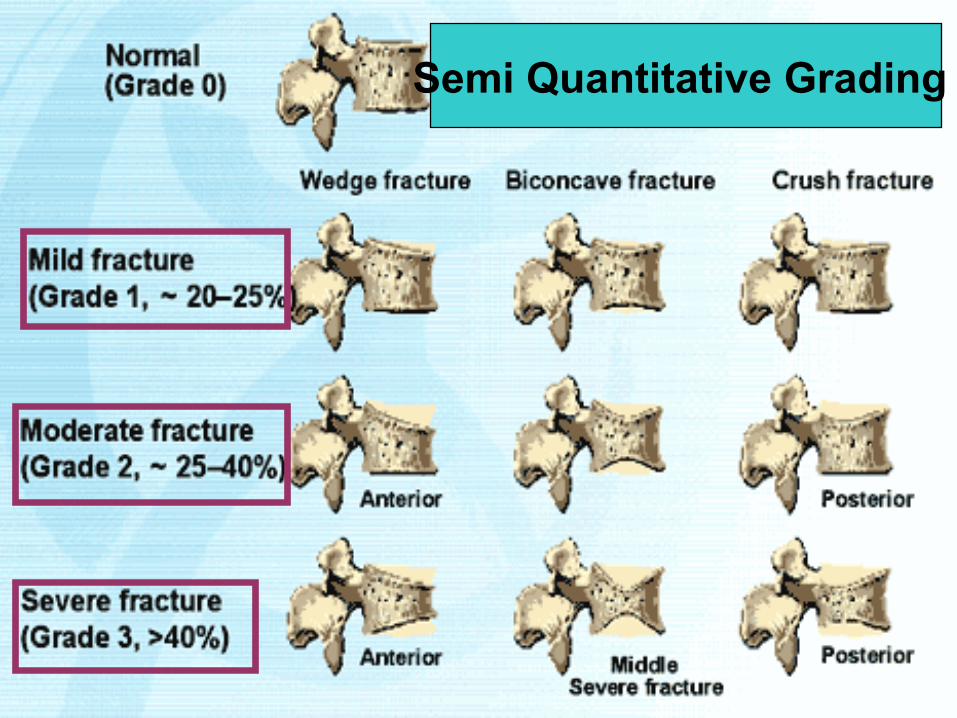
Vertebral Fractures:Osteoporotic crush fractures of the vertebrae may occur in various forms.The vertebral body may be:
Compression fracture – compressed only in the center leading to endplate concavities.
Wedged fracture – collapsed anteriorly causing kyphosis.
Collapse fracture – uniformly compressed.
Collapsed posteriorly (uncommon).
12
13
Semi Quantitative Grading

14
• Kyphosis
• Loss of height
• Bulging
abdomen
• Acute and chronic pain
• Breathing difficulties, reflux and other
GI symptoms
• Depression
REDUCED QUALITY OF LIFE

Initial indications:• Spinal X-ray, Chest X-ray or Bone Mineral
Densitometry leads to suspicion of Osteoporosis, but not confirmation.
• As Low BMD or fractures are not only due to Osteoporosis, physicians consider the differential diagnosis of causes of low BMD or fracture before concluding that the patient has osteoporosis.
15

X-rays: X-Rays usually pick up bone loss when it’s more than 40% (X-Ray Films look more bright) However, X-rays give some important diagnostic clues
like: Presence of fractures. Pathologic findings such as cancer metastatic to
bone. Deformities indicating disease states other than
osteoporosis (e.g. osteomalacia).
16

17
Kanis JA et al, J Bone Miner Res, 1994;9:1137-1141
T-ScoreNormal - 1 SD and above
Low bone mass
- 1 SD to -2.5 SD
Osteoporosis < -2.5 SD
Established osteoporosis
< -2.5 SD and one or more Osteoporotic fractures
Dual energy X-ray absorptiometry (DXA):•Two X-ray beams with differing energy levels are aimed at the patient's bones. •When soft tissue absorption is subtracted out, the BMD can be determined from the absorption of each beam by bone. •Dual energy X-ray absorptiometry is the most widely used and most thoroughly studied bone density measurement technology
18

19
DEXA MACHINE
X-Ray Source
Scanner

SurgicalNon Surgical
NSAIDS BRACING BED REST PHARMACOLOGICAL TREATMENT
20
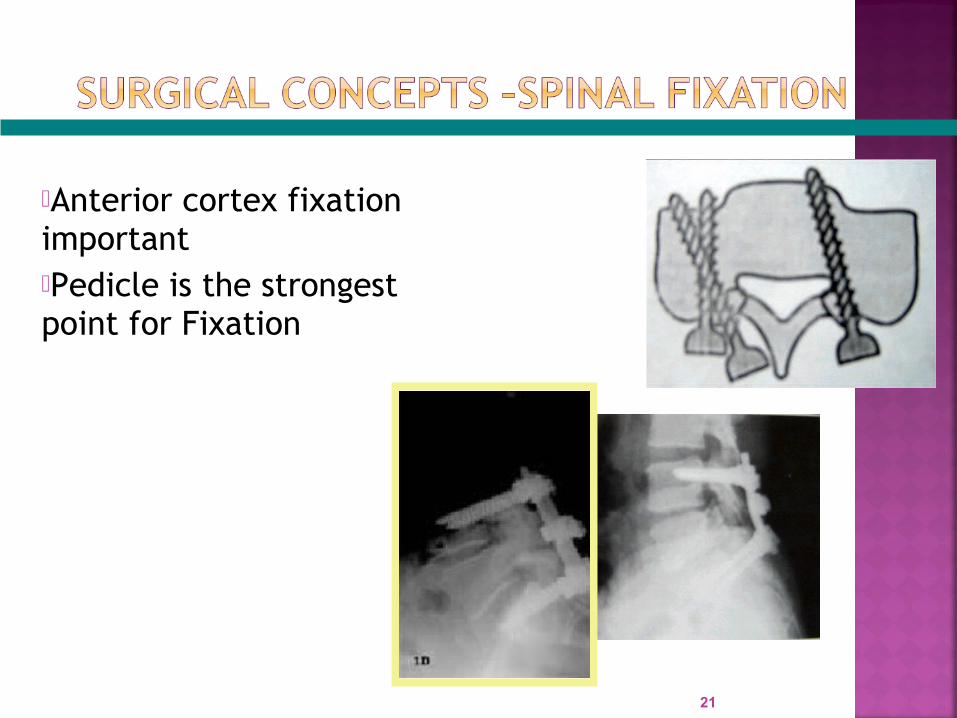
Anterior cortex fixation important Pedicle is the strongest point for Fixation
21

22
Femoral NeckFracture
Intertrochanteric Fracture

23
Dynamic Hip Screws
Prevention and Treatment methods include:• Supplemental calcium and Vitamin D• Hormone replacement therapy (HRT)• Selective estrogen receptor modulators
(SERMs)• Bisphosphonates• Calcitonin• Parathyroid hormone
24

Inhibitors of Bone loss•Estrogen•Selective Estrogen Receptor Modulators•Bisphosphonates•Calcitonin
Formation of Bone•Teriparatide( rhPTH 1-34)
25
Mixed Mechanism of ActionStrontium Ranelate

Hormone Replacement Therapy (HRT):
• Estrogen Replacement therapy (ERT) has been used successfully to arrest bone loss in post menopausal women
• However Estrogen therapy increases Risk of Breast CancerBreast Tenderness, nipple tingling, Bloating Risk of DVT and Pulmonary Embolism
26

Selective estrogen receptor modulators (SERMs):
• SERMs act as estrogen agonists on bone and cardiovascular system, but act as estrogen antagonists on endometrial and breast tissues.
• Two commonly Used SERMs TAMOXIFENE: Used in breast cancer, not in osteoporosis RALOXIFENE: Approved in Osteoporosis and management of
Breast cancer
27

Bisphosphonates:• Bisphosphonates have strong affinity towards
bone surface and eventually get incorporated into the bone crystal
• Nitrogen containing bisphosphonates inhibit the enzyme Farnesyl diphosphate synthatase
• As a result Osteoclasts are unable to resorb the bone and undergo apoptosis
• In early osteoclast precursor cells this results in inhibition of their development into osteoclasts
28
Non Nitrogen containing•Etidronate•Clodronate•Tiludronate
Nitrogen Containing•Alendronate: Osteofos •Risedronate: Actonel•Ibandronate: Bonviva•Zolendronate: Aclasta
29
Bone formation Markers
BSAP( Bone specific alkaline Phosphatase)
PINP( Amino terminal propeptide of Type 1 collagen)
PICP (Carboxy terminal propeptide of Type 1 collagen)
Osteocalcin
Bone resorption Markers
•NTX (N-terminal Telopeptide of Collagen Cross Links)
•CTx (c-terminal telopeptide of collagen cross links)
30