Embed Size (px)
Citation preview

See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/326867656
The treatment of refractory angle-closure glaucoma in a patient with X-
linked juvenile retinoschisis
Article in Ophthalmic Genetics · August 2018
DOI: 10.1080/13816810.2018.1490961
CITATIONS
2READS
65
5 authors, including:
Some of the authors of this publication are also working on these related projects:
Pathogenesis of Glaucoma View project
Angle-Closure Glaucoma View project
Sancy Low
Guy's and St Thomas' NHS Foundation Trust
24 PUBLICATIONS 346 CITATIONS
SEE PROFILE
David F Garway-Heath
Moorfields Eye Hospital NHS Foundation Trust
229 PUBLICATIONS 9,539 CITATIONS
SEE PROFILE
All content following this page was uploaded by Sancy Low on 14 August 2018.
The user has requested enhancement of the downloaded file.

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=iopg20
Ophthalmic Genetics
ISSN: 1381-6810 (Print) 1744-5094 (Online) Journal homepage: http://www.tandfonline.com/loi/iopg20
The treatment of refractory angle-closureglaucoma in a patient with X-linked juvenileretinoschisis
Sancy Low, Ryian Mohamed, Michelle Ting, Andrew R. Webster & David F.Garway-Heath
To cite this article: Sancy Low, Ryian Mohamed, Michelle Ting, Andrew R. Webster & David F.Garway-Heath (2018): The treatment of refractory angle-closure glaucoma in a patient with X-linkedjuvenile retinoschisis, Ophthalmic Genetics, DOI: 10.1080/13816810.2018.1490961
To link to this article: https://doi.org/10.1080/13816810.2018.1490961
View supplementary material
Published online: 06 Aug 2018.
Submit your article to this journal
Article views: 3
View Crossmark data

CASE REPORT
The treatment of refractory angle-closure glaucoma in a patient with X-linkedjuvenile retinoschisisSancy Low a,b, Ryian Mohamed c, Michelle Tinga, Andrew R. Webster a,b, and David F. Garway-Heatha,b
aMoorfields Eye Hospital NHS Foundation Trust, London, United Kingdom; bUCL Institute of Ophthalmology, London, United Kingdom; cDepartmentof Ophthalmology, Abergele Hospital, Abergele, Wales
ABSTRACTX-Linked Retinoschisis (XLRS) is a common genetically determined form of macular degenerationaffecting young males. XLRS is due to mutations in the RS1 gene located on chromosome Xp22which codes for retinoschisin and is estimated to affect between 1:5000 to 1:20000 individualsworldwide.We report a case of refractory angle-closure glaucoma in a thirty-nine-year-old Caucasian man withatypical XLRS. The patient presented with a two-day history of left eye pain, acutely reduced vision and anine-month history of hemicranial pain. Examination identified left intraocular pressure (IOP) of52mmHg. Gonioscopy confirmed complete angle closure.Following failure of medical management and persistently raised left IOP (43-46mmHg), the patientunderwent left phacoemulsification and intraocular lens insertion without complication. After surgery,his IOP reduced to 10-14mmHg on all follow up examinations without the need for glaucoma drops. Hisiridocorneal angle remained open and vision improved to 20/100.Our case demonstrates the additional role of lens surgery in the treatment of secondary angle-closureglaucoma in the presence of an inherited retinal dystrophy. All patients with inherited retinopathypresenting with a headache or eye pain should undergo gonioscopic examination to exclude angle-closure glaucoma.
ARTICLE HISTORYReceived 18 February 2018Revised 29 May 2018Accepted 9 June 2018
KEYWORDSAngle-closure glaucoma;lens extraction; cataractsurgery; X-linkedretinoschisis
X-linked retinoschisis (XLRS) is a common genetically deter-mined form of macular degeneration affecting young males.Worldwide estimates of XLRS prevalence range from 1:5000to 1:20,000 (1). We report a 39-year-old man with refractoryangle-closure glaucoma and genetically confirmed XLRS. Thepatient’s retinal phenotype was atypical due to the extensiveexudative retinal detachments, suggesting multiple mechan-isms contributing to his glaucoma.
The patient presented with a 2-day history of left eye painand acutely reduced vision, on a background of a 9-monthhistory of left-sided hemicranial pain. His baseline visualacuity was counting fingers in the right eye (OD) and 20/120 in the left eye (OS). On acute presentation, visual acuityreduced to hand movements OD and 20/300 OS. Prior intrao-cular pressure (IOP) measurements were 19mmHg in botheyes (OU); however, during this acute presentation, IOP OSwas 52 mmHg, and there was conjunctival injection, diffusecorneal edema, and a very shallow central and peripheralanterior chamber. Gonioscopy confirmed a completely closedangle. There was no iris or angle neovascularization, no pos-terior synechiae, and no iris bombe. The crystalline lens wasbulging anteriorly with visible glaucomflecken, but no frankphacodonesis. The patient was hypermetropic (OD +3.00/−1.00 × 120, OS +5.00/−1.25 × 25). The right eye was pseu-dophakic with inferior intraocular lens (IOL) subluxation, andhe was treated for ocular hypertension. There was previously a
dense white cataract in the right eye before cataract surgerywas performed and no history of ocular trauma. The left eyewas phakic and was his better-seeing eye. Ophthalmoscopyshowed a 360-degree retinal fold OD with a nasal tractionalretinal detachment and a cup-to-disc ratio of 0.3. There wasno view of the left fundus due to the corneal opacification.Clinical and genetic analyses related to his XLRS disease hadpreviously been undertaken by an Institutional Review Board(IRB)-approved study. He carried the NM_000330.3(RS1):c.574C>T (p.Pro192Ser) mutation.
The patient was managed medically with 1 g of intravenousacetazolamide and topical timolol/dorzolamide, latanoprost,iopidine, and dexamethasone drops in his left eye. IOP OSdecreased to 46 mmHg, with the corneal edema clearingsufficiently to permit a YAG laser peripheral iridotomy.Following iridotomy, his IOP was 45 mmHg and the irido-corneal angles remained closed. Anterior segment imagingand B-scan ultrasound excluded choroidal effusions. Hischronic exudative retinal detachment, which had previouslybeen noted in both eyes, remained unchanged. The axiallengths were 20.8 mm (OS) with an anterior chamber depth(ACD) of 1.6 mm (OS) compared to 20.9 mm (OD) and ACDof 4 mm with the subluxed lens (OD), suggesting possiblezonular laxity in the right eye. Anterior segment imagingshowed an anteriorly vaulted lens; hence, the patient wasinstructed to lie supine and was given topical cyclopentolate
CONTACT Sancy Low [email protected] Moorfields Eye Hospital and UCL Institute of Ophthalmology, 11-43 Bath Street, London EC1V 9EL, UK.Supplemental data for this article can be accessed at https://doi.org/10.1080/13816810.2018.1490961
OPHTHALMIC GENETICShttps://doi.org/10.1080/13816810.2018.1490961
© 2018 Taylor & Francis

1%. Six hours following this, the IOP decreased to 36 mmHg,but the iridocorneal angle remained closed. Urgent cyclodiodeablation of the ciliary body was performed the same day, andthe IOP decreased to 24 mmHg two hours post-laser.
A week later, the pressure in the left eye was 7 mmHg withongoing treatment with topical timolol/dorzolamide bid, lata-noprost once a day, iopidine tid, and dexamethasone qid. Twoweeks later, the IOP rose again to 43 mmHg, and he under-went a left lens extraction and IOL implantation withoutcomplications (a video showing the surgery for this patientcan be found on supplemental material), and the patient wasgiven a stat dose of atropine 1% postoperatively to reduce therisk of aqueous misdirection. Following surgery, his IOPdecreased to 10 mmHg to 14 mmHg on without the needfor glaucoma drops. His iridocorneal angle remained open.His vision improved to 20/100.
This case posed a difficult challenge, given that this was a youngpatient with an “only eye,” whose acute rise in IOP was uncon-trolled with medical treatment. Furthermore, he had a complexgenetic retinopathy including XLRS but perhaps also anotherundiagnosed hereditary ocular condition that was responsible forhis extensive bilateral exudative retinal detachments.
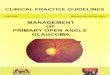
According to Ritch’s anatomical classification of angle-closure (pupil block, plateau iris/non-pupil block, lens-inducedangle-closure, and retrolenticular causes) (2), this patient isunusual as his mixed-mechanism angle-closure glaucomaincluded all four levels of block (Figure 1). Our patient under-went systematic investigation and treatment to exclude each ofthese levels of angle-closure. After failure of initial medicaltreatment, he underwent a laser peripheral iridotomy to relieveany pupil block component. An anterior segment optical coher-ence tomography scan was able to rule out plateau iris
configuration and confirmed the clinical finding that the crystal-line lens was bulging anteriorly. The B-scan ultrasound showedheavy calcification in the area of chronic exudative retinaldetachment.
At the molecular level, XLRS is due to mutations in theRS1 gene located on chromosome Xp22 (3). RS1 codes forretinoschisin, a protein known to play an important role incellular fluid balance, cellular adhesion, and cell–cell interac-tions across bipolar–photoreceptor synapses. Absence of reti-noschisin in XLRS patients subsequently leads to pathologicalextracellular fluid accumulation and reduced bipolar–photo-receptor integrity (3). XLRS patients are also at increased riskof developing ocular complications such as vitreous hemor-rhage and retinal detachment (4), but angle-closure glaucomahas not been reported previously.
Our patient had the NM_000330.3(RS1): c.574C>T (p.Pro192Ser) mutation. This RS1 mutation has been reported inother families (4–6), but the specific phenotypic details relatingto glaucoma such as axial length, refraction, and IOP were notavailable in the published reports. Interestingly, XLRS is justone cause of macular retinoschisis, of which there are severalknown causes, such as retinitis pigmentosa, myopic degenera-tion, and vitreo-macular traction. Of note, there are two casereports of angle-closure glaucoma in peripapillary schisis (7)and macular schisis (8). In both these cases, and our own, themechanism of interaction between the retinal disorder andangle-closure glaucoma is unknown. See supplemental materialfor a table summarizing inherited retinal disorders associatedwith angle-closure glaucoma.
Lens surgery in the treatment of primary angle-closureglaucoma (9) is gaining in popularity. There is an additionalrole for lens surgery in the treatment of secondary angle-
Figure 1. Diagram showing all four mechanisms of angle-closure disease. This patient’s refractory glaucoma is secondary to the mixed mechanisms, which needed tobe dealt with systematically.
2 S. LOW ET AL.

closure glaucoma in the presence of an inherited retinal dys-trophy. The present case demonstrates a systematic clinicaland therapeutic approach to refractory angle-closure glau-coma, with good outcome following lens surgery. We suggestthat patients with inherited retinal dystrophies presentingwith headache or eye pain should undergo gonioscopic exam-ination, so as to prevent the devastating visual loss which canoccur in undiagnosed angle-closure glaucoma (10).
Acknowledgement
Professors David F. Garway-Heath and Andrew R. Webster are sup-ported by the National Institute for Health Research BiomedicalResearch Centre at Moorfields Eye Hospital and UCL Institute ofOphthalmology, National Health Service, United Kingdom.
ORCID
Sancy Low http://orcid.org/0000-0001-8925-5971Ryian Mohamed http://orcid.org/0000-0001-8555-4659Andrew R. Webster http://orcid.org/0000-0001-6915-9560
References
1. George ND, Yates JR, Moore AT. X linked retinoschisis. Br JOphthalmol. 1995; 79: 697–702. 10.1136/bjo.79.7.697.
2. Ritch R, Liebmann JM. Role of ultrasound biomicroscopy in thedifferentiation of block glaucomas. Curr Opin Ophthalmol. 1998;9: 39–45. 10.1097/00055735-199804000-00008.
3. Molday RS, Kellner U, Weber BHF. X-linked juvenile retinoschisis:clinical diagnosis, genetic analysis, and molecular mechanisms. ProgRetin Eye Res. 2012; 31: 195–212. 10.1016/j.preteyeres.2011.12.002.
4. Hiriyanna KT, Bingham EL, Yashar BM, Ayyagari R, Fishman G,Small KW, Weinberg DV, Weleber RG, Lewis RA, Andreasson S,et al. Novel mutations in XLRS1 causing retinoschisis, includingfirst evidence of putative leader sequence change. Hum Mutat.1999; 14: 423–27. 10.1002/(SICI)1098-1004(199911)14:5<423::AID-HUMU8>3.0.CO;2-D.
5. Eksandh LC, Ponjavic V, Ayyagari R, Bingham EL, HiriyannaKT, Andréasson S, Ehinger B, Sieving PA, et al. Phenotypicexpression of juvenile X-linked retinoschisis in Swedishfamilies with different mutations in the XLRS1 gene. ArchOphthalmol. 2000; 118: 1098–104. 10.1001/archopht.118.8.1098.
6. Lesch B, Szabó V, Kánya M, Somfai GM, Vámos R, VarsányiB, Pámer Z, Knézy K, Salacz G, Janáky M, et al. Clinical andgenetic findings in Hungarian patients with X-linked juvenileretinoschisis. Mol Vis. 2008; 14: 2321–32.
7. Kahook MY, Noecker RJ, Ishikawa H, Wollstein G, KagemannL, Wojtkowski M, Duker JS, Srinivasan VJ, Fujimoto JG, SchumanJS, et al. Peripapillary schisis in glaucoma patients with narrowangles and increased intraocular pressure. Am J Ophthalmol.2007; 143: 697–99. 10.1016/j.ajo.2006.10.054.
8. Hollander DA, Barricks ME, Duncan JL, Irvine AR. Macularschisis detachment associated with angle-closure glaucoma.Arch Ophthalmol. 2005; 123: 270–72. 10.1001/archopht.123.3.321.
9. Azuara-Blanco A, Burr J, Ramsay C, Cooper D, FosterPJ, Friedman DS, Scotland G, Javanbakht M, CochraneC, Norrie J; EAGLE study group. Effectiveness of early lensextraction for the treatment of primary angle-closure glau-coma (EAGLE): a randomised controlled trial. Lancet. 2016;388: 1389–97. 10.1016/S0140-6736(16)30956-4.
10. Low S, Davidson AE, Holder GE, Hogg CR, BhattacharyaSS, Black GC, Foster PJ, Webster AR. Autosomal dominant Bestdisease with an unusual electrooculographic light rise and risk ofangle-closure glaucoma: a clinical and molecular genetic study.Mol Vis. 2011; 17: 2272–82.
OPHTHALMIC GENETICS 3
View publication statsView publication stats