Embed Size (px)
Citation preview

ANATOMY
© 2004 The Medicine Publishing Company Ltd394ANAESTHESIA AND INTENSIVE CARE MEDICINE 5:12
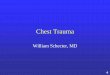
The thoracic inlet, small and kidney-shaped, is about 10 cm wide and 5 cm anteroposteriorly. It slopes forward and is bounded by the first thoracic vertebra posteriorly, the upper border of the manubrium anteriorly and the first rib and costal cartilage later-ally. It transmits the oesophagus, the trachea, and the large vessels comprising the right and left subclavian arteries, and the right and left brachiocephalic veins, which unite behind the lower border of the right first costal cartilage to form the superior vena cava. Lying on the neck of the first rib posteriorly is the sympathetic trunk. On each side is the apex of the lung, some 3 cm above the medial third of the clavicle, covered by the dome of the pleura (Figure 1). The subclavian arteries commence behind the sternoclavicular joint and curve laterally in front of the apex of the lung before passing on to the upper surface of the first rib. Both subclavian veins lie anterior to their respective arteries curving medially from the middle third of the clavicle to form the brachiocephalic vein by joining their internal jugular vein behind the sternoclavicular joint. The first rib (Figure 2) is short, wide, flattened and lies in an oblique plane, sloping forwards and downwards. It possesses a head that articulates with the body of the first thoracic vertebra, a rounded neck, a posterior tubercle and a body. The anterior end of the body bears the costal cartilage, which articulates with the manubrium. Its head bears a single facet for articulation with the first thoracic vertebra and posteriorly it bears a small tubercle posteriorly on its angle. The lower surface of the body is smooth and lies on the pleura. A small scalene tubercle on its medial border marks the attachment of the scalenus anterior muscle and this tubercle, on the upper surface of the body, separates an anterior groove for the subclavian vein from a posterior groove for the subclavian artery and the lower trunk of the brachial plexus which lies behind the artery. Scalenus medius is attached to the upper surface of the body behind the groove for the artery.Anterior to the neck of the rib and behind the pleura lie, from medial to lateral, the sympathetic trunk and the large branch of the first thoracic nerve to the brachial plexus. The proximity to the surface and the constancy of their surface anatomy allows percutaneous access to the large veins in this region; the subclavian vein can be catheterized for intravenous feeding or monitoring central venous pressure. The infraclavicular
The thoracic inlet and first ribJohn Craven
John Craven was formerly Consultant Surgeon at York District Hospital,
York, UK. He trained in Manchester, Uganda, and Cardiff. He is past
chairman of the primary examiners of the Royal College of Surgeons of
England.
approach is preferred because there is less chance of accidental puncture of the pleura by this route (Figure 3). The needle is inserted one finger’s width below the midpoint of the clavicle and directed medially and as far anteriorly as possible (to ensure that neither the pleura nor the subclavian artery is pierced) towards the jugular notch of the manubrium. The subclavian vein should be entered as it curves over the body of the first rib.
The thoracic inlet
Dome of pleura
Brachial plexus
Subclavian artery
Subclavian vein
Superior vena cava
Scalenus anterior
Phrenic nerve
Thoracic duct
Oesophagus
Trachea
First rib
Upper surface of the first rib
First thoracic nerve (upper branch)
Highestintercostalartery
Sympathetic trunk
Scalenus posteriorScalenus mediusSubclavian arterySerratus anteriorScalenus anteriorSubclavian vein
Costoclavicular ligament
Posterior
Anterior
Infraclavicular access to the large veins
Clavicle
Entry site
Subclavian veinentered above first rib
First rib
Directionof needle
Jugular notch
1
2
3