Embed Size (px)
Citation preview

Therapies in the treatment of Type II diabetesDr. S.A. Bhana
Chris Hani Baragwanath Academic Hospital; University of the Witwatersrand


Type 2 diabetes prevalence by region
Amos et al. 1997
Africa
Asia
North America
Latin America
0 10 20 30 40
Type 2 diabetes prevalence (millions)
50 60 70
Europe
Oceania

Growth of Type 2 diabetes
Amos et al. 1997
Africa
Asia
North America
Latin America
0 20 40 60 80
Increase in Type 2 diabetes prevalence 1997–2010 (%)
100 120
Europe
Oceania

Insulin Resistance: An Inherent Metabolic Abnormality of Type 2 Diabetes and CVD
Increased Free Fatty
Acids
Increased Glucose
Production
Visceral Obesity
Atherosclerosis
Insulin Resistance
Hyperinsulinemia
Type 2 Diabetes
Inflammation (CRP)
Endothelial Dysfunction
Hypertension
Impaired Fibrinolysis (PAI-1)
Dyslipidemia(HDL, sdLDL, TG)
EnvironmentGenes

UKPDS: ß-Cell Function for Patients Remaining on Diet for 6 Years
Adapted from UKPDS Group (UKPDS 16). Diabetes. 1995;44:1249-1258.
0
20
40
60
80
100
-10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6
Years After Diagnosis
-C
ell F
unction (
%
)
N=376

Ins
ulin
Se
cre
tio
n
AIR
(µ
U/m
L)
IGT
NGT
NGTNGT NGT
DIA
500
400
300
200
100
0
Insulin Sensitivity
M-low (mg/kg EMBS per minute)
Progressors
Non-Progressors
Early Insulin Secretion DecreasesWith Progression to Diabetes
Weyer C, et al. J Clin Invest. 1999;104:787–794.
1 2 3 4 5

Case scenario 1• 44 year old female with features of
metabolic syndrome. (HTN, BMI =40)
• Currently on Metformin 850mg TDS and HbA1c is >10%.
• What other information would you need prior to escalating therapy?
• What is the next best step in terms of her therapy?

T2DM treatment strategies revisited
Target-driven therapy*
Adapted from Riddle M. Endo Metab Clin NA 1997;26:659―77.
Riddle M. Am J Med 2004;116:35―95.*Individualise
STEP 1
STEP 2
STEP 4
OHA monotherapy
OHA combinations
STEP 3
Lifestyle modification
Basal insulin
Basal plus prandial

SEMDSA 2012 Algorithm


Case scenario 1• 44 year old female with features of
metabolic syndrome. (HTN, BMI =40)
• Currently on Metformin 850mg TDS and HbA1c is >10%.
• What other information would you need prior to escalating therapy?
• What is the next best step in terms of her therapy?

Case scenario 2
• 38 year old T2DM presents with established renal failure requiring dialysis and proliferative retinopathy. Her treatment includes Metformin 850mg TDS and Sulphonylurea 80mg BD. HbA1C is 8%
• What would you do next?

SGLT2 inhibitors
Metformin

Introduction
• T2DM is a poorly managed disease with fewer than 50% of pts achieving glycaemic targets.
• A uniform therapeutic approach will not be appropriate for a disease that presents with great diversity in pts
• Ideally we need to match these diverse profiles with various therapeutic options whilst still maintaining a systematic and logical approach

Optimal management
• Ongoing patient education
• Lifestyle intervention at each step
• Control glycaemia (pre- and post-prandial)• Avoidance of hypoglycemia
• Avoidance of weight gain
• Individualize therapy
• Control all CVS risk factors

Hypoglycemia
Weight gain
CVS risk
Decrease compliance
Microvascularcomplications
Challenges

Complications in Type 2 diabetes
Turner et al. 1996
01
10
20
30
40
Pa
tie
nts
wit
h e
ve
nt
(%) All diabetes-related events
Macrovascular complications
2 3 4 5 6 7 98
Time from randomisation (years)
0
Microvascular complications

Lifestyle measures
• Diet
• Weight loss
• Stop smoking
• Ongoing counseling

Goals of therapy
•HbA1C < 7%, higher if underlying CVS risk
•Glucose pre-prandial: 4-7 mmol/L
•Glucose post-prandial 4-8mmol/L
•Prevention of target organ damage

Good Glycaemic Control Reduces Incidence of Complications: Data From Landmark Trials
HbA1C
DCCT1
9%7%
Kumamot
9%7%UKPDS
3
9%7%
Retinopathy (%) 63 69 21
Nephropathy (%) 54 70 34
Neuropathy (%) 60 – –
Macrovascular disease (%) 41 – 16

The Ominous Octet
Islet -cell
Impaired
Insulin Secretion
Neurotransmitter
Dysfunction
Decreased Glucose
Uptake
Islet a-cell
Increased
Glucagon Secretion
IncreasedLipolysis
Increased Glucose
Reabsorption
Increased
HGP
DecreasedIncretin Effect

SulfonylureasGlinidesInsulin
Incretins
MetforminTZD
SGLT2 inhibitors
Metformin
MetforminInsulins
Incretins
GLP 1 analoguesAmylin mimmetics
‘OMINOUS OCTET’

Special considerations in drug selection
• Age
• Weight
• Comorbidities
• Hypoglycemia prone
• Impaired cardiac, renal and liver function

Comparison of 24-hour glucose levels in control subjects vs patients with diabetes (p<0.001).
Adapted from Polonsky K, et al. N Engl J Med 1988;318:1231―9.
Time of day (hours)
400
300
200
100
0
6 610 14 18 22 2
Pla
sma g
lucose
(m
g/dl)
Normal
Meal Meal Meal
20
15
10
5
0
Pla
sma g
lucose
(mm
ol/
l)
Treating fasting hyperglycaemia lowers the entire 24-hour plasma glucose profile
Hyperglycaemia due to an increase in fasting glucose
T2DM

Oral agents

Classes of oral agents
• Biguinides- Metformin
• Sulphonylureas- Gliclazide, Glibenclamide
• PPAR γ agonists- Rosiglitazone
• α glucosidase inhibitors- acarbose
• Glinides- nateglinide
• DPP4 inhibitors- ‘gliptins’
• SGLT2 inhibitors- Canagliflozin

Injectables

Injectables
• GLP 1 analogues- Exenatide, Liraglutide
• Insulins• Short acting
• Intermediate acting
• Long acting
• Ultra-long acting

Step 1:
First lineMetformin monotherapy
Advantages Disadvantages
Low cost GIT side effects
HbA1C 1.5% Limited durability
Low risk hypoglycemia
Modest weight loss

Step 2:
Met
form
in Sulphonylureas
Incretin
Basal insulin

Sulfonylureas
Advantages Disadvantages
Low cost Hypoglycemia
Long clinical experience Limited durability
HbA1C 1-2% Weight gain
Possible CVS risk

Incretins
• GIT hormones secreted from the entero-endocrine cells
• GIP and GLP-1
• Action: potentiates insulin secretion (glucose dependent)
• Delays gastric emptying
• Satiety
• Degraded by DPP-4 enzyme


Incretins
DPP4 inhibitors
•‘gliptins’
GLP1 analogues
•Liraglutide and exenatide

DPP4 inhibitors GLP 1 analogues
Effect on HbA1C HbA1c 0.5-1% HbA1c 1%
Advantages Weight neutral Weight loss
Low risk hypoglycemia No hypoglycemia
Improves post prandial control
Improves pre- and post-prandial glucose
Disadvantages Some cases ofpancreatitis
Some cases ofpancreatitis
safety dataNo Harm
? Medullary Ca
safety data“Leader” Better then Std.
Injectable

Step 3:
• SU
• Basal insulinMetformin
• SU
• IncretinMetformin
• SU
• Acarbose/SGLT 2Metformin

Normal renal glucose handling1–3
SGLT, sodium-glucose co-transporter. 1. Wright EM. Am J Physiol Renal Physiol 2001;280:F10–18; 2. Lee YJ, et al. Kidney Int Suppl 2007;106:S27–35; 3. Hummel CS, et al. Am J Physiol Cell Physiol 2011;300:C14–21.
SGLT2
Glucose
Majority of glucose is
reabsorbed by SGLT2
(90%)
Proximal tubule
Remaining glucose is reabsorbed by SGLT1
(10%)
Minimal to no
glucose excretion
Glucose
filtration

SGLT2 inhibitor
Proximal tubule
Glucose
filtration
SGLT2 inhibitors selectively inhibits SGLT2 in the renal proximal tubule1
SGLT2
Glucose
SGLT2 INH.
SGLT2
Increased urinary glucose excretion

Mechanism of Action of SGLT2 Inhibitors
Inhibition of SGLT2 Reversal of glucotoxicity
Insulin sensitivity in muscle• ↑ GLUT4 translocation• ↑ Insulin signaling• Other
Insulin sensitivity in liver• ↓ Glucose- 6-phosphatase
Gluconeogenesis• Decreased Cori cycle• ↓ PEP carboxykinase
-Cell function

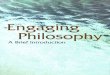
EMPA-REG OUTCOME CVOT overview
• High CV risk patients T2D (MI, stroke, CAD, UA, PAD); A1c 7-10%
Results:• Age ca. 64 yrs• BMI = 30 kg/m2• CV risk = 99%• HbA1c = 8%• T2D = >10 yrs
Primary endpoint: time to 1st occurrence of any of the following adjudicated components of the primary composite endpoint (3P-MACE)
1. CV death (including fatal stroke and fatal MI)
2. Non-fatal MI (excluding silent MI)
3. Non-fatal stroke

CV death
42
HR 0.62(95% CI 0.49, 0.77)
p<0.0001
Cumulative incidence function. HR, hazard ratio

0.5 1.0 2.0
Patients with event/analysedEmpagliflozin Placebo HR (95% CI) p-value
Intent-to-treat population
164/4687 69/2333 1.18 (0.89, 1.56) 0.2567
Fatal and non-fatal stroke
Cox regression analysis. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio; *Excluding events >30 days after last intake of study drug and patients who received study drug for <30 days (cumulative)
On-treatment analysis*
141/4607 66/2308 1.04 (0.78, 1.40) 0.7849
0.5 1.0 2.0
Favoursempagliflozin
Favoursplacebo
Numerical difference largely driven by events occurring >30 days after treatment stop Favours
empagliflozinFavoursplacebo

Patients with event/analysedEmpagliflozin Placebo HR (95% CI) p-value
3-point MACE 490/4687 282/2333 0.86 (0.74, 0.99)* 0.0382
CV death 172/4687 137/2333 0.62 (0.49, 0.77) <0.0001
Non-fatal MI 213/4687 121/2333 0.87 (0.70, 1.09) 0.2189
Non-fatal stroke 150/4687 60/2333 1.24 (0.92, 1.67) 0.1638
4-point MACE 599/4687 333/2333 0.89 (0.78, 1.01)* 0.0795
0.25 0.50 1.00 2.00
3-point MACE and 4-point MACE
44
Favours empagliflozin Favours placebo
Cox regression analysis. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio; CV, cardiovascular; MI, myocardial infarction
*95.02% CI

Heart failure
45

Hospitalisation for heart failure
46
HR 0.65(95% CI 0.50, 0.85)
p=0.0017
Cumulative incidence function. HR, hazard ratio

All-cause mortality
47

All-cause mortality
48
HR 0.68(95% CI 0.57, 0.82)
p<0.0001
Kaplan-Meier estimate. HR, hazard ratio

Insulins
Basal insulin
Premixed twice daily
Basal bolus



Advantages Disadvantages
Universally effective Hypoglycemia
Low cost Weight gain
No long term risk of cancer
Injectable
Benefit for micro vascular
complications

Newer Insulins

How to start insulin therapy
Insulin therapy in Type 2 patients on OADs can be started as:
• Supplemental therapy
• Substitution therapy



Dosage: Initial 10 units; titration* to FPG <5.5 mmol/l
(<100 mg/dl) without hypoglycaemia
FPG** mmol/l (mg/dl)
2
8
4
6
Insulin glargine dose
increment* (IU/day)
5.5―6.7 (100―120)
10.0 (180)
6.7―7.8 (120―140)
7.8―10.0 (140―180)
*Increased weekly if no severe hypoglycaemia and no PG <4 mmol/l (<72 mg/dl), using means of most recent FPG values; **over 2―3 days.
Treat-to-Target study: dose titration algorithm
Riddle M, et al. Diabetes Care 2003;26:3080―6.
Forced weekly insulin titration algorithm

LANMET study: treatment algorithm
• Patients self-adjusted dose
• FPG values transferred by modem to diabetes monitoring centre
• Insulin dose titrated to FPG 4.0―5.6 mmol/l (72―100 mg/dl)
Measure FPG daily for 3 days
If mean of FPG measurements
>5.6 mmol/l (>100 mg/dl)
ADD 2 UNITS OF BASAL INSULIN
FPG=fasting plasma glucose.
Yki-Jarvinen H, et al. Diabetes 2004;53(suppl 2). Abstract 2181-PO.
No increase in dose if FPG <4.0 mmol/l (<72 mg/dl)

LANMET study: similar HbA1c reduction achieved in both treatment groups
Study end
Bedtime NPH vs insulin glargine, plus metformin 2 g
NS=not significant.
Yki-Jarvinen H, et al. Diabetes 2004;53(suppl 2). Abstract 2181-PO.
5
6
7
5.7
FPG
(m
mol/
l)
NS
6
8
9
7
10
HbA
1c
(%)
Baseline
7.1
6.0
9.5
NPH insulin
Insulin glargine
All patients
Study end
7.1

LANMET study: significantly less hypoglycaemia with insulin glargine
NPH insulin
Insulin glargine
20
60
80
40
100
70
0
68
Insulin dose
(units/day)
1
3
4
2
5
3.5
2.6
NS
Weight gain
(kg)
0
Symptomatic
hypoglycaemia
(events/patientyear)
2
6
8
4
10
8.0
5.5
0
NS
―44%
Bedtime NPH vs insulin glargine, plus metformin 2 g
p<0.05
NS=not significant.
Yki-Jarvinen H, et al. Diabetes 2004;53(suppl 2). Abstract 2181-PO.

AT.LANTUS: no difference in the incidence of severe hypoglycaemia between clinic- and patient-driven titration algorithms
Incid
ence o
f hypogly
caem
ia (
%)
Hypoglycaemia
Severe
(<50 mg/dl)
Symptomatic Nocturnal
0.9 1.1
26.3
29.7
3.24.1
0.2 (90%CI ―0.3,
0.7)
NS
3.4 (90%CI 1.2, 5.5)
Significant
0.9 (90%CI 0.0, 1.9)
NS
30
25
20
15
10
5
0
Clinic-driven algorithm
Patient-driven algorithm
Davies M, et al. Diabetes Care 2005;28:1282―8.

AT.LANTUS: significantly greater reduction in HbA1c achieved with patient- than with clinic-driven titration algorithms
Clinic-driven
algorithm (n=2,315)
Patient-driven
algorithm (n=2,273)
―1.08
―1.22
p<0.001
HbA
1c
(%)
0
―0.25
―0.50
―0.75
―1.00
―1.25
Davies M, et al. Diabetes Care 2005;28:1282―8.

AT.LANTUS study: summary
• Simple insulin titration • A simple patient-driven titration algorithm significantly
improved glycaemic control
• No increase in severe hypoglycaemia compared with a clinic-driven algorithm
• Keys to success• Self-monitored blood glucose
• Self-adjustment of insulin dose
Davies M, et al. Diabetes Care 2005;28:1282―8.


24-hours.
The confidence of steady basal insulin release –
all day and all night.
Multiple-daily injections (1,4)
“Insulin glargine as the basal insulin combined with rapid-
acting insulin
analogues (insulin lispro, insulin aspart) is probably the most
physiological insulin substitution therapy available by
subcutaneous injection and will therefore be the basis for
future comparisons” (3)Sources: 1.Leahy JL. Insulin Therapy. New York, NY: Marcel Dekker Inc, 2002. 2.Bolli GB. Diabetalogia 1999; 42:1151-1167. 3.Owens DR, Zinman B, Bolli GB.
Insulins today and beyond. The Lancet 2001;358(9283)739-746.


A Review of Different Therapies…
Intermediate-acting insulins: NPH
• Does not mimic basal insulin profile(1,2)
— Variable absorption
— Pronounced peak
— 13-16 hour duration
— Requires twice-daily administration to provide 24-hour
basal insulin coverage
• Fear of hypoglycaemia(3)
— Major factor limiting insulin adjustmentsMultiple-daily injections (1,4)
Source: 1.Leahy JL. Insulin Therapy. New York, NY: Marcel Dekker Inc, 2002. 2. Chan JL, Mayo Clin Proc 2003;78:459-467. 3. Bergenstal RM, Endocrinology, 4th ed. Philadelphia,
PA: WB Saunders Co,: 2001:821-835. 4.Bolli GB. Diabetalogia 1999; 42:1151-1167.



Pre-Mixed Insulin regimens (1,2)
• Inadequate insulin coverage
• Poor long-term control
• Failure to match endogenous secretion pattern
• Dawn phenomenon
• Increased glycaemia
Twice-daily split-mixed regimens(1,2)
A Review of Different Therapies
Source: 1.Leahy JL. Insulin Therapy. New York, NY: Marcel Dekker Inc, 2002. 2.Bolli GB. Diabetalogia 1999; 42:1151-1167.

CVS risk modification
• Stop smoking
• BP control
• Aspirin (primary and secondary prevention)
• Lipid lowering agents (primary and secondary prevention)

Hypertension and diabetes-
therapy related benefits
Reduction in risk of complications in tight (144/82 mm Hg)
versus lower (154/87mm Hg) BP control
- 32%
- 24%
- 44%
- 56%
- 37%
UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713.
Hypertension and diabetes
Death related to
diabetes
Complications related to diabetes
Stroke
Heart failure
Microvascular complications

Goals of BP lowering
• All stages (watch ISH & low DBP) <140/90
• Diabetes mellitus <130/85
• Renal insuff (Cr >220 umol/L) <130/85
• Proteinuria<125/75
• Congestive heart failure <120/80

Number of Antihypertensive Agents Needed to Achieve Target Blood Pressure
Adapted from Bakris GL, et al. Am J Kidney Dis 2000; 36: 646–61
ALLHAT (138 mm Hg)
IDNT (138 mm Hg)
RENAAL (141 mm Hg)
UKPDS (144 mm Hg)
ABCD (132 mm Hg)
MDRD (132 mm Hg)
HOT (138 mm Hg)
AASK (128 mm Hg)
Average Number of Antihypertensive Agents/Patient
1 2 3
Trial/SBP Achieved

Total Cholesterol
LDL Cholesterol
Triglycerides
HDL Cholesterol
5
3
1.5
1.2
mmol/L
mmol/L
mmol/L
mmol/L
New SA Lipid Targets
S Afr Med J 2000;90:164-178

Turner RC, Br Med J 1998;316:823-8
Dyslipidaemia
Hypertension
Hyperglycaemia
Cigarette Smoking
LDL > 3.9 mmol/L
SBP > 142 mmHg
HBA >7.5%
current
1
Upper ThirdCut-off Point
HazardRatio
RiskFactor
2.26
1.82
1.52
1.41
Independent Risk Factors for Coronary Heart Disease in the UKPDS

0.5
1
1.5
2
2.5
3
Sm
okin
g
Micro
alb
um
inuria
Mal
e Gen
der
Tot
al C
hole
ster
ol
Sys
tolic BP
Rela
tive R
isk
MICROALBUMINURIA COMPARED TO TRADITIONAL RISK FACTORS FOR ISCHAEMIC HEART DISEASE
N=2,085; 10 year follow-up
Borch-Johnsen K, et al.
Arterioscler Thromb Vasc Biol. 1999;19(8):1992-1997.

Diabetic Nephropathy
• Diabetic nephropathy is irreversible in humans
• No case of recovery or cure has been reported in the literature
• Once the clinical signs of nephropathy have become manifest, the natural course is inexorable progressive to death
• The rate of progression is accelerated in the later stages
Kussman et al. JAMA 1976; 236:1861

Morbidity and Mortality Along the Renal Continuum
Risk Factors
Diabetes
Hypertension
Endothelial
Dysfunction
Micro-
Albuminuria
Macro-
ProteinuriaNephrotic
Proteinuria,
End-Stage
Renal Disease
Death
Adapted from Burgess
RENAAL
IDNTIRMA-2
MARVAL

OPTIMISING RENAL PROTECTION
Nephro-protection starts with prevention of proteinuria
Pro-Active Re-Active
Duration of diabetes (years)
UAE µ/min <20 20-200 >200
Normoalbuminuria Micro Macro ESRD
0 13 18 25
BENEDICT RENAALLosartan
IDNTIrbesartan
IRMA 2 Irbesartan
MICRO-HOPERamipril

CKD & CVD screening ?

IN SUMMARY……..

Step 4:
REFER SPECIALIST

Case scenario 1• 44 year old female with features of
metabolic syndrome. (HTN, BMI =40)
• Currently on Metformin 850mg TDS and HbA1c is >10%.
• What other information would you need prior to escalating therapy?
• What is the next best step in terms of her therapy?

Questions

WHO vs ADA Diagnostic Criteria
ADA
-No previous diagnosis of Diabetes
• FPG > 7mmol/l
For IFG
• FPG > 6.1 < 7mmol/l
WHO (1980-85)
For Undiagnosed Diabetes
• FPG > 7 mmol/l OR
2-h postprandial PG >11.1mmol/l
For IGT
• 2-h postprandial PG > 7.8 and < 11.1 mmol/l

Elevated LDL-cholesterol
Low HDL-cholesterol
Elevated systolic BP
Elevated glycated HB
Smoking
Risk Factors for CHD in the UKPDS

Principles of T2DM treatment
‘Treat to Target’ — to predefined goals
‘Stepwise Treatment’ — for a progressive disorder, add
and avoid switching if possible
Optimise and individualise
treatment
American Association of Clinical Endocrinologists. Endocr Pract 2002;8(suppl 1):43―84.
American Diabetes Association. Diabetes Care 2004;27(suppl 1):S15―35.
Davies M, et al. Diabetes Care 2005;28:1282―8.
International Diabetes Federation. Diabet Med 1999;16:716―30.
Japan Diabetes Society. Available at: http://www.jds.or.jp.
Riddle M, et al. Diabetes Care 2003;26:3080―6.
Yki-Jarvinen H, et al. Diabetes 2004;53(suppl 2). Abstract 2181-PO.

Riddle M, et al. Diabetes Care 2003;26:3080―6.
Treat-to-Target study: less nocturnal hypoglycaemia with insulin glargine
*p<0.05; **p<0.03; §p<0.005.
HbA1c 7% 57
Dose (units/day)
33 27*
NPH
(n=389)
Insulin glargine
(n=367)
Patients reaching glycaemic targets (%)
FPG <5.5 mmol/l
(<100 mg/dl)
22 16**
58
47.2 41.8§
36 34
without nocturnal
hypoglycaemia
without nocturnal
hypoglycaemia

Treat-to-Target study: summary
• Validated the concept that adding basal insulin
(NPH or insulin glargine) to OHAs in T2DM
restores HbA1c values to target levels in most
patients
• ~60% reached target HbA1c level <7%
Riddle M, et al. Diabetes Care 2003;26:3080―6.

Insulin initiation: substitution therapy
Stop OAD treatment
Start 2 injections of 0.2 IU/kg Long acting Insulin or premixed insulin 30/70; 2/3 of the total dose before breakfast and
1/3 before dinner
Dose to be increased by 2-4 IU every 3-4 days,if necessary
If blood glucose levels are too high after meals,premixed insulin is a better choice than long-acting Insulin

Human Insulins and Insulin Analogues
•The time course of action of any insulin can vary in different people or at different times in the same person. For this reason, time periods indicated here should only be considered general guidelines.
Insulin Preparations Onset of Action Peak of Action (h) Duration of Action (h)
Rapid-acting
Regular human insulin1 30 to 60 minutes 2 to 4 6 to 8
Insulin glulisine 5 to 15 minutes2 1 to 23 3 to 44
Insulin lispro/aspart1 5 to 15 minutes 1 to 2 3 to 4
Intermediate-acting
NPH1 1 to 3 h 5 to 7 13 to 16
Lente1 1 to 3 h 4 to 8 13 to 20
Detemir5,6,7 — 4 to 6 20 h
Long-acting
Insulin glargine1 1 to 2 h No Peak 24 h
Ultralente1 2 to 4 h 8 to 14 <20 h
Premix
Insulin NPL/lispro 75/258 10 minutes 1 to 4 10 to 20
Insulin aspart 70/309 10 minutes 1 to 4 16 to 20

Physiologic Insulin Secretion: 24-hour Profile
Source: Advances in Insulin Therapy: The New Paradigm in Diabetes Care – Martin J Abrahamson (www.Medscape.com CME Activity 27 Sept 2001)

Insulin initiation: supplemental therapy
Continue OAD treatment
Add 0.2 IU/kg Insulin at breakfast or at bedtime
Dose to be increased by 2-4 IU every 3-4 days, if necessary
If more than 30-36 IU of insulin is necessary to obtain good metabolic control, consider stopping OAD treatment and continue on insulin alone
Divide the dose into 2 daily injections:
2/3 before breakfast
1/3 at bedtime

When does the patients blood glucose start to go up?• Hyperglycemia develops only when the beta cells fail
• insufficient insulin secretion to overcome insulin resistance
• defective pattern and timing of insulin secretion
• glucose toxicity - sustained hyperglycemia increases insulin resistance and decreases glucose stimulated insulin secretion

100
60
40
20
0
80
-30 0 30 -30 0 30
Time (min)
Control(n=18)
Type 2 diabetes(n=15)
IRI(mU/mL)
Acute Insulin Response to Glucose
Robertson RP, Porte D Jr. J Clin Invest. 1973;52:870-876

Glycaemic control and riskof complications
A Desktop Guide to Type 2 Diabetes Mellitus, European Diabetes Policy Group 1999
Fasting/preprandial Postprandial HbA1c
blood glucose blood glucose (%)(mmol/l)* (mmol/l)*
Low risk < 5.5 < 7.5 < 6.5
Arterial risk > 5.5 > 7.5 > 6.5
Microvascular risk > 6.0 > 9.0 > 7.5

The level of HbA1c alone may be misleading
Service FJ et al. Diabetes Care 1980
Blo
od g
luco
se
Time
HbA1c = 7.5%
Patient 2
Patient 1
Glucose spikes

50% of Type 2 Diabetes Patients Have Complications at the Time of Diagnosis
Retinopathy,
glaucoma or
cataracts
Nephropathy
Neuropathy
MICROVASCULAR MACROVASCULAR
Cerebrovascular
disease
Coronary
heart
disease
Peripheral
vascular
disease
UK Prospective Diabetes Study Group. UKPDS 33. Lancet 1998; 352: 837–853








Metabolic control and macrovascular mortality
Standl et al. 1996
0
10
20
30
Ma
cro
va
sc
ula
r m
ort
ali
ty (
%)
40
< 6.9 % 6.9–8.8 % > 8.8 %
HbA1c
without macrovascular
disease
with macrovascular
disease

Metabolic control and mortality
Gall et al. 1995
0
10
20
Inc
ide
nc
e o
f a
ll-c
au
se
mo
rta
lity
(%
/5 y
ea
rs)
30
> 21 < 21
Urinary albumin excretion rate (mg/24h)
< 7.8
> 7.8
5
15
25

0
0.5
1
1.5
2
2.5
1990 2000 2010
0
200
400
600
800
1000
1200
1981-1990 1991-2000 2001-2010
GLOBAL MAINTENANCE TEN YEAR MEDICAL COSTS
DIALYSIS POPULATION
Lysaght. J Am Soc Nephrol., 2002
$ (
bil
lio
ns
)
mil
lio
ns

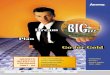
PROTEINURIA AND MORTALITY IN PIMA INDIANS
WITH TYPE 2 DIABETES
Nelson et al. Diabetes, 1988
Ag
e-
an
d s
ex
-ad
juste
d
death
s (
x 1
000 p
ers
on
-
year)
Healthy
subjects
Non
proteinuric
diabetics
Proteinuric
diabetics
97% of the excess mortality reported in diabetics is associated with overt proteinuria

30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
<4.1
4.2-5.2
5.3-6.2
6.3-7.2
>7.2
<0.91
0.91-1.16
1.17-1.29
1.3-1.55
>1.55
<120/80
120-129/80-84
130-139/85-89
140-159/90-99
>160/100
Smoker
Diabetic
Age (years)
ScoreWomen
ScoreMen
RISK FACTORS
TC (mmol/L)
HDLC (mmol/L)
BP (mmHg)
-9
-4
0
3
6
7
8
8
8
-2
0
1
1
3
5
2
1
0
-3
-3
0
0
2
3
2
4
-1
0
1
2
3
4
5
6
7
-3
0
1
2
3
2
1
0
0
-2
0
0
1
2
3
2
2
-2
-1
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
1
2
2
2
3
3
4
4
5
6
7
8
10
11
13
15
18
20
24
>27
0
2
3
3
4
5
7
8
10
13
16
20
25
31
37
45
>53
>53
>53
>53
Score Women Men
RISK PERCENTAGE
DR
UG
TH
ER
AP
YIN
DIC
AT
ED
Obesity
Family History
Sedentary Lifestyle
These risk factors should also be taken into consideration
ADD UP RISK SCORES TO OBTAIN RISK PERCENTAGE
10 year risk calculation for
myocardial infarction in
primary prevention
Wilson PWF, et al. Circulation
1998;97:1837-1847