Embed Size (px)
Citation preview

[Grab your reader’s attention with a great quote from the document or use this space to emphasize a key point. To place
this text box anywhere on the page, just drag it.]
County of Santa Barbara
Human Resources Department
One County. One Future.

3

4

6
*Per IRS rules, a portion of the covered travel expenses will be reported as taxable income to the employee. Due to
IRS regulations, on HSA plans the deductible applies but coinsurance is waived.

9

10

12

13
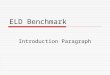
New Tandem EPO Plan This comparison chart shows a brief summary of medical benefits available.
Blue Shield Tandem EPO
How it Works You must use a Blue Shield in-network PPO contracted provider or your care will not be covered. There are no Out-of-Network benefits with these plans, except in the case of an emergency.
Medical Plan Annual Deductible Lifetime Maximum Annual Co-pay (Out-of-Pocket maximum)
$500 Individual/$1,000 Family Unlimited $3,000 Individual/$6,000 Family
Hospital Care Inpatient
- Physician - Facility Services
Carrum Health Outpatient Surgery Emergency Room Visit
- Not resulting in admission - Resulting in hospital admission
No Charge* $500/ Admission + 20%* No Charge $500/ Admission + 20%* $250 Co-pay (waived if admitted) $500/ Admission + 20%*
Physician Care Office Visit Specialist Visit Telemedicine Preventive Care/Annual Physical X-Ray. Lab & Pathology Services CT/PET scans, MRIs, MRAs Immunizations Outpatient Rehabilitation Therapy
- Physical, Speech, Occupational, Respiratory
Chiropractic Services Acupuncture Services
$25 Co-pay (not subject to deductible) $40 Co-pay (not subject to deductible) No Charge (Teladoc) No Charge (not subject to deductible) 20%* 20%* No Charge $25 Co-pay, 26 visits/yr (not subject to deductible) $15 Co-pay, 20 visits/yr, (not subject to deductible) $15 Co-pay, 20 visits/yr, (not subject to deductible)
Mental Health/Substance Abuse Inpatient - Mental Health Outpatient - Mental Health Chem. Dependency Rehab - Outpatient Detoxification - Inpatient (Detox Only)
$500/ Admission + 20%* $25/ visit (not subject to deductible) $25/ visit (not subject to deductible) $500/Admission + 20%*
Other Ambulance - ER or authorized transport Prosthetics Hearing Aid - max of $700 every 24 mths Durable Medical Equipment Home Healthcare Services Hospice
$50 per transport* 20%* No Charge* 20%* 20%* No Charge*

14
New Tandem EPO Plan Refer to the carrier Evidence of Coverage (EOC) for detailed information on the plan.
Blue Shield
Tandem EPOOther - Continued Pregnancy/Maternity Care Family Planning - Counseling - Tubal ligation - Vasectomy - Infertility Services (Diagnosis and treatment of causes only)
No Charge* No Charge No Charge $75 per Surgery* 50% of allowed charges*
Diabetes Care Devices and non-testing supplies Diabetes self-management training Rx’ n Go- device/test strips/lancets
20%* $25 Co-pay No Charge
Care Outside of Service Area (benefits provided by the BlueCard Program, for out-of-state emergency care, are provided at the preferred level of the local Blue Plan allowable amount when you use a Blue Cross/Blue Shield provider) · Within US: BlueCard Program · Outside US: BlueCard
Worldwide
See Applicable Benefit See Applicable Benefit
Express Scripts
Prescription Drugs Annual Deductible for Brand Only: $100 Ind / $300 Family***
Out-of-Pocket Maximum: $4,600 Ind / $9,200 Family
Retail: Generic/Brand/Non-formulary
$15 / $35/ $50 after annual deductible (30-day supply)
Mail Order: Generic/Brand/Non-formulary
$30 / $70 / $100 after annual deductible (90-day supply)
Specialty Medications
20% up to $100 max per script
Rx’n Go- Generic Maintenance Medications via Mail Order
$0 Co-pay for up to 90 day supply
* After annual deductible.
*** The Pharmacy Deductible does not apply to the Medical Deductible. Generic medications are not subject to the Pharmacy
Deductible.

15
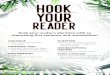
Blue Shield Medical Plans
This comparison chart shows a brief summary of the medical benefits available.
* After annual deductible.
**Chiropractic visits per year are combined with Outpatient Rehabilitation Therapy.
Blue Shield EPO Low Option
Blue Shield EPO High Option
How it Works You must use a Blue Shield in-network PPO contracted provider or your care will not be covered. There are no Out-of-Network benefits with these plans, except in the case of an emergency.
Medical Plan Annual Deductible Lifetime Maximum Annual Co-pay (Out-of-Pocket maximum)
$300 Individual/$600 Family Unlimited $2,000 Individual/$4,000 Family
None Unlimited $1,500 Individual/$3,000 Family
Hospital Care Inpatient
- Physician - Facility Services
Carrum Health Outpatient Surgery Emergency Room Visit
- Not resulting in admission - Resulting in hospital admission
No Charge* $500/ Admission + 20%* No Charge $500/ Admission + 20%* $250 Co-pay (waived if admitted) $500/ Admission + 20%*
No Charge* $300/ Admission + 20%* No Charge No Charge* $150 Co-pay (waived if admitted) $300/ Admission + 20%*
Physician Care Office Visit Specialist Visit Telemedicine Preventive Care/Annual Physical X-Ray. Lab & Pathology Services CT/PET scans, MRIs, MRAs Immunizations Outpatient Rehabilitation Therapy
- Physical, Speech, Occupational, Respiratory
Chiropractic Services Acupuncture Services
$25 Co-pay (not subject to deductible) $40 Co-pay (not subject to deductible) $25 Co-pay (Teladoc) No Charge (not subject to deductible) No Charge* No Charge* No Charge $25 Co-pay, 26 visits/yr (not subject to deductible) Not Covered Not Covered
$20 Co-pay (not subject to deductible) $30 Co-pay (not subject to deductible) $20 Co-pay (Teladoc) No Charge (not subject to deductible) No Charge* No Charge* No Charge $20 Co-pay, 26 visits/yr** (not subject to deductible) $20 Co-pay, 26 visits/yr** $20 Co-pay, 12 visits/yr
Mental Health/Substance Abuse Inpatient - Mental Health Outpatient - Mental Health Chem. Dependency Rehab - Outpatient Detoxification - Inpatient (Detox Only)
$500/ Admission + 20%* $25/ visit (not subject to deductible) $25/ visit (not subject to deductible) $500/Admission + 20%*
$300/ Admission + 20%* $20/ visit (not subject to deductible) $20/ visit (not subject to deductible) $300/ Admission + 20%*
Other Ambulance - ER or authorized transport Prosthetics Hearing Aid - max of $700 every 24 mths Durable Medical Equipment Home Healthcare Services Hospice
$50 per transport* 20%* No Charge* 20%* 20%* No Charge*
$50 per transport* No Charge* No Charge* No Charge* 20%* No Charge*

16
Blue Shield Medical Plans
Refer to the carrier Evidence of Coverage (EOC) for detailed information on the plan.
Blue Shield PPO
Blue Shield HDHP Plan (PPO)
You may see any provider when you need care. You decide whether to see an in-network or an out-of-network provider each time you need care. When you see in-network providers you typically pay less.
In-Network Out-of-Network In-Network Out-of-Network $750 Ind / $2,250 Family Unlimited $4,750 Ind/ $10,250 Family
$750 Ind / $2,250 Family Unlimited $6,750 / $14,250
$1,500/ $3,000 (combined)
Unlimited $4,500 / $9,000 (combined)
20%* $250/ Admission + 20%* No Charge 20%* $75/ visit + 20%* $250/ Admission + 20%*
40%* 40%* N/A 40%* $75/ visit + 20%* 40%*
20%* 20%* No Charge After Deductible 20%* 20%*(waived if admitted) 20%*
40%* 40%* N/A 40%* 20%*(waived if admitted) 40%*
$30 Co-pay $30 Co-pay $30 Co-pay (Teladoc) No Charge 20%* 20%* No Charge 20%*, 26 visits/ yr** 20%*, 26 visits/ yr** 20%*, 12 visits/ yr
40%* 40%* Not Covered 40%* 40%* 40%* 40%* 40%*, 26 visits/yr** Not Covered 20%*, 12 visits/ yr
20%* 20%* $40 (Teladoc) No Charge No Charge* No Charge* No Charge 20%*, 26 visits/ yr** 20%*, 26 visits/ yr** 20%*, 12 visits/ yr
40%* 40%* Not Covered 40%* 40%* 40%* 40%* Not Covered Not Covered 20%*, 12 visits/ yr
$250/ Admission + 20%* $30/ visit $30/ visit $250/ Admission + 20%*
40%* 40%* 40%* 40%*
20%* 20%* 20%* 20%*
40%* 40%* 40%* 40%*
20%* 20%* 20%* 20%* 20%* No Charge*
20%* 40%* 20%* 40%* Not Covered Not Covered
20%* 20%* 20%* 20%* 20%* No Charge*
20%* 40%* 20%* 40%* Not Covered Not Covered
Note for Out-of-Network benefits - you is responsible for the applicable copayment/coinsurance plus any amount that exceeds Blue
Shield’s allowable amount. For inpatient hospitalization, maximum allowed amount per day is $600/day. For outpatient
surgery/services, labs and x-rays, maximum allowed per day is $350 per day. For MRI/CT/PET scans, the max allowed per admit is $800.
Charges over the allowable amount do not count toward the calendar year deductible or out-of-pocket maximum.

17
Blue Shield Medical Plans This comparison chart shows a brief summary of the medical benefits available.
Blue Shield EPO
Low OptionBlue Shield EPO
High OptionOther - Continued Pregnancy/Maternity Care Family Planning - Counseling - Tubal ligation - Vasectomy - Infertility Services (Diagnosis and treatment of causes only)
No Charge* No Charge No Charge $75 per Surgery* 50% of allowed charges*
No Charge* No Charge No Charge $75 per Surgery* 50% of allowed charges*
Diabetes Care Devices and non-testing supplies Diabetes self-management training Rx’ n Go- device/test strips/lancets
20%* $25 Co-pay No Charge
No Charge* $20 Co-pay No Charge
Care Outside of Service Area (benefits provided by the BlueCard Program, for out-of-state emergency and non-emergency care, are provided at the preferred level of the local Blue Plan allowable amount when you use a Blue Cross/Blue Shield provider) · Within US: BlueCard Program · Outside US: BlueCard Worldwide
See Applicable Benefit See Applicable Benefit
See Applicable Benefit See Applicable Benefit
Express Scripts Express Scripts
Prescription Drugs Annual Deductible for Brand Only: $100 Ind / $300 Family***
Annual Deductible for Brand Only: $25 Ind / $75 Family***
Out-of-Pocket Maximum: $4,600 Ind / $9,200 Family
Out-of-Pocket Maximum: $5,100 Ind / $10,200 Family
Retail: Generic/Brand/Non-formulary
$15 / $35/ $50 after annual deductible (30-day supply)
$10 / $35/ $50 after annual deductible (30-day supply)
Mail Order: Generic/Brand/Non-formulary
$30 / $70 / $100 after annual deductible (90-day supply)
$20 / $70/ $100 after annual deductible (90-day supply)
Specialty Medications
20% up to $100 max per script 20% up to $100 max per script
Rx’n Go- Generic Maintenance Medications via Mail Order
$0 Co-pay for up to 90 day supply $0 Co-pay for up to 90 day supply
Pharmacy tip: Please read all mail from Express Scripts or Blue Shield since it will be a notice of a potential change to prescription drug(s) that you are currently taking. Find all benefit summaries at http://cosb.countyofsb.org/hr/. Please click on the “Employee Benefits” link.
* After annual deductible.
*** The Pharmacy Deductible does not apply to the Medical Deductible. Generic medications are not subject to the Pharmacy Deductible.

18
Blue Shield Medical Plans
Refer to the carrier Evidence of Coverage (EOC) for detailed information on the plan.
Blue Shield PPO Blue Shield HDHP Plan (PPO)
In-Network Out-of-Network In-Network Out-of-Network
20%* No Charge No Charge 20%* 50% of allowed charges*
40%* 40%* 40%* 40%* Not Covered
20%* No Charge No Charge 20%* 50% of allowed charges*
40%* 40%* 40%* 40%* Not Covered
20%* $30 Co-pay No Charge
40%* 40%* N/A
20%* 20%* No Charge
40%* 40%* N/A
See Applicable Benefit See Applicable Benefit
See Applicable Benefit See Applicable Benefit
See Applicable Benefit See Applicable Benefit
See Applicable Benefit See Applicable Benefit
Express Scripts Blue Shield
Annual Deductible for Brand Only: $25 Ind / $75 Family***
You must meet the annual deductible first before the noted co-insurance amounts apply.
Out-of-Pocket Maximum: $1,850 Ind / $2,950 Family
No Limit Medical and Pharmacy have a combined Out-of-Pocket Maximum
$10 / $35/ $50 after annual deductible ( 30-day supply)
$10 / $35/ $50 after annual deductible ( 30-day supply)
20%* ( 30-day supply)
20%* ( 30-day supply)
$20 / $70/ $100 after annual deductible ( 90-day supply)
Not Covered
20%* (90-day supply)
Not Covered
20% up to $100 max per script
Not Covered 20%* up to $100 max / script
Not Covered
$0 Co-pay for up to 90 days N/A $0 Co-pay for Preventive generic medications
N/A
Note for Out-of-Network benefits - you is responsible for the applicable copayment/coinsurance plus any amount that
exceeds Blue Shield’s allowable amount. For inpatient hospitalization, maximum allowed amount per day is $600/day. For
outpatient surgery/services, labs and x-rays, maximum allowed per day is $350 per day. For MRI/CT/PET scans, the max
allowed per admit is $800. Charges over the allowable amount do not count toward the calendar year deductible or out-of-
pocket maximum.

19
Kaiser Medical Plans
This comparison chart shows a brief summary of the medical benefits available.
Kaiser HMO Low Option
Kaiser HMO High Option
Medical Plan Annual Deductible Lifetime Maximum Annual Co-pay (Out-of-Pocket maximum)
None Unlimited $1,500 Individual/$3,000 Family
None Unlimited $1,500 Individual/$3,000 Family
Hospital Care Inpatient Surgery Outpatient Surgery Emergency Room Visit
- Not resulting in admission - Resulting in hospital admission
$500 per admission $20 Co-pay per procedure $100 Co-pay $500 hospital admission charge
$100 per admission $15 Co-pay per procedure $100 Co-pay $100 hospital admission charge
Physician Care Office Visit Specialist Visit Preventive Care/Annual Physical X-Ray. Lab & Pathology Services CT/PET scans, MRIs, MRAs Immunizations Chiropractic or Acupuncture Services
$20 Co-pay $20 Co-pay No Charge No Charge No Charge No Charge Not Covered
$15 Co-pay $15 Co-pay No Charge No Charge No Charge No Charge Not Covered
Mental Health/Substance Abuse Inpatient - Mental Health Outpatient - Mental Health Chem. Dependency Rehab - Outpatient Detoxification - Inpatient (Detox Only)
$500 per admission $20 Co-pay $20 Copay $500 per admission
$100 per admission $15 Co-pay $15 Co-pay $100 per admission
Other Ambulance Prosthetics Durable Medical Equipment Home Healthcare Services Hospice
$50 per transport No Charge No Charge No Charge (up to 100 visits) No Charge
$50 per transport No Charge No Charge No Charge (up to 100 visits) No Charge
Prescription Drugs Retail: Mail-Order:
$10 Co-pay Generic $35 Co-pay Brand No Non-Formulary Coverage (30-day supply) $20 Co-pay Generic $70 Co-pay Brand No Non-Formulary Coverage (100-day supply) Specialty: 20% up to $150 max per script
$10 Co-pay Generic $30 Co-pay Brand No Non-Formulary Coverage (30-day supply) $20 Co-pay Generic $65 Co-pay Brand No Non-Formulary Coverage (100-day supply) Specialty: 20% up to $150 max per script

22
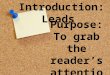
USING YOUR VSP BENEFIT IS EASY
Find a VSP doctor or print and ID card at www.vsp.com .
At your appointment, tell them you have VSP, no ID card is necessary.
Create an account online to review your benefits.

23
Medical
Premium County
Contribution Pre-Tax
Deductions*
Blue Shield Tandem EPO Medical Plan
Employee Only 403.89 (403.89) 0.00
With 1 Dependent 744.89 (403.89) 341.00
Two + Dependents 1169.39 (403.89) 765.50
Blue Shield Low Option EPO Medical Plan
Employee Only 427.39 (427.39) 0.00
With 1 Dependent 788.39 (427.39) 361.00
Two + Dependents 1237.89 (427.39) 810.50
Blue Shield High Option EPO Medical Plan
Employee Only 494.89 (427.39) 67.50
With 1 Dependent 914.39 (427.39) 487.00
Two + Dependents 1434.39 (427.39) 1007.00
Blue Shield PPO Medical Plan
Employee Only 651.39 (427.39) 224.00
With 1 Dependent 1202.89 (427.39) 775.50
Two + Dependents 1889.89 (427.39) 1462.50
Blue Shield HDHP Medical Plan
Employee Only 373.71 (373.71) 0.00
With 1 Dependent 667.21 (373.71) 293.50
Two + Dependents 1047.21 (373.71) 673.50
Kaiser Low Option Medical Plan**
Employee Only 313.89 (313.89) 0.00
With 1 Dependent 588.39 (313.89) 274.50
Two + Dependents 892.89 (313.89) 579.00

24
Medical
Premium County
Contribution Pre-Tax
Deductions*
Kaiser High Option Medical Plan**
Employee Only 326.39 (326.39) 0.00
With 1 Dependent 609.39 (326.39) 283.00
Two + Dependents 925.89 (326.39) 599.50
Dental Premium
County Contribution
Pre-Tax Deductions*
Delta Dental DHMO Dental Plan
Employee Only 16.44 (13.03) 3.41
With 1 Dependent 27.02 (13.03) 13.99
Two + Dependents 41.02 (13.03) 27.99
Delta Dental DPPO – County Self-Funded Dental Plan
Employee Only 16.61 (13.03) 3.58
With 1 Dependent 27.72 (13.03) 14.69
Two + Dependents 42.43 (13.03) 29.40
Vision Premium
County Contribution
Pre-Tax Deductions*
VSP Vision Plan
Employee Only 3.18 N/A 3.18
With 1 Dependent 4.57 N/A 4.57
Two + Dependents 8.20 N/A 8.20

25

26

28

29
“Your current
balance is
$50.”

30

31
.
BENEFICIARY REMINDER
Beneficiary means a person you name to receive death benefits.
You may name one or more beneficiaries. Make sure that you
have named a beneficiary for your basic life insurance. You may
change your beneficiary at any time. Note that some states
require a spouse be named as a beneficiary unless they sign a
waiver. Remember that a divorce or separation will not
automatically affect a beneficiary designation, so please review
you beneficiary election(s) to ensure it accurately reflects your
wishes.

32
.

33

34

35
Click on the icon to view a video
on “How To File A Claim”.

38

39
*Note: Due to IRS guidelines on the HDHP, only preventive maintenance medications are available to you for free. Rx’n GO has over 750 preventative medications on their drug list.

40
T

41

43

44

45
Benefit Terms Explained How to read an EOB
High Deductible Health Plan w/ HSA What is an FSA
HSA vs FSA EAP
Qualifying Events Preventive Care

46

47

48

49

50

51
Employee Benefits Brochure designed and developed by