Embed Size (px)
Citation preview

The value of skin tests in in patients with selective responses to NSAID
Klinik und Poliklinik für
Dermatologie und
Allergologie am
Biederstein, Technische
Universität München,
80802 München
Knut Brockow
lammintaustra
Problems in NSAID hypersensitivity skin testing
• For the majority of patients no immunological
mechanism has been demonstrated
• Skin tests remain often negative
• Heterogeneity of elicitors and clinical pictures
• Experience to test drugs has declined
• There is no standard for testing but many
different methods do exist in different centers
Patient, f, 39y, with typical history
• No atopy
• 2 years ago because of headache in Croatia
Plivadon
(paracetamol+propyphenazone+coffeine+codeine)
• “Immediately” generalised pruritus, urticaria,
dypnea and tachycardia
• 1 year ago because of back pain Demex
(propyphenazone): “immediately” dypnea,
vomiting, tachycardia and finger paresthesia
To be known by every allergist
• Skin tests are only positive in allergic reactions
• The negative predictive value depends on the sensitivity of skin tests
• The negative predictive value differs with drug, manifestation and kinetics
• Skin tests should be used as screening tests and do avoid provocation tests
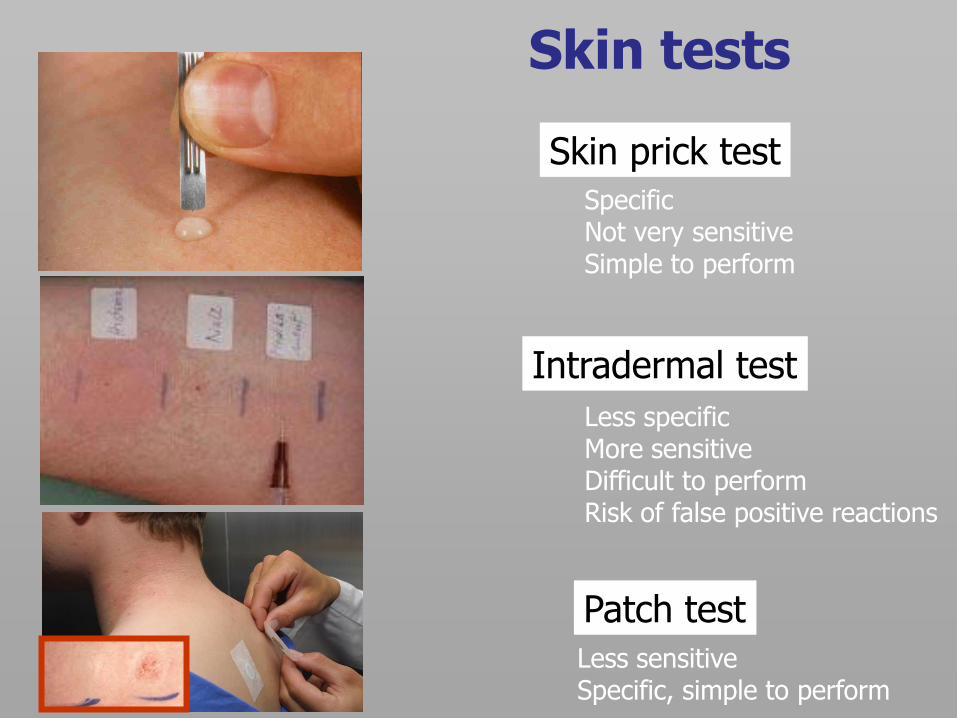
Skin prick test
Intradermal test
Patch test
Skin tests
Specific Not very sensitive Simple to perform
Less specific More sensitive Difficult to perform Risk of false positive reactions
Less sensitive Specific, simple to perform
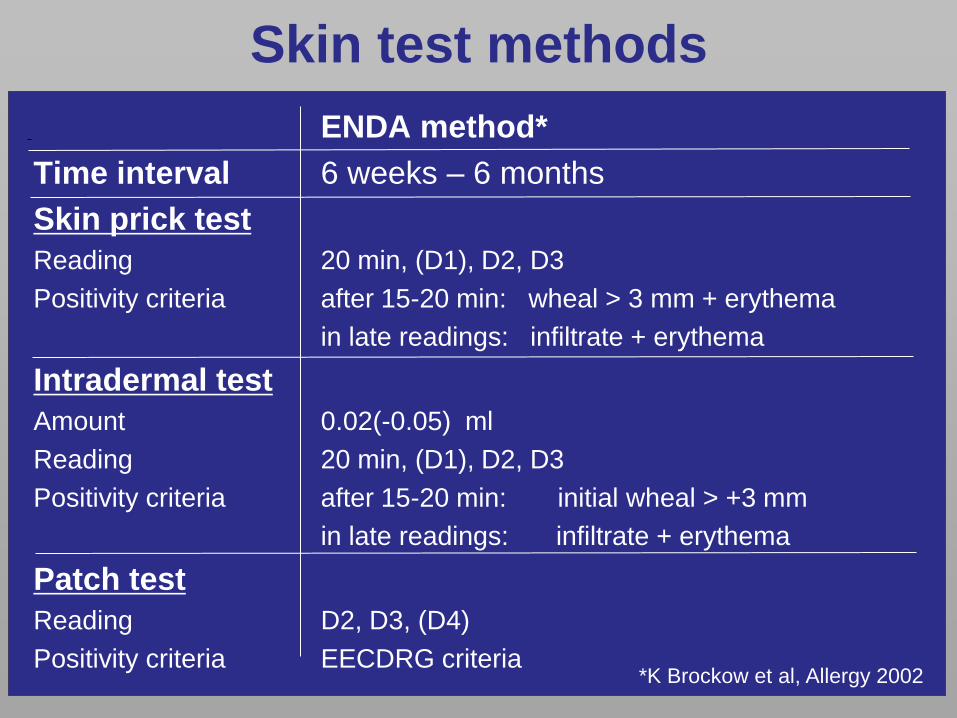
Skin test methods
ENDA method*
Time interval 6 weeks – 6 months
Skin prick test
Reading 20 min, (D1), D2, D3
Positivity criteria after 15-20 min: wheal > 3 mm + erythema
in late readings: infiltrate + erythema
Intradermal test
Amount 0.02(-0.05) ml
Reading 20 min, (D1), D2, D3
Positivity criteria after 15-20 min: initial wheal > +3 mm
in late readings: infiltrate + erythema
Patch test
Reading D2, D3, (D4)
Positivity criteria EECDRG criteria
*K Brockow et al, Allergy 2002
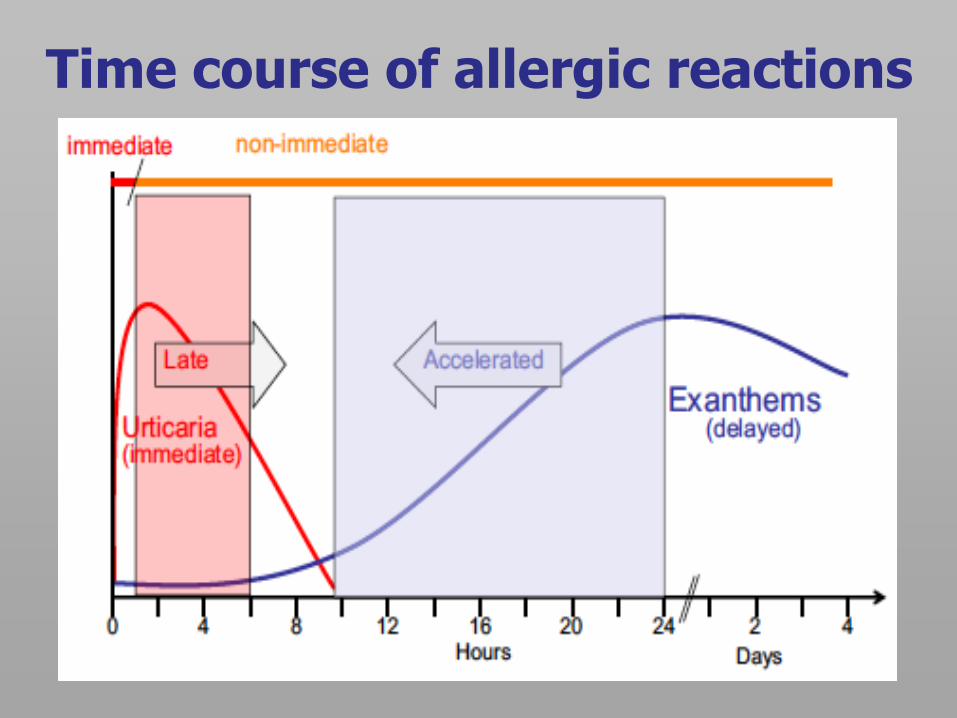
Time course of allergic reactions
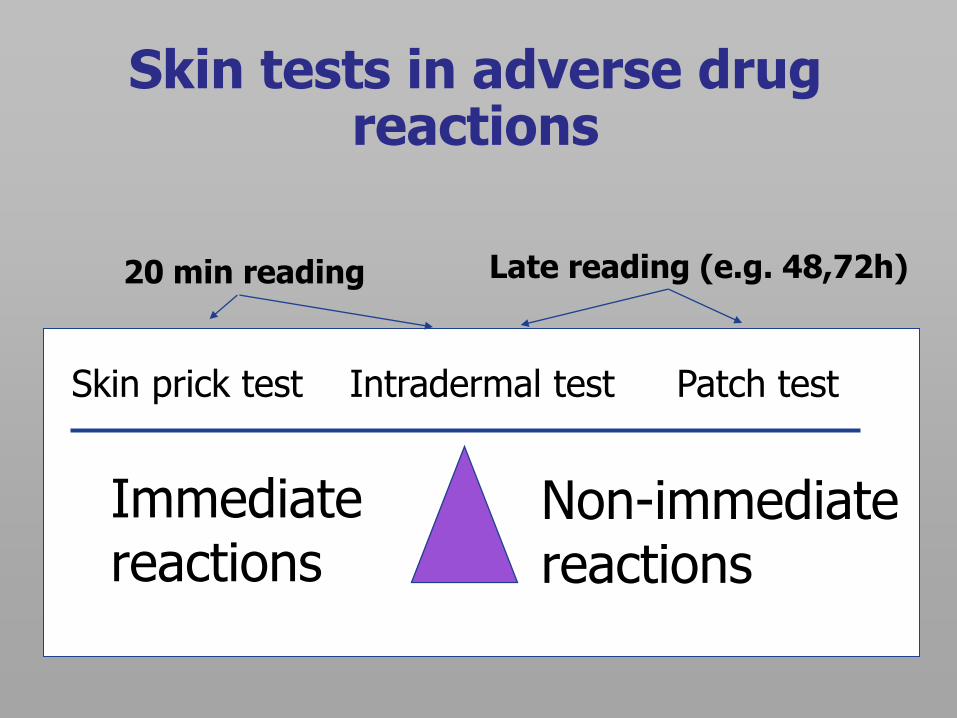
Skin tests in adverse drug reactions
Skin prick test Intradermal test Patch test
Immediate reactions
Non-immediate reactions
20 min reading Late reading (e.g. 48,72h)
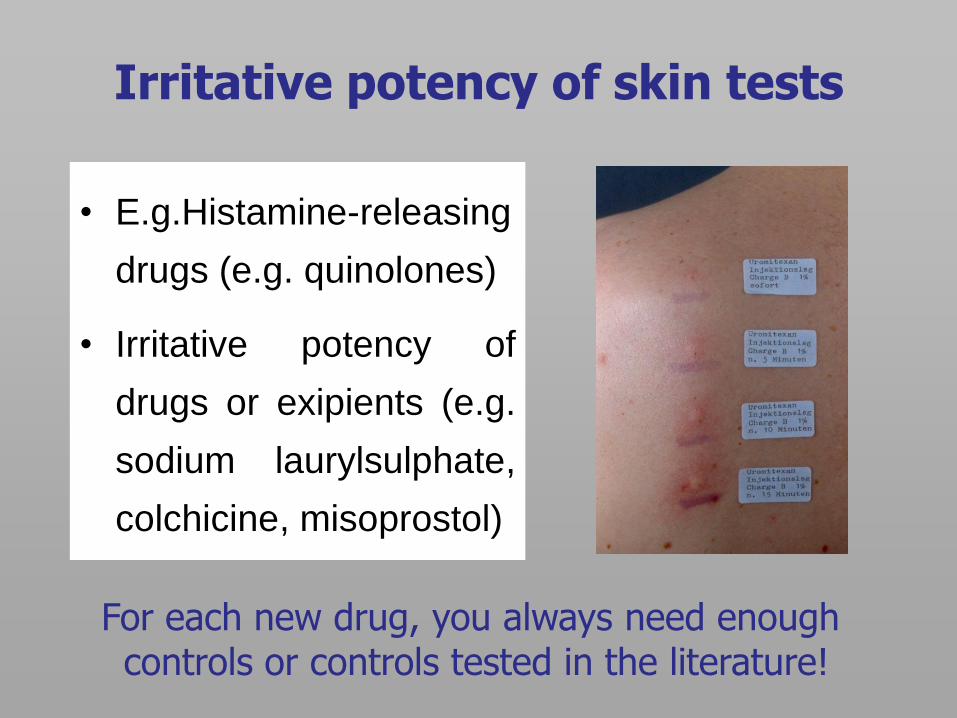
Irritative potency of skin tests
• E.g.Histamine-releasing
drugs (e.g. quinolones)
• Irritative potency of
drugs or exipients (e.g.
sodium laurylsulphate,
colchicine, misoprostol)
For each new drug, you always need enough controls or controls tested in the literature!
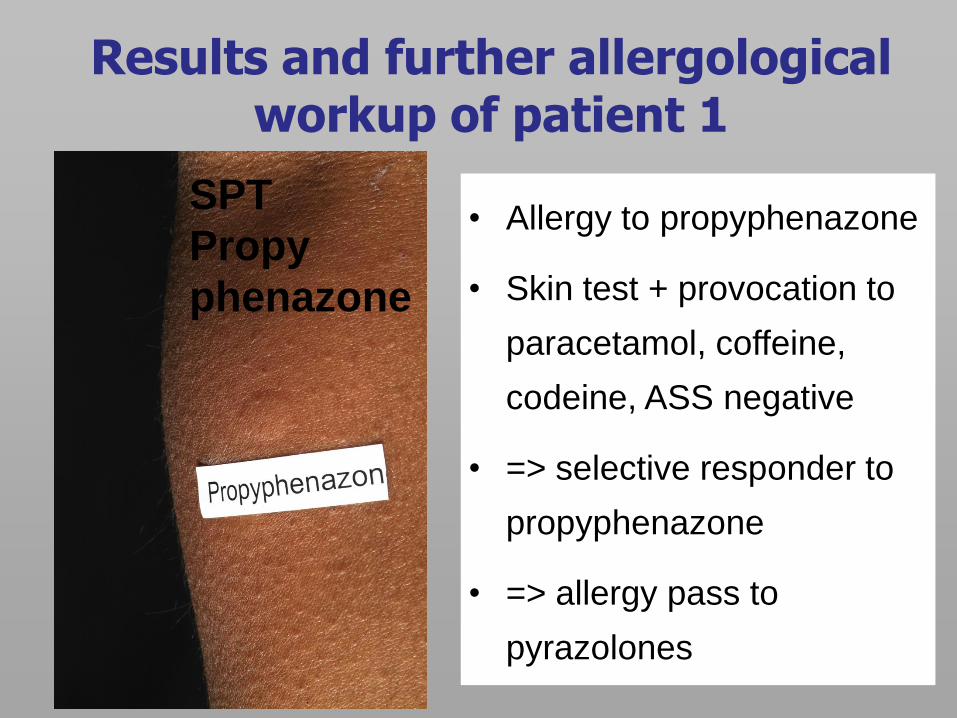
Results and further allergological workup of patient 1
• Allergy to propyphenazone
• Skin test + provocation to
paracetamol, coffeine,
codeine, ASS negative
• => selective responder to
propyphenazone
• => allergy pass to
pyrazolones
SPT
Propy
phenazone
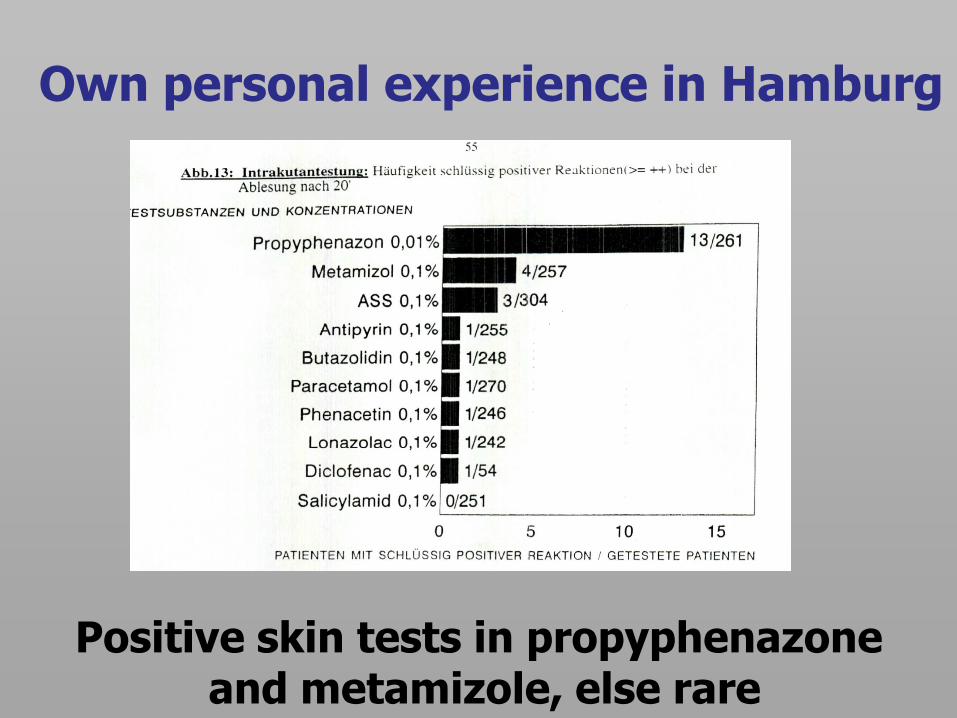
Own personal experience in Hamburg
Positive skin tests in propyphenazone and metamizole, else rare
What are Pyrazolones?
• Propyphenazone
• Phenazone (Antipyrin)
• Aminophenazone
• Noraminophenazone
• Metamizol (Dipyrone)
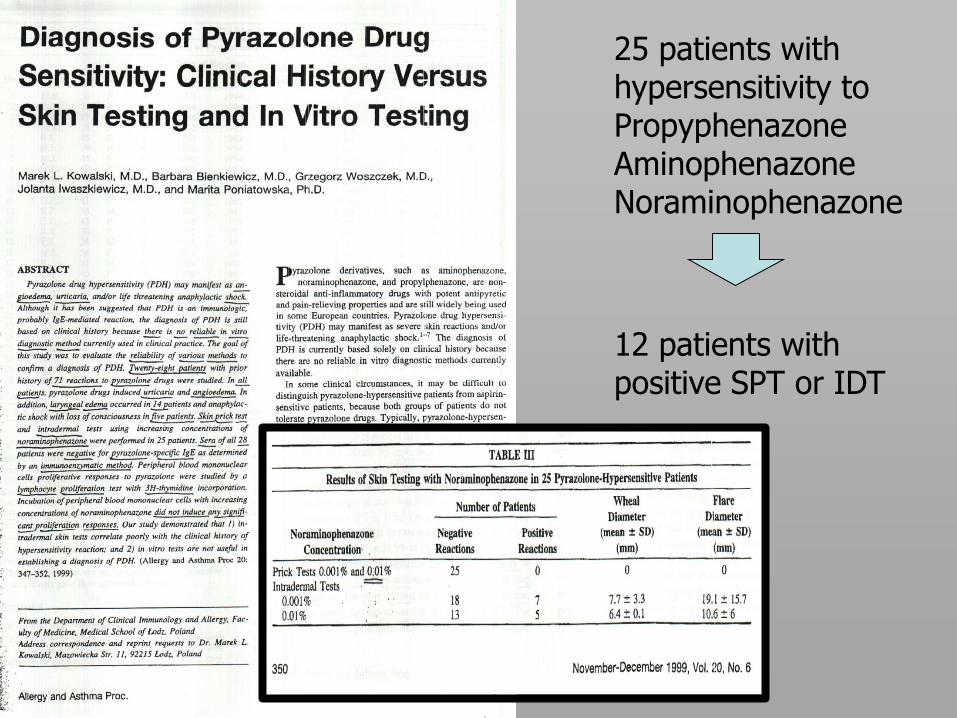
25 patients with hypersensitivity to Propyphenazone Aminophenazone Noraminophenazone
12 patients with positive SPT or IDT
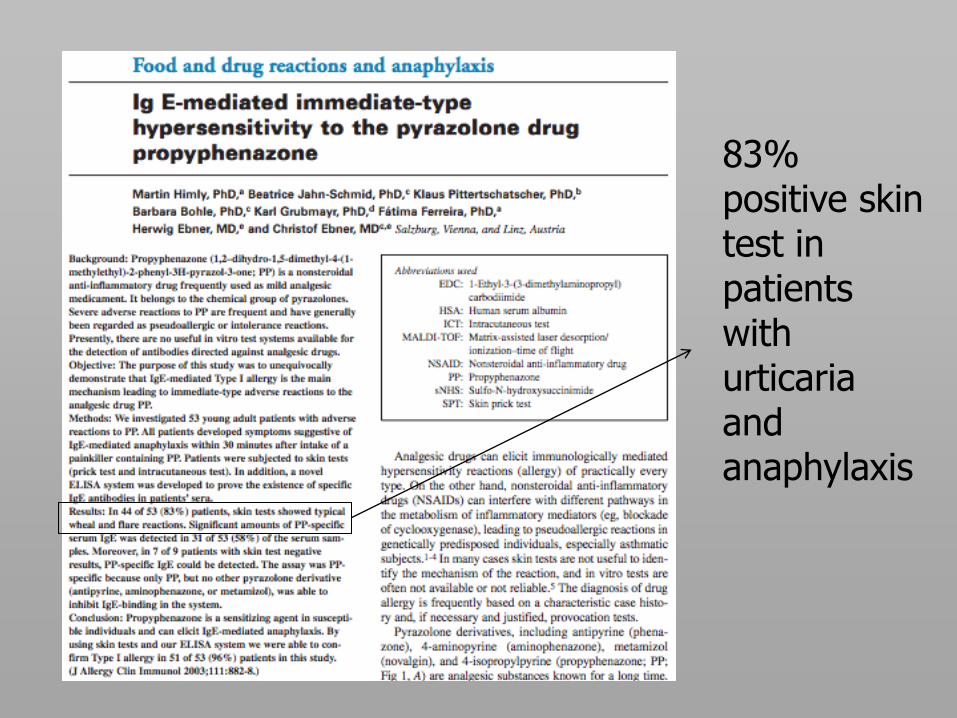
83% positive skin test in patients with urticaria and anaphylaxis
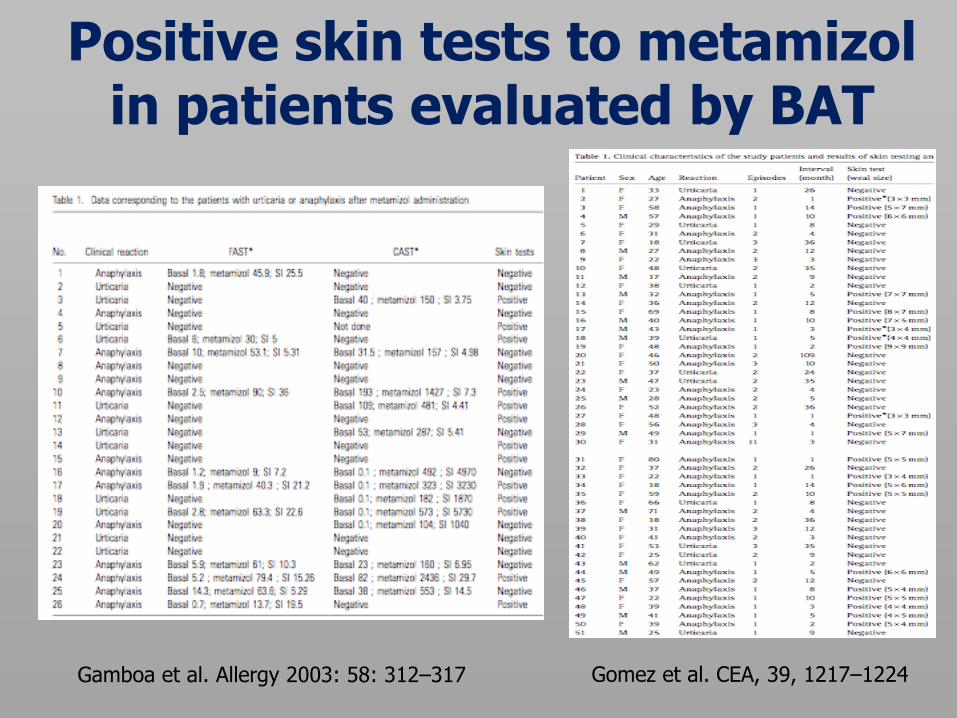
Gamboa et al. Allergy 2003: 58: 312–317 Gomez et al. CEA, 39, 1217–1224
Positive skin tests to metamizol in patients evaluated by BAT
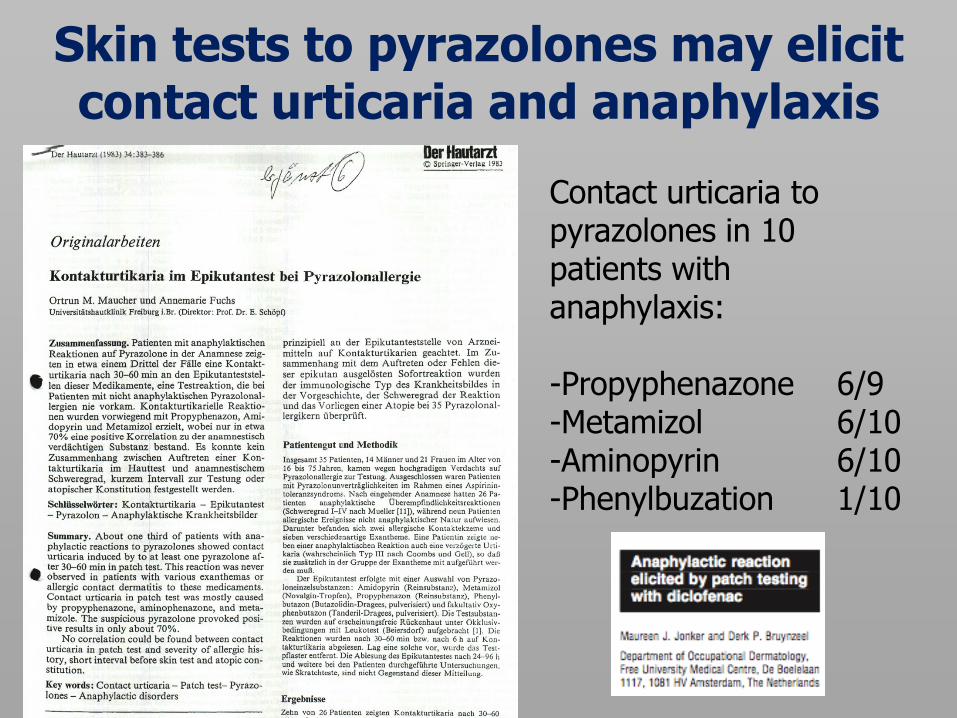
Skin tests to pyrazolones may elicit contact urticaria and anaphylaxis
Contact urticaria to pyrazolones in 10 patients with anaphylaxis: -Propyphenazone 6/9 -Metamizol 6/10 -Aminopyrin 6/10 -Phenylbuzation 1/10
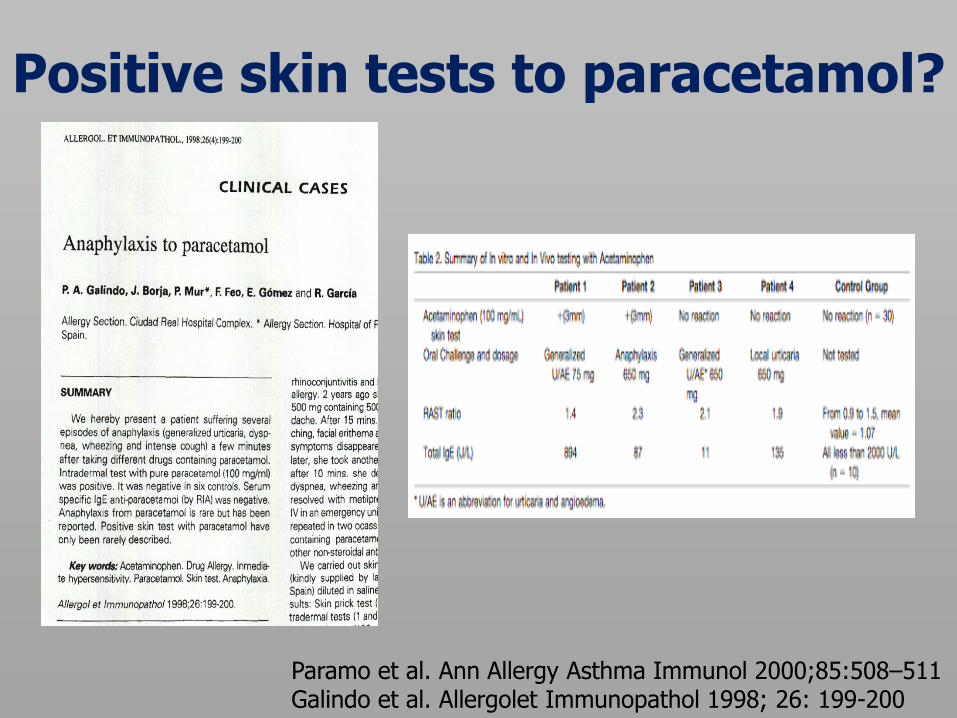
Positive skin tests to paracetamol?
Paramo et al. Ann Allergy Asthma Immunol 2000;85:508–511 Galindo et al. Allergolet Immunopathol 1998; 26: 199-200
Conclusions skin tests for anaphylaxis and urticaria
• Pyrazolones should always be tested
• Positive in ca. 20-70% of patients when tested
with pure SPT and 0.1mg/ml IDT
• Other NSAIDs are seldomly positive and testing
may be restricted to expert centers
• Exceptional skin test-positive cases should be
reported with detailed conditions
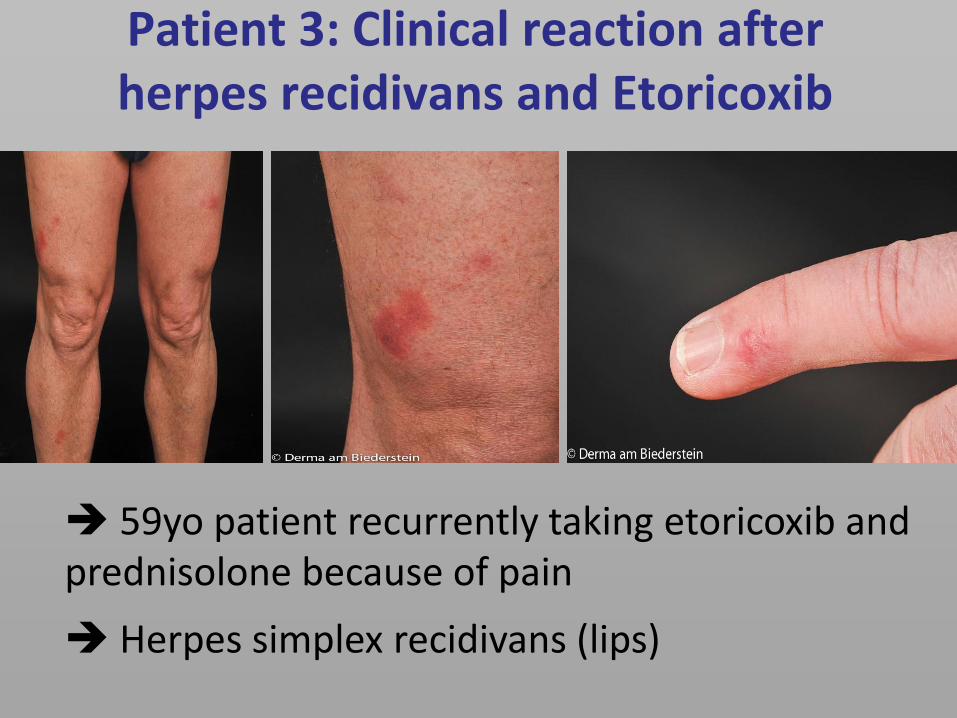
Patient 3: Clinical reaction after herpes recidivans and Etoricoxib
59yo patient recurrently taking etoricoxib and prednisolone because of pain
Herpes simplex recidivans (lips)
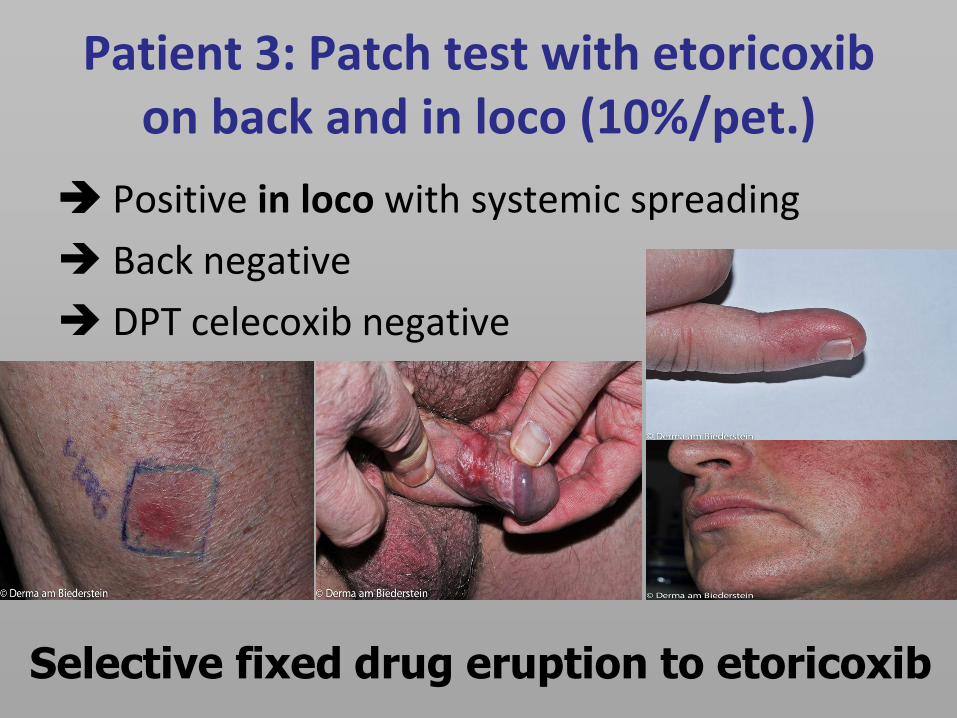
Patient 3: Patch test with etoricoxib on back and in loco (10%/pet.)
Positive in loco with systemic spreading
Back negative
DPT celecoxib negative
Selective fixed drug eruption to etoricoxib
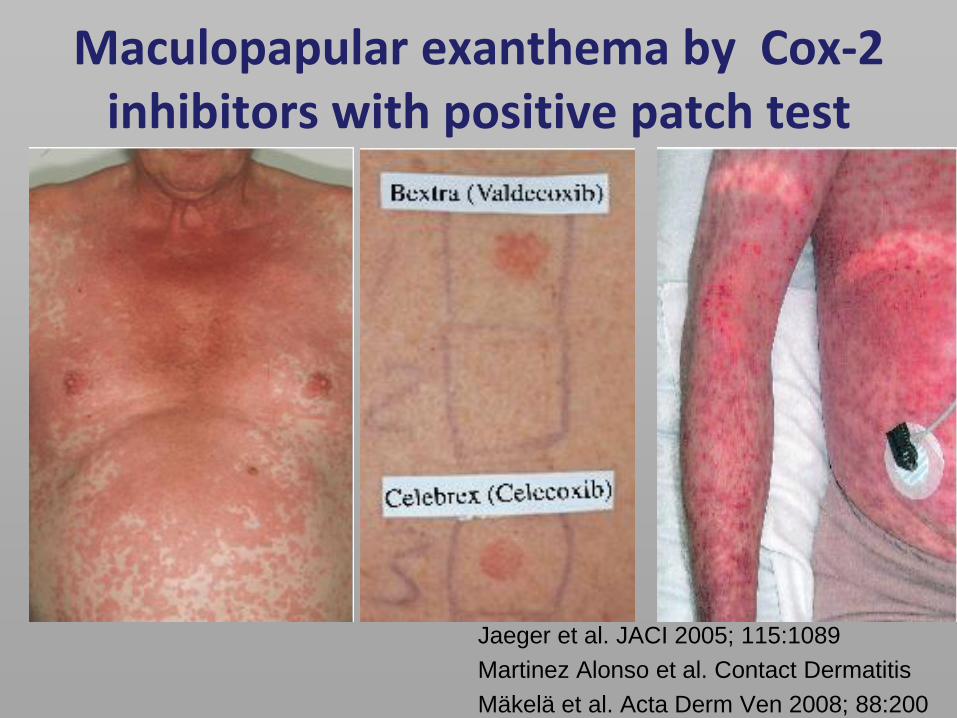
Maculopapular exanthema by Cox-2 inhibitors with positive patch test
Jaeger et al. JACI 2005; 115:1089
Martinez Alonso et al. Contact Dermatitis
Mäkelä et al. Acta Derm Ven 2008; 88:200
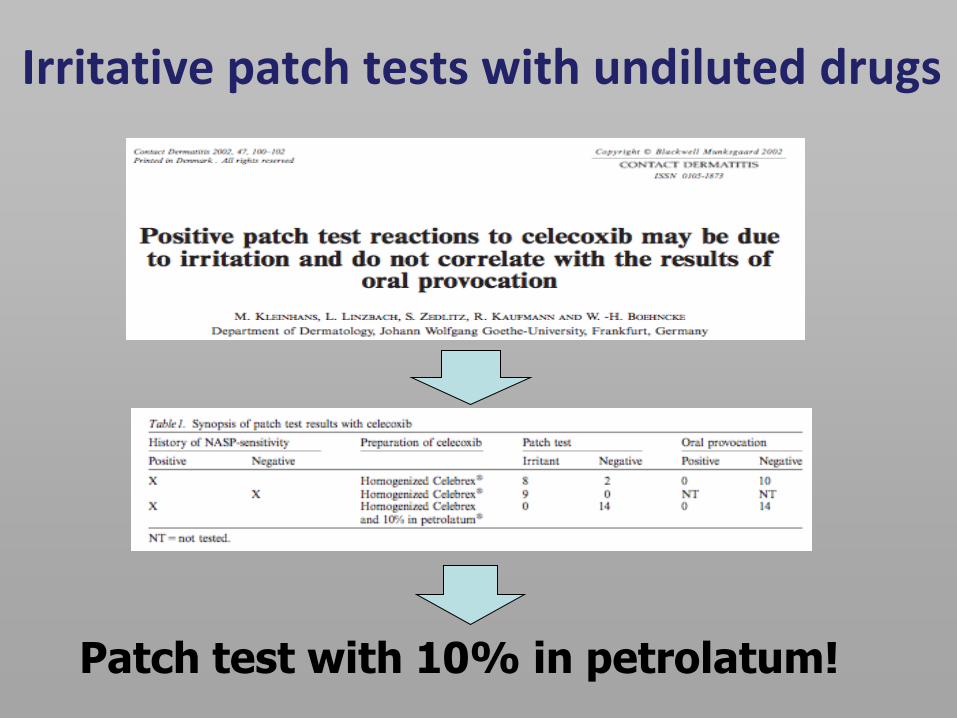
Patch test with 10% in petrolatum!
Irritative patch tests with undiluted drugs
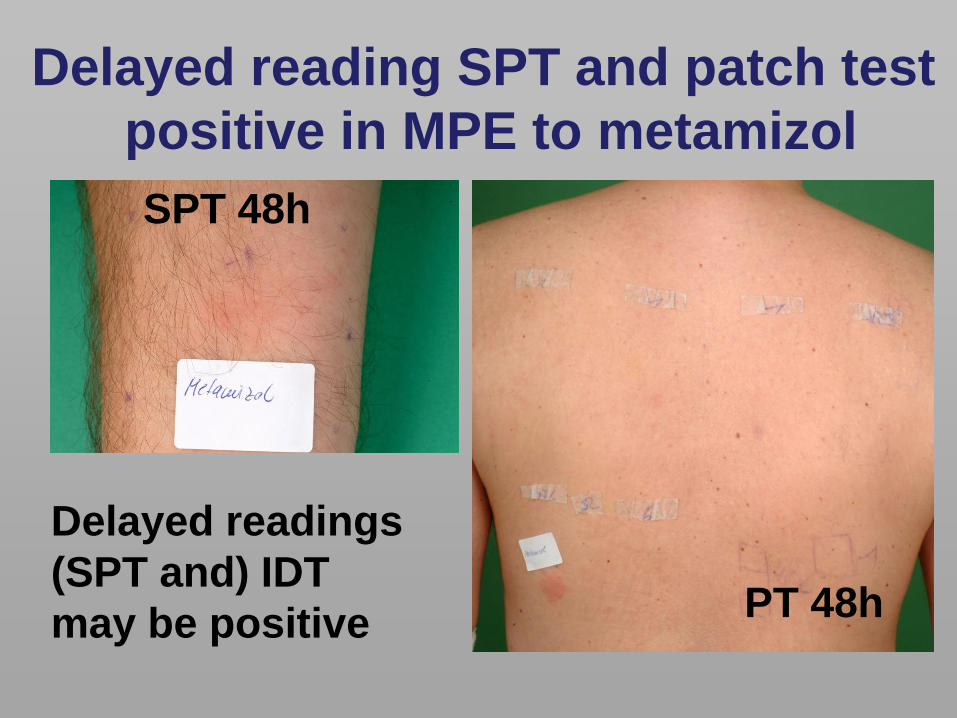
Delayed reading SPT and patch test
positive in MPE to metamizol
Delayed readings
(SPT and) IDT
may be positive
SPT 48h
PT 48h
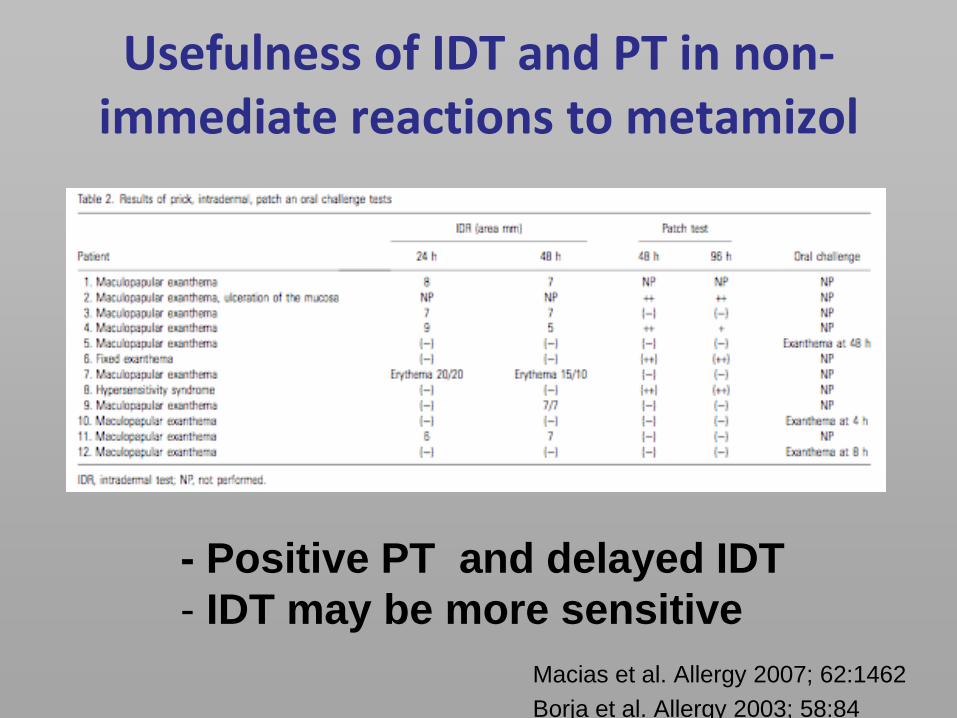
Usefulness of IDT and PT in non-immediate reactions to metamizol
Macias et al. Allergy 2007; 62:1462
Borja et al. Allergy 2003; 58:84
- Positive PT and delayed IDT
- IDT may be more sensitive
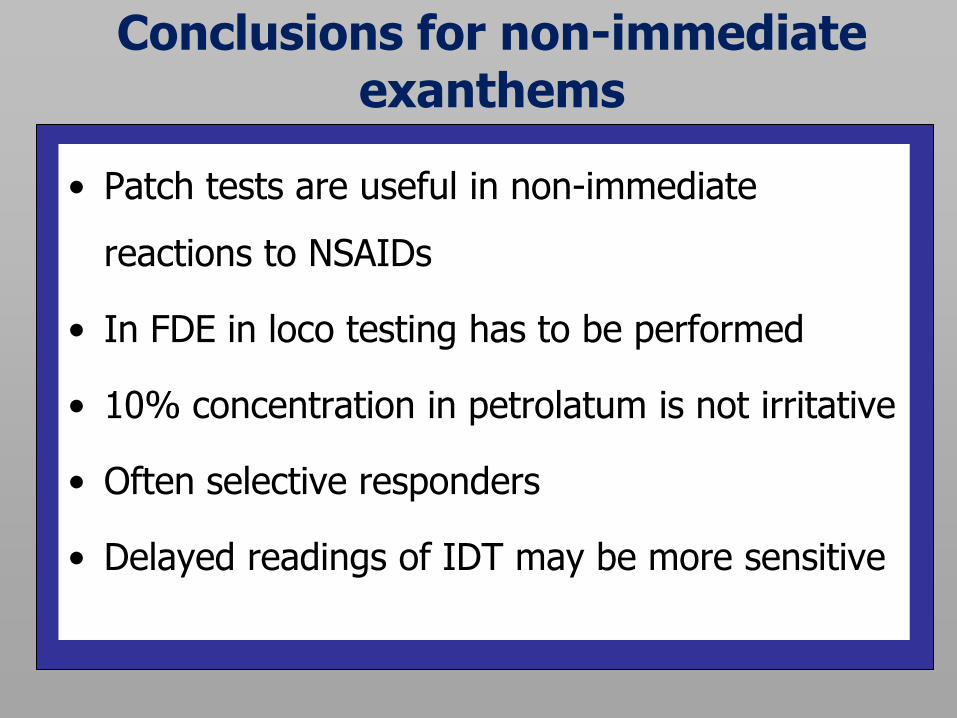
Conclusions for non-immediate exanthems
• Patch tests are useful in non-immediate
reactions to NSAIDs
• In FDE in loco testing has to be performed
• 10% concentration in petrolatum is not irritative
• Often selective responders
• Delayed readings of IDT may be more sensitive

Thank you very much for your attention!
![A Highly Sensitive and Selective Spectrofluorimetric ... · ic in drinking water was responsible to cause skin, lung and bladder cancer 5]. [Groundwater is the preferred source of](https://img.pdfslide.us/doc/110x75/5ea58a7395cf0b7ef0160bdf/a-highly-sensitive-and-selective-spectrofluorimetric-ic-in-drinking-water-was.jpg)