Embed Size (px)
Citation preview

journal of orthopaedic & sports physical therapy | volume 41 | number 9 | september 2011 | 633
[ literature review ]
Neck pain is a common musculoskeletal condition, with a 12-month prevalence among the general and work force populations of 30% to 50%.19 As a consequence, neck pain is responsible for a large proportion of physical therapy visits.3,26
A common general classification in clinical studies is mechanical
neck pain, which includes patients without an identi-fiable pathoanatomic cause and excludes patients with neurological deficits, cervi-
cogenic headache, and systemic inflam-matory conditions.3,23 The operational definition of mechanical neck pain most frequently requires that the pain be ex-acerbated by motion. However, there is variability among studies, as patients with radiculopathy or whiplash mecha-nisms, for example, have been exclud-ed.10,17,18,29 While treatment for patients classified with mechanical neck pain has been investigated, there is no consensus within the literature on a gold standard for treatment.3,6,19,28
One approach to conservative treat-ment of neck pain includes cervical mobilization and thrust manipulation. The potential for complications caused by thrust manipulation of the cervical spine, such as vertebrobasilar artery in-jury, has been extensively discussed in the literature.2,14,20,21,34 Although the risk of vertebrobasilar artery dissection has been reported to be very low,14,25 screen-ing tools to identify patients who are at
TT STUDY DESIGN: Systematic review.
TT BACKGROUND: Neck pain is a common diagno-sis in the physical therapy setting, yet there is no gold standard for treatment. This study is part of a growing body of literature on the use of thoracic spine thrust manipulation for the treatment of individuals with mechanical neck pain.
TT OBJECTIVE: The purpose of this systematic re-view was to determine the effects of thoracic spine thrust manipulation on pain, range of motion, and self-reported function in patients with mechanical neck pain.
TT METHODS: Six online databases were compre-hensively searched from their respective inception to October 2010. The primary search terms included “thoracic mobilization,” “thoracic spine mobilization,” “thoracic manipulation,” and “tho-racic spine manipulation.” Of the 44 studies as-sessed for inclusion, 6 randomized controlled trials were retained. Between-group mean differences and effect sizes for pretreatment-to-posttreatment change scores, using Cohen’s d formula, were cal-culated for pain, range of motion, and subjective
function at all stated time intervals.
TT RESULTS: Effect size point estimates for the pain change scores were significant for global assessment across all studies (range, 0.38-4.03) but not conclusively significant at the end range of active rotation (range, 0.02-1.79). Effect size point estimates were large among all range-of-motion change measures (range, 1.40-3.52), and the effect size point estimates of the change scores among the functional questionnaires (range, 0.47-3.64) also indicated a significant treatment effect.
TT CONCLUSIONS: Thoracic spine thrust manipula-tion may provide short-term improvement in patients with acute or subacute mechanical neck pain. However, the body of literature is weak, and these results may not be generalizable.
TT LEVEL OF EVIDENCE: Therapy, level 1b–. J Orthop Sports Phys Ther 2011;41(9):633-642. doi:10.2519/jospt.2011.3670
TT KEY WORDS: cervical spine, manipulative therapy, manual therapy
1Physical Therapist, UVA Healthsouth, Charlottesville, VA. 2Doctoral Candidate, University of Virginia, Charlottesville, VA. 3Assistant Professor, Creighton University, Omaha, NE. 4Joe H. Gieck Professor of Sports Medicine, University of Virginia, Charlottesville, VA. Address correspondence to Kevin Cross, 5004 Madison Court, Charlottesville, VA 22911. E-mail: [email protected]
KEVIN M. CROSS, PT, PhD, ATC1 • CHRIS KUENZE, MA, ATC2 • TERRY GRINDSTAFF, PT, PhD3 • JAY HERTEL, PhD, ATC4
Thoracic Spine Thrust Manipulation Improves Pain, Range of Motion,
and Self-Reported Function in Patients With Mechanical Neck Pain:
A Systematic Review
41-09 Cross.indd 633 8/16/2011 6:28:33 PM

634 | september 2011 | volume 41 | number 9 | journal of orthopaedic & sports physical therapy
[ literature review ]risk of adverse effects from the thrust manipulation have been proposed and their use recommended, despite a lack of evidence supporting their validity.24,27,37 Moreover, the literature has recommend-ed avoiding manual therapies at terminal ranges of motion4 and cautioned against the use of cervical thrust manipulation due to the perceived risk of serious vas-cular complications, especially in specific subgroups of the population.27,32,34 Alter-natively, thoracic spine thrust manipula-tion may effectively address mechanical neck pain.4,32
There is a recent but growing body of literature evaluating the clinical effective-ness of thoracic spine thrust manipula-tion for patients with mechanical neck pain. Therefore, the purpose of this sys-tematic review was to evaluate the effects of thoracic spine thrust manipulation on pain in patients with mechanical neck pain, and the effects of thoracic spine thrust manipulation on cervical range of motion (ROM) and patient self-reported function in that same population.
METHODS
To provide a thorough system-atic review, we referred to the PRIS-MA Explanation and Elaboration
document.35 The PRISMA checklist was used in attempt to provide comprehen-sive and high-quality research to assess the effectiveness of thoracic spine thrust manipulation in patients with mechani-cal neck pain.
Search StrategySix online databases (CINAHL, Cochrane Library, PubMed, PEDro, Sport Discus, and Web of Science) were comprehen-sively searched from their respective inception to October 2010. The search 1 query included the terms “thoracic spine manipulation,” “thoracic spine mobilization,” “thoracic manipulation,” and “thoracic mobilization,” which were all combined with the Boolean operator “OR.” The search 2 query used the terms “cervical spine pain,” “cervical pain,” and
“neck pain,” which were also combined with the Boolean operator “OR.” We then combined searches 1 and 2 using the Boolean operator “AND.” We placed no restrictions on the publication date; the only limitation was that the language had to be English. The reference lists of viable studies were cross-referenced to identify additional articles not detected in the original medical database searches.
Study SelectionFollowing the search in each database, 2 of the authors (K.M.C. and C.K.) in-dividually selected the studies to be in-cluded in the systematic review. First, the context of each study’s title was screened for relevance to the systematic review’s purpose. The abstracts of those studies with relevant titles were then reviewed for pertinence to the topic. If an abstract suggested that the manuscript provided information regarding the effect of tho-racic spine thrust manipulation on cervi-cal or neck pain, the article was read and thoroughly assessed for the inclusion or exclusion criteria. Because the primary outcome for data analysis was neck pain, the study had to report pain data that permitted a preintervention-to-postint-ervention analysis of changes in pain scores. The 2 authors then compared their search results to create 1 compre-hensive list of studies for inclusion.
Studies were included in this review if they satisfied the following criteria: (1) the treatment group received thrust manipulation to the thoracic spine; (2) only patients diagnosed with mechanical neck pain were included in the study; (3) pain needed to be reported as an outcome measure; (4) detailed eligibility criteria for the patients participating in the study were provided.31
Studies were excluded based on the following criteria: (1) absence of a com-parison group; (2) treatment group received a thrust manipulation to the cervical spine; and (3) patients were diagnosed with neurological deficits, cervicogenic headaches, or multiple di-agnoses. Based on these criteria, 2 inves-
tigators (K.M.C. and C.K.) assessed the articles for inclusion into the review.
Quality AssessmentSelected studies were evaluated using the Physiotherapy Evidence Database (PEDro) scale, which utilizes a 10-point scoring system to assess the methodologi-cal quality of randomized controlled tri-als.31 Two investigators (K.M.C. and C.K.) independently assessed each study. If a disagreement in scores occurred, the investigators discussed the study’s qual-ity to determine consensus on the final score. If consensus could not be attained, then a third investigator (J.H.), blinded to the previous assessment scores, re-solved the disagreement.
Data ExtractionTwo investigators (K.M.C. and C.K.) in-dependently extracted data from the se-lected studies using standardized forms. Specifically, each investigator docu-mented the study design, study purpose, experimental and comparison interven-tions, number of subjects in each condi-tion, follow-up intervals (as indicated by the duration from treatment initiation), outcome variables, and study quality score (PEDro). The authors compared their standardized forms for each study to verify the accuracy of data collection.
The outcomes of interest were pain, cervical spine ROM, and self-reported function. To compare the effectiveness of the experimental and comparison inter-ventions, we analyzed the change scores from the initial visit to each follow-up interval between each group.
Data AnalysisAlthough all studies included in this re-view assessed pain as one of the outcome measures, the pain and self-reported function parameters were frequently measured using different instruments. The pain measurements, specifically, were performed in varying contexts and during different activities, such as pain at rest versus pain associated with end range of cervical rotation. Most notably,
41-09 Cross.indd 634 8/16/2011 6:28:34 PM
journal of orthopaedic & sports physical therapy | volume 41 | number 9 | september 2011 | 635
all outcome assessments occurred at dif-ferent time intervals following the inter-vention. Consequently, data could not be collapsed across studies for meta-anal-ysis. In each study, the between-group mean difference (95% confidence inter-val [CI]) and effect size (95% CI) for the preintervention-to-postintervention change scores, using Cohen’s d formula, were calculated for pain, ROM, and self-reported function at each of the follow-up assessments. The effect size was calculat-ed as d = xmanipulation – xnonmanipulation/SDpooled, where x represents the average change score and SD represents the pooled stan-dard deviation between manipulation and comparison groups.
The effect size was positive if the treat-ment group that included the thoracic spine thrust manipulation had a larger treatment effect than the comparison group, as indicated by a larger preinter-vention-to-postintervention change score on the outcome variable. The effect size
was negative if the comparison group had a larger treatment effect. The strength of the effect size was determined as trivial (<0.2), small (0.2-0.39), moderate (0.4-0.7), or large (>0.7).12 All nontrivial effect sizes (small to large) with 95% CIs that did not include zero were considered to represent a significant treatment effect.22
RESULTS
Study Descriptions and Methodological Quality
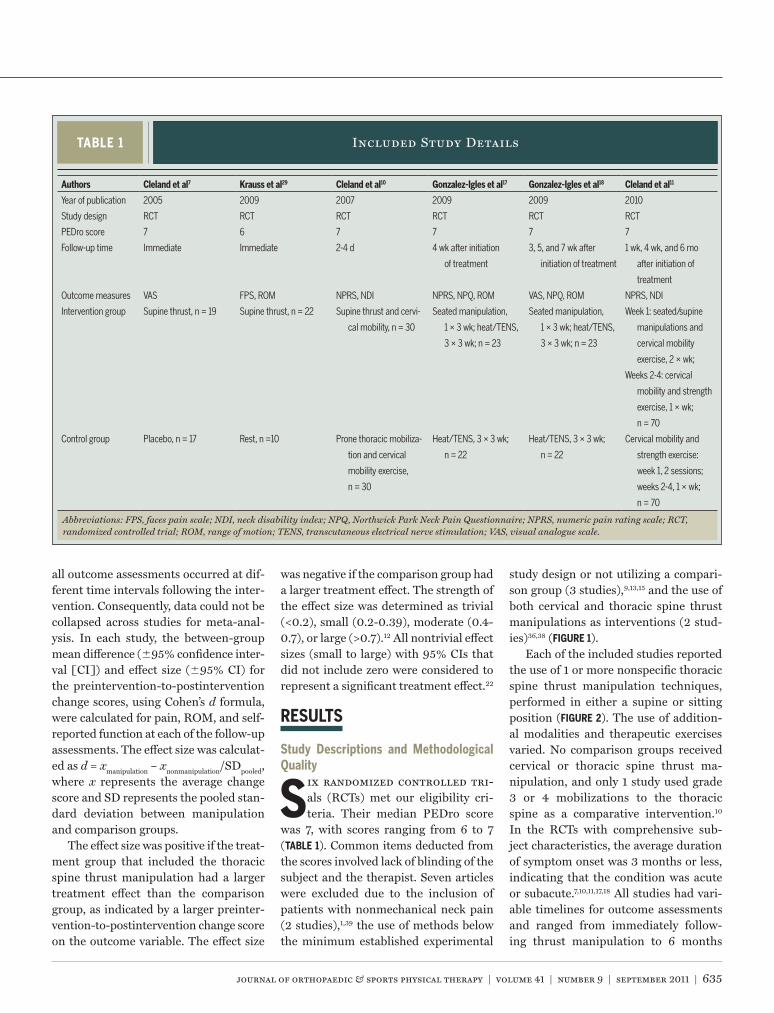
Six randomized controlled tri-als (RCTs) met our eligibility cri-teria. Their median PEDro score
was 7, with scores ranging from 6 to 7 (TABLE 1). Common items deducted from the scores involved lack of blinding of the subject and the therapist. Seven articles were excluded due to the inclusion of patients with nonmechanical neck pain (2 studies),1,39 the use of methods below the minimum established experimental
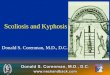
study design or not utilizing a compari-son group (3 studies),9,13,15 and the use of both cervical and thoracic spine thrust manipulations as interventions (2 stud-ies)36,38 (FIGURE 1).
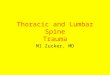
Each of the included studies reported the use of 1 or more nonspecific thoracic spine thrust manipulation techniques, performed in either a supine or sitting position (FIGURE 2). The use of addition-al modalities and therapeutic exercises varied. No comparison groups received cervical or thoracic spine thrust ma-nipulation, and only 1 study used grade 3 or 4 mobilizations to the thoracic spine as a comparative intervention.10 In the RCTs with comprehensive sub-ject characteristics, the average duration of symptom onset was 3 months or less, indicating that the condition was acute or subacute.7,10,11,17,18 All studies had vari-able timelines for outcome assessments and ranged from immediately follow-ing thrust manipulation to 6 months
TABLE 1 Included Study Details
Abbreviations: FPS, faces pain scale; NDI, neck disability index; NPQ, Northwick Park Neck Pain Questionnaire; NPRS, numeric pain rating scale; RCT, randomized controlled trial; ROM, range of motion; TENS, transcutaneous electrical nerve stimulation; VAS, visual analogue scale.
Authors Cleland et al7 Krauss et al29 Cleland et al10 Gonzalez-Igles et al17 Gonzalez-Igles et al18 Cleland et al11
Year of publication 2005 2009 2007 2009 2009 2010
Study design RCT RCT RCT RCT RCT RCT
PEDro score 7 6 7 7 7 7
Follow-up time Immediate Immediate 2-4 d 4 wk after initiation
of treatment
3, 5, and 7 wk after
initiation of treatment
1 wk, 4 wk, and 6 mo
after initiation of
treatment
Outcome measures VAS FPS, ROM NPRS, NDI NPRS, NPQ, ROM VAS, NPQ, ROM NPRS, NDI
Intervention group Supine thrust, n = 19 Supine thrust, n = 22 Supine thrust and cervi-
cal mobility, n = 30
Seated manipulation,
1 × 3 wk; heat/TENS,
3 × 3 wk; n = 23
Seated manipulation,
1 × 3 wk; heat/TENS,
3 × 3 wk; n = 23
Week 1: seated/supine
manipulations and
cervical mobility
exercise, 2 × wk;
Weeks 2-4: cervical
mobility and strength
exercise, 1 × wk;
n = 70
Control group Placebo, n = 17 Rest, n =10 Prone thoracic mobiliza-
tion and cervical
mobility exercise,
n = 30
Heat/TENS, 3 × 3 wk;
n = 22
Heat/TENS, 3 × 3 wk;
n = 22
Cervical mobility and
strength exercise:
week 1, 2 sessions;
weeks 2-4, 1 × wk;
n = 70
41-09 Cross.indd 635 8/16/2011 6:28:35 PM

636 | september 2011 | volume 41 | number 9 | journal of orthopaedic & sports physical therapy
[ literature review ]after the beginning of the intervention. TABLE 1 provides the information neces-sary to interpret the results, based on the individual study characteristics.
Outcome AssessmentWith the exception of the study by Cle-land et al,11 the average change score and either the SD7,10 or the 95% CI17,18,29 for the change score were provided for the variables in all of the included studies. In both studies by Gonzalez-Iglesias et al17,18 and the study by Krauss et al,29 the SD for the change scores was calculated from the equation for the 95% CI. The SD of the change score was needed to calculate effect sizes. For the most recent article by Cleland et al,11 the author provided, upon request, the mean and SD of the change scores for the variables of interest.
PainAll included studies reported preinter-vention and postintervention pain val-ues using either the visual analog scale,7,18 faces pain scale,29 or numeric pain rating scale.10,11,17 There was considerable vari-ability among studies regarding pain measurement and time of follow-up, so the pain data were not collapsed for anal-ysis. The effect size point estimates for the change scores of global pain ranged from small to large across all studies (0.38 to 4.03). FIGURE 3 shows the effect sizes and 95% CIs for the pain scores in each study.
In contrast to a global pain assess-ment, Krauss et al29 reported pain in patients at the end of active left and right cervical rotation as appropriate to cause symptoms. The effect size point estimates were generally smaller than those for pain at rest, ranging from 0.02 to 1.79; but the 95% CI included zero for most subgroups, indicating that conclu-sive treatment effects on pain at the end range of cervical rotation were not pres-ent (FIGURE 3).
Range of MotionKrauss et al29 assessed the immediate changes in active cervical rotation ROM following thoracic spine thrust manipula-
tion. Two separate studies by Gonzalez-Iglesias et al17,18 reported cervical ROM in all planes, following a 3-week course of electrothermal treatment and a thoracic spine thrust manipulation performed once per week. The ROM measures were taken at 3, 4, and 5 weeks follow-ing the treatment initiation. The average mean improvement for cervical flexion and extension ranged from 8.1° to 12.0° and 7.0° to 11.4°, respectively, while the mean cervical rotation improvements varied from 7.7° to 12.5°. The effect size point estimates for ROM change scores were large, varying from 1.39 to 3.23. FIGURE 4 presents the mean differences of the change scores between the thrust manipulation and comparison groups and 95% CIs for ROM measures.
Activity- and Disability-Related OutcomesFunctional outcome measures included the Neck Disability Index10,11 and the Northwick Park Neck Pain Question-
naire.17,18 Effect size point estimates for change scores among the functional questionnaires were moderate to large and varied from 0.47 to 3.64. FIGURE 5 shows the effect sizes and 95% CIs for the self-reported functional outcome measures.
Adverse EventsOnly 2 of the included studies presented complications or adverse events as a re-sult of the interventions. Cleland et al10 reported no significant differences in the number of side effects experienced by individuals in the thrust manipula-tion versus nonthrust group. Specifi-cally, aggravation of symptoms (n = 2), muscle spasm (n = 1), neck stiffness (n = 2), headache (n = 2), and radiating symptoms (n = 2) were reported in the nonthrust group, while aggravation of symptoms (n = 8), muscle spasm (n = 1), and headache (n = 1) were reported in the thrust manipulation group. The onset of
Initial search results: n = 534
Abstracts reviewed: n = 44
Manuscripts read: n = 13
Included in review: n = 6
Excluded based on title: n = 490
Excluded based on abstract: n = 31
Excluded based on content:• Nonmechanical neck pain: n = 21,39
• Lack of comparison group:n = 39,13,15
• Treatment included cervical manipulation: n = 236,38
FIGURE 1. PRISMA flowchart for study selection.
41-09 Cross.indd 636 8/16/2011 6:28:36 PM

journal of orthopaedic & sports physical therapy | volume 41 | number 9 | september 2011 | 637
these side effects was not significantly dif-ferent between groups, with individuals reporting an onset of side effects within 24 hours of treatment, with a duration of no greater than 24 hours, regardless of group assignment. In a later study by Cleland et al,11 no adverse events in either
group throughout the trial were reported.
DISCUSSION
The results of this systematic review indicate that thoracic spine thrust manipulation may be utilized
in the management of acute or subacute mechanical neck pain to reduce pain, improve cervical ROM, and improve function. Positive effects were shown to occur immediately following the first in-tervention and continued up to 6 months after participants were discharged from a 3-week program with repeated thoracic spine thrust manipulations. These re-sults, however, must be interpreted with caution. Although the individual RCTs were of high quality, as graded by the PEDro scale, the overall body of litera-ture had significant flaws that limit the generalizability of the results.
Evaluation of the Body of LiteratureThe primary limitation of the current body of literature is the limited number of RCTs. Our literature search identi-fied 6 RCTs with 3 different lead au-thors.7,10,11,17,18,29 Although the subject demographics for the 2 RCTs authored by Gonzalez-Iglesias et al17,18 were very similar, they were verified to be 2 com-pletely different samples of subjects. While our search was extensive through 6 databases, biases may exist within our search criteria. We performed literature searches in medical databases that were accessible through the medical school or accessible online. While these databases capture the vast majority of physical ther-apy trials, it is possible that they might have missed or failed to index certain tri-als.33 Moreover, our decision to limit this review to articles published only in the English language might have excluded pertinent articles in other languages. Similarly, our decision to use only pub-lished studies might have introduced bias and inadvertently magnified the effects of thoracic spine thrust manipulations. Nor were experts of spinal thrust manipula-tion and mechanical neck pain contacted to ensure that there were no unintention-ally overlooked articles within the inclu-sion and exclusion criteria. Within the considerations for bias that are normal for systematic reviews, the minimal vari-ability among the clinicians and patient types for the studies included in this sys-
FIGURE 2. Common thoracic spine thrust manipulation techniques described in the literature. (A) Supine thrust manipulation technique: the patient lies supine, with the arms wrapped across the chest. The therapist pulls the elbows of the patient toward the chest to induce passive cervical and thoracic flexion. Then, the therapist provides a high-velocity, low-amplitude thrust through the arms of the patient toward the thoracic spine at a targeted level, as dictated by the manipulative hand. (B) Seated thrust manipulation technique: the patient sits with the arms crossing the chest. The patient leans back into the chest of the therapist at the midthoracic level. Passive thoracic spine flexion is applied until the therapist perceives tension, then the therapist provides a distraction thrust in an upward direction.
–2 –1 0 1 2 3 4 5 6
Favors Comparison Favors Thoracic Spine Thrust Manipulation
0.45 (0.08, 0.83), 6 mo11
0.38 (0.04, 0.71), 4 wk11
0.79 (0.45, 1.14), 1 wk11
1.58 (1.00, 2.16), 2-4 d10
1.75 (0.98, 2.53), immediate7
1.39 (–0.28, 3.05), immediate; B to L29*
1.79 (0.05, 3.53), immediate; B to R29*
0.02 (–1.31, 1.35), immediate; L29*
0.74 (–0.48, 1.97), immediate; R29*
2.58 (1.79, 3.38), 7 wk18
1.92 (1.21, 2.62), 5 wk18
3.82 (2.84, 4.80), 4 wk17
4.03 (3.01, 5.04), 3 wk18
FIGURE 3. Effect sizes (95% confidence interval) for pain relief following thoracic spine thrust manipulation. Abbreviations: L, pain and measurement with left cervical rotation; R, pain and measurement with right cervical rotation; B to R, pain with bilateral rotation and measurement with right rotation; B to L, pain with bilateral rotation and measurement with left rotation. All time measures are relative to the initiation of interventions. *Pain measured at end range of cervical rotation.
41-09 Cross.indd 637 8/16/2011 6:28:37 PM

638 | september 2011 | volume 41 | number 9 | journal of orthopaedic & sports physical therapy
[ literature review ]
tematic review diminished the external validity of the results.
Regarding cervical spine pathology, all subjects were diagnosed with mechanical neck pain, and most of them had an aver-age symptom onset duration of less than 3 months.7,10,11,17,18 Krauss et al29 did not report the duration of symptoms of their study participants. Very few participants with chronic neck pain were included in the selected trials, which limits the gen-eralizability of the findings beyond pa-tients with acute and subacute neck pain. The broad definition of mechanical neck pain, from a pathological perspective, reflects the proposed treatment-based neck pain classification categories of pain control and conditioning and mobil-ity.5 Considering that the purpose of the treatment-based classification system is
to provide direction for physical therapy interventions,5 this systematic review of the effectiveness of thoracic spine thrust manipulation among a narrower scope of neck injuries (acute and subacute mechanical neck pain) provides support for its potential as an intervention. Due to the relatively homogeneous patient sample in the included studies, the re-sults may not be generalizable across pa-tients with differing diagnoses or onset durations.
The RTCs described 2 thoracic spine thrust manipulation techniques, yet none of the studies provided clinical reasoning for the selection of a specific technique. The specific site to which the thrust ma-nipulation was applied also varied among studies, with 4 RCTs attempting to pro-vide the thrust manipulation at 1 or more
generic locations of the midthoracic and upper thoracic spine.10,11,17,18 Cleland et al10 extrapolated on the decision for using a generic location for thoracic spine thrust manipulation, recognizing that the tech-nique does not target specific vertebral segments. In contrast, to simulate clinical practice, 2 studies7,29 attempted to specifi-cally manipulate segments that were de-termined to be hypomobile during joint mobility testing. Nevertheless, outcomes among the current studies did not appear to be influenced by the specific technique or rationale for application.
Variation among the comparative interventions also blurred the effects of thoracic spine thrust manipulation. Comparison treatments included place-bo thrust manipulation,7 rest,29 thoracic spine mobilization and cervical mobility
0 2 4 6 8 10 12 14 16 18
ROM Change Score Dierence, deg
8.10 (4.62, 11.58), 5 wk18
10.70 (8.69, 12.71), 4 wk17
12.0 (9.95, 14.04), 3 wk18
0 2 4 6 8 10 12 14 16 18
ROM Change Score Dierence, deg
7.00 (4.27, 9.73), 5 wk18
10.00 (8.14, 11.86), 4 wk17
11.40 (9.20, 13.60), 3 wk18
0 2 4 6 8 10 12 14 16 18
ROM Change Score Dierence, deg
12.10 (8.88, 15.32), 5 wk R18
8.50 (5.20, 11.80), 5 wk L18
9.60 (7.49, 11.71), 4 wk R17
8.30 (6.38, 10.22), 4 wk L17
7.69 (3.58, 11.80), immdediate L29
8.33 (3.40, 13.26), immediate R29
11.20 (8.87, 13.53), 3 wk L18
12.50 (9.80, 15.20), 3 wk R18
0 2 4 6 8 10 12 14 16
ROM Change Score Dierence, deg
8.70 (7.03, 10.37), 5 wk R18
5.90 (3.56, 8.23), 5 wk L18
8.10 (6.19, 10.00), 4 wk L17
9.60 (7.55, 11.65), 4 wk R17
9.30 (7.55, 11.05), 3 wk R18
10.80 (8.40, 13.20), 3 wk L18
A B
C D
FIGURE 4. Mean difference (95% confidence interval) in cervical ROM change scores between the thoracic spine thrust manipulation and comparison groups. Positive values favor thoracic spine thrust manipulation. All time measures are relative to the initiation of interventions. (A) Cervical flexion. (B) Cervical extension. (C) Cervical rotation. (D) Cervical lateral flexion. Abbreviations: L, left; R, right; ROM, range of motion.
41-09 Cross.indd 638 8/16/2011 6:28:38 PM

journal of orthopaedic & sports physical therapy | volume 41 | number 9 | september 2011 | 639
exercises,10 electrothermal therapies,17,18 and a comprehensive exercise program.11 Only 2 studies7,10 used a comparison in-tervention directed at the thoracic spine, and only 2 studies10,11 used a comparison intervention that directly addressed the pathological area with therapeutic ex-ercise. However, regardless of the com-parative interventions, the results of the statistical analysis suggest that treat-ment programs which incorporate a thoracic spine thrust manipulation have larger treatment effects on the outcome measures.
The follow-up intervals for all stud-ies included in this review were relatively short. The current literature has individ-ual reports for treatment effectiveness immediately following the treatment7,29 and at 2 to 4 days,10 3 to 7 weeks,17,18 and 6 months11 after treatment initiation. There is no study, to our knowledge, which in-vestigates evidence of treatment effec-tiveness beyond 6 months posttreatment initiation. Although various follow-up in-tervals have been reported, they have not been validated by other research groups, and long-term outcomes have not been reported.
Clinical ImplicationsPrior to 2005, there were no RCTs that
investigated the clinical effectiveness of a thoracic spine thrust manipulation as an isolated manual therapy technique for patients with neck pain. Since that time, there have been several investigations of the clinical utility of thoracic spine thrust manipulation in the management of me-chanical neck pain across various follow-up times and within diverse intervention programs. Within these investigations, the effectiveness of 2 distinct thoracic spine thrust manipulation techniques have been reported (FIGURE 2), both of which provided short-term improve-ments in pain, cervical ROM, and self-reported function among patients with acute or subacute mechanical neck pain.
Thoracic spine thrust manipulation, performed by itself or in combination with other interventions, may decrease neck pain, with the decrease occurring immediately after a single thrust manip-ulation intervention and persisting up to 6 months. In each study, thoracic spine thrust manipulation was found to have a positive effect size when compared to the control intervention. The range of effect sizes for change in pain following thrust manipulation intervention has been wide. Studies using a control intervention of passive treatment or a placebo7,10,17,18 reported larger positive effect sizes than
those which compared the intervention with a comprehensive exercise program.11 This reduction in effect size for the addi-tion of the thrust manipulation interven-tion highlights the therapeutic benefit of a methodically devised exercise program on managing cervical spine pain.3 While there was clear variability in the control intervention among the studies (TABLE 1), their results indicate that patients with mechanical neck pain who received tho-racic spine thrust manipulation experi-enced significant decreases in pain.
Pain at the end range of cervical ro-tation, in contrast to global pain ratings, was the primary outcome measure in 1 trial.29 Only those patients who experi-enced pain with bilateral cervical rotation reported decreased pain at the end range rotation, following the thrust manipula-tion. The authors, by assessing pain at the end ranges of cervical rotation as op-posed to at rest, have suggested that the source for mechanical pain may still be present at the end range, even though cervical spine ROM has improved.29 This would account for the lack of improve-ment in pain reported in this study as compared to the other studies in this review.
Patients who received thoracic spine thrust manipulation alone or in combi-nation with ROM exercises or modalities had increased cervical spine mobility. In all RCTs, thoracic spine thrust manipula-tion resulted in larger ROM changes and significant CIs. Each study that measured cervical ROM used the cervical range-of-motion (CROM) device, which has an es-tablished minimal detectable change for patients with neck pain.16 In the majority of follow-up intervals, the point estimate of the within-group ROM change scores exceeded the minimal detectable change only in the thoracic spine thrust manipu-lation group (TABLE 2), and the between-group ROM change scores for all ROM were positive for the thrust manipulation groups. However, there was variability in the magnitude of the treatment effect across time (FIGURE 4). Further research is necessary to examine the long-term treat-
–1 0 1 2 3 4 5 6
Favors Comparison Favors Thoracic Spine Thrust Manipulation
0.58 (0.20, 0.95), 6 mo11
2.06 (1.34, 2.79), 5 wk18
3.51 (2.58, 4.45), 4 wk17
0.47 (0.13, 0.80), 4 wk11
3.64 (2.68, 4.59), 3 wk18
0.56 (0.22, 0.89), 1 wk11
1.10 (0.56, 1.65), 2-4 d10
FIGURE 5. Effect sizes (95% confidence interval) for self-reported function following thoracic spine thrust manipulation. All time intervals are relative to the initiation of interventions.
41-09 Cross.indd 639 8/16/2011 6:28:39 PM

640 | september 2011 | volume 41 | number 9 | journal of orthopaedic & sports physical therapy
[ literature review ]
REFERENCES
1. Browder DA, Erhard RE, Piva SR. Intermittent
cervical traction and thoracic manipulation
ment effect of thoracic spine thrust ma-nipulations on cervical spine ROM and in comparison to a standardized physical therapy program.
Based on this review, the effectiveness of thoracic spine thrust manipulation, in conjunction with exercises or modalities on self-reported function in patients with mechanical neck pain, appears to depend on the duration of the follow-up interval. While only 4 studies10,11,17,18 included self-reported function as an outcome variable, all reported moderate to large effect sizes. Although there is disparity in the litera-ture regarding the psychometric proper-ties of the Neck Disability Index among
various cervical pathologies,30 the only study to report a Neck Disability Index change score conclusively greater than the minimal clinically important differ-ence among patients with mechanical neck pain8,41 was the Cleland et al11 study at the 4-week and 6-month follow-ups af-ter treatment initiation. The significance of these changes in self-reported func-tion are further illustrated by the signifi-cantly greater number of patients in the thrust manipulation and exercise group, as compared to the exercise-only group, who reported a successful outcome at the 4-week and 6-month follow-ups af-ter treatment initiation.11 Of the studies
which used the Northwick Park Neck Pain Questionnaire,17,18 the change score in only the thrust manipulation group exceeded the minimal clinically impor-tant difference at 3, 4, and 5 weeks af-ter treatment initiation.40 Unfortunately, global assessments of change scores were not provided for either group, which limits the interpretation of improve-ment by the Northwick Park Neck Pain Questionnaire.40
CONCLUSION
In the current literature, thorac-ic spine thrust manipulation reduced pain and improved ROM among pa-
tients with acute or subacute mechanical neck pain. Optimal treatment parameters are not clear from the current literature. It appears that thoracic spine thrust ma-nipulation can provide a positive treat-ment effect immediately following thrust manipulation, as well as short-term improvement in symptoms following a course of repeated thrust manipulations. However, there are several weaknesses in the body of literature, particularly in the limited number of RCTs and the con-sequent lack of variability among lead authors, which limits the generalizability of the results for multiple patient types and clinical environments. Therefore, clinicians must apply these findings to their clinical practice with caution. Tho-racic spine thrust manipulation should be considered when treating patients with mechanical neck pain, especially if cervical spine thrust manipulation is contraindicated or the patient is averse to cervical spine thrust manipulation. Future research should establish treat-ment parameters that include short- and long-term effects, as well as compare treatment effectiveness to interventions directed at the cervical spine. t
TABLE2
Comparison of Within-Group ROM Changes in the Thoracic Spine Thrust
Manipulation Groups to the CROM MDCs for Patients With Neck Pain
CervicalROM/Follow-up Within-GroupMeanDifference(95%CI) MDC9016
Cervical flexion 9.6°
3 wk18 12.4° (10.9°, 14.0°)
4 wk17 11.6° (10.0°, 13.2°)
5 wk18 11.2° (8.8°, 13.5°)
Cervical extension 7.0°
3 wk18 11.6° (10.3°, 13.6°)
4 wk17 11.2° (9.6°, 12.8°)
5 wk18 6.4° (4.3°, 9.1°)
Cervical right rotation 7.6°
Immediate29 8.2° (4.9°, 11.5°)
3 wk18 11.1° (9.1°, 12.3°)
4 wk17 9.8° (8.4°, 11.2°)
5 wk18 7.8° (5.4°, 9.7°)
Cervical left rotation 6.7°
Immediate29 7.1° (4.5°, 9.7°)
3 wk18 10.8° (9.3°, 12.4°)
4 wk17 8.9° (7.4°, 10.4°)
5 wk18 6.4° (3.9°, 8.3°)
Cervical right lateral flexion 5.9°
3 wk18 9.7° (9.1°, 11.6°)
4 wk17 11.1° (9.4°, 12.8°)
5 wk18 9.5° (8.4°, 11.5°)
Cervical left lateral flexion 9.1°
3 wk18 10.0° (8.3°, 11.7°)
4 wk17 9.4° (8.3°, 11.7°)
5 wk18 7.6° (5.6°, 9.7°)
Abbreviations: CI, confidence interval; CROM, cervical range of motion device; MDC, minimal detect-able change; ROM, range of motion.
41-09 Cross.indd 640 8/16/2011 6:28:40 PM

journal of orthopaedic & sports physical therapy | volume 41 | number 9 | september 2011 | 641
@ MORE INFORMATIONWWW.JOSPT.ORG
for management of mild cervical compressive myelopathy attributed to cervical herniated disc: a case series. J Orthop Sports Phys Ther. 2004;34:701-712.
2. Carlesso LC, Macdermid JC, Santaguida LP. Standardization of adverse event terminology and reporting in orthopaedic physical therapy: application to the cervical spine. J Orthop Sports Phys Ther. 2010;40:455-463. http://dx.doi.org/10.2519/jospt.2010.3229
3. Childs JD, Cleland JA, Elliott JM, et al. Neck pain: clinical practice guidelines linked to the International Classification of Functioning, Dis-ability, and Health from the Orthopedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38:A1-A34. http://dx.doi.org/10.2519/jospt.2008.0303
4. Childs JD, Flynn TW, Fritz JM, et al. Screening for vertebrobasilar insufficiency in patients with neck pain: manual therapy decision-making in the presence of uncertainty. J Orthop Sports Phys Ther. 2005;35:300-306. http://dx.doi.org/ 10.2519/jospt.2005.1312
5. Childs JD, Fritz JM, Piva SR, Whitman JM. Proposal of a classification system for patients with neck pain. J Orthop Sports Phys Ther. 2004;34:686-696; discussion 697-700.
6. Cleland JA, Childs JD, Fritz JM, Whitman JM, Eb-erhart SL. Development of a clinical prediction rule for guiding treatment of a subgroup of pa-tients with neck pain: use of thoracic spine ma-nipulation, exercise, and patient education. Phys Ther. 2007;87:9-23. http://dx.doi.org/10.2522/ptj.20060155
7. Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipu-lation in patients with neck pain: a randomized clinical trial. Man Ther. 2005;10:127-135. http://dx.doi.org/10.1016/j.math.2004.08.005
8. Cleland JA, Childs JD, Whitman JM. Psycho-metric properties of the Neck Disability Index and Numeric Pain Rating Scale in patients with mechanical neck pain. Arch Phys Med Rehabil. 2008;89:69-74. http://dx.doi.org/10.1016/j.apmr.2007.08.126
9. Cleland JA, Flynn TW, Childs JD, Eberhart S. The audible pop from thoracic spine thrust manipu-lation and its relation to short-term outcomes in patients with neck pain. J Man Manip Ther. 2007;15:143-154.
10. Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD. Short-term ef-fects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial. Phys Ther. 2007;87:431-440. http://dx.doi.org/10.2522/ptj.20060217
11. Cleland JA, Mintken PE, Carpenter K, et al. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: multi-center randomized clinical trial. Phys Ther. 2010;90:1239-1250. http://dx.doi.org/10.2522/ptj.20100123
12. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Law-rence Erlbaum Associates, Inc; 1988.
13. Costello M. Treatment of a patient with cervi-cal radiculopathy using thoracic spine thrust manipulation, soft tissue mobilization, and exercise. J Man Manip Ther. 2008;16:129-135.
14. Ernst E. Prospective investigations into the safety of spinal manipulation. J Pain Symptom Manage. 2001;21:238-242.
15. Fernandez-de-las-Penas C, Palomeque-del-Cerro L, Rodriguez-Blanco C, Gomez-Conesa A, Miangolarra-Page JC. Changes in neck pain and active range of motion after a single thoracic spine manipulation in subjects presenting with mechanical neck pain: a case series. J Manipu-lative Physiol Ther. 2007;30:312-320. http://dx.doi.org/10.1016/j.jmpt.2007.03.007
16. Fletcher JP, Bandy WD. Intrarater reliability of CROM measurement of cervical spine ac-tive range of motion in persons with and without neck pain. J Orthop Sports Phys Ther. 2008;38:640-645. http://dx.doi.org/10.2519/jospt.2008.2680
17. Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Alburquerque-Sendin F, Palomeque-del-Cerro L, Mendez-Sanchez R. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the man-agement of patients with acute mechanical neck pain: a randomized clinical trial. Man Ther. 2009;14:306-313. http://dx.doi.org/10.1016/j.math.2008.04.006
18. Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega Mdel R. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2009;39:20-27. http://dx.doi.org/10.2519/jospt.2009.2914
19. Haldeman S, Carroll L, Cassidy JD. Find-ings from the bone and joint decade 2000 to 2010 task force on neck pain and its as-sociated disorders. J Occup Environ Med. 2010;52:424-427. http://dx.doi.org/10.1097/JOM.0b013e3181d44f3b
20. Haldeman S, Kohlbeck FJ, McGregor M. Stroke, cerebral artery dissection, and cervi-cal spine manipulation therapy. J Neurol. 2002;249:1098-1104. http://dx.doi.org/10.1007/s00415-002-0783-4
21. Haldeman S, Kohlbeck FJ, McGregor M. Un-predictability of cerebrovascular ischemia associated with cervical spine manipulation therapy: a review of sixty-four cases after cervi-cal spine manipulation. Spine (Phila Pa 1976). 2002;27:49-55.
22. Hopkins WG, Marshall SW, Batterham AM, Hanin J. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc. 2009;41:3-13. http://dx.doi.org/10.1249/MSS.0b013e31818cb278
23. Hoving JL, Koes BW, de Vet HC, et al. Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain. A randomized, controlled trial. Ann Intern Med.
2002;136:713-722. 24. Hurley L, Yardley K, Gross AR, Hendry L,
McLaughlin L. A survey to examine attitudes and patterns of practice of physiotherapists who perform cervical spine manipulation. Man Ther. 2002;7:10-18. http://dx.doi.org/10.1054/math.2001.0430
25. Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Adverse reactions to chiropractic treatment and their effects on satisfaction and clinical outcomes among patients enrolled in the UCLA Neck Pain Study. J Manipulative Physiol Ther. 2004;27:16-25. http://dx.doi.org/10.1016/j.jmpt.2003.11.002
26. Jette AM, Smith K, Haley SM, Davis KD. Physical therapy episodes of care for patients with low back pain. Phys Ther. 1994;74:101-110; discus-sion 110-105.
27. Kerry R, Taylor AJ. Cervical arterial dysfunc-tion: knowledge and reasoning for manual physical therapists. J Orthop Sports Phys Ther. 2009;39:378-387. http://dx.doi.org/10.2519/jospt.2009.2926
28. Korthals-de Bos IB, Hoving JL, van Tulder MW, et al. Cost effectiveness of physiotherapy, manual therapy, and general practitioner care for neck pain: economic evaluation alongside a randomised controlled trial. BMJ. 2003;326:911. http://dx.doi.org/10.1136/bmj.326.7395.911
29. Krauss J, Creighton D, Ely JD, Podlewska-Ely J. The immediate effects of upper thoracic trans-latoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial. J Man Manip Ther. 2008;16:93-99.
30. MacDermid JC, Walton DM, Avery S, et al. Mea-surement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther. 2009;39:400-417. http://dx.doi.org/10.2519/jospt.2009.2930
31. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713-721.
32. Maigne J-Y. A Prevention of the Vertebrobasilar Accidents Following Cervical Thrust Manipula-tions: Recommandations of the SOFMMOO. Available at: http://www.sofmmoo.com/english_section/2_neck_pain/Cervical%20Manip.%20Recommandation%20SOFMMOO.htm. 2003.
33. Michaleff ZA, Costa LO, Moseley AM, et al. CENTRAL, PEDro, PubMed, and EMBASE are the most comprehensive databases indexing randomized controlled trials of physical therapy interventions. Phys Ther. 2011;91:190-197. http://dx.doi.org/10.2522/ptj.20100116
34. Miley ML, Wellik KE, Wingerchuk DM, Demaer-schalk BM. Does cervical manipulative therapy cause vertebral artery dissection and stroke? Neurologist. 2008;14:66-73. http://dx.doi.org/10.1097/NRL.0b013e318164e53d
35. Moher D, Liberati A, Tetzlaff J, Altman DG. Reprint--preferred reporting items for system-atic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89:873-880.
36. Parkin-Smith G, Penter C. A clinical trial investi-
41-09 Cross.indd 641 8/16/2011 6:28:41 PM

642 | september 2011 | volume 41 | number 9 | journal of orthopaedic & sports physical therapy
[ literature review ]
@ MORE INFORMATIONWWW.JOSPT.ORG
gating the effect of two manipulative approaches in the treatment of mechanical neck pain: a pilot study. J Neuromusc Syst. 1998;6:6-16.
37. Rivett D, Shirley D, Magarey M, Refshauge K. Clinical Guidelines for Assessing Vertebrobasilar Insufficiency in the Management of Cervical Spine Disorders. Available at: http://www.phys-iotherapy.asn.au/index.php/quality-practice/guidelines. Accessed November 1, 2010.
38. Rogers RG. The effects of spinal manipulation on cervical kinesthesia in patients with chronic neck pain: a pilot study. J Manipulative Physiol
Ther. 1997;20:80-85. 39. Savolainen A, Ahlberg J, Nummila H, Nis-
sinen M. Active or passive treatment for neck-shoulder pain in occupational health care? A randomized controlled trial. Occup Med (Lond). 2004;54:422-424. http://dx.doi.org/10.1093/occmed/kqh070
40. Sim J, Jordan K, Lewis M, Hill J, Hay EM, Dziedzic K. Sensitivity to change and internal consistency of the Northwick Park Neck Pain Questionnaire and derivation of a minimal clinically important difference. Clin J Pain.
2006;22:820-826. http://dx.doi.org/10.1097/01.ajp.0000210937.58439.39
41. Young BA, Walker MJ, Strunce JB, Boyles RE, Whitman JM, Childs JD. Responsiveness of the Neck Disability Index in patients with mechani-cal neck disorders. Spine J. 2009;9:802-808. http://dx.doi.org/10.1016/j.spinee.2009.06.002
PUBLISH Your Manuscript in a Journal With International Reach
JOSPT o�ers authors of accepted papers an international audience. TheJournal is currently distributed to the members of the followingorganizations as a member benefit:
• APTA's Orthopaedic and Sports Physical Therapy Sections• Sports Physiotherapy Australia (SPA) Titled Members• Physio Austria (PA) Sports Group• Belgische Vereniging van Manueel Therapeuten-Association Belge des Thérapeutes Manuels (BVMT-ABTM)• Comitê de Fisioterapia Esportiva do Estado do Rio de Janeiro (COFEERJ)• Mais Fisio• Canadian Physiotherapy Association (CPA) Orthopaedic Division• Sociedad Chilena de Kinesiologia del Deporte (SOKIDE)• Suomen Ortopedisen Manuaalisen Terapian Yhdistys ry (SOMTY)• German Federal Association of Manual Therapists (DFAMT)• Hellenic Scientific Society of Physiotherapy (HSSPT) Sports Injury Section• Chartered Physiotherapists in Sports and Exercise Medicine (CPSEM) and Chartered Physiotherapists in Manipulative Therapy (CPMT) of the Irish Society of Chartered Physiotherapists (ISCP)• Israeli Physiotherapy Society (IPTS)• Gruppo di Terapi Manuale (GTM), a special interest group of Associazione Italiana Fisioterapisti (AIFI)• New Zealand Sports and Orthopaedic Physiotherapy Association• Norwegian Sport Physiotherapy Group of the Norwegian Physiotherapist Association• Portuguese Sports Physiotherapy Group (PSPG) of the Portuguese Association of Physiotherapists• Singapore Physiotherapy Association (SPA)• Orthopaedic Manipulative Physiotherapy Group (OMPTG) of the South African Society of Physiotherapy (SASP)• Swiss Sports Physiotherapy Association (SSPA)• Association of Turkish Sports Physiotherapists (ATSP)
In addition, JOSPT reaches students and faculty, physical therapists andphysicians at more than 1,400 institutions in the United States and around the world. We invite you to review our Information for and Instructions to Authors at www.jospt.org and submit your manuscript for peer review at http://mc.manuscriptcentral.com/jospt.
41-09 Cross.indd 642 8/16/2011 6:28:42 PM

journal of orthopaedic & sports physical therapy | volume 41 | number 9 | september 2011 | 643
jospt perspectives for patients
Neck PainManipulating the Upper Back Helps
Lessen Pain and Improve Neck Motion
Neck pain is very common. In the United States, between 30% and 50% of people suffer from an aching neck each year. Although neck pain can be caused by in-jury, most of this pain results from more gradual stress-
es, such as particular sitting, standing, or work postures, lifting patterns, or sleeping positions. Typical neck pain can also cause headaches, pain between your shoulders, or a feeling of knots in your neck and upper back muscles. Although manual therapy,
sometimes called “manipulation,” is a common treatment for many types of spine pain, some people are uncomfortable hav-ing their necks manipulated. Recently, though, researchers have tested the benefits of a thrust manipulation of the upper back to treat neck pain. A study published in the September 2011 issue of JOSPT provides new insight and an evidence-based summary of the benefits of manipulating the upper back to ease and eliminate neck pain.
NEW INSIGHTS
In this study, the researchers evaluated published articles using a process called systematic review, which locates all relevant articles on a topic and selects those studies of the highest quality. Their initial search of the literature found 44 possible articles of interest. The researchers ultimately chose 6 high-quality articles that, when combined, included 187 patients who received upper back manipulation and were then compared to 173 patients who received another form of treatment. The research team found that performing upper back manipulations as part of the treatment resulted in less pain, increased neck motion, and improved function. These improvements were seen after the first treatment and continued up to 6 months after a 3-week treatment program that included several upper back manipulations.
Patients with typical neck pain may benefit from a physical therapy program that includes upper back manipulation. Potential benefits are less pain, better neck motion, and improved ability to perform daily activities. This type of manipulation is very safe and may help you feel better faster. In addition to upper back manipulation, physical therapy treatment may include exercises to help improve the strength and endurance of the muscles around your neck, decreasing your chance of feeling neck pain in the future. Your physical therapist can help determine if you are a good candidate for this treatment as part of a program designed to help get rid of the aching in your neck. For more information on the treatment of neck pain, contact your physical therapist specializing in musculoskeletal disorders.
This JOSPT Perspectives for Patients is based on an article by Cross KM et al, titled “Thoracic Spine Thrust Manipulation Improves Pain, Range of Motion, and Self-Reported Function in Patients With Mechanical Neck Pain: A Systematic Review” (J Orthop Sports Phys Ther 2011;41(9):633-642. doi:10.2519/jospt.2011.3670)
PRACTICAL ADVICE
JOSPT PERSPECTIVES FOR PATIENTS is a public service of the Journal of Orthopaedic & Sports Physical Therapy. The information and recommendations contained here are a summary of the referenced research article and are not a substitute for seeking proper healthcare to diagnose and treat this condition. For more information on the management of this condition, contact your physical therapist or healthcare provider specializing in musculoskeletal disorders. JOSPT Perspectives for Patients may be photocopied noncommercially by physical therapists and other healthcare providers to share with patients. Published by the Orthopaedic Section and the Sports Physical Therapy Section of the American Physical Therapy Association (APTA) and a recognized journal of professional organizations in several countries, JOSPT strives to offer high-quality research, immediately applicable clinical material, and useful supplemental information on musculoskeletal and sports-related rehabilitation, health, and wellness. Copyright © 2011
J Orthop Sports Phys Ther 2011;41(9):643. doi:10.2519/jospt.2011.0506
UPPER BACK THRUST MANIPULATION. The drawings above show how a therapist would manipulate your upper back while you are sitting and as you lie on your back.
For this and more topics, visit JOSPT Perspectives for Patients online at www.jospt.org.This Perspectives article was written by a team of JOSPT’s editorial board and staff, with Deydre S. Teyhen, PT, PhD, Editor, and Jeanne Robertson, Illustrator.
41-09 Perspectives.indd 643 8/16/2011 6:29:42 PM