Embed Size (px)
Citation preview
The Spine
Chapter 20Pages 488-515
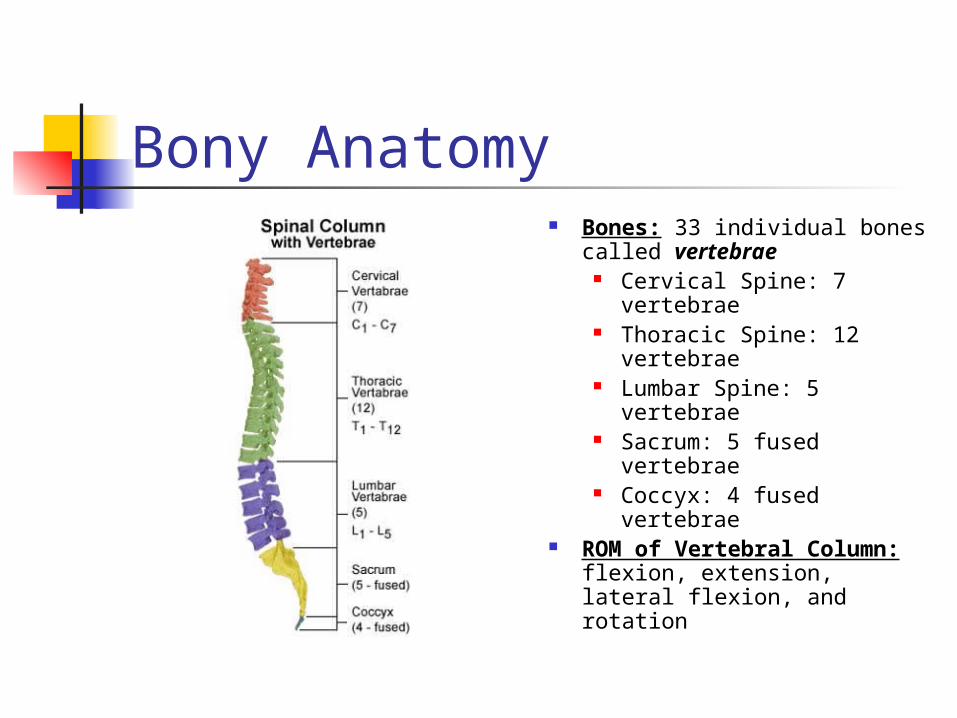
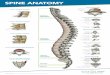
Bony Anatomy Bones: 33 individual bones
called vertebrae Cervical Spine: 7
vertebrae Thoracic Spine: 12
vertebrae Lumbar Spine: 5
vertebrae Sacrum: 5 fused
vertebrae Coccyx: 4 fused
vertebrae ROM of Vertebral
Column: flexion, extension, lateral flexion, and rotation
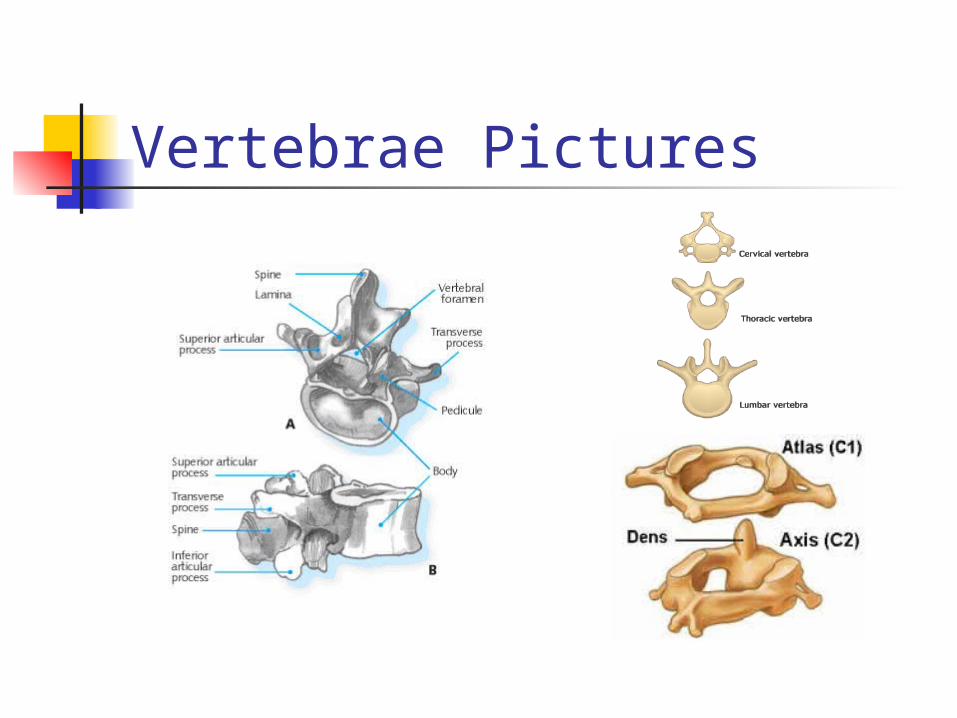
Vertebrae Pictures
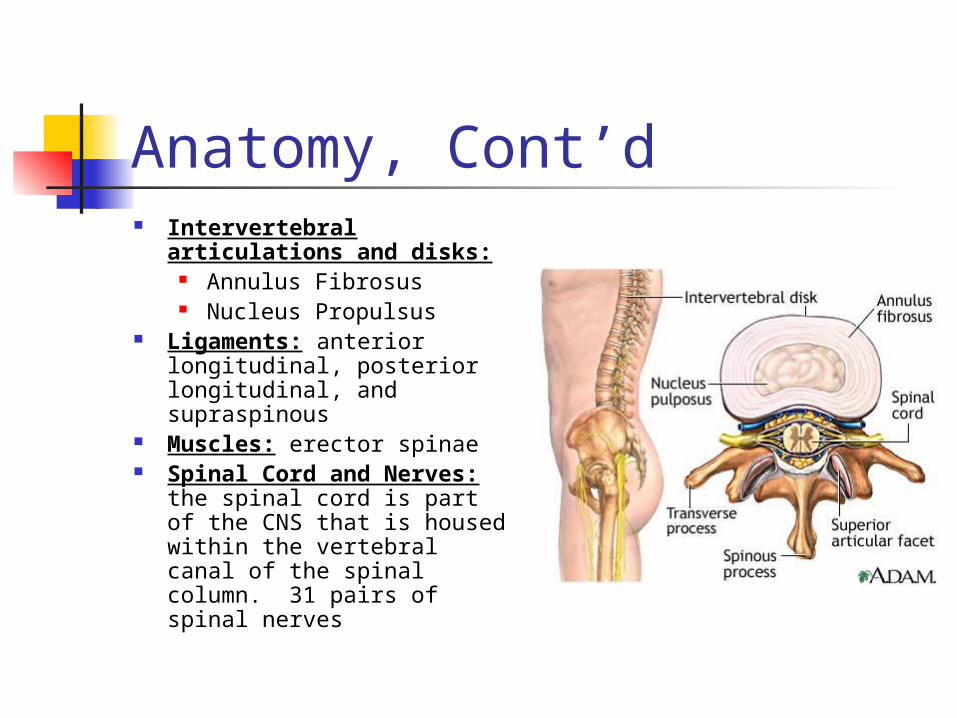
Anatomy, Cont’d Intervertebral
articulations and disks: Annulus Fibrosus Nucleus Propulsus
Ligaments: anterior longitudinal, posterior longitudinal, and supraspinous
Muscles: erector spinae Spinal Cord and Nerves:
the spinal cord is part of the CNS that is housed within the vertebral canal of the spinal column. 31 pairs of spinal nerves
Prevention of Injuries to the Spine Cervical spine
Strength Flexibility Using proper technique
Lumbar spine Strength and flexibility Using proper technique
Assessment: HHistory What do you think happened? Did you hit someone or land directly on top of
your head? Where you knocked unconscious? Do you have any pain in your neck? Do you have any tingling, numbness, or
burning in your shoulders, arms, or hands? Do you have equal muscle strength in both
hands? Are you able to move your ankles and toes? Any bowel or bladder changes?
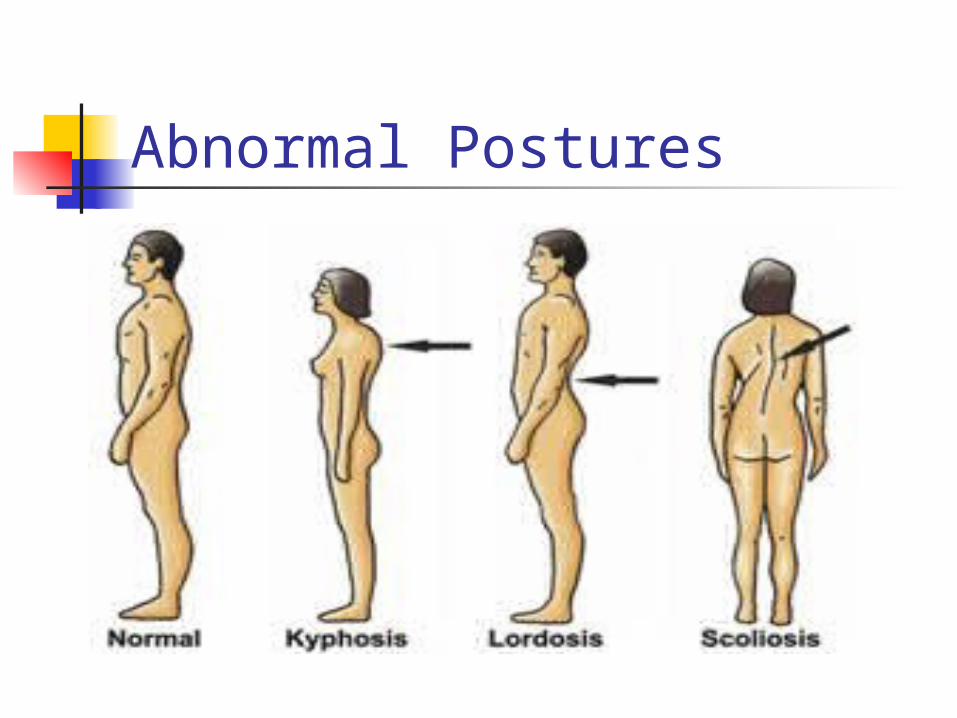
Abnormal Postures
Assessment: OObservation Does posture show signs of kyphosis, lordosis, or
scoliosis? Is the athlete willing to move the head and neck freely? Are the shoulders level and symmetrical? Is the head tilted to one side?
Is the scapula lower or more prominent than the other? Is the trunk bent or curved to one side? Is the space between the body and arm greater on one
side? Is one hip tilted? More prominent? Are the ribs more pronounced on one side? Does one arm hang lower? Forward? Is one patella lower than the other?

Assessment: PPalpation and SSpecial Tests Palpation
Athlete should be lying prone (on stomach) Bony palpation: spinous/transverse
processes, sacrum, and coccyx. Soft tissue palpation: musculature on each
side of the spine for spasm and guarding. Special Tests
Straight leg raises Compression and distraction tests
Recognition and Management of Injuries to the Cervical Spine Cervical Fractures Cervical Dislocations Acute Muscle Strains
of the Neck and Upper Back
Cervical Sprain (Whiplash)
Acute Torticollis (Wryneck)
Pinched Nerve (Brachial Plexus Injury)
Cervical Fractures MOI:
Axial loading is a blow to the top of the athlete’s head while in flexion.
S&S: Neck point tenderness, restricted movement,
cervical muscle spasm, cervical pain, pain in the chest, and extremities, numbness in the trunk/limbs, weakness/paralysis in the trunk/limbs, loss of bowel/bladder control.
Treatment: Do not move the athlete. Activate EMS. Stabilize
head and neck.
Cervical Dislocations MOI:
A result of violent flexion and rotation of the head.
S&S: Similar to cervical fracture. A unilateral dislocation causes the neck to be
tilted toward the dislocated side. Treatment:
Do not move the athlete. Activate EMS. Stabilize head and neck.
Acute Muscle Strains of the Neck and Upper Back MOI:
Forced flexion, extension, and/or rotation of the head suddenly.
Muscles: upper trapezius, SCM, scalenes, splenus capitus and cervicis.
S&S: Localized pain, point tenderness, restricted ROM,
muscle guarding. Treatment:
RICE, cervical collar, ROM, isometric exercises, isotonic exercises, and modalities for pain control.
Whiplash
Pinched Nerve MOI:
Stretching or compression of the brachial plexus. The neck is forced laterally to the opposite side while the shoulder is depressed.
S&S: Burning sensation, numbness, tingling, pain from
shoulder to the hand, loss of function of the arm and hand.
Treatment: Once the symptoms have completely resolved and
there are no neurological symptoms, the athlete may return to participation.
Strengthening and stretching of neck muscles.
Recognition and Management of Injuries to the Lumbar Spine Low Back Pain (LBP) Lumbar Vertebrae Fracture and Dislocation Low Back Muscle Strains Lumbar Sprains Back Contusions Sciatica Herniated Lumbar Disk Spondylolysis and Spondylolisthesis
Low Back Pain MOI:
Congenital anomalies and/or mechanical back defects (faulty posture, trauma to the back).
S&S: Muscular weakness, impairment of
sensation and reflex responses. Prevention:
Avoid unnecessary stresses and strains associated with standing, sitting, lying, working, or exercising.
Lumbar Vertebrae Fracture and Dislocation MOI:
Compression fractures usually occur from falling from a height and landing on the feet/buttocks, a kick and/or direct impact to the back.
S&S: May be palpable over spinous and transverse
processes, point tenderness, swelling, and muscle guarding in the area.
Treatment: Spine board the athlete and refer to physician.
Low Back Muscle Strains MOI:
Sudden extension in combination with trunk rotation and chronic strain because of faulty posture.
S&S: Pain may be diffused or in one area. Pain
with active extension and passive flexion. Treatment:
Ice, abdominal support, graduated program of stretching and strengthening .
Lumbar Sprains MOI:
Bending forward and twisting while lifting an object. S&S:
Localized pain that is lateral to the spinous process, pain becomes sharp with certain movements/postures, flexion/extension/rotational movements of the vertebrae increase pain.
Treatment: RICE, strengthening for back extensors and
abdominals, and stretching in all directions. May take some time to heal.
Back Contusions MOI:
Direct trauma. Be wary of the kidneys.
S&S: Local pain, muscle spasm, and point
tenderness, swelling, and discoloration. Treatment:
Ice for 72 hours, rest, gradual stretching. Recovery ranges from 2 days to 2 weeks.
Sciatica MOI:
Sciatica is an inflammatory condition of the sciatic nerve that can accompany recurrent/chronic LBP.
S&S: Onset may be sudden or gradual, a sharp/shooting
pain that follows the nerve pathway along posterior and medial thigh, tingling and numbness along the nerve pathway, sensitive to palpation, and pain with straight leg raises.
Treatment: Rest, identify cause of inflammation, NSAIDS,
sometimes surgery may be indicated.
Herniated Lumbar Disk MOI:
Forward bending and twisting that places abnormal strain on the lumbar region.
S&S: Centrally located pain that radiates on one side of the
buttocks and down the back of the leg or pain that spreads across the back, symptoms are worse in the morning, onset may be sudden or gradual, posture is bent forward and away from the side of pain, and pain with straight leg raises.
Treatment: Rest and ice, back extensor and abdominal
stabilization exercises, sometimes surgery is necessary.
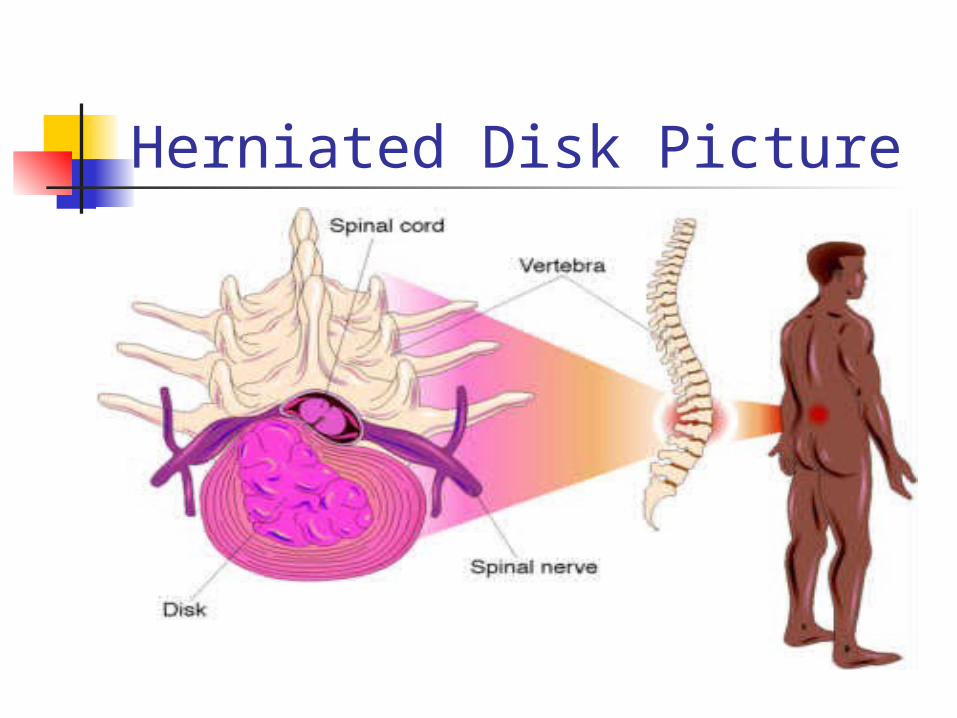
Herniated Disk Picture
Visual Aids Courtesy of the Following Websites: http://www.sci-recovery.org/sci.htm http://www.nationalpainfoundation.org/MyTreatment/
articles/BackAndNeck_Part_2.asp http://www.getbodysmart.com/ap/skeletalsystem/
skeleton/axial/vertebrae/menu/animation.html http://www.spineuniverse.com/displayarticle.php/
article2245.html http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/19469.jpg
http://lc3.littlechute.k12.wi.us/staff/hthomas1/Anatomy%20and%20Physiology/Notes/Skeletal%20System_files/image007.jpg
http://www.healthatoz.com/healthatoz/Atoz/images/ency/00042710.jpg