Embed Size (px)
Citation preview
The third international stroke trial (IST-3) of thrombolysis main results III. Effect of iv thrombolysis with iv rt-PA on death or
dependency in the 3035 patients randomised: subgroup analyses
The IST3 collaborative group - 156 hospitals in UK, Poland, Italy, Sweden, Norway, Australia, Portugal, Belgium, Austria,
Switzerland, Canada, Mexico
Disclosures: Boehringer Ingelheim donated rt-PA and placebo for the first 300 patients but had no other part in the study.
Main features of IST - 3 • Prospective, randomised, open study of i.v. rt-PA vs
control, • Target 3100 patients• < 6 h of acute ischaemic stroke • Primary outcome: the proportion of patients alive and
independent at six months • Randomisation by telephone or internet with
minimisation to balance on key prognostic factors• Baseline & F/U Imaging: CT or MR
– Blinded central expert panel review of scans
Methods: analysis plan • Pre-specified key subgroups
– age < >80 – time from stroke onset to randomisation– initial stroke severity (NIHSS) – visible ischaemia on baseline brain scan +/-
• The key test for variation in rt-PA effect in subgroups was a test for interaction
• Because of multiple testing we show 99% confidence limits for each subgroup.
• We also present an additional subgroup of prior antiplatelet therapy (ARTIS trial results to follow)
Expected direction of subgroup effects*
Relative benefit in the primary outcome will be less with: •Older age •Greater initial stroke severity•Longer delay times to treatment •Ischaemic change on baseline scan.
Null hypothesis tested: benefit does not differ between subgroup categories
*International Journal of Stroke 2012; 7: 186-187
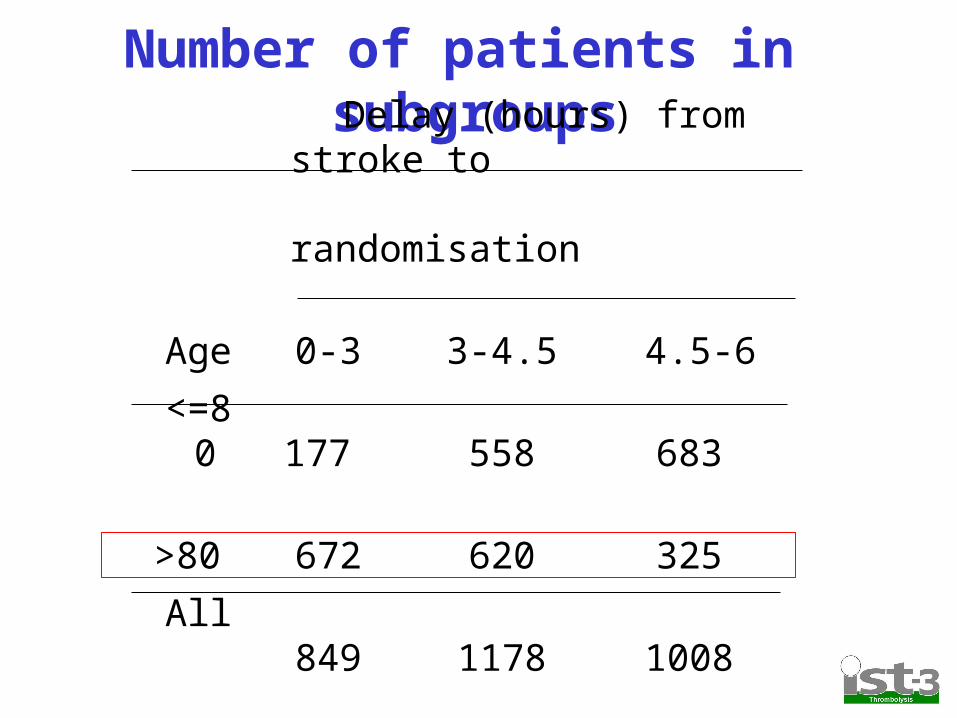
Number of patients in subgroups Delay (hours) from stroke to
randomisation
Age 0-3 3-4.5 4.5-6
<=80 177 558 683
>80 672 620 325
All 849 1178 1008

Overall Results
Outcome
Adjusted Odds Ratio
95% Confidence Interval p value
Alive and independent (mRS 0-2)
1.13 0.95 to 1.35 p = 0.181
Ordinal analysis (mRS rank)
1.27 1.10 to 1.47 p = 0.001

Detecting true subgroup differences
• Potential to be unreliable for primary outcome
• Most reliable for ordinal analysis (the most “efficient” analysis)

Effect on Alive and Independent (OHS 0-2) in key subgroups: Unadjusted analyses

Rationale for Adjusted Analyses
• Baseline data showed important trends with delay from stroke onset to randomisation.– Older randomised earlier– More severe stroke early– Visible ischaemia on CT/MR increased with
later treatment
• Therefore analyses adjusted for these factors

Effect on Alive and Independent (OHS 0-2) in key subgroups: Adjusted analyses
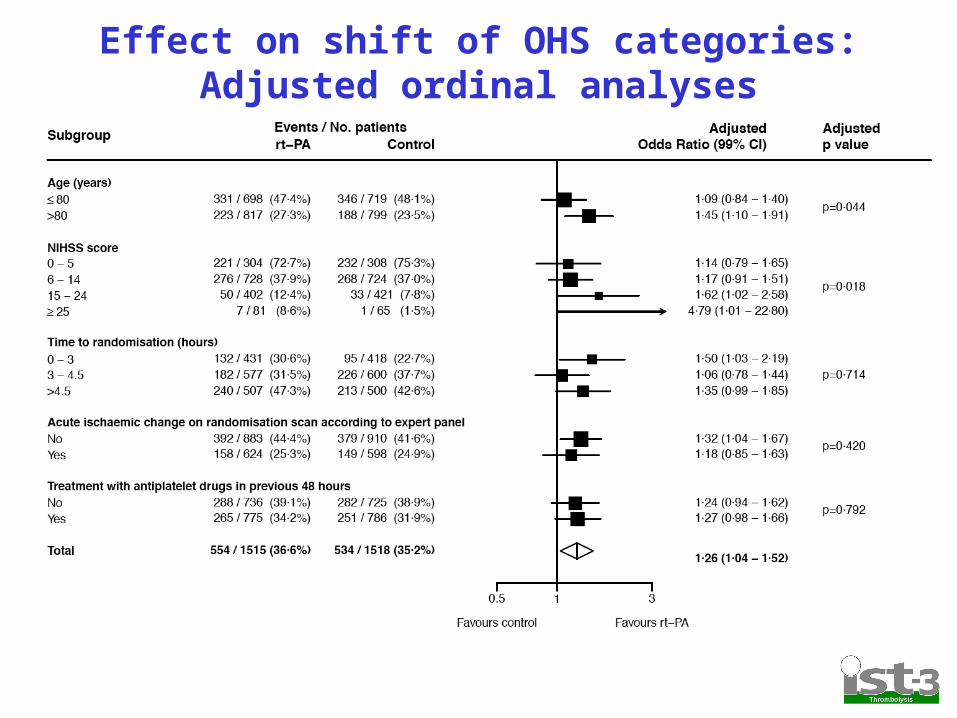
Effect on shift of OHS categories: Adjusted ordinal analyses

Delay to randomisation and treatment benefit (favourable shift in OHS)*
*Ordinal analysis adjusted for age, baseline NIHSS, and ‘visible ischaemia’
Benefit
Harm
99% CI shown
<= 2 2-3 3-4 4-5 5-6 Hours from onset – randomisation
Conclusions (1)
1) Benefit was greatest with treatment within 3 hours (80 per 1,000 more alive and independent treated within 3 hours)
2) Benefit evident •Age > 80 years•Severe stroke•Early ischaemic change seen on baseline scan.

Conclusions (2)
• Treatment with rt-PA can now be considered for a wider range of patients, particularly the elderly, provided its given early
• Remaining uncertainties, including factors that predict early hazard, will be addressed by the planned individual patient meta-analysis
Acknowledgements:The 3035 patients, the 156 hospitals in the IST-3 group, the Data
Monitoring Committee, the MRC Steering Committee, Image Reading Panel, Event adjudication panel, International Advisory Board.
Funding: Medical Research Council (managed by NIHR on behalf of the MRC-NIHR partnership), Stroke Association, The Health Foundation,, The Research Council of Norway, AFA Insurances (Sweden), the Swedish Heart Lung Fund, The Foundation of Marianne and Marcus Wallenberg, Stockholm County Council and Karolinska Institute Joint ALF-project grants (Sweden), the Government of Poland, the Australian Heart Foundation, Australian NHMRC, the Swiss National Research Foundation, the Swiss Heart Foundation, the Foundation for health and cardio-/neurovascular research, Basel, Switzerland and the Assessorato alla Sanita, Regione dell'Umbria. Drug and placebo for the 300 patients in the double-blind component of the start-up phase were supplied by Boehringer-Ingelheim GMBh. IST-3 acknowledges the extensive support of the NIHR Stroke Research Network , NHS Research Scotland (NRS), through the Scottish Stroke Research Network, and the National Institute for Social Care and Health Research Clinical Research Centre (NISCHR CRC). The imaging work was undertaken at the Brain Imaging Research Centre, a member of the SINAPSE collaboration, at the Division of Clinical Neurosciences, University of Edinburgh. SINAPSE is funded by the Scottish Funding Council (SFC) and the Chief Scientist Office of the Scottish Executive (CSO). Additional support was received from Chest Heart and Stroke Scotland, Desacc, University of Edinburgh, Danderyd Hospital R&D Department, Karolinska Institutet, the Dalhousie University Internal Medicine Research Fund.