Embed Size (px)
Citation preview

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 1 of 16
THE USE OF DONOR BREAST MILK (DBM). NEONATAL CLINICAL GUIDELINE
Insufficient mothers own breast milk. AND
Infant meets criteria for DBM
Refer mother to Breast Feeding Support Nurse for lactation support
AND Obtain informed consent for DBM
Make up total feed volume with DBM and any available Expressed Breast Milk
(EBM)
Increase feed volume to optimal level for baby e.g. 150ml/kg
Feed tolerated for 48 hours
If infant is considered ‘very high risk’ continue DBM / EBM. Monitor growth. Seek diatetic review. ‘Very High Risk’ = <27 weeks or <1000g or Recovering from NEC
Introduce Formula Day 1 – ¼ formula Day 2 – ½ formula Day 3 – ¾ formula Day 4 – Full strength formula Babies <2.0 kg and <35 weeks use preterm formula. Babies >2.0 kg and >35 weeks use post discharge formula Increase proportion of formula as tolerated

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 2 of 16
1. Aim/Purpose of this Guideline 1.1. This guideline aims to
Outline the indications for the use of DBM to provide equity of use across the South West Neonatal Network.
To outline the transition from DBM to formula.
To outline the use, safe storage and traceability of DBM.
It applies to all staff caring for babies receiving DBM.
2. The Guidance 2.1 Background. A mother’s own breast milk is the best form of nourishment for a preterm infant, in preference to infant formula or donor breast milk. Every support should be given to help mothers produce milk for their baby. Early expression to stimulate hormonal response is crucial to good on-going supply However, in some rare situations maternal expressed breast milk is not available or able to be used. Potential Benefits.
Formula fed very low birth weight babies are at significantly increased risk of Necrotising Enterocolitis (NEC) when compared with infants exclusively fed breast milk. Data suggests that DBM reduces the risk of NEC by as much as 79%.
Potential Risks.
DBM is a human body fluid and, as such, carries risks of transmission of infective agents. Donors are screened and the milk is pasteurised to minimise risk. Written consent must be obtained for the use of DBM. Handling, testing and documentation of the milk in the Donor Milk Bank and specialist feed unit is carried out according to NICE Guidelines 2010.
DBM use should be a consultant led decision. There is however, currently a lack of evidence to guide its use. Ideally DBM should only be used to ‘test’ the gut of preterm infants when there is insufficient mother’s own milk. Once the infant is tolerating 150ml/kg of milk, if DBM is required to make up the required volume, preterm formula should be gradually substituted (see algorithm)
2.2. Indications. The decision to use DBM must be documented in the notes. If a mother’s own milk is not available or contra-indicated, use of DBM should be considered the gold standard for the following babies;
All babies less than or equal to 30 weeks gestation or less than 1500g (including multiples).

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 3 of 16
Babies less than or equal to 32 weeks gestation with consistently absent/reversed end diastolic flow.
Post NEC (medically and surgically treated)
Babies transferred on DBM from another unit.
Neonatal units may choose to use DBM in the following additional circumstances;
Babies less than or equal to 35 weeks gestation with growth restriction below 2nd centile.
Following circulatory collapse requiring complex resuscitation.
Haemodynamically unstable babies e.g. requiring or recently requiring inotropic support.
Preterm babies receiving medical treatment or awaiting surgical treatment for Patent Ductus Arteriosus.
Hypoxic Ischaemic Encephalopathy (moderate/severe).
NB. Due to the limited supply of DBM, babies who do not fulfil the above criteria should not be offered DBM even if it might be for a restricted period of time e.g. parents who themselves have allergies but who do not wish to use maternal breast milk (MBM) or standard formula; those babies requiring ‘top up feeds’. Breast feeding and lactation support should continue to be provided. If the donor milk bank has insufficient supplies of milk, DBM should be prioritised on a case by case basis within each individual unit.
2.3 Obtaining Consent. THIS MUST BE DOCUMENTED IN THE INFANTS MEDICAL / NURSING NOTES. The nurse or doctor caring for the infant should explain the rationale for using DBM. Written information about DBM is available in the UKAMB leaflet ‘Donor Breast Milk – your questions answered’. UKABM leaflets Written consent must be obtained from the mother to give DBM to the baby. This consent must be documented in the baby’s notes along with the mother’s feeding intention. (Appendix 7) A parent information sheet is available to support this discussion. (Appendix 8) If DBM has been consented to, a printable checklist (Appendix 9) is available to ensure correct procedures adhered to and documentation completed. 2.4 How to obtain Donor Breast Milk. Receiving hospitals should comply with relevant clinical governance standards pertaining to the traceability and storage of breast milk before using DBM. This is outlined in the NICE donor milk bank guidelines (http:/guidance.org.uk/CG93)

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 4 of 16
North Bristol Trust. (NBT). Human Milk Bank (Precious Drops)
Marion Copeland Heidi Evans
0117 3233527 [email protected] 0117 3232972 [email protected]
Southampton Human Milk Bank
Jess MacFarlane 02380796009 [email protected]
Oxford Human Milk Bank
Sally Inch 01865221695 [email protected]
Milk courier service. 'Bloodbikes' . http://www.milkbanks.co.uk/.
All DBM administered in the NHS should be from Milk Banks that can demonstrate adherence to the NICE guideline on the operating of DBM Banks.
2.5 Storage and Usage.
All DBM received from outside of the Neonatal Unit needs to be logged onto a DBM Log-In Sheet. (Appendix 4).
DBM should be stored as directed by the DBM bank and according to each unit’s policy for all frozen milk.
Milk can be kept in the freezer for 3 months, but not beyond the expiry date.
Milk should always arrive in a frozen state. This must be checked by the member of staff that receives the delivery.
Milk must be used within 24 hours of removal from the freezer for defrosting
2.6 Traceability
Each bottle of milk must be clearly labelled with a batch number and expiry date.
Once taken from the freezer the DBM should be labelled with the name and Hospital number of the baby who is to receive the milk, and the date and time it is removed from the freezer.
A DBM Log out sheet (Appendix 5) should be completed for every bottle of DBM taken from the freezer documenting the recipient’s name and hospital number together with the batch number of the DBM.
Each baby receiving DBM should have their own individual Donor Milk Record Sheet (Appendix 6) completed to include date, time, batch number and volume of milk given. This must be signed and countersigned by the nursing staff and the form kept in the baby’s hospital records.
2.7 Duration of the use of DBM.
DBM can be used for 1-3 weeks after introduction. Once the baby has tolerated 150mls/kg DBM for 48 hours, introduction of formula should be considered (see algorithm Appendix 3)

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 5 of 16
Formula milk should be blended with DBM ¼ then ½ then ¾ strength until full strength is tolerated (see algorithm Appendix 3)
Babies <35 weeks and <2.0 kg should have preterm formula.
Preterm babies >2.0 kg and >35 weeks should have post discharge formula.
2.8 Fortification of DBM. DBM can be fortified but it is preferable to move onto preterm formula once 150ml/kg is tolerated for >48 hours. 2.9 Babies transferred to other units
A clear feeding plan should be agreed between the referral and receiving units before transfer. If the receiving hospital is not able to accept the baby on DBM, the baby should be re-graded onto formula as soon as possible before the transfer. If the hospital does accept babies on DBM then a small supply of DBM should be transferred with the infant. It is the responsibility of the receiving hospital to liaise with the established Donor Milk Bank for further supplies of DBM.
3. Monitoring compliance and effectiveness
Element to be monitored
Key changes to practice
Lead Dr. Paul Munyard
Tool Audit
Frequency As dictated by audit findings
Reporting arrangements
Child health Directorate Audit and Neonatal Clinical Guidelines Group
Acting on recommendations and Lead(s)
Dr. Paul Munyard. Consultant Paediatrician and Neonatologist
Change in practice and lessons to be shared
Required changes to practice will be identified and actioned within 3 months. A lead member of the team will be identified to take each change forward where appropriate. Lessons will be shared with all the relevant stakeholders

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 6 of 16
4. Equality and Diversity 4.1. This document complies with the Royal Cornwall Hospitals NHS Trust service Equality and Diversity statement which can be found in the 'Equality, Diversity & Human Rights Policy' or the Equality and Diversity website.
4.2. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.
Appendix 1. Governance Information
Document Title Donor Breast Milk (DBM) – Neonatal Clinical Guideline
Date Issued/Approved: March 2016
Date Valid From: JUNE 2016
Date Valid To: JUNE 2019
Directorate / Department responsible (author/owner):
Dr. Paul Munyard. Child Health. Neonatal
Contact details: 01872 252667
Brief summary of contents
This guideline aims to outline the indications for the use of Donor Breast Milk to provide equity of use across the South West Neonatal Network. To outline the transition from DBM to formula. To outline the use, safe storage and traceability of DBM.
Suggested Keywords: Neonatal. Donor Expressed Breast Milk. DEBM. DBM
Target Audience RCHT PCH CFT KCCG
Executive Director responsible for Policy:
Medical Director
Date revised: 25:05:2016
This document replaces (exact title of previous version):
New Document
Approval route (names of committees)/consultation:
Consultant Approval Child health Directorate Audit Neonatal Clinical Guidelines Group

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 7 of 16
Divisional Manager confirming approval processes
David Smith
Name and Post Title of additional signatories
Not Required
Signature of Executive Director giving approval
{Original Copy Signed}
Publication Location (refer to Policy on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Document Library Folder/Sub Folder Neonatal. Clinical. Child Health
Links to key external standards Governance Team can advise
Related Documents:
Donor Breast Milk Banks: the operation of donor milk bank services (2010) NICE guidance. CG93. Western Neonatal Network Guidelines Group – SW Neonatal Networks Guideline for the use of Donor Breast Milk www.ukamb.org
Training Need Identified? No
Version Control Table
Date Version No
Summary of Changes Changes Made by
(Name and Job Title)
20:12:15 V1.0 Initial Issue Neonatal Guidelines Group
21:01:16 V2.0 Addition of appendices Neonatal Guidelines Group
All or part of this document can be released under the Freedom of Information Act 2000
This document is to be retained for 10 years from the date of expiry.
This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust Policy on Document Production. It should not be altered in any way without the
express permission of the author or their Line Manager.

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 8 of 16
Appendix 2. Initial Equality Impact Assessment Form
Are there concerns that the policy could have differential impact on: Equality Strands: Yes No Rationale for Assessment / Existing Evidence
Age x
Name of the strategy / policy /proposal / service function to be assessed (hereafter referred to as policy) (Provide brief description): Donor Breast Milk (DBM). Neonatal Clinical Guideline
Directorate and service area: Child and Women’s Health. Neonatal
Is this a new or existing Policy? New
Name of individual completing assessment: Paul Munyard
Telephone: 01872 252667
1. Policy Aim* Who is the strategy / policy / proposal / service function aimed at?
This guideline is aimed at clinical staff responsible for the nutritional care of hospitalised infants.
2. Policy Objectives*
As above
3. Policy – intended Outcomes*
Audit
4. *How will you measure the outcome?
Audit
5. Who is intended to benefit from the policy?
Neonatal Patients Neonatal nursing and medical staff
6a) Is consultation required with the workforce, equality groups, local interest groups etc. around this policy? b) If yes, have these *groups been consulted? C). Please list any groups who have been consulted about this procedure.
No. Neonatal Guidelines Group Consultant approved guideline.
7. The Impact Please complete the following table.

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 9 of 16
Sex (male, female, trans-
gender / gender reassignment)
x
Race / Ethnic communities /groups
x
Disability - learning disability, physical disability, sensory impairment and mental health problems
x
Religion / other beliefs
x
Marriage and civil partnership
x
Pregnancy and maternity x
Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian
x
You will need to continue to a full Equality Impact Assessment if the following have been highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies which have been identified as not requiring consultation. or
Major service redesign or development
8. Please indicate if a full equality analysis is recommended. No
9. If you are not recommending a Full Impact assessment please explain why.
No area indicated
Signature of policy developer / lead manager / director Paul Munyard
Date of completion and submission 01:06:2016
Names and signatures of members carrying out the Screening Assessment
1. 2.
Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead, c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa, Truro, Cornwall, TR1 3HD A summary of the results will be published on the Trust’s web site. Signed _______kim smith________ Date _________01:06:2016_______
Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 10 of 16
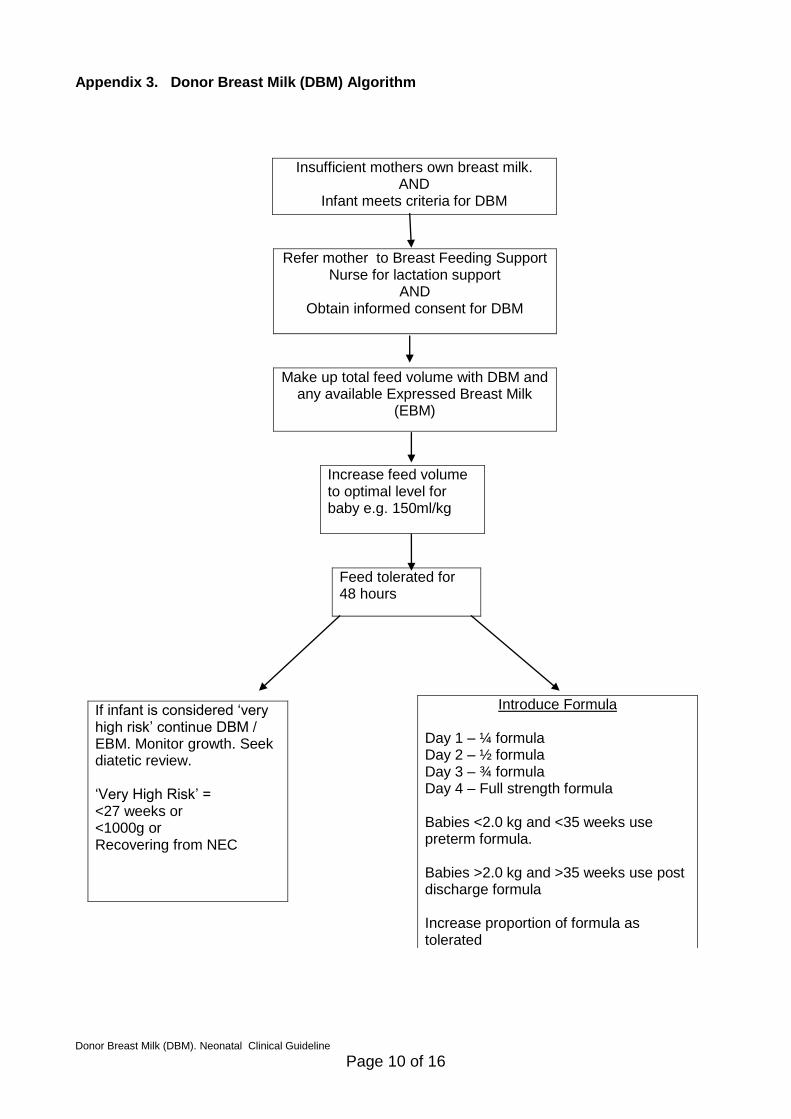
Appendix 3. Donor Breast Milk (DBM) Algorithm
Insufficient mothers own breast milk. AND
Infant meets criteria for DBM
Refer mother to Breast Feeding Support Nurse for lactation support
AND Obtain informed consent for DBM
Make up total feed volume with DBM and any available Expressed Breast Milk
(EBM)
Increase feed volume to optimal level for baby e.g. 150ml/kg
Feed tolerated for 48 hours
If infant is considered ‘very high risk’ continue DBM / EBM. Monitor growth. Seek diatetic review. ‘Very High Risk’ = <27 weeks or <1000g or Recovering from NEC
Introduce Formula Day 1 – ¼ formula Day 2 – ½ formula Day 3 – ¾ formula Day 4 – Full strength formula Babies <2.0 kg and <35 weeks use preterm formula. Babies >2.0 kg and >35 weeks use post discharge formula Increase proportion of formula as tolerated

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 11 of 16
Appendix 4. Donor Breast Milk, Log-In Sheet. For DBM accepted onto Neonatal Unit from DBM Bank or referring hospital. Completed form to be kept in DBM Folder in Nurses Office.
Donor Breast Milk Log-In Sheet
Date/Time DBM received onto the NNU
DBM Bank/ Hospital generating delivery
Batch number of bottles
Number of bottles received
Integrity of DBM. Each bottle should be checked to ensure frozen
Signature and name of receiving nurse

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 12 of 16
Appendix 5. Donor Breast Milk Log-Out Sheet. Completed form to be kept in DBM Folder, in Nurses Office.
Donor Breast Milk Log-Out Sheet
Date/Time DBM removed from freezer
Batch number Number of bottles taken
Recipients name and hospital number
Signature and Name.
Please attach baby’s label here
Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 13 of 16
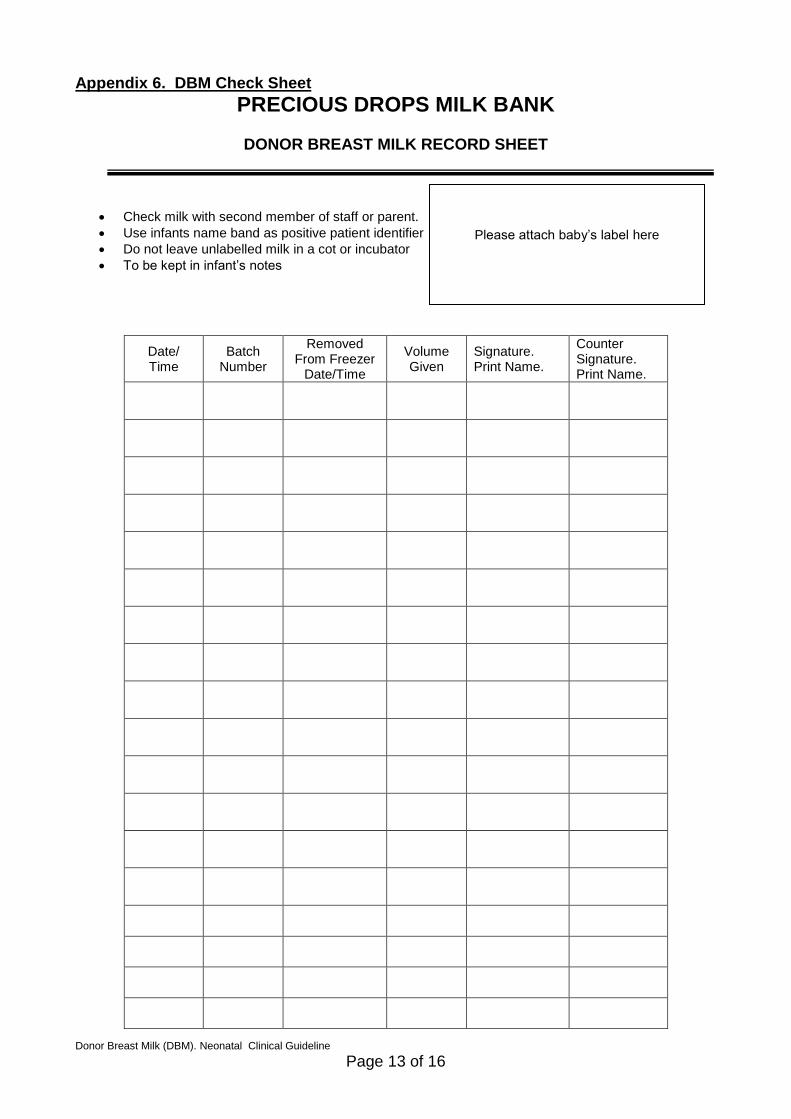
Appendix 6. DBM Check Sheet
PRECIOUS DROPS MILK BANK
DONOR BREAST MILK RECORD SHEET
Check milk with second member of staff or parent.
Use infants name band as positive patient identifier
Do not leave unlabelled milk in a cot or incubator
To be kept in infant’s notes
Date/ Time
Batch Number
Removed From Freezer
Date/Time
Volume Given
Signature. Print Name.
Counter Signature. Print Name.
Please attach baby’s label here

Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 14 of 16
Appendix 7. Donor Breast Milk Consent Form
PRECIOUS DROPS MILK BANK
DONOR BREAST MILK CONSENT FORM (RECIPIENT)
This form to be completed when Health Professional is giving donor milk to a baby
This Sheet MUST be filed in recipient’s case notes for tracking
The decision to start using donor breast milk has been documented by a doctor in the baby’s medical notes YES/NO I (name)………………………….. ………….have read the leaflet ‘Donor Breast Milk’ and give consent for my baby …………………………... ………… to receive donor breast milk. Signed………………………….. Date……………………….. Relationship to baby ……………………… I (name)………………………….….confirm that I have discussed the use of Donor Milk and have answered all questions and concerns. Signed…………………………..…Date………………………… Job Title…………………………………..
Please attach baby’s label here
Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 15 of 16
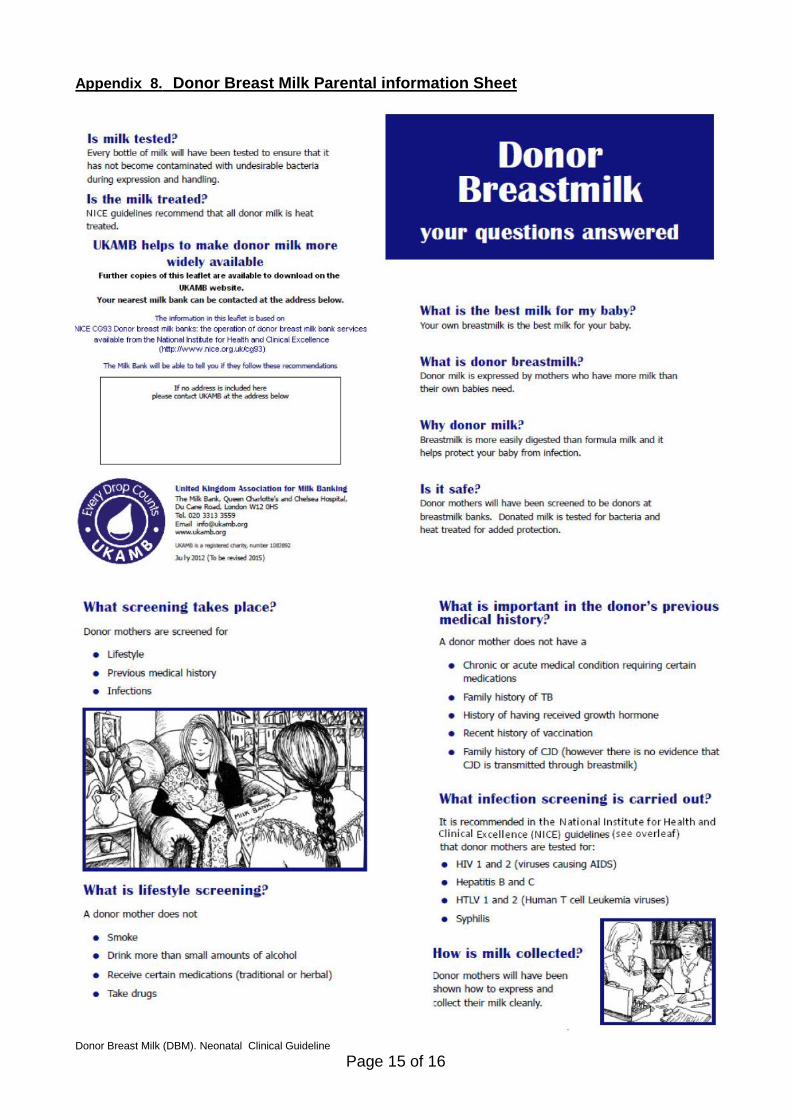
Appendix 8. Donor Breast Milk Parental information Sheet
Donor Breast Milk (DBM). Neonatal Clinical Guideline
Page 16 of 16
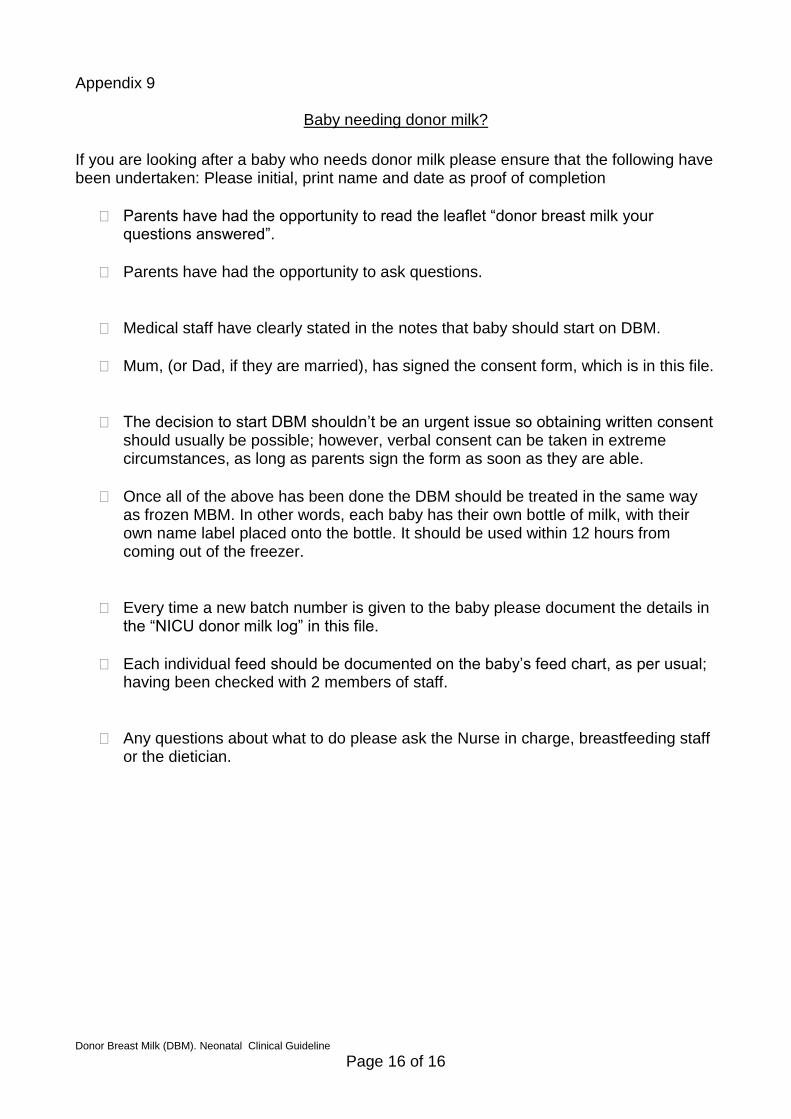
Appendix 9
Baby needing donor milk?
If you are looking after a baby who needs donor milk please ensure that the following have been undertaken: Please initial, print name and date as proof of completion
Parents have had the opportunity to read the leaflet “donor breast milk your questions answered”.
Parents have had the opportunity to ask questions.
Medical staff have clearly stated in the notes that baby should start on DBM.
Mum, (or Dad, if they are married), has signed the consent form, which is in this file.
The decision to start DBM shouldn’t be an urgent issue so obtaining written consent should usually be possible; however, verbal consent can be taken in extreme circumstances, as long as parents sign the form as soon as they are able.
Once all of the above has been done the DBM should be treated in the same way as frozen MBM. In other words, each baby has their own bottle of milk, with their own name label placed onto the bottle. It should be used within 12 hours from coming out of the freezer.
Every time a new batch number is given to the baby please document the details in the “NICU donor milk log” in this file.
Each individual feed should be documented on the baby’s feed chart, as per usual; having been checked with 2 members of staff.
Any questions about what to do please ask the Nurse in charge, breastfeeding staff or the dietician.





























