Embed Size (px)
Citation preview

The Sella and
Parasellar Region
John R. Hesselink, M.D.
Department of Radiology
University of California
San Diego

Adenohypophysis
Hormones: Prolactin, Gonadotropin
Somatotropin (growth hormone)
Adrenocorticotropin (ACTH)
Thyroid stimulating hormone (TSH)
Follicle stimulating hormone (FSH)
Luteinizing hormone (LH)
Hypothalamus produces releasing factors
Portal-hypophysial system between
median eminence and anterior lobe
Anatomy & Function

Pituitary
Gland
Neurohypophysis
Hormones:
Vasopressin (ADH) & Oxytocin
Produced in supraoptic
& paraventricular nuclei
Transported via axonal flow
Stored in neurosecretory granules
Anatomy & Function

Pituitary Gland
Posterior Lobe
The Normal Pituitary Gland
Gland height 8 mm
Size normally increases in adolescent
females & during pregnancy
Gland parenchyma relatively homogeneous
Signal intensity on T1W images
Anterior lobe = isointense
Posterior lobe = hyperintense
Gland, stalk & median eminence enhance
<

Normal
Pituitary
Gland
Coronal
Plane

Normal Pituitary Gland
Sagittal Plane - Gadolinium

Normal Newborn Pituitary Gland
71

Pituitary Gland
T1W SE coronal Gadolinium injection
T1W SE coronal T1W SE sagittal
Pulse Sequences
Note: Use overlapped 3 mm sections, 512/256 matrix,
18 cm FOV, 2/4 NEX. Include T2W FSE for hypothalamic
lesions. For post-op sella, use fat suppression with Gd.

Pituitary Pathology
Abnormalities of size or position
Pituitary adenoma
Other rare tumors
Diabetes insipidus
Lymphocytic hypophysitis

Pituitary Gland
Benign pituitary hyperplasia
Pituitary hypoplasia
The empty sella
Ectopic pituitary
Sheehan's syndrome
Abnormalities of Size & Position

Intrasellar Position
of the Carotid Artery
L 15

History: 26 y.o. female presents with small
stature and panhypopituitarism
140

Dx: Small gland,
absent stalk &
ectopic bright spot
{Page 2}

395
Partially
Empty Sella

Ectopic Posterior Pituitary
L 4

Sheehan’s Syndrome

Pituitary Adenoma
Arise within the adenohypophysis
Nonsecreting adenomas cause mass effect
Bitemporal hemianopsia
Secreting adenomas cause endocrine syndrome
Prolactinemia
Acromegaly, Giantism
Cushing's disease
Hyperprolactinemia
Physiologic Pregnancy
Nursing
Nipple
stimulation
Sexual
intercourse
Exercise
Sleep
Stress
Pathologic
Prolactinoma
Hypothalamic
tumors
Chronic renal
failure
Cirrhosis
Intercostal nerve
stimulation
Pharmacologic
Hypoglycemia
Hyperaminoacidemia
Hormone: estrogen, TRH
Dopaminergic Antagonists
Catecholamine
inhibitors/depleters
Serotonin precursors
GABA agonists
Histamine H2 antagonists
Opiates

Microadenoma

History: 26 y.o. female with headaches
and blurred vision
83
1 2

Dx: Microadenoma
{Page 2}
6
5
4
3

Dx: Prolactinoma
History: 45 y/o woman with
headaches & elevated prolactin
671

Dx: Pituitary hyperplasia
History: 38 y/o female
with anemia, hypothyroid,
increased TSH & prolactin
382

Cushing's Disease
L 33-5
ACTH Levels
Right petrosal vein = 34 ppm
Left petrosal vein = 866 ppm

History: 50 y/o woman
with headaches & visual changes
367

Dx: Pituitary macroadenoma
{Page 2}

Dx: Pituitary apoplexy
History: 24 y/o female
with a visual deficit
554

History: 35 y/o female with visual
loss & ophthalmoplegia
514

Dx: Prolactin = 7000
{Page 2}

Choristoma Myoblastoma, Granular cell tumor, Pituicytoma

163
History: 35 y/o
HIV+ male with
severe anemia

Dx: Meningioma
Anemia {Page 2}

Lymphocytic Hypophysitis
L 10-11

Dx: Brucellosis
pituitary abscess
History: 47 y.o. woman with
headache, fever & vomiting.
12
Suprasellar Pathology
Craniopharyngioma, Rathke's cleft cyst
Chiasmatic & hypothalamic gliomas
Hamartoma, Germinoma
Lymphoma
Arachnoid cyst, Epidermoid, Dermoid
Granulomatous disease

Perisellar Anatomy
A - Pituitary gland
B - Optic chiasm
C - Supraclinoid
carotid artery
D - 3rd nerve
E - Intracavernous
carotid artery
F - Ophthalmic nerve
G - Cavernous sinus
H - Sphenoid sinus

Craniopharyngioma
Arise from epithelial remnants
of Rathke's pouch
Suprasellar location
Benign but produce mass effect
Cysts & calcification common
Nodular enhancement

History: 74 y/o woman with frontal
headaches & light sensitivity
731
Dx: Papillary craniopharyngioma
{Page 2}

History: 53 y/o man with bitemporal hemianopia
271

{Page 2}
Dx: Craniopharyngioma

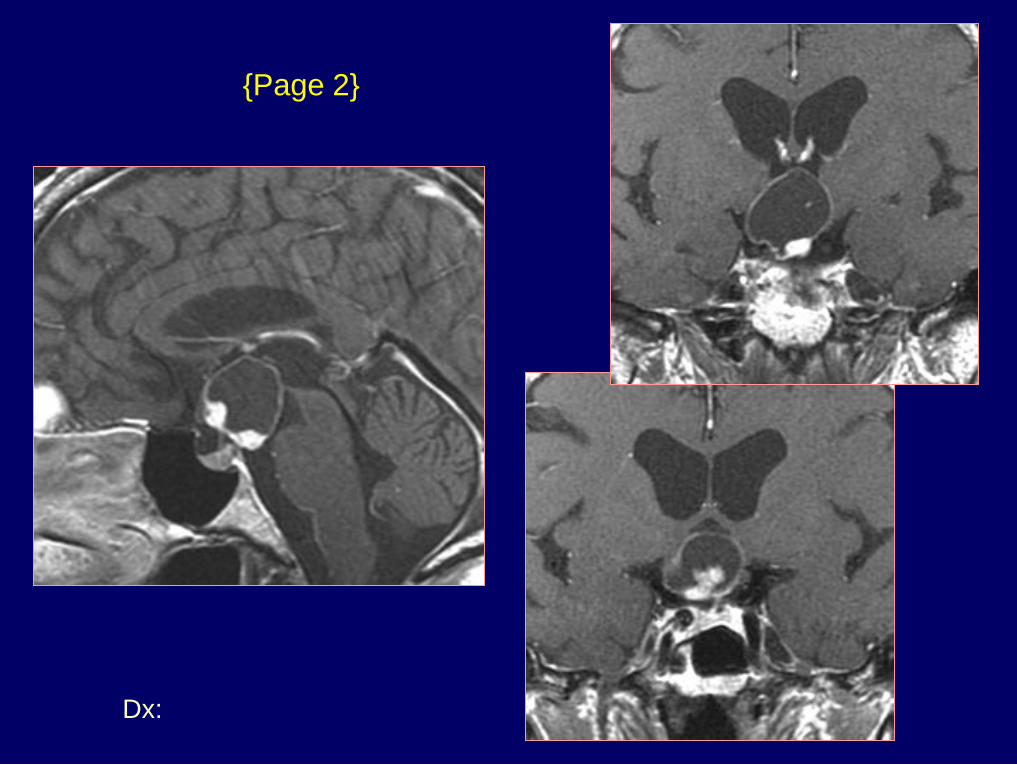
History: 63 y/o man with
hyponatremia & hypopituitarism
393

{Page 2}
Dx: Rathke's cleft cyst

Hypothalamic Glioma
F 74-6

Central Diabetes Insipidus
Trauma or surgery - 50% of cases
Idiopathic - 25% of cases
Craniopharyngioma
Hypothalamic glioma
Germinoma
Granulomatous disease
Etiology

Dx: Diabetes insipidus –
idiopathic vs lymphocytic
hypophysitis
History: 20 y/o male with polyuria
& polydypsia for 2 weeks
745 - 22855969

History: 23 y/o male
with epilepsy
571

Dx: Hamartoma – tuber cinereum
{Page 2}

Suprasellar Arachnoid Cyst
F 93-5

EL-7342
History: 57 y.o. man with blurred vision

Dx: Epidermoid cyst
{Page 2}
FS
FS

Suprasellar Pathology
Langerhan's cell histiocytosis
Sarcoidosis
Tuberculosis
Fungal infections
Granulomatous Disease

History: 54 y.o. man with headaches for 2
months & decreased mental status

{Page 2}

History: 44 y/o man
with chronic headaches

{Page 2}

Cavernous Sinus
& Parasellar Pathology
Meningioma
Nerve sheath tumors
Skull base tumors
Vascular lesions
Inflammatory disease

165
History: 83 y/o man
with decreasing vision
in the left eye

Dx: Cavernous sinus
meningioma
Decreasing vision
{Page 2}

History: 38 y/o male with
right facial numbness
657 - Telerad

Dx: Schwannoma
{Page 2}

History: 9 y.o. girl
with multiple bilateral
cranial nerve palsies

History: 35 y/o woman with right eye
pain and amenorrhea
370

{Page 2}

Eye pain
{Page 3}
Dx: Chondrosarcoma

History: 31 y/o female with recurrent
otitis, headache, and diplopia
694

Dx: Chordoma
{Page 2}
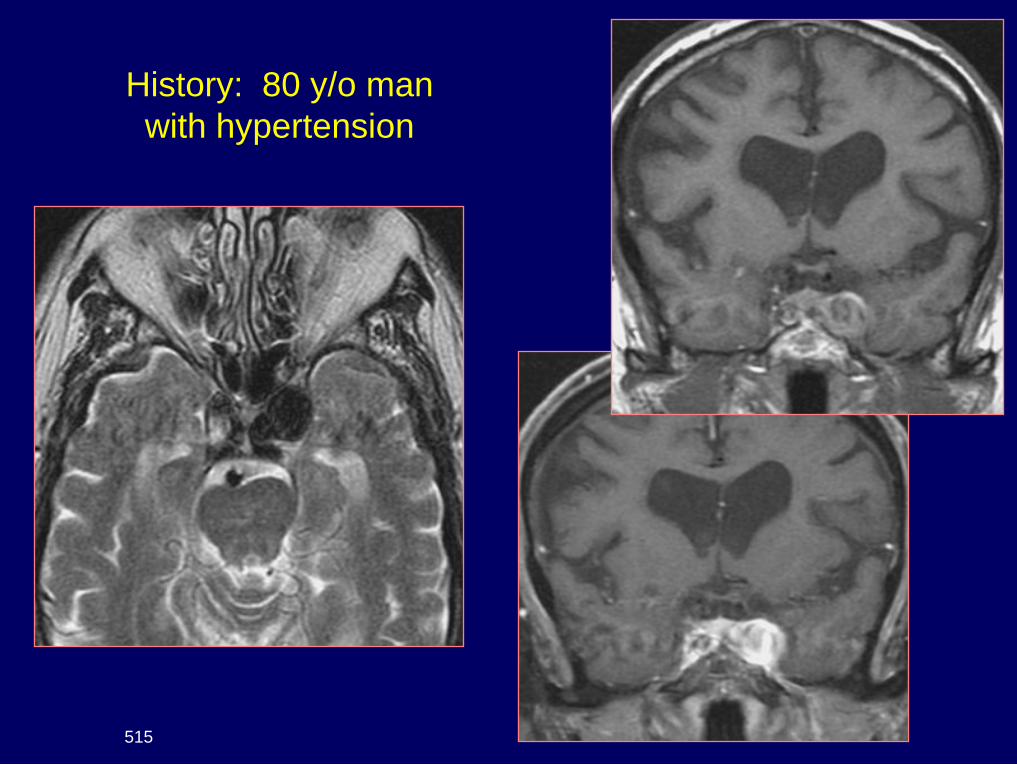
History: 80 y/o man
with hypertension
515

Dx: Cavernous aneurysm
{Page 2}

History: 46 y.o. man with a left 3rd nerve palsy
15

Dx: Septic thrombosis
of the left
cavernous sinus
{Page 2}