Embed Size (px)
Citation preview
The Tripodal Foundation For Success in Crown and Bridges
Shankar Iyer DDS, MDSClin Asst. Prof. NYU
Clin Asst. Prof. UMDNJ
Bio-EstheticFixed Restorations
Restoring Form and Function

The Tripodal Foundation
TheBio-EstheticRestoration
ToothPreps The
InterimRestoration
SoftTissues

Commonly encountered clinical problems
Recession and exposed margins
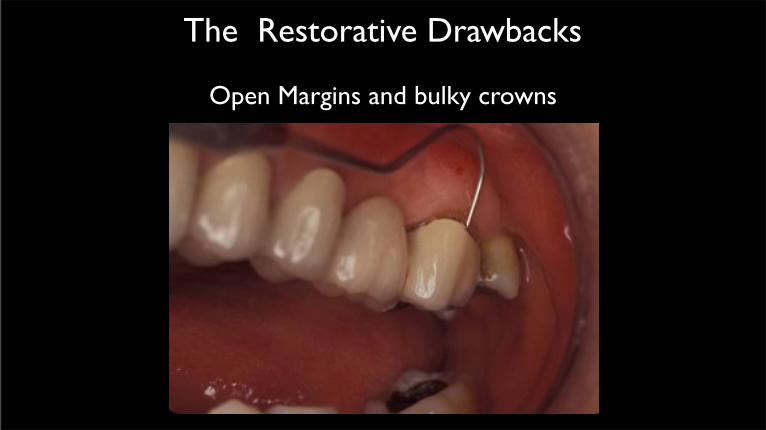
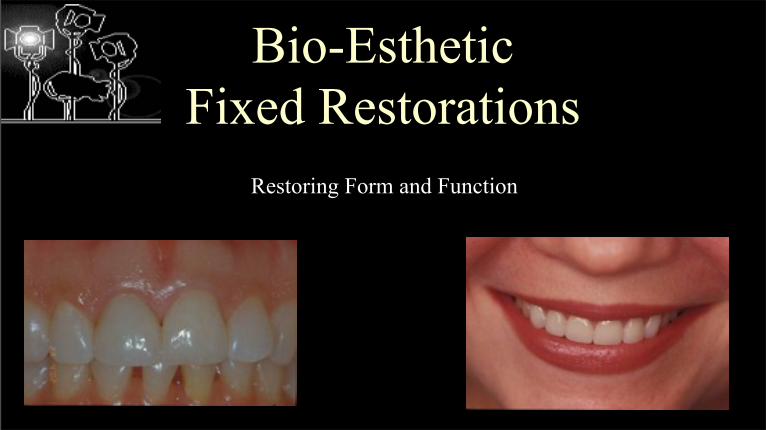
The Restorative Drawbacks
Open Margins and bulky crowns
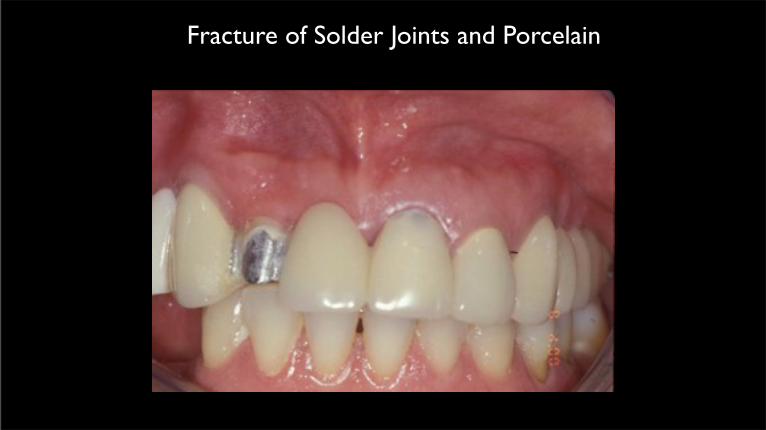
Fracture of Solder Joints and Porcelain
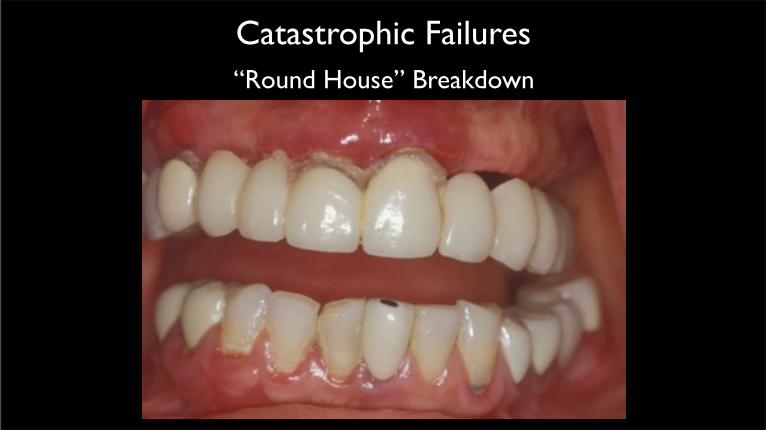
Catastrophic Failures
“Round House” Breakdown
Principles of Fixed Prosthesis
• Accommodation of Restorations(Tooth Preparation)
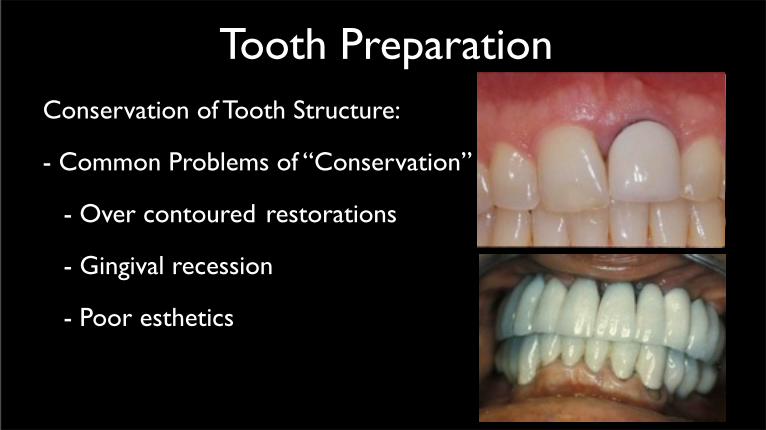
Tooth Preparation • Conservation of Tooth Structure:
- Common Problems of “Conservation”
- Over contoured restorations
- Gingival recession
- Poor esthetics
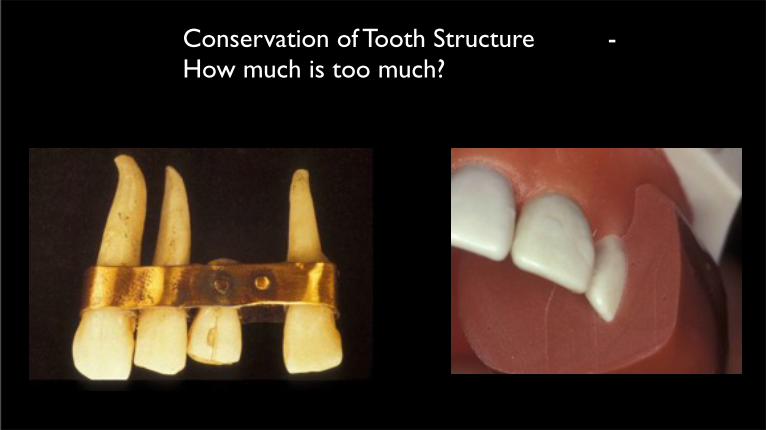
• Conservation of Tooth Structure - How much is too much?

•Depth Orientation Grooves
•Cl I / II Cavity Prep

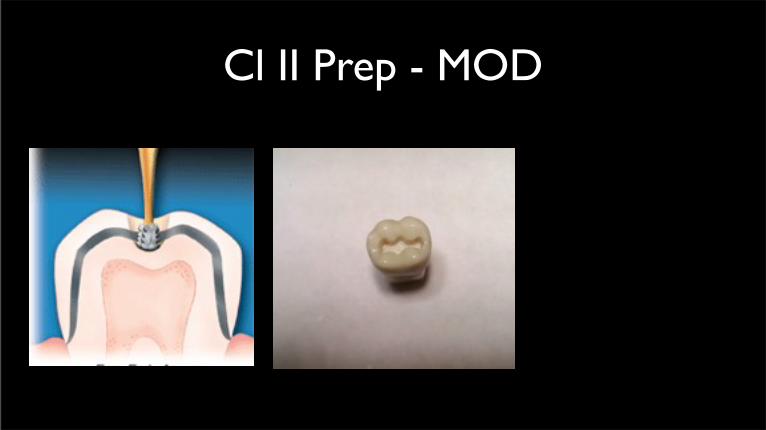
Cl II Prep - MOD
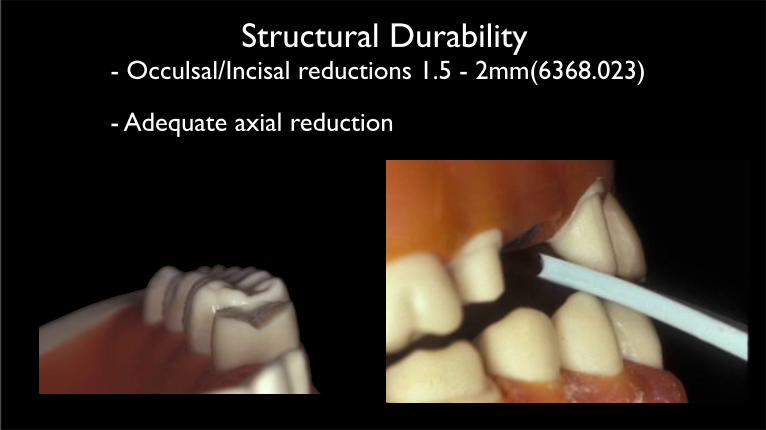
Structural Durability
- Occulsal/Incisal reductions 1.5 - 2mm(6368.023)
- Adequate axial reduction
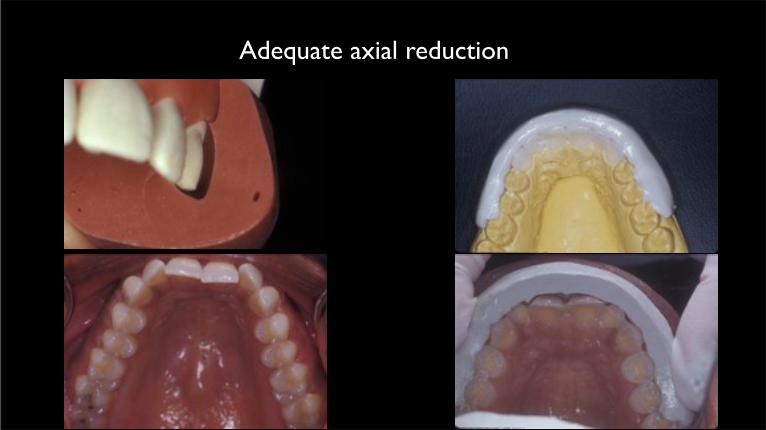
Adequate axial reduction

Retention Forms - Factors affecting retention:
Nearly parallel walls
- 6 - 9o taper100-150
240
• Resistance Forms
- Arc of rotation
- long preparations
- grooves and boxes
- increased surface area
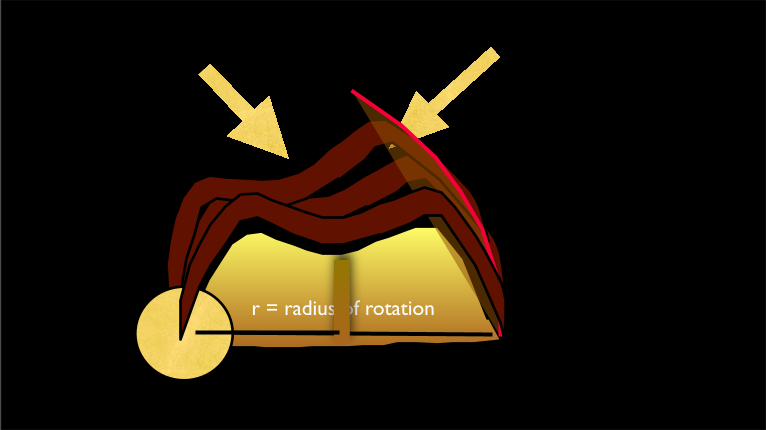
r = radius of rotation

• Marginal Integrity
- Choice of finish lines
Factors:
* type of restoration

• Marginal Integrity
- Choice of finish lines
* anterior or posterior teeth

• Marginal Integrity
- Choice of finish lines
Factors:
* condition of tooth
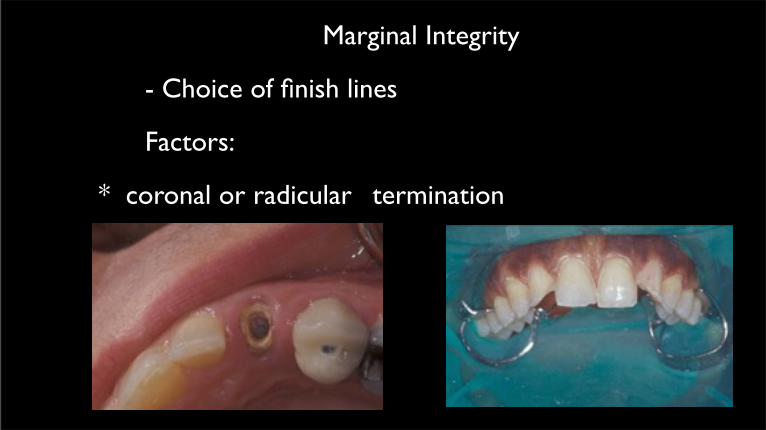
• Marginal Integrity
- Choice of finish lines
Factors:
* coronal or radicular termination

The Main Factor: Tissue Biotype

“The Tissue is The Issue”



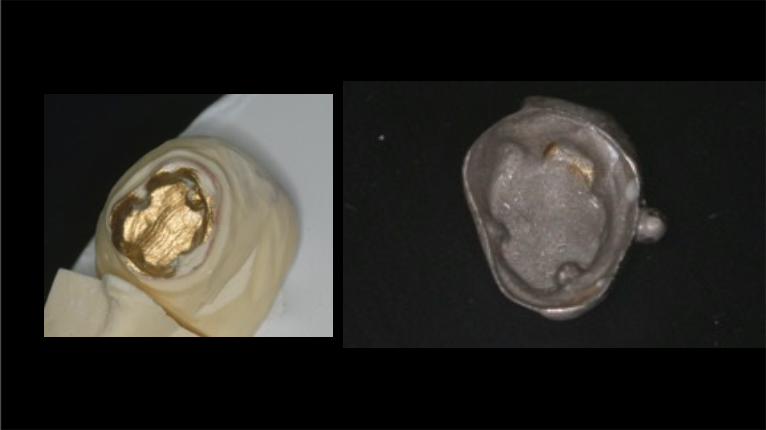
The Ferrule Effect!

Ferrules
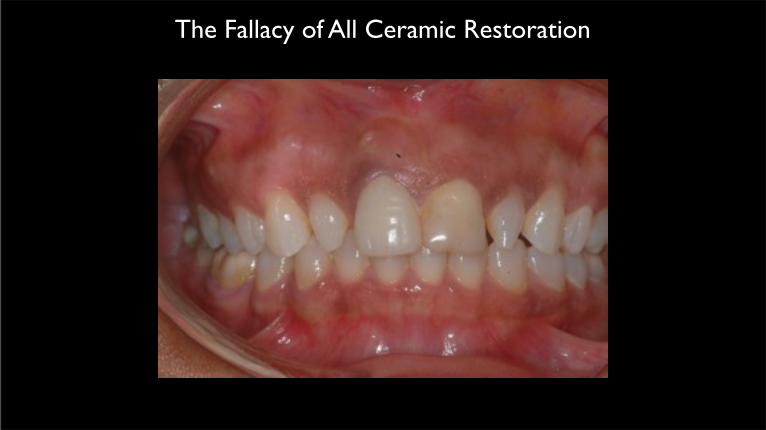
The Fallacy of All Ceramic Restoration

The Ferrule Effect
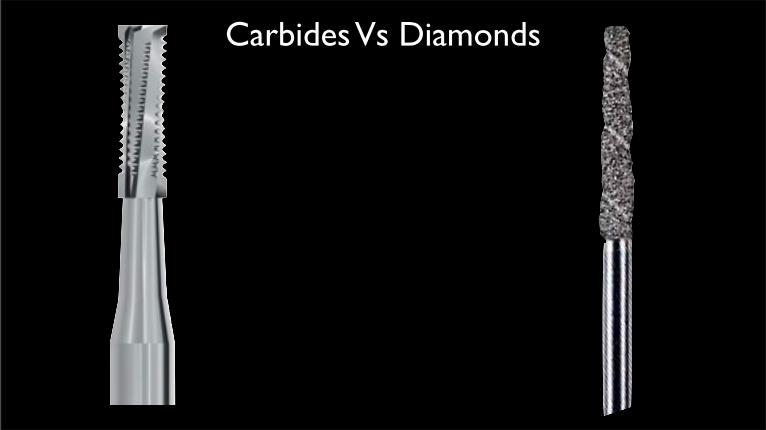
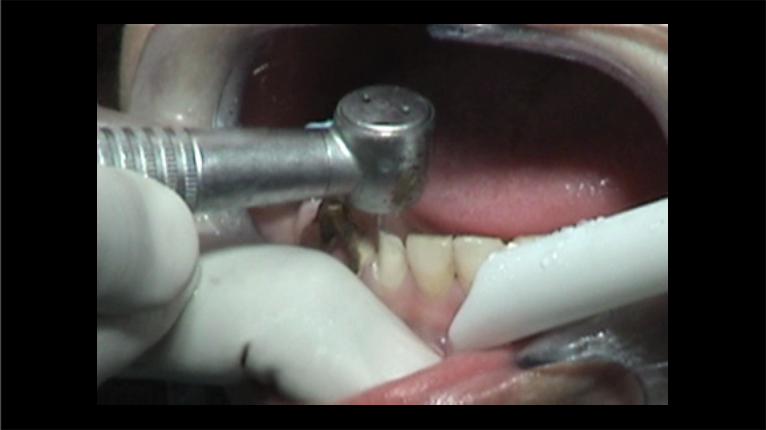
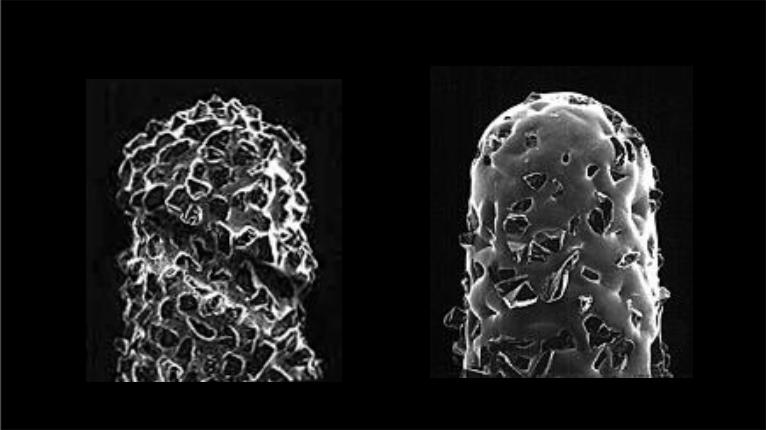
Carbides Vs Diamonds
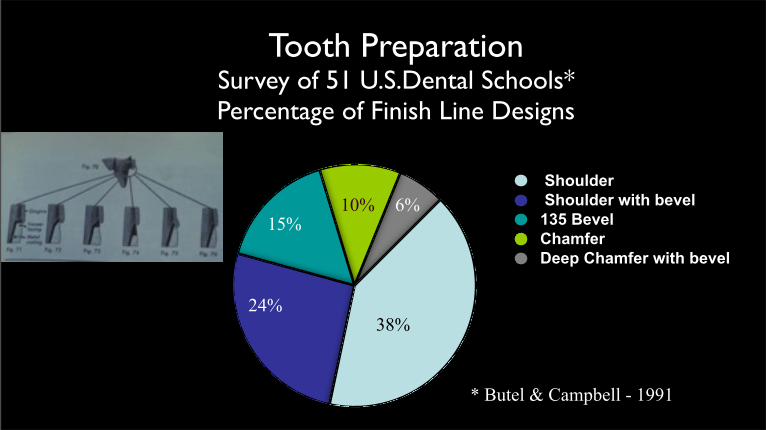
Tooth PreparationSurvey of 51 U.S.Dental Schools*Percentage of Finish Line Designs
Shoulder Shoulder with bevel135 BevelChamferDeep Chamfer with bevel
* Butel & Campbell - 1991
38%24%
15% 10% 6%
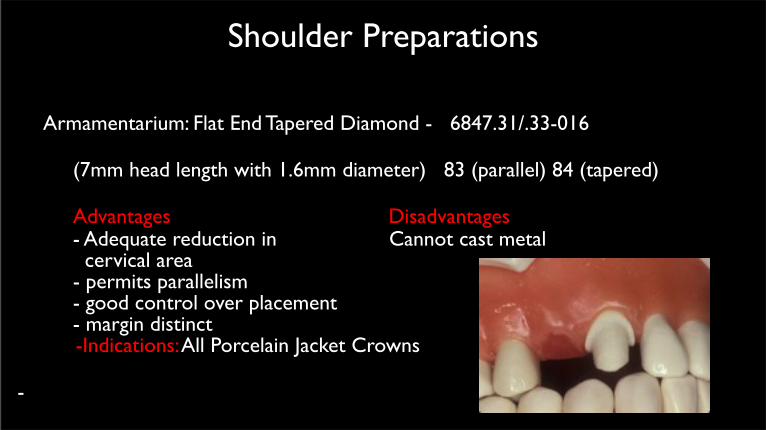
Shoulder Preparations
• Armamentarium: Flat End Tapered Diamond - 6847.31/.33-016
– (7mm head length with 1.6mm diameter) 83 (parallel) 84 (tapered)
– Advantages Disadvantages– - Adequate reduction in Cannot cast metal– cervical area – - permits parallelism – - good control over placement– - margin distinct
-Indications: All Porcelain Jacket Crowns
-
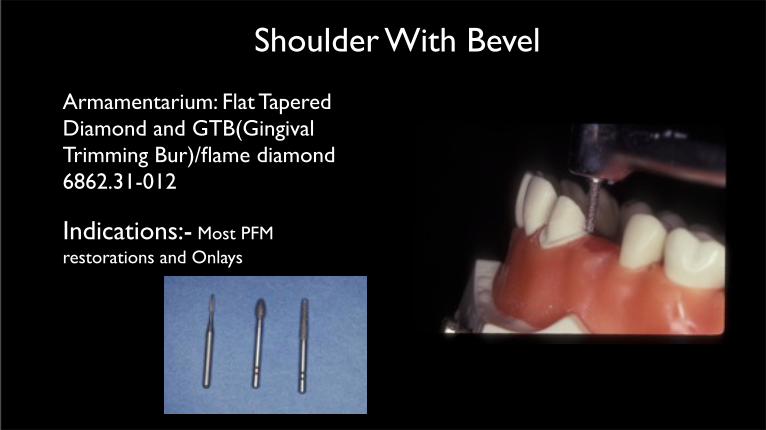
Shoulder With Bevel
• Armamentarium: Flat Tapered Diamond and GTB(Gingival Trimming Bur)/flame diamond 6862.31-012
• Indications:- Most PFM restorations and Onlays


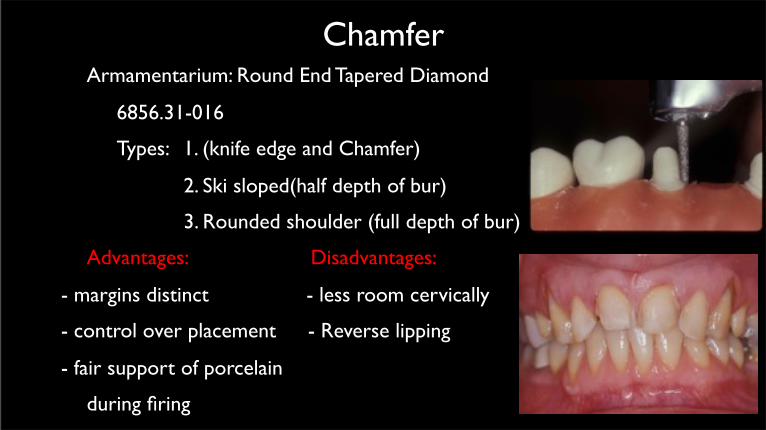
Chamfer• Armamentarium: Round End Tapered Diamond
– 6856.31-016
– Types: 1. (knife edge and Chamfer)
2. Ski sloped(half depth of bur)
3. Rounded shoulder (full depth of bur)
• Advantages: Disadvantages:
- margins distinct - less room cervically
- control over placement - Reverse lipping
- fair support of porcelain
during firing

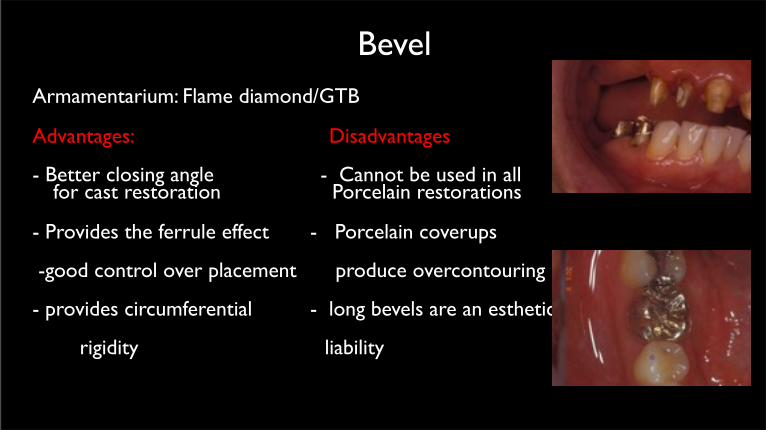
Bevel• Armamentarium: Flame diamond/GTB
• Advantages: Disadvantages
- Better closing angle - Cannot be used in all for cast restoration Porcelain restorations
- Provides the ferrule effect - Porcelain coverups
-good control over placement produce overcontouring
- provides circumferential - long bevels are an esthetic
rigidity liability
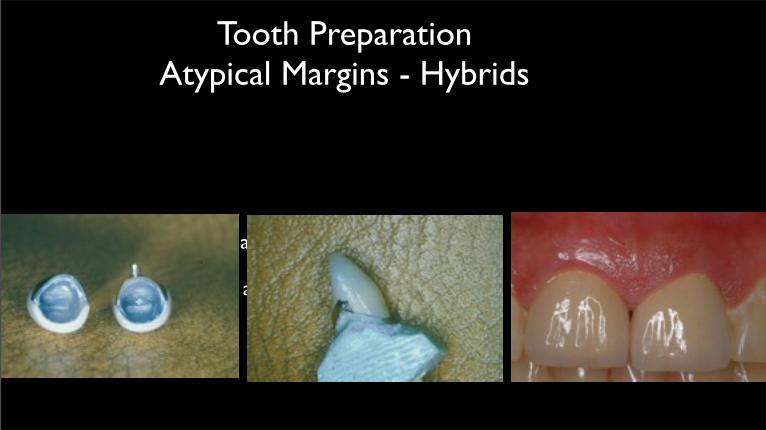
Tooth PreparationAtypical Margins - Hybrids
Hybrid - Beveled Shoulder and Chamfer
- Facial Shoulder and Chamfer
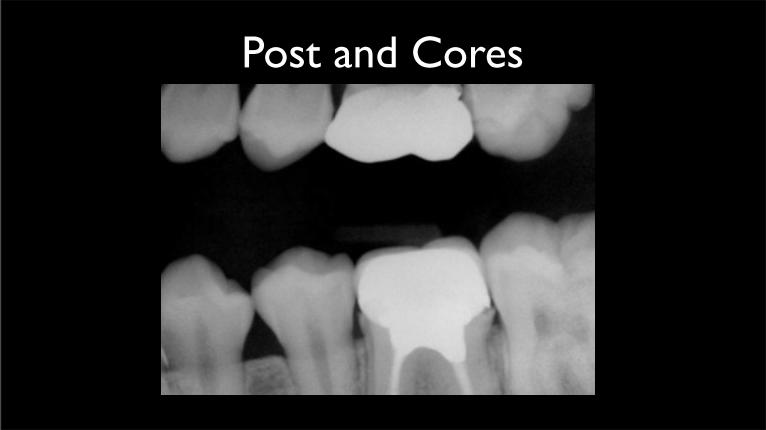
Post and Cores
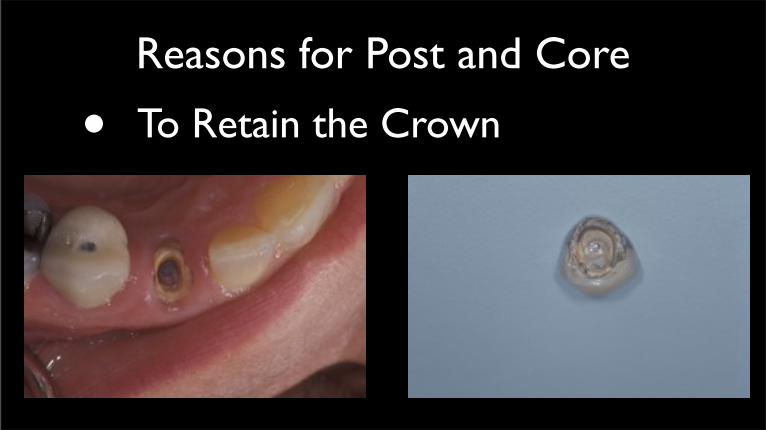
Reasons for Post and Core
• To Retain the Crown

Post and Cores
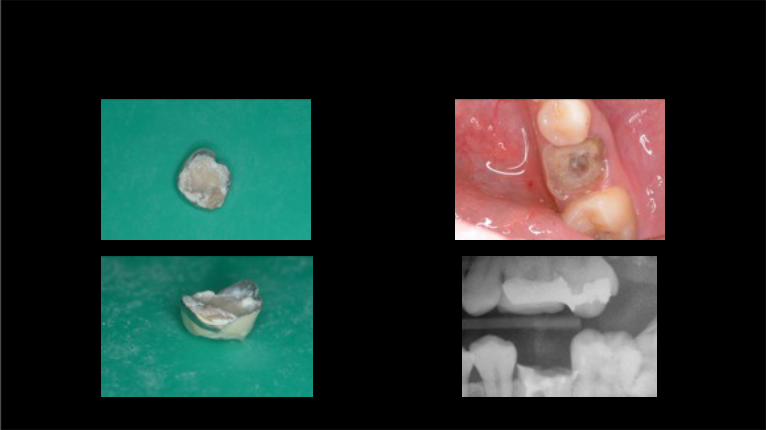
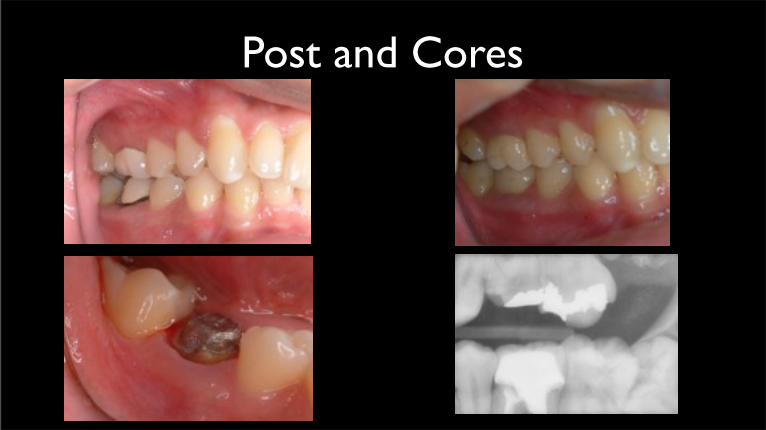
Post and Cores
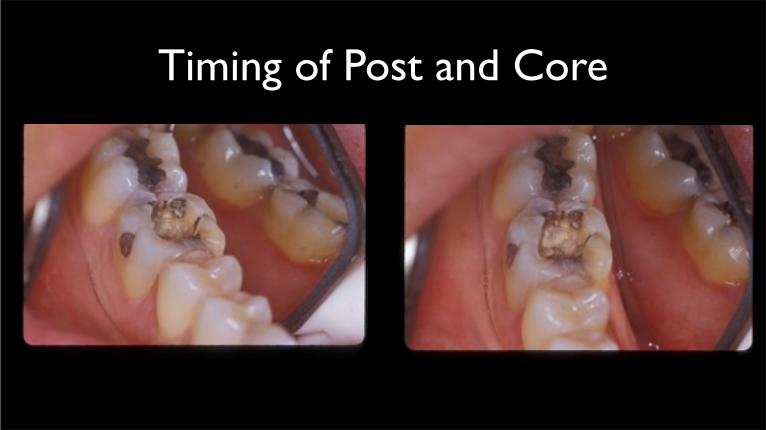
Timing of Post and Core
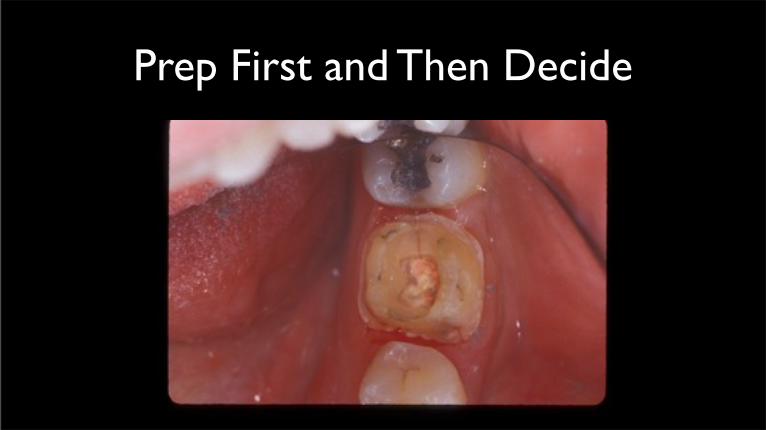
Prep First and Then Decide


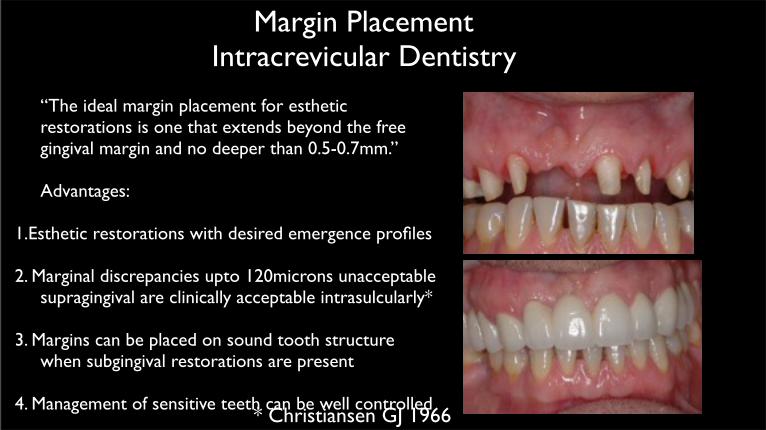
Margin PlacementIntracrevicular Dentistry
• “The ideal margin placement for esthetic restorations is one that extends beyond the free gingival margin and no deeper than 0.5-0.7mm.”
• Advantages:
1.Esthetic restorations with desired emergence profiles
2. Marginal discrepancies upto 120microns unacceptable supragingival are clinically acceptable intrasulcularly*
3. Margins can be placed on sound tooth structure when subgingival restorations are present
4. Management of sensitive teeth can be well controlled* Christiansen GJ 1966

Emergence Profile
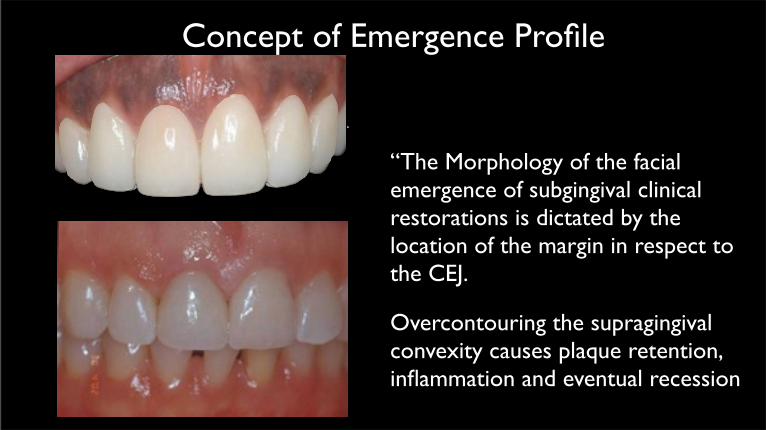
Concept of Emergence Profile
• “The Morphology of the facial emergence of subgingival clinical restorations is dictated by the location of the margin in respect to the CEJ.
• Overcontouring the supragingival convexity causes plaque retention, inflammation and eventual recession
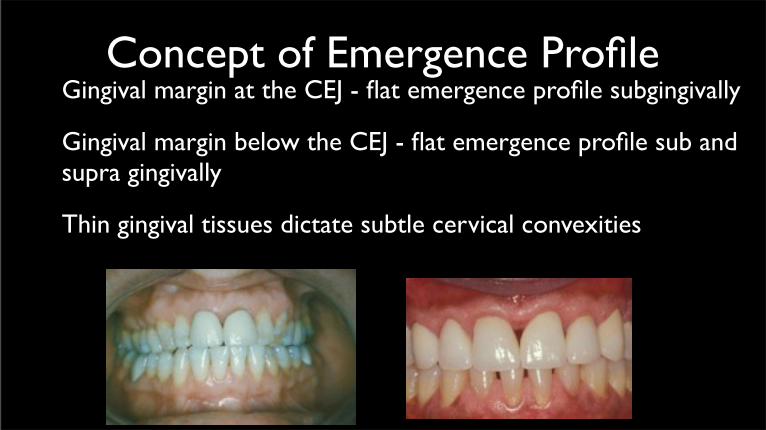
Concept of Emergence Profile• Gingival margin at the CEJ - flat emergence profile subgingivally
• Gingival margin below the CEJ - flat emergence profile sub and supra gingivally
• Thin gingival tissues dictate subtle cervical convexities
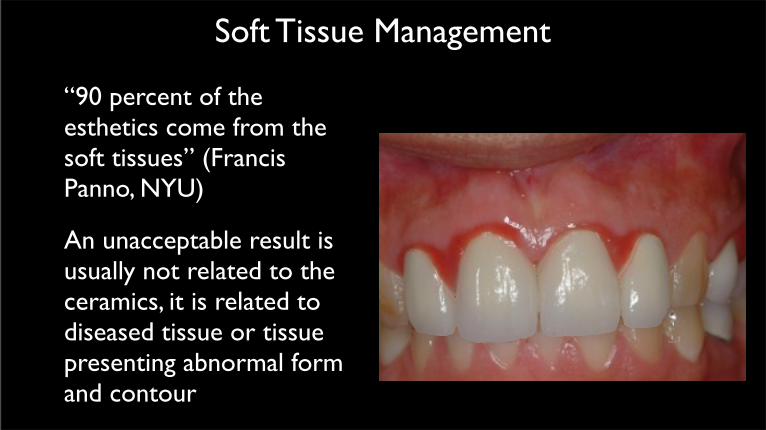
Soft Tissue Management
• “90 percent of the esthetics come from the soft tissues” (Francis Panno, NYU)
• An unacceptable result is usually not related to the ceramics, it is related to diseased tissue or tissue presenting abnormal form and contour


Provisional Restoration
• Purpose: maintain -* abutment relationships* pulpal integrity* function* periodontal health * esthetic, phonetic and functional occlulsal characteristics for every patient

Provisional Restoration
• Requirements
* good marginal adaptation
* physiologic contours and embrasures
* strength and durability
* good esthetics
* comfort during function
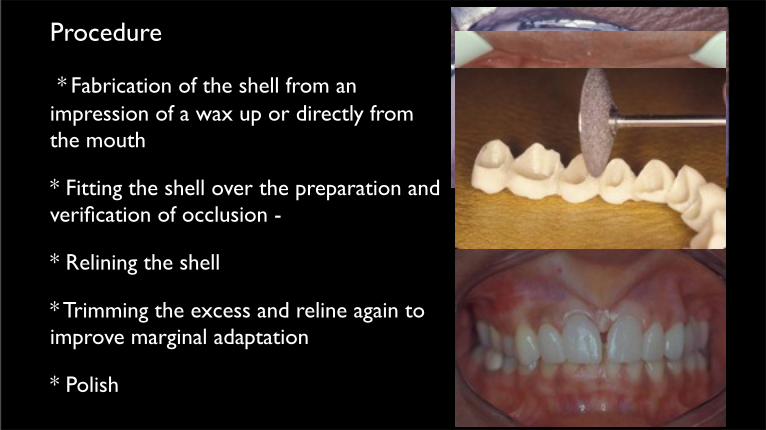
Provisional RestorationThe Shell Technique
• Procedure
• * Fabrication of the shell from an impression of a wax up or directly from the mouth
* Fitting the shell over the preparation and verification of occlusion -
* Relining the shell
* Trimming the excess and reline again to improve marginal adaptation
* Polish

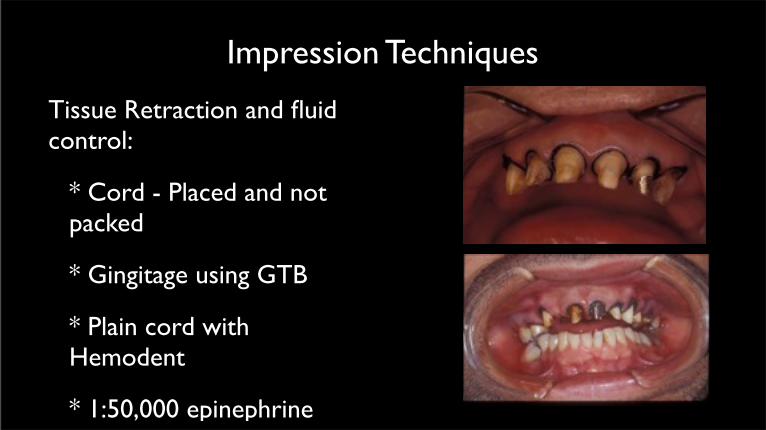
Impression Techniques
• Tissue Retraction and fluid control:
* Cord - Placed and not packed
* Gingitage using GTB
* Plain cord with Hemodent
* 1:50,000 epinephrine
Impression Techniques
• Polyether (Impregum)Single mix technique
• Polovinyl Siloxane (addition cured)-Double mix Single Impression (Sandwich Tech)
• Polyvinyl Siloxane (addition cured)- Double mix double impression technique
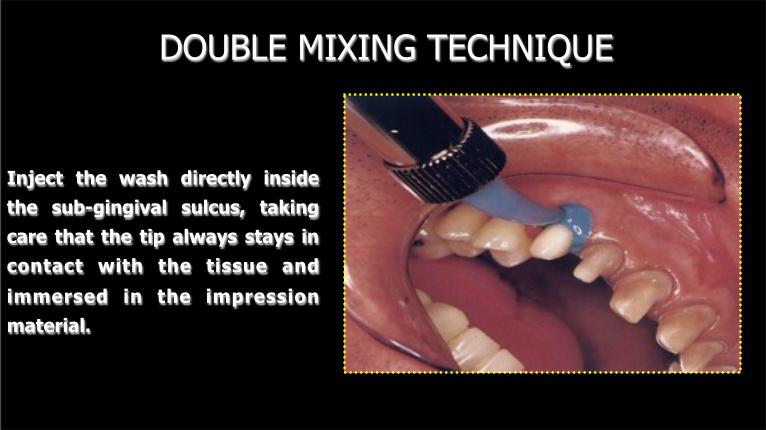
DOUBLE MIXING TECHNIQUE
Inject the wash directly inside
the sub-gingival sulcus, taking
care that the tip always stays in
contact with the tissue and
immersed in the impression
material.

DOUBLE MIXING TECHNIQUE
The tray with the high viscosity
material must be inserted when
the wash is still operating –
therefore, perfect co-operation
between dentist and assistant
is essential.
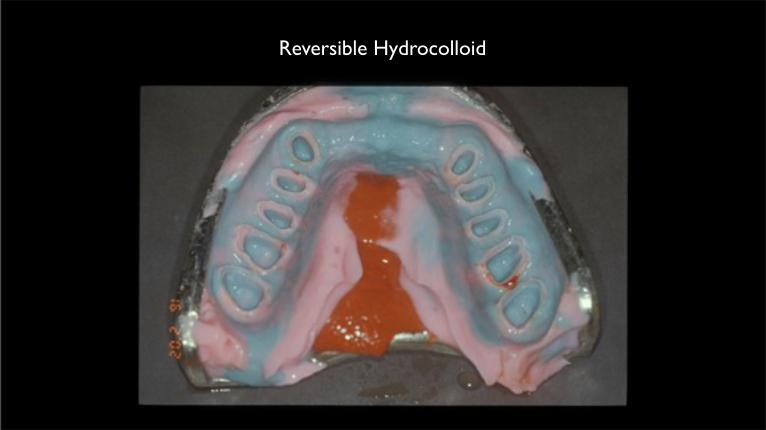
Reversible Hydrocolloid
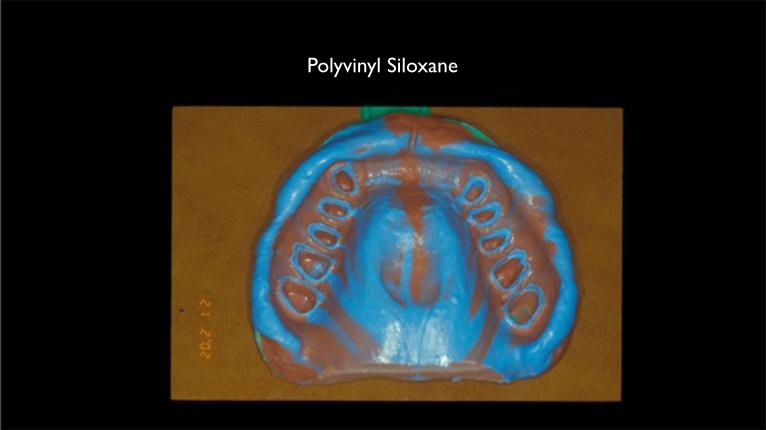
Polyvinyl Siloxane
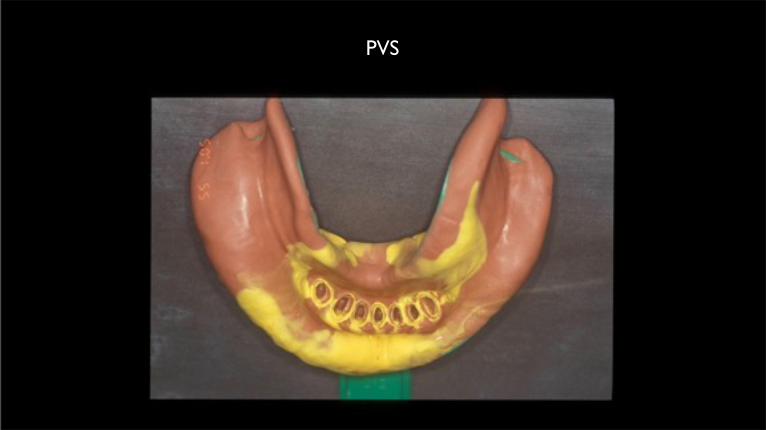
PVS
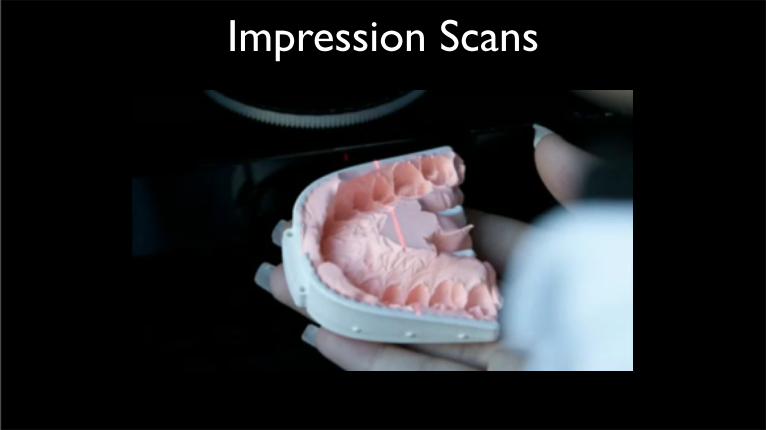
Impression Scans

Digital Impressions

Digital Scans and CAM
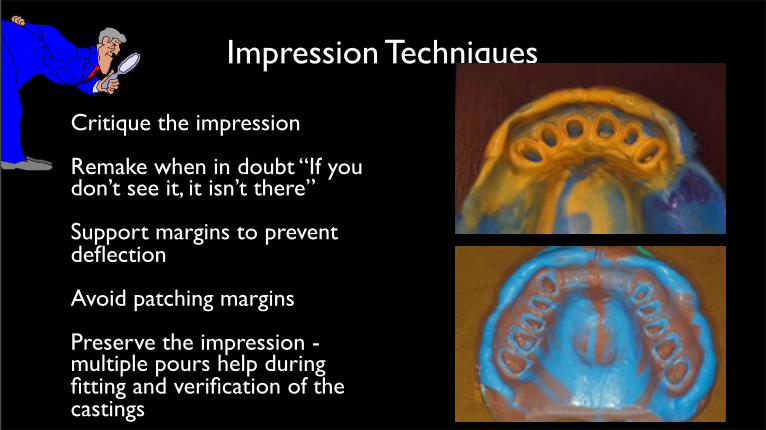
Impression Techniques
• Critique the impression
• Remake when in doubt “If you don’t see it, it isn’t there”
• Support margins to prevent deflection
• Avoid patching margins
• Preserve the impression - multiple pours help during fitting and verification of the castings

Casting Verification
• Verify margins and fit of the castings - silicone disclosing medium
• Obtain individual castings/copings instead of one piece - (3 units or more) Casting shrinkage:Gold 1.83% Base Metals 2.23%
• If the copings are not retentive “stop and backtrack”

Pick-up and Assemblage
• Relate castings to each other with Duralay and pick up in plaster for soldering. Soldering compensates casting shrinkage
•
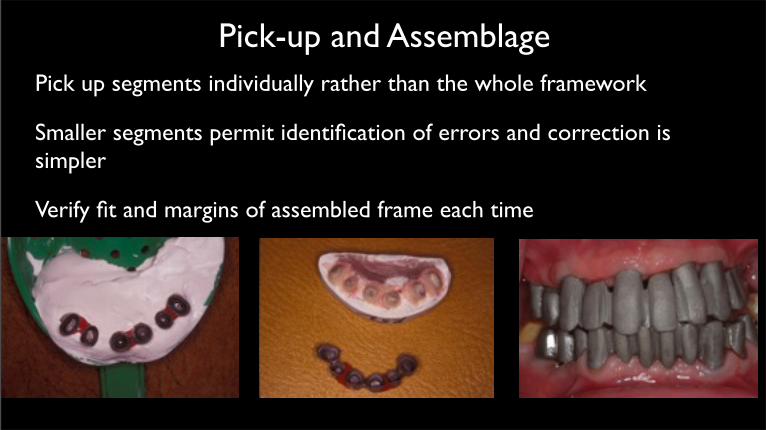
Pick-up and Assemblage• Pick up segments individually rather than the whole framework
• Smaller segments permit identification of errors and correction is simpler
• Verify fit and margins of assembled frame each time



Rules For Splinting
• Pathological Migration
• Progressive Mobility

Avoid Splinting:
•Short Clinical Crowns
•Increase Retention
•Better stability and resistance

Ill Effects of Splinting

Tilted Abutments

Tilted Abutments

Tilted Abutments
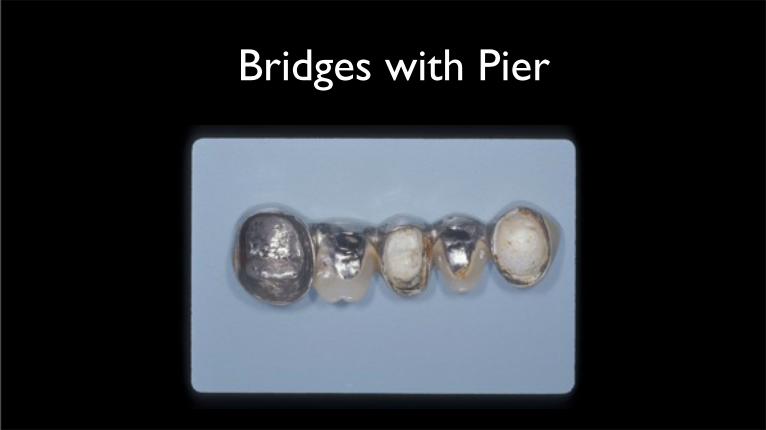
Bridges with PierImage3.jpg


Attachments
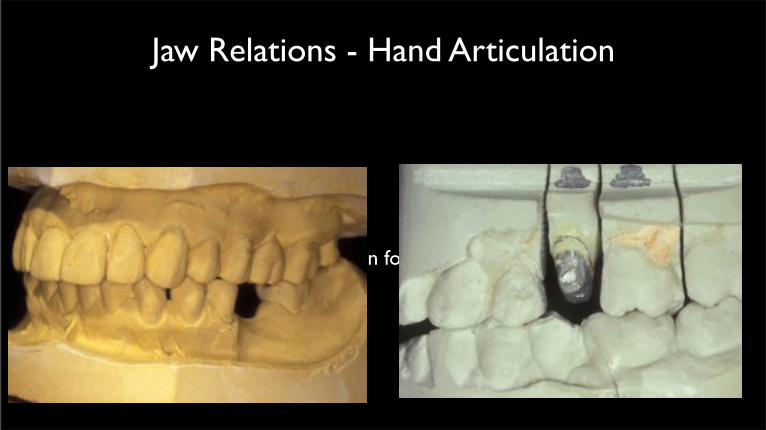
Jaw Relations - Hand Articulation
Hand articulation for bounded units

Sequence of Single crown insertion

Jaw Relations
Interocclusal records for unsupported, prepared units only

Jaw Relations
Utilize Provisional splints as guide for complete arch JR

Jaw Relations
Utilize CR only for complete arch reconstruction - “always MIP”


Jaw Relations - Never a complete arch record
Avoid complete arch bites

Occlusal SchemesReestablish Anterior Guidance, Cuspid Protected Occlusion
(Mutually protected occlusion) for most FPD cases

“W I I F M”
“What’s In It For Me”


THANK YOU