Embed Size (px)
Citation preview

NOACs – Update 2016
PD Dr. Jan Steffel
Leitender Arzt, Klinik für KardiologieCo-Leiter Rhythmologie
Universitätsspital Zürich

Conflict of Interest Statement
o Consulting: Amgen, Astra Zeneca, AtriCure, Bayer, Biosense Webster,
Biotronik, BMS, Boehringer Ingelheim, Boston Scientific, Daiichi-Sankyo,
Medtronic, Pfizer, Sanofi-Aventis, SJM
o Speaker honoraria: Astra Zeneca, Bayer, Biosense Webster, Biotronik, BMS,
Boehringer Ingelheim, Daiichi-Sankyo, Medtronic, Novartis, Pfizer, Roche,
Sanofi-Aventis, SJM, Sorin, Zoll
o Grants (through institution): Bayer, Biotronik, Boston Scientific, Daiichi-
Sankyo, Medtronic, St. Jude Medical
o Co-president CorXL
o Collaboration with TIMI study group (ENGAGE AF-TIMI 48)

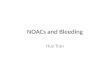
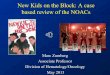
Relative Hazard Ratio (95% CI)
Favors NOAC Favors warfarin0.4 0.6 1.00.2 0.8 1.4 1.61.2 1.8
RE-LY: 110 mg BIDRE-LY: 150 mg BID
Dabigatran
ROCKET-AF: 20 mg QD
Rivaroxaban (safety AT)
ARISTOTLE: 5 mg BID
Apixaban
ENGAGE-AF: 30 mg QDENGAGE-AF: 60 mg QD
Edoxaban
P=0.13
P=0.051
P=0.073
P=0.047
P=0.006P=0.08
0.91
0.88
0.85
0.89
0.87
0.92
1. Connolly et al. N Engl J Med 2009;361:1139–1151; 2. Patel et al. N Engl J Med 2011;365:883–8913. Granger et al. N Engl J Med 2011;365:981–992; 4. Giugliano et al. N Engl J Med 2013; e-pub ahead of print
Phase III AF trials: All-cause mortality
For illustrative purpose only! No head-to-head comparisons!

‘Real Life’ Data aims to complement
Clinical Trial Data
Clinical trial RLE study
• Patients are selected by stringent
protocol criteria
• Treatment / observation is defined
in the protocol
• Methodology aims for reducing
bias when a randomized design is
used
• Patients are selected by the
treating physician
• Over- and under-reporting
of events possible
• Observation of real-life subgroups
possible

FDA Study on Medicare Patients
FDA, Mai 2014 - http://www.fda.gov/drugs/drugsafety/ucm396470.htm

XANTUS: Study Objective and Design
• Objective: Prospective Real world study on the safety profile of rivaroxaban
in patients wit nvAF
Final visit:
1 year#
Data collection at initial visit, hospital
discharge (if applicable) and quarterly*Population: Consecutively enrolled adult patients with NVAF receiving rivaroxaban for stroke/non-CNS SE prevention
Rivaroxaban: treatment
duration and dose at
physician’s discretion
Prospective, single-arm, observational, non-interventional phase IV study
Statistical analyses were descriptive and exploratory in nature
1 year
N=6,784
1. Camm AJ, et al, Vasc Health Risk Manag 2014.
2. Camm AJ, et al, Eur Heart J 2015.
* Exact referral dates for follow-up visits not defined (every 3 months recommended)
# For rivaroxaban discontinuation ≤1 year, observation period ends 30 days after last dose.
Observational design means no interference with clinical practice was allowed
• Primary outcomes: major bleeding (ISTH definition), all-cause mortality,
any other adverse events
• Secondary outcomes: symptomatic thromboembolic events (stroke, SE, TIA)
and MI, non-major bleeding events (all adjudicated centrally by an independent committee
(CAC ) blinded to individual patient data)

L.CH.MKT.HC.04.2016.0867-DE
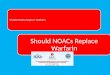
Rivaroxaban was associated with a
Significant 47% reduction in ICH vs. VKA
Comparable rate of ischemic stroke vs. VKA
Significant 39% reduction in the combined endpoint of ICH
and ischemic stroke vs. VKA
REVISIT-US - Significant Reduction in the
Combined Endpoint for Rivaroxaban vs. VKA
Rivaroxaban VKA HR (95% CI)
Rivaroxaban vs.
VKA
HR (95% CI)
Rivaroxaban vs. VKARate
(%/year)
Rate
(%/year)
ICH 0.49 0.96 0.53 (0.35–0.79)*
Ischemic stroke 0.54 0.83 0.71 (0.47–1.07)
Combined 0.95 1.6 0.61 (0.45–0.82)*
FavorsRivaroxaban
Favors VKA
0,125 0,25 0,5 1 2 4*p<0.05 vs. VKA
Coleman CI et al. Real-world EVIdence on Stroke prevention In patients with aTrial Fibrillation in the United States (REVISIT-US) [Presentation at
ECAS 2016] Available at: http://clinicaltrialresults.org/Slides/REVISIT_US_Slides.pptx

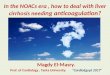
US retrospective real-world database research (MarketScan® commercial & Medicare supplemental database)
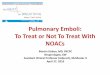
Unadjusted incidence rates of major bleeding (in-patient bleeding per 100 person-year) and adjusted HR1* for apixaban vs warfarin
4.66%
2.35%
0
1
2
3
4
5
Warfarin(n=12,713)
Apixaban(n=2,402)
Adjusted HR=0.52(95% CI: 0.30-0.89)
Un
adju
sted
maj
or
ble
edin
g in
cid
ence
(%
/ y
ear)
Adapted from Lip et al. 2015
*Cox-proportional hazards model was used to assess the risk of first major bleed across index OAC prescription categories, adjusted for age, gender, region, embolic or primary ischaemic stroke, dyspepsia or stomach discomfort, congestive heart failure, coronary artery disease, diabetes, hypertension, renal disease, myocardial infarction, history of stroke or transient ischaemic attack, history of bleeding, Charlsoncomorbidity index, and co-medications at baseline.
Of the 2,402 apixaban patients, 85.6% received apixaban 5 mg BD
Lip GYH et al. Real world comparison of major bleeding risk among non-valvular atrial fibrillation patients newly initiated on apixaban, dabigatran, rivaroxaban or warfarin. Poster presented at: ESC Congress; 29 August–2 September, 2015: London, UK. Poster P6217.
Data from retrospective real-world research, not a randomisedcontrolled trial

Net clinical benefit: CHADS-VASC vs. HAS-BLED
Banerjee et al., Thromb & Hemost 2012
• Event rates / 100 pys for ischemic stroke and intracranial
hemorrhage were calculated using data from the Danish
study population for patients on no treatment and on warfarin
• Using data from recent trials of the new OACs, the event
rates for ischemic stroke and intracranial hemorrhage were
estimated for the Danish population

Net clinical benefit: CHADS-VASC vs. HAS-BLED
Banerjee et al., Thromb & Hemost 2012

Net clinical benefit: CHADS-VASC vs. HAS-BLED
Banerjee et al., Thromb & Hemost 2012

Idarucizumab
Enriquez et al., Europace 2014

REVERSE-AD
Pollack et al., NEJM 2015

REVERSE-AD
Pollack et al., NEJM 2015

Andexanet Alfa
Reversal of anticoagulation by factor Xa inhibitors1
1. Lu G, et al. Nature Medicine 2013;19(4):446-51
Recombinant engineered version of human factor Xa
• Acts as a factor Xa decoy
• High affinity for all direct factor Xa inhibitors
• Changed in a way that catalytic activity is eliminated (serine alanine) and
prothrombin cleavage is prevented
• GLA domain removed to prevent anticoagulation effect
GLA
S419
S S
Factor Xa
GLA
A419
S S
Andexanet Alfa
Factor Xa Inhibitor
Catalytic Domain
Factor Xa Inhibitor

ANNEXA-A / ANNEXA-R
Siegal et al., NEJM 2015

PROTECT-AF long-term data
Reddy et al., JAMA 2014

PROTECT-AF long-term data
Reddy et al., JAMA 2014

PREVAIL over time
Waksman and Pendyala. AJC 2015

Summary and Take Home Message
NOACs are standard therapy for stroke
prevention in AF
Real World data very consistent
Net Clinical Benefit matters for patients!
Direct antagonists are available (idarucizumab)
or just around the corner (for Xa inhibitors)
LAA occluder: Good option for special patient
populations (esp contraindicated for
anticoagulation)

NOACs – Update 2016
PD Dr. Jan Steffel
Leitender Arzt, Klinik für KardiologieCo-Leiter Rhythmologie
Universitätsspital Zürich

LAAOs vs. NOACs
NOACs in real world vs. LAAO in real world (efficacy and safety)
Not all AF is created equal
o Valvular vs. non-valvular
o "Paroxysmal" vs. "Persistent" many shortcomings!
Careful in extrapolating "off-label" use of NOACs and LAAOs
o No data for patients with contraindication for anticoagulation
(PROTECT-AF vs. ASAP)
Careful in extrapolating (rather) small scale trials to the entire AF
population, and combining trial results

LAAOs vs. NOACs
NOACs in real world vs. LAAO in real world (efficacy and safety)
Not all AF is created equal
o Valvular vs. non-valvular
o "Paroxysmal" vs. "Persistent" many shortcomings!
Careful in extrapolating "off-label" use of NOACs and LAAOs
o No data for patients with contraindication for anticoagulation
(PROTECT-AF vs. ASAP)
Careful in extrapolating (rather) small scale trials to the entire AF
population, and combining trial results
Only a well-designed RCT will answer this question!
All strokes from LAA…?
How does LAAO compare with NOACs ?
o Beware of cross-trial comparisons…

ENGAGE-AF: "Increased Risk of Falls"
In ENGAGE-AF, investigators prospectively categorizedpatients as having an increased risk of falling particularly ifthey had any of the following 8 criteria at randomization:
• A prior history of falls
• Lower extremity weakness
• Poor balance
• Cognitive impairment
• Orthostatic hypotension
• Use of psychotropic drugs
• Severe arthritis
• Dizziness
Steffel et al., submitted (presented at AHA 2015)

Edoxaban versus Warfarin in Patients with an Increased Risk of Falls
Steffel et al., submitted (presented at AHA 2015)
Fall Risk (n = 900, 4%)
No Fall Risk (n = 20205, 96%)
p-value
Male gender 51% 62% <0.001Age (years) 77 72 <0.001CHADS2 score (mean) 3.3 2.8 <0.001CHA2DS2VASc score (mean) 5.1 4.3 <0.001CHADS2 score >3 39% 22% <0.001History of Stroke (incl. TIA) 41% 28% <0.001CrCl (ml/min, median) 58 71 <0.001TTR (warfarin arm, median) 67 69 0.15

2,7
9,1
7,1
4,7
0,9
4,7
1,8
5,1
3,9
2,7
0,5
1,7
0
2
4
6
8
10
12
Stroke/SEE All cause death/ Stroke / SEE
All-causedeath
Major bleed ICH Bone Fracturedue to Fall
At risk Not at risk
aHR 1.2
(0.9-1.5)
aHR 1.4
(1.2-1.7)aHR 1.5
(1.2-1.7)
aHR 1.3
(1.0-1.6)
aHR 1.4
(0.8-2.4)
aHR 1.9
(1.5-2.4)
***
***
***
*
Edoxaban versus Warfarin in Patients with an Increased Risk of Falls
Steffel et al., submitted (presented at AHA 2015)

2,8
9,3
7,1
5,4
2,8
10,0
7,8
5,6
1,5
4,83,9
1,8
5,44,2
0
2
4
6
8
10
12
Stroke/SEE All cause death/Stroke/SEE All-cause death Major bleed
HDE At risk
Warfarin At risk
HDE Not at risk
Warfarin Not at risk
Edoxaban versus Warfarin in Patients with an Increased Risk of Falls
Steffel et al., submitted (presented at AHA 2015)

Steffel et al., submitted (presented at AHA 2015)
Edoxaban versus Warfarin in Patients with an Increased Risk of Falls





















![lecture vka -7 [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/577d2ed01a28ab4e1eb01069/lecture-vka-7-compatibility-mode.jpg)