Embed Size (px)
Citation preview
The use of Aspergillus nidulans to identify the genetic defect responsible
for the human metabolic disorders Alkaptonuria and Type I Tyrosinemia.
A slide set provided by Prof Miguel A Penalva
Centro de Investigaciones Biologicas del CSIC, Madrid 28006, Spain.

Alkaptonuria is a rare genetic disorder. The discovery of the gene responsible for alkaptonuria and a number of genes responsible for human inborn errors of metabolism, have exploited the mold Aspergillus nidulans.
This fungus has the experimental advantages of:
• rapid growth
• easy genetic manipulation
• growth requirements that are readily manipulated
• this filamentous fungi happens to share the same pathway of aromatic amino acid metabolism as humans, lending itself exquisitely to their study.
Aspergillus nidulans –a useful genetic model.
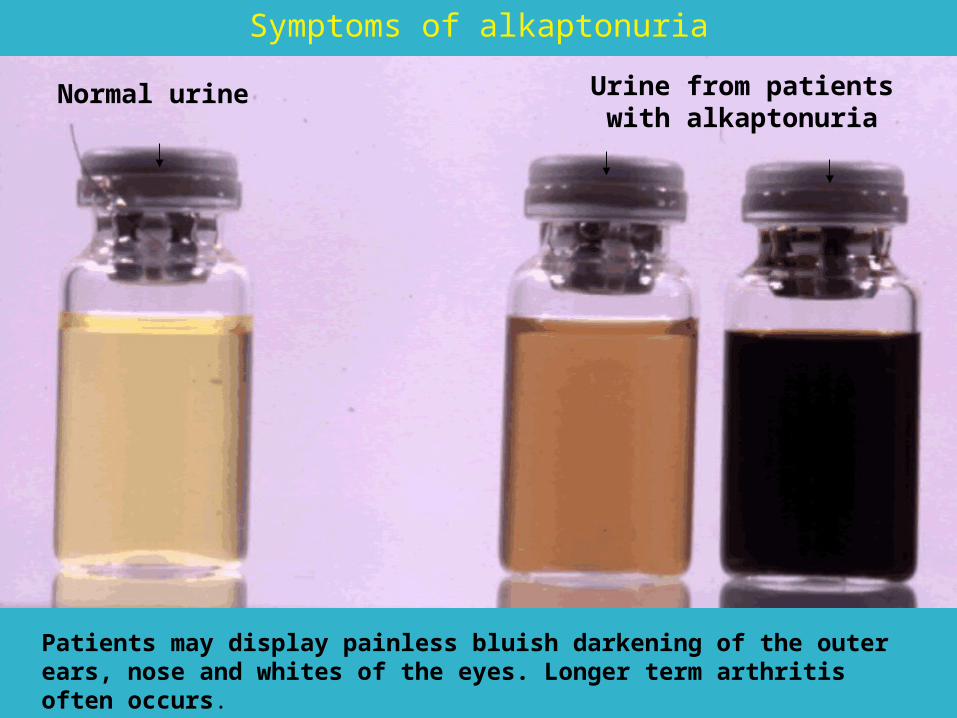
Normal urine Urine from patients with alkaptonuria
Symptoms of alkaptonuria
Patients may display painless bluish darkening of the outer ears, nose and whites of the eyes. Longer term arthritis often occurs.
OH
OH
CH2
COOH
HGO
homogentisic acid
CH CH
C
O
CH2
C
O
CH2 COOH
maleylacetoacetic acid
HOOC
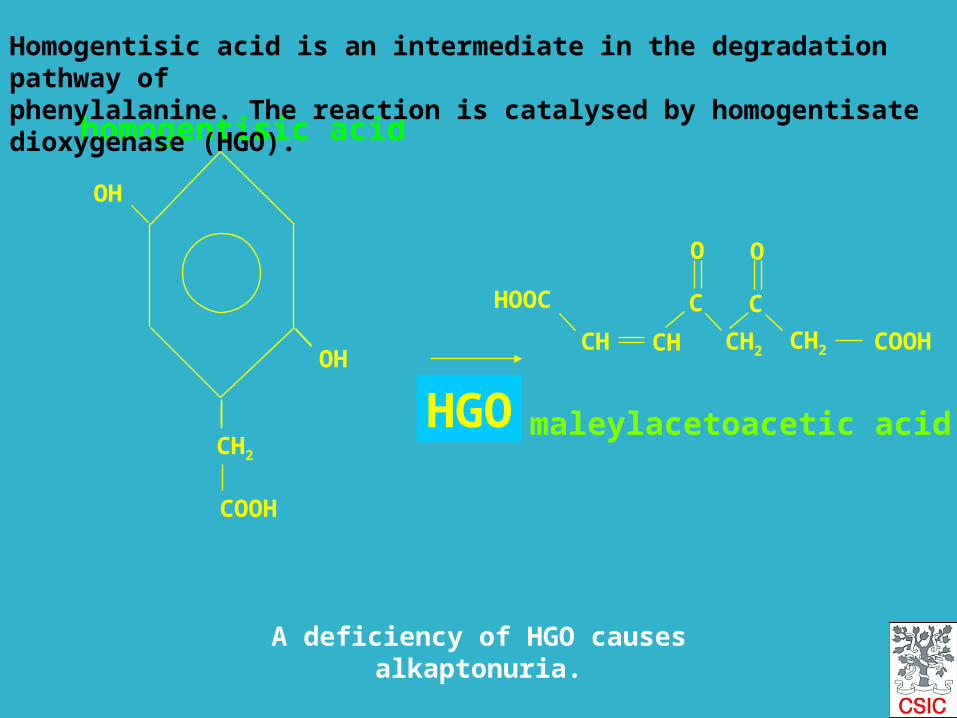
Homogentisic acid is an intermediate in the degradation pathway of phenylalanine. The reaction is catalysed by homogentisate dioxygenase (HGO).
A deficiency of HGO causes alkaptonuria.

Defect here causes Type I Tyrosinemia
Defect here causes alkaptonuria
Catabolic pathway for phenylalanine and tyrosine
Homogentisate dioxygenase
Fumarylacetoacetate hydrolase
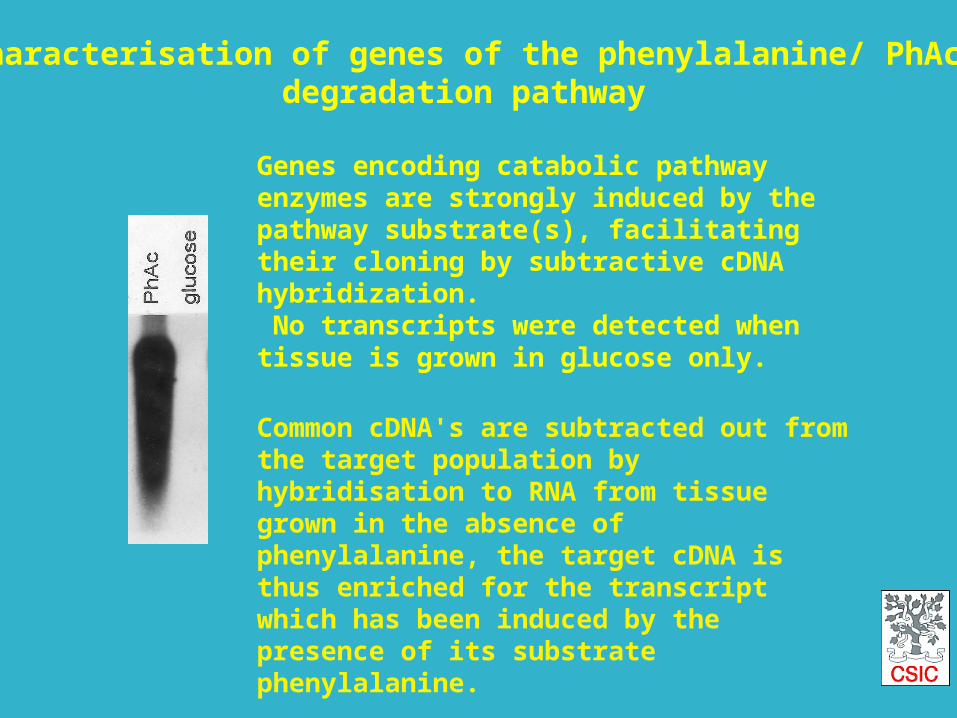
Genes encoding catabolic pathway enzymes are strongly induced by the pathway substrate(s), facilitating their cloning by subtractive cDNA hybridization. No transcripts were detected when tissue is grown in glucose only.
Common cDNA's are subtracted out from the target population by hybridisation to RNA from tissue grown in the absence of phenylalanine, the target cDNA is thus enriched for the transcript which has been induced by the presence of its substrate phenylalanine.
Characterisation of genes of the phenylalanine/ PhAcdegradation pathway
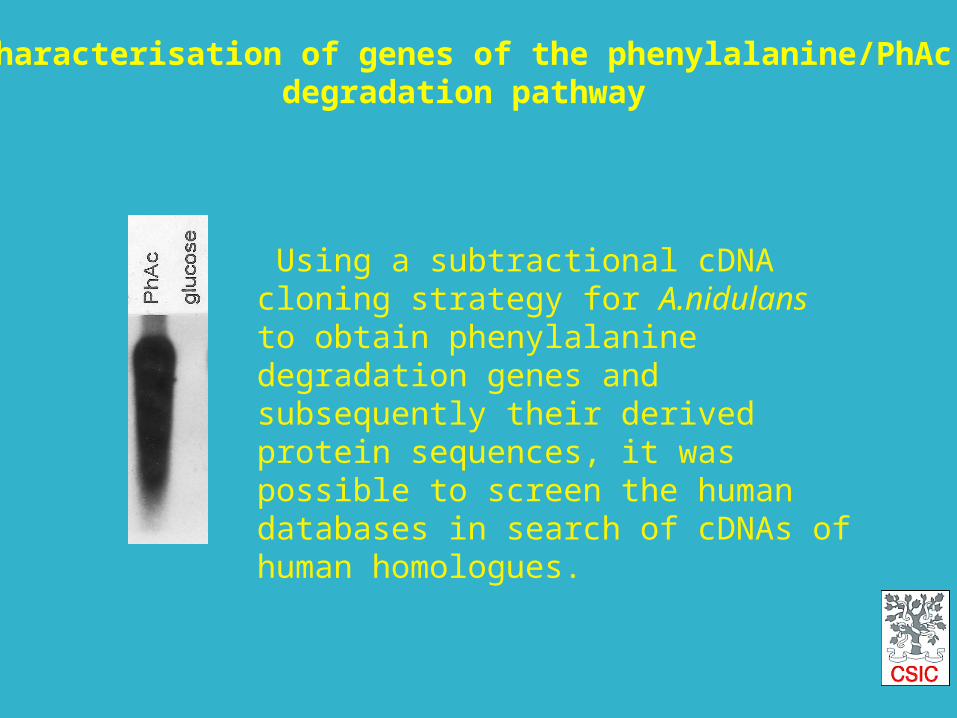
Using a subtractional cDNA cloning strategy for A.nidulans to obtain phenylalanine degradation genes and subsequently their derived protein sequences, it was possible to screen the human databases in search of cDNAs of human homologues.
Characterisation of genes of the phenylalanine/PhAcdegradation pathway
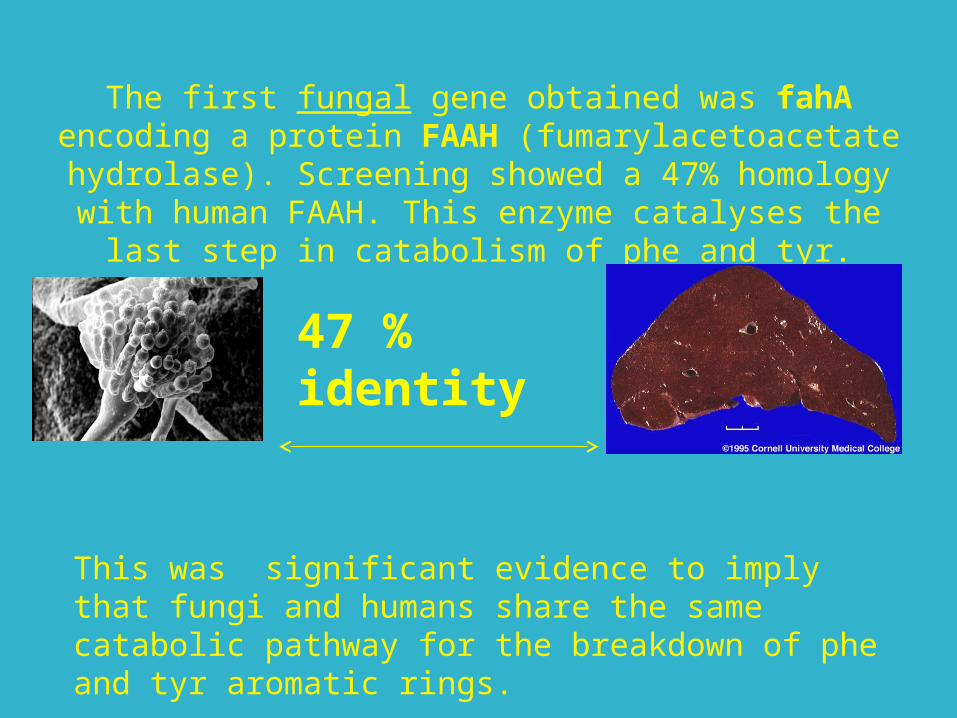
47 % identity
The first fungal gene obtained was fahA encoding a protein FAAH (fumarylacetoacetate hydrolase).
Screening showed a 47% homology with human FAAH. This enzyme catalyses the last step in catabolism of
phe and tyr.
This was significant evidence to imply that fungi and humans share the same catabolic pathway for the breakdown of phe and tyr aromatic rings.
HOOC
CH CH
C
O
CH2
C
O
CH2 COOH
HOOC
CH CH CH2 COOH
C
O
CH2
C
O
maleylacetoacetic acid
Fumarate + acetoacetate
HOOC - CH2 - CH2 - C - CH2 - C - CH2 -
= =O O
COOH
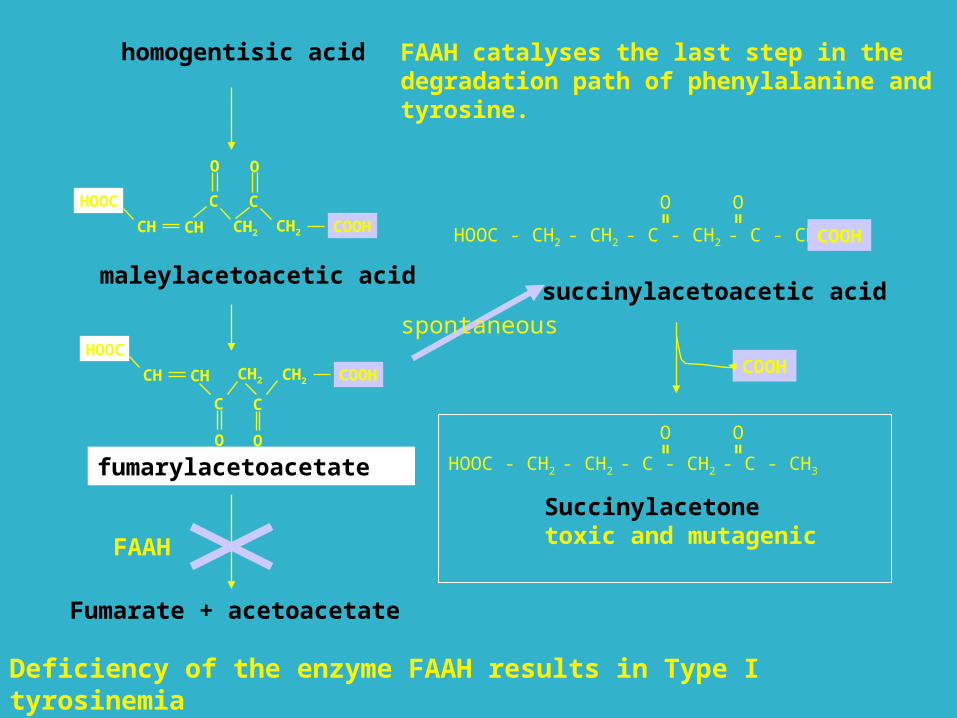
succinylacetoacetic acid
HOOC - CH2 - CH2 - C - CH2 - C - CH3
= =O O
COOH
Succinylacetonetoxic and mutagenic
homogentisic acid
Deficiency of the enzyme FAAH results in Type I tyrosinemia
FAAH catalyses the last step in the degradation path of phenylalanine and tyrosine.
fumarylacetoacetate
spontaneous
FAAH
WHAT ARE THE SYMPTOMS OF TYROSINEMIA? The clinical features of the disease ten to fall into two categories, acute and chronic.In the so-called acute form of the disease, abnormalities appear in the first month of life. Babies may show poor weight gain, an enlarged liver and spleen, a distended abdomen, swelling of the legs, and an increased tendency to bleeding, particularly nose bleeds. Jaundice may or may not be prominent. Despite vigorous therapy, death from hepatic failure frequently occurs between three and nine months of age unless a liver transplantation is performed.
Tyrosinemia is diagnosed by a blood and urine test. Tyrosinemia is treated by a low protein diet (low in phenylalanine, methionine and tyrosine) and a drug called NTCB.
But the search for the defective enzyme responsible for alkaptonuria was still on.
•In TBLASTIN searches of the human EST database the amino acid sequence of fungal HGO identified candidate cDNAs for human HGO.
•Most of these ESTs, which represent a single transcript, came from liver cDNA libraries.
•The human protein encoded by this transcript showed 52% homology to fungal HGO and when expressed in bacteria it gave HGO activity.
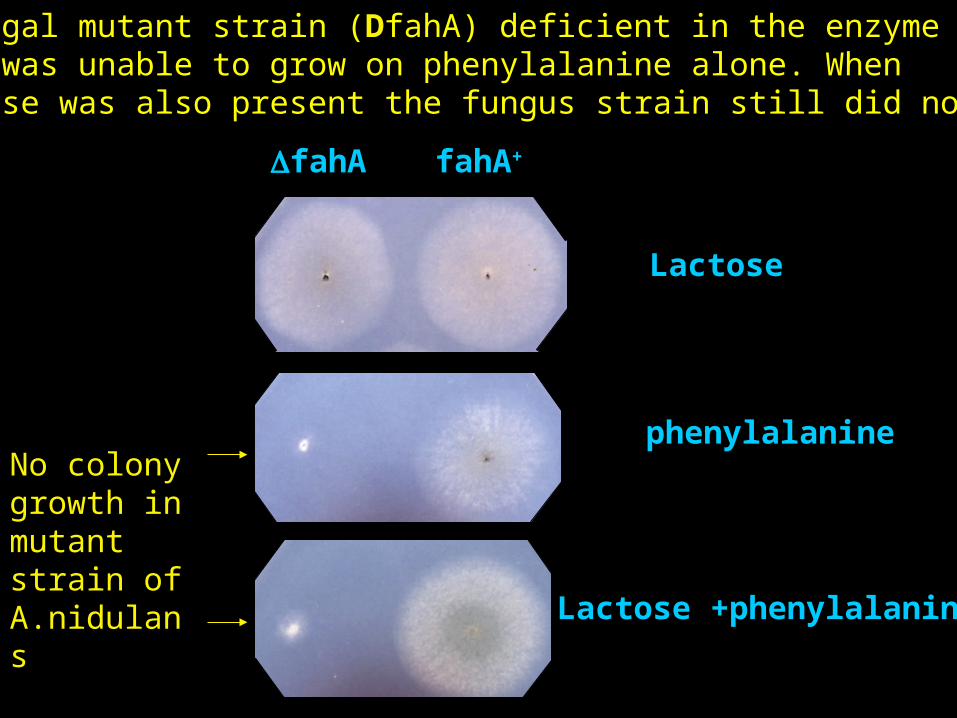
Lactose
phenylalanine
Lactose +phenylalanine
fahA fahA+
A fungal mutant strain (DfahA) deficient in the enzyme FAAH was unable to grow on phenylalanine alone. When lactose was also present the fungus strain still did not grow
No colony growth in mutant strain of A.nidulans
Then further colonies of the FAAH deficient strain developed which had resistance to the toxic
phenylalanine.
It was thought that other enzyme mutations upstream from FAAH were responsible.

Lac + Phe
lactose
Phe
fahA
Wild type
fahA hmgA-
Phe
Tyr
pHPP
HGA
MAA
FAA
F + AcAc
The double mutant colonies were able to grow in the presence of phenylalanine and secreted a brown pigment identified as homogentisate.
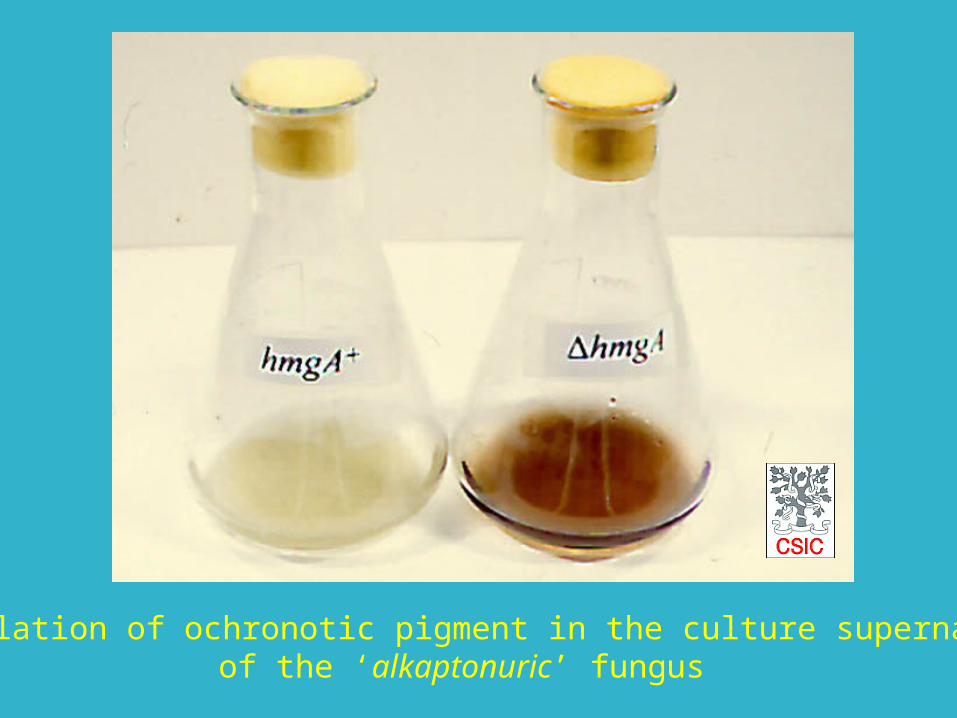
Accumulation of ochronotic pigment in the culture supernatantof the ‘alkaptonuric’ fungus
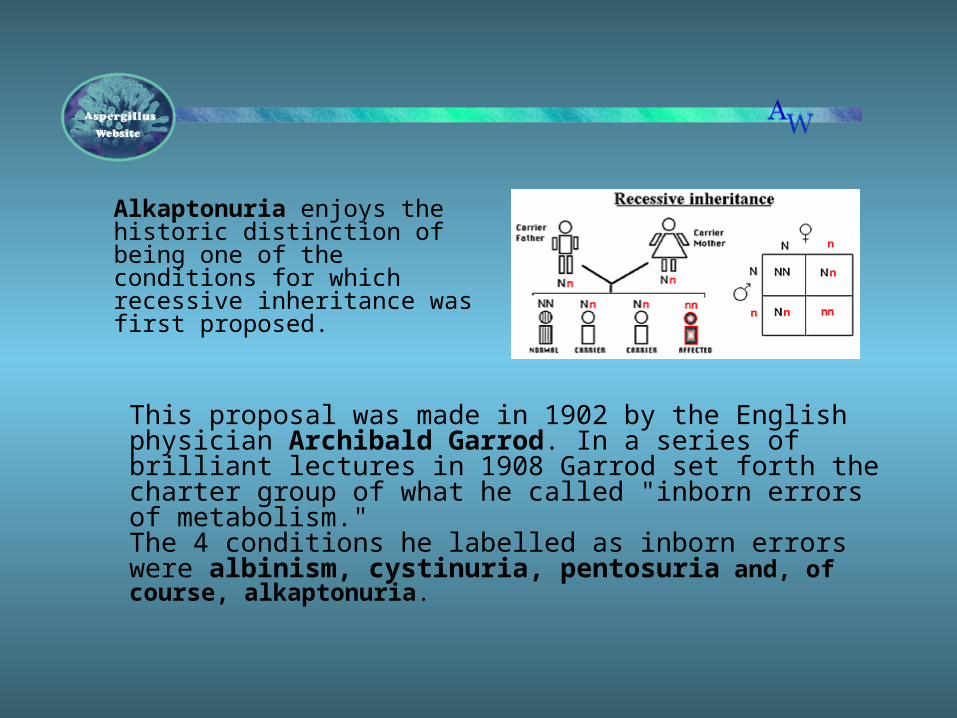
Alkaptonuria enjoys the historic distinction of being one of the conditions for which recessive inheritance was first proposed.
This proposal was made in 1902 by the English physician Archibald Garrod. In a series of brilliant lectures in 1908 Garrod set forth the charter group of what he called "inborn errors of metabolism." The 4 conditions he labelled as inborn errors were albinism, cystinuria, pentosuria and, of course, alkaptonuria.
These slides were adapted from material kindly provided by Miguel A Penalva, Centro de Investigaciones Biologicas del CSIC, Madrid 28006, Spain.
With acknowedgement of the following people;Santiago Rodríguez de CórdobaMagdalena UgarteDavid TimmJosé M. Fernández CañónJosé M. Rodríguez Rodríguez



![In Vivo Correction of Murine Tyrosinemia Type I by DNA ...web.stanford.edu/group/markkaylab/publications/12498772.pdf · model of hereditary tyrosinemia type 1 (HT1) [19], be-cause](https://img.pdfslide.us/doc/110x75/5fadaef398034276572c5af9/in-vivo-correction-of-murine-tyrosinemia-type-i-by-dna-web-model-of-hereditary.jpg)

























