Embed Size (px)
Citation preview
Clinical Gastroenterology and Hepatology 2014;12:1046–1050
BRIEF COMMUNICATIONS
Therapy-Associated Polyposis as a Late Sequela ofCancer Treatment
Matthew B. Yurgelun,*,‡ Jason L. Hornick,§ Victoriana K. Curry,* Chinedu I. Ukaegbu,*Emily K. Brown,* Elaine Hiller,* Anu Chittenden,* Joel E. Goldberg,k and Sapna Syngal‡
*Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts; ‡Department of Medicine,§Department of Pathology, and kDepartment of Surgery, Brigham and Women’s Hospital and Harvard Medical School,Boston, Massachusetts
Abbreviations used in this paper: APC, adenomatous polyposis coli; AFAP,attenuated familial adenomatous polyposis; EGD, esophagogas-troduodenoscopy; FAP, familial adenomatous polyposis; MUTYH, MutYhomolog; TAP, therapy-associated polyposis.
© 2014 by the AGA Institute1542-3565/$36.00
http://dx.doi.org/10.1016/j.cgh.2013.11.040
Survivors of childhood cancers are at increased risk ofdeveloping secondary gastrointestinal cancers, includingcolorectal cancer, later in life, possibly from exposure toabdominopelvic radiotherapy and/or alkylating chemo-therapy. Profuse gastrointestinal polyposis is associatedwith rare, inherited colorectal cancer predispositionsyndromes, most commonly caused by mutations in theadenomatous polyposis coli (APC) or mutY homolog(MUTYH) genes. We describe 5 patients who developedgastrointestinal polyposis many years after radiotherapyand chemotherapy for a childhood cancer. Genetic analysisof all 5 subjects did not identify pathogenic germline mu-tations in APC or MUTYH. Chemotherapy and/or radio-therapy therefore might cause gastrointestinal polyposis insome patients by undiscovered mechanisms.
Keywords: Polyps; Radiation; Adenomas; Chemotherapy.
Childhood cancer survivors are at increased risk forsecondary gastrointestinal cancers, including
colorectal cancer, later in life.1–6 Although the pathogenicmechanisms remain poorly understood, various studieshave suggested an association with alkylating chemo-therapy and/or abdominopelvic radiotherapy exposure.1–4
Because of this increased risk, the Children’s OncologyGroup recommends that childhood cancer survivorsexposed to at least 30 Gy of abdominal radiotherapy un-dergo screening colonoscopy every 5 years beginning atage 35, or 10 years after radiation exposure.7
Gastrointestinal polyposis is the primary manifesta-tion of various rare, high-penetrance hereditary colorectalcancer syndromes, most notably familial adenomatouspolyposis (FAP), attenuated FAP (AFAP), MutY homolog(MUTYH)–associated polyposis, and the hamartomatouspolyposis syndromes. Although many patients undergo-ing genetic evaluation for hereditary polyposis syn-dromes are not identified to have germline mutations,8,9
there are virtually no known forms of acquired gastroin-testinal polyposis. Other loosely described forms of he-reditary polyposis include serrated polyposis and mixedpolyposis, although their genetic basis remainsundefined.10–14
We present 5 cases of nonfamilial gastrointestinalpolyposis occurring many years after chemotherapy and
radiotherapy for childhood cancer. None of the patientscarry detectable adenomatous polyposis coli (APC) orMUTYH mutations. We hypothesize that alkylatingchemotherapy and/or radiation exposure may be anunrecognized risk factor for acquired gastrointestinalpolyposis.
Methods
All 5 subjects were referred to the Dana-FarberCancer Institute’s Cancer Genetics and PreventionProgram for clinical evaluation of possible familialpolyposis, based on their personal history of gastro-intestinal polyposis. All subjects or their legal guard-ians provided informed consent to participate in aninstitutional review board–approved institutionalresearch registry developed for the purposes ofinvestigating possible genetic and biologic factors thatcontribute to cancer risk. As part of this protocol,subjects were asked to provide an optional one-timeblood sample.
Clinical information, including sex, age, and medicaland family histories were obtained from medical recordsdeveloped as part of the subjects’ routine clinical care. Allgastrointestinal polyp information was obtained fromavailable medical records, including official pathologyreports, endoscopy reports, and surgical notes issued aspart of the subjects’ routine medical care. A gastroin-testinal pathologist (J.L.H.) reviewed all available andrelevant gastrointestinal pathology specimens to confirmthe histologic classification. All subjects underwentcomprehensive germline testing with full sequencing andlarge rearrangement analysis of the APC gene and fullsequencing of the MUTYH gene by a commercial labo-ratory (Myriad Genetics Laboratories, Inc, Salt Lake City,
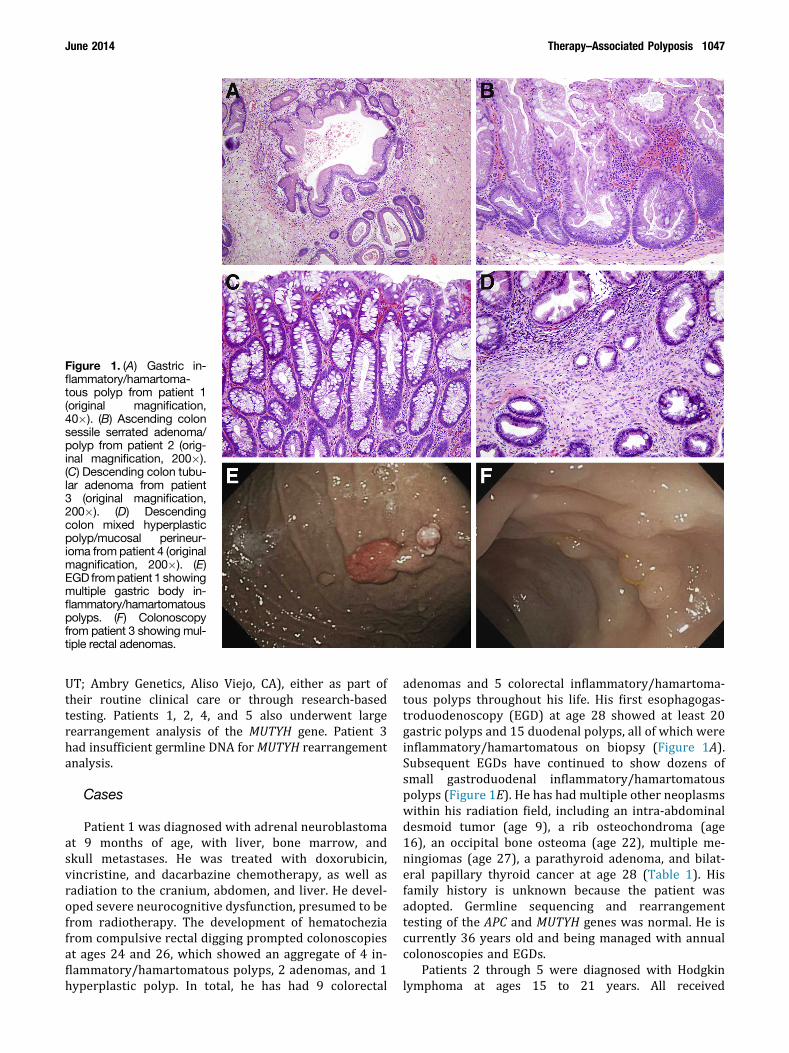
Figure 1. (A) Gastric in-flammatory/hamartoma-tous polyp from patient 1(original magnification,40�). (B) Ascending colonsessile serrated adenoma/polyp from patient 2 (orig-inal magnification, 200�).(C) Descending colon tubu-lar adenoma from patient3 (original magnification,200�). (D) Descendingcolon mixed hyperplasticpolyp/mucosal perineur-ioma from patient 4 (originalmagnification, 200�). (E)EGD frompatient 1 showingmultiple gastric body in-flammatory/hamartomatouspolyps. (F) Colonoscopyfrom patient 3 showing mul-tiple rectal adenomas.
June 2014 Therapy–Associated Polyposis 1047
UT; Ambry Genetics, Aliso Viejo, CA), either as part oftheir routine clinical care or through research-basedtesting. Patients 1, 2, 4, and 5 also underwent largerearrangement analysis of the MUTYH gene. Patient 3had insufficient germline DNA for MUTYH rearrangementanalysis.
Cases
Patient 1 was diagnosed with adrenal neuroblastomaat 9 months of age, with liver, bone marrow, andskull metastases. He was treated with doxorubicin,vincristine, and dacarbazine chemotherapy, as well asradiation to the cranium, abdomen, and liver. He devel-oped severe neurocognitive dysfunction, presumed to befrom radiotherapy. The development of hematocheziafrom compulsive rectal digging prompted colonoscopiesat ages 24 and 26, which showed an aggregate of 4 in-flammatory/hamartomatous polyps, 2 adenomas, and 1hyperplastic polyp. In total, he has had 9 colorectal
adenomas and 5 colorectal inflammatory/hamartoma-tous polyps throughout his life. His first esophagogas-troduodenoscopy (EGD) at age 28 showed at least 20gastric polyps and 15 duodenal polyps, all of which wereinflammatory/hamartomatous on biopsy (Figure 1A).Subsequent EGDs have continued to show dozens ofsmall gastroduodenal inflammatory/hamartomatouspolyps (Figure 1E). He has had multiple other neoplasmswithin his radiation field, including an intra-abdominaldesmoid tumor (age 9), a rib osteochondroma (age16), an occipital bone osteoma (age 22), multiple me-ningiomas (age 27), a parathyroid adenoma, and bilat-eral papillary thyroid cancer at age 28 (Table 1). Hisfamily history is unknown because the patient wasadopted. Germline sequencing and rearrangementtesting of the APC and MUTYH genes was normal. He iscurrently 36 years old and being managed with annualcolonoscopies and EGDs.
Patients 2 through 5 were diagnosed with Hodgkinlymphoma at ages 15 to 21 years. All received

Table 1.Gastrointestinal Polyposis and Other Clinical Characteristics in 5 Survivors of Childhood Cancer
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5
Sex Male Female Female Male FemaleOriginal cancer/
stageMetastatic
neuroblastomaStage IIIA Hodgkin
lymphomaStage IIB Hodgkin
lymphomaStage IIA Hodgkin
lymphomaStage IIA Hodgkin
lymphomaAge at original
cancer9 mo 21 y 15 y 18 y (para-aortic
relapse at age 20)16 y
Chemotherapy Doxorubicin,vincristine,dacarbazine
MOPP MOPP MOPP (age 20) MOPP
Sites of radiationtherapy
Cranium, abdomen,liver
Mantle, para-aorticnodes
Mantle, para-aorticnodes
Mantle (age 18); para-aortic, iliac, inguinalnodes (age 20)
Mantle, axilla, para-aortic, pelviclymph nodes
Age at recognitionof first polyp, y
24 47 43 33 51
Latency betweenchemoradiationand recognitionof polyposis, y
22 26 28 13 35
Primary polypmanifestation
Gastroduodenalhamartomas
Colorectal sessileserrated polyps
Colorectal adenomas Colorectal adenomas Colorectal sessileserrated polyps
Other GI neoplasia Multiple colorectaladenomas andhamartomas
Multiple colorectaladenomas andhyperplasticpolyps, Barrett’sesophagus
Multiple colorectalsessile serrated andhyperplastic polyps,multiple fundicgland polyps
Multiple colorectalmixed hyperplasticpolyp/mucosalperineuriomas,multiple fundicgland polyps
Multiple fundic glandpolyps
Family history Adopted/unknown No known GI cancers;mother with <10lifetime colorectalpolyps
No known GI cancers;2 siblings each with<5 colorectalpolyps
Adopted/unknown No known GI cancersor polyps
Currentmanagement ofpolyposis
Annual EGD andcolonoscopy
Annual colonoscopy Annual colonoscopy Annual colonoscopy Status-post totalproctocolectomy
Other neoplasia Retroperitonealdesmoid tumor(age 9), occipitalosteoma (age 22),papillary thyroidcancer (age 28),multiplemeningiomas,parathyroidadenoma
Invasive ductal breastcancer (age 32),extra-abdominaldesmoid tumor(age 44)
Papillary thyroid cancer(age 32), unilateralinvasive breastcancer and bilateralDCIS (age 40)
None None
Non-neoplasticmedical historysincechemoradiation
Cognitive/behavioraldeficits,osteopoikilosis
High-grade heartblock requiringpacemaker
Pneumonitis, earlyonset coronaryartery disease,aortic stenosis,cardiomyopathy
None Hypothyroidism,cardiomyopathy
DCIS, ductal carcinoma in situ; GI, gastrointestinal; MOPP, mechlorethamine, vincristine, procarbazine, prednisone.
1048 Yurgelun et al Clinical Gastroenterology and Hepatology Vol. 12, No. 6
mechlorethamine, vincristine, procarbazine, and predni-sone chemotherapy and radiotherapy to the mantle andpara-aortic lymph nodes (Table 1). All were foundto have colorectal polyposis on their first screeningcolonoscopies: patient 2 had more than 30 to 40 sessileserrated adenomas/polyps (Figure 1B); patient 3 hadapproximately 40 adenomas (Figure 1C); patient 4 hadapproximately 50 polyps that were a mix of adenomas,inflammatory polyps, and mixed hyperplastic polyps/mucosal perineuriomas (Figure 1D); and patient 5 hadmany flat, carpet-like sessile serrated adenomas/polypsthroughout the entire colorectum. All 4 patients have had
continued polyp formation on follow-up colonoscopies(Figure 1F). Three patients had multiple fundic glandpolyps on EGD, 1 patient had a chest wall desmoid tumorin her prior radiation field (age 44), and 1 patient hadpapillary thyroid cancer (age 32). Three of these patientsare being managed by annual endoscopic surveillanceand the fourth patient underwent total proctocolectomy.Table 1 provides further information regarding otherneoplastic and non-neoplastic findings in these patients.Genetic testing of patients 2 through 5 showed nogermline abnormalities in either the APC or MUTYHgenes.

June 2014 Therapy–Associated Polyposis 1049
Discussion
This report brings to light a potentially novel etio-logy of acquired gastrointestinal polyposis, which wehypothesize to be therapy-associated polyposis (TAP).These 5 patients were recognized to have gastrointes-tinal polyposis at a mean of 24.8 years (range, 13–35 y)after exposure to alkylating chemotherapy and abdom-inal radiotherapy for a childhood cancer. Intriguingly,1 patient showed predominantly upper gastrointestinalinflammatory/hamartomatous polyposis, 2 patientsfulfilled the 2010 World Health Organization clinicalcriteria for serrated polyposis syndrome,14 and 2 patientsshowed a phenotype of AFAP (defined as 20–99 lifetimecolorectal adenomas), suggesting potentially differentmechanisms of neoplasia. This study generates thehypothesis of an association between chemoradiotherapyexposure and the development of acquired gastrointes-tinal polyposis.
We recognize that the small number of patients andtheir heterogeneous phenotypes are significant limita-tions to this report, and we clearly cannot claim anydefinitive causality between chemoradiotherapy and ourpatients’ polyposis. Despite such limitations, however,we believe that these patients’ striking phenotypes raisean important and biologically plausible hypothesis ofan association between their polyposis and chemo-radiotherapy exposure, which itself generates intriguingquestions and theories about the pathophysiology ofacquired polyposis and of therapy-related toxicities.There are, for example, multiple reports linking chemo-therapy and radiotherapy exposure to the risk of sub-sequent colorectal and gastric cancers,1,2 prompting thehypothesis that gastrointestinal epithelium can beinduced to undergo accelerated neoplasia. The mecha-nisms underlying such neoplasia are speculative, butmay involve abnormalities in Wnt signaling. TheAPCMin/þ mouse is a well-studied animal model of FAP inwhich mice carrying a truncating APC mutation showrapid multifocal colorectal neoplasia caused by un-checked Wnt signaling activation. Intriguingly, priorwork has shown that radiation exposure increases theburden of intestinal tumor development in APCMin/þ
mice in a dose-dependent manner, possibly throughadditional downstream effects on Wnt signaling.15
All 5 patients showed extracolonic features associ-ated with FAP within their radiation fields, including3 patients with fundic gland polyps, 2 patients withdesmoid tumors, 2 patients with papillary thyroid can-cer, and 1 patient with an osteoma (Table 1), whichraises the question as to whether these subjects simplycould have unrecognized FAP/AFAP. We acknowledgethat our data do not eliminate the possibility of one ormore of these subjects having FAP/AFAP from an un-identifiable germline mutation, although their mixedpolyp histologies are inconsistent with classically definedFAP/AFAP with underlying germline APC mutations.
This illustrates a common problem in the clinicalevaluation of patients with moderate degrees of polyp-osis, in which most patients are not identified to havegermline APC or MUTYH mutations.8 In such situations,counseling recommendations for patients and theirfamily members usually rely on the assumption that thepolyposis is hereditary, although our intent in presentingthis series is to raise the hypothesis of the existence,in a subset of such patients, of an acquired form ofpolyposis.
Curiously, 4 patients experienced significant toxicitiesbeyond these FAP-like manifestations, presumably alsorelated to chemoradiation: 3 patients have young-onsetcardiovascular disease, 1 patient has severe neuro-cognitive deficits, and 2 patients had young-onset breastcancer. These findings raise speculation that such patientsmay have a systemic predisposition to chemotherapyand/or radiotherapy toxicities beyond their gastrointes-tinal epithelium.
To summarize, we present 5 cases of therapy-associated polyposis occurring many years after expo-sure to alkylating chemotherapy and radiotherapy for achildhood cancer. All 5 patients display extracolonicfeatures mimicking FAP/AFAP, although none have afamily history or genetic testing results suggesting aninherited syndrome. Our data are insufficient to deter-mine the optimal management of patients with TAP. Thefact that none of these patients have had a gastrointes-tinal malignancy and that 4 patients are being managedwith aggressive endoscopic surveillance, however,suggests that some TAP patients may be able to avoidprophylactic colectomy, which is considered to be astandard risk-reducing intervention for FAP patients.Furthermore, family members of TAP patients may bereassured that the predisposition to polyps may not behereditary. These findings and proposed hypothesesshould be studied in larger cohorts of childhood cancersurvivors to better understand the prevalence, patho-physiology, and management of TAP.
References
1. Nottage K, McFarlane J, Krasin MJ, et al. Secondary colorectalcarcinoma after childhood cancer. J Clin Oncol 2012;30:2552–2558.
2. Morton LM, Dores GM, Curtis RE, et al. Stomach cancer riskafter treatment for Hodgkin lymphoma. J Clin Oncol 2013;31:3369–3377.
3. Henderson TO, Oeffinger KC, Whitton J, et al. Secondarygastrointestinal cancer in childhood cancer survivors: a cohortstudy. Ann Intern Med 2012;156:757–766.
4. Swerdlow AJ, Barber JA, Hudson GV, et al. Risk of secondmalignancy after Hodgkin’s disease in a collaborative Britishcohort: the relation to age at treatment. J Clin Oncol 2000;18:498–509.
5. Reulen RC, Frobisher C, Winter DL, et al. Long-term risks ofsubsequent primary neoplasms among survivors of childhoodcancer. JAMA 2011;305:2311–2319.
6. van Leeuwen FE, Klokman WJ, Veer MB, et al. Long-term risk ofsecond malignancy in survivors of Hodgkin’s disease treated

1050 Yurgelun et al Clinical Gastroenterology and Hepatology Vol. 12, No. 6
during adolescence or young adulthood. J Clin Oncol 2000;18:487–497.
7. Children’s Oncology Group. Long-term follow-up guide-lines for survivors of childhood, adolescent, and young adultcancer. Version 3.0. Available at: http://www.survivorshipguidelines.org/pdf/LTFUGuidelines.pdf. Accessed June 19,2013.
8. Grover S, Kastrinos F, Steyerberg EW, et al. Prevalence andphenotypes of APC and MUTYH mutations in patients withmultiple colorectal adenomas. JAMA 2012;308:485–492.
9. Mongin C, Coulet F, Lefevre JH, et al. Unexplained polyposis: achallenge for geneticists, pathologists and gastroenterologists.Clin Genet 2012;81:38–46.
10. Lanspa SJ, Ahnen DJ, Lynch HT. Serrated polyposis: the last (oronly the latest?) frontier of familial polyposis? Am J Gastro-enterol 2012;107:779–781.
11. Cheah PY, Wong YH, Chau YP, et al. Germline bone morpho-genesis protein receptor 1A mutation causes colorectal tumor-igenesis in hereditary mixed polyposis syndrome. Am JGastroenterol 2009;104:3027–3033.
12. Boparai KS, Dekker E, Van Eeden S, et al. Hyperplastic po-lyps and sessile serrated adenomas as a phenotypic expres-sion of MYH-associated polyposis. Gastroenterology 2008;135:2014–2018.
13. Vogt S, Jones N, Christian D, et al. Expanded extracolonic tumorspectrum in MUTYH-associated polyposis. Gastroenterology2009;137:1976–1985.
14. Rex DK, Ahnen DJ, Baron JA, et al. Serrated lesions of thecolorectum: review and recommendations from an expert panel.Am J Gastroenterol 2012;107:1315–1329.
15. Ellender M, Harrison JD, Meijne E, et al. Intestinal tumoursinduced in Apc(Min/þ) mice by X-rays and neutrons. Int J RadiatBiol 2011;87:385–399.
Reprint requestsAddress requests for reprints to: Matthew B. Yurgelun, MD, Department ofMedical Oncology, Gastrointestinal Cancer Center, Dana-Farber Cancer Insti-tute, 450 Brookline Avenue, Boston, Massachusetts 02215. e-mail:[email protected]; fax: (617) 632-5370.
AcknowledgmentsAn abstract of this work was presented as a poster at the 15th Annual Meetingof the Collaborative Group of the Americas on Inherited Colorectal Cancer,October 27–29, 2012, Boston, MA.
Conflicts of interestThe authors disclose no conflicts.
FundingSupported by the National Institutes of Health (National Cancer Institute)(K24CA113433 to S.S.).