Embed Size (px)
Citation preview

The role of growth factors myelodysplastic syndromes: what is new?
Rodolfo D. CançadoProf. Adjunto da FCM da Santa Casa de São Paulo
Coordenador do Serviço de Hematologia da Santa Casa de São PauloMédico Hematologista do Hospital Samaritano/SP

Priorities of therapeutic interventions in patients with MDS according to disease stage
Platzbecker U et. Al.Blood First Edition Paper, prepublished online January 22, 2019.

Over two-thirds of the newly diagnosed MDS patients have lower-risk disease
IWG-PM, International Working Group for Prognosis in MDS. Greenberg PL, et al. Blood. 2012;120:2454-65.
Low
Int-1
Int-2
High
16%7%
37%
40%
IWG-PM database (n = 7,012)
Risk level

Italian registry for MDS: Age distribution and presence of Comorbidities
194
430
670
301
0
100
200
300
400
500
600
700
≤ 60 61–70 71–80 > 80
42% 19%27%12%
Age, years
Pat
ien
ts, n
Della Porta MG, et al. Haematologica. 2011;96:441-9.
(n = 1,617)
142
99
7770
0
20
40
60
80
100
120
140
160
Grade 0–2 1 2 > 2
20% 18%37%37%
Pat
ien
ts, n
Comorbidities
(n = 388)
63% with comorbidities (CIRS)

Best supportive care
ESAs
ESA, erythropoiesis-stimulating agent; ; G-CSF, granulocyte colony-stimulating factor.
Improving cytopenias
Neutropenia
Anaemia
2/3 of MDS pts
50% with Hb < 10 g/dL
G-CSF / GM-CSF
Thrombocytopenia Thrombopoetin receptor agonists

Erythropoiesis-Stimulating Agents Treatment in MDS
1. Hellström-Lindberg E, et al. Semin Hematol. 2008;45:14-22; 2. Seastone DJ, et al. Expert Rev Hematol. 2015;8:139-146; 3. Park S, et al. Blood. 2008;111:574-582. 4. Fenaux P, et al. Ann Oncol. 2014;25(suppl 3):iii57-iii69. 5. Rizzo JD, et al. J Oncol Prac. 2010;6:317-320.
Can induce ⇑ Hb and ⇓ blood transfusions
May have a favourable survival impact in MDS
Some of the studies reported improved quality of life
ESMO, ASCO, ASH, ELN, NCCN guidelines
ELN, European LeukemiaNet;
• Erythoid response (ER) rates: 45-73% in ESA-naïve MDS pts
• Median time to ER: 5 weeks (range, 4-9 weeks)
• Duration of response: from 8 to more than 48 months

1. Hellström-Lindberg E, et al. Semin Hematol. 2008;45:14-22; 2. Seastone DJ, et al. Expert Rev Hematol. 2015;8:139-146; 3. Park S, et al. Blood. 2008;111:574-582. 4. Fenaux P, et al. Ann Oncol. 2014;25(suppl 3):iii57-iii69. 5. Rizzo JD, et al. J Oncol Prac. 2010;6:317-320.ELN, European LeukemiaNet;
To whom ?
Which dose/regimen ?
For how long ?
Erythropoiesis-Stimulating Agents Treatment in MDS

Clinical• transfusion
independence• short duration of disease
Santini V. Oncologist. 2011;16 Suppl 3:35-42.
What factors should be considered when deciding on ESA therapy?
Del(5q) (+/- 10% of patients with low-risk MDS) Lenalidomide frequently induces transfusion independence
Biological• IPSS Low or Int-1• diagnosis of refractory anaemia• EPO levels < 500 mIU/mL• marrow blast < 10%• normal karyotype• short duration of disease
Predictive variables for an ESA response in MDS

MDS
Very Good
Intermediate
EPO therapyNOT
recommended
Response Probability
Treatment Response Criteria (responses must last at least 8 weeks)
• Hb increase by 1.5 g/dL• Relevant reduction transfusion ( 4U/8weeks)• Only RBC transfusions given for Hb of 9.0 g/dL pretreatment
Treatment Response Score
Serum EPO
(U/L)
< 100 +2
100-500 +1
> 500 -3
Transfusion
requirement
(pRBC/month)
< 2 +2
2 -2
Score: 4
Score: 3
Score: -1;+1
Score < -1
Good
MDS IPSS
Low or int-1
Hb < 10g/dL
Refining Hellström-Lindberg Score (Revised HLS): Which Patients Could Benefit from Standard Dose EPO?
Marta Riva et al. Blood 2017;130:2981

1. Hellström-Lindberg E, et al. Semin Hematol. 2008;45:14-22; 2. Seastone DJ, et al. Expert Rev Hematol. 2015;8:139-146; 3. Park S, et al. Blood. 2008;111:574-582. 4. Fenaux P, et al. Ann Oncol. 2014;25(suppl 3):iii57-iii69. 5. Rizzo JD, et al. J Oncol Prac. 2010;6:317-320.ELN, European LeukemiaNet;
Epoetin alfa:
150 to 300 units/Kg daily
≥ 150 units/Kg 3 times per week
40,000 units once per week
Darbepoetin alfa:
75 to 400 mcg once/week
500 mcg every 2-3 weeks
Erythropoiesis-Stimulating Agents Treatment in MDS
Which dose/regimen ?
40,000 units once per week
40,000 units twice a week
150-300 mcg every week
500 mcg every 2-3 weeks

Park S, Greenberg P, Yucel A, et al. Br J Haematol 2019; 184:134.
Park S, Fenaux P, Greenberg P, et al. Br J Haematol 2016; 174:730..
• It will take about 12 weeks before concluding that ESA therapy is ineffective
• Transfusions may be needed to manage symptoms while awaiting an ER
• ESAs should not be continued > 6-9 months if no response is observed.
Erythropoiesis-Stimulating Agents Treatment in MDS
For how long ?
ER, erythroid responseG-CSFgranulocyte colony-stimulating factor

Weekly epoetin alfa in low-risk MDS patients
Patients and study design
• Open-label, uncontrolled study, n = 133
• Loading dose: 80,000 IU/week for 4 weeks (40,000 IU twice a week)
• In non-responders, continue loading dose for 4 weeks
• Maintenance: epoetin alfa 40,000 IU/week s.c. up to 24 weeks
Baseline status Patients, n Patients, % Hb (g/dL)
Transfusion independent 79 8.84 0.81
Transfusion dependent 54 8.19 1.20
RA 62
RARS 24
RAEB 14
Aloe Spiriti MA, et al. Ann Hematol. 2005;84:167-76.RA, refractory anaemia; RAEB, RA with excess blasts; RARS, RA with ringed sideroblasts.

Nearly all transfusion-independent patients (n = 78) remained transfusion independent during 8 weeks of epoetin alfa treatment
Transfusion independence is maintained with epoetin alfa treatment Aloe Spiriti MA, et al. Ann Hematol. 2005;84:167-76.
Erythroid response rate:Overall: 68%Transfusion-independent patients: 74%Transfusion-dependent patients: 59%
Response duration
Re
sp
on
se
ra
te
(%)
Time (weeks)
100
60
40
20
0
80
All
Transfusion independent
Transfusion dependent
8 12 16 20 24
Erythroid response to epoetin alfa is higher and of longer duration in
transfusion-independent patients

EPO vs. EPO + G-CSF to treat anaemia in low-risk MDS
• Retrospective study
• 30 MDS patients with < 10% bone marrow blasts
• 37% transfusion dependent
• Randomized: EPO 30,000 U/w versus EPO + G-CSF 600 µg/w
Balleari E, et al. Ann Hematol. 2006;85:174-80.
Parameter EPO EPO + G-CSF
Response 40% 73%
Transformation to AML 13% 13%
Addition of G-CSF to EPO in non-responders induced a response in 4/9 (45%) pts

Pts not heavily RBC transfusion dependent (< 2 units/month)
Serum EPO < 500 mIU/mL
Who have not responded to ESAs alone
Santini V, et al. Leuk Res. 2010;34:1576-88.
Recommendations for the use of ESA and G-CSF combined
When ring sideroblasts are present, MDS patients will not respond to erythropoietin alone but may respond to EPO + G-CSF

IMRAW, International MDS Risk Analysis Workshop.
Park S, et al. Blood. 2008;111:574-82.
Prolonged survival of MDS patients treated with ESAs
Time since diagnosis or
recombinant EPO treatment (years)
Pati
en
ts a
live (
%)
0
20
40
60
80
100
10
30
50
70
90
0 2 4 6 7 1081 3 5 9
p < 0.001
EPO response
EPO no response
IMRAW

EPO + G-CSF therapy and AML
Jädersten M, et al. J Clin Oncol. 2008;26:3607-13.
HR = 0.89(95% CI: 0.52–1.52)p = 0.66
Pro
bab
ility
of
fre
ed
om
fr
om
AM
L, %
Time, years
EPO-G treated
Untreated
100
80
60
40
20
00 2 4 6 8 10 12 14 16

EPO + G-CSF in patients with lower-risk MDS: impact on overall survival
Jädersten M, et al. J Clin Oncol. 2008;26:3607-13.
EPO + G-CSF (n = 121)
Untreated (n = 237)
100
80
60
40
20
0
Pat
ien
ts s
urv
ivin
g, %
Time, years
p = 0.002
0 2 4 6 8 10 12 14 16
Increased OS was
observed in patients with
IPSS Low-risk MDS
(p = 0.033) but not in
patients with higher-risk MDS (p = n.s.)

Gabrilove J, et al. Br J Haematol. 2008;142:379-93. ; Giraldo P, et al. Cancer. 2006;107:2807-16. ; Mannone L, et al. Br J Haematol. 2006;133:513-9.; Musto P, et al. Br J Haematol. 2005;128:204-9.; Stasi R, et al. Ann Oncol. 2005;16:1921-7.
Darbepoetin in MDS
Reference Patients, n Dose/week Response rate, % Prognostic factor
Stasi (2005) 53 150 μg 45 EPO < 200 IU/L
Musto (2005) 37 150 μg 40.5
EPO < 100 IU/L
No transfusion
Blasts < 5%
Giraldo (2006) 69 150 μg 55 (30 major, 25 minor) ESA naive
Mannone (2006) 63 300 μg 71 (55 major, 16 minor)EPO < 200 IU/L
No transfusion
Gabrilove
(2008)
ESA naive: 144
Prior ESA: 62
500 µg/3 weeks(every 2 weeks in
poor responders)
71 (49 major, 22 minor)
44 (26 major, 18 minor)
ESA naive
EPO < 100 IU/L

ARCADE Study of Darbepoetin alfa for the Treatment of Anemiain Patients With MDS Phase 3, Randomized, Double-blind, Placebo-Controlled
2 weeks 0 24 weeks 84 weeks48 weeks
Screening (n = 226)
Main eligibility criteria:• IPSS low-/int-1–risk• Hb ≤ 10 g/dL• Low transfusion burdena
• EPO ≤ 500 mU/mL• ESA-naïve
Ran
do
miz
atio
n 2
:1
(N =
14
7)
Darbepoetin alfa 500 mcg Q3W
(n = 97)b
Placebo Q3W (n = 49)
Active Treatment
Darbepoetin alfa 500 mcg Q3W
(Could increase from Q3W to Q2W
from week 31 on)
Long-term follow-up for survival
and AML evolution
End
of
blin
de
d t
reat
me
nt
Objective: To assess the reduction in RBC transfusions and safety
aLow transfusion burden was defined as < 4 RBC transfusion units in each of 2 consecutive 8-week periods before randomization.bOne patient did not receive darbepoetin alfa; serum EPO was ≤ 500 mU/ml locally but > 500 mU/ml centrally, so the patient was withdrawn..
Platzbecker U, et al. Leukemia. 2017;31:1944-1950

Transfusion incidence from weeks 5–24 was significantly lower with
darbepoetin alfa (36.1% (35/97) versus placebo versus 59.2% (29/49),
P = 0.008)
Erythroid response rates increased significantly with darbepoetin alfa
(14.7% (11/75 evaluable) versus 0% (0/35 evaluable), P = 0.016).
In the 48-week open-label period, dose frequency increased from Q3W
to Q2W in 81% (102/126) of patients
ARCADE Study: Results

The overall rate of AML progression was 2.2%; median time to AML progression was not reached in either treatment group
ARCADE Study: Time to AML Progression
Study WeekPatients at risk:
PBO: 46 45 41 36 36 36 35 34 34 32 32 31 30 29 28 26 20 15 6 2 1 1 0
DA: 95 95 93 85 84 83 83 82 81 79 77 75 71 69 63 45 21 19 5 1 0
00
2
4
6
8
10
PBO (n = 46)
DA (n = 95)
Log-rank test (adjusted): P = 0.9781
Pro
gre
ssio
n t
o A
ML, %
20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170 180 190 200 210 22010

Stratification factor for Log-rank test is IPSS score
• 41 deaths occurred on study:
• 27 (28%) in the darbepoetin alfa group and 14 (29%) in the placebo group
• Most died during long-term follow-up (darbepoetin alfa, 93%; placebo, 79%)
ARCADE Study: Time to Death
PBO (n = 48)
DA (n = 98)
Log-rank test (adjusted): P = 0.7822
0
20
40
60
80
100
Study Week
Pa
tien
ts w
ith
Fata
l E
ve
nt,
%
Patients at risk:
48 48 42 41 41 41 40 38 37 36 36 33 32 31 30 28 22 16 6 2 1 1 0
98 97 93 90 89 88 86 86 83 83 81 78 75 75 69 52 27 24 6 3 1 0
PBO:
DA:
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170 180 190 200 210 220
DA, darbepoetin alfa; PBO, placebo.Platzbecker U, et al. Slides presented at 23rd European Hematology Association Congress;
June 14-17, 2018; Stockholm, Sweden. Abstract EHA-3168. Graph adapted from Reference.

• ESA schedule able to the maintain Hb between 10 and 12 g/dL
• If the patient responds to ESA treatment, an attempt should be made to
reduce the dose (or the frequency of administration)
• During ESA treatment, iron supplementation should be considered
–for patients with a transferrin saturation lower than 20%
Santini V, et al. Leuk Res. 2010;34:1576-88.
Recommendations for ESA dose and iron supplementation

212 cases of deep vein thrombosis in 5,673 patients
Weiss Smith S, et al. Haematologica. 2012;97:15-20.
ESA treatment does not increase risk of thrombosis in patients with MDS
Parameter OR 95% CI
Use of ESA 1.21 0.60−2.43
RBC transfusion 4.60 2.29−9.23
Central venous
catheter placement6.47 2.37−17.62

Baso E, basophilic erythroblast; EPO, erythropoietin; IL-3, interleukin 3;; Ortho E, orthochromatic erythroblast; Poly E, polychromatic erythroblast; Pro E, proerythroblast; SCF, stem cell factor.
Positive regulator
of RBC production
EPO
Differentiation/maturation
Negative regulator
of RBC production
TGF-b superfamily ligands
Proliferation
500 cells 8–64 cells
EPO
EPO-dependent
EPO-responsive
SCFIL-3EPO
BFU-E CFU-E Pro E Baso E Poly E Ortho E Reticulocyte RBC
Emerging agents as treatment for anemia in patients with low-risk MDS
Modifiedextracellular
domainof ActRIIB
Fc domainof human
IgG1antibody
Luspatercept
Extracellulardomain
of ActRIIA
Fc domainof human
IgG1 antibody
Sotatercept
(ACE-011) (ACE-536)
Galunisertib

ALK, activin-like kinase receptor; GDF, growth differentiation factor; TIF transcriptional
intermediary factor.
TGF-βfamily members
regulate haemopoiesis
+
P
P
P
Transphosphorylated TβR complex (ALK5)
Phosphorylated SMAD2/3 complex
SMAD2 SMAD3
P
TIF γSMAD4
SMAD6/7
+
P
P P
P
P
P
ALK4
Activin receptor ligands, GDFs
TGF-β
Altered erythroid differentiationIneffective haemopoiesis
P
Inhibition of proliferation
Galunisertib
Luspatercept

Pierre Fenaux et al. Blood 2019;133:790-794.
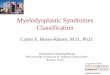
Luspatercept for the treatment of anemia in myelodysplastic syndromes and primary myelofibrosis
Luspatercept: first-in-class erythroid maturation agent
• Blocks aberrant Smad2/3 signaling to augment late-stage erythropoiesis
• Promising clinical activity in lower-risk MDS patients with anemia[1]

MEDALIST: Study Design
International, randomized, double-blind, placebo-controlled phase III trial
Fenaux. ASH 2018. Abstr 1. NCT02631070.
Primary endpoint: RBC TI for ≥ 8 wks between Wk 1 and Wk 24
Secondary endpoints: RBC TI for ≥ 12 wks between Wk 1 and Wk 24, modified hematologic improvement–erythroid response per IWG 2006 criteria, DoR, Hb change from baseline
Patients ≥ 18 yrs of age Non-del(5q) MDS Ring sideroblasts (WHO 2016 criteria) IPSS-R risk: very low, low, or
intermediate Refractory, intolerant, or ineligible for
ESAs RBC transfusion dependent (N = 229)
Luspatercept 1.0 mg/kg* SC Q3W for ≥ 24 wks
(n = 153)
Placebo SC Q3W for ≥ 24 wks
(n = 76)
Randomized 2:1
*Could be titrated up to 1.75 mg/kg if needed.
Treatment continued until lack of clinical benefit or PD

MEDALIST: Efficacy
Outcome, %Luspatercept
(n = 153)Placebo(n = 76)
P Value
RBC TI ≥ 8 wks in Wks 1-24 37.9 13.2 < .0001
mHI-E* ≥ 8 wks in Wks 1-48
Hb increase of ≥ 1.5 g/dL
58.869.6
17.15.0
< .0001
*Defined as transfusion reduction of ≥ 4 units/8 wks or mean hemoglobin increase ≥ 1.5 g/dL/8 wks in absence of transfusions
Among primary endpoint responders, the median duration of RBC TI response was 30.6 wks in the luspatercept arm vs 13.6 wks in the placebo arm
Fenaux. ASH 2018. Abstr 1. NCT02631070.

Conclusions
Erythropoiesis-Stimulating Agents Treatment in MDS
Right PatientRight DoseRight time