Embed Size (px)
Citation preview

The Structure of Economic Incentives in the Robert Wood Johnson/HUD Program on Chronic Mental Illness 1988 Richard G. Frank, Ph.D. Catherine A. Jackson, Ph.D. Frances L. Lynch, M.S.P.H.
Abstract This paper describes the financial arrangements put into place by cities participating in the Robert
Wood Johnson Foundation's Program on Chronic Mental Illness. Descriptive information is given on the level of expenditure, the mix of revenues, and the terms under which local, federal, and Medicaid dollars are allocated to local programs. Data are presented on the use of state hospitals and the number of severely mentally ill individuals in treatment. These data are used to make obser- vations on the initial stages of the demonstration.
Introduction Public mental health systems have evolved into a constellation of services providers whose activi-
ties are funded by public dollars for the treatment of persons with severe mental illness. A body of influential thought regarding the structure of these service systems has forwarded the idea that a primary goal of a service system should be to recreate the functions of the mental hospital in a community contextJ Specifically, the public mental health system should be able to respond to the range of needs exhibited by the severely mentally ill living in the community. These needs include housing, subsistence, social services, and health and mental health care. Moreover, the service system should ideally be sufficiently flexible to accommodate client needs in the variety of circumstances in which the mentally ill are found (e.g., prisons, sheltered housing, and the mainstream of society).
Clinical experiments have demonstrated that coordination of diverse services results in improved outcomes at comparable costs. 2,3 These experimental results, coupled with the persistently high levels of emergency room and public mental hospital use by severely mentally ill individuals dependent on the public system, have led to the suggestion that improved coordination of services at the service
Address correspondence to Richard G. Frank, Ph.D., Department of Health Policy and Management, School of Hygiene and Public Health, Johns Hopkins University, 624 N. Broadway, Baltimore, MD 21205.
Catherine A. Jackson, Ph.D., is with the Rand Corporation. Frances L. Lynch, M.S.P.H., is with Johns Hopkins University. The national evaluation of the Robert Wood Johnson Foundation Program on Chronic Mental Illness (RWJ-PCMI) is
supported by grants from the Robert Wood Johnson Foundation, the Ohio Department of Mental Health, the National Institute of Mental Health and several other federal agencies to the Mental Health Policy Studies Program, Department of Psychiatry, University of Maryland School of Medicine.
20 The Journal of Mental Health Administration 20:1 Spring 1993

system level is necessary in order to improve the performance of the public mental health system. 4.s The Robert Wood Johnson Foundation Program on Chronic Mental Illness (RWJ-PCMI) is found-
ed on these ideas about how the public mental health system should be structured. A major goal of the program is the centralization of clinical, administrative, and financial responsibility for public mental health care at the local level. 6
This paper examines the fmancing mechanisms within the public mental health system, focusing on the economic incentives created alongside centralization of the local mental health system. Specif- ically, the mental health services systems in the nine RWJ-PCMI demonstration cities are described with emphasis on the incentives provided through the different mix of financing mechanisms avail- able in each area. This description is then used to assess the potential for reaching the overall RWJ- PCMI program goals. The paper is organized as follows. First, the conceptual framework for the examination will be discussed. Next the data sources are reviewed. A comparison of the dimensions of system structure for the nine RWJ demonstration sites is then presented. Finally, a summary and set of conclusions close the paper.
Conceptual Framework The RWJ-PCMI was designed to effect changes in the financing of services for the severely
mentally ill by providing local mental health authorities the incentives and flexibility to innovate in order to improve the performance of the services system. A number of federal, state, and local policies determine funding for the local public mental health system. The structure of each of these programs along with the interrelationships between these programs influence local mental health authority design and the provision of local mental health services. The terms of intergovemmental transfers between federal, state, and local government shape both the type of services provided and the popula- tion groups served at the local level. The nine RWJ sites have used different mixtures of financing policies in order to address some of the limitations of the current public mental health system. The remainder of this paper will focus on several key policies shaping public mental health services.
One critical component of the financing of care is local policies for funding mental health services. Local decisions about financing of mental health care such as property tax levies and allocations from county general funds provide very flexible sources of funding for local mental health authorities. For example, in several of the RWJ-PCMI sites, localities may raise money through an earmarked proper- ty tax levy. Ohio has this type of levy system. This type of policy gives local mental health authorities a great deal of flexibility in the design of local services. These funds have fewer restrictions than funds received through intergovemmental transfer programs.
Another important aspect of financing of local mental health services is the design of state Medic- aid programs. State Medicaid programs can be tailored by individual states to offer an array of benefits in addition to certain minimum benefit requirements set by the federal government. Taube, Goldman, and Salkever 7 argue that Medicaid programs should be structured to encourage the use of existing community treatment technologies. The Medicaid program is the largest payer for commtmi- ty mental health services in the nation; however, it has traditionally created strong incentives for hospital treatment of the mentally ill by providing low reimbursement for outpatient treatment and restricting the types and delivery locations of services which are reimbursed/In recent years, the federal rules governing the program have become more flexible, making innovation increasingly possible where states choose to make program changes.
A third important policy that has been proposed for improving mental health systems is the creation of mechanisms which reduce the resources devoted to public mental hospitals? Currently, roughly 65% of the money spent by state mental health agencies is allocated to public mental hospital systems. A consensus has emerged suggesting that there are "too many resources" devoted to public
Economic Incentives in RWJ-PCMI FRANK, JACKSON, LYNCH 21
hospital systems of the United States. 9 This view contributed to the development of the Ohio Mental Health Act of 1988, which provided mechanisms to transfer both responsibility and funding to local mental health authorities as a means of reducing use of state mental hospitals.
The typical public mental health system is structured so that the local mental health authority may use the state hospital at no "on-budget" cost, subject to a capacity constraint. In addition, there is generally excess demand for community treatment. As a result, local programs are able to avoid treating the most severely disabled patients, who are also the most costly to serve, by making use of the "free" services of the state mental hospital.
Efforts to alter the allocation of resources between community programs and institutional care rely on two sets of policy tools: capacity constraints on state mental hospitals and the terms of intergovern- mental transfers. Both approaches are represented in the cases described below.
Measurement of System Structure Data for this analysis were collected from several major sources. Data on budgets and financing of
public mental health services were obtained from the annual reports of state and local agencies, state budget allocation documents, agencies' computerized management information systems, and person- al correspondence with individual agencies. Information on the structure of intergovemmental finan- cial relations (primarily at the state and local levels) was obtained from site visit interviews with state and local officials, operation policy manuals, legislation, and special reports produced by state and local government units responsible for mental health care. Goldman, Morrissey, and Ridgely 1~ de- scribe elsewhere the organizational aspects of the local mental health authorities participating in the demonstration.
Information on state mental hospital use was obtained primarily from the management information systems in each city. Descriptions of the various state Medicaid programs were obtained from the Health Care Financing Administration, state Medicaid plans, the Congressional Research Service, and the National Mental Health Association (a detailed appendix of the governmental documents used can be obtained from the authors).
Comparative Dimensions of System Structure in the Nine RWJ Sites The ability of local mental health authorities to provide a rich array of services for the severely
mentally ill is affected by the economic parameters under which those authorities operate. Specifical- ly, total resources devoted to mental health care services, the sources of revenues for community mental health services, and local autonomy allowed by different funding sources in the use of resourc- es are important dimensions in the economic environment of public mental health services systems.
Total Financial Resources Total financial resources in the local mental health system indicate the degree to which resources
are available to serve the at-risk population in the community. Therefore, expenditures on services in public mental hospitals are excluded. Table 1 summarizes the 1988 expenditure levels per capita for the nine RWJ-PCMI demonstration cities. The numbers are not perfectly comparable; this is partly because of an inability to segregate dollars for special purposes in some cases and because of the absence of data on certain elements for certain cities. Nevertheless, the numbers are broadly reflective of the total commitment of resources in each city.
For interpretation of the data, it is important to recognize that economic factors such as labor costs may vary considerably across the nine cities. Thus, a portion of the observed variation in per capita community mental health expenditures is, no doubt, due to variations in the cost of living and other
22 The Journal of Mental Health Administration 20:1 Spring 1993

Table 1 Mental Health Expenditures (1988)
Site Total $ Population Per Capita $
Austin 14,333,490 545,587 26.27 Baltimore 23,266,087 753,000 30.90 Charlotte 18,285,505 466,100 39.23 Cincinnati 28,656,576 873,900 32.79 Columbus 41,241,818 939,676 43.89 Denver* 23,984,478 505,000 47.49 Honolulu** 35,827,922 1,098,000 32.63 Philadelphia*** 110,822,977 1,643,000 67.45 Toledo 19,590,032 462,900 42.32
* Inpatient expenditures are from estimates for FY 1990, adjusted to 1988 dollars. The other components are actual 1988 figures.
** 1988-1989. Total budget and population for entire state of Hawaii. *** 1989 figures, adjusted to 1988 dollars.
such factors. However, there are rather dramatic differences in per capita public mental health expen- ditures across the nine cities which exceed any cost-of-living adjustment. For example, there is more than a 100% difference between the city with the lowest level of per capita expenditures (Austin) and the city with the highest level of per capita expenditures (Philadelphia). Even if Austin and Philadel- phia are eliminated from consideration, there is still a 50% difference between the highest and lowest levels of per capita expenditures in the seven remaining cities (i.e., Baltimore with $30.90 per capita and Denver with $47.49 per capita). The results reported in Table 1 indicate important differences in the resources available to each local mental health authority for providing public mental health care. Although a high level of resource commitment is not the only important determinant of the potential of a local area to serve the severely mentally ill, it provides a baseline indication of the degree to which service improvement is possible.
Sources of Revenue One indicator of the opportunity for a local mental health authority to innovate to meet local needs
is the portion of the public mental health system budget that stems from local sources such as the city and county. It has been posited that successful organization of mental health services relates to the financial autonomy of the local mental health authority. This is based on the notion that the greater the local fiscal control, the more the local mental health system can be structured to meet the specific circumstances of the locality.
Table 1 describes the overall resources per capita in each RWJ site, and Table 2 presents the revenue shares by funding source for the nine demonstration cities. Tables 1 and 2 together suggest four general scenarios for mix of funding: (1) several cities exhibit both high commitments of re- sources and high levels of local control over resources - - Charlotte, Columbus, and Toledo; (2) two cities exhibit low levels of resource commitment in the mental health system coupled with high levels of local control - - Austin and Cincinnati; (3) two cities have high levels of expenditures with virtually no local dollars in the budget - - Denver and Philadelphia; and (4) two cities have both relatively low levels of expenditures and little local financial participation in the mental health system - - Baltimore and Honolulu. These scenarios suggest that financing of public mental health services has at least two
Economic Incentives in RWJ-PCMI FRANK, JACKSON, LYNCH 23

Table 2 Percent Distribution of Revenues by Source (1988)
Medicaid Site State Federal Local and Fees
Austin 46 9 44 1 Baltimore 52 4 1 43 Charlotte 44 5 49 2 Cincinnati 24 4 49 18 Columbus 29 8 45 15 Denver 54 2 4 40 Honolulu* 86 14 0 0 Philadelphia 42 N/A 4 29 Toledo 27 10 35 25
* Distribution for mental health revenues FY 1989.
dimensions: level of funding and local control. Figure 1 characterizes the nine demonstration cities within these two dimensions.
Funding Sources Here is a detailed breakdown of the sources of funding available in each RWJ site.
Local Funding Column 3 of Table 2 presents the share of the total expenditures on mental health care that comes
from local sources. The three cities in Ohio (Cincinnati, Columbus, and Toledo), along with Char- lotte, N.C., have the highest portions of their budgets originating locally, while the funding for the remainder of the sites is spread predominantly between state funds, Medicaid, and patient fees. The mental health boards in Ohio are organized as special districts (similar to school boards in the rest of the nation) and are permitted to propose a direct property tax levy to local voters every five years. The tax revenues from these levies are controlled directly by the local mental health board. In Charlotte, where local dollars also comprise a large share of the budget, the mental health authority is a direct line item in the county budget, allowing the authority considerable latitude in what services are provided. Austin receives contracts directly from both the city and county to provide mental health services. Philadelphia receives some local funding; Medicaid revenues, however, are returned to the state general revenue fund, effectively placing a 100% tax on CMHC Medicaid reimbursements. The other three cities represent situations where the state and/or the Medicaid program are the primary sources of funding.
The mechanisms used for local financing of mental health care indicate the degree of discretion and programmatic autonomy of the local mental health authority. Table 3 displays the method of funding of local mental health authorities by city. Contract, in-kind services, and matching dollars offer the least discretion, constraining the authority's ability to innovate in service delivery. For example, in the city of Denver, virtually the entire local contribution consists of in-kind services in the form of inpatient mental health care provided by the city-owned general hospital's psychiatric unit. Thus, while the city's contribution to the local mental health authority may appear large, the local mental health authority cannot vary the types of services that are delivered, thus reducing the level of
24 The Journal of Mental Health Administration 20:1 Spring 1993

Figure 1 Dimensions of Public Mental Health Funding
Overall Funding Level
high
Local Control
little
Denver Philadelphia
Baltimore Honolulu
Charlotte Columbus
Toledo
Austin Cincinnati
a lot
low
funding for innovation in services delivery. In contrast, dollars from taxes earmarked for local public mental health services, such as those in the Ohio cities, offer the most autonomy since the local mental health authority can develop services that meet the needs of the community. Line item allocations, as found in Charlotte, also offer considerable discretion in a fashion similar to a block grant. A comparison of Tables 2 and 3 reveals that those cities with low rates of local financial participation also tend to receive the dollars in a form that offer the mental health authority tittle programmatic discretion (i.e., Denver and Philadelphia).
State Funds State government policy toward the provision of mental health care at the local level can also
create opportunities for local control and innovation. States make decisions with respect to (1) the method by which state general funds are transferred to localities and (2) the design of the Medicaid
Table 3 Financing from Local Sources
City Financing Source
Austin local contracts Baltimore city allocation Charlotte allocation from county + match Cincinnati local tax levy Columbus local tax levy Denver in-kind contribution Honolulu not applicable Philadelphia match for state dollars Toledo local tax levy
Economic Incentives in RWJ-PCMI FRANK, JACKSON, LYNCH 25

Table 4 State Policies Concerning Local Control of Mental Health Services
City
Overall State General Local Mental Medicaid Funds
Control Health Options Eligibility Program Incentives
Austin L L R LG W Baltimore L C SR G M Charlotte E L SR LG W Cincinnati E C R G S Columbus E C R G S Denver L C R S M Honolulu NA L R LG W Philadelphia L L I G W Toledo E C R LG S
Key: L, limits L, limited R, restrictive LG, less generous S, strong
E, encourages C, compr- SR, somewhat G, generous W, weak ehensive restrictive
NA, not applicable I, inclusive S, stringent M, moderate
program. States may make transfers to localities that offer each mental health authority considerable discretion in program design. At one extreme lies the block grant form of intergovernmental transfer. This method transfers to a locality a lump sum of money to be spent as the local authority chooses. This is the most flexible approach and is similar to line item funding. At the opposite extreme is the fee for service arrangement with a spending limit, where a locality must deliver a specified number of units of service within a spending limit constraint. Such an approach offers little opportunity to creatively bundle services to meet the diverse needs of people with severe mental illness. Column 1 of Table 4 summarizes the states' policies toward local mental health authorities control over funding. Column 5 of Table 4 describes the level of incentive - - strong, moderate, or weak - - provided by state polices regarding the transfer of state general funds.
The closed-end matching arrangement found in North Carolina offers considerable flexibility to the locality, while at the same time encouraging local fmancial participation in the mental health system. Ohio's system of categorical grants represents a middle ground that retains flexibility for the local board within a general program category defined by the state.
State Medicaid programs are another important component of state funding. Three aspects of state Medicaid programs are important determinants of utilization of services by the severely mentally ill. First, the number of mental health related optional services covered and the degree of limitation placed on these services can be critical constraints in providing care for the severely mentally ill. Second, the design of eligibility policies can either encourage or limit coverage of severely mentally ill people. For example, the coverage of optional SSI categories is especially important for the SMI. Finally, the overall generosity of a Medicaid program, indicated by the entire package of benefits and reimbursement policies, can create incentives for mental health authorities to seek Medicaid reim- bursement for clients, which may add dollars to the mental health system.
Columns 2, 3, and 4 of Table 4 categorize the Medicaid programs in the seven states represented in the demonstration with respect to service options available, eligibility requirements, and overall pro-
26 The Journal of Mental Health Administration 20:1 Spring 1993
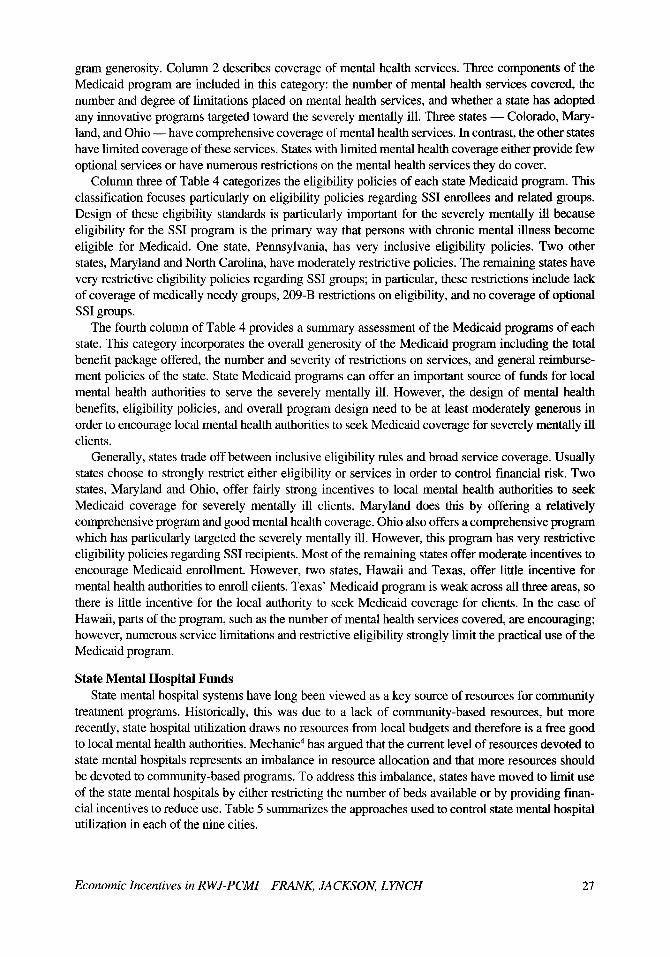
gram generosity. Column 2 describes coverage of mental health services. Three components of the Medicaid program are included in this category: the number of mental health services covered, the number and degree of limitations placed on mental health services, and whether a state has adopted any innovative programs targeted toward the severely mentally ill. Three states - - Colorado, Mary- land, and Ohio - - have comprehensive coverage of mental health services. In contrast, the other states have limited coverage of these services. States with limited mental health coverage either provide few optional services or have numerous restrictions on the mental health services they do cover.
Column three of Table 4 categorizes the eligibility policies of each state Medicaid program. This classification focuses particularly on eligibility policies regarding SSI enrollees and related groups. Design of these eligibility standards is particularly important for the severely mentally ill because eligibility for the SSI program is the primary way that persons with chronic mental illness become eligible for Medicaid. One state, Pennsylvania, has very inclusive eligibility policies. Two other states, Maryland and North Carolina, have moderately restrictive policies. The remaining states have very restrictive eligibility policies regarding SSI groups; in particular, these restrictions include lack of coverage of medically needy groups, 209-B restrictions on eligibility, and no coverage of optional SSI groups.
The fourth column of Table 4 provides a summary assessment of the Medicaid programs of each state. This category incorporates the overall generosity of the Medicaid program including the total benefit package offered, the number and severity of restrictions on services, and general reimburse- ment policies of the state. State Medicaid programs can offer an important source of funds for local mental health authorities to serve the severely mentally ill. However, the design of mental health benefits, eligibility policies, and overall program design need to be at least moderately generous in order to encourage local mental health authorities to seek Medicaid coverage for severely mentally ill clients.
Generally, states trade off between inclusive eligibility rules and broad service coverage. Usually states choose to strongly restrict either eligibility or services in order to control financial risk. Two states, Maryland and Ohio, offer fairly strong incentives to local mental health authorities to seek Medicaid coverage for severely mentally ill clients. Maryland does this by offering a relatively comprehensive program and good mental health coverage. Ohio also offers a comprehensive program which has particularly targeted the severely mentally ill. However, this program has very restrictive eligibility policies regarding SSI recipients. Most of the remaining states offer moderate incentives to encourage Medicaid enrollment. However, two states, Hawaii and Texas, offer little incentive for mental health authorities to enroll clients. Texas' Medicaid program is weak across all three areas, so there is little incentive for the local authority to seek Medicaid coverage for clients. In the case of Hawaii, parts of the program, such as the number of mental health services covered, are encouraging; however, numerous service limitations and restrictive eligibility strongly limit the practical use of the Medicaid program.
State Mental Hospital Funds State mental hospital systems have long been viewed as a key source of resources for community
treatment programs. Historically, this was due to a lack of community-based resources, but more recently, state hospital utilization draws no resources from local budgets and therefore is a free good to local mental health authorities. Mechanic 4 has argued that the current level of resources devoted to state mental hospitals represents an imbalance in resource allocation and that more resources should be devoted to community-based programs. To address this imbalance, states have moved to limit use of the state mental hospitals by either restricting the number of beds available or by providing finan- cial incentives to reduce use. Table 5 summarizes the approaches used to control state mental hospital utilization in each of the nine cities.
Economic Incentives in RWJ-PCMI FRANK, JACKSON, LYNCH 27
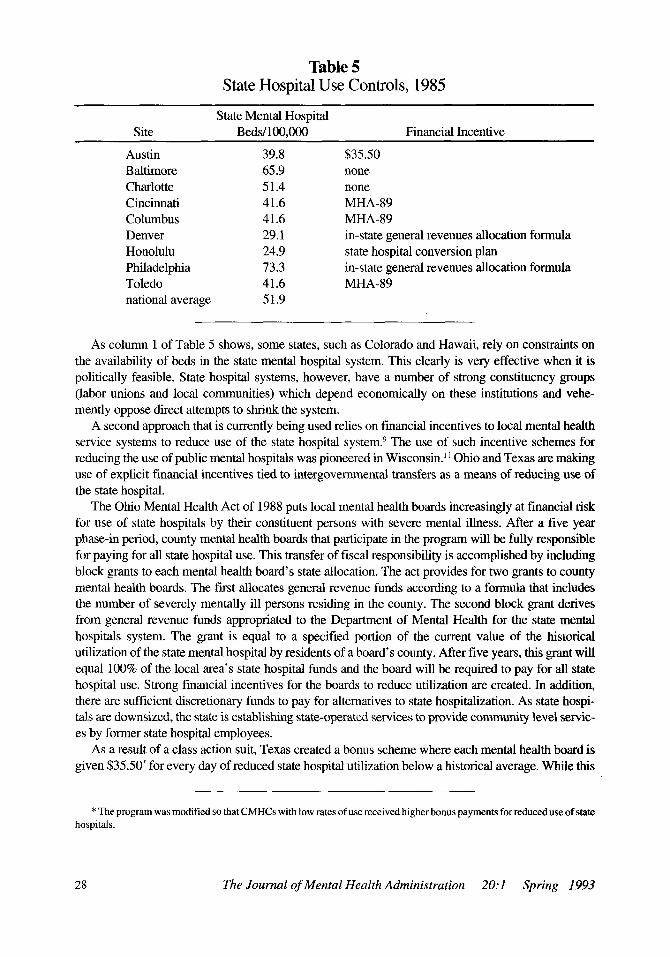
Table 5 State Hospital Use Controls, 1985
State Mental Hospital Site Beds/100,000 Financial Incentive
Austin 39.8 $35.50 Baltimore 65.9 none Charlotte 51.4 none Cincinnati 41.6 MHA-89 Columbus 41.6 MHA-89 Denver 29.1 in-state general revenues allocation formula Honolulu 24.9 state hospital conversion plan Philadelphia 73.3 in-state general revenues allocation formula Toledo 41.6 MHA-89 national average 51.9
As column 1 of Table 5 shows, some states, such as Colorado and Hawaii, rely on constraints on the availability of beds in the state mental hospital system. This clearly is very effective when it is politically feasible. State hospital systems, however, have a number of strong constituency groups (labor unions and local communities) which depend economically on these institutions and vehe- mently oppose direct attempts to shrink the system.
A second approach that is currently being used relies on financial incentives to local mental health service systems to reduce use of the state hospital system. 9 The use of such incentive schemes for reducing the use of public mental hospitals was pioneered in Wisconsin. 1~ Ohio and Texas are making use of explicit financial incentives tied to intergovernmental transfers as a means of reducing use of the state hospital.
The Ohio Mental Health Act of 1988 puts local mental health boards increasingly at financial risk for use of state hospitals by their constituent persons with severe mental illness. After a five year phase-in period, county mental health boards that participate in the program will be fully responsible for paying for all state hospital use. This transfer of fiscal responsibility is accomplished by including block grants to each mental health board's state allocation. The act provides for two grants to county mental health boards. The first allocates general revenue funds according to a formula that includes the number of severely mentally ill persons residing in the county. The second block grant derives from general revenue funds appropriated to the Department of Mental Health for the state mental hospitals system. The grant is equal to a specified portion of the current value of the historical utilization of the state mental hospital by residents of a board's county. After five years, this grant will equal 100% of the local area's state hospital funds and the board will be required to pay for all state hospital use. Strong financial incentives for the boards to reduce utilization are created. In addition, there are sufficient discretionary funds to pay for alternatives to state hospitalization. As state hospi- tals are downsized, the state is establishing state-operated services to provide community level servic- es by former state hospital employees.
As a result of a class action suit, Texas created a bonus scheme where each mental health board is given $35.50* for every day of reduced state hospital utilization below a historical average. While this
* The program was modified so that CMHCs with low rates of use received higher bonus payments for reduced use of state hospitals.
28 The Journal of Mental Health Administration 20:1 Spring 1993

Table 6 State Hospital Utilization
Statewide Avg. Site-Specific Site CMI Served* Hospitalization, 1985 Hospitalization, 1988
Austin** 3,457 145.2 170.6 Baltimore*** 4,543 174.5 307.70 Charlotte 1,210 152.3 81.1 Cincinnati 7,465 137.9 172.7 Columbus 5,182 137.9 81.2 Denver 2,531 83.8 5.9 Honolulu 1,302 64.8 73.9 Philadelphia* * 14,646 58.9 313.2 Toledo 2,353 137.9 111.3
* Number of CMI served from RWJ quarterly reports for 1988. ** Local area state hospital admissions are from the RWJ quarterly report summary for 1988. *** State hospital admissions for Baltimore are for 1989 and include children.
system encourages reduced use of state mental hospitals, it relies on a relatively small carrot ($35.50) and no stick. Other states employ methods which take into account state hospital utilization in rather complicated funding formulas. The incentives to reduce use in these schemes tend to be quite small (e.g., Colorado and Pennsylvania).
A comparison of the information displayed in columns 1 and 2 of Table 5 reveals additional patterns. Three states with the largest number of beds - - Maryland, North Carolina and Pennsylvania - - have adopted neither strong bed constraints nor any incentive scheme for controlling the use of the public mental hospital system. One of these, Pennsylvania, also has the highest per capita expendi- tures for mental health services among the seven states represented in the Demonstration.
Table 6 shows the rates of state hospital utilization in each of the nine demonstration cities. The first column provides background, indicating the approximate size of the chronically mentally ill population served by the state hospital system in each area. The second column describes the state- wide average rate of hospitalization to state mental hospitals for each state which has an RWJ site. The last column indicates the specific hospitalization rate for each RWJ-PCMI site in 1988. The utilization data suggest that in the early stages of the demonstration only the bed availability con- straint appears to be effective. However, these 1988 data do not reflect the impact of the Ohio Mental Health Act of 1988. Therefore, we expect to see stronger incentive effects in later stages of the demonstration for the Ohio sites.
Conclusion The information collected to date reveals a mixed picture of the effects that the economic incen-
tives of each financing strategy have on local area provision of mental health services. As indicated, the RWJ-PCMI program implements a set of financial smactures that may strongly affect how local mental health authorities control resources for mental health care. The economic incentives of the Medicaid program and other funding programs can impede or promote programmatic flexibility in adopting treatment technologies that have been shown, under experimental conditions, to be success- ful in treating the severely mentally ill in the community.
Economic Incentives in RWJ-PCMI FRANK, JACKSON, LYNCH 29
The RWJ-PCMI demonstration was designed to effect changes at the local level. However, as this paper indicates, state policies have as much, or more, influence on the type and mix of mental health care provided locally as do local policies. It appears to be extremely difficult to simultaneously get (a) a strong commitment of resources from both state and local government, (b) flexibility in use of state funds by local mental health authorities, (c) state government to adopt policies that limit use of state hospitals in order to shift dollars to community programs, and (d) states to adopt mental health benefits under Medicaid that enable innovative programs to be financed with these leveraged state dollars.
The evidence from the RWJ-PCMI demonstration indicates that the intergovernmental financial relationship between state government and local mental health authorities is critical to any local structural innovation. The RWJ-PCMI demonstration is as much a study of seven states as of nine cities. Any efforts to improve local mental health services must necessarily additionally focus on state policies if effective changes are to be made.
Acknowledgment We acknowledge Howard H. Goldman, M.D., Ph.D., as the principal investigator. Coinvestigators
at the University of Maryland include Anthony F. Lehman, M.D., M.S.P.H., Catherine A. Jackson, Ph.D., and Susan Ridgely, M.S.W.
Collaborating sites and coinvestigators include University of North Carolina at Chapel Hill, Center for Health Services Research (Joseph P. Morrissey, Ph.D.); Johns Hopkins University, Institute for Policy Studies (Sandra J. Newman, Ph.D.); and Johns Hopkins University, School of Hygiene and Public Health, Health Services Research and Development Center (Richard G. Frank, Ph.D., Donald M. Steinwachs, Ph.D., and E. Ann Skinner, M.S.W.).
Funding collaborators include Ohio Department of Mental Health (Dee Roth, M.A.), National Institute of Mental Health (Cille Kennedy, Ph.D. and Thomas Plant, Ph.D.), and the Robert Wood Johnson Foundation (Marjorie Guttman, Ph.D. and Joel Cantor, Ph.D.). We are grateful to Martin Cohen, Dee Roth, Tom Plant and three referees for helpful comments on earlier drafts of this paper.
References 1. Mechanic D, Aiken LH: Improving the care of patients with chronic mental illness. New England Journal
of Medicine 1987; 317(26): 1634-1638. 2. Stein L1, Test MA: Alternatives to Mental Hospital Treatment. New York: Plenum Press, 1978. 3. Weisbrod BA: A guide to benefit-cost analysis as seen through a controlled experiment in treating the
mentally ill. Journal of Health Politics, Policy and Law 1983; 7(4):808-845. 4. Mechanic D: Correcting misconceptions in mental health policy: strategies for improved care of the
seriously mentally ill. Milbank Quarterly 1987; 65:203-230. 5. Surles RC, McGurrin MC: Increased use of psychiatric emergency services by young chronically mentally
ill patients. Hospital and Community Psychiatry 1987; 38:401-405. 6. Aiken LH, Somers SA, Shore MF: Private foundations in health affairs: a case study of the development of
a national initiative for the chronically mentally ill. American Psychologist 1986; 41:1290-1295. 7. Taube CA, Goldman HH, Salkever D: Medicaid coverage for mental illness. Health Affairs 1990; 9(1) 5-
18. 8. Taube CA, Goldman HH: State strategies to restructm'e psychiatric hospitals. Inquiry 1989; 26(2):146-
156. 9. Frank RG, Gaynor M: Incentives, Optimality and Publicly Provided Goods: The Case of Mental Health
Services. Working Paper, Interdepartment Program in Public Health Economics, Johns Hopkins Universi- ty, July 1990.
30 The Journal of Mental Health Administration 20:1 Spring 1993

10. Goldman HH, Morrissey JP, Ridgely MS: Form and function of mental health authorities at RWJ Foun- dation program sites: preliminary observations. Hospital and Community Psychiatry 1990; 41(11):1222- 1230.
11. Stein LI, Ganser LJ: Wisconsin's system for funding mental health services. In Talbott J (ed.): Unified Mental Health Services. San Francisco: Jossey Bass, 1983.
Economic Incentives in RWJ-PCMI FRANK, JACKSON, LYNCH 31