Embed Size (px)
Citation preview

The Treatment of Benign Intracranial Hypertension: A Review of 134 Cases
Ian Johnston, F.R.C.S.,* A. Paterson, F.R.C.S., t and M. Besser, F.R.A.C.S.*
The treatment of benign intracranial hypertension in 134 patients is reviewed. No treatment was required in 16 pa- tients, although the diagnosis may have been doubtful in a number of these. Serial lumbar punctures had only a 38.8% success rate when used alone. Steroids were effec- tive as primary treatment in 81.1% of the patients, al- though recurrence (13.5%) and complications of therapy were significant in this group. Subtemporal decompression was relatively ineffectual, particularly on the measured cerebrospinal fluid (CSF) pressure. CSF shunting, espe- cially lumboperitoneal, was very effective, although com- plications were important. The basis of treatment in be- nign intracranial hypertension is reviewed in light of the current theories of its pathogenesis.
Johnston l, Paterson A, Besser M: The treatment of benign intracranial hypertension: a review of 134 cases. Surg Neurol 16:218-224, 1981
Lack of knowledge of the pathophysiology and natural his- tory of benign intracranial hypertension has precluded a ra- tional approach to therapy. Assessment of methods of treatment has also been hampered by diagnostic inaccuracy and by the frequent use of a combination of methods in the individual patient. The present paper reviews the treat- ment of 134 patients with benign intracranial hypertension and illustrates the variability of response to different forms of therapy. To explain this variation, the effects of steroids, lumbar puncture, and subtemporal decompression on intra- cranial pressure were examined in detail. Current treatment modalities have been critically evaluated, and an attempt has been made to seek a more rational basis for the therapy of this condition.
Patients and Methods The 134 patients included in the study comprised the fol- lowing:
From tThe Institute of Neurological Sciences, Southern General Hospi- tal, Glasgow, Scotland, and *The Royal Alexandra Hospital for Children. Sydney, Australia. Address reprint requests to Mr. Ian Johnston, The Royal Alexandra Hos- pital for Children. Pyrmont Bridge Rd,, Camperdown, NSW 2050 Aus- tralia.
Key words: benign intracranial hypertension; pseudotumor cerebri; steroids; lumbar puncture; subtemporal decompression; shunt.
I. One hundred and ten patients with an established diagnosis of benign intracranial hypertension were in- vestigated and treated at The Institute of Neurological Sciences, Glasgow, between 1942 and 1972. Follow-up until 1972 was accomplished in all but 5 of these pa- tients, with a mean follow-up of 11.6 years. In the re- maining 5 patients who were lost to follow-up, the mean follow-up was 7 years.
2. Nineteen patients with benign intracranial hyperten- sion were investigated and treated at The Royal Alexandra Hospital for Children, Sydney, between 1970 and 1979. Current follow-up (mean, 2.9 years) was obtained on all of these patients.
3. Five patients were treated by one of the authors (I. J.) at The Royal Prince Alfred Hospital, Sydney, between 1975 and 1979. Current follow-up (mean, 2 years) was obtained on all patients.
A summary of the methods of treatment used in the study is given in Table 1. The effect of steroids on intracranial pressure was studied in 7 patients in whom the diagnosis was established by means of continuous intracranial pres- sure monitoring, isotope cisternography, and (in 5 patients) fluorescein angiography.
Results No Treatment Sixteen patients had either no treatment or only a single lumbar or ventricular puncture primarily for diagnostic pur- poses. Thirteen of the 16 had no further symptoms (mean follow-up, 7 years), while 3 had persistent symptoms de- spite (in 2 patients) subsequent treatment. Of the 13, only 1, whose symptoms resolved without treatment, had a well-documented increase in intracranial pressure (on con- tinuous pressure monitoring), and this was relatively slight. In the other 12, the diagnosis was made on clinical grounds alone. They had normal pressure on direct measurement, an impression only of increased intracranial tension at ventriculography, or no cerebrospinal fluid (CSF) pressure measurement. In several of these patients, the optic discs remained abnormal despite complete resolution of symp- toms.
218 0090-3019/81/090218-07501.25 © 1981 by Little, Brown and Company (Inc.)
Johnston et al: Benign Intracranial Hypertension 219
Table 1. Methods of Treatment and Results in 134 Patients with Benign Intracranial Hypertension
Initial Treatment--Used Alone
Total Required Type of No. of No. of Additional Treatment Patients Patients Resolved Treatment Recurrence
Initial Treatment in Combination
Subsequent Treatment
None 16 16 13 3 0 Serial lumbar 83 67 26 41 0
punctures Steroids 48 37 30 7 7 Subtemporal 43 5 1 4 0
decompression CSF shunts 14 1 1 0 0 Other 12 1 1 0 0
0 0 12 4
9 2 0 38
0 13 7 4
Serial Lumbar Punctures
This was the sole initial treatment in 67 patients. It proved adequate in only 26 (38.8%), who required an average of 9 punctures each. There were no recurrences among these 26 patients (mean follow-up, 12.7 years), and 23 were clear of symptoms and signs within three months. The initial CSF pressure was, however, relatively low (mean, 210 mm CSF) in 11 of the 26 patients.
Serial lumbar punctures proved inadequate in 41 of the 67 patients (61.2%). They failed to improve clinically, with persistence of symptoms and papilledema and, in 3 patients, further visual deterioration. In none of the 41 was the initial CSF pressure less than 300 mm CSF, and all required other forms of treatment after an average of 24 punctures. In 12 patients, serial lumbar punctures were combined with steroids, subtemporal decompression, or acetazolamide as an initial therapy; 10 showed rapid resolu- tion, while 2 required further treatment.
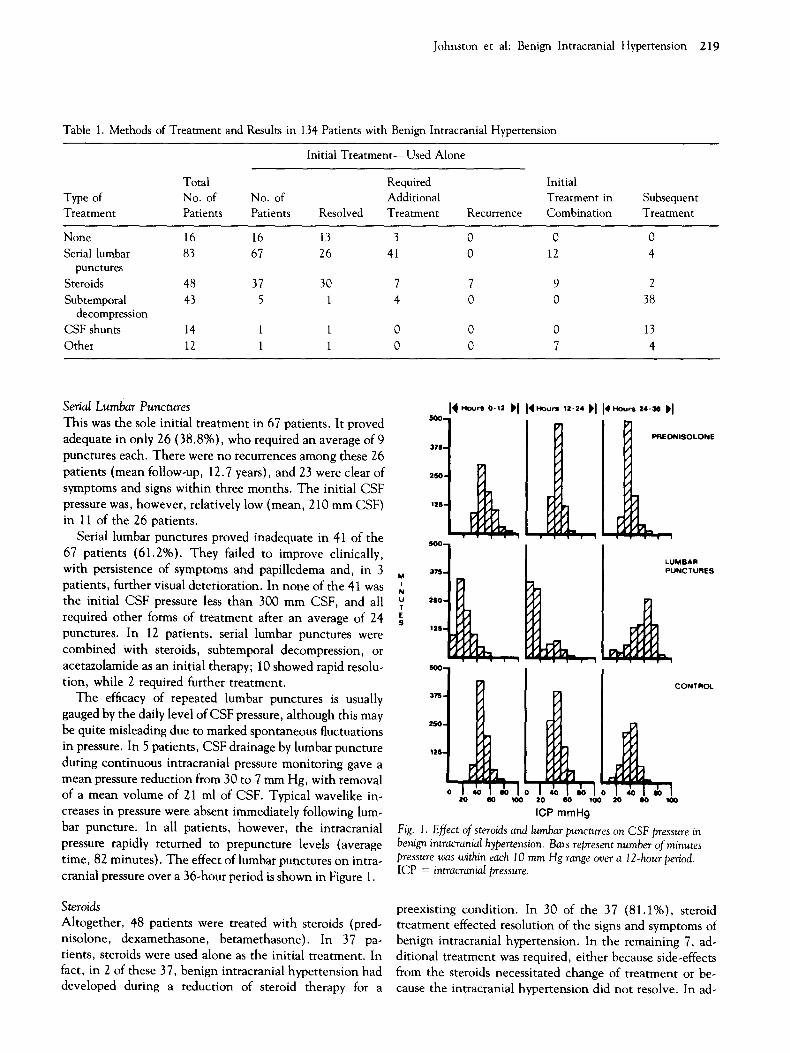
The efficacy of repeated lumbar punctures is usually gauged by the daily level of CSF pressure, although this may be quite misleading due to marked spontaneous fluctuations in pressure. In 5 patients, CSF drainage by lumbar puncture during continuous intracranial pressure monitoring gave a mean pressure reduction from 30 to 7 mm Hg, with removal of a mean volume of 21 ml of CSF. Typical wavelike in- creases in pressure were absent immediately following lum- bar puncture. In all patients, however, the intracranial pressure rapidly returned to prepuncture levels (average time, 82 minutes). The effect of lumbar punctures on intra- cranial pressure over a 36-hour period is shown in Figure 1.
Steroids
Altogether, 48 patients were treated with steroids (pred- nisolone, dexamethasone, betamethasone). In 37 pa- tients, steroids were used alone as the initial treatment. In fact, in 2 of these 37, benign intracranial hypertension had developed during a reduction of steroid therapy for a
M I
N U T E S
SO0.
37S-
2S0-
125-
500 -
3 / 3 -
2$0 -
12S-
375-
2 S 0 -
12S-
4 ,.,o.,. o-,= H I~ ~o.. , ,=-=4 ~'114 ' ~ - , .-am ~'1
• • • w ,
L LUMBAR PUNCTURES
i ! 1
2O eo too 20 80 100
ICP mmHg
CONTROL
20 60
Fig. 1. Effect of steroids and lumbar punctures on CSF pressure in benign intracranial hypertension. Bars represent number of minutes pressure was within each 10 mm Hg range over a 12-hour period. ICP = intracranial pressure.
preexisting condition. In 30 of the 37 (81.1%), steroid treatment effected resolution of the signs and symptoms of benign intracranial hypertension. In the remaining 7, ad- ditional treatment was required, either because side-effects from the steroids necessitated change of treatment or be- cause the intracranial hypertension did not resolve. In ad-

220 Surgical Neurology Vol 16 No 3 September 1981
dition, 5 of the 37 patients who initially responded de- veloped recurrence; 3 of 5 responded to a further course of steroids, while another 2 required additional treatment.
In 9 patients, the initial treatment consisted of steroids in combination with either lumbar punctures or diuretics. All of these patients showed rapid resolution of their intra- cranial hypertension, although there were 2 late recur- rences. In a further 2 patients, steroids were added late in treatment after other measures had failed, with good ef- fect in both patients.
The initial success rate for steroids alone was 81.1%, with a recurrence rate of 13.5%. Complications of steroid therapy included diabetes mellitus, peptic ulceration, fluid retention, marked obesity, and probable psychotic symp- toms. Significant complications occurred in 3 of the last 23 patients treated--a rate of 13%.
Seven patients were treated with steroids after the diag- nosis of benign intracrania[ hypertension had been estab- lished using continuous intracranial pressure monitoring and fluorescein angiography. In 5 patients, prednisolone was used: in 2 an initial dose consisted of 40 mg followed by 10 mg every 6 hours, and in 3 an initial dose of 80 mg was followed by 20 mg every 6 hours. With the other 2 patients, equivalent doses of dexamethasone were given. In all pa- tients, steroids were gradually reduced over a two-month period and then stopped. CSF pressure was monitored by the lumbar route at one week in 5 patients and at three months in 7 patients after the start of treatment, while fluorescein angiograms were done before and one month after the end of treatment {i.e., at three months). The re- sults are shown in Table 2. In all patients, signs and symp- toms of intracranial hypertension had resolved completely within three months. Despite this, the CSF pressure was still quite raised one week after the start of therapy and remained well above normal in all patients after three
Table 2. CSF Pressures Before, During, and After a Two-Month Course of Prednisolone ~
CSF Pressure (ram Hg)
Patient Before 1 Week 1 Month No. Treatment after Start after End
Mean SD
P
28 . . . 19 23 25 17 31 32 28 20 23 14 34 29 28
27.2 27.3 21.2 5.7 4.0 6.5
• . . N S < 0 . 0 1
"All 5 patients were free of signs and symptoms at the time of the last CSF pressure measurement.
SD = standard deviat ion; p = probability; NS = not slgnmcant.
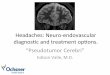
months. Although there had been a significant reduction in the mean pressure for the group, 2 patients showed very little change from pretreatment levels (Fig. 2). There were, however, no recurrences (follow-up, six to twenty-four months). Another patient with marked delay in CSF ab- sorption shown on isotope cisternography still had delayed absorption after four weeks on steroids despite considerable clinical improvement. Finally, 1 patient who developed intracranial hypertension while on steroids showed a marked reduction in pressure after one week of increased steroid dosage.
Fig. 2. CSF pressures before and one month after a two-month course (/f steroids in a patient with benign intracranial hypertension. Con- tinuous recording was done from the lumbar-subarachnoid space. CSFP = cerebrospinal fluid pressure.
CBFP rnmHg
6 0 - BEFORE TREATMENT AFTER 3/12 STEROIDS
50-
40-
10
i i I I
20 40
MINUTES
I I 20 40

Johnston et al: Benign Intracranial Hypertension 221
Subtemporal Decompression Right subtemporal decompression was performed in 43 pa- tients, in 5 as initial treatment due either to the severity of papilledema and rapidity of visual deterioration (4 patients) or failure of the patient to cooperate for lumbar punctures (1 patient). Decompression alone proved adequate in only 1 of these 5. In 38 patients subtemporal decompression was used as a second or third line of treatment, mainly after repeated lumbar punctures had failed to control intracranial hypertension. Of the total 43 patients who underwent de- compression, 30 showed resolution of all signs and symp- toms within six months, and 7 within one year; in 6 patients symptoms persisted for more than a year. However, in 13 of the 43 patients additional treatment was needed; in 5 of these 13, further visual deterioration occurred after decom- pression.
Decompression had relatively little immediate effect on measured CSF pressure (Fig. 3). Complications following decompression included epilepsy (12 patients), hemiparesis ( 1 patient), and late bacterial meningitis ( 1 patient). There were two recurrences in the patients treated with lumbar punctures and subtemporal decompression after 2 and 14 years, but in neither patient was further treatment required.
CSF Shunts Fourteen patients had a CSF shunt inserted (6 ven- triculoperitoneal, 8 lumboperitoneal). In only 1 patient was a shunt (lumboperitoneal, using the Tuohy needle method) used as the first line of treatment, and this patient showed rapid and complete resolution of all symptoms.
Of the 6 patients having a ventriculoperitoneal shunt, 4 showed complete resolution of all signs and symptoms within six months despite earlier failure to respond to other forms of treatment. Of the other 2 patients, the shunt blocked in 1, requiring revision, and became infected in the
Fig. 3. Mean CSF pressures in 12 patients before and after subtem- poral decompression (STD).
other, necessitating removal. Three of the 6 patients de- veloped late recurrence, but in none was further treatment required.
Of the 8 patients who had a lumboperitoneal shunt, all showed complete resolution of signs and symptoms within one month of the shunt insertion. In 3 of the patients who had a percutaneous lumboperitoneal shunt, the shunt was removed after an interval of 1 to 3 years, when the shunts were shown by isotope study to be nonfunctioning. In no patients was there recurrence. Four of the 8 patients had a standard-valved lumboperitoneal shunt. One of these 4 had severe low-pressure symptoms, necessitating a change to a high-pressure valve. The shunt subsequently became in- fected and was converted to a cisternoatrial shunt with a high-pressure valve, which has been functioning satisfac- torily for a year. The other 3 patients showed resolution of their symptoms, which have not recurred.
Other Treatment Other forms of treatment were used in 12 patients. Frusemide (furosemide) was used in 3 patients--in combi- nation with steroids in 2 and with steroids and lumbar puncture in 1. In 2 of the 3 there was resolution, while the other needed additional treatment. Acetazolamide in com- bination with other forms of therapy was also used in 3 pa- tients. In 1 patient, resolution occurred within three months, but the other 2 required further treatment. Two patients had posterior fossa decompressions coupled with lumbar punctures; both patients recovered within three months. Additional occasional methods of treatment in- cluded Benadryl (diphenhydramine), other diuretics, and magnesium sulfate, but these were always used in combina- tion with one or more of the major forms of therapy.
Discussion The treatment of benign intracranial hypertension has, in the absence of a clear understanding of the cause of the condition, remained empirical. Not only is a specific cause
BEFORE STO A F T E R STD
loot i |SO
i _ z~
t
DAYS

222 Surgical Neurology Vol 16 No 3 September 1981
of intracranial hypertension yet to be defined, but even the intracranial compartment involved--whether blood, brain, or CSF--is still a subject of controversy [11, 16, 17, 19, 21]. Indeed, despite several decades of discussion, each compartment still has its champions. This question has been reviewed in another paper [12], where it was con- cluded that an increase in the CSF volume is the cause of the intracranial hypertension although the precise mecha- nism involved in the change of CSF dynamics remains un- clear. Subsequent studies would seem to support this con- cept of increased CSF volume [25].
Other problems that hamper assessment of treatment methods include the variable natural history of benign in- tracranial hypertension and also the uncertainty as to whether a single disease entity is involved. Thus, the view is widely held that many cases of benign intracranial hypertension resolve spontaneously [3, 5, 7, 26], and the number of such cases ( 11.9% in the present study) has been reported to be as high as 35% [8].
Without additional investigations such as continuous intracranial pressure monitoring and fluorescein angiog- raphy, it is now clear that the diagnosis of benign intracra- nial hypertension may be inaccurate in a significant number of cases. Cases said to remit without treatment may, there- fore, include those without genuine intracranial hyperten- sion. In addition, some cases labeled benign intracranial hypertension or pseudotumor cerebri should clearly not be so described; this further confuses the issue with regard to treatment [15].
To establish a rational basis for treatment, it is first nec- essary to understand the pathophysiology of benign intra- cranial hypertension. If, as has been suggested, defective CSF absorption leading to an increase in CSF volume is the underlying mechanism, then the defect in absorption may be due to an increase either in sagittal sinus pressure (Pss) or in resistance to flow of CSF across the absorptive channels (Ray). It is remarkable, however, that only a very small proportion of patients exposed to the known precipitating factors of this condition [9] do develop intracranial hyper- tension. It may be that there is an underlying abnormality of CSF absorption in these patients, which is insufficient alone to cause significant intracranial hypertension al- though it may do so when some additional precipitating factor is present (i.e., a compensated system is decompen- sated by either an increase in P~s or by a further increase in Rav ). In treatment, therefore, the primary aim must be to reduce Pss or Ray directly during the period of decompensa- tion in the absorptive process.
Reports of such direct approaches to therapy have been few. Initial attempts to reduce Pss in patients with estab- lished venous obstruction have been without success [2, 18]. More recently, however, the use of a venous bypass procedure has been reported, with good effect [24]. Also
encouraging is the recent attempt to alter Ray by use of escin [23], although adequate evaluation of this method must await more detailed reports. Steroids may also have a direct effect on Ray [13], but this remains somewhat speculative.
Almost all reported cases of benign intracranial hy- pertension have been treated empirically by one or more of the variety of treatments advocated to date: serial lumbar punctures, subtemporal decompressions, steroids, acetazolamide, diuretics, CSF shunting, osmotic agents, cardiac glycosides, and division of the optic nerve sheath. All except the last two will certainly reduce intracranial tension, either by reducing the volume of one or more of the major compartments or by increasing the cranial capacity (in the case of subtemporal decompression). It is therefore not surprising that all are, to a greater or lesser degree, effective in controlling intracranial hypertension, particularly in a situation in which the problem may be only a temporary one.
Serial lumbar punctures, although advocated by Greer [8] and others, had a significant failure rate (61.2% when used alone) in the present study. Indeed, CSF drainage by lumbar puncture is likely to be inadequate except in mild cases, since with a relatively normal rate of CSF formation the fluid will rapidly reaccumulate, as has been shown by Johnston and Paterson [14]. Subtemporal decompression likewise had a high failure rate (80%) when used alone. Recent studies* using intracranial pressure monitoring in craniostenosis have shown how ineffective subtemporal de- compression can be in controlling relatively mild intracra- nial hypertension, although in patients with benign intra- cranial hypertension in whom vision is threatened, the drop in pressure may still be sufficient to protect the optic nerves. Nevertheless, subtemporal decompression now has little to recommend it as a treatment method.
In recent years steroids have emerged as the most com- mon primary form of treatment [27]; indeed, the success rate in the present study is high. The side effects of steroids range, however, from merely irritating (obesity) to life- threatening (gastrointestinal hemorrhage) and may occur in a significant number of patients. Moreover, intracranial pressure monitoring has shown that despite resolution of the signs and symptoms with prolonged steroid therapy, the intracranial pressure may remain relatively h igh-- in fact, only marginally reduced from pretreatment levels.
The possible mechanisms of action of steroids are also of interest. Certainly steroids are active at the cell membrane [29], and it may be that the steroids directly influence the conditions of fluid transfer across the arachnoid villi.
*Besser M, Johnston I: Intracranial hypertension in craniostenosis. Studies using continuous intracranial pressure monitoring. (In prepara- tion. )

Johnston et ah Benign Intracranial Hypertension 223
Under experimental conditions, acute withdrawal of steroids following high-dose administration in dogs did cause an in- crease in the resistance to flow across the absorptive chan- nels, although there were no changes in resistance while the high doses were being administered [13]. Steroids may also act by decreasing CSF production, thereby reducing CSF volume [22, 28]. In addition, they may also act by reducing brain bulk, whether in the normal or the edema- tous brain.
Diamox (acetazolamide) and cardiac glycosides are theoretically attractive in that both reduce CSF production [ 1, 20]. There has been, however, no satisfactory study of the efficacy of either one when used alone in benign intra- cranial hypertension, and the impression gained has been that neither is particularly effective.
CSF shunting has gained increasing favor in recent years, particularly with the use of lumboperitoneal shunting to overcome the problems of small ventricles [6]. Cer- tainly rapid and complete resolution of intracranial hyper- tension can be achieved by lumboperitoneal shunting, al- though against this must be balanced the complications of shunting (particularly obstruction, infection, and low- pressure symptoms). In addition, there is the possibility of error in diagnosis with the resultant risk of brain herniat ion being precipitated by the shunt procedure. In the present study, 8 patients were treated by lumboperitoneal shunting, in each patient with control of the intracranial hyperten- sion. Nevertheless, 3 patients required shunt revision, with 1 requiring more than one revision.
Both diuretics and osmotic agents have been used, primarily aimed at reducing brain bulk [10]. However, as with Diamox and cardiac glycosides, the information on both is inadequate for providing a basis for judgment.
Operat ive division of the optic nerve sheath has also been advocated in recent years [4]. While this may be ef- fective in some cases in protecting optic nerve function, it can have no influence on the disease process and seems to have nothing to commend it, for example, ahead of lum- boperitoneal shunting unless there is real doubt as to the true diagnosis.
In summary, in the majority of cases there is no satisfac- tory direct therapeutic approach to the underlying defect in benign intracranial hypertension, although recent reports (such as that concerning the use of escin) are encouraging and may represent an advance in this direction. A t present, therefore, therapy must remain indirect, aimed at reducing intracranial volume. It seems probable that relatively small changes will be sufficient not only to protect vision but also to alleviate symptoms, and that all forms of t reatment dis- cussed will have some measure of success. To judge from the available figures, however, steroids would seem the most appropriate initial form of treatment. If intracranial hyper- tension persists or recurs after a course of steroids, particu-
larly if there is evidence of visual deterioration, lum- boperitoneal shunting should be the next step in treatment. In those patients in whom there is doubt concerning the diagnosis, optic nerve sheath decompression or ventricular shunting may be preferable. For the future it is to be hoped that a clearer understanding of the basic disorder in benign intracranial hypertension may allow an increasingly more direct approach to therapy in the majority of patients.
References 1. Ames A, Higashi K, Nesbett FB: Effects of pCO2, acetazolamide and
ouabain on volume and composition of choroid plexus fluid. J Physiol 181:516-524, 1965
2. Bresnan MJ, Strand R, Rosenbaum A: Jugular venous block asso- ciated with benign intracranial hypertension. Neurology (Minneap) 23:390, 1973
3. Dandy WE: Intracranial pressure without brain tumor. Ann Surg 106:492-513, 1937
4. Davies G, Zilkha KJ: Decompression of the optic nerve in benign intracranial hypertension. Trans Ophthalmol Soc UK 96:427-429, 1976
5. Foley J: Benign forms of intracranial hypertension. Toxic and otitic hydrocephalus. Brain 78:1-41, 1955
6. Giicer G, Viemstein L: Long-term intracranial pressure recording in the management of pseudotumor cerebri. J Neurosurg 49:256-263, 1978
7. Grant DN: Benign intracranial hypertension. A review of 79 cases in infancy and childhood. Arch Dis Child 46:651-655, 1971
8. Greer M: Management of benign intracranial hypertension. Clin Neurosurg 15:161-174, 1968
9. Greer M: Benign intracranial hypertension (pseudotumour cerebri), in Vinken PJ, Bruyn GW (eds): Handbook of Clinical Neurology. Amsterdam, New York: North Holland/American Elsevier, 1974, Vol 16, Pt 1, pp 150-166
10. Jefferson AA, Clark J: Treatment of benign intracranial hypertension by dehydrating agents. J Neurol Neurosurg Psychiatry 39:627-639, 1976
11. Johnston h The reduced CSF absorption syndrome: a reappraisal of benign intracranial hypertension and related conditions. Lancet 2:418-420, 1973
12. Johnston I: The definition of a reduced CSF absorption syndrome: a reappraisal of benign intracranial hypertension and related condi- tions. Med Hypotheses 1:10-14, 1975
13. Johnston I, Gilday DL, Hendrick EB: The effects of steroids and steroid withdrawal on CSF absorption. An experimental study in- dogs. J Neurosurg 42:690-695, 1974
14. Johnston I, Paterson A: Benign intracranial hypertension. 2: CSF pressure and circulation. Brain 97:301-312, 1974
15. Mantovani JF, Naidich TP, Prensky AL, Dodson WE, Williams JC: MSUD: Presentation with pseudotumor cerebri and CT abnor- malities. J Pediatr 96:279-281, 1980
16. Mathew NT, Meyer JS, Otto E: Increased cerebral blood volume in benign intracranial hypertension. Neurology (Minneap) 25:646-649, 1975
17. Raichle ME, Grubb RL Jr, Phelps ME, Gado MH, Caronna JJ: Cere- bral hemodynamics and metabolism in pseudotumor cerebri. Ann Neurol 4:104-111, 1978
18. Ray BS, Dunbar HS: Thrombosis of the dural venous sinuses as a cause of pseudotumor cerebri. Ann Surg 134:576-586, 1951
19. Rottenberg DA, Foley KM, Posner JB: The pathogenesis of pseudotumor cerebri. Med Hypotheses 6:913-918, 1980
20. Rubin RC, Henderson ES, Walker MO, Rall DD: The production of cerebrospinal fluid in man and its modification by acetazolamide. J Neurosurg 25:430-436, 1966
21. Sahs AL, Joynt RJ: Brain swelling of unknown cause. Neurology (Minneap) 6:791-803, 1956

224 Surgical Neurology Vol 16 No 3 September 1981
22. Sato O, Hara M, Asai T: The effect of dexamethasone phosphate on the production rate of cerebrospinal fluid in the spinal subarachnoid space of do~s. J Neurosurg 39:480-484, 1973
23. Scanarini M, Mingrino S, d'Avella D, Della Corte V: Benign intra- cranial hypertension without papilledema. Neurosurgery 5:366-367, 1979
24. Sindou M, Mercier P, Bokor J, Bmnon J: Bilateral thrombosis of the transverse sinuses: microsurgical revascularization with venous by- pass. Surg Neurol 13:215-220, 1980
25. Sklar FH, Beyer CW, Ramanathan M, Cooper PR, Clark WK: CSF
dynamics in patients with pseudotumor cerebri. Neurosurgery 5:208-216, 1979
26. Smith JL: Pseudotumor cerebri. Trans Am Acad Ophthalmol 62:432-440, 1958
27. Vassilouthis J, Uttley D: Benign intracranial hypertension: clinical features and diagnosis using CT and treatment. Surg Neurol 12:384- 392, 1979
28. Weiss MH, Nulsen FE: The effect of glucocorticoids on CSF flow in dogs. J Neurosurg 32:452-458, 1970
29. Wiltmer EN: Steroids and cell surfaces. Biol Rev 36:368-398, 1961
Editorial: Writing
Frequently editors of medical journals are asked to tell pro- spective authors how to write. Efforts in this direction are largely futile except for the most elementary advice. It should be obvious that writing a scientific article requires entirely different language from that which is used in writ- ing short stories or novels. Scientific articles should be written in a straightforward manner and should be clear and concise. No effort should be made to impress the reader with one's ability to form complex sentences or to use ex- otic words and phrases. Writers must always bear in mind that their purpose is to convey as clearly as possible their thoughts and ideas as well as the results of their research or clinical study. To attain this end, authors of articles for publication in Surgical Neuro~gy must bear in mind that approximately 40% of the readers of the journal reside outside of the United States and have a language other than English as their native language. For them English is an acquired language and their mastery of it varies widely. To convey one's thoughts to them requires that one express himself succinctly.
For years the University of Iowa has had one of the most outstanding Writers' Workshops in the world. Undoubtedly the success of this workshop can be attributed largely to the efforts of its three succeeding directors, Wilbur Schramm, his successor, Paul Engle, and the present Director, John W. Legget. This workshop has no set means of creating writers who can use the English language appropriately. In- stead they have endeavored to create an atmosphere of friendliness and respect for the art. One of the graduates of the Iowa workshop, Gail Godwin (Master's Degree, 1968; Ph.D., 1971) has described the atmosphere there well. She wrote:
I had never been in a situation like that before, a situation where 1 had to take myself seriously, both because I had the time, the space, the quiet, and because other people around me were writ- ing. So I came of age there. I blossomed. I finally got down to writing. 1 became a professional writer at Iowa.
The first spring I was there I found it all so stimulating that I began staying up all night and writing. Then I would sleep in the daytime until two o'clock . . . . For the first time, I felt that I was alone with what mattered. It was not only the writing, and the people who were writers that impressed me. It was also the place, this mythical place with all its ghosts of famous writers from the past. In the wintertime it's like a blank page.
The Editors of Surgical Neurology cannot teach you how to write, but they can point out some of the common pit- falls which you should avoid. First, follow the adage, "Keep it simple, simple." Avoid long, complicated sentences and unfamiliar words and phrases. Do not use any but the most familiar abbreviations. Anyone who reads in a foreign lan- guage can appreciate the frustration when one encounters an abbreviation with an unknown meaning. Recently, in a single letter in The Lancet, one encounters such abbrevia- tions as "AFP," " N T D , " and "ACHE." The amount of ink and paper saved by using these abbreviations does not com- pensate for the difficulty in reading and comprehension that these abbreviations cause.
Would that we all could at tend the Iowa Writers' Work- shop. Since that is impossible, we must do the next best. Always ask someone not directly concerned with the re- search or the clinical study to read your article for clarity of meaning before you submit it to any editor.
Paul C. Bucy, M.D., Editor


























![[J] Evidence review for managing intracranial hypertension](https://img.pdfslide.us/doc/110x75/61f6c94d34312d56685df001/j-evidence-review-for-managing-intracranial-hypertension.jpg)
