Embed Size (px)
Citation preview
1
Introduction to Chronic Venous Insufficiency
1
Greg Curry
Vascular Ultrasound
Monash Health
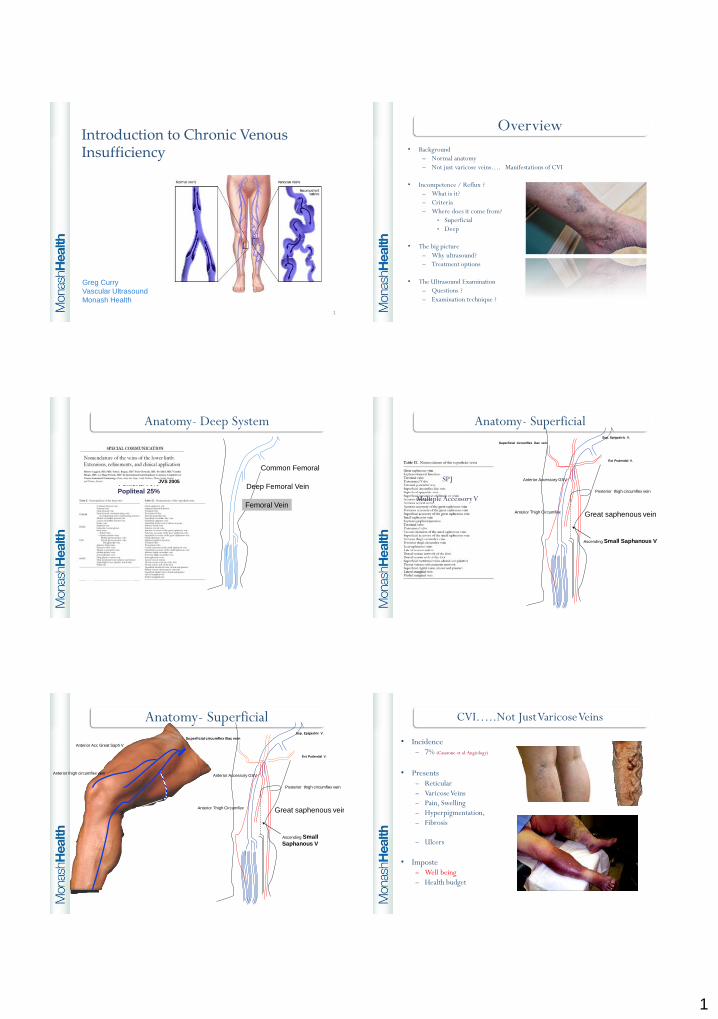
Overview
• Background
– Normal anatomy
– Not just varicose veins…. Manifestations of CVI
• Incompetence / Reflux ?
– What is it?
– Criteria
– Where does it come from?
• Superficial
• Deep
• The big picture
– Why ultrasound?
– Treatment options
• The Ultrasound Examination
– Questions ?
– Examination technique ?
Paired SystemsFemoral 70%
Popliteal 25%
Proximal/ DistalUse Inferior/ Superior
Gastroc/ Soleal
Foot Venous Drainage
Anatomy- Deep System
Common Femoral
Femoral Vein
Deep Femoral VeinJVS 2005
Sup. Epigastric V.
Ext Pudendal V.
SPJ
Multiple Accessory V
Anterior Accessory GSV
Great saphenous vein
Superficial circumflex iliac vein
Posterior thigh circumflex vein
Ascending Small Saphanous V
Anterior Thigh Circumflex
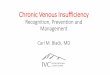
Anatomy- Superficial
Anatomy- Superficial
Anterior thigh circumflex vein
Anterior Acc Great Saph V
Anterior Accessory GSV
Great saphenous vein
Superficial circumflex iliac vein
Posterior thigh circumflex vein
Ascending Small
Saphanous V
Anterior Thigh Circumflex
Sup. Epigastric V.
Ext Pudendal V.
CVI…..Not Just Varicose Veins
• Incidence – 7% (Casarone et al Angiology)
• Presents– Reticular
– Varicose Veins
– Pain, Swelling
– Hyperpigmentation,
– Fibrosis
– Ulcers
• Imposte– Well being
– Health budget
2
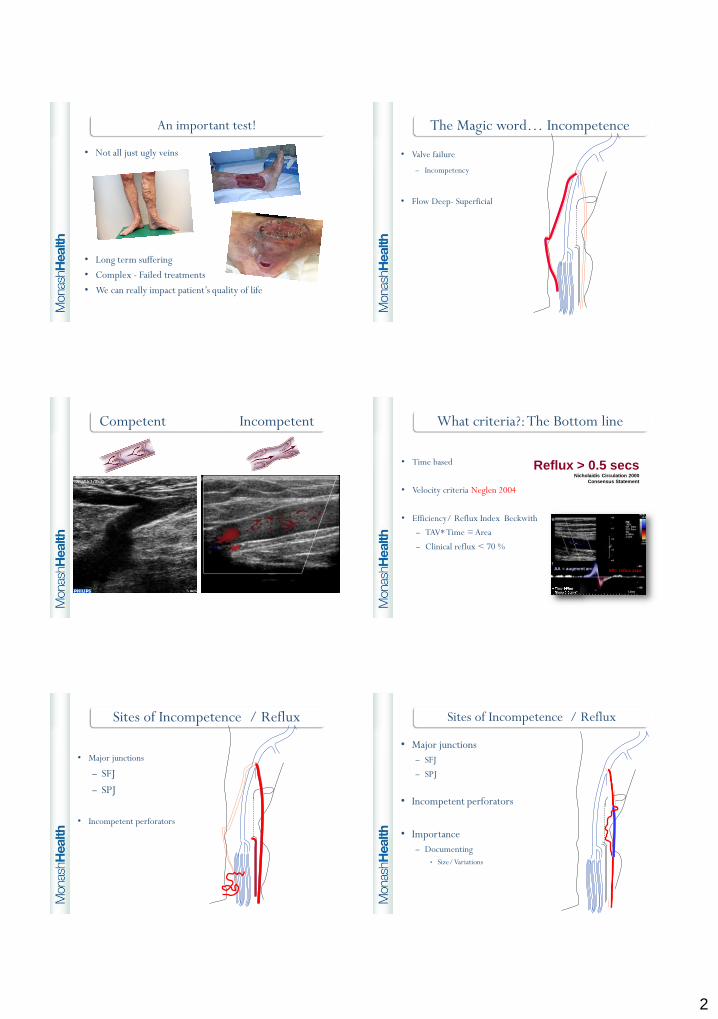
An important test!
• Not all just ugly veins
• Long term suffering
• Complex - Failed treatments
• We can really impact patient’s quality of life
The Magic word… Incompetence
• Valve failure
– Incompetency
• Flow Deep- Superficial
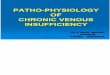
Competent Incompetent What criteria?: The Bottom line
• Time based
• Velocity criteria Neglen 2004
• Efficiency/ Reflux Index Beckwith
– TAV* Time = Area
– Clinical reflux < 70 %
Reflux > 0.5 secsNicholaidis Circulation 2000
Consensus Statement
AA = augment area AR= reflux area
Sites of Incompetence / Reflux
• Major junctions
– SFJ
– SPJ
• Incompetent perforators
Sites of Incompetence / Reflux
• Major junctions
– SFJ
– SPJ
• Incompetent perforators
• Importance
– Documenting
• Size/ Variations
3
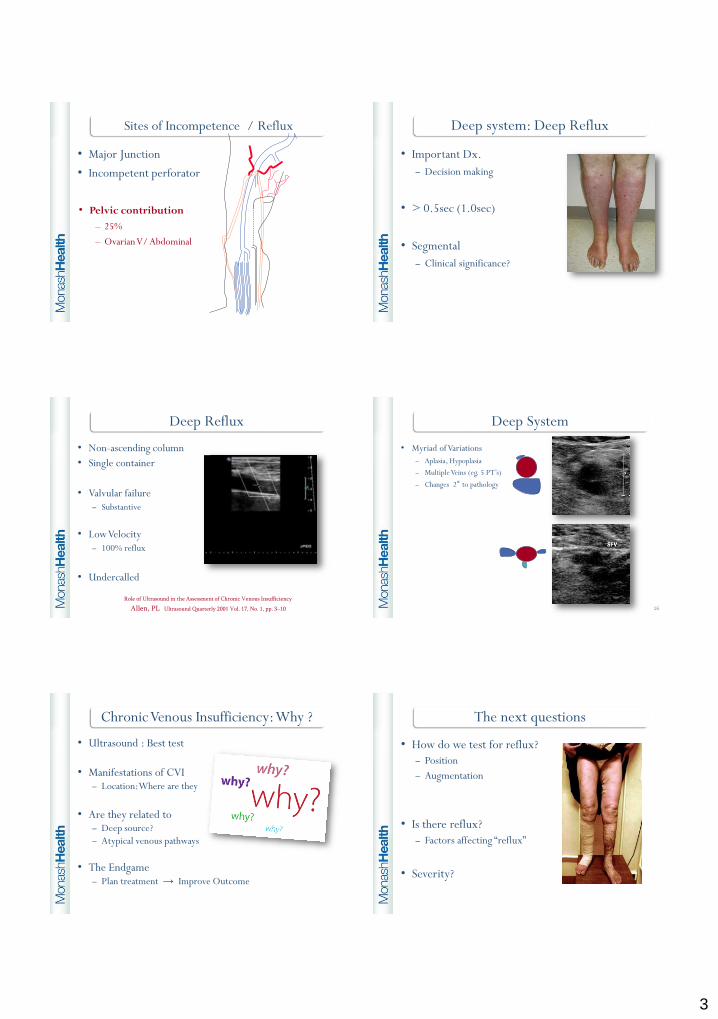
Sites of Incompetence / Reflux
• Major Junction
• Incompetent perforator
• Pelvic contribution
– 25%
– Ovarian V/ Abdominal
Deep system: Deep Reflux
• Important Dx.
– Decision making
• > 0.5sec (1.0sec)
• Segmental
– Clinical significance?
Deep Reflux
• Non-ascending column
• Single container
• Valvular failure
– Substantive
• Low Velocity
– 100% reflux
• Undercalled
Role of Ultrasound in the Assessment of Chronic Venous Insufficiency
Allen, PL Ultrasound Quarterly 2001 Vol. 17, No. 1, pp. 3–10
Deep System
• Myriad of Variations
– Aplasia, Hypoplasia
– Multiple Veins (eg. 5 PT’s)
– Changes 2° to pathology
16
Chronic Venous Insufficiency: Why ?
• Ultrasound : Best test
• Manifestations of CVI– Location: Where are they
• Are they related to– Deep source?
– Atypical venous pathways
• The Endgame – Plan treatment → Improve Outcome
The next questions
• How do we test for reflux?
– Position
– Augmentation
• Is there reflux?
– Factors affecting “reflux”
• Severity?
4
How do we test for reflux?
Aim: Create physiological reflux ?
Reproduce Gravity
How do we test for reflux?
• Primary
– Augment,
• Secondary• Valsalva,
– Dorsi flexion
• Patient Position
How do we test? Creating physiological reflux
• Augment
– Various techniques
• Valsalva
– Strain down
• Toe/ Foot Movement
• Reproducible/ Physiologic
How do we test for reflux? Positions
Multiple positions/ Multiple testing methods
How do we test for reflux? Augmentation
• Manual squeeze
– Create significant void
• Thigh
• Calf
• Foot
Is there Reflux?
Valve closure time
Venous bed
Venous outflow
Testing technique
Location of cursor
Weather, time of day, etc
0.5 sec… 1.0 sec…2.0 sec

5
Grading Incompetence - Severity
• Qualitative- Subjective (experience)
1. SIGNIFICANT - (Moderate -> Gross)
2. MILD
3. V. mild/trickle flow ? Clinical Significance
• Time > 0.5 sec.
• Efficiency Index (Qualitative)
• Clinical Presentation
• Tool for communication
The examination
• Take a minute to ponder how you do this exam?
• First…. What are the key questions to be
answered?
26
Chronic Venous Insufficiency: The Questions
1. Superficial venous reflux
– Is there reflux?
– Where does it come from?
– Where does it distribute to?
– Severity
– R’ship to clinical presentation...
2. Is there deep venous reflux
3. Deep vein patency (?old/recent DVT)
Now its time to do the examination…
• Clinical examination
• Explanation
• Set – up
• Scanning
28
Clinical Examination
Look !!
Ensure your worksheet explains all manifestations of
CVI
29
Do you have a good opening spiel…
“Today we are doing a scan on the veins on your leg.
Your referrer can see where the veins are but can’t see where
they come from. This is why we do the test.
I need to start at the groin where there is a main valve
and then work my way down”
30
6
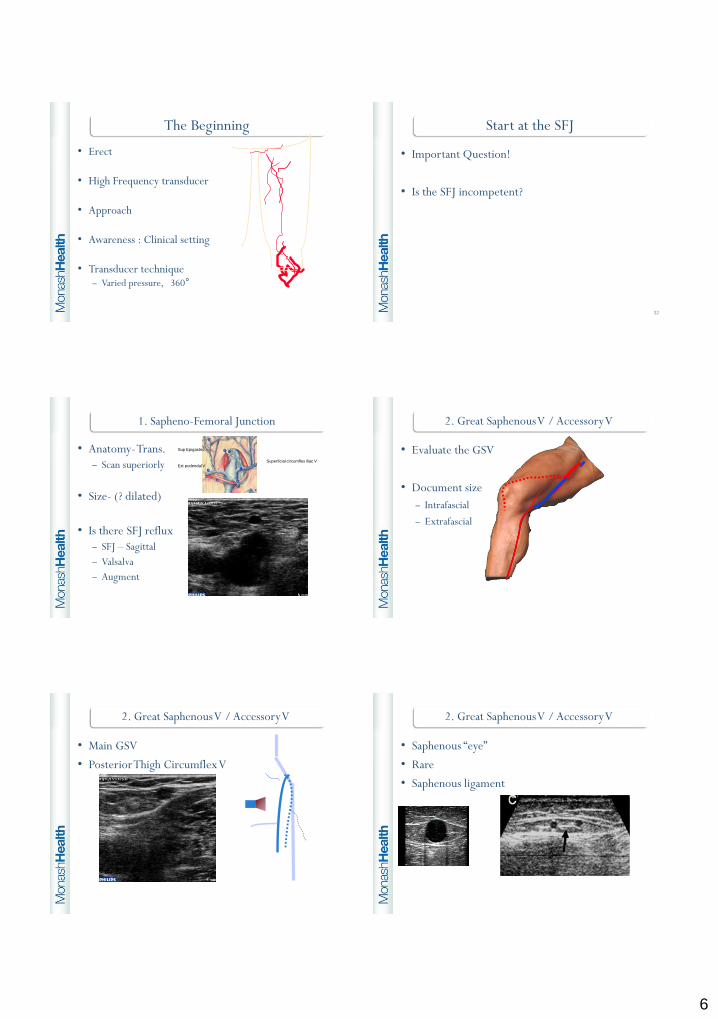
The Beginning
• Erect
• High Frequency transducer
• Approach
• Awareness : Clinical setting
• Transducer technique– Varied pressure, 360°
Start at the SFJ
• Important Question!
• Is the SFJ incompetent?
32
1. Sapheno-Femoral Junction
• Anatomy-Trans.
– Scan superiorly
• Size- (? dilated)
• Is there SFJ reflux
– SFJ – Sagittal
– Valsalva
– Augment
Ext pudendal V
Sup Epigastric
Superficial circumflex iliac V
2. Great Saphenous V / Accessory V
• Evaluate the GSV
• Document size
– Intrafascial
– Extrafascial
2. Great Saphenous V / Accessory V
• Main GSV
• Posterior Thigh Circumflex V
• Saphenous “eye”
• Rare
• Saphenous ligament
2. Great Saphenous V / Accessory V
7
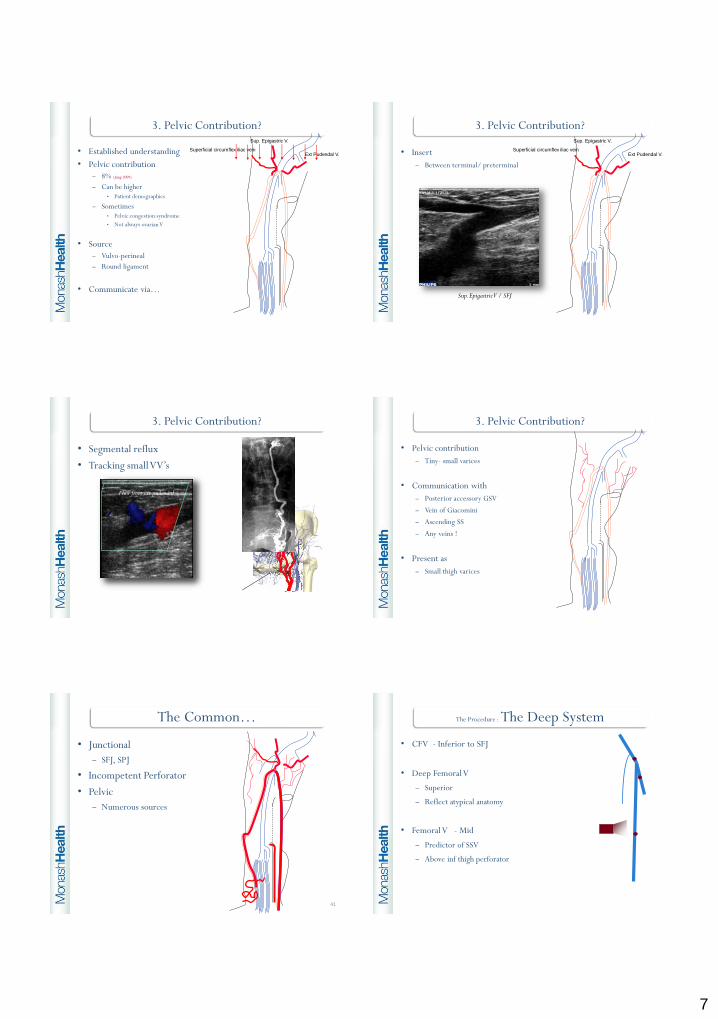
3. Pelvic Contribution?
• Established understanding
• Pelvic contribution
– 8% (Jung 2009)
– Can be higher • Patient demographics
– Sometimes• Pelvic congestion syndrome
• Not always ovarian V
• Source
– Vulvo-perineal
– Round ligament
• Communicate via…
Superficial circumflex iliac vein
Sup. Epigastric V.
Ext Pudendal V.
3. Pelvic Contribution?
• Insert
– Between terminal/ preterminal
Superficial circumflex iliac vein
Sup. Epigastric V.
Ext Pudendal V.
Sup. Epigastric V / SFJ
3. Pelvic Contribution?
• Segmental reflux
• Tracking small VV’s
Flow from ext pudendal
3. Pelvic Contribution?
• Pelvic contribution
– Tiny- small varices
• Communication with
– Posterior accessory GSV
– Vein of Giacomini
– Ascending SS
– Any veins !
• Present as
– Small thigh varices
The Common…
• Junctional
– SFJ, SPJ
• Incompetent Perforator
• Pelvic
– Numerous sources
41
The Procedure : The Deep System
• CFV - Inferior to SFJ
• Deep Femoral V
– Superior
– Reflect atypical anatomy
• Femoral V - Mid
– Predictor of SSV
– Above inf thigh perforator

8
The question to ask at this point….
• Have I resolved the upper leg?
Now the popliteal fossa…
44
The Procedure : Small Saphenous Vein
• Anatomical variants– Insertion
• Via GV• Direct• FV• Internal Iliac V
• Size - ? Dilated
• Insertion – Meas. from knee crease
• Reflux
• LSV reflux → SSV “syphon”
Intersaphenous connection
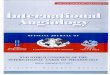
Sites of interrogation- Small Saphenous
V of Giac.
Add canal
SPJ
SSV- Pop fossa
SSV - Mid calf
The Procedure : Popliteal Fossa
• Gastrocnemius Vein
• Incompetent perforator
• Baker’s cystGV
Perforator
The Procedure : Deep System: Lower leg
• Popliteal
• Gastrocnemius V
• Posterior Tibial, Peroneal
– Only if inf. popliteal reflux
Peroneal
PT
Tibio-per. trunk

9
Next…..Incompetent Perforators
• Size
• Location - (fascia)
• Dist. from Med. malleolus
• MARKING -No Black/Blue texta
• ALL OF LEG MUST BE EXAMINED
Testing of Perforators (Below line → Deep- Superficial)
Inferior calf augment Valsalva
The toe wiggle Tourniquet: Upper calf
Perforator Testing
• Time based Negle´n JVS 2004
– 0.5 sec (3 consecutive augments) Delis JVS 2004, Delis Radiology 2004
• Size Negle´n JVS 2004
– > 4.0 mm
• Describe
– Location
– Presence of reflux
– Relationship to VV’s
• DON’T Overcall / Note if dilated but is just inflow
Perforators
Nomenclature of the veins of the lower limbs: An
international interdisciplinary consensus statement
Alberto Caggiati, et al 2002 JVS
The Procedure : DVT Study
• Limited
• Full study
– Hx of DVT
– Leg swelling
– Significant deep venous reflux
Communication
• Quality worksheet
• Structured reporting
• Liaise Vascular consultant
– Feedback
– Detail
• Vein Sizes
SSV
GSV
AAGSV
10
The worksheet
55
Take home messages
• Important test
• CVI US is challenging and
rewarding
– Clinical question
– Know your anatomy
– Technique is important
– “Contextual reporting”
56