Embed Size (px)
Citation preview
Thrombophilia Failure of the Inherent Anticoagulation
Defense System
Mervyn A. Sahud, M.D., A.B.I.M.-Hem.Medical Director, Coagulation, Quest Diagnostics Nichols Institute
2
Outline• Thrombophilia (impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
3
• Thrombophilia (impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
Outline
4
Deep Vein Thrombosis — A Leg Up on Blood Clots
5
Valve Cusp Thrombus (Autopsy Specimen)
6
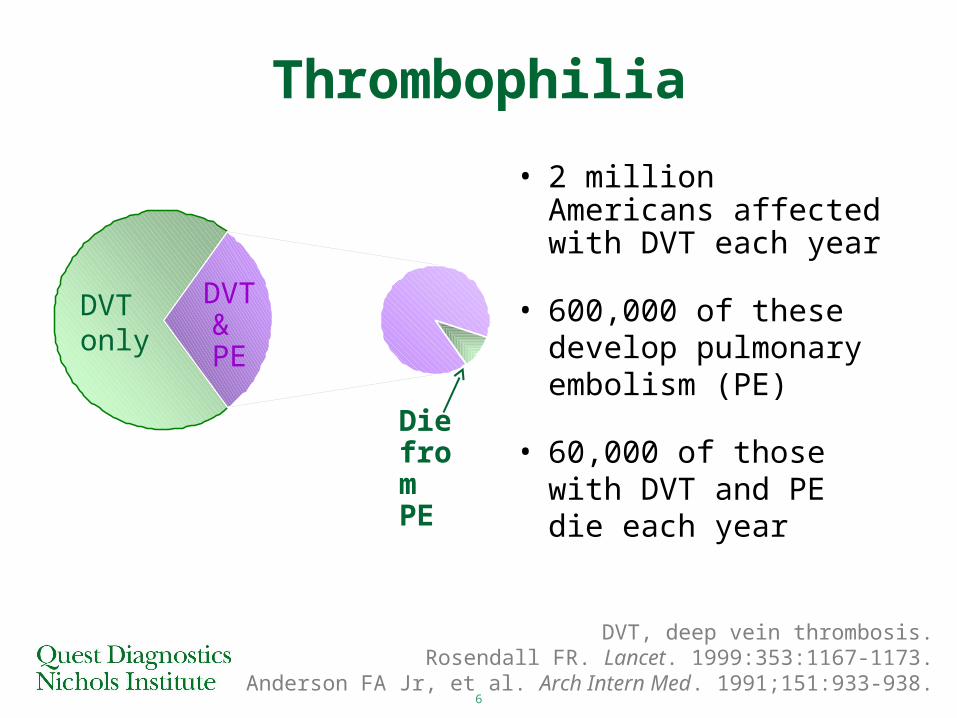
DVT only
DVT & PE
Die from PE
• 2 million Americans affected with DVT each year
• 600,000 of these develop pulmonary embolism (PE)
• 60,000 of those with DVT and PE die each year
Thrombophilia
DVT, deep vein thrombosis.Rosendall FR. Lancet. 1999:353:1167-1173.
Anderson FA Jr, et al. Arch Intern Med. 1991;151:933-938.
7
• 5% - 8% of population affected by genetic defects leading to thrombosis predisposition
• 25% suffer chronic swelling, skin ulceration, and impaired mobility secondary to “venous hypertension”
Thrombophilia
8
DVT…What’s New?• 50% (soon to be 100%) of “unprovoked” DVT
cases associated with hereditary thrombophilia
• 60% of DVT cases in pregnant women associated with factor V Leiden mutation (A1698G)
• DVT often associated with multiple genetic and acquired risk factors
• DVT responds to prolonged anticoagulant therapy (eg, low molecular weight heparin)
Bucciarelli P, et al. Arterioscler Thromb Vasc Biol. 1999;19:1026-1033.
9
DVT…What’s New?• New anticoagulants available for non-responsive
patients and those who experience side-effects from standard anticoagulants
• Family members request DVT screening prior to being placed in a “high-risk” situation
• Elevated D-dimer level often indicates thrombosis
• Normal D-dimer level has strong NPV
NPV, negative predictive value..
10
What Else is New?• Pulmonary embolism
– 4 million patients present to U.S. emergency departments with shortness of breath each year
– Shortness of breath = heart failure or pulmonary embolism (PE)
– 60% of patients who die in the hospital have PE
– PE diagnosis missed in 70% of hospital cases
– 10% of patients with acute PE die within first 60 minutes
Clagett GP. Chest. 1998;114(Suppl 5):531S-560S.
11
Thrombophilia Is Often Multigenic
Multiple risk factors raises the risk of thrombosis
12
• Thrombophilia (Impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
Outline
13
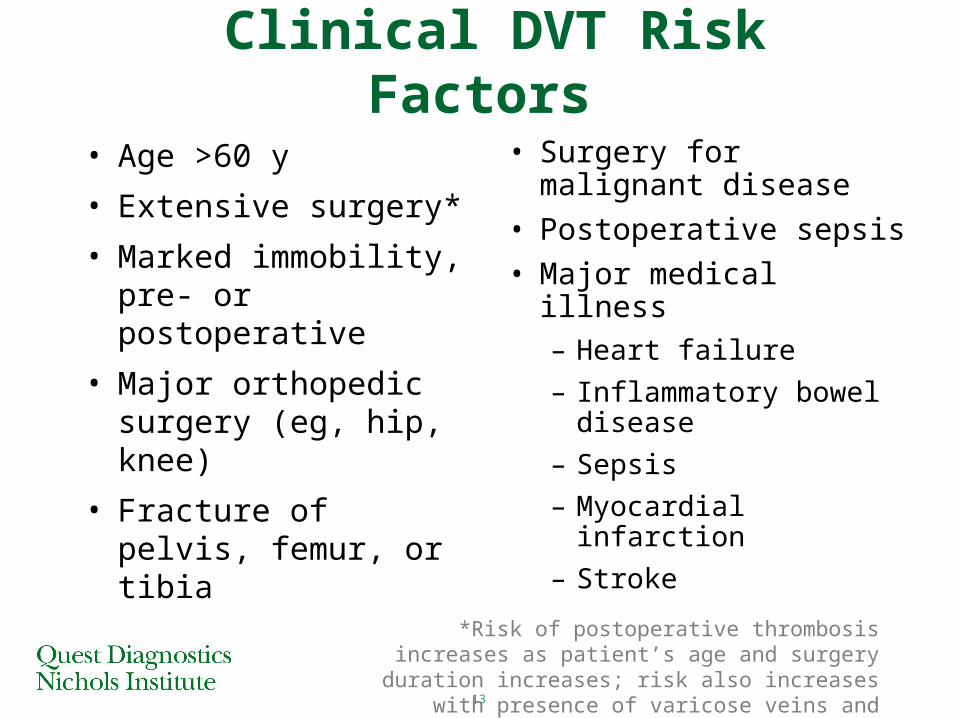
Clinical DVT Risk Factors
• Age >60 y
• Extensive surgery*
• Marked immobility, pre- or postoperative
• Major orthopedic surgery (eg, hip, knee)
• Fracture of pelvis, femur, or tibia
*Risk of postoperative thrombosis increases as patient’s age and surgery duration increases; risk also increases with presence of varicose veins and obesity.
• Surgery for malignant disease
• Postoperative sepsis
• Major medical illness– Heart failure
– Inflammatory bowel disease
– Sepsis
– Myocardial infarction
– Stroke
14
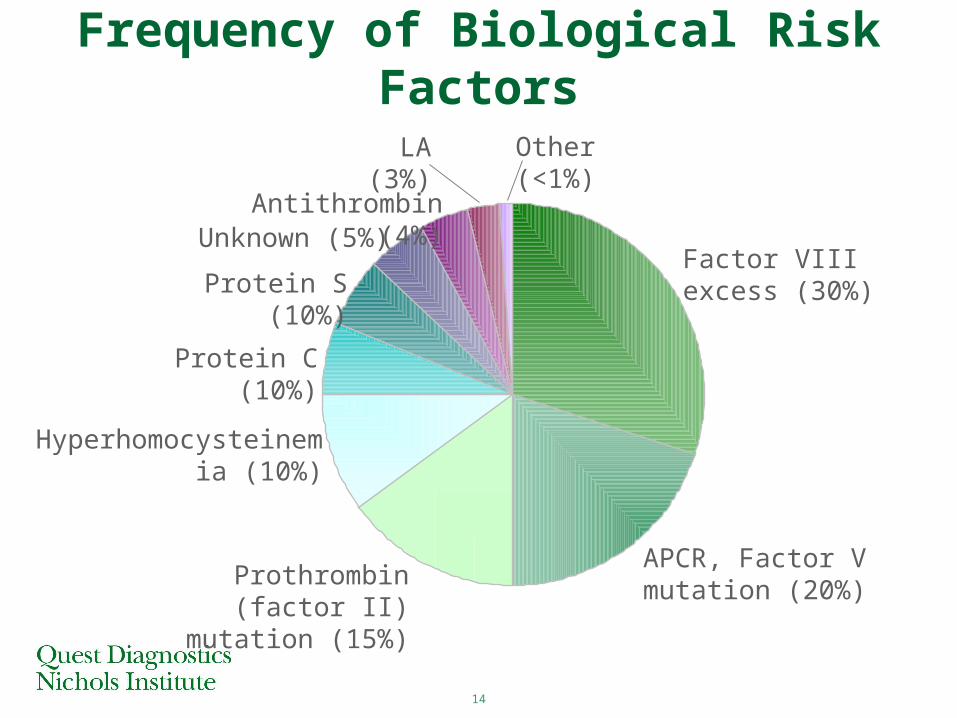
Frequency of Biological Risk Factors
Factor VIII excess (30%)
APCR, Factor V mutation (20%)
Prothrombin (factor II) mutation (15%)
Hyperhomocysteinemia (10%)
Protein C (10%)
Protein S (10%)
Unknown (5%)Antithrombin (4%)
LA (3%) Other (<1%)
15
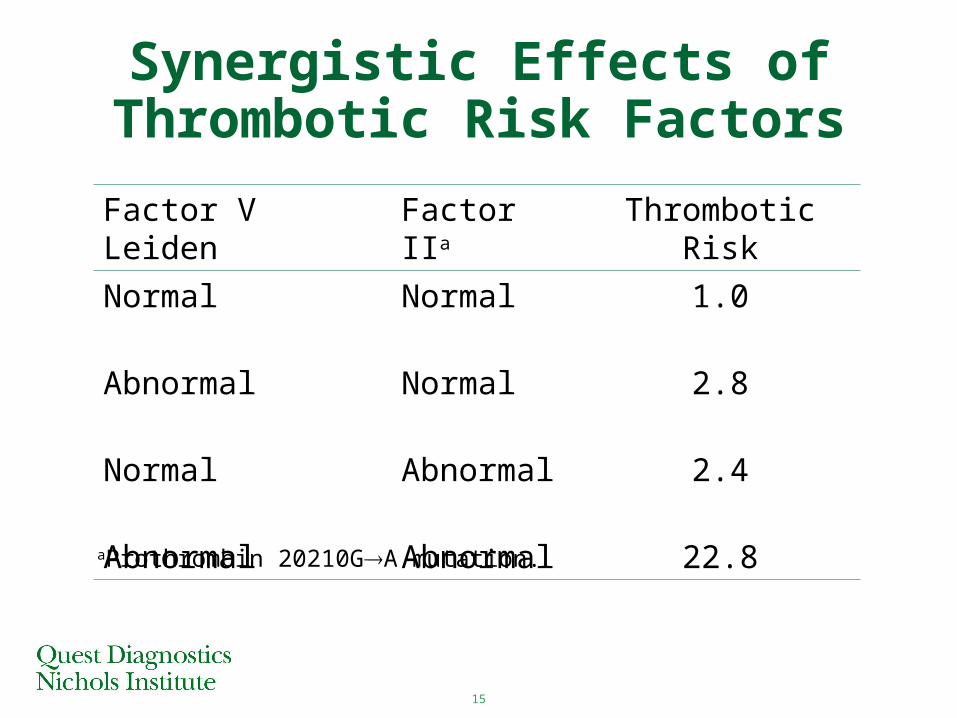
Synergistic Effects of Thrombotic Risk Factors
Factor V Leiden Factor IIa Thrombotic Risk
Normal Normal 1.0
Abnormal Normal 2.8
Normal Abnormal 2.4
Abnormal Abnormal 22.8aProthrombin 20210GA mutation.
16
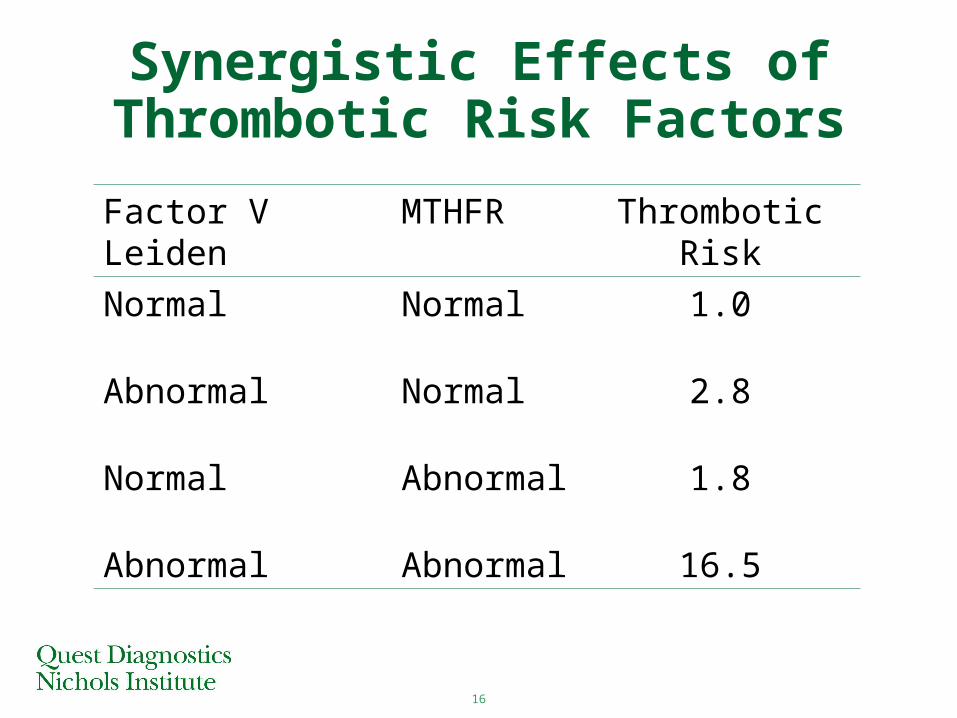
Synergistic Effects of Thrombotic Risk Factors
Factor V Leiden MTHFR Thrombotic Risk
Normal Normal 1.0
Abnormal Normal 2.8
Normal Abnormal 1.8
Abnormal Abnormal 16.5
17
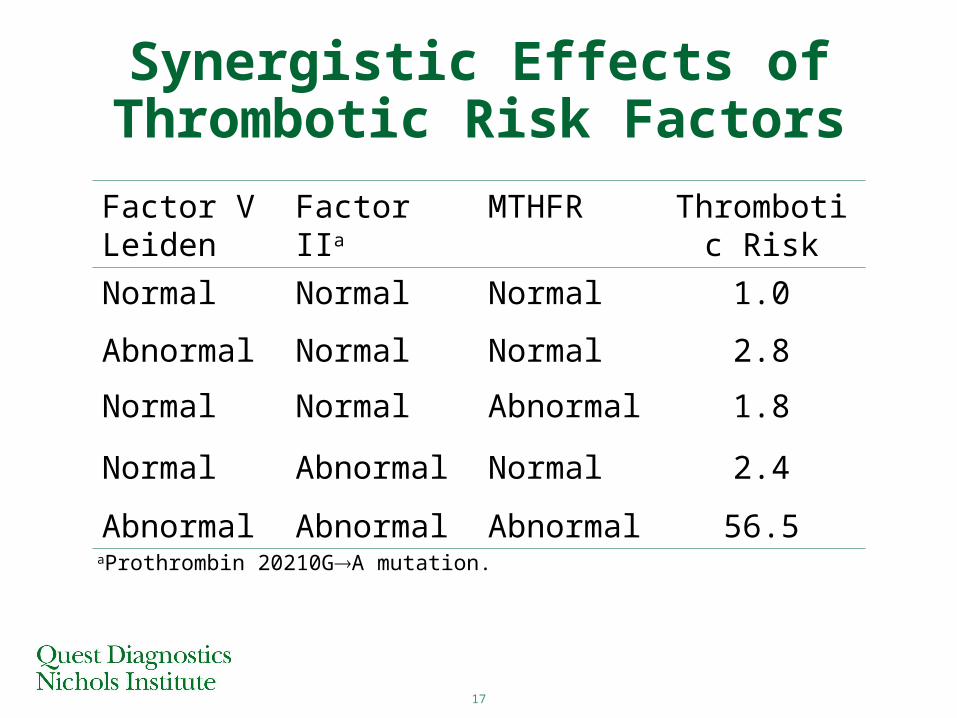
Synergistic Effects of Thrombotic Risk Factors
Factor V Leiden
Factor IIa MTHFR Thrombotic Risk
Normal Normal Normal 1.0
Abnormal Normal Normal 2.8
Normal Normal Abnormal 1.8
Normal Abnormal Normal 2.4
Abnormal Abnormal Abnormal 56.5aProthrombin 20210GA mutation.
18
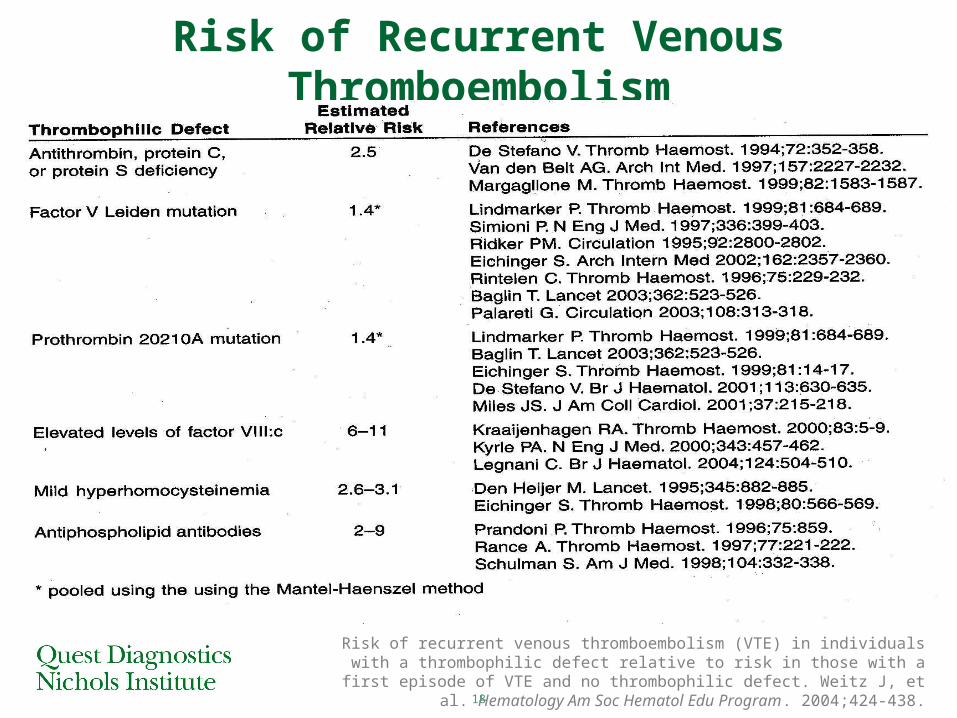
Risk of Recurrent Venous Thromboembolism
Risk of recurrent venous thromboembolism (VTE) in individuals with a thrombophilic defect relative to risk in those with a first episode of VTE and no thrombophilic defect.
Weitz J, et al. Hematology Am Soc Hematol Edu Program. 2004;424-438.
19
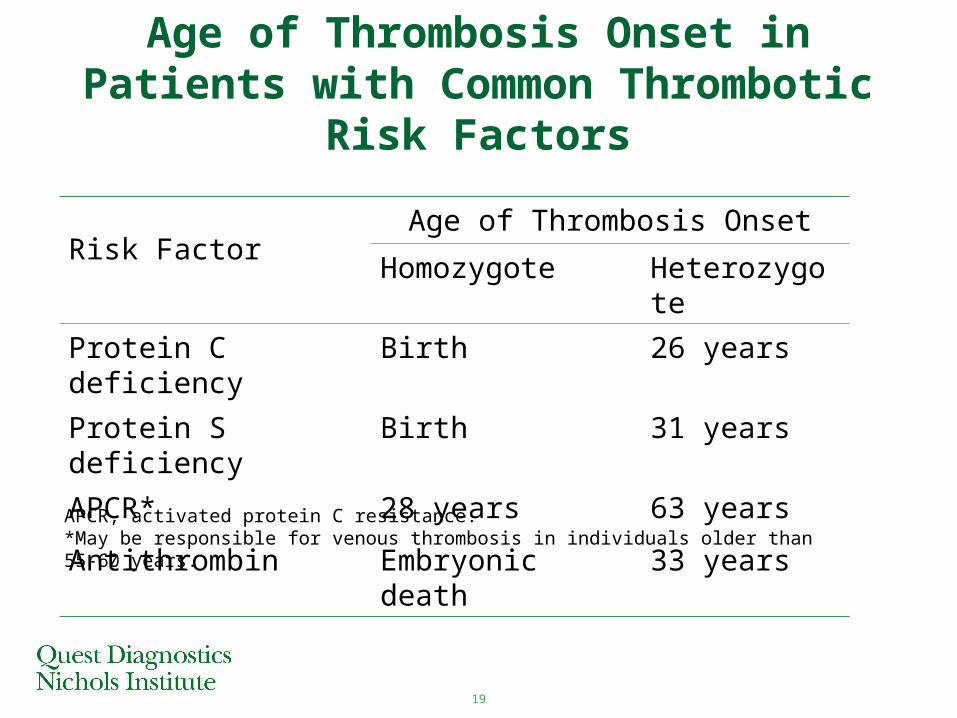
Age of Thrombosis Onset in Patients with Common Thrombotic Risk Factors
Risk FactorAge of Thrombosis Onset
Homozygote Heterozygote
Protein C deficiency Birth 26 years
Protein S deficiency Birth 31 years
APCR* 28 years 63 years
Antithrombin Embryonic death 33 yearsAPCR, activated protein C resistance.*May be responsible for venous thrombosis in individuals older than 55-60 years.
20
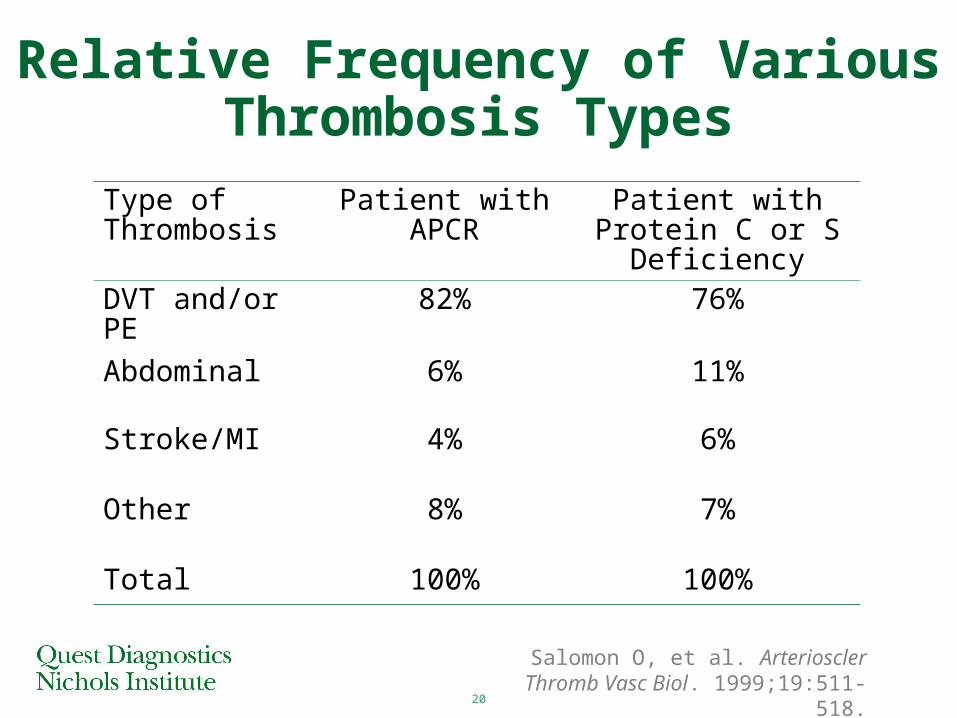
Relative Frequency of Various Thrombosis Types
Type of Thrombosis
Patient with APCR Patient with Protein C or S Deficiency
DVT and/or PE 82% 76%
Abdominal 6% 11%
Stroke/MI 4% 6%
Other 8% 7%
Total 100% 100%
Salomon O, et al. Arterioscler Thromb Vasc Biol. 1999;19:511-518.
21
• Thrombophilia (impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
Outline
22
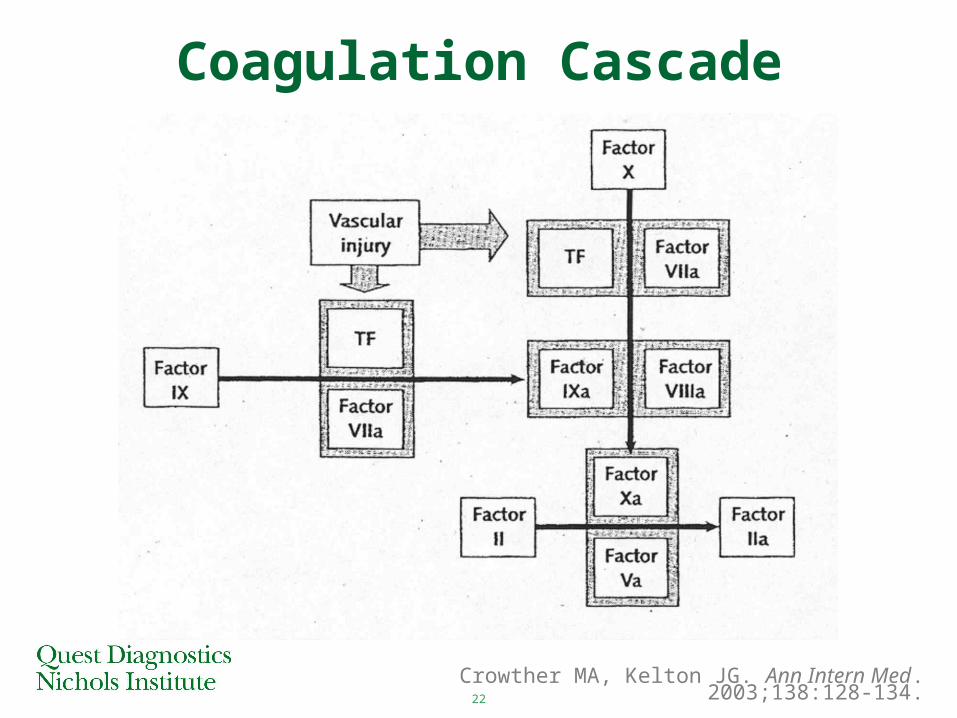
Coagulation Cascade
Crowther MA, Kelton JG. Ann Intern Med. 2003;138:128-134.
23
Coagulation Cascade
Factor VIIa binds to tissue factor (TF) at sites of vascular injury, causing a cascade that ultimately leads to factor IIa (thrombin) generation. Thrombin activates platelets; converts fibrinogen to fibrin; leads to generation of additional thrombin through an autocatalytic loop; converts factor XIII to factor XIIIa, which stabilizes the thrombus; inhibits fibrinolysis; and acts as an anticoagulant by activating protein C. The principal inhibitors of coagulation are activated protein C (which, in concert with protein S, inactivates factors Va and VIIIa), antithrombin (which forms an inactive covalent complex with thrombin and factors Xa, IXa, and XIa), and tissue factor pathway inhibitor (which bonds with and inactivates the tissue factor-factor VIIa complex).
Crowther MA, Kelton JG. Ann Intern Med. 2003;138:128-134.
24
• Thrombophilia (impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
Outline
25
How to test?
When to test? What to test?
Why test?
Whom to test?
Thrombophilia Testing
26
Antithrombin Deficiency
Genetic deficiency
• Rare
– <1% of general population
– ~1% - 8% of those with VTE
• Heterozygotes
– VTE by ~30 years of age
– 5- to 50-fold increased risk of VTE
– High risk of VTE during pregnancy and postpartum
27
Antithrombin Deficiency
Acquired deficiency• Causes
– Liver disease– Malnutrition – Inflammatory bowel disease – Prematurity– DIC– Transfusion reactions – Chemotherapy – Heparin therapy
28
AT
IIa
AT
Inactive Complexes
IIa
IIa
AT
Xa
AT
IXa
AT
XIa
AT
XIIa
AT
Heparin
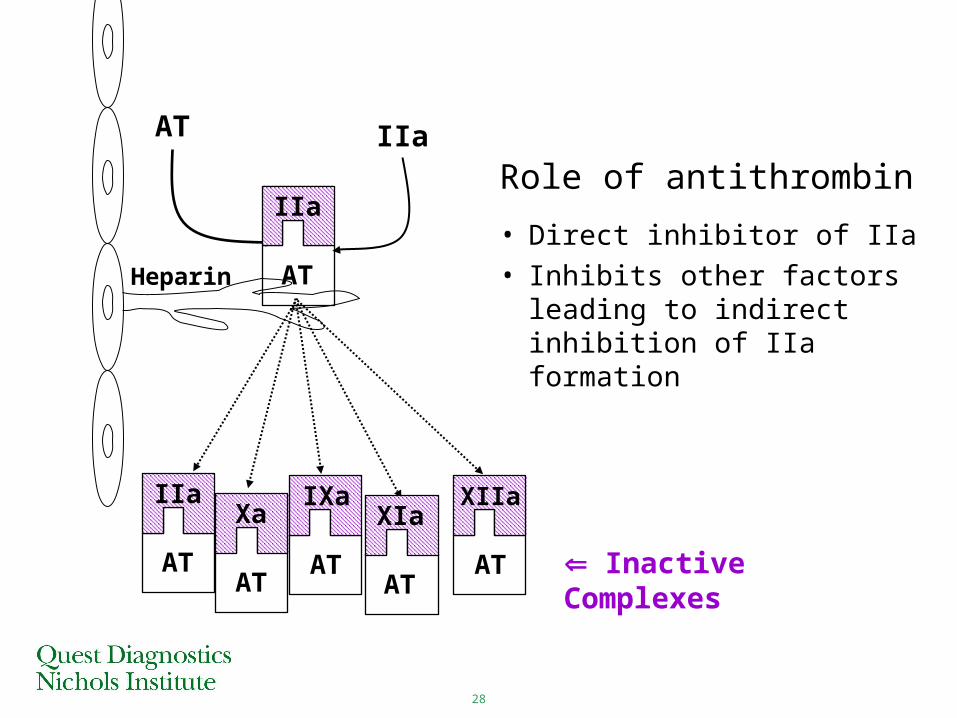
Role of antithrombin
• Direct inhibitor of IIa
• Inhibits other factors leading to indirect inhibition of IIa formation
29
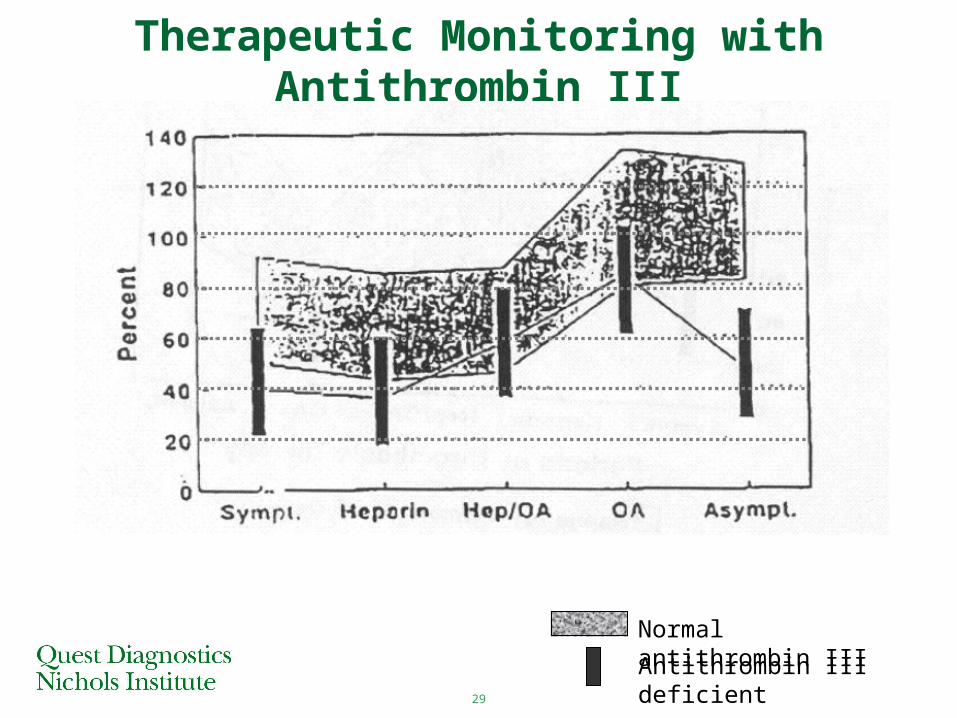
Therapeutic Monitoring with Antithrombin III
Normal antithrombin III
Antithrombin III deficient
30
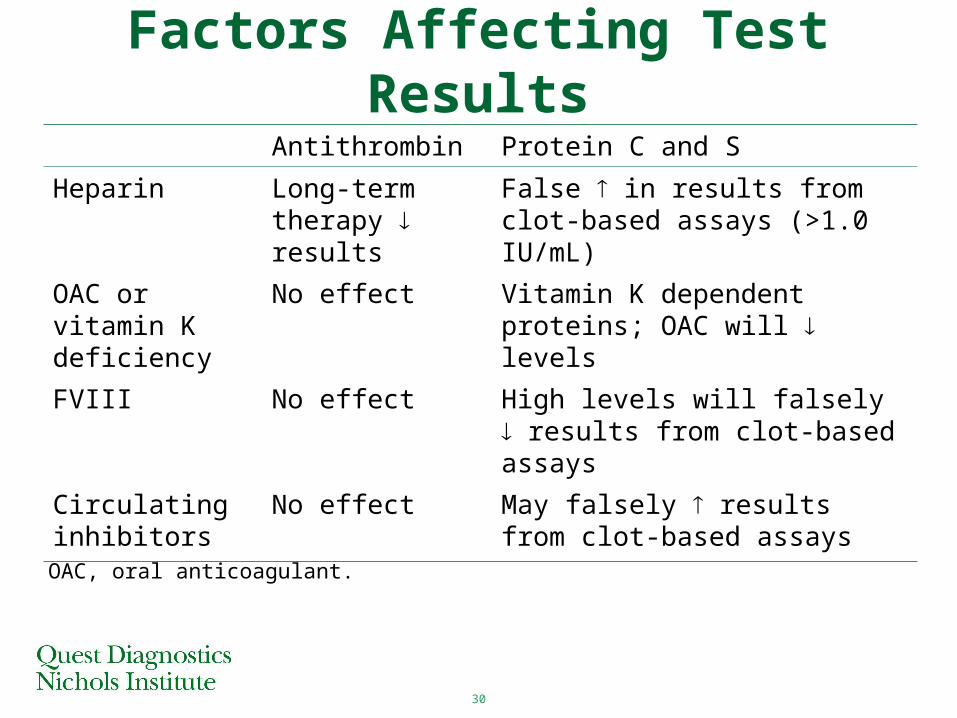
Factors Affecting Test Results
Antithrombin Protein C and S
Heparin Long-term therapy results
False in results from clot-based assays (>1.0 IU/mL)
OAC or vitamin K deficiency
No effect Vitamin K dependent proteins; OAC will levels
FVIII No effect High levels will falsely results from clot-based assays
Circulating inhibitors
No effect May falsely results from clot-based assays
OAC, oral anticoagulant.
31
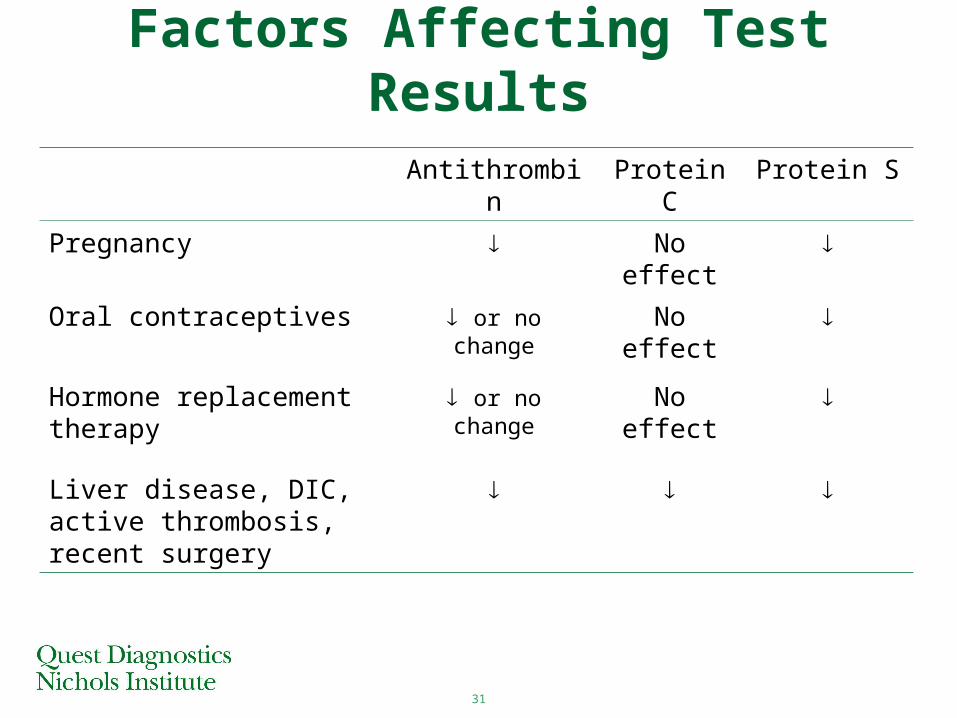
Factors Affecting Test Results
Antithrombin Protein C Protein S
Pregnancy No effect
Oral contraceptives or no change No effect
Hormone replacement therapy
or no change No effect
Liver disease, DIC, active thrombosis, recent surgery
32
Protein C Deficiency – Genetic Mechanism
Autosomal inheritance
• Complete penetrance (dominant mutation)– Heterozygotes– Primary symptom: venous thrombosis
• Mild or no penetrance (recessive mutation)– Homozygotes: symptomatic (purpura fulminans)– Heterozygotes: asymptomatic
33
Protein C Deficiency• Genetic deficiency
– Rare– Heterozygotes
• <1% of population
• ~1-11% of patients with VTE
• 30% will have an event during lifetime
• ~50% experience VTE by age 40
• Acquired deficiencies– Warfarin, vitamin K deficiency, liver disease,
DIC, renal insufficiency
34
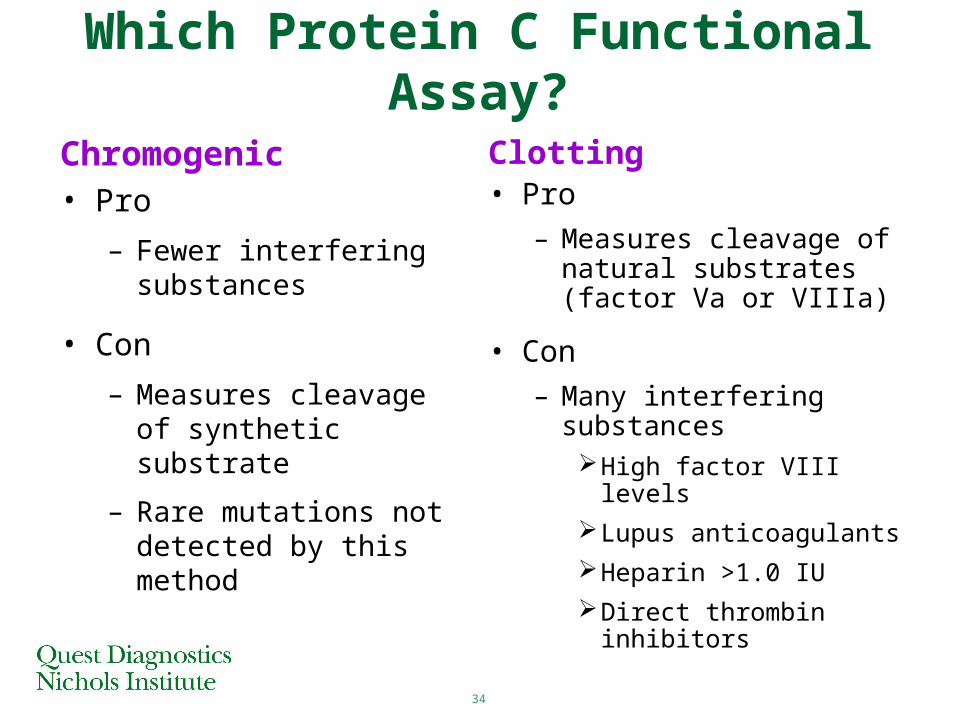
Which Protein C Functional Assay?
Chromogenic• Pro
– Fewer interfering substances
• Con
– Measures cleavage of synthetic substrate
– Rare mutations not detected by this method
Clotting
• Pro
– Measures cleavage of natural substrates (factor Va or VIIIa)
• Con
– Many interfering substancesHigh factor VIII levels
Lupus anticoagulants
Heparin >1.0 IU
Direct thrombin inhibitors
35
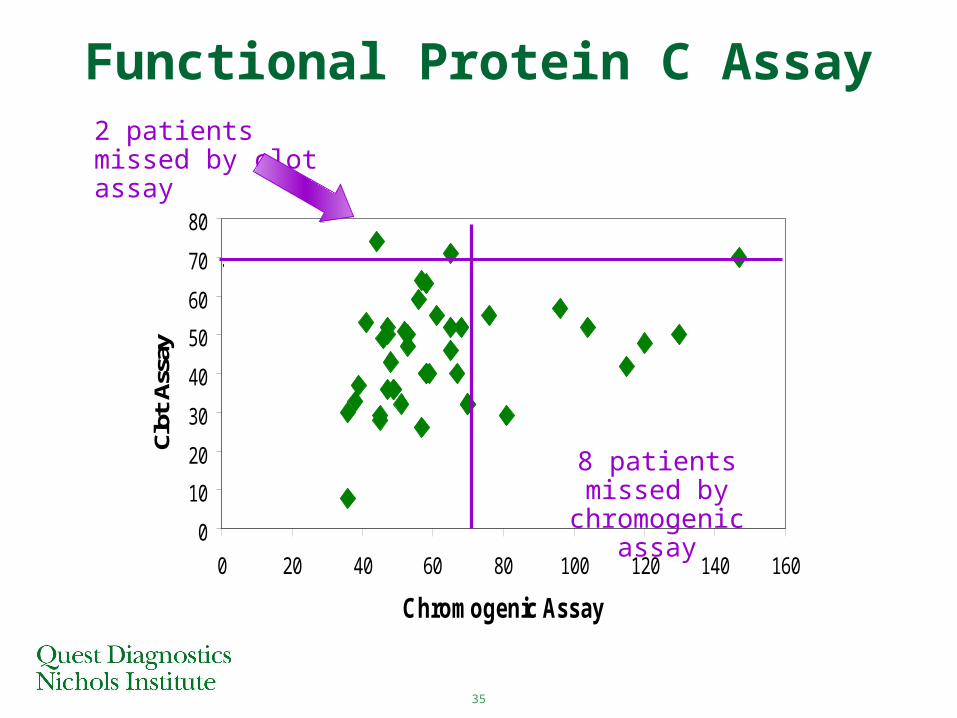
Functional Protein C Assay
0
10
20
30
40
50
60
70
80
0 20 40 60 80 100 120 140 160
Chromogenic Assay
Clot
Ass
ay2 patients missed by clot assay
8 patients missed by chromogenic assay
36Normal adult reference range: 70%
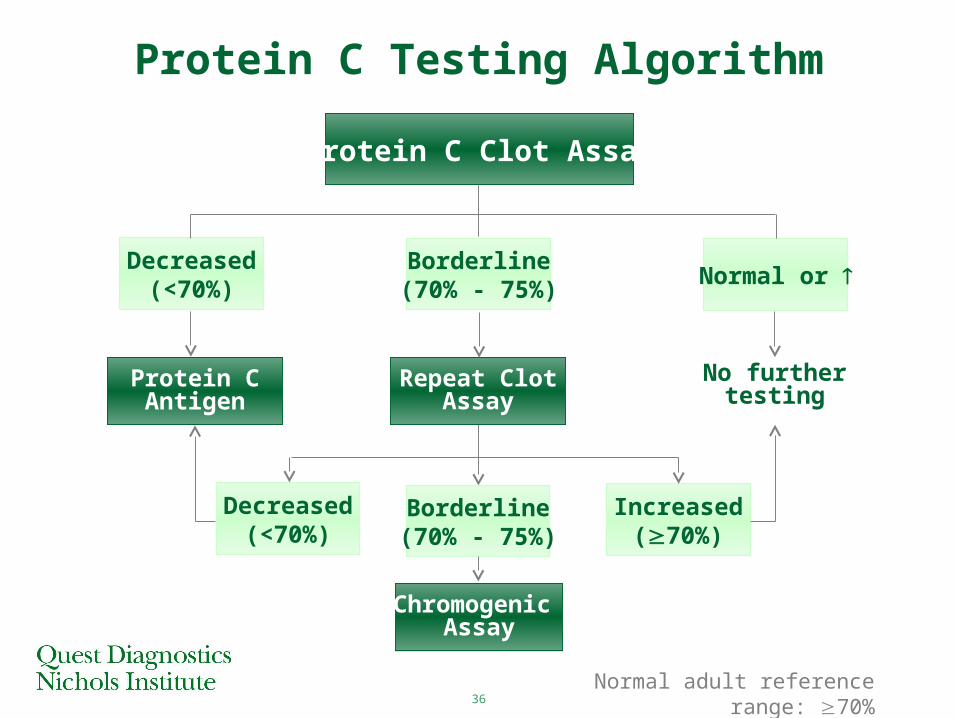
Protein C Testing Algorithm
No further testing
Protein C Clot Assay
Decreased(<70%)
Borderline(70% - 75%)
Normal or
Protein CAntigen
Repeat ClotAssay
Decreased(<70%)
Increased(70%)
Borderline(70% - 75%)
Chromogenic Assay
37
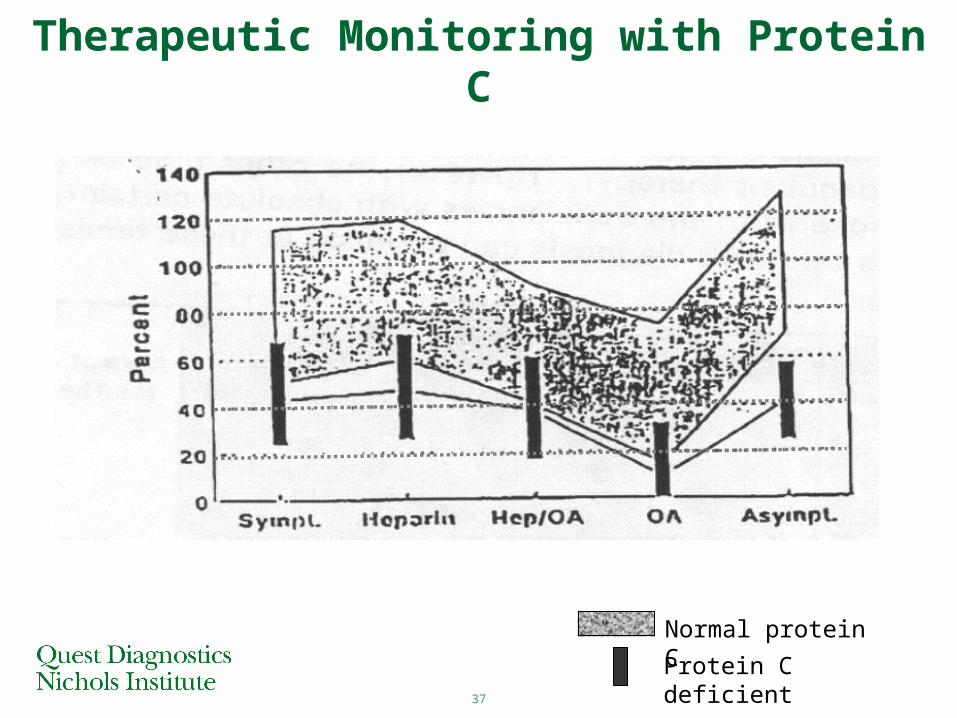
Therapeutic Monitoring with Protein C
Normal protein C
Protein C deficient
38
Protein S DeficiencyGenetic deficiency
• Homozygous (rare) – Purpura fulminans
• Heterozygous – < 1% of general population – ~1% to 3% of VTE population– ~50% experience first VTE by 45 years of age
Acquired deficiency• Pregnancy and oral contraceptive/HRT use• Inflammation and acute thrombosis
39
Protein CfPS
PS
TM
TM
TM
IIa
PC
APC
Va or VIIIa
VIIIai or Vai
Free PS
C4b-B
P
IIa
fPS
Inactive Cofactors
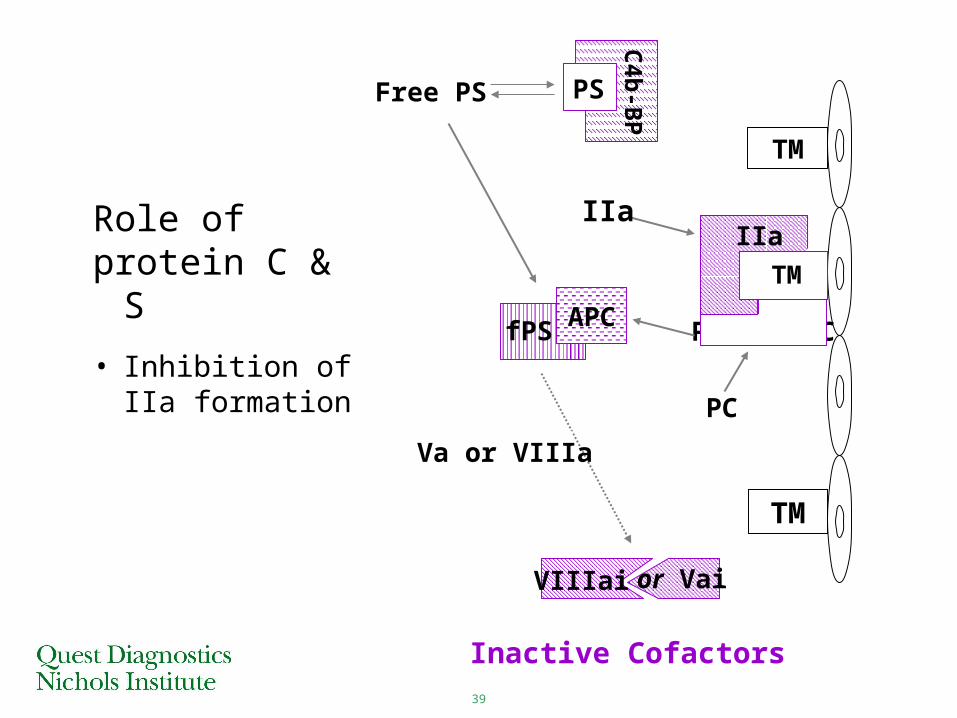
Role ofprotein C & S
• Inhibition of IIa formation
40
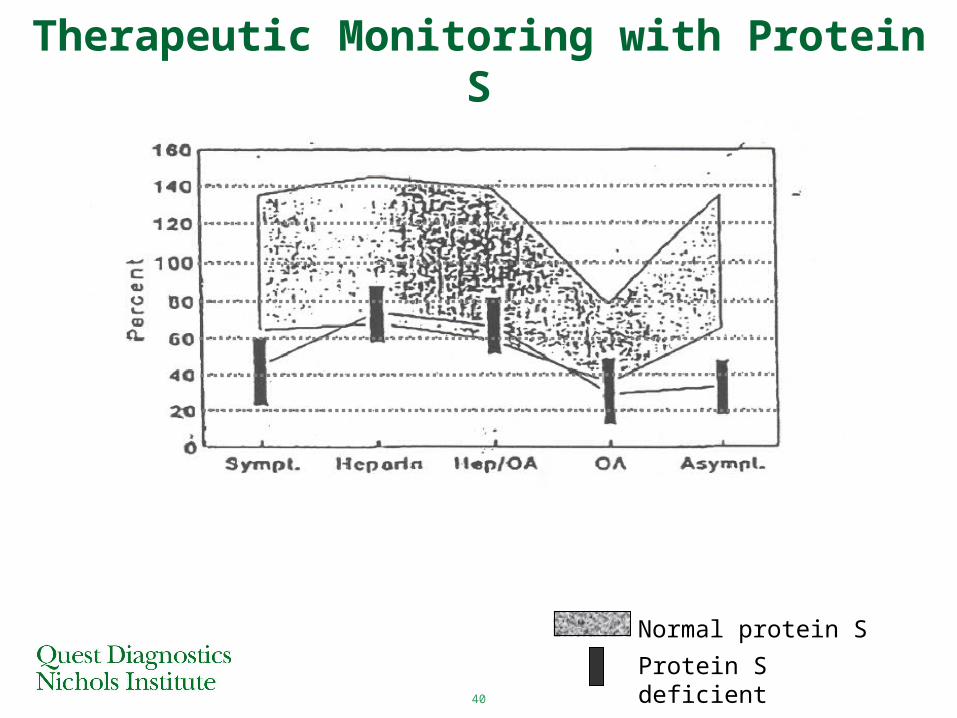
Therapeutic Monitoring with Protein S
Normal protein S
Protein S deficient
41
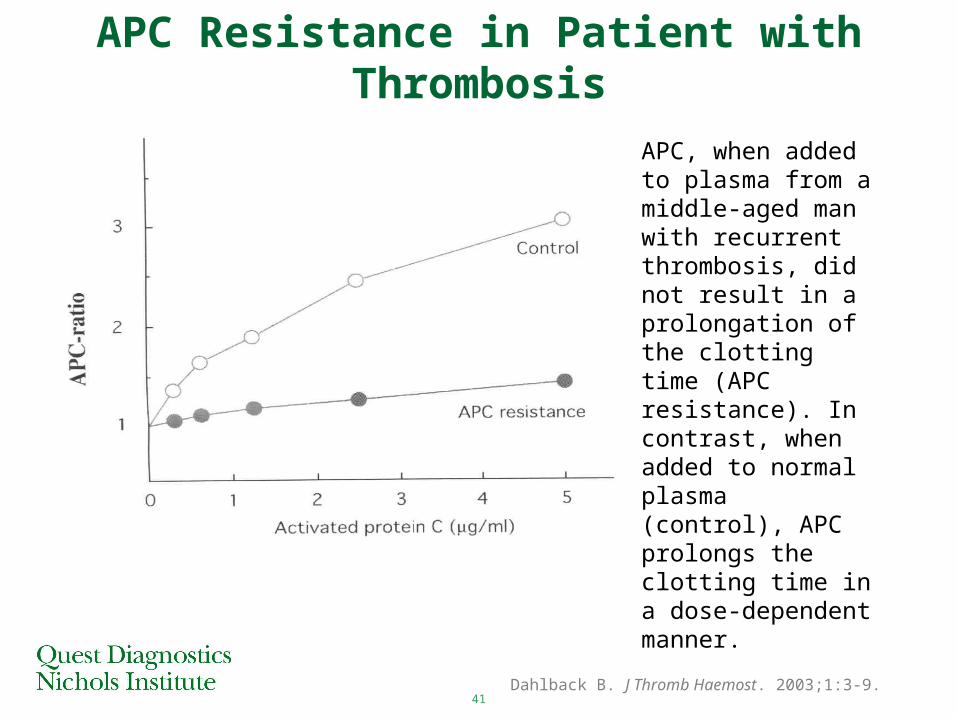
APC Resistance in Patient with Thrombosis
APC, when added to plasma from a middle-aged man with recurrent thrombosis, did not result in a prolongation of the clotting time (APC resistance). In contrast, when added to normal plasma (control), APC prolongs the clotting time in a dose-dependent manner.
Dahlback B. J Thromb Haemost. 2003;1:3-9.
42
APC Resistance – Genetic Mechanism
• Molecular cause Mutation of APC cleavage site within Factor Va
• Mutation site Amino acid #506 (arginine) mutates to a glutamine
Amino acid: Arg506→ GinNucleotide: CGA→ CAA
43
APC Resistance – Genetic Mechanism
• Molecular function– APC cleaves bond between arginine and
glycine
– If Arg506 residue is mutated
Bond not cleaved
Factor Va not inactivated by APC
Continued generation of thrombin and clot formation
Thrombosis
44
Acquired APC Resistance
Associated with:
• Increased plasma levels of FVIIIa
• Presence of antiphospholipid antibodies
• 3rd generation oral contraceptives, relative to 2nd generation oral contraceptives
• Pregnancy
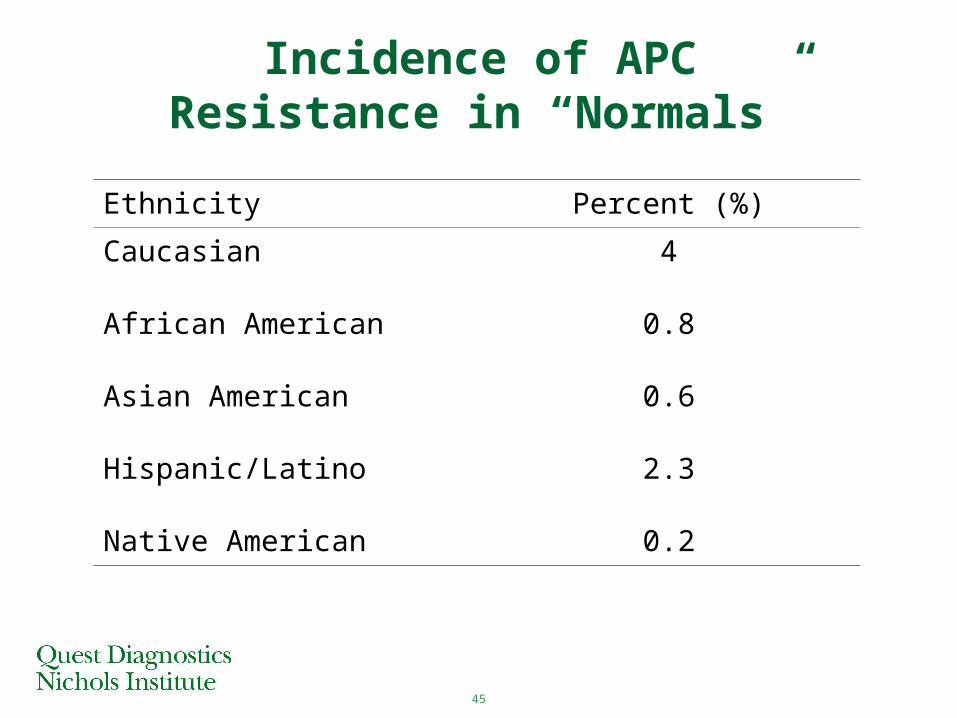
45
Incidence of APC Resistance in “Normals”
Ethnicity Percent (%)
Caucasian 4
African American 0.8
Asian American 0.6
Hispanic/Latino 2.3
Native American 0.2
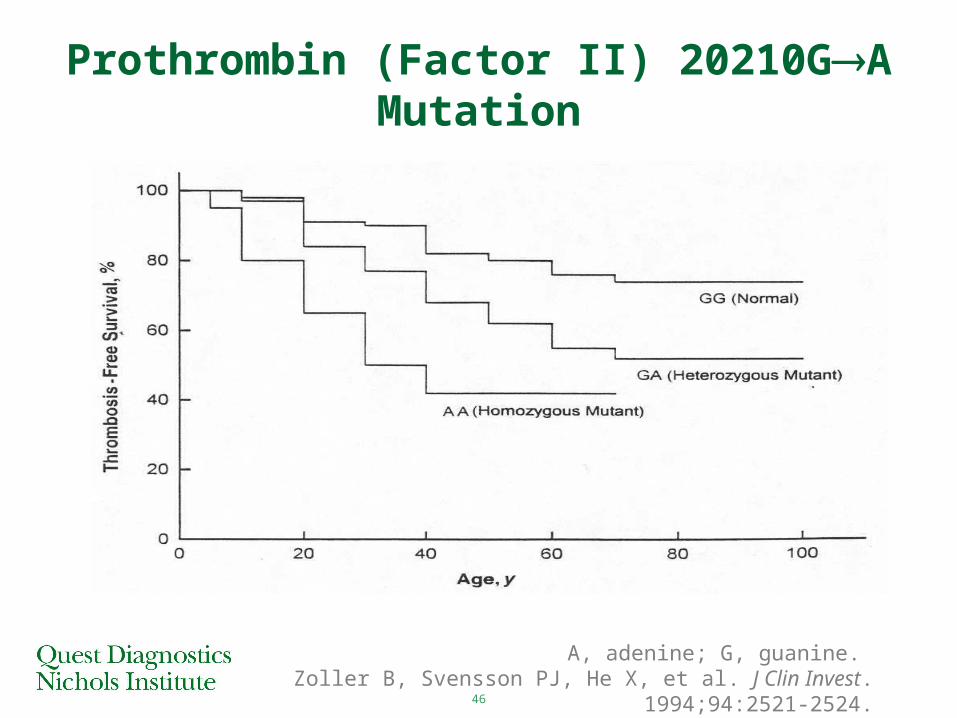
46
Prothrombin (Factor II) 20210GA Mutation
A, adenine; G, guanine. Zoller B, Svensson PJ, He X, et al. J Clin Invest. 1994;94:2521-2524.
47
Lupus Anticoagulant Screening
• Screening tests– LA sensitive aPTT reagent– Kaolin clotting time (KCT)– Dilute russell viper venom time (dRVVT)– Dilute prothrombin time (dPT)
• Minimum of 2 screening tests
48
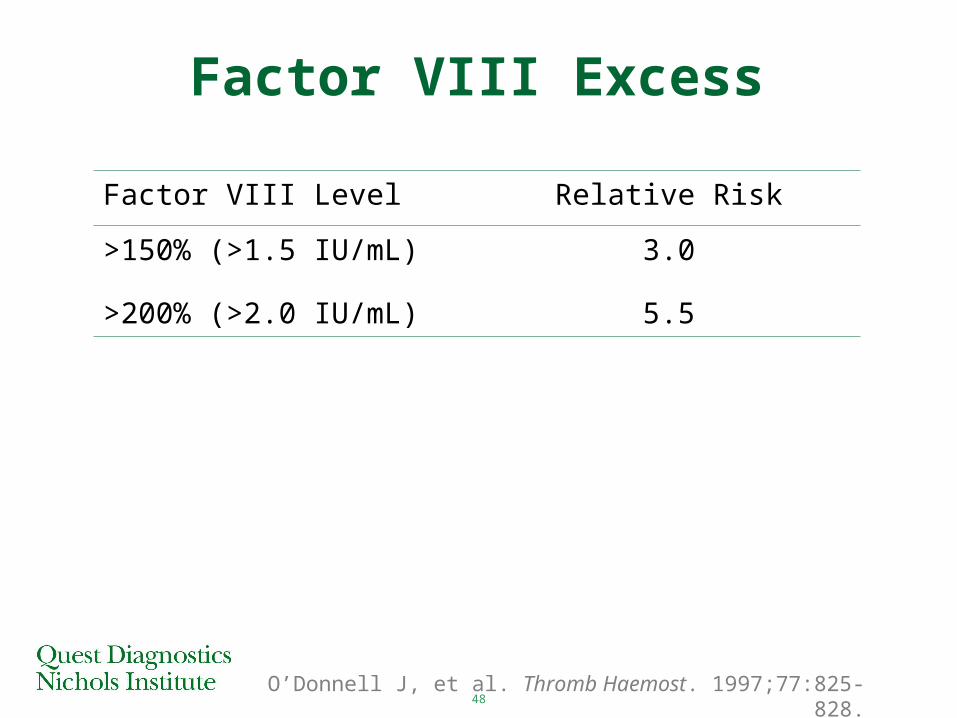
Factor VIII Excess
O’Donnell J, et al. Thromb Haemost. 1997;77:825-828.
Factor VIII Level Relative Risk
>150% (>1.5 IU/mL) 3.0
>200% (>2.0 IU/mL) 5.5
49
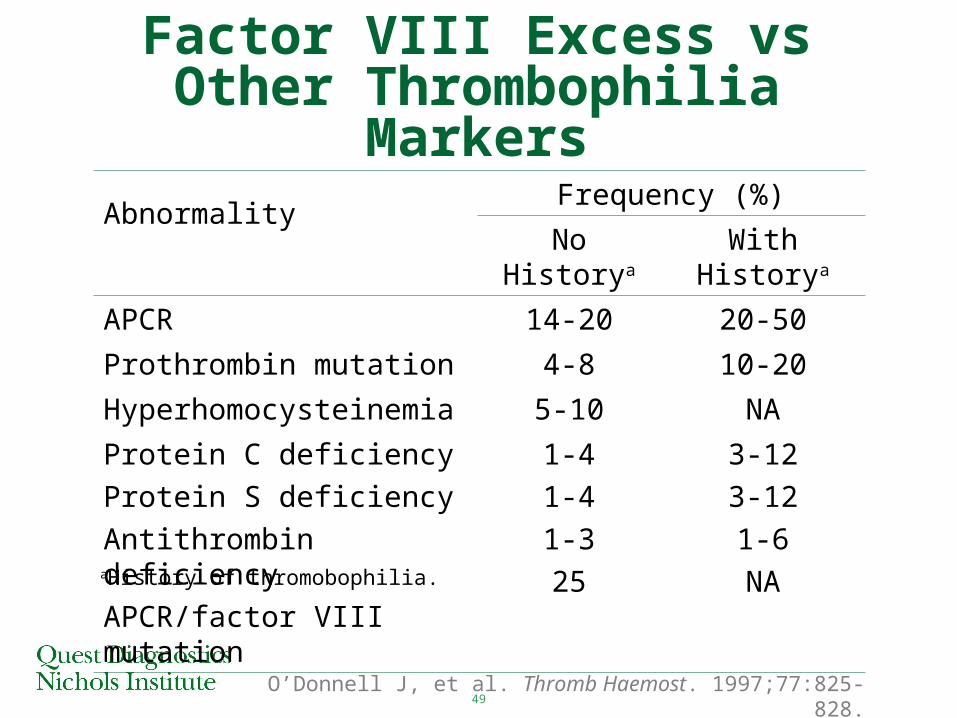
Factor VIII Excess vs Other Thrombophilia Markers
AbnormalityFrequency (%)
No Historya With Historya
APCR 14-20 20-50
Prothrombin mutation 4-8 10-20
Hyperhomocysteinemia 5-10 NA
Protein C deficiency
Protein S deficiency
Antithrombin deficiency
APCR/factor VIII mutation
1-4
1-4
1-3
25
3-12
3-12
1-6
NA
O’Donnell J, et al. Thromb Haemost. 1997;77:825-828.
aHistory of thromobophilia.
50
• Thrombophilia (impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
Outline
51
Case Study #1• 61 year-old white male with multiple myeloma
(in remission)
• Receiving no treatment
• Flies to Singapore for vacation
• Experiences discomfort in right leg, no swelling, no rubor
• 2 days later, sudden dyspnea, left pleuritic chest pain
• Hospitalized with DVT/PE
• Returns home 2 weeks later on coumadin
52
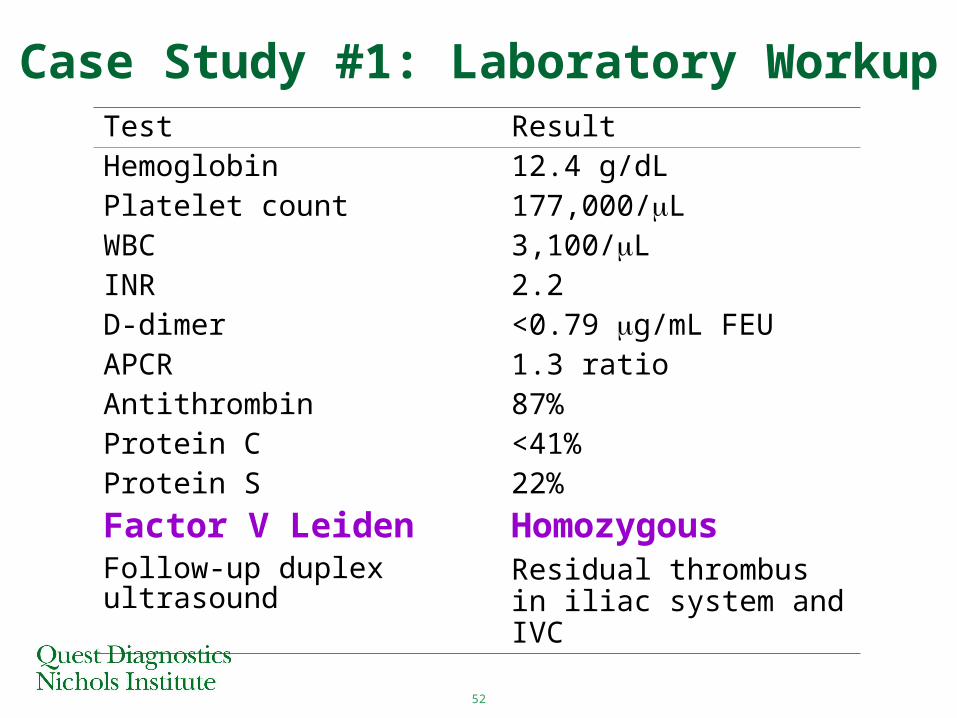
Case Study #1: Laboratory WorkupTest ResultHemoglobin 12.4 g/dLPlatelet count 177,000/LWBC 3,100/LINR 2.2D-dimer <0.79 g/mL FEUAPCR 1.3 ratioAntithrombin 87%Protein C <41%Protein S 22%
Factor V Leiden HomozygousFollow-up duplex ultrasound Residual thrombus in iliac
system and IVC
53
Case Study #2
• 37 y/o, G1P1 W/F attempting to get pregnant for the 2nd time
• 1st childbirth at age 21 y without incident
• Family history of protein S deficiency– Mother on long-term coumadin– Sister had DVT/PE while on birth control
• Lab results at 12 weeks– Protein S 47% (normal, 60-120%)– Protein C 141% (normal, 60-130%)– Antithrombin III 78% (normal, 60-120%)
54
Case Study #2 (cont’d)
• 2 weeks later, concern raised about need for prophylactic anticoagulant
• Lab results– C4 binding protein 212 mg/L (normal, 75-140)– Total protein S 81%– Free protein S 53%– Functional protein S43%
55
Case Study #2 (cont’d)
• Physician discusses drug therapy– Coumadin – Unfractionated heparin – Low molecular weight heparin– Arixtra (fondaparinux)
• Decision made to use graded elastic stockings and aspirin
• Lab results at 20 weeks– Protein S 33%– Protein C 162%
56
Case Study #2 (cont’d)
• Lab results at 36 weeks– Protein S 21%
• Enoxaparin initiated: 40 mg s.c. daily
• Delivery of baby uneventful
• Lab results 4 weeks postpartum– Protein S 31%
• Patient told she probably has hereditary protein S deficiency.
• Restarts enoxaparin for 4 weeks, daily 40 ng s.c.
57
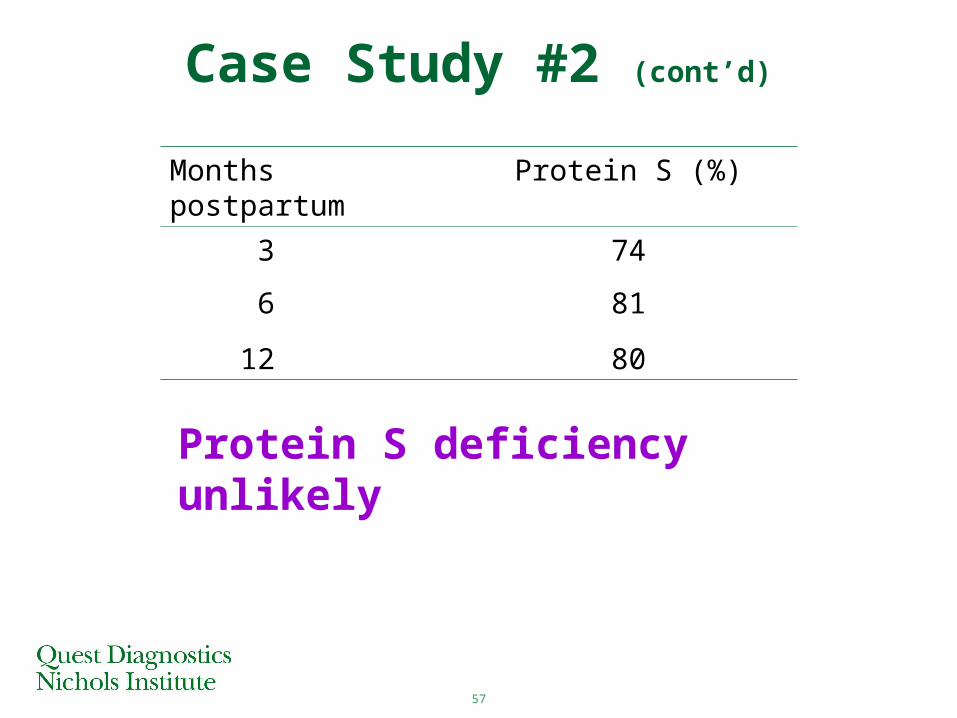
Case Study #2 (cont’d)
Months postpartum Protein S (%)
3 74
6 81
12 80
Protein S deficiency unlikely
58
Case Study #3• 39 year-old, physically active, white male bicyclist
develops rapidly progressive drawing pain in right calf after 40-mile event
• History of DVT in left lower extremity after laparoscopic knee surgery at age 21
• Mother on coumadin
• Father died mysteriously of unknown causes at age 51 years
• Sister has had recurrent miscarriages
59
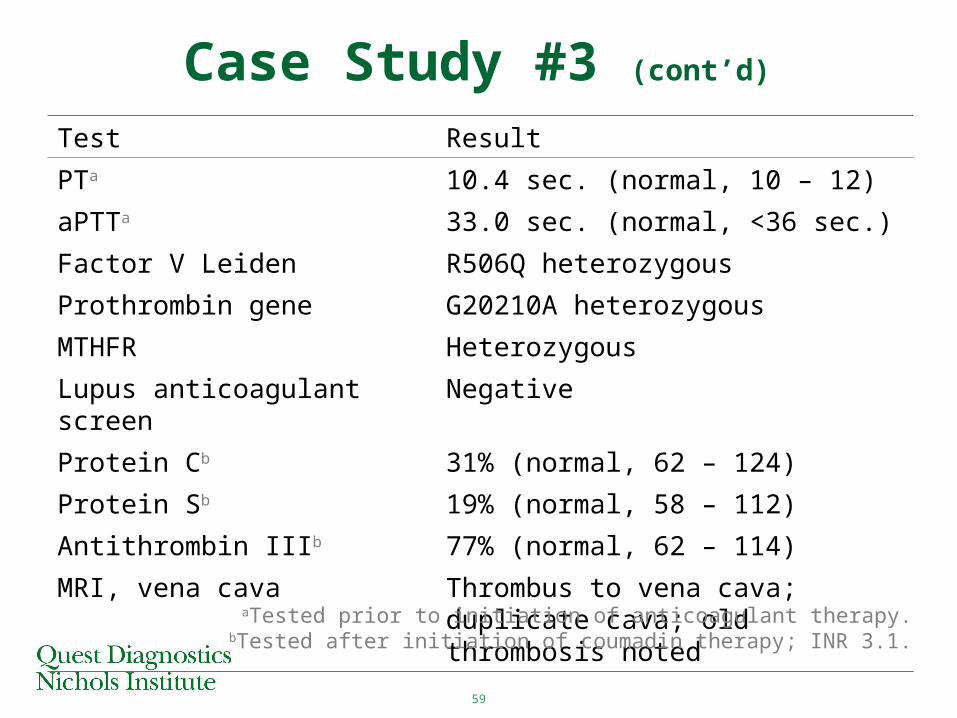
Case Study #3 (cont’d)
Test Result
PTa 10.4 sec. (normal, 10 – 12)
aPTTa 33.0 sec. (normal, <36 sec.)
Factor V Leiden R506Q heterozygous
Prothrombin gene G20210A heterozygous
MTHFR Heterozygous
Lupus anticoagulant screen Negative
Protein Cb 31% (normal, 62 – 124)
Protein Sb 19% (normal, 58 – 112)
Antithrombin IIIb 77% (normal, 62 – 114)
MRI, vena cava Thrombus to vena cava; duplicate cava; old thrombosis noted
aTested prior to initiation of anticoagulant therapy.bTested after initiation of coumadin therapy; INR 3.1.
60
Case Study #3 Conclusion
Long-term anticoagulation indicated
Schulman S, et al. N Engl J Med. 1997;336:393-398.
61
Case Study #4• Active 49 year-old white male experienced “charley horse” of right leg for >6 days
• Pain, swelling, and redness progressed to lower thigh area
• 16-year history of smoking
• Episode of superficial phlebitis following IV insertion during routine colonoscopy
62
Case Study #4 (cont’d)
• Thrombophilic workup negative for– Factor V G1691A– Prothrombin G20210A– Lupus anticoagulant– Protein C and S– Antithrombin
• Ultrasound duplex assessment demonstrated DVT involving both lower extremities
• Patient hospitalized for IV heparin therapy followed by coumadin therapy
63
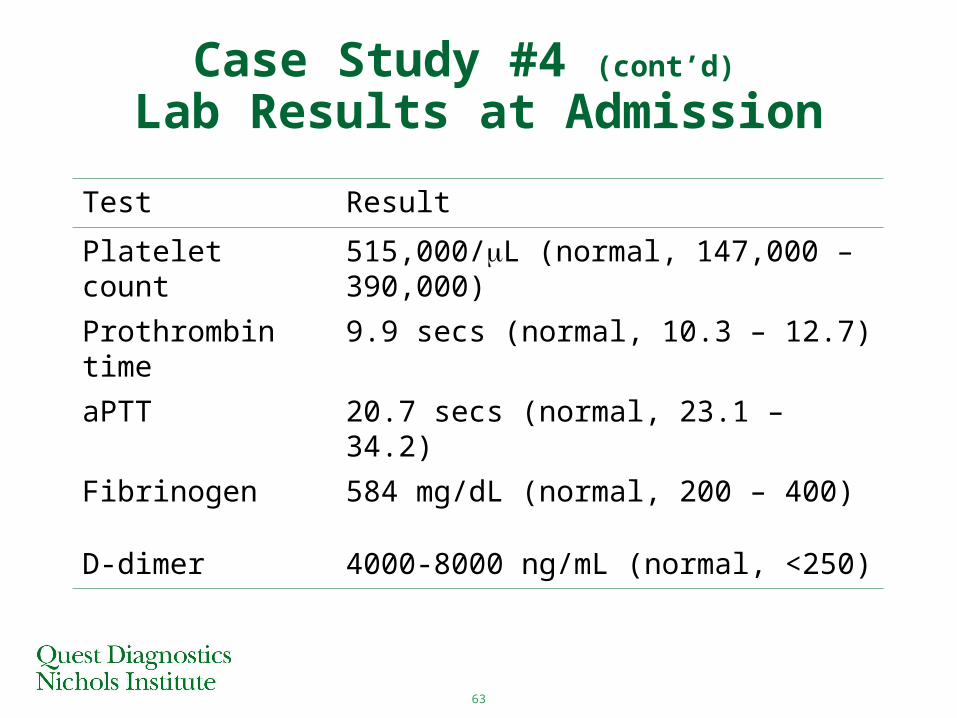
Case Study #4 (cont’d) Lab Results at Admission
Test Result
Platelet count 515,000/L (normal, 147,000 – 390,000)
Prothrombin time 9.9 secs (normal, 10.3 – 12.7)
aPTT 20.7 secs (normal, 23.1 – 34.2)
Fibrinogen 584 mg/dL (normal, 200 – 400)
D-dimer 4000-8000 ng/mL (normal, <250)
64
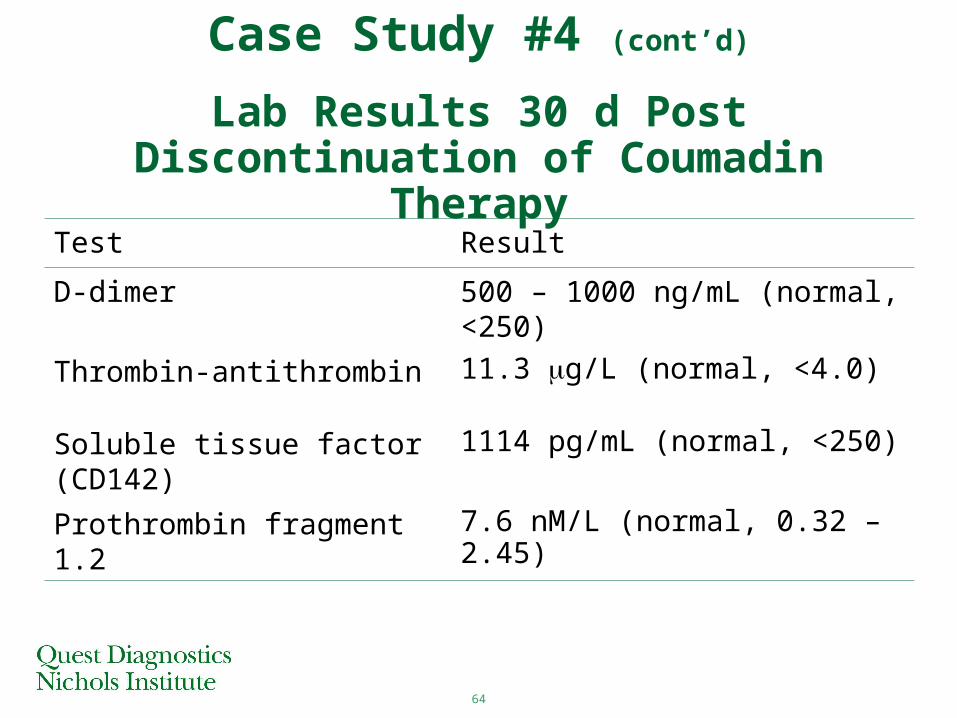
Test Result
D-dimer 500 – 1000 ng/mL (normal, <250)
Thrombin-antithrombin 11.3 g/L (normal, <4.0)
Soluble tissue factor (CD142) 1114 pg/mL (normal, <250)
Prothrombin fragment 1.2 7.6 nM/L (normal, 0.32 – 2.45)
Case Study #4 (cont’d)
Lab Results 30 d Post Discontinuation of Coumadin Therapy
65
Case Study #4 Conclusions1. Finding of unprovoked DVT and negative
thrombophilic workup requires closer look for possible malignancy even without referable symptoms
2. Development of superficial thrombophlebitis after brief IV insertion and subsequent development of unprovoked bilateral DVT is significant
3. High level of fibrinogen, elevated platelet counts, and shortened prothrombin time and aPTT are suggestive of hypercoagulability
66
Case Study #4 Conclusions4. Elevated thrombin generation markers 14
days post coumadin therapy are turning point in this patient’s workup & eventual diagnosis
5. High level of thrombin generation markers and presence of soluble tissue factor suggest antithrombin or Xa inhibitors (eg, low molecular weight heparins) would be more appropriate therapy
6. CT scan of chest reveals 3 cm mass, and bronchoscopic washing demonstrated malignant cells, ie, bronchogenic carcinoma
67
Case Study #5
• 19 year-old ballet dancer strains left calf and ankle
• Recently recovered from infectious mononucleosis
• Negative ultrasound duplex exam
68
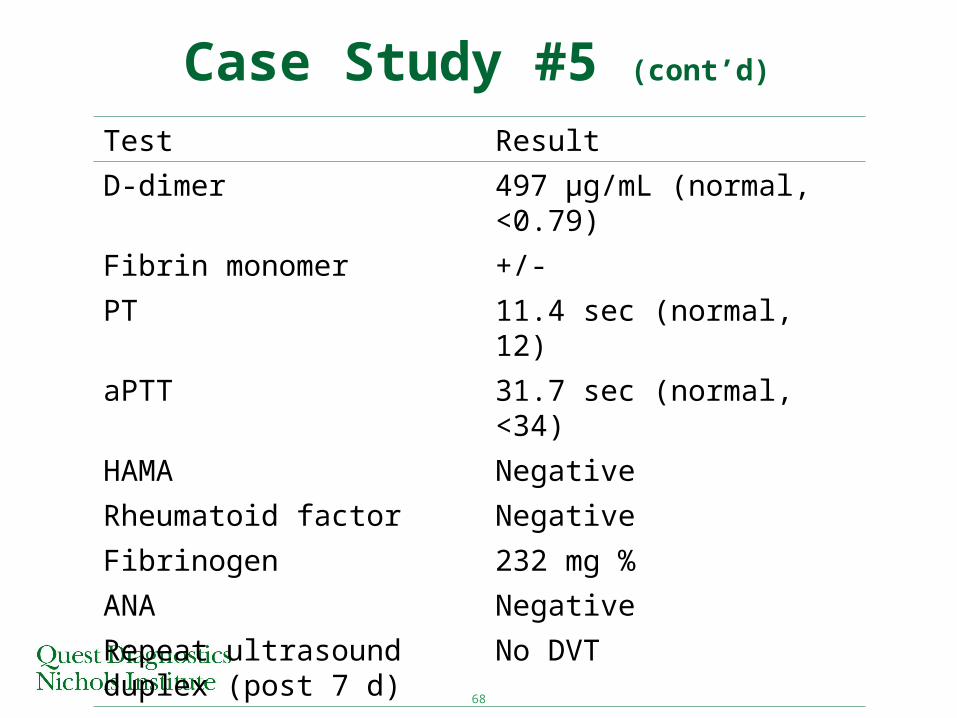
Test Result
D-dimer 497 µg/mL (normal, <0.79)
Fibrin monomer +/-
PT 11.4 sec (normal, 12)
aPTT 31.7 sec (normal, <34)
HAMA Negative
Rheumatoid factor Negative
Fibrinogen 232 mg %
ANA Negative
Repeat ultrasound duplex (post 7 d)
No DVT
Case Study #5 (cont’d)
69Medical Devices Agency 2002 Evaluation Report.
• Patient recovers, but D-dimer still elevated (241 µg/mL)
• False-positive identified
1. Demonstrated high heterophile antibody titer in patient serum
2. Incubated serum w/ heterophile blocking antibody, then repeated D-dimer test
3. Repeat D-dimer test normal
Case Study #5 (cont’d)
70
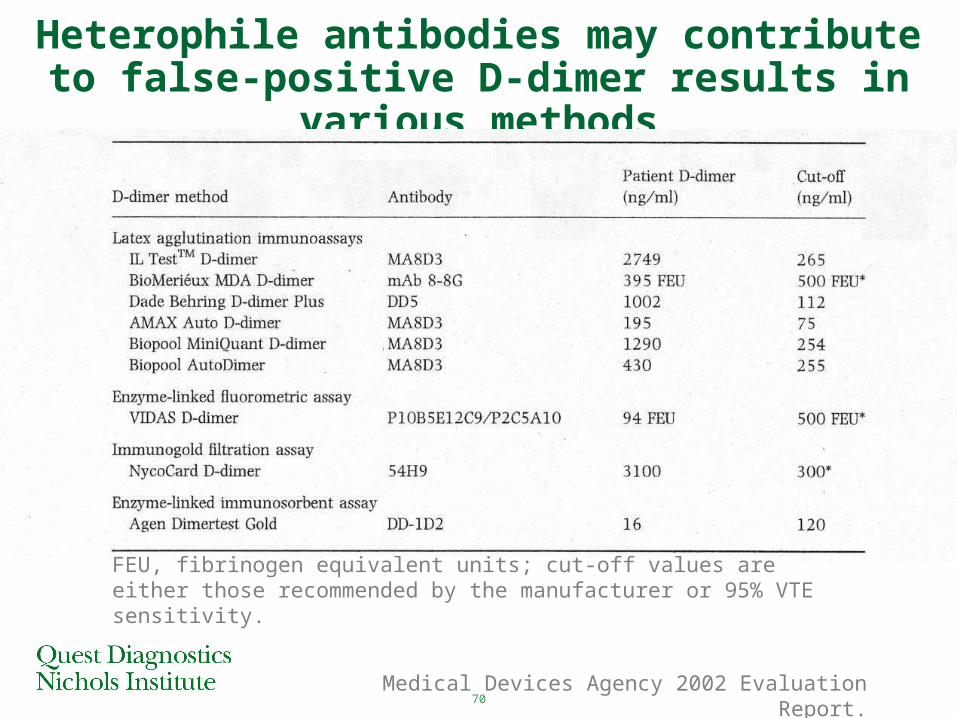
Heterophile antibodies may contribute to false-positive D-dimer results in various methods
Medical Devices Agency 2002 Evaluation Report.
FEU, fibrinogen equivalent units; cut-off values are either those recommended by the manufacturer or 95% VTE sensitivity.
71
• Thrombophilia (impact on DVT and PE)
• Risk factors
• Coagulation cascade
• Thrombophilia testing– Antithrombin– Protein C– Protein S– Activated protein C resistance (APCR)– Prothrombin (factor II) mutation– Lupus anticoagulant– Factor VIII excess
• Case studies• Recommended work-ups
Outline
72
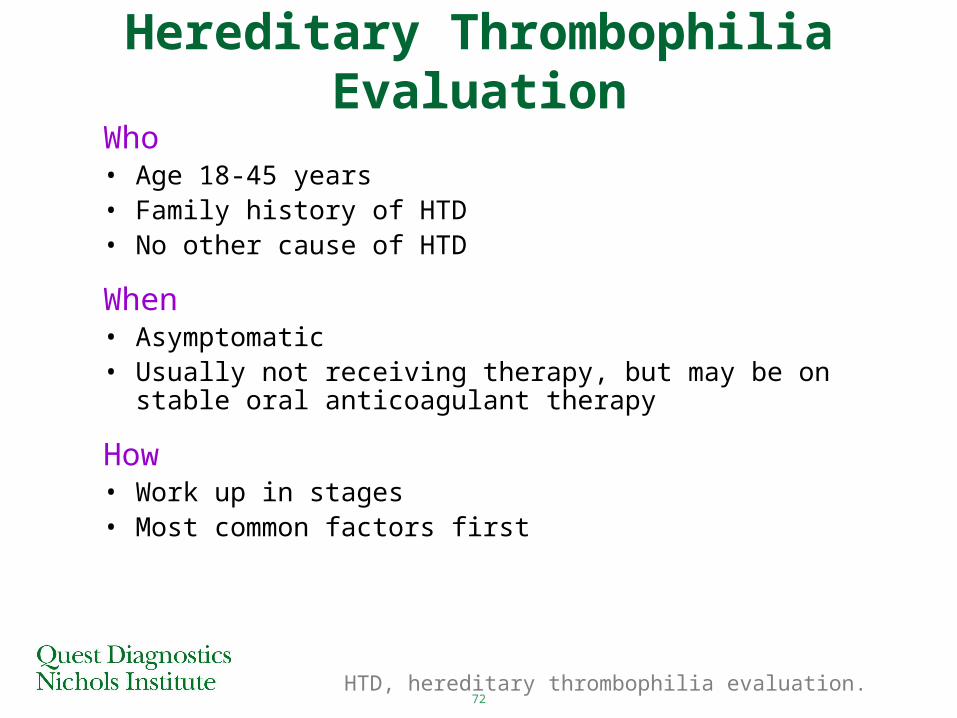
Hereditary Thrombophilia Evaluation
Who• Age 18-45 years • Family history of HTD• No other cause of HTD
When• Asymptomatic• Usually not receiving therapy, but may be on stable oral
anticoagulant therapy
How• Work up in stages• Most common factors first
HTD, hereditary thrombophilia evaluation.
73
Cost-Effective Hypercoagulation Workup
Below Age 45• APCR• Protein C• Protein S• Antithrombin
If APCR is abnormal or borderline normal, perform factor V Leiden mutation analysis.
If aPTT is abnormal, complete LA workup.
If homocysteine is abnormal, perform MTHFR mutation analysis.
• Prothrombin mutation• Homocysteine• LA (aPTT) and
ACA/APS
74
Cost-Effective Hypercoagulation Workup
Over Age 45• APCR• Homocysteine• Prothrombin mutation• LA (aPTT) and ACA/APS
If APCR is abnormal or borderline normal, perform factor V Leiden mutation analysis.
If aPTT is abnormal, complete LA workup.
If homocysteine is abnormal, perform MTHFR mutation analysis.
Thrombophilia Quiz
76
Thrombophilia Quiz
Which of the following statement(s) concerningactivated protein C resistance is/are true?
a. Activated protein C resistance is the most commonly inherited thrombophilic condition.
b. Factor V Leiden mutation is reported in 3% to 7% of the Caucasian population.
c. Approximately 20% to 60% of patients with venous thromboembolism have the Factor V Leiden mutation.
d. All of these
77
Thrombophilia Quiz
Which of the following statements concerningprothrombin mutation are true?
a. A mutated 20210 allele is a risk factor for venous and arterial thrombosis.
b. The increased thrombotic risk in patients with a mutated 20210 allele appears to be caused by excessive activation of the coagulation pathway.
c. In patients with a history of venous thrombosis, there is a 9- to 11-fold increase in the presence of the mutant 20210 allele.
d. All of these
78
Thrombophilia Quiz
All of the following statements concerningantithrombin are true except:
a. Patients with homozygous antithrombin deficiency usually present in the neonatal period with purpura fulminans.
b. Antithrombin is a major regulator of coagulation and inhibits activated Factor II, IX, X, XI, and XII.
c. Thrombosis is recurrent in approximately 60% of antithrombin deficient patients.
d. There are multiple amino acid substitutions responsible for congenital deficiencies of antithrombin.
79
Thrombophilia Quiz
Of patients who experience venous thrombosis,deficiencies of protein C, protein S, andantithrombin are collectively present in:
a. Approximately 15% of patients
b. Approximately 30% of patients
c. Approximately 50% of patients
d. Approximately 70% of patients
80
Thrombophilia Quiz
Patients with deficiency of protein C, protein S,or antithrombin usually present with:
a. Arterial thrombosis
b. Venous thrombosis
c. Recurrent arterial thromboembolic disease
d. All of these
81
Thrombophilia Quiz
Which of the following statement(s) concerningmethylene tetrahydrofolate reductase (MTHFR)is/are true?
a. MTHFR and cystathionine β synthase are the primary enzymes responsible for methionine metabolism.
b. At least 7 mutations of MTHFR have been reported to increase plasma homocysteine levels.
c. It is estimated that up to ½ of the North American population is heterozygous for a MTHFR mutation.
d. All of these
82
Thank You




















![[Mervyn Frost] Global Ethics(BookFi.org)](https://img.pdfslide.us/doc/110x75/55cf98fd550346d0339ae273/mervyn-frost-global-ethicsbookfiorg.jpg)

