Embed Size (px)
Citation preview


The Science and Medicine of The Science and Medicine of Thrombosis in CancerThrombosis in Cancer
The Evolving and Foundation Role of LMWHs in Cancer and The Evolving and Foundation Role of LMWHs in Cancer and Thrombosis: Applying Science, Expert Analysis, and Thrombosis: Applying Science, Expert Analysis, and
Landmark Trials to the Front Lines of Specialty PracticeLandmark Trials to the Front Lines of Specialty Practice
Program ChairmanProgram ChairmanCraig M. Kessler, MDCraig M. Kessler, MD
Professor of Medicine and PathologyProfessor of Medicine and PathologyGeorgetown University Medical CenterGeorgetown University Medical CenterDirector of the Division of CoagulationDirector of the Division of Coagulation
Department of Laboratory MedicineDepartment of Laboratory MedicineLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Washington, DCWashington, DC
Mechanisms ● Mortality ● TherapeuticsMechanisms ● Mortality ● Therapeutics

Welcome and Program OverviewWelcome and Program Overview
CME-accredited symposium CME-accredited symposium jointly sponsored by the University of jointly sponsored by the University of Massachusetts Medical Center, office of CME and CMEducation Massachusetts Medical Center, office of CME and CMEducation Resources, LLCResources, LLC
Mission statement: Mission statement: Improve patient care through evidence-based Improve patient care through evidence-based education, expert analysis, and case study-based managementeducation, expert analysis, and case study-based management
Processes: Processes: Strives for fair balance, clinical relevance, on-label Strives for fair balance, clinical relevance, on-label indications for agents discussed, and emerging evidence and indications for agents discussed, and emerging evidence and information from recent studiesinformation from recent studies
COI: COI: Full faculty disclosures provided in syllabus and at the Full faculty disclosures provided in syllabus and at the beginning of the programbeginning of the program

Program Educational ObjectivesProgram Educational Objectives
As a result of this session, participants will:As a result of this session, participants will: ► Learn about recent trials, research, and expert analysis of issues Learn about recent trials, research, and expert analysis of issues
focused on thrombosis and cancer.focused on thrombosis and cancer.
► Learn about mechanisms, morbidity, mortality, and therapeutic issues Learn about mechanisms, morbidity, mortality, and therapeutic issues focused on thrombosis and cancer.focused on thrombosis and cancer.
► Learn about relationships among the clotting cascade, agents Learn about relationships among the clotting cascade, agents affecting the coagulation system, and mortality outcomes in cancer affecting the coagulation system, and mortality outcomes in cancer patients.patients.
► Learn about strategies for risk-directed prophylaxis against VTE in at Learn about strategies for risk-directed prophylaxis against VTE in at risk patients with cancer. risk patients with cancer.
► Learn how to assess and manage special needs of cancer patients Learn how to assess and manage special needs of cancer patients at-risk for VTE, with a focus on protecting against recurrent DVTat-risk for VTE, with a focus on protecting against recurrent DVT..

Program FacultyProgram Faculty
Craig M. Kessler, MD—Program ChairmanCraig M. Kessler, MD—Program ChairmanProfessor of Medicine and PathologyProfessor of Medicine and PathologyGeorgetown University Medical CenterGeorgetown University Medical CenterLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer CenterChief, Division of CoagulationChief, Division of CoagulationWashington, DCWashington, DC
Frederick R. Rickles, MD, FACP Frederick R. Rickles, MD, FACP Center for Health InnovationCenter for Health InnovationPublic Sector Healthcare, NoblisPublic Sector Healthcare, NoblisProfessor of Medicine, Pediatrics and Pharmacology and Physiology Professor of Medicine, Pediatrics and Pharmacology and Physiology The George Washington UniversityThe George Washington UniversityWashington, DCWashington, DC
Edith Nutescu, Pharm.D., FCCP Edith Nutescu, Pharm.D., FCCP Clinical Associate Professor, Pharmacy Practice Clinical Associate Professor, Pharmacy Practice Affiliate Faculty, Center for Pharmacoeconomic Research Affiliate Faculty, Center for Pharmacoeconomic Research Director, Antithrombosis Center Director, Antithrombosis Center The University of Illinois at Chicago The University of Illinois at Chicago College of Pharmacy & Medical Center College of Pharmacy & Medical Center Chicago, Illinois Chicago, Illinois

Faculty COI Financial DisclosuresFaculty COI Financial Disclosures
Craig M. Kessler, MD - Co-ChairmanCraig M. Kessler, MD - Co-ChairmanGrant/Research Support: Grant/Research Support: GlaxoSmithKlineGlaxoSmithKlineConsultant: Consultant: sanofi-aventis, Eisai Pharmaceuticalssanofi-aventis, Eisai PharmaceuticalsSpeaker’s Bureau: Speaker’s Bureau: sanofi-aventis, GlaxoSmithKlinesanofi-aventis, GlaxoSmithKline
Frederick R. Rickles, MDFrederick R. Rickles, MDConsultant: Consultant: Eisai Pharmaceuticals, Genmab, PharmacyclicsEisai Pharmaceuticals, Genmab, PharmacyclicsSpeaker’s Bureau: Speaker’s Bureau: Eisai PharmaceuticalsEisai Pharmaceuticals
Edith Nutescu, PharmDEdith Nutescu, PharmDSpeakers Bureau: Speakers Bureau: Eisai Inc., GlaxoSmithKline, sanofi-aventis U.S. Eisai Inc., GlaxoSmithKline, sanofi-aventis U.S. Advisory Committees or Review Panels, Board Membership, etc.: Advisory Committees or Review Panels, Board Membership, etc.: Boehringer Ingelheim Pharmaceuticals, Inc., Scios Inc. Boehringer Ingelheim Pharmaceuticals, Inc., Scios Inc.

Clotting, Cancer, and Controversies
What the Trials, Emerging Science, and Current Thinking Tell Us About The Evolving Science and Foundation Role of
Anticoagulation in the Setting of Cancer
Clotting, Cancer, and Controversies
What the Trials, Emerging Science, and Current Thinking Tell Us About The Evolving Science and Foundation Role of
Anticoagulation in the Setting of Cancer
Program ChairmanProgram ChairmanCraig Kessler, MD MACPCraig Kessler, MD MACP
Director, Division of CoagulationDirector, Division of CoagulationLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Georgetown University Medical CenterGeorgetown University Medical CenterWashington, DCWashington, DC
Program ChairmanProgram ChairmanCraig Kessler, MD MACPCraig Kessler, MD MACP
Director, Division of CoagulationDirector, Division of CoagulationLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Georgetown University Medical CenterGeorgetown University Medical CenterWashington, DCWashington, DC
Innovation ● Investigation ● ApplicationInnovation ● Investigation ● Application

VTE and Cancer—A Looming VTE and Cancer—A Looming National Healthcare CrisisNational Healthcare Crisis
MISSION AND CHALLENGESMISSION AND CHALLENGES
Recognizing cancer patients at risk for DVT Recognizing cancer patients at risk for DVT and identifying appropriate candidates for and identifying appropriate candidates for long-term prophylaxis and/or treatment with long-term prophylaxis and/or treatment with approved and indicated therapies are among approved and indicated therapies are among the most important challenges encountered in the most important challenges encountered in contemporary pharmacy and clinical practice.contemporary pharmacy and clinical practice.
MISSION AND CHALLENGESMISSION AND CHALLENGES
Recognizing cancer patients at risk for DVT Recognizing cancer patients at risk for DVT and identifying appropriate candidates for and identifying appropriate candidates for long-term prophylaxis and/or treatment with long-term prophylaxis and/or treatment with approved and indicated therapies are among approved and indicated therapies are among the most important challenges encountered in the most important challenges encountered in contemporary pharmacy and clinical practice.contemporary pharmacy and clinical practice.

COMORBIDITYCOMORBIDITYCONNECTIONCONNECTION
CAPCAPUTIUTICancerCancerHeart Failure Heart Failure ABE/COPDABE/COPDRespiratory FailureRespiratory Failure Myeloproliferative DisorderMyeloproliferative DisorderThrombophiliaThrombophiliaSurgerySurgeryHistory of DVTHistory of DVTOtherOther
COMORBIDITYCOMORBIDITYCONNECTIONCONNECTION
CAPCAPUTIUTICancerCancerHeart Failure Heart Failure ABE/COPDABE/COPDRespiratory FailureRespiratory Failure Myeloproliferative DisorderMyeloproliferative DisorderThrombophiliaThrombophiliaSurgerySurgeryHistory of DVTHistory of DVTOtherOther
SUBSPECIALISTSUBSPECIALISTSTAKEHOLDERSSTAKEHOLDERS
Infectious diseasesInfectious diseasesOncologyOncologyPHARMACISTSPHARMACISTSCardiology Cardiology Pulmonary medicinePulmonary medicineHematologyHematologyOncology/hematologyOncology/hematologyInterventional RadiologyInterventional RadiologyHospitalistHospitalistSurgeonsSurgeonsEMEMPCPPCP
SUBSPECIALISTSUBSPECIALISTSTAKEHOLDERSSTAKEHOLDERS
Infectious diseasesInfectious diseasesOncologyOncologyPHARMACISTSPHARMACISTSCardiology Cardiology Pulmonary medicinePulmonary medicineHematologyHematologyOncology/hematologyOncology/hematologyInterventional RadiologyInterventional RadiologyHospitalistHospitalistSurgeonsSurgeonsEMEMPCPPCP
Comorbidity ConnectionComorbidity Connection

Epidemiology of First-Time VTEEpidemiology of First-Time VTE
White R. White R. CirculationCirculation. 2003;107:I-4 –I-8.). 2003;107:I-4 –I-8.)
VariableVariable FindingFinding
Seasonal VariationSeasonal Variation Possibly more common in winter and less Possibly more common in winter and less common in summercommon in summer
Risk FactorsRisk Factors25% to 50% “idiopathic”25% to 50% “idiopathic”
15%-25% associated with cancer15%-25% associated with cancer20% following surgery (3 months)20% following surgery (3 months)
Recurrent VTERecurrent VTE
6-month incidence, 7%;6-month incidence, 7%;Higher rate in patients with cancerHigher rate in patients with cancer
Recurrent PE more likely after PE than Recurrent PE more likely after PE than after DVTafter DVT
Death After Treated VTEDeath After Treated VTE
30-day incidence 6% after incident DVT30-day incidence 6% after incident DVT30-day incidence 12% after PE30-day incidence 12% after PE
Death strongly associated with Death strongly associated with cancercancer, , age, and cardiovascular diseaseage, and cardiovascular disease

Epidemiology of VTEEpidemiology of VTE
White R. White R. CirculationCirculation. 2003;107:I-4–I-8.). 2003;107:I-4–I-8.)
► One major risk factor for VTE is One major risk factor for VTE is ethnicityethnicity, with a , with a significantly higher incidence among Caucasians significantly higher incidence among Caucasians and African Americans than among Hispanic and African Americans than among Hispanic persons and Asian-Pacific Islanders. persons and Asian-Pacific Islanders.
► Overall, about 25% to 50% of patient with first-Overall, about 25% to 50% of patient with first-time VTE have an time VTE have an idiopathic conditionidiopathic condition, without a , without a readily identifiable risk factor. readily identifiable risk factor.
► Early mortality after VTE is strongly associated Early mortality after VTE is strongly associated with presentation as PE, advanced agewith presentation as PE, advanced age, , cancer,cancer, and underlying cardiovascular disease. and underlying cardiovascular disease.
► One major risk factor for VTE is One major risk factor for VTE is ethnicityethnicity, with a , with a significantly higher incidence among Caucasians significantly higher incidence among Caucasians and African Americans than among Hispanic and African Americans than among Hispanic persons and Asian-Pacific Islanders. persons and Asian-Pacific Islanders.
► Overall, about 25% to 50% of patient with first-Overall, about 25% to 50% of patient with first-time VTE have an time VTE have an idiopathic conditionidiopathic condition, without a , without a readily identifiable risk factor. readily identifiable risk factor.
► Early mortality after VTE is strongly associated Early mortality after VTE is strongly associated with presentation as PE, advanced agewith presentation as PE, advanced age, , cancer,cancer, and underlying cardiovascular disease. and underlying cardiovascular disease.

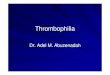
Thrombophilia Enhances Risks of Thrombophilia Enhances Risks of Thrombosis in Cancer PatientsThrombosis in Cancer Patients
H. Decousus et al. Thrombosis Research 120 Suppl. 2 (2007) S51-S61H. Decousus et al. Thrombosis Research 120 Suppl. 2 (2007) S51-S61
Risk of thrombosis in cancer patients within the previous five years according Risk of thrombosis in cancer patients within the previous five years according to the presence of factor V Leiden or G20210A prothrombin gene mutationto the presence of factor V Leiden or G20210A prothrombin gene mutation
MutationMutation CancerCancer
Patients with Patients with first venous first venous thrombosis thrombosis
(n=2706)(n=2706)
Control without Control without venous venous
thrombosis thrombosis (n=1757)(n=1757)
Age- and sex-Age- and sex-adjusted odds adjusted odds ratio (95% CI)ratio (95% CI)
Factor V LeidenFactor V Leiden
NoNoYesYes 21252125 16351635 1.001.00
YesYes 162162 2626 5.1 (3.3-7.7)5.1 (3.3-7.7)
YesYesNoNo 403403 9595 3.3 (2.6-4.1)3.3 (2.6-4.1)
YesYes 1616 11 12.1 (1.6-88.1)12.1 (1.6-88.1)
Prothombin 20210AProthombin 20210A
NoNoNoNo 24102410 16931693 1.001.00
YesYes 164164 2727 4.5 (3.0-6.8)4.5 (3.0-6.8)
YesYesNoNo 118118 3636 2.3 (1.6-3.3)2.3 (1.6-3.3)
YesYes 1414 00 Not determinedNot determined

Acute Medical Illness and VTEAcute Medical Illness and VTE
Multivariate Logistic Regression ModelMultivariate Logistic Regression Modelfor Definite Venous Thromboembolism (VTE)for Definite Venous Thromboembolism (VTE)
Alikhan R, Cohen A, et al. Alikhan R, Cohen A, et al. Arch Intern MedArch Intern Med. 2004;164:963-968. 2004;164:963-968
Risk FactorRisk Factor Odds RatioOdds Ratio(95% CI)(95% CI)
XX22
Age > 75 yearsAge > 75 yearsCancerCancer
Previous VTEPrevious VTE
1.03 (1.00-1.06)1.03 (1.00-1.06)1.62 (0.93-2.75)1.62 (0.93-2.75)2.06 (1.10-3.69)2.06 (1.10-3.69)
0.00010.00010.080.080.020.02
Acute infectious Acute infectious diseasedisease
1.74 (1.12-2.75)1.74 (1.12-2.75) 0.020.02

VTE RecurrenceVTE Recurrence
Predictors of First VTE/ RecurrencePredictors of First VTE/ Recurrence
Heit J, Mohr D, et al. Heit J, Mohr D, et al. Arch Intern MedArch Intern Med. 2000;160:761-768. 2000;160:761-768
Baseline CharacteristicBaseline Characteristic Hazard RatioHazard Ratio(95% CI)(95% CI)
AgeAge 1.17 (1.11-1.24)1.17 (1.11-1.24)
Body Mass IndexBody Mass Index 1.24 (1.04-1.7)1.24 (1.04-1.7)
Neurologic disease Neurologic disease with extremity paresiswith extremity paresis
1.87 (1.28-2.73)1.87 (1.28-2.73)
Malignant neoplasmMalignant neoplasmWith chemotherapyWith chemotherapy
Without chemotherapyWithout chemotherapy4.24 (2.58-6.95)4.24 (2.58-6.95)2.21 (1.60-3.06)2.21 (1.60-3.06)

Progression of Chronic Venous InsufficiencyProgression of Chronic Venous Insufficiency
From UpToDate 2006From UpToDate 2006

Rising VTE Incidence in Hospitalized PatientsRising VTE Incidence in Hospitalized Patients
Stein PD et al. Am J Cardiol 2005; 95: 1525-1526Stein PD et al. Am J Cardiol 2005; 95: 1525-1526
22
1.51.5
11
0.50.5
00
79 81 83 85 87 89 91 93 95 97 9979 81 83 85 87 89 91 93 95 97 99
YearYear
VTEVTE
DVTDVT
PEPE
%%

DVT Registry (N=5,451)DVT Registry (N=5,451)Top 5 Medical ComorbiditiesTop 5 Medical Comorbidities
Am J Cardiol 2004; 93: 259-262Am J Cardiol 2004; 93: 259-262
1.1. HypertensionHypertension
2.2. ImmobilityImmobility
3.3. CancerCancer
4.4. Obesity (BMI > 30)Obesity (BMI > 30)
5.5. Cigarette SmokingCigarette Smoking

Implementation of Guidelines Implementation of Guidelines in Cancer Patientsin Cancer Patients
Implementation of VTE prophylaxis Implementation of VTE prophylaxis continues to be problematic, despite continues to be problematic, despite
detailed North American and European detailed North American and European Consensus guidelinesConsensus guidelines..

Symposium Themes—Cancer/DVTSymposium Themes—Cancer/DVT
1.1. Cancer rates are increasing as treatment for heart Cancer rates are increasing as treatment for heart disease and cancer improvedisease and cancer improve
2.2. Cancer increases VTE riskCancer increases VTE risk
3.3. VTE is preventable (immunize!)VTE is preventable (immunize!)
4.4. VTE prophylaxis may slow cancerVTE prophylaxis may slow cancer
5.5. Increased emphasis on prophylaxis: OSG, NCCN, Increased emphasis on prophylaxis: OSG, NCCN, ASCO, ACCP, NATFASCO, ACCP, NATF
6.6. Facilitate Facilitate prophylaxis with alertsprophylaxis with alerts

Cancer, Thrombosis, and the Cancer, Thrombosis, and the Biology of Malignancy Biology of Malignancy
Scientific Foundations for the Role ofScientific Foundations for the Role ofLow-Molecular-Weight Heparin in Cancer PatientsLow-Molecular-Weight Heparin in Cancer Patients
Cancer, Thrombosis, and the Cancer, Thrombosis, and the Biology of Malignancy Biology of Malignancy
Scientific Foundations for the Role ofScientific Foundations for the Role ofLow-Molecular-Weight Heparin in Cancer PatientsLow-Molecular-Weight Heparin in Cancer Patients
Frederick R. Rickles, MDFrederick R. Rickles, MDProfessor of Medicine, Pediatrics, Professor of Medicine, Pediatrics,
Pharmacology and PhysiologyPharmacology and PhysiologyThe George Washington UniversityThe George Washington University
Washington, DCWashington, DC
Frederick R. Rickles, MDFrederick R. Rickles, MDProfessor of Medicine, Pediatrics, Professor of Medicine, Pediatrics,
Pharmacology and PhysiologyPharmacology and PhysiologyThe George Washington UniversityThe George Washington University
Washington, DCWashington, DC
Clotting, Cancer, and ControversiesClotting, Cancer, and Controversies

(1801–1867)(1801–1867)
Cancer and Venous ThromboembolismCancer and Venous ThromboembolismThe Legacy of The Legacy of Armand TrousseauArmand Trousseau

Professor Armand TrousseauProfessor Armand TrousseauLectures in Clinical MedicineLectures in Clinical Medicine
“ “ I have always been struck with the frequency I have always been struck with the frequency with which cancerous patients are affected with which cancerous patients are affected with painful oedema of the superior or inferior with painful oedema of the superior or inferior extremities….”extremities….”
New Syndenham Society – 1865New Syndenham Society – 1865

Professor Armand TrousseauProfessor Armand TrousseauMore Observations About Cancer and ThrombosisMore Observations About Cancer and Thrombosis
Lectures in Clinical Medicine, 1865Lectures in Clinical Medicine, 1865
““In other cases, in which the absence of In other cases, in which the absence of appreciable tumour made me hesitate as to the appreciable tumour made me hesitate as to the nature of the disease of the stomach, my doubts nature of the disease of the stomach, my doubts were removed, and I knew the disease to be were removed, and I knew the disease to be cancerous when cancerous when phlegmasia alba dolens phlegmasia alba dolens appeared in one of the limbs.”appeared in one of the limbs.”

Trousseau’s SyndromeTrousseau’s Syndrome
Ironically, Trousseau died of gastric carcinoma six Ironically, Trousseau died of gastric carcinoma six months after writing to his student, Peter, on January months after writing to his student, Peter, on January 1st, 1867:1st, 1867:
““I am lost . . . the phlebitis that has just I am lost . . . the phlebitis that has just appeared tonight leaves me no doubt as to appeared tonight leaves me no doubt as to the nature of my illness”the nature of my illness”

Trousseau’s SyndromeTrousseau’s Syndrome
► Occult cancerOccult cancer in patients with idiopathic in patients with idiopathic venous thromboembolismvenous thromboembolism
► ThrombophlebitisThrombophlebitis in patients with cancerin patients with cancer

Silver Silver In: In: The Hematologist - modified from Blom et. al. The Hematologist - modified from Blom et. al. JAMAJAMA 2005;293:715 2005;293:715
• Population-based MEGA study• N=3220 consecutive patients with 1st VTE
vs. n=2131 control subjects• CA patients = OR 7x VTE risk vs. non-CA
patients
• Population-based MEGA study• N=3220 consecutive patients with 1st VTE
vs. n=2131 control subjects• CA patients = OR 7x VTE risk vs. non-CA
patients
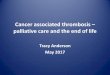
Effect of Malignancy on Risk of Effect of Malignancy on Risk of Venous Thromboembolism (VTE)Venous Thromboembolism (VTE)
00
10
20
30
40
50
Hem
atol
ogic
alH
emat
olog
ical
Lung
Lung
Gas
troi
ntes
tinal
Gas
troi
ntes
tinal
Bre
ast
Bre
ast
Dis
tant
Dis
tant
met
asta
ses
met
asta
ses
0 to
3 m
onth
s0
to 3
mon
ths
3 to
12
mon
ths
3 to
12
mon
ths
1 to
3 y
ears
1 to
3 y
ears
5 to
10
year
s5
to 1
0 ye
ars
> 1
5 ye
ars
> 1
5 ye
ars
Adj
uste
d od
ds r
atio
Adj
uste
d od
ds r
atio
Type of cancerType of cancer Time since cancer diagnosis Time since cancer diagnosis
2828
22.222.220.320.3
4.94.9
19.819.8
53.553.5
14.314.3
2.62.6 1.11.13.63.6

Cancer, Mortality, and VTECancer, Mortality, and VTEEpidemiology and RiskEpidemiology and Risk
► Patients with cancer have a 4- to 6-fold increased risk for Patients with cancer have a 4- to 6-fold increased risk for VTE vs. non-cancer patientsVTE vs. non-cancer patients
► Patients with cancer have a 3-fold increased risk for Patients with cancer have a 3-fold increased risk for recurrence of VTE vs. non-cancer patientsrecurrence of VTE vs. non-cancer patients
► Cancer patients undergoing surgery have a 2-fold Cancer patients undergoing surgery have a 2-fold increased risk for postoperative VTEincreased risk for postoperative VTE
► Death rate from cancer is four-fold higher if patient has Death rate from cancer is four-fold higher if patient has concurrent VTEconcurrent VTE
► VTE 2VTE 2ndnd most common cause of death in ambulatory most common cause of death in ambulatory cancer patients (tied with infection)cancer patients (tied with infection)
Heit et al Heit et al Arch Int Med Arch Int Med 2000;160:809-815 and 2002;162:1245-1248; Prandoni et al 2000;160:809-815 and 2002;162:1245-1248; Prandoni et al Blood Blood 2002;100:3484-3488; White et al 2002;100:3484-3488; White et al Thromb Haemost Thromb Haemost 2003;90:446-455; Sorensen et al 2003;90:446-455; Sorensen et al New Engl J New Engl J Med Med 2000;343:1846-1850); Levitan et al 2000;343:1846-1850); Levitan et al Medicine Medicine 1999;78:285-291; Khorana et al1999;78:285-291; Khorana et al J Thromb Haemost 2007;5:632-4

Mechanisms of Cancer-Induced Thrombosis Mechanisms of Cancer-Induced Thrombosis Critical Interfaces and QuestionsCritical Interfaces and Questions
1.1. Pathogenesis?Pathogenesis?
2.2. Biological significance?Biological significance?
3.3. Potential importance for cancer therapy?Potential importance for cancer therapy?

““There appears in the cachexiae…a There appears in the cachexiae…a
particular condition of the blood that particular condition of the blood that
predisposes it to spontaneouspredisposes it to spontaneous
coagulation.”coagulation.”
Lectures in Clinical Medicine, 1865Lectures in Clinical Medicine, 1865
Trousseau’s Observations (continued)Trousseau’s Observations (continued)

Copyright ©2007 American Society of Hematology. Copyright restrictions may apply.
Varki, A. Blood 2007;110:1723-1729
Multiple Mechanisms in Multiple Mechanisms in Trousseau's SyndromeTrousseau's Syndrome
Tissue Factor microparticlesTissue Factor microparticles

Fibrinolytic activitiesFibrinolytic activities::t-PA, u-PA, u-PAR, t-PA, u-PA, u-PAR, PAI-1, PAI-2PAI-1, PAI-2
Procoagulant Activities Procoagulant Activities
FIBRINFIBRIN
Endothelial cellsEndothelial cells
IL-1, IL-1, TNF-TNF-VEGVEGFF
MonocyteMonocyte
PMN leukocytePMN leukocyte
Activation of Activation of coagulationcoagulation
PlateletsPlatelets
Angiogenesis,Angiogenesis,Basement matrix Basement matrix degradationdegradation
Falanga and Rickles, Falanga and Rickles, New Oncology: ThrombosisNew Oncology: Thrombosis, 2005; , 2005; Hematology, Hematology, 20072007
Interface of Biology and CancerInterface of Biology and Cancer
Tumor Cells

Pathogenesis of Thrombosis in Cancer – Pathogenesis of Thrombosis in Cancer – A Modification of Virchow’s TriadA Modification of Virchow’s Triad
1.1. StasisStasis Prolonged bed restProlonged bed rest Extrinsic compression of blood vessels by tumorExtrinsic compression of blood vessels by tumor
2.2. Vascular InjuryVascular Injury Direct invasion by tumorDirect invasion by tumor Prolonged use of central venous cathetersProlonged use of central venous catheters Endothelial damage by chemotherapy drugsEndothelial damage by chemotherapy drugs Effect of tumor cytokines on vascular endotheliumEffect of tumor cytokines on vascular endothelium
3.3. HypercoagulabilityHypercoagulability Tumor-associated procoagulants and cytokines (tissue factor, Tumor-associated procoagulants and cytokines (tissue factor,
CP, TNFCP, TNF, IL-1, IL-1, VEGF, etc.), VEGF, etc.) Impaired endothelial cell defense mechanisms (APC resistance; Impaired endothelial cell defense mechanisms (APC resistance;
deficiencies of AT, Protein C and S) deficiencies of AT, Protein C and S) Enhanced selectin/integrin-mediated, adhesive interactions Enhanced selectin/integrin-mediated, adhesive interactions
between tumor cells,vascular endothelial cells, platelets and host between tumor cells,vascular endothelial cells, platelets and host macrophagesmacrophages

Mechanisms of Cancer-Induced Thrombosis Mechanisms of Cancer-Induced Thrombosis Clot and Cancer InterfacesClot and Cancer Interfaces
1.1. Pathogenesis?Pathogenesis?
2.2. Biological significance?Biological significance?
3.3. Potential importance for cancer therapy?Potential importance for cancer therapy?

Activation of Blood Coagulation in CancerActivation of Blood Coagulation in CancerBiological Significance?Biological Significance?
► EpiphenomenonEpiphenomenon? ?
Is this a generic secondary event where Is this a generic secondary event where thrombosis is an incidental findingthrombosis is an incidental finding
oor, is clotting activation . . .r, is clotting activation . . .
► A Primary Event?A Primary Event?
Linked to malignant transformation Linked to malignant transformation

TF
VEGF
Angiogenesis
Endothelial cellsEndothelial cells
IL-8IL-8
Blood CoagulationActivation
FIBRIN
PAR-2
Angiogenesis
FVII/FVIIaFVII/FVIIa
THROMBINTHROMBIN
Tumor Cell
TF
Falanga and Rickles, New Oncology:Thrombosis, 2005;1:9-16
Interface of Clotting Activation Interface of Clotting Activation and Tumor Biology and Tumor Biology

Coagulation Cascade and Tumor BiologyCoagulation Cascade and Tumor Biology
Clotting-Clotting-dependentdependent
Clotting-Clotting-dependentdependent
Clotting-Clotting-independentindependent
Clotting-Clotting-dependentdependent
Clotting-Clotting-independentindependent
Fernandez, Patierno and Rickles. Fernandez, Patierno and Rickles. Sem Hem Thromb Sem Hem Thromb 2004;30:31; Ruf. 2004;30:31; Ruf. J Thromb Haemost J Thromb Haemost 2007;5:15842007;5:1584
VIIaVIIa XaXa
Angiogenesis, Tumor Growth and Metastasis
TF Thrombin Fibrin
PARs

Regulation of Vascular Endothelial Growth Factor Production Regulation of Vascular Endothelial Growth Factor Production and Angiogenesis by the Cytoplasmic Tail of Tissue Factorand Angiogenesis by the Cytoplasmic Tail of Tissue Factor
Abe et al Abe et al Proc Nat Acad SciProc Nat Acad Sci 1999;96:8663-8668; Ruf et al 1999;96:8663-8668; Ruf et al Nature MedNature Med 2004;10:502-509 2004;10:502-509
1.1. TF regulates VEGF expression in human cancer cell TF regulates VEGF expression in human cancer cell lineslines
2.2. Human cancer cells with increased TF are more Human cancer cells with increased TF are more angiogenic (and, therefore, more “metastatic’) angiogenic (and, therefore, more “metastatic’) in vivoin vivo due to high VEGF productiondue to high VEGF production

3.3. The cytoplasmic tail of TF, which contains three The cytoplasmic tail of TF, which contains three serine residues, appears to play a role in regulating serine residues, appears to play a role in regulating VEGF expression in human cancer cells, perhaps VEGF expression in human cancer cells, perhaps by mediating signal transductionby mediating signal transduction
4.4. Data consistent with new mechanism(s) by which Data consistent with new mechanism(s) by which TF signals VEGF synthesis in human cancer cells TF signals VEGF synthesis in human cancer cells may provide insight into the relationship between may provide insight into the relationship between clotting and cancerclotting and cancer
Abe et al Abe et al Proc Nat Acad SciProc Nat Acad Sci 1999;96:8663-8668; Ruf et.al. 1999;96:8663-8668; Ruf et.al. Nature MedNature Med 2004;10:502-509 2004;10:502-509
Regulation of Vascular Endothelial Growth Factor Production Regulation of Vascular Endothelial Growth Factor Production and Angiogenesis by the Cytoplasmic Tail of Tissue Factorand Angiogenesis by the Cytoplasmic Tail of Tissue Factor

ActivationActivation of Blood Coagulation of Blood Coagulation in Cancer and Malignant Transformationin Cancer and Malignant Transformation
► Epiphenomenon vs. Epiphenomenon vs. Linked to Malignant Linked to Malignant Transformation?Transformation?
1.1. METMET oncogene induction produces DIC in human liver oncogene induction produces DIC in human liver carcinomacarcinoma (Boccaccio lab) (Boccaccio lab)
(Boccaccio et al (Boccaccio et al Nature 2005;434:396-400) 2005;434:396-400)
2.2. PtenPten loss and loss and EGFREGFR amplification produce TF activation amplification produce TF activation and pseudopalisading necrosis through JunD/Activator and pseudopalisading necrosis through JunD/Activator Protein-1 in human glioblastomaProtein-1 in human glioblastoma (Bratt lab)(Bratt lab)
(Rong et al (Rong et al Ca Res 2005;65:1406-1413; 2005;65:1406-1413; Ca Res 2009;69:2540-9)2009;69:2540-9)
3.3. K-K-rasras oncogene, p53 inactivation and TF induction in oncogene, p53 inactivation and TF induction in human colorectal carcinoma; TF and angiogenesis human colorectal carcinoma; TF and angiogenesis regulation in epithelial tumors by regulation in epithelial tumors by EGFR (EGFR (ErbB1ErbB1)) – – relationship to EMTsrelationship to EMTs (Rak lab) (Rak lab)
(Yu et al (Yu et al Blood 2005;105:1734-1741; Milson et al 2005;105:1734-1741; Milson et al Ca Res 2008;68:10068-76) 2008;68:10068-76)

► METMET encodes a tyrosine kinase receptor for hepatocyte encodes a tyrosine kinase receptor for hepatocyte growth factor/scatter factor (HGF/SF) growth factor/scatter factor (HGF/SF) Drives physiologicalDrives physiological cellular program of “invasive cellular program of “invasive
growth” (tissue morphogenesis, angiogenesis growth” (tissue morphogenesis, angiogenesis and repair)and repair)
Aberrant execution (e.g. hypoxia-induced Aberrant execution (e.g. hypoxia-induced transcription) is associated with neoplastic transcription) is associated with neoplastic transformation, invasion, and metastasistransformation, invasion, and metastasis
Boccaccio et al Boccaccio et al Nature 2005;434:396-4002005;434:396-400
““1. 1. METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation

► Mouse model of Trousseau’s SyndromeMouse model of Trousseau’s Syndrome Targeted activated human Targeted activated human METMET to the mouse liver to the mouse liver
with lentiviral vector and liver-specific promoter with lentiviral vector and liver-specific promoter slowly, progressive hepatocarcinogenesisslowly, progressive hepatocarcinogenesis
Preceded and accompanied by a thrombo-Preceded and accompanied by a thrombo-hemorrhagic syndrome hemorrhagic syndrome
Thrombosis in tail vein occurs early and is followed Thrombosis in tail vein occurs early and is followed by fatal internal hemorrhageby fatal internal hemorrhage
Syndrome characterized by Syndrome characterized by d-dimer and PT and d-dimer and PT and platelet count (DIC)platelet count (DIC)
““METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”
““METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”

Blood Coagulation Parameters in Mice Blood Coagulation Parameters in Mice Transduced with the Transduced with the MET MET OncogeneOncogene
TransgeneTransgene ParameterParameter
Time after Transduction (days)Time after Transduction (days)
0 30 900 30 90GFPGFP
METMET
Platelets (x10Platelets (x1033))
D-dimer (µg/ml)D-dimer (µg/ml)
PT (s)PT (s)
Platelets (x10Platelets (x1033))
D-dimer (µg/ml)D-dimer (µg/ml)
PT (s)PT (s)
968 656 800 968 656 800
<0.05 <0.05 <0.05<0.05 <0.05 <0.05
12.4 11.6 11.412.4 11.6 11.4
974 350 150974 350 150
<0.05 0.11 0.22<0.05 0.11 0.22
12.9 11.8 25.112.9 11.8 25.1

““METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”
““METMET Oncogene Drives a Genetic Programme Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis”Linking Cancer to Haemostasis”
Mouse model of Trousseau’s SyndromeMouse model of Trousseau’s Syndrome
● Genome-wide expression profiling of Genome-wide expression profiling of hepatocytes expressing hepatocytes expressing METMET - - upregulation upregulation ofof PAI-1PAI-1 and and COX-2COX-2 genes with 2-3x genes with 2-3x circulating protein levelscirculating protein levels
● Using either XR5118 (Using either XR5118 (PAI-1 inhibitorPAI-1 inhibitor) or ) or rofecoxib (Vioxx;rofecoxib (Vioxx; COX-2 inhibitorCOX-2 inhibitor) resulted in ) resulted in inhibition of clinical and laboratory evidence inhibition of clinical and laboratory evidence for DIC in micefor DIC in mice

Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
2. “2. “PtenPten and Hypoxia Regulate Tissue Factor and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Expression and Plasma Coagulation By
Glioblastoma”Glioblastoma”► PtenPten = tumor suppressor with lipid and protein = tumor suppressor with lipid and protein
phosphatase activityphosphatase activity
► Loss or inactivation of Loss or inactivation of Pten Pten (70-80% of (70-80% of glioblastomas) leads to Akt activation and glioblastomas) leads to Akt activation and upregulation of upregulation of RasRas/MEK/ERK/MEK/ERK signaling cascade signaling cascade
Rong et al Rong et al Ca ResCa Res 2005;65:1406-1413 2005;65:1406-1413

► Glioblastomas characterized histologically by Glioblastomas characterized histologically by “pseudopalisading necrosis” “pseudopalisading necrosis”
► Thought to be wave of tumor cells migrating away Thought to be wave of tumor cells migrating away from a central hypoxic zone, perhaps created by from a central hypoxic zone, perhaps created by thrombosisthrombosis
► Pseudopalisading cells produce VEGF and IL-8 Pseudopalisading cells produce VEGF and IL-8 and drive angiogenesis and rapid tumor growth and drive angiogenesis and rapid tumor growth
► TF expressed by >90% of grade 3 and 4 malignant TF expressed by >90% of grade 3 and 4 malignant astrocytomas (but only 10% of grades 1 and 2)astrocytomas (but only 10% of grades 1 and 2)
““PtenPten and Hypoxia Regulate Tissue Factor Expression and and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”Plasma Coagulation By Glioblastoma”

Results:Results:
1.1. Hypoxia and Hypoxia and PTEN PTEN loss loss TF (mRNA, Ag and TF (mRNA, Ag and procoagulant activity); partially reversed with procoagulant activity); partially reversed with induction of induction of PTEN PTEN
2.2. Both Both AktAkt and and RasRas pathways modulated TF in pathways modulated TF in sequentially transformed astrocytessequentially transformed astrocytes
3.3. Ex vivo Ex vivo data: data: TF (by IH-chemical staining) in TF (by IH-chemical staining) in pseudopalisades of # 7 human glioblastoma pseudopalisades of # 7 human glioblastoma specimensspecimens
““PtenPten and Hypoxia Regulate Tissue Factor Expression and and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”Plasma Coagulation By Glioblastoma”

Both Both AktAkt and and RasRas Pathways Modulate TF Pathways Modulate TF Expression By Transformed AstrocytesExpression By Transformed Astrocytes
N = NormoxiaN = Normoxia
H = HypoxiaH = Hypoxia
Similar data Similar data for EGFR – for EGFR – upregulationupregulationof TF via JunD/of TF via JunD/AP-1 transcriptionAP-1 transcription((CA Res CA Res 2009;69:2540-9)2009;69:2540-9)

H&EH&E
TF IHC
““PtenPten and Hypoxia Regulate Tissue Factor Expression and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”and Plasma Coagulation By Glioblastoma”
Vascular Endothelium
Pseudopalisading necrosis

Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
3. “Oncogenic Events Regulate Tissue Factor 3. “Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Expression In Colorectal Cancer Cells: Implications For Tumor Progression And Angiogenesis”Tumor Progression And Angiogenesis”
► Activation of K-Activation of K-ras ras oncogene and inactivation of oncogene and inactivation of p53 p53 tumor tumor suppressor suppressor TF expression in TF expression in human human colorectal cancer cellscolorectal cancer cells
► Transforming events dependent on MEK/MAPK and PI3KTransforming events dependent on MEK/MAPK and PI3K► Cell-associated and MP-associated TF activity linked to genetic Cell-associated and MP-associated TF activity linked to genetic
status of cancer cellsstatus of cancer cells► TF siRNA reduced cell surface TF expression, tumor growth and TF siRNA reduced cell surface TF expression, tumor growth and
angiogenesis angiogenesis ► TF may be required for K-TF may be required for K-ras-ras-driven phenotype driven phenotype
Yu et al Yu et al Blood 2005;105:1734-412005;105:1734-41

““Oncogenic Events Regulate Tissue Factor Expression In Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Tumor Progression Colorectal Cancer Cells: Implications For Tumor Progression
And Angiogenesis”And Angiogenesis”TF expression in cancer cells parallels genetic tumor progression TF expression in cancer cells parallels genetic tumor progression
with an impact of K-with an impact of K-ras ras and and p53 p53 statusstatus
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
0
50
100
150
200
250
300
350
400
450
HKh-2 HCT116 379.2
0
20
40
60
80
100
120
140
160
HKh-2 HCT116 379.2Mea
n C
han
nel T
F F
lour
esce
nce
Mea
n C
han
nel T
F F
lour
esce
nce
TF
Act
ivity
(U
/10
TF
Act
ivity
(U
/1066
cells
) c
ells
)
del/+del/+ mut/+mut/+ mut/+mut/++/++/+ +/++/+ del/deldel/del

““Oncogenic Events Regulate Tissue Factor Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Expression In Colorectal Cancer Cells:
Implications For Tumor Progression And Implications For Tumor Progression And Angiogenesis”Angiogenesis”
Effect of TF si mRNA on tumor growth Effect of TF si mRNA on tumor growth in vitro in vitro and and in vivoin vivo
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation

0
2
4
6
8
10
12
14
HCT116 SI-2 SI-3 MG only
Effect of TF si mRNA on new vessel formation in colon cancerEffect of TF si mRNA on new vessel formation in colon cancer
““Oncogenic Events Regulate Tissue Factor Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells”Expression In Colorectal Cancer Cells”
%V
WF
-Pos
itive
Are
a%
VW
F-P
ositi
ve A
rea

““Oncogenic Events Regulate Tissue Factor Expression In Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Tumor Colorectal Cancer Cells: Implications For Tumor
Progression And Angiogenesis”Progression And Angiogenesis”
Matrigel Assay: (D) HCT 116; (E) SI-3 cells – vWF immunohistologyMatrigel Assay: (D) HCT 116; (E) SI-3 cells – vWF immunohistology
Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
Similar amplification of TF with upregulated VEGF induced by mutated EGFR in glioblastoma and lung Similar amplification of TF with upregulated VEGF induced by mutated EGFR in glioblastoma and lung cancer cells, accompanied by epithelial-to-mesenchymal transition (EMT)cancer cells, accompanied by epithelial-to-mesenchymal transition (EMT)
Milsom et al Milsom et al CA Res 2008;68:10068-762008;68:10068-76

Kalluri and Kansaki Kalluri and Kansaki Nature Nature 2008;452:5432008;452:543
(21 nucleotides)*
* Kleinman et al * Kleinman et al NatureNature 2008;452:5912008;452:591
Class Effect of siRNA for Angiogenesis Inhibition Class Effect of siRNA for Angiogenesis Inhibition via Toll-Like Receptior 3 (TLR 3)via Toll-Like Receptior 3 (TLR 3)

Mechanisms of Cancer-Induced Thrombosis Mechanisms of Cancer-Induced Thrombosis ClinicalClinical ImplicationsImplications
1.1. Pathogenesis?Pathogenesis?
2.2. Biological significance?Biological significance?
3.3. Potential importance for cancer Potential importance for cancer therapy?therapy?

Activation of Blood Coagulation Activation of Blood Coagulation in Cancer: Malignant Transformationin Cancer: Malignant Transformation
► QQ: What do all of these experiments in : What do all of these experiments in micemice have to do with real have to do with real patientspatients with cancer? with cancer?
► AA: They suggest two things:: They suggest two things:● Tumor cell-derived, Tumor cell-derived, TF-rich microparticlesTF-rich microparticles
(MPs) may be important as a predictive test (MPs) may be important as a predictive test for VTEfor VTE
● All patients with oncogene-driven cancer may All patients with oncogene-driven cancer may need prophylactic anticoagulation need prophylactic anticoagulation

► Retrospective study Retrospective study
► Immunohistologic (IH) and microarray data on Immunohistologic (IH) and microarray data on expression of TF and VEGF, as well as microvascular expression of TF and VEGF, as well as microvascular density (MVD) in:density (MVD) in: Normal pancreas (10)Normal pancreas (10) Pre-malignant pancreatic lesions:Pre-malignant pancreatic lesions:
• Intraductal papillary mucinous neoplasms (IPMN; 70)Intraductal papillary mucinous neoplasms (IPMN; 70)• Pancreatic intrepithelial neoplasia (PanIN; 40)Pancreatic intrepithelial neoplasia (PanIN; 40)
Resected or metastatic pancreatic adenoca (130)Resected or metastatic pancreatic adenoca (130)
► SurvivalSurvival
► VTE RateVTE Rate
Tissue Factor Expression, Angiogenesis, and Tissue Factor Expression, Angiogenesis, and Thrombosis in Human Pancreatic CancerThrombosis in Human Pancreatic Cancer
Khorana et al CKhorana et al Clin Cancer Reslin Cancer Res 2007;13:2870 2007;13:2870

Immunohistologic Correlation of TF with the Expression of Immunohistologic Correlation of TF with the Expression of Other Angiogenesis Variables in Resected Pancreatic CancerOther Angiogenesis Variables in Resected Pancreatic Cancer
Khorana et.al. Clin CA Res 2007:13:2870
High TF High TF ExpressionExpression
Low TF Low TF ExpressionExpression P ValueP Value
VEGF ExpressionVEGF Expression
NegativeNegative 1313 4141 <0.0001<0.0001
PositivePositive 5353 1515
Microvessel DensityMicrovessel Density
V6 per tissue coreV6 per tissue core 2727 3333 0.0470.047
>6 per tissue core>6 per tissue core 3939 2323
MedianMedian 88 66 0.010.01

Symptomatic VTE in Pancreatic CancerSymptomatic VTE in Pancreatic Cancer
Khorana et al Clin CA Res 2007;13:2872
5/19; 5/19; 26.3%26.3%
1/22; 1/22; 4.5%4.5%

Median Survival of 122 Median Survival of 122 Resected Pancreatic Cancer PatientsResected Pancreatic Cancer Patients
Mo
nth
sM
on
ths
17.917.9
12.612.6
P P = 0.16= 0.16(HR 2.06; (HR 2.06; 0.74-5.7)0.74-5.7)
Khorana et al Clin CA Res 2007;13:2872

1. 1. Does activation of blood coagulation affect Does activation of blood coagulation affect the biology of cancer positively or the biology of cancer positively or negatively?negatively?
2. 2. Can we treat tumors more effectively Can we treat tumors more effectively using using coagulation protein targets?coagulation protein targets?
3. 3. Can anticoagulation alter the biology of Can anticoagulation alter the biology of cancer?cancer?
Cancer and ThrombosisCancer and ThrombosisYear 2009 State-of-the-Science UpdateYear 2009 State-of-the-Science Update
Key QuestionsKey Questions Key QuestionsKey Questions

1. 1. Epidemiologic evidence is Epidemiologic evidence is suggestivesuggestive that VTE is a bad that VTE is a bad prognostic sign in cancerprognostic sign in cancer
2. 2. Experimental evidence is Experimental evidence is supportive supportive of the use of of the use of antithrombotic strategies for both prevention of antithrombotic strategies for both prevention of thrombosis and inhibition of tumor growth thrombosis and inhibition of tumor growth
3. 3. Results of recent, randomized clinical trials of LMWHs in Results of recent, randomized clinical trials of LMWHs in cancer patients indicate superiority to oral agents in cancer patients indicate superiority to oral agents in preventing recurrent VTE, as well as increasing survival preventing recurrent VTE, as well as increasing survival ((notnot due to prevention of VTE) due to prevention of VTE)
Cancer and ThrombosisCancer and ThrombosisYear 2009 State-of-the-Science UpdateYear 2009 State-of-the-Science Update
Tentative AnswersTentative Answers

LMWH and Prolongation LMWH and Prolongation of Cancer Survivalof Cancer Survival
Mechanistic Explanations
Coagulation Proteases
Direct Heparin
OtherVTE

Heparins and Tumour BiologyHeparins and Tumour Biology
Multiple Potential Modes of Action
Angiogenesis Apoptosis Heparanase Adhesion

Ex VivoEx Vivo Angiogenesis: Angiogenesis: Embryonic Chick Aortic RingsEmbryonic Chick Aortic Rings
Control Aortic Ring: Day 5Control Aortic Ring: Day 5 10U/ml Dalteparin-Treated Aortic Ring: 10U/ml Dalteparin-Treated Aortic Ring: Day 5 Day 5
Fernandez, Patierno and Rickles. Fernandez, Patierno and Rickles. Proc AACR Proc AACR 2003;44:698 (Abstr. #3055)2003;44:698 (Abstr. #3055)

Effects of Low-Molecular Weight Heparin on Effects of Low-Molecular Weight Heparin on Lung Cancer Cell ApoptosisLung Cancer Cell Apoptosis
P<0.05P<0.05
Chen et al Chen et al Cancer Invest 2008;Cancer Invest 2008;26:718-2426:718-24
• G1 arrestG1 arrest• Decrease in Decrease in S phaseS phase• 3-fold 3-fold in p21 in p21WAF1 WAF1
and p27and p27KIP1 KIP1 ((p p <0.01)<0.01) • Reversed apoptosisReversed apoptosis and G1 arrest with and G1 arrest with p21 or p27 siRNAp21 or p27 siRNA

0
100
200
300
400
500
VEGFVEGF FGF-2FGF-2 TNF-TNF-
**
*
*
**
CytokineCytokine +enoxaparin+enoxaparin +dalteparin+dalteparin+UFH+UFH
§
§ §
ControlControl
** *
Marchetti et al.Marchetti et al. Thromb Res Thromb Res 20082008;121:637-645;121:637-645
Heparins Inhibit Cytokine–Induced Heparins Inhibit Cytokine–Induced Capillary Tube FormationCapillary Tube Formation
§ = p<0.05 vs control, * = p<0.05 vs cytokine
Tub
e Le
ngth
(m
m/c
mT
ube
Leng
th (
mm
/cm 22
))

LMWH and VEGF Antisense Oligonucleotides Inhibit LMWH and VEGF Antisense Oligonucleotides Inhibit Growth and Metastasis of 3LL Tumors in MiceGrowth and Metastasis of 3LL Tumors in Mice
► 40 mice with Lewis Lung Cancer (3LL)40 mice with Lewis Lung Cancer (3LL)► Rx qod x 15 with:Rx qod x 15 with:
● Control (saline)Control (saline)● VEGF antisense oligos (ASODN)VEGF antisense oligos (ASODN)● VEGF mismatch sense oligo (MSODN)VEGF mismatch sense oligo (MSODN)● LMWH (dalteparin)LMWH (dalteparin)● LMWH + ASODNLMWH + ASODN
► RESULTSRESULTS: : Growth InhibitGrowth Inhibit** Lung MetsLung Mets**
● ASODNASODN 47%47% 38%38%● LMWHLMWH 27%27% 38%38%● CombinedCombined 59%59% 25%25%
* * P < 0.05P < 0.05
Zhang YH et al Zhang YH et al Chinese Med JChinese Med J 2006;86:749-52 2006;86:749-52

Inhibition of Binding of Selectins to Inhibition of Binding of Selectins to Human Colon Carcinoma by Heparins Human Colon Carcinoma by Heparins
Stevenson et al Clin Ca Res 2005;11:7003-11

Heparin Inhibition of B16 Melanoma Heparin Inhibition of B16 Melanoma Lung Metastasis in MiceLung Metastasis in Mice
Stevenson et al Stevenson et al Clin Ca Res Clin Ca Res 2005;11:7003-112005;11:7003-11

Coagulation Cascade and Tumor BiologyCoagulation Cascade and Tumor Biology
Clotting-Clotting-dependentdependent
Clotting-Clotting-dependentdependent
Clotting-Clotting-independentindependent
Clotting-Clotting-dependentdependent
Clotting-Clotting-independentindependent
Fernandez, Patierno and Rickles. Fernandez, Patierno and Rickles. Sem Hem Thromb Sem Hem Thromb 2004;30:31; Ruf.2004;30:31; Ruf. J Thromb Haemost J Thromb Haemost 2007; 5:1584; 2007; 5:1584; Varki Varki Blood Blood 2007;110:1723-17292007;110:1723-1729
VIIaVIIa XaXa
Angiogenesis, Tumor Growth and Metastasis
??
LMWHs LMWHs (e.g. (e.g. dalteparindalteparin); Non-anticoagulant heparins or inhibitors ); Non-anticoagulant heparins or inhibitors
??
TF Thrombin Fibrin
PARs

A Systematic Analysis of VTE A Systematic Analysis of VTE Prophylaxis in the Setting of Cancer Prophylaxis in the Setting of Cancer
Linking Science and Evidence to Clinical Practice—Linking Science and Evidence to Clinical Practice—What Do Trials Teach?What Do Trials Teach?
A Systematic Analysis of VTE A Systematic Analysis of VTE Prophylaxis in the Setting of Cancer Prophylaxis in the Setting of Cancer
Linking Science and Evidence to Clinical Practice—Linking Science and Evidence to Clinical Practice—What Do Trials Teach?What Do Trials Teach?
Program ChairmanProgram ChairmanCraig Kessler, MD MACPCraig Kessler, MD MACP
Director, Division of CoagulationDirector, Division of CoagulationLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Georgetown University Medical CenterGeorgetown University Medical CenterWashington, DCWashington, DC
Program ChairmanProgram ChairmanCraig Kessler, MD MACPCraig Kessler, MD MACP
Director, Division of CoagulationDirector, Division of CoagulationLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Georgetown University Medical CenterGeorgetown University Medical CenterWashington, DCWashington, DC
Innovation ● Investigation ● ApplicationInnovation ● Investigation ● Application

VTE and Cancer: EpidemiologyVTE and Cancer: Epidemiology
► Of all cases of VTE:Of all cases of VTE:● About 20% occur in cancer patientsAbout 20% occur in cancer patients● Annual incidence of VTE in cancer Annual incidence of VTE in cancer
patients ≈ 1/250patients ≈ 1/250
► Of all cancer patients:Of all cancer patients:● 15% will have symptomatic VTE15% will have symptomatic VTE● As many as 50% have VTE at autopsyAs many as 50% have VTE at autopsy
► Compared to patients without cancer:Compared to patients without cancer:● Higher risk of first and recurrent VTEHigher risk of first and recurrent VTE● Higher risk of bleeding on anticoagulantsHigher risk of bleeding on anticoagulants● Higher risk of dyingHigher risk of dying
Lee AY, Levine MN. Lee AY, Levine MN. CirculationCirculation. 2003;107:23 Suppl 1:I17-I21. 2003;107:23 Suppl 1:I17-I21

1.1. Ambrus JL et al. Ambrus JL et al. J MedJ Med. 1975;6:61-64. 1975;6:61-642.2. Donati MB. Donati MB. HaemostasisHaemostasis. 1994;24:128-131. 1994;24:128-1313.3. Johnson MJ et al. Johnson MJ et al. Clin Lab HaemClin Lab Haem. 1999;21:51-54. 1999;21:51-544.4. Prandoni P et al. Prandoni P et al. Ann Intern MedAnn Intern Med. 1996;125:1-7. 1996;125:1-7
DVT and PE in CancerDVT and PE in Cancer Facts, Findings, and Natural HistoryFacts, Findings, and Natural History
► VTE is the second leading cause of death VTE is the second leading cause of death in hospitalized in hospitalized cancer patientscancer patients1,21,2
► The risk of VTE in cancer patients undergoing surgery is The risk of VTE in cancer patients undergoing surgery is 3-3- to 5-fold higher to 5-fold higher than those without cancerthan those without cancer22
► Up to Up to 50% of cancer patients 50% of cancer patients may have evidence of may have evidence of asymptomatic DVT/PEasymptomatic DVT/PE33
► Cancer patients with symptomatic DVT exhibit a Cancer patients with symptomatic DVT exhibit a high risk high risk for recurrent DVT/PE that persists for many yearsfor recurrent DVT/PE that persists for many years44

Clinical Features of VTE in CancerClinical Features of VTE in Cancer
► VTE has significant negative impact on quality VTE has significant negative impact on quality of lifeof life
► VTE may be the presenting sign of occult VTE may be the presenting sign of occult malignancymalignancy● 10% with idiopathic VTE develop cancer within 10% with idiopathic VTE develop cancer within
2 years2 years● 20% have recurrent idiopathic VTE20% have recurrent idiopathic VTE● 25% have bilateral DVT25% have bilateral DVT
Bura Bura et. al.,et. al., J Thromb HaemostJ Thromb Haemost 2004;2:445-51 2004;2:445-51

Thrombosis and SurvivalThrombosis and SurvivalLikelihood of Death After HospitalizationLikelihood of Death After Hospitalization
00 20 20 40 40 60 60 80 80 100 100 120 120140 160 180140 160 1800.000.00
0.200.20
0.400.40
1.001.00
0.800.80
0.600.60
DVT/PE and Malignant DiseaseDVT/PE and Malignant Disease
Malignant DiseaseMalignant Disease
DVT/PE OnlyDVT/PE Only
Nonmalignant DiseaseNonmalignant Disease
Number of DaysNumber of Days
Pro
bab
ility
of D
ea
thP
roba
bili
ty o
f De
ath
Levitan N, et al. Medicine 1999;78:285Levitan N, et al. Medicine 1999;78:285

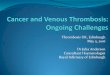
Incidence of VTE and Colon Cancer StageIncidence of VTE and Colon Cancer StageIncidence of VTE and Colon Cancer StageIncidence of VTE and Colon Cancer Stage
White RH et al. Thrombosis Research 120 Suppl. 2 (2007) S29-40White RH et al. Thrombosis Research 120 Suppl. 2 (2007) S29-40
Days after Cancer DiagnosisDays after Cancer Diagnosis
Inci
denc
e of
VT
E (
%)
Inci
denc
e of
VT
E (
%)
0 50 100 150 200 250 300 350 4000 50 100 150 200 250 300 350 400
7%7%
6%6%
5%5%
4%4%
3%3%
2%2%
1%1%
0%0%
Local Regional RemoteLocal Regional Remote

R.H. White et al. Thombosis Research 120 Suppl. 2 (2007) S29-S40R.H. White et al. Thombosis Research 120 Suppl. 2 (2007) S29-S40
Cancer typeCancer typeHazard ratio (95% CI) for death within one year, cases Hazard ratio (95% CI) for death within one year, cases
with VTE diagnosed in year 1 vs. no VTE, by stagewith VTE diagnosed in year 1 vs. no VTE, by stage
LocalLocal RegionalRegional RemoteRemote
ProstateProstate 5.6 (3.8-8.5)5.6 (3.8-8.5)‡‡ 4.7 (1.9-11.5)4.7 (1.9-11.5) ‡ ‡ 2.8 (1.5-5.0)2.8 (1.5-5.0) †
BreastBreast 6.6 (3.7-11.8)6.6 (3.7-11.8) ‡ ‡ 2.4 (1.3-4.5)2.4 (1.3-4.5) ‡ ‡ 1.8 (1.1-2.9)*1.8 (1.1-2.9)*
LungLung 3.1 (2.1-4.5)3.1 (2.1-4.5) ‡ ‡ 2.9 (2.3-3.5)2.9 (2.3-3.5) ‡ ‡ 2.5 (2.3-2.7)2.5 (2.3-2.7) ‡ ‡
Colon/rectumColon/rectum 3.2 (1.8-5.5)3.2 (1.8-5.5) ‡ ‡ 2.2 (1.7-3.0)2.2 (1.7-3.0) ‡ ‡ 2.0 (1.7-2.4)2.0 (1.7-2.4) ‡ ‡
MelanomaMelanoma 14.4 (4.6-45.2)14.4 (4.6-45.2) ‡ ‡ N/AN/A 2.8 (1.5-5.3)2.8 (1.5-5.3) †
Non-Hodgkin’s lymphomaNon-Hodgkin’s lymphoma 3.2 (1.9-5.3)3.2 (1.9-5.3) ‡ ‡ 2.0 (1.3-3.2)2.0 (1.3-3.2) † 2.3 (1.7-3.1)2.3 (1.7-3.1) ‡ ‡
UterusUterus 7.0 (3.4-14.2)7.0 (3.4-14.2) ‡ ‡ 9.1 (4.8-17.2)9.1 (4.8-17.2) ‡ ‡ 1.7 (1.0-3.0)*1.7 (1.0-3.0)*
BladderBladder 3.2 (1.7-6.2)3.2 (1.7-6.2) ‡ ‡ 3.3 (1.7-6.4)3.3 (1.7-6.4) ‡ ‡ 3.3 (1.8-6.2)3.3 (1.8-6.2) ‡ ‡
PancreasPancreas 2.3 (1.2-4.6)*2.3 (1.2-4.6)* 3.8 (2.8-5.1)3.8 (2.8-5.1) ‡ ‡ 2.3 (1.9-2.7)2.3 (1.9-2.7) ‡ ‡
StomachStomach 2.4 (1.1-5.1)*2.4 (1.1-5.1)* 1.5 (1.0-2.1)*1.5 (1.0-2.1)* 1.8 (1.4-2.3)1.8 (1.4-2.3) ‡ ‡
OvaryOvary 11.3 (2.5-51.7)11.3 (2.5-51.7) † 4.8 (1.1-20.4)*4.8 (1.1-20.4)* 2.3 (1.7-3.0)2.3 (1.7-3.0) ‡ ‡
KidneyKidney 3.2 (1.2-8.8)*3.2 (1.2-8.8)* 1.4 (0.6-3.2)1.4 (0.6-3.2) 1.3 (0.9-2.0)1.3 (0.9-2.0)
* p<0.05; * p<0.05; †p<0.01); p<0.01); ‡ p<0.001)p<0.001)
Symptomatic VTE in Cancer Reduces Survival Symptomatic VTE in Cancer Reduces Survival Counterintuitively, Magnitude of Effect on Survival is Greatest with Counterintuitively, Magnitude of Effect on Survival is Greatest with
Local Stage Disease Local Stage Disease

VTE Associated with Accelerated Death in Breast Cancer VTE Associated with Accelerated Death in Breast Cancer Does Symptomatic VTE Reflect Presence or Emergence Does Symptomatic VTE Reflect Presence or Emergence
of Metastatic, Aggressive Cancer?of Metastatic, Aggressive Cancer?
White, et al. Thromb Res,120 suppl. 2 (2007)White, et al. Thromb Res,120 suppl. 2 (2007)White, et al. Thromb Res,120 suppl. 2 (2007)White, et al. Thromb Res,120 suppl. 2 (2007)

Recurrent Ovarian CancerRecurrent Ovarian Cancer
Fotopoulou C et al. Thromb Res 2009Fotopoulou C et al. Thromb Res 2009
• • 7% symptomatic VTE (2.8-6.1% in primary ovarian Cancer)7% symptomatic VTE (2.8-6.1% in primary ovarian Cancer)• 78% of VTE in ROC occur within 2 months of second line chemo regimen: • 78% of VTE in ROC occur within 2 months of second line chemo regimen: cisplatin-relatedcisplatin-related• Ascites is the only independent risk factor for VTE (HR=2.2) • Ascites is the only independent risk factor for VTE (HR=2.2)
• • 7% symptomatic VTE (2.8-6.1% in primary ovarian Cancer)7% symptomatic VTE (2.8-6.1% in primary ovarian Cancer)• 78% of VTE in ROC occur within 2 months of second line chemo regimen: • 78% of VTE in ROC occur within 2 months of second line chemo regimen: cisplatin-relatedcisplatin-related• Ascites is the only independent risk factor for VTE (HR=2.2) • Ascites is the only independent risk factor for VTE (HR=2.2)

Hospital Mortality With or Without VTEHospital Mortality With or Without VTE
Khorana, JCO, 2006Khorana, JCO, 2006
Mor
talit
y (%
)M
orta
lity
(%)
Mor
talit
y (%
)M
orta
lity
(%)
N=66,016N=66,016 N=20,591N=20,591 N=17,360N=17,360

Thrombosis Risk In Cancer Thrombosis Risk In Cancer
Primary ProphylaxisPrimary Prophylaxis► Medical InpatientsMedical Inpatients
► SurgerySurgery
► RadiotherapyRadiotherapy
► Central Venous CathetersCentral Venous Catheters

Risk Factors for Cancer-Associated VTERisk Factors for Cancer-Associated VTE
► CancerCancer● Type Type
• Men: prostate, colon, brain, lungMen: prostate, colon, brain, lung• Women: breast, ovary, lungWomen: breast, ovary, lung
● StageStage► TreatmentsTreatments
● SurgerySurgery• 10-20% proximal DVT10-20% proximal DVT• 4-10% clinically evident PE4-10% clinically evident PE• 0.2-5% fatal PE0.2-5% fatal PE
● ChemotherapyChemotherapy● Central venous cathetersCentral venous catheters (~4% generate clinically (~4% generate clinically
relevant VTE)relevant VTE)► PatientPatient
● Prior VTEPrior VTE● ComorbiditiesComorbidities● Genetic backgroundGenetic background

Medical InpatientsMedical Inpatients
Cancer and ThrombosisCancer and Thrombosis

PharmacologicPharmacologic(Prophylaxis & Treatment)(Prophylaxis & Treatment)
NonpharmacologicNonpharmacologic(Prophylaxis)(Prophylaxis)
Antithrombotic Therapy: ChoicesAntithrombotic Therapy: Choices
IntermittentPneumaticCompression
Elastic Stockings
InferiorVena CavaFilter
OralAnticoagulants
UnfractionatedHeparin (UH)
Low Molecular Weight Heparin (LMWH)
New Agents: e.g. Fondaparinux,Direct anti-Xa inhibitors,Direct anti-IIa, etc.?

Prophylaxis Studies in Medical PatientsProphylaxis Studies in Medical Patients
Francis, NEJM, 2007Francis, NEJM, 2007
Placebo EnoxaparinPlacebo Enoxaparin MEDENOX TrialMEDENOX Trial
Placebo DalteparinPlacebo Dalteparin PREVENTPREVENT
Placebo FondaparinuxPlacebo Fondaparinux ARTEMISARTEMIS
Rat
e of
VT
E (
%)
Rat
e of
VT
E (
%)
Relative Relative risk risk
reduction reduction 63%63%
Relative Relative risk risk
reduction reduction 44%44%
Relative Relative risk risk
reduction reduction 47%47%

ASCO GuidelinesASCO Guidelines
1. SHOULD HOSPITALIZED PATIENTS WITH1. SHOULD HOSPITALIZED PATIENTS WITHCANCER RECEIVE ANTICOAGULATION FORCANCER RECEIVE ANTICOAGULATION FORVTE PROPHYLAXISVTE PROPHYLAXIS??
Recommendation. Recommendation. Hospitalized patients with Hospitalized patients with cancer should be considered candidates for cancer should be considered candidates for VTE prophylaxis with anticoagulants in the VTE prophylaxis with anticoagulants in the absence of bleeding or other contraindications absence of bleeding or other contraindications to anticoagulation.to anticoagulation.
Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505.Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505.

Surgical PatientsSurgical Patients
Cancer and ThrombosisCancer and Thrombosis

► Cancer patients have Cancer patients have 2-fold risk of post-operative DVT/PE 2-fold risk of post-operative DVT/PE and >3-fold risk of fatal PE despite prophylaxis:and >3-fold risk of fatal PE despite prophylaxis:
Kakkar AK, et al. Kakkar AK, et al. Thromb HaemostThromb Haemost 2001; 86 (suppl 1): OC1732 2001; 86 (suppl 1): OC1732
Incidence of VTE in Surgical PatientsIncidence of VTE in Surgical Patients
No CancerNo CancerN=16,954N=16,954
CancerCancerN=6124N=6124
P-valueP-value
Post-op VTEPost-op VTE 0.61%0.61% 1.26%1.26% <0.0001<0.0001
Non-fatal PENon-fatal PE 0.27%0.27% 0.54%0.54% <0.0003<0.0003
Autopsy PEAutopsy PE 0.11%0.11% 0.41%0.41% <0.0001<0.0001
DeathDeath 0.71%0.71% 3.14%3.14% <0.0001<0.0001

Natural History of VTE in Cancer Surgery: Natural History of VTE in Cancer Surgery: The @RISTOS RegistryThe @RISTOS Registry
► Web-Based Registry of Cancer SurgeryWeb-Based Registry of Cancer Surgery Tracked 30-day incidence of VTE in 2373 patientsTracked 30-day incidence of VTE in 2373 patients
Type of surgeryType of surgery • • 52% General 52% General • • 29% Urological29% Urological • • 19% Gynecologic19% Gynecologic
82% received in-hospital thromboprophylaxis82% received in-hospital thromboprophylaxis
31% received post-discharge thromboprophylaxis31% received post-discharge thromboprophylaxis
FindingsFindings
► 2.1% incidence of clinically overt VTE (0.8% fatal)2.1% incidence of clinically overt VTE (0.8% fatal)
► Most events occur after hospital discharge Most events occur after hospital discharge
► Most common cause of 30-day post-op deathMost common cause of 30-day post-op death
Agnelli, Ann Surg 2006; 243: 89-95Agnelli, Ann Surg 2006; 243: 89-95

LMWH vs. UFHLMWH vs. UFH► Abdominal or pelvic surgery for cancer (mostly colorectal)Abdominal or pelvic surgery for cancer (mostly colorectal)
► LMWH once daily vs. UFH tid for 7–10 days post-opLMWH once daily vs. UFH tid for 7–10 days post-op
► DVT on venography at day 7–10 and symptomatic VTEDVT on venography at day 7–10 and symptomatic VTE
1. ENOXACAN Study Group. 1. ENOXACAN Study Group. Br J SurgBr J Surg 1997;84:1099–103 1997;84:1099–1032. McLeod R, et al. 2. McLeod R, et al. Ann SurgAnn Surg 2001;233:438-444 2001;233:438-444
Prophylaxis in Surgical PatientsProphylaxis in Surgical Patients
StudyStudy NN DesignDesign RegimensRegimens
ENOXACAN ENOXACAN 11 631631 double-blinddouble-blind enoxaparin vs. UFHenoxaparin vs. UFH
Canadian Colorectal Canadian Colorectal DVT Prophylaxis DVT Prophylaxis 22 475475 double-blinddouble-blind enoxaparin vs. UFHenoxaparin vs. UFH

Canadian Canadian Colorectal DVT Colorectal DVT Prophylaxis TrialProphylaxis Trial13.9%13.9%
1.5% 2.7%1.5% 2.7%
16.9%16.9%
N=234N=234
N=241N=241
McLeod R, et al. McLeod R, et al. Ann SurgAnn Surg 2001;233:438-444 2001;233:438-444
P=0.052P=0.052
In
cide
nce
of O
utco
me
Eve
ntIn
cide
nce
of O
utco
me
Eve
nt
VTEVTE Major BleedingMajor Bleeding(Cancer) (All)(Cancer) (All)
Prophylaxis in Surgical PatientsProphylaxis in Surgical Patients

VTE Prox Any MajorVTE Prox Any Major DVT Bleeding BleedingDVT Bleeding Bleeding
P=0.02
5.1%
1.8%
Bergqvist D, et al. (for the ENOXACAN II investigators) Bergqvist D, et al. (for the ENOXACAN II investigators) N Engl J MedN Engl J Med 2002;346:975-980 2002;346:975-980
ENOXACAN IIENOXACAN II
In
cide
nce
of O
utco
me
Eve
ntIn
cide
nce
of O
utco
me
Eve
nt
N=167
N=165
0% 0.4%
12.0%
4.8%
NNT = 140.6%
3.6%
Extended Prophylaxis inExtended Prophylaxis inSurgical PatientsSurgical Patients

► A multicenter, prospective, assessor-blinded, open-label, A multicenter, prospective, assessor-blinded, open-label, randomized trial: randomized trial: Dalteparin administered for 28 days after Dalteparin administered for 28 days after major abdominal surgery major abdominal surgery compared to 7 days of treatmentcompared to 7 days of treatment
► RESULTS:RESULTS: Cumulative Cumulative incidence of VTE was reduced from incidence of VTE was reduced from 16.3% with short-term thromboprophylaxis (29/178 16.3% with short-term thromboprophylaxis (29/178 patients) to 7.3%patients) to 7.3% after prolonged thromboprophylaxis after prolonged thromboprophylaxis (12/165) (12/165) (relative risk reduction 55%; (relative risk reduction 55%; 95% confidence 95% confidence interval 15-76; P=0.012).interval 15-76; P=0.012).
► CONCLUSIONS:CONCLUSIONS: 4-week administration of dalteparin, 5000 4-week administration of dalteparin, 5000 IU once daily, after major abdominal surgery significantly IU once daily, after major abdominal surgery significantly reduces the rate of VTEreduces the rate of VTE, without increasing the risk of , without increasing the risk of bleeding, compared with 1 week of thromboprophylaxis.bleeding, compared with 1 week of thromboprophylaxis.
Major Abdominal Surgery: FAME InvestigatorsMajor Abdominal Surgery: FAME Investigators—Dalteparin Extended —Dalteparin Extended
Rasmussen, J Thromb Haemost. 2006 Nov;4(11):2384-90. Epub 2006 Aug 1.Rasmussen, J Thromb Haemost. 2006 Nov;4(11):2384-90. Epub 2006 Aug 1.

ASCO Guidelines: VTE ProphylaxisASCO Guidelines: VTE Prophylaxis
► All patients undergoing major surgical intervention All patients undergoing major surgical intervention for malignant disease should be considered for for malignant disease should be considered for prophylaxis.prophylaxis.
► Patients undergoing laparotomy, laparoscopy, or Patients undergoing laparotomy, laparoscopy, or thoracotomy lasting > 30 min should receive thoracotomy lasting > 30 min should receive pharmacologic prophylaxis.pharmacologic prophylaxis.
► Prophylaxis should be continued at least 7 – 10 Prophylaxis should be continued at least 7 – 10 days post-op. Prolonged prophylaxis for up to 4 days post-op. Prolonged prophylaxis for up to 4 weeks may be considered in patients undergoing weeks may be considered in patients undergoing major surgery for cancer with high-risk features.major surgery for cancer with high-risk features.
Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505.Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505.

Thrombosis is a potential complication of central Thrombosis is a potential complication of central venous catheters, including these events:venous catheters, including these events:
–Fibrin sheath formationFibrin sheath formation
–Superficial phlebitisSuperficial phlebitis
–Ball-valve clotBall-valve clot
–Deep vein thrombosis (DVT)Deep vein thrombosis (DVT)
Central Venous CathetersCentral Venous Catheters
Geerts W, et al. Geerts W, et al. ChestChest Jun 2008: 381S–453S Jun 2008: 381S–453S

Placebo-Controlled TrialsPlacebo-Controlled Trials
StudyStudy RegimenRegimen NN CRT (%)CRT (%)
Reichardt* Reichardt* 20022002
Dalteparin 5000 U dailyDalteparin 5000 U dailyplaceboplacebo
285285140140
11 (3.7)11 (3.7) 5 (3.4)5 (3.4)
Couban*Couban*20022002
Warfarin 1mg dailyWarfarin 1mg dailyplaceboplacebo
130130125125
6 (4.6)6 (4.6) 5 (4.0)5 (4.0)
ETHICSETHICS††
20042004Enoxaparin 40 mg dailyEnoxaparin 40 mg daily
placeboplacebo155155155155
22 (14.2)22 (14.2)28 (18.1)28 (18.1)
**symptomatic outcomessymptomatic outcomes;; ††routine venography at 6 weeksroutine venography at 6 weeks
Prophylaxis for Venous CathetersProphylaxis for Venous Catheters
Reichardt P, et al. Reichardt P, et al. Proc ASCOProc ASCO 2002;21:369a; Couban S, et al, 2002;21:369a; Couban S, et al, BloodBlood 2002;100:703a; Agnelli G, et 2002;100:703a; Agnelli G, et al. al. Proc ASCOProc ASCO 2004;23:730 2004;23:730

Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567
Thrombotic Thrombotic EventsEvents
Warfarin evaluationWarfarin evaluation Dose evaluationDose evaluation
No No warfarin warfarin (n=404)(n=404)
Warfarin Warfarin (n=408)(n=408)
Relative risk Relative risk (95% CI, p value)(95% CI, p value)
Fixed-Fixed-dose dose
warfarin warfarin (n=471)(n=471)
Dose-Dose-adjusted adjusted warfarin warfarin (n=473)(n=473)
Relative risk Relative risk (95% CI, p value)(95% CI, p value)
Catheter-Catheter-related related
thrombotic thrombotic eventsevents
24 24 (6%)(6%)
24 24 (6%)(6%)
0.990.99(0.57-1.72, 0.98)(0.57-1.72, 0.98)
34 34 (7%)(7%)
13 13 (3%)(3%)
0.38 0.38 (0.20-0.71,0.002)(0.20-0.71,0.002)
No catheter-No catheter-related eventrelated event
370 370 (92%)(92%)
372 372 (91%)(91%) --
433 433 (92%)(92%)
448 448 (95%)(95%) --
Not knownNot known 10 10 (2%)(2%)
12 12 (3%)(3%)
4 4 (<1%)(<1%)
12 12 (3%)(3%)
All thrombotic All thrombotic eventsevents
38 38 (9%)(9%)
30 30 (7%)(7%)
0.78 0.78 (0.50-1.24), 0.30(0.50-1.24), 0.30
37 37 (8%)(8%)
26 26 (6%)(6%)
0.70 0.70 (0.43-1.14, 0.15)(0.43-1.14, 0.15)
WARP: Prophylactic Warfarin Does Not WARP: Prophylactic Warfarin Does Not Reduce Catheter-Associated Thrombosis in CAReduce Catheter-Associated Thrombosis in CA

Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567
WARP: Prophylactic Warfarin Does Not WARP: Prophylactic Warfarin Does Not Reduce Catheter-Associated Thrombosis in CAReduce Catheter-Associated Thrombosis in CA
Bleeding Bleeding and Raised and Raised
INRINR
Warfarin evaluationWarfarin evaluation Dose evaluationDose evaluation
No No warfarin warfarin (n=404)(n=404)
Warfarin Warfarin (n=408)(n=408)
Relative risk Relative risk (95% CI, p value)(95% CI, p value)
Fixed-Fixed-dose dose
warfarin warfarin (n=471)(n=471)
Dose-Dose-adjusted adjusted warfarin warfarin (n=473)(n=473)
Relative risk Relative risk (95% CI, p value)(95% CI, p value)
Major Major bleeding and bleeding and no reported no reported raised INRraised INR
1 (<1%)1 (<1%) 3 (<1%)3 (<1%) -- 5 (1%)5 (1%) 7 (1%)7 (1%) --
Major Major bleeding and bleeding and raised INRraised INR
00 4 (<1%)4 (<1%) -- 2 (<1%)2 (<1%) 9 (2%)9 (2%) --
Total major Total major bleedingbleeding 1 (<1%)1 (<1%) 7 (2%)7 (2%) 6.93 6.93
(0.85-56.08, 0.07)(0.85-56.08, 0.07) 7 (1%)7 (1%) 16 (3%)16 (3%) 2.282.28(0.95-5.48, 0.09)(0.95-5.48, 0.09)
Moderate and Moderate and severe raised severe raised INR and no INR and no
major major bleedingbleeding
00 3 (<1%)3 (<1%) -- 1 (<1%)1 (<1%) 12 (3%)12 (3%) --
Minor Minor bleedingbleeding 1 (<1%)1 (<1%) 14 (3%)14 (3%) -- 21 (4%)21 (4%) 24 (5%)24 (5%) --

Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567Young AM et al. Lancet 2009;373:567
WARP: Prophylactic Warfarin Does Not WARP: Prophylactic Warfarin Does Not Reduce Catheter-Associated Thrombosis in CAReduce Catheter-Associated Thrombosis in CA
Combined Combined thrombosis thrombosis and major and major bleeding bleeding eventsevents
Warfarin evaluationWarfarin evaluation Dose evaluationDose evaluation
No No warfarin warfarin (n=404)(n=404)
Warfarin Warfarin (n=408)(n=408)
Relative risk Relative risk (95% CI, p value)(95% CI, p value)
Fixed-Fixed-dose dose
warfarin warfarin (n=471)(n=471)
Dose-Dose-adjusted adjusted warfarin warfarin (n=473)(n=473)
Relative risk Relative risk (95% CI, p value)(95% CI, p value)
Total Total catheter-catheter-related related
thrombosis thrombosis and major and major bleeding bleeding eventsevents
25 (6%)25 (6%) 31 (8%)31 (8%) 1.231.23(0.83-1.52, 0.51)(0.83-1.52, 0.51) 41 (9%)41 (9%) 29 (6%)29 (6%) 0.840.84
(0.74-2.04, 0.17)(0.74-2.04, 0.17)
All thrombotic All thrombotic and major and major bleeding bleeding eventsevents
39 (10%)39 (10%) 37 (9%)37 (9%) 0.940.94(0.61-1.44, 0.87)(0.61-1.44, 0.87) 44 (9%)44 (9%) 42 (9%)42 (9%) 0.95 0.95
(0.64-1.42, 0.89)(0.64-1.42, 0.89)

Tolerability of Low-Dose WarfarinTolerability of Low-Dose Warfarin
► 95 cancer patients receiving FU-based infusion 95 cancer patients receiving FU-based infusion chemotherapy and 1 mg warfarin dailychemotherapy and 1 mg warfarin daily
► INR measured at baseline and four time pointsINR measured at baseline and four time points
► 10% of all recorded INRs >1.510% of all recorded INRs >1.5
► Patients with elevated INRPatients with elevated INR2.0–2.92.0–2.9 6% 6%
3.0–4.93.0–4.9 19%19%
>5.0>5.0 7% 7%
Central Venous Catheters: WarfarinCentral Venous Catheters: Warfarin
Masci et al. Masci et al. J Clin Oncol.J Clin Oncol. 2003;21:736-739 2003;21:736-739

In 10 studies involving more than 1250 cancer patients with In 10 studies involving more than 1250 cancer patients with CVADs vs CA controls:CVADs vs CA controls:
The attributable risk of catheter associated thrombosis The attributable risk of catheter associated thrombosis conferred by:conferred by:
In 10 studies involving more than 1250 cancer patients with In 10 studies involving more than 1250 cancer patients with CVADs vs CA controls:CVADs vs CA controls:
The attributable risk of catheter associated thrombosis The attributable risk of catheter associated thrombosis conferred by:conferred by:
Dentali F et al. JTH 2007; 5(Suppl 2):P-S-564Dentali F et al. JTH 2007; 5(Suppl 2):P-S-564Dentali F et al. JTH 2007; 5(Suppl 2):P-S-564Dentali F et al. JTH 2007; 5(Suppl 2):P-S-564
Influence of Thrombophilia on Thrombotic Influence of Thrombophilia on Thrombotic Complications of CVADs in CancerComplications of CVADs in Cancer
CA + FVL OR=5.18 (95% confidence interval: 3.0-8.8)
CA + G20210A OR=3.95 (95% confidence interval: 1.5-10.6)
FVL 13.5%
G20210A 3.6%

88thth ACCP Consensus Guidelines ACCP Consensus Guidelines
No routine prophylaxis to prevent No routine prophylaxis to prevent thrombosis secondary to central thrombosis secondary to central venous catheters, including LMWH venous catheters, including LMWH (2B) and fixed-dose warfarin (1B)(2B) and fixed-dose warfarin (1B)
Revised 2009 NCCN guidelines Revised 2009 NCCN guidelines diverge from this philosophy diverge from this philosophy
ChestChest Jun 2008: 454S–545S Jun 2008: 454S–545S

Primary Prophylaxis in Cancer RadiotherapyPrimary Prophylaxis in Cancer Radiotherapy The Ambulatory Patient The Ambulatory Patient
► No recommendations from ACCPNo recommendations from ACCP
► No data from randomized trials (RCTs)No data from randomized trials (RCTs)
► Weak data from observational studies in Weak data from observational studies in high risk tumors (e.g. brain tumors; high risk tumors (e.g. brain tumors; mucin-secreting adenocarcinomas: mucin-secreting adenocarcinomas: Colorectal, pancreatic, lung, renal cell, Colorectal, pancreatic, lung, renal cell, ovarian)ovarian)
► Recommendations extrapolated from Recommendations extrapolated from other groups of patients if additional risk other groups of patients if additional risk factors present (e.g., hemiparesis in brain factors present (e.g., hemiparesis in brain tumors, etc.)tumors, etc.)

Risk Factors for VTE inRisk Factors for VTE inMedical Oncology PatientsMedical Oncology Patients
► Tumor typeTumor type● Ovary, brain, pancreas, lung, colonOvary, brain, pancreas, lung, colon
► Stage, grade, and extent of cancerStage, grade, and extent of cancer● Metastatic disease, venous stasis due to Metastatic disease, venous stasis due to
bulky diseasebulky disease
► Type of antineoplastic treatmentType of antineoplastic treatment● Multiagent regimens, hormones,Multiagent regimens, hormones,
anti-VEGF, radiationanti-VEGF, radiation
► Miscellaneous VTE risk factorsMiscellaneous VTE risk factors● Previous VTE, Previous VTE, hospitalization, immobility, hospitalization, immobility,
infection, thrombophiliainfection, thrombophilia

Independent Risk Factors for DVT/PEIndependent Risk Factors for DVT/PE
Risk Factor/CharacteristicRisk Factor/Characteristic O.R.O.R.
Recent surgery with institutionalizationRecent surgery with institutionalization 21.7221.72
TraumaTrauma 12.6912.69
Institutionalization without recent surgeryInstitutionalization without recent surgery 7.987.98
Malignancy with chemotherapyMalignancy with chemotherapy 6.536.53
Prior CVAD or pacemakerPrior CVAD or pacemaker 5.555.55
Prior superficial vein thrombosisPrior superficial vein thrombosis 4.324.32
Malignancy without chemotherapyMalignancy without chemotherapy 4.054.05
Neurologic disease w/ extremity paresisNeurologic disease w/ extremity paresis 3.043.04
Serious liver diseaseSerious liver disease 0.100.10
Heit JA et al. Heit JA et al. Thromb HaemostThromb Haemost. 2001;86:452-463. 2001;86:452-463

VTE Incidence In Various TumorsVTE Incidence In Various Tumors
Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17
Oncology SettingOncology Setting VTE VTE IncidenceIncidence
Breast cancer (Stage I & II) w/o further treatmentBreast cancer (Stage I & II) w/o further treatment 0.2%0.2%
Breast cancer (Stage I & II) w/ chemoBreast cancer (Stage I & II) w/ chemo 2%2%
Breast cancer (Stage IV) w/ chemoBreast cancer (Stage IV) w/ chemo 8%8%
Non-Hodgkin’s lymphomas w/ chemoNon-Hodgkin’s lymphomas w/ chemo 3%3%
Hodgkin’s disease w/ chemoHodgkin’s disease w/ chemo 6%6%
Advanced cancer (1-year survival=12%)Advanced cancer (1-year survival=12%) 9%9%
High-grade gliomaHigh-grade glioma 26%26%
Multiple myeloma (thalidomide + chemo)Multiple myeloma (thalidomide + chemo) 28%28%
Renal cell carcinoma Renal cell carcinoma 43%43%
Solid tumors (anti-VEGF + chemo)Solid tumors (anti-VEGF + chemo) 47%47%
Wilms tumor (cavoatrial extension) Wilms tumor (cavoatrial extension) 4%4%

PrimaryPrimary VTE Prophylaxis VTE Prophylaxis
► Recommended for hospitalized Recommended for hospitalized cancer patientscancer patients
► Not universally recommended for Not universally recommended for outpatients, but there are exceptionsoutpatients, but there are exceptions● New data for certain agentsNew data for certain agents● Heterogeneous populationHeterogeneous population
Need for risk stratificationNeed for risk stratification

Naluri SR et al. JAMA. 2008;300:2277Naluri SR et al. JAMA. 2008;300:2277
VTE Risk with Bevacizumab in Colorectal Cancer VTE Risk with Bevacizumab in Colorectal Cancer Approaches Risk of Antiangiogenesis in MyelomaApproaches Risk of Antiangiogenesis in Myeloma
All-Grade Venous All-Grade Venous Thromboembolism, Thromboembolism,
No./Total No.No./Total No.
Tumor TypeTumor Type No. of No. of StudiesStudies BevacizumabBevacizumab ControlControl Incidence Incidence
(95% CI), %(95% CI), %RR (95% RR (95%
CI)CI)
OverallOverall 66 155/1196155/1196 107/1083107/1083 11.9 11.9 (6.8-19.9)(6.8-19.9)
1.29 1.29 (1.03-1.63)(1.03-1.63)
Colorectal Colorectal cancercancer 33 108/564108/564 85/53285/532 19.1 19.1
(16.1-22.6)(16.1-22.6)1.19 1.19
(0.92-1.55)(0.92-1.55)
NSCLCNSCLC 11 10/6610/66 3/323/32 14.9 14.9 (8.2-25.5)(8.2-25.5)
1.59 1.59 (0.47-5.37)(0.47-5.37)
Breast Breast cancercancer 11 17/22917/229 12/21512/215 7.3 7.3
(4.6-11.5)(4.6-11.5)1.30 1.30
(0.64-2.67)(0.64-2.67)
Renal cell Renal cell carcinomacarcinoma 11 20/33720/337 6/3046/304 3.0 3.0
(1.6-5.5)(1.6-5.5)3.00 3.00
(1.23-7.33)(1.23-7.33)

Naluri SR et al. JAMA.Naluri SR et al. JAMA. 2008;300:2277 2008;300:2277
Bevacizumab Increases Risk of Bevacizumab Increases Risk of Symptomatic VTE by 33% vs ControlsSymptomatic VTE by 33% vs Controls

Knight: N Engl J Med.2006,354:2079Knight: N Engl J Med.2006,354:2079
► rEPO used rEPO used more in USA more in USA and Canadaand Canada
► L+Dex:L+Dex: 23% 23% VTE with EPO VTE with EPO vs 5% w/o vs 5% w/o EPOEPO
► Placebo + Dex:Placebo + Dex: 7% VTE with 7% VTE with EPO vs 1% EPO vs 1% without EPOwithout EPO
Incidence of VTE: USA and Canada Greater Incidence of VTE: USA and Canada Greater than Israel, Australia, and Europethan Israel, Australia, and Europe
Multivariate Analysis of the Risk of Thrombosis Associated Multivariate Analysis of the Risk of Thrombosis Associated with Lenalidomide plus High-Dose Dexamethasone and with Lenalidomide plus High-Dose Dexamethasone and Concomitant Erythropoietin for the Treatment of Multiple Concomitant Erythropoietin for the Treatment of Multiple Myeloma Myeloma
TreatmentTreatment Odds RatioOdds Ratio P ValueP Value(95% CI)(95% CI)
Lenalidomide plusLenalidomide plus 3.51 (1.77-6.97)3.51 (1.77-6.97) <0.001<0.001High-dose dexamethasoneHigh-dose dexamethasone
Concomitant erythropoietin Concomitant erythropoietin 3.21 (1.72-6.01)3.21 (1.72-6.01) <0.001<0.001

Oral Anticoagulant TherapyOral Anticoagulant Therapyin Cancer Patients: Problematicin Cancer Patients: Problematic
► Warfarin therapy is complicated by:Warfarin therapy is complicated by:
● Difficulty maintaining tight therapeutic control, due Difficulty maintaining tight therapeutic control, due to anorexia, vomiting, drug interactions, etc. to anorexia, vomiting, drug interactions, etc.
● Frequent interruptions for thrombocytopenia and Frequent interruptions for thrombocytopenia and proceduresprocedures
● Difficulty in venous access for monitoringDifficulty in venous access for monitoring● Increased risk of both recurrence and bleedingIncreased risk of both recurrence and bleeding
► Is it reasonable to substitute long-term LMWH Is it reasonable to substitute long-term LMWH for warfarin ? When? How? Why?for warfarin ? When? How? Why?

CLOT: Landmark Cancer/VTE TrialCLOT: Landmark Cancer/VTE Trial
[N = 677] [N = 677]
► Primary Endpoints:Primary Endpoints: Recurrent VTE and Bleeding Recurrent VTE and Bleeding► Secondary EndpointSecondary Endpoint:: Survival Survival
Lee, Levine, Kakkar, Rickles et.al. Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146
Dalteparin Dalteparin
Dalteparin Oral Anticoagulant
CANCER PATIENTS WITH
ACUTE DVT or PERandomization

Landmark CLOT Cancer TrialLandmark CLOT Cancer TrialReduction in Recurrent VTEReduction in Recurrent VTE
00
55
1010
1515
2020
2525
Days Post RandomizationDays Post Randomization
00 3030 6060 9090 120120 150150 180180 210210
Pro
bab
ility
of R
ecu
rre
nt V
TE
, %P
roba
bili
ty o
f Re
curr
en
t VT
E, % Risk reduction = 52%Risk reduction = 52%
pp-value = 0.0017-value = 0.0017
DalteparinDalteparin
OACOAC
Recurrent VTERecurrent VTE
Lee, Levine, Kakkar, Rickles et.al. Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

DalteparinDalteparin N=338N=338
OACOACN=335N=335
P-value*P-value*
Major bleedMajor bleed 19 ( 5.6%) 19 ( 5.6%) 12 ( 3.6%)12 ( 3.6%) 0.270.27
Any bleedAny bleed 46 (13.6%)46 (13.6%) 62 (18.5%)62 (18.5%) 0.0930.093
* Fisher’s exact test* Fisher’s exact test
Bleeding Events in CLOTBleeding Events in CLOT
Lee, Levine, Kakkar, Rickles et.al. Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, N Engl J Med, 2003;349:1462003;349:146

Treatment of Cancer-Associated VTETreatment of Cancer-Associated VTE
StudyStudy DesignDesignLength of Length of TherapyTherapy(Months)(Months)
NNRecurrent Recurrent
VTE VTE (%)(%)
Major Major BleedingBleeding
(%)(%)
DeathDeath(%)(%)
CLOT TrialCLOT Trial(Lee 2003)(Lee 2003)
DalteparinDalteparinOACOAC
6 6 336336336336
991717
6644
39394141
CANTHENOXCANTHENOX(Meyer 2002)(Meyer 2002)
EnoxaparinEnoxaparinOACOAC
3367677171
11112121
771616
11112323
LITELITE(Hull ISTH 2003)(Hull ISTH 2003)
TinzaparinTinzaparinOACOAC
3380808787
661111
6688
23232222
ONCENOXONCENOX(Deitcher ISTH (Deitcher ISTH 2003)2003)
Enox (Low)Enox (Low)Enox (High)Enox (High)OACOAC
66323236363434
3.43.43.13.16.76.7
NS
NS0.03
NS
NS0.002
NS
NS
NR
0.09 0.030.09

Treatment and 2Treatment and 2° Prevention of VTE ° Prevention of VTE in Cancer – Bottom Linein Cancer – Bottom Line
► New standard of care is LMWH at therapeutic doses New standard of care is LMWH at therapeutic doses for a for a minimum of 3-6 months (Grade 1A minimum of 3-6 months (Grade 1A recommendation—ACCP) recommendation—ACCP)
► NOTE: Dalteparin is only LMWH approved (May, NOTE: Dalteparin is only LMWH approved (May, 2007) for both the 2007) for both the treatment and secondary preventiontreatment and secondary prevention of VTE in cancer (NCCN preferred agent)of VTE in cancer (NCCN preferred agent)
► Oral anticoagulant therapy to follow for as long as Oral anticoagulant therapy to follow for as long as cancer is active (Grade 1C recommendation—ACCP)cancer is active (Grade 1C recommendation—ACCP)
ChestChest Jun 2008: 454S–545S Jun 2008: 454S–545S
New DevelopmentNew Development

CLOT 12-month MortalityCLOT 12-month MortalityAll PatientsAll Patients
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100
00 3030 6060 9090 120120 180180 240240 300300 360360
DalteparinDalteparin
OACOAC
HR 0.94 P-value = 0.40HR 0.94 P-value = 0.40
Days Post RandomizationDays Post Randomization
Pro
bab
ility
of S
urv
iva
l, %
Pro
bab
ility
of S
urv
iva
l, %
Lee AY et al. Lee AY et al. J Clin Oncol. J Clin Oncol. 2005; 23:2123-9.2005; 23:2123-9.

00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100
Days Post RandomizationDays Post Randomization00 3030 6060 9090 120120 150150 180180 240240 300300 360360
Pro
bab
ility
of S
urv
iva
l, %
Pro
bab
ility
of S
urv
iva
l, %
OACOAC
DalteparinDalteparin
HR = 0.50 P-value = 0.03HR = 0.50 P-value = 0.03
Anti-Tumor Effects of LMWHAnti-Tumor Effects of LMWHCLOT 12-month MortalityCLOT 12-month Mortality
Patients Without Metastases (N=150)Patients Without Metastases (N=150)
Lee AY et al. Lee AY et al. J Clin Oncol. J Clin Oncol. 2005; 23:2123-9.2005; 23:2123-9.

LMWH Influences Survival of Patients with LMWH Influences Survival of Patients with Advanced Solid Tumor MalignanciesAdvanced Solid Tumor Malignancies
<6 mos anticipated survival<6 mos anticipated survival >6 mos anticipated survival>6 mos anticipated survival
6 wks LMWH immediately post diagnosis of CA-no initial chemo 6 wks LMWH immediately post diagnosis of CA-no initial chemo 6 wks LMWH immediately post diagnosis of CA-no initial chemo 6 wks LMWH immediately post diagnosis of CA-no initial chemo
Klerk, C. P.W. et al. J Clin Oncol; 23:2130-2135 2005Klerk, C. P.W. et al. J Clin Oncol; 23:2130-2135 2005Klerk, C. P.W. et al. J Clin Oncol; 23:2130-2135 2005Klerk, C. P.W. et al. J Clin Oncol; 23:2130-2135 2005

► 84 patients randomized: Chemo +/- LMWH (18 weeks)84 patients randomized: Chemo +/- LMWH (18 weeks)
► Patients balanced for age, gender, stage, smoking Patients balanced for age, gender, stage, smoking history, ECOG performance statushistory, ECOG performance status
LMWH for Small Cell Lung CancerLMWH for Small Cell Lung CancerTurkish StudyTurkish Study
Altinbas et al. J Thromb Haemost 2004;2:1266.Altinbas et al. J Thromb Haemost 2004;2:1266.
ChemotherapyChemotherapyplus Dalteparinplus Dalteparin Chemo aloneChemo alone P-valueP-value
1-y overall survival, %1-y overall survival, % 51.351.3 29.529.5 0.010.01
2-y overall survival, %2-y overall survival, % 17.217.2 0.00.0 0.010.01
Median survival, mMedian survival, m 13.013.0 8.08.0 0.010.01
CEV = cyclophosphamide, epirubicin, vincristine; CEV = cyclophosphamide, epirubicin, vincristine; LMWH = Dalteparin, 5000 units dailyLMWH = Dalteparin, 5000 units daily

VTE Prophylaxis Is Underused VTE Prophylaxis Is Underused in Patients With Cancer in Patients With Cancer
1.Kakkar AK et al. Oncologist. 2003;8:381-3882.Stratton MA et al. Arch Intern Med. 2000;160:334-3403.Bratzler DW et al. Arch Intern Med. 1998;158:1909-1912
Cancer:Cancer:FRONTLINE SurveyFRONTLINE Survey11— — 3891 Clinician 3891 Clinician RespondentsRespondents
Rat
e of
App
ropr
iate
Pro
phyl
axis
, %R
ate
of A
ppro
pria
te P
roph
ylax
is, %
Major Major SurgerySurgery22
Major Major Abdominothoracic Abdominothoracic Surgery (Elderly)Surgery (Elderly)33 Medical Medical
InpatientsInpatients44
Confirmed DVT Confirmed DVT (Inpatients)(Inpatients)55
Cancer: Cancer: SurgicalSurgical
Cancer: Cancer: MedicalMedical
4.Rahim SA et al. Thromb Res. 2003;111:215-2195.Goldhaber SZ et al. Am J Cardiol. 2004;93:259-262

Conclusions and SummaryConclusions and Summary
► Risk factors for VTE in the setting of cancer have Risk factors for VTE in the setting of cancer have been well characterized: solid tumors, chemotherapy, been well characterized: solid tumors, chemotherapy, surgery, thrombocytopeniasurgery, thrombocytopenia
► Long-term secondary prevention with LMWH has Long-term secondary prevention with LMWH has been shown to produce better outcomes than warfarinbeen shown to produce better outcomes than warfarin
► Guidelines and landmark trials support administration Guidelines and landmark trials support administration of LMWH in at risk patientsof LMWH in at risk patients
► Cancer patients are under-prophylaxed for VTECancer patients are under-prophylaxed for VTE
► Health system pharmacists can play a pivotal role in Health system pharmacists can play a pivotal role in improving clinical outcomes in this patient populationimproving clinical outcomes in this patient population

Pharmacologic Prophylaxis of Pharmacologic Prophylaxis of DVT in Special PopulationsDVT in Special Populations
Edith Nutescu, PharmD, FCCPClinical Associate Professor
Pharmacy PracticeAffiliate Faculty, Center for
Pharmacoeconomic ResearchDirector, Antithrombosis Center
The University of Illinois at Chicago College of Pharmacy & Medical Center
Chicago, IL
Edith Nutescu, PharmD, FCCPClinical Associate Professor
Pharmacy PracticeAffiliate Faculty, Center for
Pharmacoeconomic ResearchDirector, Antithrombosis Center
The University of Illinois at Chicago College of Pharmacy & Medical Center
Chicago, IL
Mechanisms ● Mortality ● TherapeuticsMechanisms ● Mortality ● Therapeutics

ObjectivesObjectives
1.1. Differentiate data with various LMWHs in special Differentiate data with various LMWHs in special populationspopulations
2.2. Review appropriate dosing and monitoring of Review appropriate dosing and monitoring of LMWHs in patients with obesity and renal failureLMWHs in patients with obesity and renal failure

Risk of Inadequate Therapy Risk of Inadequate Therapy in High Risk Patientsin High Risk Patients
► 524 VTE Patients524 VTE Patients● Active Cancer in 26%Active Cancer in 26%
• Only 1/3Only 1/3rdrd on LMWH monotherapy on LMWH monotherapy
● Weight > 100Kg in 15%Weight > 100Kg in 15%• Under-dosing of LMWH by > 10%Under-dosing of LMWH by > 10%
– 36% of > pts 100Kg36% of > pts 100Kg– 8% of pts < 100Kg (p < 0.001)8% of pts < 100Kg (p < 0.001)
● CrCL < 30mL/min in 5%CrCL < 30mL/min in 5%• LMWH tx in 67%LMWH tx in 67%
Cook LM, et.al. J Thromb Hemost 2007;5;937-41.Cook LM, et.al. J Thromb Hemost 2007;5;937-41.

88thth ACCP Conference on ACCP Conference on Antithrombotic TherapyAntithrombotic Therapy
““In obese patients given LMWH prophylaxis or In obese patients given LMWH prophylaxis or treatment, we suggest weight-based dosing treatment, we suggest weight-based dosing (Grade 2C).”(Grade 2C).”
► What is this weight-based dosing and how does it differ What is this weight-based dosing and how does it differ from typical dosing?from typical dosing?
► At what weight do we move away from standard dosing At what weight do we move away from standard dosing and move to weight-based dosing?and move to weight-based dosing?
Hirsh J et al. Hirsh J et al. ChestChest. 2008;133(suppl):141S-159S.. 2008;133(suppl):141S-159S.
Obese PatientsObese Patients

Pharmacokinetic Characteristics of Pharmacokinetic Characteristics of Low Molecular Weight HeparinsLow Molecular Weight Heparins
Lipid solubilityLipid solubility LOWLOW
Plasma protein bindingPlasma protein binding HIGHHIGH
Tissue bindingTissue binding LOWLOW
Volume of distributionVolume of distribution 5-7 L5-7 L
Logical conclusion:Logical conclusion:IBW may be a better predictor of LMWH dosing than TBWIBW may be a better predictor of LMWH dosing than TBW

LMWH: Maximum Weights StudiedLMWH: Maximum Weights Studied
* max dose 18,000 - 20,000 IU/day * max dose 18,000 - 20,000 IU/day
Duplaga BA et al. Pharmacotherapy 2001; 21:218-34.Duplaga BA et al. Pharmacotherapy 2001; 21:218-34.Synergy Trial: Data on File Synergy Trial: Data on File Davidson, et al. J Thromb Haem 2007;5:1191-4Davidson, et al. J Thromb Haem 2007;5:1191-4
Kinetic Kinetic StudiesStudies Clinical TrialsClinical Trials
DalteparinDalteparin 190 kg190 kg 128 kg*128 kg*
EnoxaparinEnoxaparin 144 kg144 kg 194 kg194 kg
TinzaparinTinzaparin 165 kg165 kg 88 kg88 kg
FondaparinuxFondaparinux 175.5 kg175.5 kg

LMWH Pharmacokinetics in ObesityLMWH Pharmacokinetics in Obesity
Actual body weight correlates best with anticoagulant response to Actual body weight correlates best with anticoagulant response to LMWHs as measured by anti-factor Xa levelsLMWHs as measured by anti-factor Xa levels
Clin Pharmacol Ther 2002;72:308-18. Thromb Haemost 2002;87:817-23.Clin Pharmacol Ther 2002;72:308-18. Thromb Haemost 2002;87:817-23.

DalteparinDalteparinPharmacokinetics in Obesity Pharmacokinetics in Obesity
Yee JYV, Duffull SB. Yee JYV, Duffull SB. Eur J Clin PharmacolEur J Clin Pharmacol 2000; 56:293-7. 2000; 56:293-7.
Dose: 200 U/kg qdDuration: routine
Obese (BMI > 30)Obese (BMI > 30) Normal (BMI < 30)Normal (BMI < 30)
NN 1010 1010
TBW (mean +/- SD)TBW (mean +/- SD) 106.4 +/- 22.1106.4 +/- 22.1 69.7 +/- 9.369.7 +/- 9.3
LBW (mean +/- SD)LBW (mean +/- SD) 64.1 +/- 12.364.1 +/- 12.3 66.1 +/- 8.766.1 +/- 8.7
Mean Vd (l)Mean Vd (l) 12.3912.39 8.368.36
Mean CI (l/hr)Mean CI (l/hr) 1.301.30 1.111.11

DalteparinDalteparinPharmacokinetics In Obesity Pharmacokinetics In Obesity
Correlation Coefficient Between Vd and:Correlation Coefficient Between Vd and:
LBWLBW 0.050.05
ABWABW 0.520.52
TBWTBW 0.550.55
Correlation Coefficient Between Cl and:Correlation Coefficient Between Cl and:
LBWLBW 0.010.01
ABWABW 0.320.32
TBWTBW 0.390.39
Conclusion:Conclusion:TBW may be a better predictor of LMWH dose than IBWTBW may be a better predictor of LMWH dose than IBW
Yee JYV et al. Yee JYV et al. Eur J Clin PharmacolEur J Clin Pharmacol 2000; 56:293-7. 2000; 56:293-7.

Conclusion: Body mass does not appear to have an important effect on the Conclusion: Body mass does not appear to have an important effect on the response to LMWH up to a weight of 190kg in patients with normal renal function.response to LMWH up to a weight of 190kg in patients with normal renal function.
DalteparinDalteparinPharmacokinetics In Obesity Pharmacokinetics In Obesity
Dose: 200 U/kg qdDuration: 5 DaysMax TBW: 190kg
<20% of <20% of IBWIBW
20-40% of 20-40% of IBWIBW
> 40% of > 40% of IBWIBW
NN 1313 1414 1010
Mean Dose (U)Mean Dose (U) 14,03014,030 17,64617,646 23,56523,565
Ant-Xa Activity (u/ml)Ant-Xa Activity (u/ml)
Day 3 PeakDay 3 Peak 1.011.01 0.970.97 1.12 NS1.12 NS
Day 3 TroughDay 3 Trough 0.120.12 0.110.11 0.11 NS0.11 NS
Wilson SJ et al. Wilson SJ et al. HemostasisHemostasis 2001; 31:42-8. 2001; 31:42-8.

LMWH Safety and Effectiveness Using TBWLMWH Safety and Effectiveness Using TBWEnoxaparin In ACS (ESSENCE/TIMI IIb)Enoxaparin In ACS (ESSENCE/TIMI IIb)
14.3%14.3%
16.1%16.1%
P=0.39P=0.39
P=0.13P=0.13
Obese: BMI Obese: BMI >> 30mg/m2 30mg/m2Enoxaparin max weight 158 kgEnoxaparin max weight 158 kg
Spinler SA et al. Spinler SA et al. Am Heart JAm Heart J 2003; 146:33-41 2003; 146:33-41
0.4%0.4%1.6%1.6%

Safety Of TBW-based Dosing of DalteparinSafety Of TBW-based Dosing of Dalteparinfor Treatment of Acute VTE in Obese Patientsfor Treatment of Acute VTE in Obese Patients
Al-Yaseen E et al. Al-Yaseen E et al. J Thromb HaemostJ Thromb Haemost 2004; 3:100-2. 2004; 3:100-2.
N = 193 patients N = 193 patients 3 month outcomes: major bleeding = 1.0% (n=2)3 month outcomes: major bleeding = 1.0% (n=2) > 90 kg> 90 kg recurrent VTE = 1.6% (n=3) recurrent VTE = 1.6% (n=3)
WEIGHTWEIGHT(kg) (kg) NN
MeanMeanDoseDose
Full dose Full dose +/- 5%+/- 5%
QD QD DosingDosing
BIDBIDDosingDosing
90-9990-99 4040 19,30019,300 3939 2424 1616
100-109100-109 5252 20,85020,850 4949 2525 1717
110-119110-119 4141 21,47021,470 2121 2626 1515
120-129120-129 2525 24,30024,300 2222 1616 99
130-139130-139 1616 25,25025,250 88 1010 66
140-149140-149 99 26,92026,920 66 55 44
>> 150 150 1010 28,28028,280 66 66 44

Fondaparinux In ObesityFondaparinux In ObesityResults From the Matisse TrialsResults From the Matisse Trials
Davidson BL et al. Davidson BL et al. J Thrombosis HaemostJ Thrombosis Haemost 2007; 5:1191-4. 2007; 5:1191-4.
Fondaparinux:Fondaparinux:< 50kg: 5mg qd< 50kg: 5mg qd50-100kg: 7.5mg qd50-100kg: 7.5mg qd> 100kg: 10mg qd> 100kg: 10mg qd
Enoxaparin: Enoxaparin: ((Matisse DVT)Matisse DVT)1mg/kg q12h1mg/kg q12h
Heparin:Heparin:(Matisse PE)(Matisse PE)Adjusted per aPTT Adjusted per aPTT
No weight-dependentdifference in efficacy or safety

Body Weight and Anti-Xa ActivityBody Weight and Anti-Xa Activityfor Prophylactic Doses of LMWHfor Prophylactic Doses of LMWH
N = 17 patients and 2 volunteersN = 17 patients and 2 volunteersEnoxaparin 40mg SQ x1 doseEnoxaparin 40mg SQ x1 doseAntiXa levels hourly x10 hoursAntiXa levels hourly x10 hours
Frederiksen SG et al. Frederiksen SG et al. Br J SurgeryBr J Surgery 2003; 90:547-8 2003; 90:547-8
40 60 80 100 120 140 16040 60 80 100 120 140 160
Body Weight (kg)Body Weight (kg)
Are
a un
der
the
curv
e fo
r 10
hA
rea
unde
r th
e cu
rve
for
10 h 200
150
100
50
0
200
150
100
50
0
Regression line95% CI for line95% CI for data points
Regression line95% CI for line95% CI for data points

Kucher N et al. Kucher N et al. Arch Int MedArch Int Med 2005;165:341-5. 2005;165:341-5.
0.010.01 0.10.1 0.55 0.55 1.01.0 10.010.0
Favors Dalteparin Favor Placebo Favors Dalteparin Favor Placebo
Relative RiskRelative Risk
< 25 37.5< 25 37.525-29.925-29.9 33.1 33.130-34.930-34.9 18.9 18.935-39.935-39.9 7.1 7.1>> 40 3.3 40 3.3
Overall Prevent TrialOverall Prevent Trial
DalteparinDalteparinFixed Dosing For VTE PreventionFixed Dosing For VTE Prevention
Subgroup analysis of PREVENT TRIAL (dalteparin vs placebo in medically ill)Subgroup analysis of PREVENT TRIAL (dalteparin vs placebo in medically ill)
BMI (kg/m2) Patients %BMI (kg/m2) Patients %
Dalteparin 5,000 units daily was similarly effective in obese and non-obese patients (except Dalteparin 5,000 units daily was similarly effective in obese and non-obese patients (except patients with BMI>40) with no observed difference in mortality or major bleedingpatients with BMI>40) with no observed difference in mortality or major bleeding

Enoxaparin VTE Prophylaxis in Enoxaparin VTE Prophylaxis in TKA/THA/TraumaTKA/THA/Trauma
Samama MM et alSamama MM et al. Thromb Haemost . Thromb Haemost 1995; 73:977.1995; 73:977.
N: 807 Dose: 40 mg qd Obese : BMI>32kg/mN: 807 Dose: 40 mg qd Obese : BMI>32kg/m22
31.8%31.8%
16.7%16.7%
p<0.001p<0.001

Enoxaparin: Enoxaparin: VTE Prophylaxis in Bariatric SurgeryVTE Prophylaxis in Bariatric Surgery
Scholten Obes Surg 2002; 12:19-24.Scholten Obes Surg 2002; 12:19-24.
30mg bid: n=9230mg bid: n=92BMI 51.7kg/mBMI 51.7kg/m22
5.4%5.4%
0.6%0.6%
p<0.01p<0.01
40mg bid: n=38940mg bid: n=389BMI 50.3kg/mBMI 50.3kg/m22

Anti-factor Xa levelAnti-factor Xa level Number of patient Number of patient (%)(%) Body weight (kg)Body weight (kg)
Below target value (<0.2 UI/ml)Below target value (<0.2 UI/ml) 41 (30.4%)41 (30.4%) 159.4 ± 35.8159.4 ± 35.8
Target value (0.2–0.5 UI/ml)Target value (0.2–0.5 UI/ml) 81 (60.0%)81 (60.0%) 145.7 ± 28.4145.7 ± 28.4
Above target value (>0.5 UI/ml)Above target value (>0.5 UI/ml) 13 (9.6%)13 (9.6%) 134.6 ± 24.2134.6 ± 24.2
pp value value 0.0152 0.0152
N=135N=135Bariatric SurgeryBariatric SurgeryMean Weight: 148.8KgMean Weight: 148.8KgMean BMI: 53.7Mean BMI: 53.7Dalteparin: 7,500 IU dailyDalteparin: 7,500 IU daily
Dalteparin in Morbid Obesity: Bariatric SurgeryDalteparin in Morbid Obesity: Bariatric Surgery
Simonneau MD, et.al. Obes Surg. 2008; [Epub ahead of print] Simonneau MD, et.al. Obes Surg. 2008; [Epub ahead of print]
P=0.031P=0.031
P=0.052P=0.052P=0.444P=0.444
Under target value<0.2 IU/mL
n-=41
Under target value<0.2 IU/mL
n-=41
Target value<0.2-0.5 IU/mL
n-=81
Target value<0.2-0.5 IU/mL
n-=81
Over target value<>0.5 IU/mL
n=13
Over target value<>0.5 IU/mL
n=13
200
180
160
140
120
0
200
180
160
140
120
0B
ody
Wei
ght
(kg)
Bod
y W
eigh
t (k
g)

LMWH in Obesity: Summary LMWH in Obesity: Summary
► Treatment: Treatment: in controlled trials, LMWH dosing has been based on TBW in controlled trials, LMWH dosing has been based on TBW (max 160-190 kg)(max 160-190 kg)
● DalteparinDalteparin • Dose based on TBWDose based on TBW• PI recommends dose capping PI recommends dose capping • Recent clinical data supports TBW dosingRecent clinical data supports TBW dosing
– QD or BID dosing QD or BID dosing
● EnoxaparinEnoxaparin• Dose based on TBWDose based on TBW• Dose capping NOT recommendedDose capping NOT recommended• BID dosing preferredBID dosing preferred
● TinzaparinTinzaparin • Dose based on TBW, NO dose adjustment or cappingDose based on TBW, NO dose adjustment or capping
● Anti-Xa monitoring not necessary for TBW < 190kgAnti-Xa monitoring not necessary for TBW < 190kg► Prophylaxis: Prophylaxis: a 25-30% dose increase (a 25-30% dose increase (or 50IU/kg in high risk patientsor 50IU/kg in high risk patients))
Nutescu E, et.al. Ann Pharmacother; 2009; 43(6):1064-83.Nutescu E, et.al. Ann Pharmacother; 2009; 43(6):1064-83.

88thth ACCP Conference on Antithrombotic Therapy ACCP Conference on Antithrombotic TherapyRenal ImpairmentRenal Impairment
► For each of the antithrombotic agents, we recommend that For each of the antithrombotic agents, we recommend that clinicians follow manufacturer-suggested dosing guidelines clinicians follow manufacturer-suggested dosing guidelines (Grade 1C)(Grade 1C)
► We recommend that renal function be considered when We recommend that renal function be considered when making decisions about the use of and/or dose of LMWH or making decisions about the use of and/or dose of LMWH or fondaparinux (Grade 1A)fondaparinux (Grade 1A)
► Options for patients with renal impairment (Grade 1B)Options for patients with renal impairment (Grade 1B)
● Avoid agents that renal accumulateAvoid agents that renal accumulate● Use a lower doseUse a lower dose● Monitor the drug level or anticoagulant effectMonitor the drug level or anticoagulant effect
Geerts WH. Geerts WH. ChestChest 2008;133(suppl):381S-453S. 2008;133(suppl):381S-453S.

LMWH in Renal DysfunctionLMWH in Renal DysfunctionManufacturer RecommendationsManufacturer Recommendations
DalteparinDalteparin● ““should be should be used with cautionused with caution in patients with severe kidney in patients with severe kidney
insufficiency.”insufficiency.”• Monitor anti-Factor Xa for dose guiding with therapeutic dosesMonitor anti-Factor Xa for dose guiding with therapeutic doses
EnoxaparinEnoxaparin● ““adjustment of dose is adjustment of dose is recommendedrecommended for patients with severe for patients with severe
renal impairment (CrCL < 30 mL/min).”renal impairment (CrCL < 30 mL/min).”
TinzaparinTinzaparin● ““patients with severe renal impairment should be dosed patients with severe renal impairment should be dosed with with
cautioncaution.”.”
FondaparinuxFondaparinux- Contraindicated in CrCL < 30mL/min- Contraindicated in CrCL < 30mL/min

Study; yearStudy; yearPatients w/ Patients w/ renal insuff. renal insuff.
(n/n)(n/n)
Patients w/ no Patients w/ no renal insuff.renal insuff.
(n/n)(n/n)
Peto ORPeto OR(95%, CI)(95%, CI)
Weight Weight (%)(%)
Peto ORPeto OR(95%, CI)(95%, CI)
Collet, et al; 2001Collet, et al; 2001 0/280/28 1/831/83 2.012.01 0.26 (0.00 – 23.94)0.26 (0.00 – 23.94)Paulas, et al; 2002Paulas, et al; 2002 0/510/51 3/1493/149 6.026.02 0.26 (0.02 – 3.50)0.26 (0.02 – 3.50)Siguret, et al; 2000Siguret, et al; 2000 0/170/17 0/130/13 Not estimableNot estimable
Chow, et al; 2003Chow, et al; 2003 0/50/5 0/130/13 Not estimableNot estimable
Khazan, et al. (adj.); 2003Khazan, et al. (adj.); 2003 0/100/10 3/423/42 4.784.78 0.28 (0.01 – 5.16)0.28 (0.01 – 5.16)(Prophylactic) 2003(Prophylactic) 2003 3/363/36 3/473/47 14.7714.77 1.33 (0.25 – 7.05)1.33 (0.25 – 7.05)(Therapeutic) 2003(Therapeutic) 2003 2/172/17 3/613/61 8.628.62 3.09 (0.35 – 27.31)3.09 (0.35 – 27.31)
Spinler, et al; 2003Spinler, et al; 2003 5/695/69 74/3,43274/3,432 15.9315.93 10.05 (2.02 – 49.98)10.05 (2.02 – 49.98)
Green, et al; 2005Green, et al; 2005 1/181/18 0/200/20 2.662.66 8.26 (0.16 – 418.42)8.26 (0.16 – 418.42)
Kruse & Lee; 2004Kruse & Lee; 2004 0/500/50 1/1201/120 2.222.22 0.24 (0.00 – 17.90)0.24 (0.00 – 17.90)
Macie, et al; 2004Macie, et al; 2004 2/72/7 6/2016/201 2.682.68 977.78 (19.61 – 48,752.07)977.78 (19.61 – 48,752.07)
Peng, et al; 2004Peng, et al; 2004 0/70/7 0/430/43 Not estimableNot estimable
Thorevska, et al; 2004Thorevska, et al; 2004 7/657/65 11/17111/171 35.5635.56 1.85 (0.63 – 5.40)1.85 (0.63 – 5.40)
Bazinet, et al; 2005Bazinet, et al; 2005 1/361/36 2/1602/160 4.754.75 2.74 (0.15 – 51.73)2.74 (0.15 – 51.73)
Total (95%, CI)Total (95%, CI) 21/41621/416 107/4,555107/4,555 100.00100.00 2.25 (1.19 – 4.27)2.25 (1.19 – 4.27)
Recent Meta-Analysis of LMWHs and Bleeding Recent Meta-Analysis of LMWHs and Bleeding In Patients With Severe Renal DysfunctionIn Patients With Severe Renal Dysfunction
Lim W, et al. Lim W, et al. Ann Intern Med.Ann Intern Med. 2006;144:673-684. 2006;144:673-684.
Dosage adjustmentsDosage adjustmentsfor renal dysfunctionfor renal dysfunction
0.010.01 0.1 0.1 11 1010 100100
Favors ↓’edFavors ↓’ed Favors ↑’edFavors ↑’edbleeding bleeding

Sanderink GJCM. Thromb Res 2002;105:225-31.Sanderink GJCM. Thromb Res 2002;105:225-31.
Enoxaparin PK and PD in Renal ImpairmentEnoxaparin PK and PD in Renal Impairment
Result:Tmax: 3-4 hoursAmax: 10-35% higher in RI groupsCI/F linearly correlated with CrCl
Result:Tmax: 3-4 hoursAmax: 10-35% higher in RI groupsCI/F linearly correlated with CrCl
Day 4Day 4 CL/FCL/F(L/h)(L/h)
Half-lifeHalf-life(h)(h)
AUC (0-24)AUC (0-24)(h●IU/mL)(h●IU/mL)
NormalsNormals 0.980.98 6.876.87
Mild RIMild RI 0.870.87 9.949.94 20% ↑20% ↑
Moderate RIModerate RI 0.760.76 11.311.3 21% ↑21% ↑
Severe RISevere RI 0.580.58 15.915.9 65% ↑65% ↑

LMWH Renal Dosing in NSTE ACS PatientsLMWH Renal Dosing in NSTE ACS Patients
► 56 UA pts with CrCl <60 ml/min56 UA pts with CrCl <60 ml/min
► Enoxaparin dose empirically Enoxaparin dose empirically and and anti-Xa level measured after 3anti-Xa level measured after 3rdrd dosedose
CrClCrCl (ml/min)(ml/min)
<30 <30 (n = 28)(n = 28)
>30 and <60>30 and <60 (n =28)(n =28)
AgeAge 76+/-376+/-3 73+/-373+/-3
Enoxaparin (mg/kg/12h)Enoxaparin (mg/kg/12h) 0.640.64 0.840.84
Anti-Xa (IU/ml)Anti-Xa (IU/ml) 0.950.95 0.950.95
Collet JP et al. International J Cardiol 2001;80:81-2.Collet JP et al. International J Cardiol 2001;80:81-2.
• Dose may be Dose may be to 0.6mg/kg/ q12h if to 0.6mg/kg/ q12h if CrCL <30mL/min; or 0.8 mg/kg/q12h if CrCL <30mL/min; or 0.8 mg/kg/q12h if CrCl 30-60 ml/minCrCl 30-60 ml/min
• Anti-Xa monitoring Anti-Xa monitoring
• Doses “appeared safe”Doses “appeared safe”
• Further prospective evaluation neededFurther prospective evaluation needed

Clinical Use Of Recommended Clinical Use Of Recommended Enoxaparin Dosage in Renal ImpairmentEnoxaparin Dosage in Renal Impairment
Lachish T et al. Lachish T et al. PharmacotherapyPharmacotherapy 2007; 27:1347-52. 2007; 27:1347-52.
PEAK ANTI-Xa LEVELSPEAK ANTI-Xa LEVELS TROUGH ANTI-Xa LEVELSTROUGH ANTI-Xa LEVELS
N = 19 pts with Clcr < 30ml/min receiving enoxaparin 1mg/kg q24hN = 19 pts with Clcr < 30ml/min receiving enoxaparin 1mg/kg q24h
First doseFirst dose Subsequent doses(second and third)Subsequent doses(second and third)
1.0.
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
1.0.
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Median 25-75% interquartile rangeMedian 25-75% interquartile range
Ant
ifact
or
X1
Leve
l (U
/mL)
Ant
ifact
or
X1
Leve
l (U
/mL)
6
5
4
3
2
1
0
6
5
4
3
2
1
0
0.05 0.10 0.15 0.20 0.25 0.30 0.35 0.40 0.45 0.50 0.550.05 0.10 0.15 0.20 0.25 0.30 0.35 0.40 0.45 0.50 0.55
Trough Antifactor Xa Level (U/mL)Trough Antifactor Xa Level (U/mL)Trough Antifactor Xa Level (U/mL)Trough Antifactor Xa Level (U/mL)
Num
ber
of
Pat
ien
tsN
umb
er o
f P
atie
nts

Tinzaparin 175 U/kgTinzaparin 175 U/kgPeak Anti-Xa Levels According to Renal FunctionPeak Anti-Xa Levels According to Renal Function
Siguret V et al. Siguret V et al. Thromb HaemostThromb Haemost 2000;84:800-4. 2000;84:800-4.
No correlation between peak anti-Xa activity and Clcr No correlation between peak anti-Xa activity and Clcr No accumulation of Anti-Xa activity after 10 days of therapyNo accumulation of Anti-Xa activity after 10 days of therapy

Pharmacokinetics of ProphylacticPharmacokinetics of ProphylacticEnoxaparin vs TinzaparinEnoxaparin vs Tinzaparin
Mahe I et al. Thromb Haemost 2007; 97:581-6.Mahe I et al. Thromb Haemost 2007; 97:581-6.
Enoxaparin 40mg qdEnoxaparin 40mg qd or or Tinazaparin 4500 IU qdTinazaparin 4500 IU qd
N = 52 patientsN = 52 patients
Mean age = 87.7 yrsMean age = 87.7 yrsMean wt = 52.3kgMean wt = 52.3kgMean Clcr = 34.7ml/minMean Clcr = 34.7ml/min

Pharmacokinetics ofPharmacokinetics ofProphylactic Doses of DalteparinProphylactic Doses of Dalteparin
Tincani E et al. Tincani E et al. HaematologicaHaematologica 2006; 91:976-9. 2006; 91:976-9.
N = 115 elderly (age > 65) pts with acute medical illness and elevated SCrN = 115 elderly (age > 65) pts with acute medical illness and elevated SCrTx: dalteparin 5000 U or 2500 U SQ qd (risk-based) for VTE prophylaxisTx: dalteparin 5000 U or 2500 U SQ qd (risk-based) for VTE prophylaxis
Renal FailureRenal Failure MildMild(n=12)(n=12)
ModerateModerate(n=73)(n=73)
SevereSevere(n=24)(n=24)
CrCL (ml/min)CrCL (ml/min) 60-8960-89 30-5930-59 <30<30
Day 6 peak anti-XaDay 6 peak anti-Xa 0.0300.030 0.0330.033 0.0480.048
Minor BleedingMinor Bleeding 00 33 00
Major BleedingMajor Bleeding 00 00 00
P=0.72P=0.72P=0.72P=0.72
► No evidence of accumulation of anti-Xa activity► No relationship between the degree of renal impairment and peak
anti-Xa level on Day 6► No association between creatinine clearance and anti-Xa levels

Dalteparin Thromboprophylaxis in Critically Ill Patients Dalteparin Thromboprophylaxis in Critically Ill Patients with Severe Renal Insufficiency: The Direct Studywith Severe Renal Insufficiency: The Direct Study
► N=138 critically ill patientsN=138 critically ill patients► CrCl < 30 ml/min CrCl < 30 ml/min
• Mean CrCL 18.9ml/minMean CrCL 18.9ml/min► Dalteparin 5000 IU sc daily Dalteparin 5000 IU sc daily ► Serial anti Xa levels measured on days 3, 10, and 17Serial anti Xa levels measured on days 3, 10, and 17► Bioaccumulation defined as trough anti-Xa level > 0.40 IU/mLBioaccumulation defined as trough anti-Xa level > 0.40 IU/mL
Results:Results:► The median duration of dalteparin exposure was 7 (4-12) days The median duration of dalteparin exposure was 7 (4-12) days ► No patient had a trough anti Xa level > 0.4 IU/mlNo patient had a trough anti Xa level > 0.4 IU/ml► Based on serial measurementsBased on serial measurements
• peak anti-Xa levels were 0.29 to 0.34 IU/mLpeak anti-Xa levels were 0.29 to 0.34 IU/mL• trough levels were lower than 0.06 IU/mLtrough levels were lower than 0.06 IU/mL
Douketis, et al. Arch Intern Med. 2008 Sep 8;168(16):1805-12. Douketis, et al. Arch Intern Med. 2008 Sep 8;168(16):1805-12.

Dosing of LMWHs In Renal Impairment Dosing of LMWHs In Renal Impairment RecommendationsRecommendations
FOR CrCL < 30 ml/minFOR CrCL < 30 ml/min► Enoxaparin:Enoxaparin:
● Prophylaxis doses: 30 mg sq QDProphylaxis doses: 30 mg sq QD● Treatment doses: 1mg/Kg sq QDTreatment doses: 1mg/Kg sq QD
► Dalteparin and Tinzaparin:Dalteparin and Tinzaparin:● no specific dosing guidelinesno specific dosing guidelines● No or lower degree of accumulation expectedNo or lower degree of accumulation expected● Anti-Factor Xa activity monitoringAnti-Factor Xa activity monitoring
FOR CrCL 30-50 mL/minFOR CrCL 30-50 mL/min► No specific recommendations No specific recommendations ► Concern with prolonged use > 10 days with enoxaparin (15-25% Concern with prolonged use > 10 days with enoxaparin (15-25%
dose decrease ?)dose decrease ?)► Monitoring anti-Xa ?Monitoring anti-Xa ?
Nutescu E, et.al. Ann Pharmacother; 2009; 43(6):1064-83.Nutescu E, et.al. Ann Pharmacother; 2009; 43(6):1064-83.

Unresolved Issues in Unresolved Issues in Renal Dosing of LMWHsRenal Dosing of LMWHs
CrCl (mL/min)CrCl (mL/min) RecommendationsRecommendations
< 30< 30 Dose of enoxaparin should be adjusted; dalteparin and Dose of enoxaparin should be adjusted; dalteparin and tinzaparin no short term accumulation expected.tinzaparin no short term accumulation expected.
< 20-15< 20-15LMWHs have not been adequately studied as repeated LMWHs have not been adequately studied as repeated doses for prophylaxis and treatment indications; UFH is doses for prophylaxis and treatment indications; UFH is preferred in these patients.preferred in these patients.
Issues with anti-factor Xa testing include: Issues with anti-factor Xa testing include: true therapeutic range, standardization, availability, recommendations true therapeutic range, standardization, availability, recommendations
for dose adjustmentfor dose adjustment

Anti-Xa Activity Level MonitoringAnti-Xa Activity Level Monitoring
Enoxaparin 1mg/kg SQ pharmacokinetic profileEnoxaparin 1mg/kg SQ pharmacokinetic profile
Peak (goal ~ 0.5-1 U/ml) at 3-4 hrs
Trough (goal < 0.5 U/ml) at 11-12 hrs
Laposata et al. Laposata et al. Arch Pathol Lab MedArch Pathol Lab Med. 1998;122:799-807.. 1998;122:799-807.

Fondaparinux Use in Patients Fondaparinux Use in Patients with with Impaired Renal FunctionImpaired Renal Function
► Total clearance lower than in patients Total clearance lower than in patients with normal renal functionwith normal renal function
● Mild impairmentMild impairment ~25%~25%
● Moderate impairmentModerate impairment ~40%~40%
● Severe impairmentSevere impairment ~55%~55%
Fondaparinux: PIFondaparinux: PI

Applying National Guidelines to Applying National Guidelines to Clinical PracticeClinical Practice
Current Status of ASCO and NCCN Guidelines for VTE Prophylaxis in Cancer Patients
Applying National Guidelines to Applying National Guidelines to Clinical PracticeClinical Practice
Current Status of ASCO and NCCN Guidelines for VTE Prophylaxis in Cancer Patients
Program ChairmanProgram ChairmanCraig M. Kessler, MDCraig M. Kessler, MD
Professor of Medicine and PathologyProfessor of Medicine and PathologyGeorgetown University Medical CenterGeorgetown University Medical CenterDirector of the Division of CoagulationDirector of the Division of Coagulation
Department of Laboratory MedicineDepartment of Laboratory MedicineLombardi Comprehensive Cancer CenterLombardi Comprehensive Cancer Center
Washington, DCWashington, DC
Mechanisms ● Mortality ● TherapeuticsMechanisms ● Mortality ● Therapeutics

ASCO Guidelines ASCO Guidelines Hospitalized Patients with CancerHospitalized Patients with Cancer
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
Patients with cancer should be Patients with cancer should be considered candidates for VTE considered candidates for VTE prophylaxis with anticoagulants prophylaxis with anticoagulants (UFH, LMWH, or fondaparinux) in (UFH, LMWH, or fondaparinux) in the absence of bleeding or other the absence of bleeding or other contraindications to anticoagulationcontraindications to anticoagulation
Multiple RCTs of hospitalized Multiple RCTs of hospitalized medical patients with subgroups of medical patients with subgroups of patients with cancer. The 8th ACCP patients with cancer. The 8th ACCP guidelines strongly recommend guidelines strongly recommend (1A) prophylaxis with either low-(1A) prophylaxis with either low-dose heparin or LMWH for dose heparin or LMWH for bedridden patients with active bedridden patients with active cancer.cancer.

Ambulatory Patients with Cancer Without VTE Ambulatory Patients with Cancer Without VTE Receiving Systemic ChemotherapyReceiving Systemic Chemotherapy
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
Routine prophylaxis with an Routine prophylaxis with an antithrombotic agents is not antithrombotic agents is not recommended recommended except as noted belowexcept as noted below
Routine prophylaxis in ambulatory Routine prophylaxis in ambulatory patients receiving chemotherapy is not patients receiving chemotherapy is not recommended due to conflicting trials, recommended due to conflicting trials, potential bleeding, the need for potential bleeding, the need for laboratory monitoring and dose laboratory monitoring and dose adjustment, and the relatively low adjustment, and the relatively low incidence of VTE.incidence of VTE.
LMWH or adjusted dose warfarin (INR LMWH or adjusted dose warfarin (INR ~ 1.5) is recommended in myeloma ~ 1.5) is recommended in myeloma patients on thalidomide or lenalidomide patients on thalidomide or lenalidomide plus chemotherapy or dexamethasoneplus chemotherapy or dexamethasone
This recommendation is based on This recommendation is based on nonrandomized trial data and nonrandomized trial data and extrapolation from studies of extrapolation from studies of postoperative prophylaxis in orthopedic postoperative prophylaxis in orthopedic surgery and a trial of adjusted-dose surgery and a trial of adjusted-dose warfarin in breast cancerwarfarin in breast cancer

Patients with Cancer Undergoing SurgeryPatients with Cancer Undergoing Surgery
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
All patients undergoing major surgical All patients undergoing major surgical intervention for malignant disease intervention for malignant disease should be considered for should be considered for thromboprophylaxis with low- dose thromboprophylaxis with low- dose UFH, LMWH, or fondaparinux starting UFH, LMWH, or fondaparinux starting as early as possible for at least 7-10 as early as possible for at least 7-10 days unless contraindicated.days unless contraindicated.
RCTs of UFH and those comparing RCTs of UFH and those comparing the effects of LMWH and UFH on DVT the effects of LMWH and UFH on DVT rates on patients with cancer indicate rates on patients with cancer indicate broadly similar prophylactic efficacies broadly similar prophylactic efficacies for these two agentsfor these two agents
Mechanical methods may be added to Mechanical methods may be added to anticoagulation in very high risk anticoagulation in very high risk patients but should not be used alone patients but should not be used alone unless anticoagulation in unless anticoagulation in contraindicated.contraindicated.
A Cochrane review of 19 studiesA Cochrane review of 19 studies

Patients with Cancer Patients with Cancer Undergoing Surgery Undergoing Surgery (continued)(continued)
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
LMWH for up to 4 weeks may be LMWH for up to 4 weeks may be considered after major considered after major abdominal/pelvic surgery with residual abdominal/pelvic surgery with residual malignant disease, obesity, and a malignant disease, obesity, and a previous history of VTEprevious history of VTE
Recent RCTs suggest that prolonging Recent RCTs suggest that prolonging prophylaxis up to 4 weeks is more prophylaxis up to 4 weeks is more effective than short-course prophylaxiseffective than short-course prophylaxis in reducing postoperative VTE.in reducing postoperative VTE.

Treatment of Patients with Established Treatment of Patients with Established VTE to Prevent RecurrenceVTE to Prevent Recurrence
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
LMWH is the preferred approach for the initial LMWH is the preferred approach for the initial 5-10 days in cancer patient with established 5-10 days in cancer patient with established VTE.VTE.
LMWH for 3-6 months is LMWH for 3-6 months is more effective than vitamin K more effective than vitamin K antagonists given for a antagonists given for a similar duration for similar duration for preventing recurrent VTE.preventing recurrent VTE.
LMWH for at least 6 months is preferred for LMWH for at least 6 months is preferred for long-term anticoagulant therapy. Vitamin K long-term anticoagulant therapy. Vitamin K antagonists with a targeted INR of 2-3 are antagonists with a targeted INR of 2-3 are acceptable when LMWH is not available. The acceptable when LMWH is not available. The CLOT study demonstrated a relative risk CLOT study demonstrated a relative risk reduction of 49% with LMWH vs. a vitamin K reduction of 49% with LMWH vs. a vitamin K antagonist. Dalteparin sodium approved by the antagonist. Dalteparin sodium approved by the FDA for extended treatment of symptomatic FDA for extended treatment of symptomatic VTE to reduce the risk of recurrence of VTE in VTE to reduce the risk of recurrence of VTE in patients with cancerpatients with cancer (FDA 2007) (FDA 2007)

Treatment of Patients with Established Treatment of Patients with Established VTE to Prevent Recurrence VTE to Prevent Recurrence (continued)(continued)
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
Anticoagulation for an indefinite period Anticoagulation for an indefinite period should be considered for patients with should be considered for patients with active cancer (metastatic disease, active cancer (metastatic disease, continuing chemotherapy)continuing chemotherapy)
In the absence of clinical trials, In the absence of clinical trials, benefits and risks of benefits and risks of continuing LMWH continuing LMWH beyond 6 months is a clinical beyond 6 months is a clinical judgment in the individual patient.judgment in the individual patient. Caution is urged in elderly patients Caution is urged in elderly patients and those with intracranial and those with intracranial malignancy.malignancy.
Inferior vena cava filters are reserved Inferior vena cava filters are reserved for those with contraindications to for those with contraindications to anticoagulation or PE despite anticoagulation or PE despite adequate long-term LMWH.adequate long-term LMWH.
Consensus recommendations due to Consensus recommendations due to lack of date in cancer-specific lack of date in cancer-specific populationspopulations

Anticoagulants in the Absence of Anticoagulants in the Absence of Established VTE to Improve SurvivalEstablished VTE to Improve Survival
Role of VTE ProphylaxisRole of VTE Prophylaxis EvidenceEvidence
Anticoagulants are not currently Anticoagulants are not currently recommended to improve survival in recommended to improve survival in patients with cancer without VTE.patients with cancer without VTE.
RCTs and meta-analysis of warfarin, RCTs and meta-analysis of warfarin, UFH and LMWH have reported UFH and LMWH have reported encouraging but variable results encouraging but variable results generally showing clinical benefit only generally showing clinical benefit only in subgroup analyses.in subgroup analyses.

Summary of NCCN Guidelines UpdatesSummary of NCCN Guidelines Updates
Summary of Major Changes in the Summary of Major Changes in the 1.2009 Version of the NCCN Venous 1.2009 Version of the NCCN Venous Thromboembolic Disease GuidelinesThromboembolic Disease Guidelines

Changes in 2009 NCCN GuidelinesChanges in 2009 NCCN Guidelines
Stage 1 Immediate:Stage 1 Immediate:► ““Stage 1 Immediate: Concomitant with diagnosis or while diagnosis Stage 1 Immediate: Concomitant with diagnosis or while diagnosis
and risk assessment (heparin phase)” changed to “Stage 1 and risk assessment (heparin phase)” changed to “Stage 1 Immediate: At diagnosis or during diagnostic evaluation”Immediate: At diagnosis or during diagnostic evaluation”
► Low –molecular-weight-heparin: New footnote “6” was added that Low –molecular-weight-heparin: New footnote “6” was added that states, states, “Although each of the low molecular weight heparins “Although each of the low molecular weight heparins (LMWH), have been studies in randomized control trials in cancer (LMWH), have been studies in randomized control trials in cancer patients, dalteparin’s efficacy in this population is supported by the patients, dalteparin’s efficacy in this population is supported by the highest quality evidence and it is the only LMWH approved by the highest quality evidence and it is the only LMWH approved by the FDA for this indicationFDA for this indication.”.”
► Unfractionated heparin (IV): target aPTT range changed from “2.0-Unfractionated heparin (IV): target aPTT range changed from “2.0-2.9 x control) to “2.0-2.5 x control…” (Also for VTE-H) in these 2.9 x control) to “2.0-2.5 x control…” (Also for VTE-H) in these patients.patients.

Changes in 2009 NCCN GuidelinesChanges in 2009 NCCN Guidelines
Stage 3 Chronic:Stage 3 Chronic:
► ““Third bullet: “Consider indefinite anticoagulation….” Third bullet: “Consider indefinite anticoagulation….” changed to “changed to “Recommend indefinite anticoagulation….”Recommend indefinite anticoagulation….”
► Fourth bullet: “For catheter associated thrombosis, Fourth bullet: “For catheter associated thrombosis, anticoagulate as long as catheter is in place and for at anticoagulate as long as catheter is in place and for at least 3 months after catheter removal”.least 3 months after catheter removal”.

Changes in 2009 NCCN GuidelinesChanges in 2009 NCCN Guidelines
► 66Although each of the low molecular weight heparins Although each of the low molecular weight heparins (LMWH) have been studied in randomized controlled (LMWH) have been studied in randomized controlled trials in cancer patients, trials in cancer patients, dalteparin’s efficacy in this dalteparin’s efficacy in this population is supported by the highest quality evidence population is supported by the highest quality evidence and is the only LMWH approved by the FDA for this and is the only LMWH approved by the FDA for this indication.indication.
Lee AYY, Levine MN, Baker RI, Bowden C, et al. Low-molecular-weight Lee AYY, Levine MN, Baker RI, Bowden C, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous heparin versus a coumarin for the prevention of recurrent venous thromboembolism on patients with cancer. New Eng J Med 2003;349(2): thromboembolism on patients with cancer. New Eng J Med 2003;349(2): 146-153.146-153.

(VTE-D): (VTE-D): Therapeutic Anticoagulation Therapeutic Anticoagulation Treatment for VenousThromboembolismTreatment for VenousThromboembolism
► The NCCN panel recommends VTE thromboprophylaxis for all The NCCN panel recommends VTE thromboprophylaxis for all hospitalized patients with cancer who do not have hospitalized patients with cancer who do not have contraindications to such therapy, and the panel also contraindications to such therapy, and the panel also emphasized that an increased level of clinical suspicion of emphasized that an increased level of clinical suspicion of VTE should be maintained for cancer patients. VTE should be maintained for cancer patients. Following Following hospital discharge, it is recommended that patients at high-risk hospital discharge, it is recommended that patients at high-risk of VTE (e.g. cancer surgery patients) continue to receive VTE of VTE (e.g. cancer surgery patients) continue to receive VTE prophylaxis for up to 4 weeks post-operation.prophylaxis for up to 4 weeks post-operation. Careful Careful evaluation and follow-up of cancer patients in whom VTE is evaluation and follow-up of cancer patients in whom VTE is suspected and prompt treatment and follow-up for patients suspected and prompt treatment and follow-up for patients diagnosed with VTE is recommended after the cancer status diagnosed with VTE is recommended after the cancer status of the patient is assessed and the risks and benefits of of the patient is assessed and the risks and benefits of treatment are considered. treatment are considered.

(VTE-D): (VTE-D): Therapeutic Anticoagulation Therapeutic Anticoagulation Treatment for VenousThromboembolismTreatment for VenousThromboembolism
Stage 1 Stage 1 ImmediateImmediate: At diagnosis or during diagnostic : At diagnosis or during diagnostic evaluation:evaluation:
► Low-molecular-weight heparin (LMWH)Low-molecular-weight heparin (LMWH)• Dalteparin (200 units/kg subcutaneous daily)Dalteparin (200 units/kg subcutaneous daily)• Enoxaparin (1 mg/kg subcutaneous every 12 hours)Enoxaparin (1 mg/kg subcutaneous every 12 hours)• Tinzaparin (175 units/kg subcutaneous daily)Tinzaparin (175 units/kg subcutaneous daily)
► Fondaparinux (5 mg [<50 kg]; 7.5 mg [50-100 kg]; 10 mg [> 100 kg] Fondaparinux (5 mg [<50 kg]; 7.5 mg [50-100 kg]; 10 mg [> 100 kg] subcutaneous dailysubcutaneous daily
► Unfractionated heparinUnfractionated heparin (IV) (80 units/kg load, then 18 (IV) (80 units/kg load, then 18 units/kg per hour, target aPTT of 2.0-2.5 x control or per units/kg per hour, target aPTT of 2.0-2.5 x control or per hospital SOP)hospital SOP)

(VTE-D): (VTE-D): Therapeutic Anticoagulation Therapeutic Anticoagulation Treatment for VenousThromboembolismTreatment for VenousThromboembolism
► Additional VTE risk factors for surgical oncology patients Additional VTE risk factors for surgical oncology patients with a previous episode of VTE include anesthesia times with a previous episode of VTE include anesthesia times longer than 2 hours, advanced stage disease, bed rest, longer than 2 hours, advanced stage disease, bed rest, >> 44 days and patients age 60 years or older. Extended days and patients age 60 years or older. Extended prophylaxis out to prophylaxis out to 44 weeks post-surgery was associated weeks post-surgery was associated with a greater than 50% reduction in venographic VTEwith a greater than 50% reduction in venographic VTE

(VTE-D): (VTE-D): Therapeutic Anticoagulation Therapeutic Anticoagulation Treatment for VenousThromboembolismTreatment for VenousThromboembolism
Stage 2 Acute: Short term, during transition to chronic Stage 2 Acute: Short term, during transition to chronic phase:phase:
► LMWH (category 1) is preferred as monotherapyLMWH (category 1) is preferred as monotherapy without without warfarin in patients with proximal DVT or PE and warfarin in patients with proximal DVT or PE and prevention of recurrent VTE in patients with advanced or prevention of recurrent VTE in patients with advanced or metastatic cancermetastatic cancer
► If UFH or factor Xa antagonist, transition to LMWH or If UFH or factor Xa antagonist, transition to LMWH or warfarinwarfarin
► Warfarin (2.5-5 mg every day initially, subsequent dosing Warfarin (2.5-5 mg every day initially, subsequent dosing based on INR value; target INR 2.0-3.0)based on INR value; target INR 2.0-3.0)

Therapeutic Anticoagulation FailureTherapeutic Anticoagulation Failure
Therapeutic INR
Switch to heparin (LMWH preferred)
or fondaparinux
Increase warfarin dose and treat with
parenteral agent until INR target achieved or consider switching
to heparin (LMWH preferred) or fondaparinux
Patient on
warfarin
Check INR
Sub-therapeutic
INR

Therapeutic Anticoagulation FailureTherapeutic Anticoagulation Failure
Therapeutic aPTT
Increase dose of heparin or Switch to LMWH or Switch to fondaparinux and Consider placement of IVC filter and Consider HIT
Increase dose of heparin to reach therapeutic level
Patient on
heparin
Check aPTT levels
Sub-therapeutic
aPTT

Thank YouThank You
Questions?Questions?
Mechanisms ● Mortality ● TherapeuticsMechanisms ● Mortality ● Therapeutics