Embed Size (px)
Citation preview

aritti
CASE REPORTS
Thrombotic Endotracheal Tube Occlusion After Administration of RecombinantFactor VIIa
Claudia Benkwitz, MD, PhD, and Gregory Benson Hammer, MD
16dunapRtsriccb
c7Ec
c
RECOMBINANT HUMAN FACTOR VIIa (rFVIIa) pro-motes hemostasis by interacting with both the extrinsic
nd intrinsic pathways of the coagulation cascade.1 AlthoughFVIIa may be very effective in the treatment of severe bleed-ng after cardiac surgery, its cost and potential to cause majorhrombotic complications have limited its use. Data describinghrombotic events associated with rFVIIa are scarce, and theres a debate as to the role of rFVIIa after cardiac surgery.2-4 A
case in which the administration of rFVIIa for persistent bleed-ing after cardiopulmonary bypass (CPB) in a child was fol-lowed by repeated, complete thrombotic occlusion of the en-dotracheal tube (ETT) is presented.
CASE PRESENTATION
A 7.3-kg, 20-month-old female with tetralogy of Fallot, pulmonaryatresia, and major aortopulmonary collaterals was scheduled for revi-sion of unifocalization of the left and right pulmonary arteries, replace-ment of a right ventricle–to–pulmonary artery (RV-to-PA) conduit, andaortopexy. The infant’s past medical history included DiGeorge syn-drome with 22q11.2 deletion, hypocalcemia, impaired hepatic function,anemia, and thrombocytopenia. She also had subglottic stenosis. Thepatient had undergone unifocalization and central aortopulmonaryshunt placement at the age of 3 months. At 9 months of age, sheunderwent revision of the unifocalization and replacement of the cen-tral shunt by an RV-to-PA conduit. The patient’s history was furthercomplicated by several bleeding episodes, including an abdominalbleed during a prior hospitalization and pulmonary hemorrhages after 2diagnostic cardiac catheterizations performed 4 months and 1 monthbefore the current admission.
The patient was admitted to the hospital with progressive hypox-emia. A diagnostic evaluation revealed severe RV-to-PA conduit in-sufficiency, bilateral pulmonary artery branch stenoses, systemic rightventricular pressure, and compression of the distal trachea and main-stem bronchi. Laboratory values on the day of the surgery included ahemoglobin level of 9.5 mg/dL, a serum calcium level of 7.6 mg/dL, aplatelet count of 63,000/�L, a prothrombin time of 16.3 seconds, andan international normalized ratio of 1.4. The partial thromboplastin
From the Department of Anesthesia, Stanford University School ofMedicine, Stanford, CA.
Address reprint requests to Claudia Benkwitz, MD, PhD, Depart-ment of Anesthesia, Stanford University School of Medicine, 300 Pas-teur Drive, Room H3580, MC 5640, Stanford, CA 94305. E-mail:[email protected]
© 2013 Elsevier Inc. All rights reserved.1053-0770/2706-0001$36.00/0http://dx.doi.org/10.1053/j.jvca.2012.07.003Key words: recombinant factor VIIa, complications, coagulopathy,
pediatric cardiac surgery, congenital heart disease, DiGeorge Syn-
odrome (22q11.2del), tetralogy of Fallot1330 Journal of Cardiothoracic and
time was normal. The patient was transported from the cardiovascularintensive care unit (CVICU) to the operating room with an indwelling4.0-mm internal diameter, uncuffed ETT with a built-in closed suction-ing system with an 8F suction catheter (KimVent; Kimberley-ClarkWorldwide, Inc, Neenah, WI) (Fig 1). A positive leak test was obtainedat 20 cmH2O. Anesthesia was induced with ketamine, fentanyl, androcuronium and was maintained with isoflurane, ketamine, and fenta-nyl, with an FIO2 of 1.0. Central and peripheral intravenous and arterialcatheters were placed. An initial dose of aminocaproic acid, 150 mg/kg,was administered followed by a continuous infusion at a rate of 50mg/kg/h throughout the procedure. The pre-CPB period was prolongedbecause of intrathoracic adhesions and distorted cardiac anatomy. After4 hours of dissection, the patient was heparinized with 400 U/kg ofheparin, placed on CPB, and cooled to 25°C. The heart remainedbeating throughout the procedure. After 5 hours of CPB time, theprocedure was completed. The patient was rewarmed and weaned fromCPB without difficulty. Heparin was reversed with protamine, 50 mg,and the Hepcon (Medtronic, Minneapolis, MN) showed no residualheparin effect. Six units of platelets, 2 U of cryoprecipitate, and 20mL/kg of fresh frozen plasma were administered. However, bleedingfrom the surgical wound and aspiration of bloody secretions from theETT persisted. Over the next 1 to 2 hours, additional blood productswere transfused, including 3 U of platelets, 2 U of cryoprecipitate, and30 mL/kg of fresh frozen plasma. Despite this, bleeding from thewound and ETT continued. In agreement with the surgeon, the authorsadministered 90 �g/kg of rFVIIa (NovoSeven; Novo Nordisk, Inc,Princeton, NJ) intravenously.
Within 20 minutes, there was markedly diminished bleeding fromthe surgical field. Ten minutes later, the SpO2 decreased rapidly from00% to 60%, concomitant with increases in peak airway pressures to0 cmH2O and a loss of end-tidal CO2. No breath sounds were audibleespite manual ventilation with high inflating pressures. Inspectionnder the drapes revealed no kinks in the ETT or breathing circuit ando chest movement with attempted ventilation. The authors were un-ble to pass an 8F suction catheter through the integrated inline suctionort (Ballard Inline Suction Catheter; Kimberly-Clark Health Care,oswell, GA) and the ETT lumen directly. With the SpO2 decreasing
o as low as 37%, the authors decided to reintubate the trachea as theurgeons prepared to emergently replace the vascular cannulae andeinstitute CPB. The indwelling ETT was removed, and the trachea wasmmediately reintubated with another 4.0-mm internal diameter, un-uffed ETT under direct laryngoscopy. Peak airway pressures de-reased to 20 to 25 cmH2O, a normal capnograph reappeared, andilateral breath sounds and chest rise were again appreciated. The SpO2
returned to 100% (FIO2 � 1.0) within 2 minutes. The patient had stableirculatory parameters throughout, with mean arterial pressures of 50 to0 mmHg and a heart rate of 110 to 130 beats/min. Inspection of theTT that was removed revealed that it was completely occluded bylotted blood.
The remainder of the anesthetic was without further incident until theompletion of surgery. Thereafter, the patient was moved from the
perating room table to the CVICU bed and was ventilated with aVascular Anesthesia, Vol 27, No 6 (December), 2013: pp 1330-1333

iiaac
raa2rtiaw
tf
srut
s
otosteg
1331THROMBOTIC ENDOTRACHEAL TUBE OCCLUSION
Mapelson D circuit in preparation for transport. Within 2 minutes, thechest compliance appeared to decrease suddenly, with minimal chestexcursion and a decrease in SpO2 to the low 90 seconds despite highnflating pressures. Direct laryngoscopy revealed that the ETT was stilln the trachea. A 10F suction catheter was passed via the ETT, initiallygainst elevated resistance, and clotted blood was aspirated repeatedlyfter irrigation with saline. The ETT eventually was cleared of blood,hest compliance improved, and the SpO2 returned to 100%. The
patient was transported to the CVICU without incident. Laboratoryvalues at that time included a hemoglobin level of 12.1 mg/dL, aplatelet count of 268,000/�L, a prothrombin time of 15.2 seconds, andan internal normalized ratio of 1.3. For the ensuing 12 hours, the ETTwas irrigated and suctioned every hour to prevent recurrent occlusion.No additional doses of rFVIIa were administered. The patient toleratedthis well and later made an uneventful recovery from surgery.
DISCUSSION
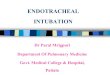
A case of occlusion of an ETT with thrombus associatedwith the administration of rFVIIa in a child undergoing cardiacsurgery is presented. Emergency reintubation under the surgicaldrapes restored ventilation as well as an oxygen saturation of100%. Reinstitution of CPB was averted. Factors likely con-tributing to ETT occlusion included bleeding in the airwayscaused by surgical manipulation and coagulopathy. Prior irri-gation and suctioning of the ETT was limited by the use of aninline suction catheter device. The size of the largest usablesuction catheter was 8F, whereas a 10F catheter would passthrough the ETT without the device (Fig 1).
rFVIIa (NovoSeven) is recombinant human coagulation fac-tor VIIa. It is a glycoprotein consisting of 406 amino acidresidues and is synthesized by the cloning and expression of thehuman factor VII in baby hamster kidney cells. It is similarstructurally to human plasma–derived factor VIIa and is ad-ministered for promoting hemostasis. Although vitamin K isrequired as a cofactor for the �-carboxylation of glutamic acidesidues and, thus, the synthesis of both functional recombinantnd human-derived FVII, recombinant FVII is fully active ondministration because of proteolytic conversion into its active-chain form during chromatographic purification. The mainole of rFVIIa is to initiate the coagulation process in conjunc-ion with the tissue factor (TF). The “VIIa-TF” complex facil-tates the activation of factor X to Xa (ie, the extrinsic pathway)nd the conversion of factor IX to IXa (ie, the intrinsic path-
Fig 1. The Ballard in-line suction system. The diameter of the
suction catheter channel limits the size of the largest catheter that
can be used. Although an 8F catheter can be used with a 4.0-mm
internal-diameter ETT with the built-in suction port, a 10F catheter
can be passed through the same ETT without the Ballard system.
This reduces the ability to evacuate viscous secretions and blood
from the ETT.
ay). In each case, factor Xa ultimately converts prothrombin
o thrombin, which, in turn, leads to the formation of fibrinrom fibrinogen.1
In the United States, rFVIIa has been on the market for morethan 10 years. It is Food and Drug Administration approvedonly for the treatment and prevention of bleeding in patientswith hemophilia A or B with antibodies to factor VIII or IX andcongenital factor VII deficiency.1 However, over the last sev-eral years, rFVIIa has been used off-label for intracerebralhemorrhage5 and intractable bleeding associated with trauma6
or cardiac surgery.3,7 Published data on rFVIIa are limited to amall number of controlled trials, case reports, case series, oretrospective studies. There are very few data available on these of rFVIIa factor in the pediatric cardiac surgery popula-ion.2,4
Neonates and children are at a particularly high risk foradverse effects of cardiac surgery and CPB on coagulationfunction. Severe postoperative bleeding is a major cause ofmorbidity, mortality, and cost in this population. The 2 factorsthat most constrain the use of rFVIIa are cost and the absenceof a well-defined risk/benefit ratio in view of reported throm-botic complications including life-threatening cerebrovascularaccidents, myocardial infarction, and pulmonary embolism inboth pediatric and adult cardiac patients. The incidence ofthrombotic complications remains unknown. A recent Co-chrane review suggested an association between rFVIIa andthromboembolic adverse events, whereas “its effectiveness as amore general hemostatic drug remains unproven.”8
Given that there are fewer than 200 published cases ofrFVIIa use in the pediatric cardiac surgical population, noconclusive statement can be made regarding its safety andefficacy.2,4,9-12 In agreement with the present authors’ observa-tion, most case reports describe the control of an otherwiserefractory post-CPB hemorrhage after the administration ofrFVIIa. In contrast, the only published prospective randomizedtrial did not find differences in bleeding or transfusion outcomebetween the control and rFVIIa treatment groups.13 However, ithould be noted that in that study, only low-dose rFVIIa (40
�k/kg) was administered, in contrast to recommended dosingf 90 to 120 �g/kg as in the present case.14-16 The incidence ofhrombotic complications after rFVIIa administration in post-perative pediatric cardiac surgery patients is unknown. In 1tudy,9 the incidence of thrombotic complications was foundo be as high as 25%. Other authors reported no thromboticvents or no difference between the treatment and controlroups.11,13,15,17
The authors would like to point out the following issues that,in their opinion, are important to consider based on the casedescribed.
1. In addition to the higher susceptibility of the pediatricpopulation to post-CPB coagulopathy, the present pa-tient had been diagnosed with 22q.11.2 deletion. Thismay have significantly aggravated the post-CPB co-agulopathy. Salient features of DiGeorge syndrome(22q.11.2 deletion syndrome) include congenital heartdisease, mainly tetralogy of Fallot, abnormal facies,thymic aplasia resulting in recurrent infections, cleftpalate, and hypocalcemia caused by hypoparathyroid-ism. Although less well known, coagulopathy of a
different etiology consistently has been described in
(
a2
f2
V
ers
h
ai
tp
fa
1332 BENKWITZ AND HAMMER
affected individuals. This should be kept in mind whencaring for these patients. Thrombocytopenia, some-times clearly attributable to autoimmune dysregulationand frequently associated with platelet dysfunction, is acommon, usually late-occurring, finding in these pa-tients and may present with significant bleeding epi-sodes.18-21 Likewise, although less frequently, liver dis-ease, to a varying extent, including noncirrhotic portalhypertension, can coexist, thereby further promotinghemorrhagic diathesis in these patients.19,22,23 Labora-tory data and prior episodes of pulmonary and abdom-inal hemorrhages in the present patient fit into thispicture.
2. The small diameter of the ETT (ie, a 4.0-mm internaldiameter) necessitated by the patient’s subglottic ste-nosis may have facilitated complete occlusion by ablood clot.
3. The authors cannot prove that rFVIIa was the solecausative agent for the repeated thrombotic occlusionof the ETT. However, the fact that ETT occlusionoccurred about 20 minutes after the administration ofrFVIIa in association with hemostasis in the surgicalfield is highly suggestive that this complication wasrelated to rFVIIa. This agrees with the time course ofmaximum thrombin generation in in vitro studies ofTF-initiated blood coagulation.24
4. The activation of rFVIIa and the subsequent initiationof the coagulation cascade should, in theory, be local-ized to the site of the endovascular injury. This iswhere TF-expressing cells are exposed to the blood-stream, allowing the complex formation of TF withVII. How can this be reconciled with the ongoing bloodclot formation in the ETT in the present cardiac case?
Inflammatory states, which include CPB proceduresREN
tric cardiac surgery. Ann Thorac Surg 84:161-168, 2007
rp2
oi
V2
idsftvn
c7
Uen
(ie, 1 tumor necrosis factor �), induce TF expressionon the surface of cell types that normally do not expressTF, including endothelial cells and monocytes. In vitrostudies have shown that the timeframe for the inductionof TF expression on the surface of monocytes but notlymphocytes in the setting of simulated extracorporealcirculation can be as short as 2 hours.25 FVIIa also caninitiate the coagulation process even in the absence ofTF by generating FXa and FIXa on the surface ofactivated platelets. This TF-independent activity ofrFVIIa increases with decreasing temperatures. Fi-nally, in addition to the constitutive expression of TFin smooth vascular cells and fibroblasts, surroundingvessels, the heart, and the lung also possess largeamounts of TF procoagulant activity. Injury in thesetissues may be particularly potent in the generationof thrombus.24,26
In summary, with currently very limited and partially contra-dictory data available, the debate on the safety and efficacy ofrFVIIa administration in pediatric heart surgery is ongoing. Inview of the risk of life-threatening thrombotic complications,further research consisting of randomized, controlled trials isnecessary to establish the role of rFVIIa in the treatment ofpost–cardiac surgery coagulopathy in infants and children.
The authors concluded that life-threatening thrombotic oc-clusion of the ETT, heralded by a sudden and rapid increase inairway pressure and a concomitant decrease in SpO2, representsa major complication associated with the administration ofrFVIIa. The use of ETTs with built-in suction ports, routinelyused in intensive care units, should be used with caution in theoperating room setting. These devices may use small cathetersand may preclude the passage of larger catheters for tracheal
suctioning.REFE
1. Hedner U, Lee CA: First 20 years with recombinant FVIIaNovoSeven). Haemophilia 17:e172-e182, 2011
2. Eaton MP, Iannoli EM: Coagulation considerations for infantsnd children undergoing cardiopulmonary bypass. Paediatr Anaesth1:31-42, 20113. Despotis G, Avidan M, Lublin DM: Off-label use of recombinant
actor VIIa concentrates after cardiac surgery. Ann Thorac Surg 80:3-5,0054. Hammer GB, Williams GD: Use of recombinant activated factor
II in children. Paediatr Anaesth 17:1123-1125, 20075. Diringer MN, Skolnick BE, Mayer SA, et al: Thromboembolic
vents with recombinant activated factor VII in spontaneous intrace-ebral hemorrhage: Results from the factor seven for acute hemorrhagictroke (FAST) trial. Stroke 41:48-53, 2010
6. Patanwala AE: Factor VIIa (recombinant) for acute traumaticemorrhage. Am J Health Syst Pharm 65:1616-1623, 20087. Yank V, Tuohy CV, Logan AC, et al: Systematic review: Benefits
nd harms of in-hospital use of recombinant factor VIIa for off-labelndications. Ann Intern Med 154:529-540, 2011
8. Lin Y, Stanworth S, Birchall J, et al: Recombinant factor VIIa forhe prevention and treatment of bleeding in patients without haemo-hilia. Cochrane Database Syst Rev 2:CD005011, 20119. Agarwal HS, Bennett JE, Churchwell KB, et al: Recombinant
actor seven therapy for postoperative bleeding in neonatal and pedi-
CES
10. Avci Z, Malbora B, Gokdemir M, et al: Successful use ofecombinant factor VIIa (NovoSeven) during cardiac surgery in aediatric patient with congenital factor XI deficiency. Pediatr Cardiol9:220-222, 200811. Karsies TJ, Nicol KK, Galantowicz ME, et al: Thrombotic risk
f recombinant factor seven in pediatric cardiac surgery: A singlenstitution experience. Ann Thorac Surg 89:570-576, 2010
12. Kylasam S, Mos K, Fijtin S, et al: Recombinant activated factorII following pediatric cardiac surgery. J Int Care Med 24:116-121,00913. Ekert H, Brizard C, Eyers R, et al: Elective administration in
nfants of low-dose recombinant activated factor VII (rFVIIa) in car-iopulmonary bypass surgery for congenital heart disease does nothorten time to chest closure or reduce blood loss and need for trans-usions: A randomized, double-blind, parallel group, placebo-con-rolled study of rFVIIa and standard haemostatic replacement therapyersus standard haemostatic replacement therapy. Blood Coagul Fibri-olysis 17:389-395, 200614. Mathew P: The use of rFVIIa in non-haemophilia bleeding
onditions in paediatrics. A systematic review. Thromb Haemost 92:38-746, 200415. Pychynska-Pokorska M, Pagowska-Klimek I, Krajewski W, et al:
se of recombinant activated factor VII for controlling refractory postop-rative bleeding in children undergoing cardiac surgery with cardiopulmo-
ary bypass. J Cardiothorac Vasc Anesth 25:987-994, 2011
1333THROMBOTIC ENDOTRACHEAL TUBE OCCLUSION
16. Veldman A, Neuhaeuser C, Akintuerk H, et al: RFVIIa in thetreatment of persistent hemorrhage in pediatric patients on ECMOfollowing surgery for congenital heart disease. Paediatr Anaesth 17:1176-1181, 2007
17. Tobias JD, Simsic JM, Weinstein S, et al: Recombinant factor VIIato control excessive bleeding following surgery for congenital heart dis-ease in pediatric patients. J Intensive Care Med 19:270-273, 2004
18. Lawrence S, McDonald-McGinn DM, Zackai E, et al: Throm-bocytopenia in patients with chromosome 22q11.2 deletion syndrome.J Pediatr 143:277-278, 2003
19. Pinchas-Hamiel O, Mandel M, Engelberg S, et al: Immunehemolytic anemia, thrombocytopenia and liver disease in a patient withDiGeorge syndrome. Isr J Med Sci 30:530-532, 1994
20. Akar NA, Adekile AD: Chromosome 22q11.2 deletion present-ing with immune-mediated cytopenias, macrothrombocytopenia and
platelet dysfunction. Med Princ Pract 16:318-320, 200721. Hernández-Nieto L, Yamazaki-Nakashimada MA, Lieberman-Hernández E, et al: Autoimmune thrombocytopenic purpura in partialDiGeorge syndrome: Case presentation. J Pediatr Hematol Oncol 33:465-466, 2011
22. Seaver LH, Brumblay JM, Wilson CM: Noncirrhotic portalhypertension in a child with velocardiofacial syndrome. Am J MedGenet A 143A:2623-2624, 2007
23. Washington K, Gossage DL, Gottfried MR: Pathology of theliver in severe combined immunodeficiency and DiGeorge syndrome.Pediatr Pathol 13:485-504, 1993
24. Butenas S, Brummel KE, Branda RF, et al: Mechanism of factorVIIa-dependent coagulation in hemophilia blood. Blood 99:923-930, 2002
25. Kappelmayer J, Bernabei A, Edmunds LH Jr, et al: Tissue factoris expressed on monocytes during simulated extracorporeal circulation.Circ Res 72:1075-1081, 1993
26. Mackman N: The role of tissue factor and factor VIIa in hemo-
stasis. Anesth Analg 108:1447-1452, 2009