Embed Size (px)
Citation preview

73
The role of electrodiagnostics in the study ofmuscle kinesiology, muscle fatigue andperipheral nerve injuries in sports medicine
Joseph H. Feinberg∗Sports Medicine Kessler Institute for Rehabilitation,West Orange, NJ, USA
Athletes are susceptible to peripheral nerve injuries becauseof the extreme physical challenges to which they are exposed.These injuries are often associated with subtle abnormalitiesand can be difficult to diagnose. They may be overlooked be-cause the well motivated and conditioned athlete often com-pensates for or is not aware of mild weakness and sensorydeficits. Electrodiagnostic studies play an important role indiagnosing peripheral injuries, objectifying neurologic dam-age and prognosticating outcome. They are also being usedto study muscle kinesiology and fatigue. This article willreview some of the basic neurophysiologic and electrophys-iologic principles relevant to peripheral nerve injuries, andintroduce the clinician treating athletes to the role of elec-trodiagnostics in sports medicine and some of the commonperipheral nerves injured.
Keywords: EMG; sports medicine; peripheral nerve; athlete,neurophysiology, kinesiology, muscle fatigue
1. Basic concepts
1.1. Neurophysiology
Seddon’s original classification of nerve injury in-cludes grades I-III [1]. Grade I or neuropraxia is aninjury to the myelin sheath and leads to conductionslowing or a complete conduction block. The tran-sient numbness and/or weakness athletes sustains aftera shoulder subluxation or with a “burner or stinger” is
∗Correspondence to: Joseph Feinberg, MD, Director, SportsMedicine, Kessler Institute for Rehabilitation, 1199 Pleasant ValleyWay, West Orange, NJ 07052, USA. Tel.: +1 973 736 9090; Fax: +1973 243 6861.
often a neuropraxic injury and full neurologic recoveryshould be expected in these cases [2].
Grades II and III represent an axonal injury. Thereis no interuption of the connective tissue framework(endoneurium, perineurium, epineurium) with Grade IIinjuries. Numbness and/or weakness can last weeks tomonths or can even be permanent. This will dependon whether the cause of nerve injury is a reversible(e.g. a ganglion cyst compressing the suprascapularnerve) or on the distance between the site of injuryand the muscle denervated. Grade III or neurotmesisis a disruption of the nerve and its connective tissueframework leading to axonal degeneration. Axonalregeneration will usually take at least several months.Traction injuries in sports can often lead to disruption ofthe connective tissue elements and subsequent axonaldegeneration (e.g. axillary nerve injuries associatedwith shoulder dislocations) [3].
Seddon’s classification was modified by Sunderlandwho expanded grade III into grades III, IV, and V [4].Grade III is a disruption of the endoneurium with sub-sequent axonal degeneration, but with both the per-ineurium and epineurium remaining intact. Grade IVis a disruption of the endoneurium and perineurium butwith the epineurium remaining intact. Grade V is adisruption of all three connective tissue support struc-tures, the endoneurium, perineurium and epineurium(i.e., the nerve is severed).
Grades III through V can last months or be perma-nent. Recovery will depend on some of the same fac-tors mentioned for a Grade II injury. Injury to and lossof the supportive architectural framework of the nervewill impair axonal regeneration and aberrant regenera-tion is more likely to occur. If continuity of the connec-tive tissue framework of the nerve is not re-established,there is little chance that axonal regeneration will leadto functional recovery.
Both Seddon’s and Sunderland’s classifications cat-egorize the entire nerve as either neuropraxic or axonal.
Journal of Back and Musculoskeletal Rehabilitation 12 (1999) 73–88ISSN 1053-8127 / $8.00 1999, IOS Press. All rights reserved

74 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
More often, different axons of the same nerve bundlewill be injured to a variable extent. Some axons may bein a neuropraxic state while others may have undergoneaxonal degeneration. Even the neurpraxic componentmay vary widely. Electrodiagnostic studies can help toclassify these nerve injuries.
A focal injury to a nerve from compression or trac-tion first affects the myelin [4]. Relatively mild injuriesmay lead to temporary loss or slowing of conductionacross the segment involved. This can last seconds tominutes, can be completely reversible and represents amild neuropraxia; the myelin remains intact. An ex-ample of this is handlebar palsy seen in cyclists. Pro-longed resting of the wrist on the handlebar can lead toexcessive compression over Guyon’s canal and injurethe ulnar nerve. Symptoms will initially spontaneouslyresolve when the pressure is relieved.
A greater degree of compression or traction lastingfor longer periods of time, can result in loss of myelin.This represents a more severe neuropraxia; and slow-ing or loss of conduction which can last days to weeks.If not addressed, symptoms can last indefinitely andmay lead to axonal degeneration. The repair of myelinand reversibility of the injury will depend on the extentand time since the myelin damage, the intergrity of theSchwann cell and most importantly, reversing the causeof compression or traction causing the myelin damage.An ulnar neuropathy can develop in throwers from trac-tion on the nerve in the ulnar groove or compressionwithin the cubital tunnel as a result of valgus overloadto the elbow. A change in throwing mechanics andexercises to strengthen the elbow’s medial joint stabi-lizers can help reduce the valgus loads and the sourceof compression/traction.
An injury to the myelin sheath usually results inslowing or complete blockage of electrical conduction.Since each axon has its own myelin sheath, conduc-tion across an entire nerve represents conduction ofthe many axons that make up the nerve. Severe in-jury to the myelin sheath of all axons can lead to notransmission and a complete conduction block of thenerve. As discussed earlier, different axons within thesame nerve are affected to a greater or lesser extent.The conduction velocity of some axons may be nor-mal or slow, while others may have complete conduc-tion block. The electrical recording or waveform of anerve stimulated proximal to or above the segment ofinjured nerve would be dispersed and reduced in height(amplitude). This is called temporal dispersion. Thewaveform of a nerve stimulated distal to or below thesegment of the injured nerve is usually normal as long
as the injury is completely neuropraxic and there is noaxonal damage to the nerve.
Axonal degeneration can occur after death the of itsanterior horn cell, axon transection, or from significanttraction or compression [5,6]. A conduction block mayexist across the injured segment, but the axon distal tothe site of injury may still be able to conduct an impulsefor several days. The distal segment of nerve can nolonger conduct impulses after aproximately 3 to 7 daysfor motor axons and 6 to 11 days for sensory axons [7].
1.2. Nerve conduction testing
1.2.1. Peripheral nerves studiedAlthough all peripheral nerves can be electrically
excited, conventional nerve conduction testing usuallyinvolves the study of sensory nerves that provide cuta-neous sensation and muscles of motor nerves that areanatomically superficial. Nerves to deep muscles canbe studied, but this requires an intramuscular (needleor fine wire) electrode and is technically more difficultto perform and interpret.
Distal nerves of the upper extremity such as the ul-nar, median and radial and most of the muscles theyinnervate are relatively superficial. The nerves are easyto stimulate and the responses can be recorded withskin surface electrodes. Their small size allows forconsistent and reproducible electrode placement.
Proximal nerves of the upper extremity such as thesuprascapular, axillary and musculocutaneous nerveare deep and therefore less accessable to stimulation.These nerves can be excited by stimulating the brachialplexus (proximal to the point of their departure) at thelevel of Erb’s point at the supraclavicular fossa or bystimulating the nerve root with an intramuscular elec-trode. Motor nerves are usually studied by stimulat-ing the nerve proximally and recording the compoundmuscle action potential (CMAP) over the muscle belly.The compound muscle action potential represents thedepolarization of muscle fibers.
CMAPs can be recorded either with a surface or in-tramuscular electrode. When recording from the del-toid for the axillary nerve, the biceps for the muscu-locutaneous nerve, or the infraspinatus when studyingthe suprascapular nerve both surface and intramuscularelectrodes can be used. However, when studying thesuprascapular nerve and recording from the supraspina-tus one must always use an intramuscular recordingelectrode.
The key to recording the CMAP of a motor nerve isproper placement of the recording electrode giving a

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 75
waveform with a clear and definitive “take-off”. This isnecessary if distal latencies and conduction velocitiesare to be accurately measured. Intramuscular recordingelectrodes can yield a CMAP with a much greater am-plitude and a more definitive onset latency. Though thisis time consuming, tedious and requires frequent elec-trode repositioning, the waveforms obtained will havemore definitive latencies and reliable conduction veloc-ities. Side to side comparisons should be made sincestandard reference values for intramuscular recordinghave not been well established.
The recorded response of a sensory nerve is calledthe sensory nerve action potential or SNAP. The SNAPamplitude is much smaller than CMAPs (usually ap-proximately 100 times smaller), but the actual amountof axons being studied is similar to those recorded in theCMAP [8,9]. Because nerve conduction studies evalu-ate lower motor neuron processes, SNAPs are rarely re-duced with cervical radiculopathies because of sparingof the dorsal root ganglia as cervical root compressionsare generally pre-ganglionic. SNAPs can be reducedwith isolated peripheral nerve injuries, brachial plexusinjuries and with post-ganglionic root injuries.
A mixed nerve (motor and sensory) action potentialcalled the MNAP can also be studied. Both stimulationand recording of the nerve action potential is performedover the entire nerve bundle. The tibial plantar mixednerve can be studied to rule tarsal tunnel syndrome,an uncommon entrapment neuropathy causing pain andnumbness in the feet of runners. The nerve can bestimulated over the plantar surface of the foot mediallyand recorded posterior to the medial malleolus. Themedian mixed nerve of the wrist can be compressedin cylcists and lead to carpal tunnel syndrome. It canbe stimulated in the palm and recorded at the wrist.Entrapment of the ulnar nerve at the ulnar groove canbe studied by stimulating the ulnar mixed nerve belowthe ulnar groove and recording above it.
The sensitivity and reliability of doing nerve conduc-tion testing can depend on the population of axons stud-ied. For example, when recording the median distallatency to digit II with a ring electrode, only the smallpercentage of axons supplying sensation to digit II arebeing examined. Segmental stimulation of the medianmixed nerve across the carpal tunnel or the ulnar mixednerve across the ulnar groove allows the electromyo-grapher to study the entire population of the axons asthey cross the site of injury. This technique requiresthat the nerve being studied be superficial at both thesite of stimulation (distal to the site of injury) and siteof recording (proximal to the site of injury). Though
technically more challenging and time consuming thanthe more conventional methods, segmental nerve stud-ies give a better picture of nerve function in a focalregion. They also give the electrodiagnostician a betterassessment of the patient’s baseline nerve conductionvelocities in multiple regions of several nerves.
The H reflex and F wave are two long latency re-sponses. Their value during routine electrodiagnostictesting is limited. They allow the electromyographerto study the path of electrical conduction proximallywhere a nerve may be deep and less accessible to beingstudied.
The H reflex involves stimulation of a sensory path-way not usually studied. A submaximal shock excitesthe 1A sensory afferent which in turn excites the alphamotor neuron. The response time represents the musclestretch reflex arc.
The F wave entails stimulation of all alpha motoraxons antidromically which activates only a small per-centage of the same group of alpha motor axons or-thodromically. This requires a supramaximal stimulis.Unlike the H reflex, the F wave is not a true physi-ologic reflex or relay but allows an electrical stimu-lus to pass the possible site of injury or compressiontwice. This may help identify a site of injury that mightnot be picked up on routine nerve conduction studies,particularly those that are proximal.
1.3. The motor unit
1.3.1. Motor unit sizeAlthough muscle fibers are distinct structures capa-
ble of individual contracting, the functional unit of mus-cle tissue is the motor unit. This includes all musclefibers innervated by the same axon. When an excitedaxon causes motor unit activation, there is an electricaldepolarization with a di or triphasic configuration. Ax-ons innervating larger and greater numbers of musclefibers have larger motor units and greater amplitudes.The ratio of muscle fibers to axon by which they areinnervated is called the ratio of innervation. This canbe as small as 10 : 1 as in the extraocular muscles or aslarge as 2,000 : 1 as in the quadriceps [10]. Muscleswith lower ratios of innervation such as the extraocularmuscles or hand intrinsics are designed for finer motorskills.
1.3.2. Polyphasic potentialsThe waveform of a normal motor unit is usually ei-
ther biphasic or triphasic (Fig. 1). Motor units becomepolyphasic potentials after axonal degeneration from

76 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
Fig. 1. A normal triphasic motor unit.
terminal collateral sprouting or from axonal regenera-tion.
Terminal collateral sprouting occurs after an axonundergoes Wallerian degeneration. A nearby uninjuredaxon can send out nerve sprouts from its most termi-nal point to reinnervate denervated muscle at the levelof the neuromuscular junction (NMJ). The immaturesprouts are poorly myelinated, depolarize more slowlyand increase the number of phases to the motor unit.This in turn increases the motor unit’s length. Themotor unit is now called a long duration (> 12msec)polyphasic potential (> 4 phases) (Fig. 2). Maturationof the collateral sprouts will cause the motor unit tocondense in length and increase in amplitude. Whenthe motor unit size exceeds 8mV, it is then called a“giant motor unit”. This requires significant muscledenervation and enough time for the terminal collateralsprouts to mature.
Long duration polyphasic potential (LDPPs) fromterminal collateral sprouting can be identified 4 weeksfrom the time of injury. This occurs regardless of thelength of the nerve injured because the terminal sproutsalways arise from uninjured nerves distally and a shortdistance from the denervated NMJ. These LDPPs areindicative only of terminal collateral sprouting, not oftrue axonal regeneration and have a distinct configu-ration. To help differentiate this type of polyphasic
Fig. 2. A long duration polyphasic motor unit or “Terminal Collat-eral Sprout Polyphasic Potential”. The motor represents a normaltriphasic motor unit that has sent out terminal collateral sprouts toinnervate denervated muscle fibers.
Fig. 3. A long duration polyphasic motor unit or “Axonal Regener-ating Polyphasic Potential”.
potential from those seen with axonal regeneration wewill call them “terminal collateral sprout polyphasics”(TCSP).
Axonal regeneration also results in the formation ofa polyphasic potential. Axons that have undergone de-generation are capable of regenerating if the remain-ing axon and the cell body (anterior horn cell) are vi-able. This occurs at a rate of approximately 1–4 mmper day. As the regenerating axon reaches the muscletissue, small nerve sprouts find their way to the NMJ.Unlike the TCSPs, these regenerating sprouts are notpart of another axon and motor unit. They exist bythemselves and are initially low in amplitude (< 100microvolts). Their length or duration will initially beshort but lengthen as additional sprouts arise from thesame regenerating axon (Fig. 3). These polyphasic po-tentials indicate true axonal regeneration and have beencalled nascent potentials. To distinguish these polypha-sics from TCSPs and they will be called “axonal regen-eration polyphsics” (ARP).
ARPs take at least several months before they canbe identified electromyographically. This time period

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 77
will be directly dependent on the length of the axonthat has undergone degeneration and is regenerating.TCSPs will always be identified before ARPs duringthe recovery phase when there is an incomplete nerveinjury.
1.4. Motor unit recruitment
When the signal to contract muscle is initiated andsent from the motor cortex, an alpha motor neurontransmits an impulse which activate a motor unit. Eachmotor unit has a rate at which it fires. The firing rateof a motor unit increases with demands of a greatercontraction to a point where a second motor unit beginsto fire and share the burden of the contraction. Thisis called recruitment. The firing rate of the first motorunit can still increase after other motor units have beenrecruited. The ability to further increase the firing rateas other motor units are recruited varies widely frommuscle to muscle.
Axonal degeneration and/or conduction blocks willaffect motor unit recruitment. As motor units drop out,the firing rate of the remaining motor units increasesand the time interval between firing of the same motorunit decreases. This is called a decreased recruitmentinterval. The loss of motor units firing can be observedwith the inability to fill up the entire EMG screen withmotor units. In severe cases of motor unit drop-out,individual motor units can still be identified when theindividual gives a maximum voluntary effort. Theseforms of decreased recruitment patterns are known asneuropathic recruitment patterns.
Recruitment patterns can be used to determine thesite and to a certain extent, the degree of nerve injury.A change in recruitment pattern is the one EMG abnor-mal finding that can be identified immediately follow-ing neurologic injury. Recruitment can not determinewhether motor unit drop out is secondary to a conduc-tion block (severe neuropraxia) or from axonal degen-eration. One must then look for the presence or absenceof positive sharp waves which usually take 7–10 daysto develop and fibrillation potentials which usually take10–14 days.
1.5. Quantitative EMG and fiber typing
Muscle fibers are characterized as either type I ortype IIA, IIB and IIC [11]. Type I fibers are primarilyaerobic, type IIA fibers are primarily glycolytic, anaer-obic and type IIB and IIC are glycolytic with moreaerobic capabilities. All muscle fibers of a motor unit
have the same fiber type. The fiber type is based onits enzyme makeup which will determine whether itsmetabolism is primarily aerobic, anaerobic or moreequally mixed.
The fiber type has very important physiologic im-plications regarding muscle function. Type I motorunits are always recruited first and are more resistantto fatigue. They have a slower twitch time than type IIfibers and therefore can not generate the speed or powertype II fibers can. A spectrum of frequencies calledthe power spectrum can be determined from the mus-cle’s electrical signal with a mathematical formula, afast Fourier transformation. The slower twitch time orslower rate of depolarization of the type I fibers lowersthe median frequency by shifting the power spectrumto the left [12,13]. Conversely, type II fibers have afaster twitch time, a faster rate of depolarization andwhen recruited shift the power spectrum to the right byraising the median frequency.
Fiber type composition has historically been deter-mined histologically by staining muscle fibers for theirenzyme characteristics. Quantitative EMG utilizingskin surface electrodes has been used more recently asa non-invasive technique to determine the relationshipand predominance of type I and type II fibers in a mus-cle [14]. A power spectrum analyses is performed dur-ing an isometric contraction and based on the medianfrequency, an estimation of the relative amounts of typeI and type II fibers is made.
Quantitative EMG has been demonstrated to be areliable technique for studying muscle fatigue [15,16].The muscle contraction must be isometric for at least20% of the maximum voluntary contraction so thatblood flow is impaired and the muscle tissue begins toundergo anaerobic metabolism [17,18]. This causes aslowing of the muscle fiber conduction velocity whichis a linear decline in the median frequency and an in-crease in the EMG amplitude measured by the averagerectified and root mean square values. A decline in themean or median frequency of the EMG signal during asustained isometric contraction has been demonstratedto be the more reliable method than those measure-ments reflecting amplitude changes [19]. Grabiner etal. studied fatigue patterns with surface EMG in thequadriceps of asymptomatic patients and demonstratedno difference in the rate of fatigue between the vastusmedialis and vastus lateralis [20]. Roy et al. utiliz-ing surface EMG found evidence of earlier fatigue insome of the paraspinal muscles of rowers with backpain in comparison to asymptomatic rowers [21]. Hag-berg et al. found the trapezius and supraspinatus to be

78 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
the first muscles to fatigue in the shoulder girdle withshoulder exercises, but used intramuscular electrodesfor the supraspinatus and a surface electrodes for allothers [22]. Since intramuscular electrodes are moresensitive but less reproducible detectors of muscle fa-tigue, it may not be valid to compare the two differ-ent techniques used in different muscles. Additionally,only surface EMG recording has been validated as areliable and reproducible technique for studying mus-cle fatigue. Intramuscular electrodes have been shownto be more sensitive to muscle fatigue, but have notyet been proven as a reproducible and reliable tech-nique [23,24].
Quantitative electromyography has been used exten-sively to study muscle kinesiology. Most of this workhas focused on the shoulder [25–30] and the knee [31–37]. Much work has been compiled to better understandmuscle firing patterns during highly skilled sports activ-ities such as baseball [38–41], swimming [39,40], ten-nis [44–46], golf [47–49], cycling [50,51], running [52,53] and dancing [54]. The clinical significance of manyof these studies has also been reviewed [55,56].
Basmajian and DeLuca [57] have demonstrated thatthe relationship between the amplitude of the EMGsignal and muscle force is not consistantly linear andvaries with different muscles. Therefore, one shouldbe careful about estimating muscle forces on the basisof the EMG amplitude.
Quantitative EMG has also been used to help clini-cians isolate muscles for physical examination and de-sign appropriate rehabilitation programs. This includesfinding positions during the physical exam that best iso-lates individual muscle groups of the shoulder [58–60],identifying exercises appropriate for rehabilitation pro-grams for the shoulder [61–66] and for the knee [67–80]. Jenp [59] found the subscapularis was best isolatedwith the shoulder in the scapular plane at 90 degrees ofelevation while the infraspinatus was best isolated alsowith the shoulder in the scapular plane at 90 degrees ofelevation, but with the arm externally rotated beyondneutral.
Moritani et al. has studied the EMG relationshipbetween eccentric and concentric strengthening [81].They have demonstrated that EMG activity is greaterduring a concentric contraction compared to an eccen-tric contraction when the same amount of force is gen-erated. This supports the concept that eccentric con-tractions are more efficient than concentric contractionsfrom an EMG perspective.
2. Indications for ordering electrodiagnosticstudies
2.1. Neurologic deficits
The primary role of electrodiagnostic studies (EDXs)in sports medicine is to quantify and localize neurologicinjury. They can be used to determine if there is a pe-ripheral neurologic injury. The nerve roots, plexus andperipheral nerves are the structures that can be poten-tailly injured. Precise localization and quantificationof the extent of the injury is necessary for diagnosis,management and prognosis.
Athletes present a challenge to the clinician. Theyare usually highly motivated and may be able to maskor compensate for neurologic deficits. They may evenbe unaware of subtle sensory or motor deficits. Weak-ness may not be appreciable with manual muscle test-ing until there is more severe and possibly irreversibleneurologic damage.
Since both neuropraxia and axonotmesis are poten-tially reversible, quantification can help guide the clin-ician in managing and answering the following ques-tions:
– What is the mechanism of injury to this nerve?– Can the athlete still participate safely and what are
the risks for permanent injury?– Are the deficits reversible and how much recovery
is expected?– What type of non-surgical intervention would be
helpful and when is surgical intervention indi-cated?
2.2. Referred symptoms
Referred numbness, tingling and/or pain usually hasa neurologic etiology, but many non-neurologic condi-tions can cause similar symptoms. Cardiac angina cancause pain to radiate into the left upper extremity. Di-aphragmatic irritation from a ruptured spleen can pro-duce referred pain into the shoulder. Osteoarthrosis ofthe hip can refer pain to the medial knee [82]. Triggerpoints can cause the referral of pain and even numbnessor tingling to many areas [83] in both the upper andlower extremities. Electrodiagnostic studies can helprule in or rule out a peripheral nerve injury as a causeof referred symptoms.

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 79
2.3. Chronicity of injury
EDXs can be used to determine whether an injury isacute or chronic and in some situations, the degree ofchronicity . Positive sharp waves take approximately7 days and fibrillation potentials take several weeks todevelop following axonal nerve injuries. The maxi-mum amount of abnormal spontaneous activity takes3 to 5 weeks from the time of injury to develop [7].Fibrillation potential amplitudes decrease in size overtime and their size can then be an indicator whetheran injury is acute or chronic. Both types of abnormalspontaneous activity are first found in the most proxi-mal muscles innervated by the injured nerve before be-ing detected distally. The presence of terminal collat-eral sprouting polyphasics (TCSPs) date the injury to atleast 3–4 weeks old. Axonal regeneration polyphasics(ARPs) date the injury to at least several months. Thepresence of giant motor units indicate an axonal injuryof at least several years.
2.4. Return to participation
Electrodiagnostic studies can help guide a physicianin making decisions about returning an athlete back toparticipation. Because electrodiagnostic abnormalitiescan lag well behind clinical recovery, they should not beused alone to decide when it is safe for an athlete to re-turn to practice or competition. Following a neurologicinjury, decisions about returning an athlete to partici-pation should be based on the overall clinical picture.The presence of weakness, a change in reflexes or lossof sensation does not automatically mean it is unsafefor the athlete to return to participate. The decisionmust be individualized, based on the functional perfor-mance, the sport and the athlete’s position. Neurologicdeficits such as residual weakness in the biceps maymake the athlete less effective on the playing field, butcarry less risk for re-injury or catastrophic injury thanthe limitations in neck motion from an incompletelyrehabilitated cervical root injury.
3. Common peripheral nerve injuries
3.1. The burner syndrome
One of the most commonly reported peripheral nerveinjury in athletes is the “burner” or “stinger”. Burnersare primarily seen in football and affect between 20%and 70% of college players [84–86]; however it also
Fig. 4. Atrophy of the rotator cuff following a complete tear.
occurs, less frequently in wrestling and hockey [84,87]. Burners have also been reported in boxers, weightlifters [88], and basketball players [89].
Several mechanisms of nerve injury have been de-scribed. A simultaneous depression of the ipsilat-eral shoulder and oblique extension or lateral flexionof the neck to the contralateral side was initially de-scribed [89]. This motion stretches the upper trunk ofthe brachial plexus and the upper (C5 and/or C6) cer-vical nerve roots and can lead to a traction nerve injury(Fig. 4). Some believe that ipsilateral neck oblique ex-tension leads to compression of the cervical root [90](Fig. 5) while others report that a direct blow to thesuperior aspect of the ipsilateral shoulder can injure theupper trunk of the brachial plexus [84] (Fig. 6). It islikely that all three mechanisms lead to “burner” symp-toms, but root compression from ipsilateral shoulderdepression and contralateral neck bending is the mostcommon in our athletes. Whether this is primarily acervical root or brachial plexus injury still remains con-troversial but our experience as well as recent litera-ture suggests that the cervical root is the more commonanatomic site [91].
An athlete who has sustained a “burner” will usu-ally complain of acute burning or stinging pain and/or

80 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
Fig. 5. Atrophy of the rotator cuff from a C5 radiculopathy.
Fig. 6. Atrophy of the infraspinatus secondary to a suprascapularneuropathy.
numbness radiating down one upper extremity [2].Symptoms usually last seconds to minutes and sud-den full recovery is the general rule. Weakness whenpresent is also usually transitory, but residual weaknessmay go undetected. The athlete will often deny neck
pain which may only be evident when full neck motionis tested. The Spurling’s maneuver (passive obliqueextension with axial compression) usually reproducesthe athletes symptoms and will confirm a nerve rootinjury. In a recent study, this was found to be posi-tive in 70% of athletes experiencing recurrent burnersymptoms [91]. Athletes will often keep their headin a flexed position to avoid the pain associated withroot compression. This potentially dangerous positioncould lead to “spear” tackling and increase the likeli-hood of a cervical cord injury. A positive Tinel’s signin the supraclavicular fossa may suggest upper trunkplexopathy. Any muscle of the C5 or C6 myotomecan be weak. Sensation will be decreased along theC5 and/or C6 dermatome and the biceps and brachio-radialis reflex (both are C5/C6 root and upper trunkinnervated muscles) may be decreased or absent. Thepronator teres reflex (C6/7 root, upper and middle trunkinnervated muscle) may also be reduced [92].
The shoulder should also be carefully exam-ined with burner symptoms since shoulder subluxa-tion/dislocations can also injure the plexus or periph-eral nerves, cause radiating symptoms and peripheralneurologic deficits [3,93]. Shoulder subluxations ordislocations are associated primarily with injuries tothe posterior cord or axillary nerve and can be distin-guished from a burner syndrome by the physical examfindings. They will often have a positive apprehensionsign of the shoulder and range of motion testing of theshoulder will usually be painful. One should look forother clinical signs of instability such as a sulcus sign,anterior drawer, and posterior drawer. The neck examshould be unremarkable. Neurologic deficitis will usu-ally correspond to an axilllary nerve or posterior corddistribution, but injuries to the suprascapular or mus-culocutaneous nerve are also associated with shouldertrauma.
3.1.1. Electrodiagnostic testingElectrodiagnostic studies are indicated when there
are persistant neurologic deficits and the degree of neu-rologic injury needs to be objectively identified. Theycan help localize the anatomic site of injury (nerve root,brachial plexus, peripheral nerve). For instance, nerveroot or proximal plexus injuries will be proximal to Er-b’s point and since Erb’s stimulation will be distal to thesite of injury nerve conduction velocities will be nor-mal. Motor amplitudes may be reduced with both rootand plexus injuries while sensory amplitudes are usu-ally reduced only with post-ganglionic cervical root,brachial plexus or isolated nerve injuries [7]. Nerve

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 81
conduction studies are necessary to rule out a more dis-tal peripheral nerve injury or an underlying peripheraldisorder.
The needle exam or EMG will not show evidenceof acute denervation within the first week. Therefore,motor unit recuitment patterns which can be reducedimmediately following the injury can be used as anearly EMG indicator of a severe neuropraxic or axonalinjury. In these cases, a repeat needle exam in twoto three weeks is usually recommended. Abnormalfindings in the cervical paraspinal muscles (posteriorrami innervated muscles) will help localize the injury tothe root level. The absence of positive sharp waves andfibrillation potentials however, does not absolutely ruleout a cervical root injury and rule in a brachial plexusinjury. There are three reasons for this: 1) It is possiblefor a cervical root injury to involve a select group ofnerve fasicles in the posterior primary ramus and leavethose of the posterior primary ramus uninjured, 2) Adistal root injury could involve the nerve beyond thepoint of departure of the posterior ramus and beforethe upper trunk of the brachial plexus has been formed,3) Downward traction of the upper extremity is likelyto create greater traction and injure the anterior ramusmore than the posterior ramus because the posteriorramus innervates and is anchored into the paraspinalmuscles.
Terminal collateral sprout polyphasic potentials(TCSP) identified within the first few weeks follow-ing injury signify this as a chronic or recurrent injury.Axonal regeneration polyphasic potentials (ARP) datethe injury back even further by at least several months.Both types of polyphasics can also be used to help de-fine the anatomic site of injury (i.e. plexus vs cervicalnerve root).
3.2. Suprascapular neuropathy
The suprascapular nerve is a branch off the uppertrunk of the brachial plexus, can come off the C5root rarely, and is the most common proximal periph-eral nerve injured. Fifty percent of the time it has aC4 contribution. It passes through the suprascapularnotch, its first common site of entrapment before in-nervating the supraspinatus muscle. The nerve thencontinues and passes through the spinoglenoid notch,the other common site of entrapment before innervat-ing the infraspinatus. Entrapment or traction at eithernotch can occur from a ganglion cyst, a hypertrophiedligament, an anomalous ligament or mechanical trac-tion [94–121]. Suprascapular neuropathies have been
reported in association with shoulder dislocations [93,122] or can be idiopathic as in Parsonage Turner Syn-drome [123]. Traction of the suprascapular nerve canoccur as it passes beneath the transverse scapula lig-ament during shoulder abduction and external rota-tion [94]. This has been described as the “sling effect”.It is likely that extreme scapular motion especially withsudden deceleration makes the suprascapular nerve sus-ceptible to injury at its two points of intimate associa-tion (suprascapular and spinoglenoid notches) with thescapula.
The suprascapular notch has been shown to varyanatomically [94] making the nerve more susceptibleto entrapment. Entrapment at the suprascapular notchhas been reported in baseball pitchers, tennis players,backpackers and weight lifters [106,119,120]. Weak-ness will be appreciated with shoulder elevation. Theathlete may have a positive shrug sign mimicking arotator cuff tear or a positive impingement sign mim-icking subacromial bursitis or rotator cuff tendonitis.Though the suprascapular nerve has no cutaneous sen-sation, shoulder pain is common with entrapments atthe suprascapular notch because of the sensation thenerve supplies to the scapula, glenohumeral joint andA-C joint.
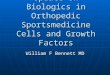
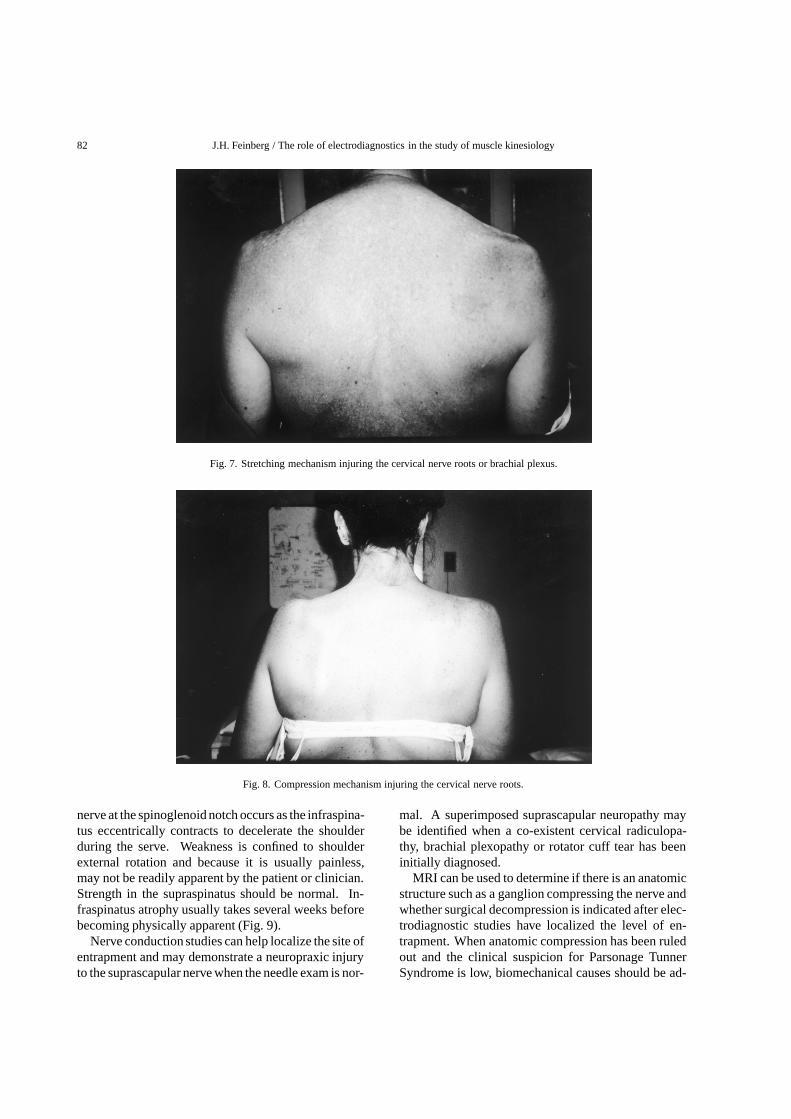
Muscle atrophy of the supraspinatus and infraspina-tus is common with suprascapular neuropathies, butcan also develop from disuse after a complete rota-tor cuff tear (Fig. 7). Wasting of the infraspinatus ismost easily noticed in the infrascapular fossa severalweeks after a suprascapular nerve injury. Because itis superficial and has well defined bony borders, it isalso often the first muscle to show visible signs of atro-phy with C5/6 radiculopathies or upper trunk brachialplexopathies (Fig. 8). This is because other C5/6 rootor upper brachial plexus trunk muscles such as the bi-ceps or deltoid have less well defined by boney land-marks. Atrophy may not be as obvious with incompletenerve injury. Similarly, supraspinatus atrophy whichalso occur, with entrapment in the suprascapular notch,may not be as obvious because of the overlying uppertrapezius muscle.
Entrapment at the spinoglenoid notch has been re-ported in pitchers, racquet sport players, volleyballplayers, a football player, a gymnast, a dancer andweight lifters [95,96,103,109,110,116,121,124,125].The use of an arm pulley on weight machines has alsoproduced a suprascapular neuropathy [124]. A supras-capular neuropathy at the level of the spinoglenoidnotch has been described in 12 of 96 asymptomatictop level volleyball players [113]. Compression of the
82 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
Fig. 7. Stretching mechanism injuring the cervical nerve roots or brachial plexus.
Fig. 8. Compression mechanism injuring the cervical nerve roots.
nerve at the spinoglenoid notch occurs as the infraspina-tus eccentrically contracts to decelerate the shoulderduring the serve. Weakness is confined to shoulderexternal rotation and because it is usually painless,may not be readily apparent by the patient or clinician.Strength in the supraspinatus should be normal. In-fraspinatus atrophy usually takes several weeks beforebecoming physically apparent (Fig. 9).
Nerve conduction studies can help localize the site ofentrapment and may demonstrate a neuropraxic injuryto the suprascapular nerve when the needle exam is nor-
mal. A superimposed suprascapular neuropathy maybe identified when a co-existent cervical radiculopa-thy, brachial plexopathy or rotator cuff tear has beeninitially diagnosed.
MRI can be used to determine if there is an anatomicstructure such as a ganglion compressing the nerve andwhether surgical decompression is indicated after elec-trodiagnostic studies have localized the level of en-trapment. When anatomic compression has been ruledout and the clinical suspicion for Parsonage TunnerSyndrome is low, biomechanical causes should be ad-

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 83
Fig. 9. Direct blow mechanism injuring brachial plexus.
dressed in the management of the nerve injury. For ath-letes engaged in throwing and racquet sports, scapularstability should be evaluated. The entire kinetic chainshould also be studied to look for limits in hip, trunk,and/or spine motion that might lead to compensatoryincreased motion in the shoulder.
3.2.1. Nerve conduction studies to the infraspinatusThe infraspinatus muscle can be studied with a skin
surface or intramuscular electrode. Obtaining a wave-form with a clear take-off is necessary when record-ing any CMAP. This is most easily obtained with asurface electrode placed over the infraspinatus musclebelly. The active electrode is placed 2 cm medial to thescapula’s medial border and 1 cm inferior to the spineof the scapula. The nerve is stimulated at Erb’s pointand the response is compared to the uninvolved side.Sometimes, the surface active electrode must be moveduntil a suitable CMAP is obtained. Amplitudes rangebetween 2mV and 4mV. Intramuscular electrodes willalso often require repositioning before an acceptableCMAP has been obtained. These amplitudes can rangefrom 15mV to 30mV. If both the latency and ampli-tude are similar bilaterally, further testing is not usuallynecessary. A prolonged latency or temporal dispersionindicates there is at least a neuropraxic injury to thesuprascapular nerve. Localization to the spinoglenoidnotch can be done if the latency to the supraspinatusmuscle is normal. A significantly decreased amplitudewith no change in latency means one of three things: 1)the site of pathology is proximal to Erb’s point (i.e. cer-
vical root vs upper trunk of plexus), 2) the suprascapu-lar neuropathy is axonal (i.e. Parsonage Turner Syn-drome), 3) the active electrode is not properly placed.
3.2.2. Nerve conduction studies to the supraspinatusAn intramuscular electrode must be used when
studying conduction to the supraspinatus muscle. Aneedle is inserted 1 cm superior to the suprascapularspine approximately midway from the medial scapulaborder. The needle is passed downward through the up-per trapezius, supraspinatus and then withdrawn 0.5 cmafter hitting the periosteum of the suprascapular fossa.The needle often needs to be repositioned in order toobtain a CMAP with a clear take-off. This is then com-pared to the uninvolved side. If the latency is signifi-cantly prolonged then the site of injury is most likely ator proximal to the suprascapular notch. Because seg-mental conduction studies of the suprascapular nerveare technically difficult, one can not assume that a pro-longed distal latency to the supraspinatus or abnormalEMG findings in the supraspinatus localize entrapmentat the suprascapular. If the latency is normal, at thesupraspinatus but was prolonged when recording fromthe infraspinatus then the site of injury is most likelyat the spinoglenoid notch. These results will coincidewith the needle exam when there is axonal degenera-tion.
3.3. Axillary neuropathy
The axillary nerve is the last branch of the posteriorcord before it becomes the radial nerve. A branch inner-

84 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
vates the teres minor before coursing through the quad-rangular space, a common site of entrapment and theninnervates the deltoid. Its cutaneous branch suppliesa small area of sensation in the proximal and lateralregion of the shoulder.
Athletes with axillary nerve injuries will complain ofweakness in the shoulder and may have subtle weaknessin shoulder external rotation from involvement of theteres minor. They are often unaware of the loss ofproximal shoulder sensation until it is tested on physicalexam. Atrophy may be appreciated by noting a moreprominent A-C joint or acromion on the symptomaticside.
Axillary nerve injuries are the most common pe-ripheral nerve injured with anterior shoulder disloca-tions, occurring in 9–18% of patients [98,126–130].They can result from compression secondary to teth-ering within the quadrangular space, from mechani-cal traction, or from a direct blow to the quadrangularspace [131]. Neuralgia amyotrophy can also lead toan isolated axillary nerve palsy [132] and has been re-ported in baseball players [133], a football player [131,134] and wrestling [131].
Vascular compression syndromes can simulate ax-illary nerve injuries. A thrower was reported to haveweakness, numbness, and pain in the shoulder duringfull abduction and rotation of the shoulder. Electro-diagnostic studies were normal, but vascular studiesdemonstrated quadrilateral space compression of theposterior humeral circumflex artery [135].
3.3.1. Nerve conduction studies of the axillary nerveNerve conduction studies are done when the needle
exam is normal to rule out a neuropraxic injury andto rule out a superimposed axillary nerve injury whena C5/C6 radiculopathy or upper trunk plexopathy hasalso been diagnosed. Both skin surface or intramus-cular electrodes can be used to record a potential or awaveform. A CMAP with a clear take-off can be ob-tained by placing the active electrode over the middledeltoid 2/3 distal from the tip of the acromium. Theresponse should be compared to the uninvolved side.A prolonged distal latency and/or temporal dispersionindicates a neuropraxic axillary nerve injury. A lowamplitude with a normal latency indicates one of threethings: 1) the site of pathology is proximal to Erb’spoint (i.e. cervical root vs upper trunk of plexus), 2) theaxillary neuropathy is axonal (i.e. Parsonage TurnerSyndrome), 3) the active electrode is not properly po-sitioned.
3.4. Ulnar neuropathy
The ulnar nerve is a continuation of the medial cordof the brachial plexus after it sends a branch to join thelateral cord to from the median. It runs medially downthe arm where it passes under the Arcade of Struthers,absent in 30% of patients [136] and through the ulnargroove deep to the two bands of the ulnar collateralligament. It then courses through the two heads of theflexor carpi ulnaris, the cubital tunnel, and then passesthrough Guyon’s canal in the volar wrist before givingoff the digital nerve branches to supply sensation to the4th and 5th fingers.
Traction overload of the ulnar nerve can occur in theulnar groove from valgus overload in baseball [137–139], football and javelin throwers; in the cubital tun-nel from muscle hypertrophy in stickhandlers and agolfer [140]; and in guyon’s canal from handelbar com-pression in cylcists [141]. Compression from a hy-pertrophied medial triceps head has been reported inweight lifters [142]. Athletes will complain of numb-ness and/or tingling in digits 4 and 5. Weakness will bepresent in the hand intrinsics with entrapment in guy-on’s canal, in the hand intrinsics and flexor digitorumprofundus4 and 5 with entrapment in the cubital tunnel,and in the hand intrinsics, flexor digitorum profundus4 and 5, and the flexor carpi ulnaris with entrapment atthe ulnar groove. Atrophy can usually first be detectedby checking muscle bulk in the first dorsal interosseous.
3.4.1. Nerve conduction studies of the ulnar nerveBecause of the superficial course of the ulnar nerve,
precise localization should be standard during EDXs.It is essential for both surgical planning or conservativemanagement. When the 5th digital ulnar nerve sensoryamplitude is decreased, comparing side to side differ-ences in the dorsal ulnar cutaneous nerve can help rulein or out entrapment at the wrist in guyon’s canal [143].Segmental conduction from the palm to wrist will showslowing (< 50 meters/sec) and can be compared to seg-mental conduction of the median nerve in the palm towrist. Entrapment in Guyon’s canal can lead to den-ervation of the hand intrinsics and an abnormal nee-dle exam. If the dorsal ulnar cutaneous nerve is alsodecreased, one can compare amplitudes of the medialantebrachial cutaneous nerves in both sides. A signif-icantly decreased amplitude suggests a site of injuryproximal to the elbow while similar amplitudes indi-cates compression at or below the elbow.
Segmental stimulation or the inching technique de-scribed by Kimura [144] can often pinpoint localization

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 85
to differentiate between an ulnar groove verses cubitaltunnel entrapment. When using the inching techniqueand measuring across short distances, conduction ve-locities are unreliable. A more accurate and physio-logic way is to look for a drop in CMAP amplitude withtemporal dispersion.
Segmental stimulation of the ulnar mixed nerveacross the elbow has been described [145]. Stimulat-ing the ulnar nerve at a distal site below the elbow andrecording proximally above the elbow can help elim-inate motor artifact. This technique also allows oneto study the entire ulnar nerve rather than the smallpercentage of fibers studied when recording the moretraditional CMAP. Nevertheless, Kothari et al foundthat CMAP recording with segmental ulnar nerve con-duction studies performed orthodromically is the moresensitive technique [146]. Regardless of the segmentaltechnique used, repeating the conduction studies canhelp minimze the measurement error inherent in study-ing nerve conductions across short distances.
4. Conclusion
Peripheral nerve injuries can lead to significant dis-ability in any patient. The great demands of athleticsincreases the risk of these injuries. Early detection isessential to minimize permanent deficits and to enablethe athlete to return to participation with minimal de-lay. Electrodiagnostic studies help the clinician identifythese injuries particularly when the symptoms are in-sidious or the athlete is well conditioned and motivated.They can help objectively quantify neurologic damageand prognosticate neurologic recovery. Electrodiag-nostic studies have also been used in sports medicine tohelp us better understand muscle kinesiology, musclefatigue and devise appropriate exercise programs forbetter performance and rehabilitation programs.
Acknowledgements
I would like to thank Jane Flannery for her assistancein preparation of this manuscript and Dr. Alice Chenand Dr. Jay Bowen for their comments.
References
[1] Seddon H, Three types of nerve injury, Brain 66 (1943),237–288.
[2] Rockett F, Observations on the burner: traumatic cervicalradiculopathy, Clin Orthop 164 (1982), 18.
[3] Travlos J, Goldberg I and Boome R, Brachial plexus lesionsassociated with dislocated shoulders, J Bone Joint Surg Br72 (1990), 68–71.
[4] Sunderland S, The anatomy and physiology of nerve injury,Muscle Nerve 13 (1990), 771–784.
[5] Bonney G, Iatrogenic Injuries of Nerves, J Bone Joint SurgBr 68 (1986), 9–13.
[6] Wall EJ, Massie JB, Kwan MK, et al., Experimental stretchneuropathy; changes in nerve conduction under tension, JBone Joint Surg Br 74 (1992), 126–129.
[7] Wilbourn, A, Electrodiagnosis of Plexopathies, NeurologClinics 3(3) (1985), 511–528.
[8] Ma D. and Liveson JA, Nerve Conduction Handbook,Philadelphia, F.A. Davis Company, 1983.
[9] DeLisa J.A., Lee H.G., Baran E.M., Lai K. and Spielholz N,Manual of nerve conduction velocity and clinical neurophys-iology, Raven Press 3rd ed., New York 1994.
[10] Feinstein B., Lindegard B., Nyman E., et al., Morphologicstudies of motor units in normal human muscles, Acta Anat23 (1995), 124–142.
[11] Garrett W E. Jr., Mumma M and Lucaveche C L., Ultra-structural differences in human skeletal muscle fiber types,Orthop Clinics No America 14(2) (1983), 413–425.
[12] Linssen W, Im HJP, Stegeman DF, Joosten MG, BinkhorstRA, Merks Mieke JH, Ter Laak HJ and Notermans ServaasLH, Fatigue in Type I fiber predominance: A muscle forceand surface EMG study on the relative role of Type I andType II muscle fibers, Muscle Nerve 14 (1991), 829–837.
[13] Hannaford B and Lehman S, Short time fourier analysis ofthe electromyogram: fast movements and constant contrac-tion, IEEE Transactions of Biomed Engineering BME 33(12)(1986), 1173–1181.
[14] Mannion AF, Dumas GA, Stevenson JM and Cooper RG, Theinfluence of muscle fiber size and type distribution on elec-tromyographic measures of back muscle fatigability, SPINE23(5) (1998), 576–584.
[15] Moritani T, Nagata A and Muro M, Electromyographic man-ifestations of muscle fatigue, Med Sci Sports Exer 14(3)(1982), 198–202.
[16] Stulen FB and De Luca CJ, Muscle fatigue monitor: A nonin-vasive device for observing localized muscular fatigue, IEEETrans Biomed Eng 29 (1982), 760.
[17] Rohter F and Hyman C, Blood flow in arm and finger duringmuscle contraction and joint position changes, J Appl Physiol17(5) (1962), 819–823.
[18] Jarvholm U, Styf J, Suurkula M and Herberts P, Intramuscularpressure and muscle blood flow in supraspinatus, Eur J ApplPhysiol 58 (1988), 219–224.
[19] Merletti R, Knaflitz M and DeLucaCJ, Myoelectric manifes-tations of fatigue in voluntary and electrically elicited con-traction, J Appl Physiol 69 (1990), 1810–1820.
[20] Grabiner MD, Koh TJ and Miller GF, Fatigue rates of vas-tus medialis oblique and vastus lateralis during static anddynamic knee extension, J Orthop Res 9 (1991), 391–397.
[21] Roy SH, De Luca CJ, Synder-Mackler L, Emley MS, Cren-shaw RL and Lyons JP, Fatigue, recovery, and low back painin varsity rowers, Med Sci Sports Exerc 22(4) (1990), 463–469.
[22] Hagberg, M, Electromyographic signs of shoulder muscularfatigue in two elevated arm positions, Am J Phys Med 60(1981), 111–121.
86 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
[23] Krivickas LS, Nadler SF, Davies MR, Petroski GF and Fein-berg JH, Spectral analysis during fatigue, Am J Phys MedRehabil 75 (1996), 1139–1143.
[24] Davis BA, Krivickas LS, Maniar R, Newandee DA and Fein-berg JH, The reliability of monopolar and bipolar fine wireelectromyographic measurement of muscle fatigue, Med SciSports Exerc 30 (1998), 1328–1335.
[25] Inman VT, Saunders JB and Abbot LC, Observations on thefunction of the shoulder joint, J Bone Joint Surg 26 (1944),1–30.
[26] Shevlin MG, Lehmann J, Feinberg MD and Lucci JA, Elec-tromyographic study of the function of some muscles cross-ing the glenohumeral joint, Arch Phys Med Rehabil 50(1969), 264–270.
[27] VanderHelm FC, Analysis of the kinematic and dynamicbehavior of the shoulder mechanism, J Biomed 27 (1994),527–550.
[28] Kronberg M, Nmeth G and Brostrm, L, Muscle activity andcoordination in the normal shoulder. An electromyographicstudy, Clin Orthop Relat Res 257 (1990), 76–85.
[29] Kronberg M, Brostrm L and Nmeth G, Differences in shoul-der muscle activity between patients with generalized jointlaxity and normal controls, Clin Orthop Relat Res 269 (1991),181–192.
[30] Pande P, Hawkins R and Peat M, Electromyography in vol-untary posterior instability of the shoulder, Am J Sports Med17(5) (1989), 644–648.
[31] Mariani PP and Caruso I, An electromyographic investiga-tion of subluxation of the patella, J Bone Joint Surg Br 61B(1979), 169–171.
[32] Souza DR and Gross MT, Comparison of vastus medialisobliquus: vastus lateralis muscle integrated electromyo-graphic ratios between healthy subjects and patients withpatellofemoral pain, Phys Ther 71 (1991), 310–320.
[33] Boucher JP, King MA, Lefebvre R and Pepin A, Quadricepsfemoris muscle activity in patellofemoral pain syndrome, AmJ Sports Med 20 (1992), 527–532.
[34] Sczepanski TL, Gross MT, Duncan PW and Chandler JM,Effect of contraction type, angular velocity, and arc of motionon VMO:VL EMG ratio, J Orthop Sports Phys Ther 14(1991), 256–262.
[35] Voight Ml and Wieder DL, Comparative reflex response timesof vastus medialis obliquus and vastus lateralis in normalsubjects and subjects with extensor mechanism dysfunction,Am J Sports Med 19 (1991), 131–137.
[36] Reynolds L, Levin TA, Medeiros JM, Adler NS and HallumA, EMG activity of the vastus medialis oblique and the vastuslateralis in their role in patellar alignment, Am J Phys Med62 (1983), 61–69.
[37] Basmajian JV, Harden TP and Regenos EM, Integrated ac-tions of the four heads of quadriceps femoris: an electromyo-graphic study, Anat Rec 172 (1971), 15–20.
[38] Jobe FW, Tibone JE, Perry J and Moynes D, An EMG analysisof the shoulder in pitching, Am J Sports Med 11(1) (1983),3–5.
[39] Jobe FW, Moynes D, Tibone JE and Perry J, An EMG analysisof the shoulder in pitching, Am J Sports Med 12(3) (1984),218–220.
[40] Glousman R, Jobe F, Tibone J, Moynes D, Antonelli D andPerry J, Dynamic electromyographic analysis of the throwingshoulder with glenohumeral instability, J Bone Joint Surg Am70 (1988), 220–226.
[41] Glousman RE, Barron J, Jobe FW, Perry J and Pink M, Anelectromyographic analysis of the elbow in normal and in-
jured pitchers with medial collateral ligament insufficiency,Am J Sports Med 20(3) (1992), 311–317.
[42] Nuber GW, Jobe FW, Perry J, Moynes DR and AntonelliD, Fine wire electromyography analysis of muscles of theshoulder during swimming, Am J Sports Med 14(1) (1986),7–11.
[43] Scovazzo ML, Browne A, Pink M, Jobe FW and KerriganJ, The painful shoulder during freestyle swimming: an elec-tromyographic cinematographic analysis of twelve muscles,Am J Sports Med 19(6) (1991), 577–582.
[44] Anderson MB, Comparison of muscle patterning in the over-arm throw and tennis serve, Research Quarterly 50(4) (1979),541–553.
[45] Morris M, Jobe FW, Perry J, Pink M and Healy BS, Elec-tromyographic analysis of elbow function in tennis players,Am J Sports Med 17(2) (1989), 241–247.
[46] Giangarra CE, Conroy B, Jobe FW, Pink M and Perry J,Electromyographic and cinematographic analysis of elbowfunction in tennis players using single- and double-handedbackhand strokes, Am J Sports Med 21(3) (1993), 394–399.
[47] Jobe FW, Perry J and Pink M, Electromyographic shoulderactivity in men and women professional golfers, Am J SportsMed 17(6) (1989), 782–787.
[48] Pink M, Perry J and Jobe FW, Electromyographic analysis ofthe trunk in golfers, Am J Sports Med 21(3) (1993), 385–388.
[49] Bechler JR, Jobe FW, Pink M, Perry J and Ruwe PA, Elec-tromyographic analysis of the hip and knee during the golfswing, Clin J Sport Med 5(3) (1995), 162–166.
[50] Jorge M and Hull ML, Analysis of EMG measurements dur-ing bicycle pedaling, J Biomech 19 (1986), 683–694.
[51] deGroot G. Welbergen E, Clijsen L, Clarijs J, Cabri J and An-tonis J, Power, muscle work, and external forces in cycling,Ergonomics 37(1) (1994), 31–42.
[52] Montgomery WH, Pink M and Perry J, Electromyographicanalysis of hip and knee musculature during running, Am JSports Med 22 (1994), 272–278.
[53] Reber L, Perry J and Pink M, Muscular control of the anklein running, Am J Sports Med 21 (1993), 805–810.
[54] Trepman E, Gellman RE, Solomon R, Murthy KR, MicheliLJ and DeLuca CJ, Electromyographic analysis of standingposture and demi-plie in ballet and modern dancers, Med SciSports Exerc 26 (1994), 771–782.
[55] Feinberg JH, Electromyography and the study of muscle ki-nesiology and fatigue, Sports Neuro, 2nd ed., Philadelphia:Lippincott-Raven Publishers, 1998, pp. 77–90.
[56] Bradley JP and Tibone JE, Electromyographic analysis ofmuscle action about the shoulder, Clinics Sports Med 10(4)(1991), 789–805.
[57] Basmajian JV and DeLuca CJ, Muscles alive: their functionsrevealed by electromyography, 5th ed., Baltimore: Williamsand Wilkins, 1988, pp. 1–21.
[58] Rowlands LK, Wertsch JJ, Primack SJ, Spreitzer AM andRoberts MM, Kinesiology of the empty can test, Am J PhysMed Rehabil 74 (1995), 302–304.
[59] Jenp YN, Malanga GA, Growney ES and An KN, Activationof the rotator cuff in generating isometric shoulder rotationtorque, Am J Sports Med 24(4) (1996), 477–485.
[60] Stefko J, Jobe FW, VanderWilde RS, Carden E and Pink M,Electromyographic and nerve block analysis of the subscapu-laris liftoff test, J Shoulder Elbow Surg 6 (1997), 347–355.
[61] Pappas AM, Zawacki RM and McCarthy CF, Rehabilitationof the pitching shoulder, AM J Sports Med 14(1) (1986),7–11.

J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology 87
[62] Townsend H, Jobe FW, Pink M and Perry J, Electromyo-graphic analysis of the glenohumeral muscles during a base-ball rehabilitation program, Am J Sports Med 19 (1991),264–272.
[63] Moseley JB Jr, Jobe FW, Pink M, Perry J and Tibone J,EMG analysis of the scapular muscles during a shoulderrehabilitation program, Am J Sports Med 20(2) (1992), 128–134.
[64] McCann PD, Wootten ME, Kadaba MP and Bigliani LU,Kinematic and electromyographic study of shoulder rehabil-itation exercises, Clin Orthop 288 (1993), 179–188.
[65] Ballantyne BT, O’Hare SJ, Paschall JL, Pavia-Smith MM,Pitz AM, Gillon JF and Soderberg GL, Electromyographicactivity of selected shoulder muscles in commonly used ther-apeutic exercises, Phys Ther 73 (1993), 668–682.
[66] Cordasco FA, Wolfe IN, Wootten ME and Bigliani L, Anelectromyographic analysis of the shoulder during a medicineball rehabilitation program, Am J Sports Med 24(3) (1996),386–392.
[67] Pocock GS, Electromyographic study of the quadriceps dur-ing resistive exercise, J Am Phys Ther Assoc 43 (1963), 427–434.
[68] Allington R, Baxter, ML, Koepke GH and Christopher RP,Strengthening techniques of the quadriceps muscles; an elec-tromyographic evaluation, J Am Phys Ther Assoc 46 (1966),1173–1176.
[69] Gough HV and Ladley G, An investigation into the effective-ness of various forms of quadriceps extension, Phys Ther 57(1971), 356–361.
[70] Skurja M, Perry J, Cronley J and Hislop HJ, Quadricepsaction in straight leg raise versus isolated knee extension(EMG and tension study), Phys Ther 60 (1980), 582.
[71] Antich TJ and Brewster CE, Modification of quadricepsfemoris muscle exercises during knee rehabilitation, PhysTher 66 (1985), 1246–1251.
[72] Soderberg GL, Minor SD, Arnold K, et al., Electromyo-graphic analysis of knee exercises in healthy subjects and inpatients with knee pathologies, Phys Ther 67 (1987), 1691–1696.
[73] Hanten WP and Schulthies SS, Exercise effect on elec-tromyographic activity of the vastus medialis oblique andvastus lateralis muscles, Phys Ther 70 (1990), 561–565.
[74] Baratta R, Solomonow M, Zhour BH, Letson ED, ChuinardR and D’Ambrosia R, Muscular coactivation: the role of theantagonist musculature in maintaining knee stability, Am JSports Med 16 (1988), 113–122.
[75] Gryzlo SM, Patek RM, Pink M and Perry J, Electromyo-graphic analysis of knee rehabilitation exercises, J OrthopSports Phys Ther 20 (1994), 36–43.
[76] Carlson S and Nordstrand A, The coordination of the kneemuscles in some voluntary movements and in the gait in caseswith and without knee injuries, Acta Chir Scand 134 (1968),423.
[77] Branch TP, Hunter R and Donath M, Dynamic EMG analysisof anterior cruciate deficient legs with and without bracingduring cutting, Am J Sports Med 17 (1989), 35–41.
[78] Lutz GE, Palmitier RA, An KN and Chao EY, Comparison oftibiofemoral joint forces during open kinetic chain and closekinetic chain exercises, J Bone Joint Surg Am 75A (1993),732–739.
[79] Tibone JE, Antich MS, Fanton GS, Moynes DR and Perry J,Functional analysis of anterior cruciate ligament instability,Am J Sports Med 14 (1986), 276–284.
[80] Limbird TJ, Shiavi R, Frazer M and Borra H, EMG profiles ofknee joint musculature during walking; changes induced byanterior cruciate ligament deficiency, J Orthop Res 6 (1988),630–638.
[81] Moritani T, Muramatsu S and Muro M, Activity of motorunits during concentric and eccentric contractions, Am J PhysMed 66 (1988), 338–351.
[82] Turek SL, Orthopaedics: principles and their application,Philadelphia: Lippincott, 1984, pp. 1109–1268.
[83] Travell J and Simons DG, Myofascial pain and dysfunction,The trigger point manual. Baltimore: Williams and Wilkins,1983.
[84] DiBenedetto M and Markey K, Electrodiagnostic localizationof traumatic upper trunk brachial plexopathy, Arch Phys MedRehabil 65 (1984), 15–17.
[85] Clancy W, Bergfeld JA, Brand R, et al., Upper trunk brachialplexus injuries in contact sports, Am J Sports Med 5(5)(1977), 209–216.
[86] Sallis R, Jones K and Knopp W, Burners: offensive strategyfor an underreported injury, Phys Sportsmed 20(11) (1992),47–55.
[87] Wroble RR and Albright JP, Neck and low back injuries inwrestling, Clin Sports Med 5(2) (1986), 295–325.
[88] Wilbourn AJ, Electrodiagnostic testing of neurologic injuriesin athletes, Clin Sports Med 9(2) (1990), 229–245.
[89] Chrisman OD and Snook GA, Lateral-flexion neck injuriesin athletic competition, JAMA 192 (1965), 117.
[90] Watkins RG, Nerve injuries in football players, Clin SportsMed 5 (1986), 215–246.
[91] Levitz C, Reilly P and Torg J, The pathomechanics of chronic,recurrent cervical nerve root neurapraxia, Am J Sports Med25(1) (1997), 73–76.
[92] Malanga GA and Campagnolo DI, Classification of thepronator reflex, Am J Phys Med Rehabil 73 (1994), 338–340.
[93] Liveson J, Nerve lesions associated with shoulder disloca-tion: an electrodiagnostic study of 11 cases, J Neurol Neu-rosurg Psychiatry 47 (1984), 742–744.
[94] Regarchary S, Burr D, Lucas S, et al., Suprascapular entrap-ment neuropathy: a clinical, anatomical, and comparativestudy, Neurosurg 5(4) (1979), 447–451.
[95] Thompson R, Schneider W and Kennedy T, Entrapment neu-ropathy of the inferior branch of the suprascapular nerve byganglia, Clin Orthop 166 (1982), 185–187.
[96] Liveson J, Bronson M and Pollack M, Suprascapular nervelesions at the spinogleonid notch: report of three cases andreview of the literature, J Neurol Neurosurg Psychiatry 54(1991), 241–243.
[97] Alon M, Weiss S, Fishel B, et al., Bilateral suprascapular en-trapment syndrome due to an anomalous transverse scapularligament, Clin Orthop 234 (1988), 31–33.
[98] Aiello I, Serra G, Traina GC, et al., Entrapment of the supras-capular nerve at the spinoglenoid notch, Ann Neurol 12(3)(1982), 314–316.
[99] Kiss G and Komar J, Suprascapular nerve compression at thespinoglenoid notch, Muscle Nerve 13 (1990), 556–557.
[100] Henlin J, Rousselot J, Monnier G, et al., Suprascapular nerveentrapment at the spinoglenoid notch (in French), Rev Neurol(Paris) 148(5) (1992), 362–367.
[101] Glennon T, Isolated injury to the infraspinatus branch ofthe suprascapular nerve, Arch Phys Med Rehabil 73 (1992),201–202.
[102] Steinman I, Painless infraspinatus atrophy due to suprascapu-lar nerve entrapment, Arch Phys Med Rehabil 69 (1988),641–643.
88 J.H. Feinberg / The role of electrodiagnostics in the study of muscle kinesiology
[103] Bryan WJ and Wild JJ, Isolated infraspinatus atrophy: acommon cause of posterior shoulder pain and weakness inthrowing athletes, Am J Sports Med 17 (1989), 130–131.
[104] Callahan J, Scully T, Shapiro SA, et al., Suprascapular nerveentrapment, J Neurosurg 74 (1991), 893–896.
[105] Hirayama T and Takemitsu Y, Compression of the supras-capular nerve by a ganglion at the suprascapular arch, ClinOrthop 155 (1981), 95–96.
[106] Hadley M, Sonntag V and Pittman H, Suprascapular nerveentrapment, J Neurosurg 64 (1986), 843–848.
[107] Torres-Ramos F and Biundo J, Suprascapular neuropathyduring progressive resistive exercises in a cardiac rehabilita-tion program, Arch Phys Med Rehabil 73 (1992), 1107–1111.
[108] Takagishi K, Maeda K, Ohimi H, et al., Ganglion causingparalysis of the suprascapular nerve, Acta Orthop Scand62(4) (1991), 391–393.
[109] Ganzhorn RW, Hocker JT, Horowitz M, et al., Suprascapularnerve entrapment, J Bone Joint Surg Am 63 (1981), 492–494.
[110] Jackson D, Farrage J, Hynninen BC, et al., Suprascapularneuropathy in athletes: case reports, Clin J Sports Med 5(2)(1995), 134–137.
[111] Vastamaki M and Goransson H, Suprascapular nerve entrap-ment, Clin Orthop Relat Res 297 (1993), 135–143.
[112] Zuckerman J, Polonsky L and Edelson G, Suprascapularnerve palsy in a young athlete, Bull Hosp Jt Dis 53(2) (1993),11–12.
[113] Ferretti A, Cerullo G and Russo G, Suprascapular neuropathyin volleyball players, J Bone Joint Surg Am 69 (1987), 260–263.
[114] Garcia G and McQueen D, Bilateral suprascapular nerveentrapment syndrome, J Bone Joint Surg Am 63 (1981), 491–492.
[115] Fritz R, Helms C, Steinbach LS, et al., Suprascapular nerveentrapment: evaluation with MR imaging, Radiology 182(1992), 437–444.
[116] Kukowski B, Suprascapular nerve lesion as an occupationalneuropathy in a semiprofessional dancer, Arch Phys MedRehabil 74(70) (1993), 768–769.
[117] Clein LJ, Suprascapular entrapment neuropathy, J Neurosurg43 (1975), 337–342.
[118] Post M and Mayer J, Suprascapular nerve entrapment: diag-nosis and treatment, Clin Orthop 223 (1987), 126–136.
[119] Agre J, Ash N, Cameron MC, et al., Suprascapular neuropa-thy after intensive progressive resistive exercise: case report,Arch Phys Med Rehabil 68(4) (1987), 236–238.
[120] Ringle S, Treihaft M, Carry M, et al., Suprascapular neu-ropathy in pitchers, Am J Sports Med 18(1) (1990), 80–86.
[121] Smith AN, Suprascapular neuropathy in collegiate pitcher, JAthl Train 30(1) (1995), 43–46.
[122] Zoltan J, Injury to the suprascapular nerve associated withanterior dislocation of the shoulder: case report and reviewof the literature, J Trauma 19(3) (1979), 203–206.
[123] Parsonage MJ and Turner JWA, Neuralgic amyotrophy: theshoulder-girdle syndrome, Lancet I (1948), 973–978.
[124] Goodman CE, Unusual nerve injuries in recreational activi-
ties, Am J Sports Med 11(4) (1983), 224–7.126.[125] Laulund T, Fedders O, Sogaard I, et al., Suprascapular nerve
compression syndrome, Surg Neurol 22 (1984), 308–312.[126] Hoyt W, Etiology of shoulder injuries in adults, J Bone Joint
Surg Am 49 (1967), 755–766.[127] Brown JT, Nerve injuries complicating dislocation of the
shoulder, J Bone Joint Surg Br 34 (1972), 526.[128] Neviaser R, Neviaser T and Neviaser J, Concurrent rupture of
the rotator cuff and anterior dislocation of the shoulder in theolder patient, J Bone Joint Surg Am 70 (1988), 1308–1311.
[129] Pasila M, Jaroma H, Kiviluoto O, et al., Early complicationsof primary shoulder dislocations, Acta Orthop Scand 49(3)(1978), 260–263.
[130] Artico M, Isolated lesion of the axillary nerve, Neurosurg 29(1991), 697–700.
[131] Bateman JE, Nerve injuries about the shoulder in sports, JBone Joint Surg Am 49 (1967), 755–766.
[132] Neuralgic amyotrophy: still a clinical syndrome (editorial),Lancet II(8197) (1980), 729–730.
[133] Bennett G, Shoulder and elbow lesions of the professionalbaseball player, JAMA 117 (1941), 510–514.
[134] Kessler K and Uribe J, Complete isolated axillary nerve palsyin college and professional football players: a report of sixcases, Clin J Sports Med 4(4) (1994), 272–274.
[135] Redler M, Ruland L and McCue F, Quadrilateral space syn-drome in a throwing athlete, Am J Sports Med 14(6) (1986),511–513.
[136] Wadsworth TG and Williams JR, Cubital tunnel externalcompression syndrome, BMJ 1 (1973), 662–666.
[137] Hang YS, Tardy ulnar neuritis in a little league baseballplayer, Am J Sports Med 9 (1981), 244–246.
[138] Glousman RE, Ulnar nerve problems in the athlete’s elbow,Clin Sports Med 9 (1990), 365–377.
[139] Jobe FW and Nuber G, Throwing injuries of the elbow, ClinSports Med 5 (1986), 621–636.
[140] Campbell WW, Pridgeon RM and Salmi SK, Entrapmentneuropathy of the ulnar nerve at its point of exit from theflexor carpi ulnaris muscle, Muscle Nerve 11 (1988), 467–470.
[141] Eckman PB and Perlstein G, Altrocchi PH. Ulnar neuropathyin bicycle riders, Arch Neurol 32 (1975), 130–131.
[142] Dangles CJ and Bilos ZJ, Ulnar neuritis in a world championweightlifter, Am J Sports Med 8 (1980), 443–445.
[143] Bromberg MA and Jaros L, Symmetry of normal motor andsensory nerve conduction measurements, Muscle Nerve 21(1998), 498–509.
[144] Kimura J, Principles and pitfalls of nerve conduction studies,Ann Neurol 16 (1984), 415–429.
[145] Raynor EM, Shefner JM, Preston DC and Logigian EL, Sen-sory and mixed nerve conduction studies in the evaluationof ulnar neuropathy at the elbow, Muscle Nerve 17 (1994),785–792.
[146] Kothari MJ, Heistand M and Rutkove S, Three ulnar nerveconduction studies in patients with ulnar neuropathy at theelbow, Arch Phys Med Rehabil 79 (1998), 87–89.