Embed Size (px)
Citation preview

384 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
University of Zagreb School of Medicine, Department of Cardiovascular Diseases, University Hospital Center Zagreb, Kišpaticeva 12, 10000 Zagreb, Croatia (M. Cikes). St George’s Hospital, Blackshaw Road, Tooting, London SW17 0QT, UK (G. R. Sutherland, L. J. Anderson). Catalan Institution for Research and Advanced Studies, Universitat Pompeu Fabra, Carrer Tànger 122–140, 08018 Barcelona, Spain (B. H. Bijnens).
Correspondence to: M. Cikes maja_cikes@ yahoo.com
The role of echocardiographic deformation imaging in hypertrophic myopathiesMaja Cikes, George R. Sutherland, Lisa J. Anderson and Bart H. Bijnens
Abstract | Echocardiography has a leading role in the routine assessment and diagnosis of hypertrophic ventricles. However, the use of M‑mode echocardiography and measurement of global left ventricular function may be misleading. Traditionally, systolic function was thought to be preserved in patients with hypertrophic myopathies until the late stages of the disease, and hypertrophic myopathies were thought to affect the myocardium more diffusely than ischemic heart disease. Ultrasound deformation imaging, either by Doppler myocardial imaging or speckle tracking, provides more‑sensitive detection of regional myocardial motion and deformation than standard echocardiography. Basic and clinical studies that apply these techniques have revealed early, often subclinical impairment in systolic function. This information allows the detection and treatment of myocardial dysfunction at an early stage, which is of high clinical importance. Physiological hypertrophic remodeling seen in athletes differs from pathological myocardial hypertrophy, which can be caused by compensatory reactive hypertrophy owing to pressure overload in patients with aortic stenosis or hypertension, as well as amyloidosis, Fabry disease or Friedreich ataxia. Each of the etiologies associated with hypertrophy demonstrate distinct regional changes in myocardial deformation, which allows identification of the underlying processes, and will improve the assessment and follow‑up of patients with hypertrophic myopathies.
Cikes, M. et al. Nat. Rev. Cardiol. 7, 384–396 (2010); published online 11 May 2010; doi:10.1038/nrcardio.2010.56
IntroductionHypertrophy of the myocardium often occurs in response to a discrepancy between available pump performance and an increased demand in work. Physiological hypertrophic
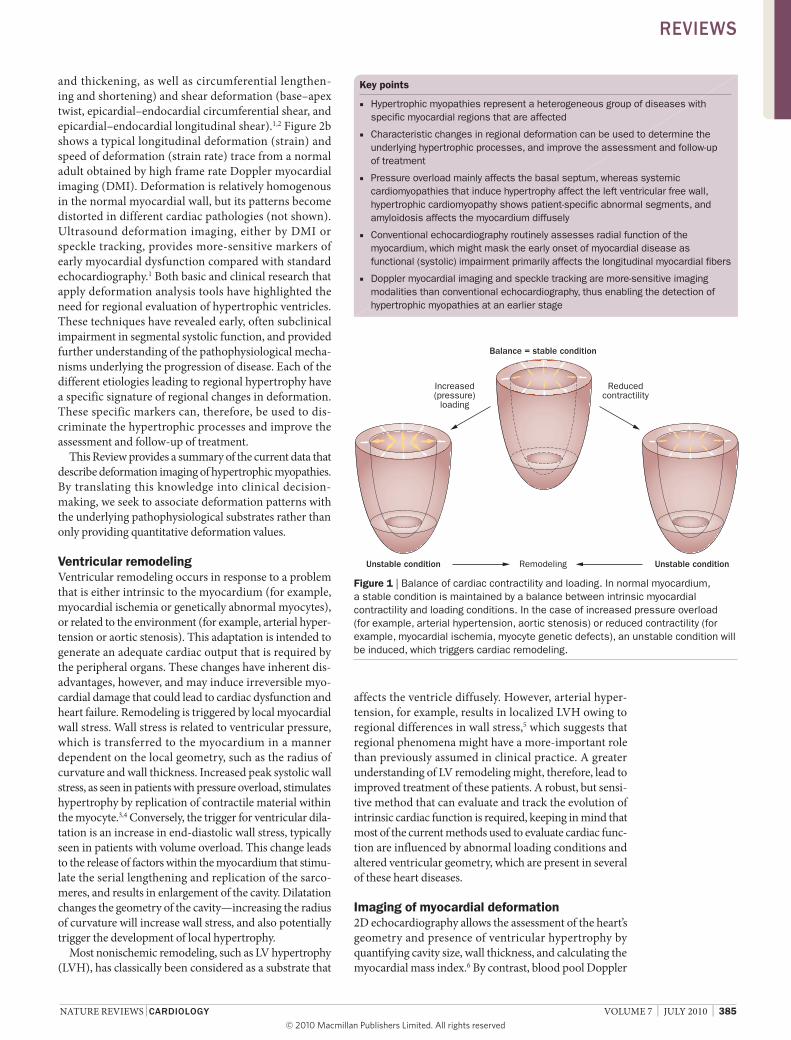
remodeling is sometimes seen in athletes, whereas patho-logical hypertrophy occurs as a result of pressure overload in patients with hypertension or aortic stenosis (Figure 1). This reactive hypertrophy compensates for the increase in afterload, but high values of wall stress eventually cause irreversible damage. Other conditions associated with hypertrophy include hypertrophic cardiomyopathy (HCM), amyloidosis, Fabry disease and Friedreich ataxia. If these conditions are undiagnosed and left untreated, the final stage of heart involvement results in impaired systolic and diastolic function, with low cardiac output leading to congestive heart failure. A greater understanding of the pathways that give rise to the adaptive changes in cardiac function, together with more specific evaluation of all of these conditions, might lead to improved patient manage-ment. In the long-term it would be preferable to prevent the occurrence of myocardial fibrosis and irreversible myocyte degeneration, prevent arrhythmias, and optimize diastolic function. Thus, it is of high clinical importance to detect and treat myocardial dysfunction at an early stage before the onset of irreversible myocyte injury.
Some techniques, such as M-mode or two- dimensional (2D) echocardiography-based global measurements of left ventricular (LV) function, may be inadequate to assess hypertrophic remodeled myocardium. Advances in echocardiography have provided insight into regional myocardial motion and deformation. The defor mation of a myocardial region throughout the cardiac cycle (Figure 2) consists of normal deformation (longi-tudinal lengthening and shortening, radial thinning
Competing interestsThe authors, the Journal Editor B. Mearns and the CME questions author C. P. Vega declare no competing interests.
Continuing Medical Education online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Nature Publishing Group. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this educational activity for a maximum of 1.0 AMA PRA Category 1 CreditsTM. Physicians should only claim credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post‑test and/or complete the evaluation at http://www.medscapecme.com/journal/nrcardio; and (4) view/print certificate.
Learning objectivesUpon completion of this activity, participants should be able to: 1 Describe characteristics that distinguish between hypertrophic
cardiomyopathy and physiologic cardiac hypertrophy.2 Recognize features consistent with different etiologies
of hypertrophic myopathies on the basis of findings from ultrasound deformation imaging.
REVIEWS
nrcardio_56_JUL10.indd 384 10/6/10 12:07:35
© 20 Macmillan Publishers Limited. All rights reserved10
nATure reVIewS | CARdioLoGy VOLuMe 7 | JuLY 2010 | 385
and thickening, as well as circumferential lengthen-ing and shortening) and shear deformation (base–apex twist, epicardial–endocardial circumferential shear, and epicardial– endocardial longitudinal shear).1,2 Figure 2b shows a typical longitudinal deformation (strain) and speed of deformation (strain rate) trace from a normal adult obtained by high frame rate Doppler myocardial imaging (DMI). Deformation is relatively homogenous in the normal myocardial wall, but its patterns become distorted in different cardiac pathologies (not shown). ultrasound deformation imaging, either by DMI or speckle tracking, provides more-sensitive markers of early myocardial dysfunction compared with standard echocardiography.1 Both basic and clinical research that apply deformation analysis tools have highlighted the need for regional evaluation of hypertrophic ventricles. These techniques have revealed early, often subclinical impairment in segmental systolic function, and provided further understan ding of the pathophysiological mecha-nisms underlying the progression of disease. each of the different etio logies leading to regional hypertrophy have a specific signature of regional changes in deformation. These specific markers can, therefore, be used to dis-criminate the hypertrophic processes and improve the assessment and follow-up of treatment.
This review provides a summary of the current data that describe deformation imaging of hypertrophic myo pathies. By translating this knowledge into clinical decision- making, we seek to associate deformation patterns with the underlying pathophysiological substrates rather than only providing quantitative deformation values.
Ventricular remodelingVentricular remodeling occurs in response to a problem that is either intrinsic to the myocardium (for example, myocardial ischemia or genetically abnormal myocytes), or related to the environment (for example, arter ial hyper-tension or aortic stenosis). This adaptation is intended to generate an adequate cardiac output that is required by the peripheral organs. These changes have inherent dis-advantages, however, and may induce ir reversible myo-cardial damage that could lead to cardiac dysfunction and heart failure. remodeling is triggered by local myocardial wall stress. wall stress is related to ventri cular pressure, which is transferred to the myo cardium in a manner dependent on the local geometry, such as the radius of curvature and wall thickness. Increased peak systolic wall stress, as seen in patients with pressure overload, stimulates hypertrophy by replication of contractile material within the myocyte.3,4 Conversely, the trigger for ventricular dila-tation is an increase in end-diastolic wall stress, typically seen in patients with volume overload. This change leads to the release of factors within the myo cardium that stimu-late the serial lengthening and replication of the sarco-meres, and results in enlargement of the cavity. Dilatation changes the geometry of the cavity— increasing the radius of curvature will increase wall stress, and also potentially trigger the development of local hypertrophy.
Most nonischemic remodeling, such as LV hypertrophy (LVH), has classically been considered as a substrate that
Key points
Hypertrophic myopathies represent a heterogeneous group of diseases with ■specific myocardial regions that are affected
Characteristic changes in regional deformation can be used to determine the ■underlying hypertrophic processes, and improve the assessment and follow‑up of treatment
Pressure overload mainly affects the basal septum, whereas systemic ■cardiomyopathies that induce hypertrophy affect the left ventricular free wall, hypertrophic cardiomyopathy shows patient‑specific abnormal segments, and amyloidosis affects the myocardium diffusely
Conventional echocardiography routinely assesses radial function of the ■myocardium, which might mask the early onset of myocardial disease as functional (systolic) impairment primarily affects the longitudinal myocardial fibers
Doppler myocardial imaging and speckle tracking are more‑sensitive imaging ■modalities than conventional echocardiography, thus enabling the detection of hypertrophic myopathies at an earlier stage
Increased(pressure)
loading
Reducedcontractility
Unstable condition Unstable condition
Balance = stable condition
Remodeling
affects the ventricle diffusely. However, arterial hyper-tension, for example, results in localized LVH owing to regional differences in wall stress,5 which suggests that regional phenomena might have a more-important role than previously assumed in clinical practice. A greater understanding of LV remodeling might, therefore, lead to improved treatment of these patients. A robust, but sensi-tive method that can evaluate and track the evolution of intrinsic cardiac function is required, keeping in mind that most of the current methods used to evaluate cardiac func-tion are influenced by abnormal loading conditions and altered ventricular geometry, which are present in several of these heart diseases.
Imaging of myocardial deformation2D echocardiography allows the assessment of the heart’s geometry and presence of ventricular hypertrophy by quantifying cavity size, wall thickness, and calculating the myocardial mass index.6 By contrast, blood pool Doppler
Figure 1 | Balance of cardiac contractility and loading. In normal myocardium, a stable condition is maintained by a balance between intrinsic myocardial contractility and loading conditions. In the case of increased pressure overload (for example, arterial hypertension, aortic stenosis) or reduced contractility (for example, myocardial ischemia, myocyte genetic defects), an unstable condition will be induced, which triggers cardiac remodeling.
ReviewS
nrcardio_56_JUL10.indd 385 10/6/10 12:07:37
© 20 Macmillan Publishers Limited. All rights reserved10

386 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
echocardiography provides direct insight into cardiac hemodynamics by measuring blood velocities through the heart valves, and pressure gradients between the different chambers. Additionally, the intrinsic fiber and myocyte properties are important in the evaluation of sys-tolic myocardial function, since they determine whether a chronic condition has affected the myo cardium and whether irreversible injury has occurred. Only indirect measurements of contractility and pump performance are possible in current clinical practice, which are mainly derived from noninvasive cardiac imaging techniques, such as echocardiography, CT, and cardiac MrI (CMrI), using volume-derived indices, such as ejection fraction or fractional shortening. The evaluation of intrinsic myocardial function based on these indices often relies on geometric assumptions, such as in M-mode and 2D echocardiography. The influence of ventricular shape, wall thickness and cavity size on these indices is not well known. In hypertrophic ventricles, supranormal values of ejection fraction are frequently measured, although whether these values are reflective of true contractility changes is unclear.7 Another limi ta tion of all volume-
derived indices is load dependency. During the pro-gression of disease, alterations in loading conditions or geometry will influence the evaluation of global func-tion. Furthermore, conventional imaging indices assess only global cardiac function, whereas the evaluation of regional cardiac function is relevant in most conditions that affect myocardial contractility. Moreover, some of the methods that evaluate global function focus entirely on radial indices and omit longitudinal function, which is affected prior to the changes in radial function in most cases of cardiac pathology;8 an increase in radial func-tion often compensates for the impairment of global longi tudinal function. Finally, measurements of global function do not consider segment interactions, which may only result in regional wall deformation, and do not contribute to pressure increase or a reduction in overall ventricular volume.9,10
In the context of these limitations, echocardiographic methods that focus on regional ventricular function have been proposed. DMI (also known as myocardial velocity imaging, or tissue Doppler imaging), as well as grayscale 2D speckle tracking, are techniques that allow the quantification of myocardial segmental motion and defor mation.1 Postprocessing of velocity data or image-processing of grayscale data allows the calcula-tion of regional myocardial deformation. Myocardial defor mation can be quantified by strain rate, as well as by strain. when using myocardial velocities, strain rate is calculated as the spatial derivative of local myocardial velocities, while strain is derived as a temporal integral of strain rate. Tracking the motion of the speckle patterns shown in grayscale images provides potentially similar information. unlike a normal base–apex gradient that occurs in myocardial velocities with the highest velo cities at the base of the heart, a homogenous distri bution of peak systolic strain rate values appear within the normal LV walls. Furthermore, the main limitation of velocity data is the influence of myocardial segment inter action and overall heart motion. This limitation has been resolved by deformation imaging, which measures local changes of deformation within a myocardial segment, and should thus better reflect intrinsic contractile function.1
Longitudinal motion and deformation (describing the basal LV displacement towards a stationary apex) can be evaluated from an apical view. From a parasternal (short axis or long axis, or both) view, the inward radial deformation (Doppler-based techniques most suitable) as well as the circumferential shortening (speckle track-ing approaches most suitable) can be measured.9 These normal strain components—radial, longitudinal, and to a lesser extent circumferential—have usually been studied. Quantification of LV rotational mechanics by echo cardiography became possible using 2D speckle tracking. The unique fiber architecture of the left vent-ricle, with epicardial and endocardial layers consisting of longi tudinal fibers, and midmyocardial layers consist-ing of circumferentially oriented fibres,11 results in a torsion of the ventricle during contraction. The angle of the fibers with regard to the LV short axis plane changes from approximately –60° to –80° at the epicardial side,
0
–20
0
–20
Strain rate (1/s)
Apical
Mid
Basal
AVC MVO AVC MVO
Strain (%)
0
–20
0–1
1
–2
2
0–1
1
–2
2
0–1
1
–2
2
Cardiac cycle Cardiac cycle
AVO AVO
rotation
Circumferentialshortening
Radialdeformation
Longitudinaldeformation
(radial)thickening
(long
itudi
nal)
shor
teni
ng
a
b
Figure 2 | Normal myocardial motion and deformation, and typical profiles of strain rate and strain traces.9 a | Normal myocardial motion and deformation and its three major components: longitudinal, radial and circumferential motion and deformation. b | Typical profiles of strain rate and strain traces from a normal adult. Abbreviations: AVC, aortic valve closure; AVO, aortic valve opening; MVO, mitral valve opening. Adapted from Bijnens, B. H. et al. Velocity and deformation imaging for the assessment of myocardial dysfunction. Eur. J. Echocardiogr. 2009, 10(2), 216–226, by permission of Oxford University Press.
ReviewS
nrcardio_56_JUL10.indd 386 10/6/10 12:07:38
© 20 Macmillan Publishers Limited. All rights reserved10

nATure reVIewS | CARdioLoGy VOLuMe 7 | JuLY 2010 | 387
to approximately +60° to +80° at the endo cardial side.11
when the fibers contract, the overall result is a clock-wise rotation seen from the apex of the basal plane, and a counterclockwise rotation of the apical short axis plane. whereas the resulting LV torsion develops evenly during the ejection phase, normal early filling is associated with a rapid untwisting of the left ventricle,12 which contributes to the initial suction phase of filling. The first systems that analyze three-dimensional echo cardiographic images to obtain strain measurements have been introduced.13 These systems might allow a complete description of all components of regional deformation within the same cardiac cycle.
The most important limitation of DMI and defor-mation estimation is the angle dependency. Doppler-based approaches usually measure radial and longitudinal motion and deformation since circumferential motion is difficult to align with the ultrasound beam, which is required by this method. To resolve all mechanical events within the myocardial walls, especially during the iso-volumic periods, high frame rates (>150 Hz) are required. These frame rates are possible to achieve in Doppler-based methods by a combination of using decreased sector angle and less spatial resolution.1 Speckle track-ing approaches that are based on 2D grayscale imaging, currently have a limited temporal resolution of approxi-mately 90 Hz. Speckle tracking-based deformation ana-lysis intrinsically requires little user interaction, whereas it is crucial to perform accurate manual tracking of the tissue for Doppler-based approaches to ensure that the same muscle is analyzed during its motion. A study showed that manual tracking resulted in an interobserver variability of 6.6%, 14.4% and 13.6% for Doppler-based longi tudinal velocity, strain rate, and strain data, respec-tively, and the measured intraobserver variability was 5.3%, 11.8% and 12.9%.14 Another study of interobserver and intra observer variability comparing 2D and velocity- derived longitudinal strain provided values of 7.5% and 7.9% for 2D strain; velocity-derived strain produced an inter observer variability of 13.7% and intraobserver vari-ability of 14.5%.15 Limited information is available for the variability of strain rate in grayscale-based techniques since their inherent limited temporal resolution makes strain rate calculations less accurate. Speckle tracking is, therefore, more reproducible and is less dependent on user expertise, but inherently requires more temporal and spatial averaging of the obtained traces, which results in substantially lower measured values than DMI, and less sensitivity to detect smaller, abnormal myo cardial segments (Table 1).9,16–19
Deformation analysis is inherently load- dependent. Changes in preload and afterload influence the measure-ments, and care has to be taken when interpreting changes in deformation, especially when only analyzing maximal or minimal values instead of the shape of the deformation profile during the cardiac cycle. Deformation imaging can still be used in clinical practice, however, particularly when comparing different regions within the ventricle or for the quantitative longi tudinal follow-up of specific patient groups.1
using DMI and speckle tracking for deformation analy-sis, myocardial dysfunction has been studied in a wide variety of diseases, such as coronary artery disease (includ-ing stress echocardiography),20–23 heart valve disease,24,25 arterial hypertension,5 hyper trophic cardio myopathy,26 heart transplantation,27 cardiac resynchronization therapy,28 amyloidosis,29 and genetic cardiomyopathies.30,31
Echocardiography in hypertrophyPhysiological hypertrophyThe athlete’s heart is a form of physiological hyper-trophic remodeling that may occur as a result of long-term exercise. Magnetic resonance spectroscopy studies have reported that LVH in athletes is associated with a normal cardiac energy metabolism, both at rest and during atropine–dobutamine stress.32,33 However, long-term LV adaptation in high-level endurance athletes may also lead to cavity dilatation.34 Different hyper trophic remodeling patterns are associated with two basic train-ing substrates:35 isotonic exercise, such as swimming or running, leads to an increase in LV mass and mean LV end-diastolic volumes, similar to chronic volume over-load; by contrast, isometric exercise, such as wrestling and shot put, also induces an increase in LV mass, although with normal values of mean LV end-diastolic volumes, mimicking chronic pressure overload.36
exercise-induced remodeling has also been described in animals.37 Physiological LVH leads to an increase in ventricular mass with underlying normal cardiac struc-tural organization and no collagen increase, which is in contrast to pathological LVH characterized by structural changes, collagen accumulation and myocyte hyper-trophy.38–40 An animal study demonstrated that both exercise and aortic banding led to similar and sub stantial LVH.38 nevertheless, systolic and diastolic myocardial velocity gradients (strain rates) were similar in seden-tary and exercising rats, indicating that exercise leads to physiologic hypertrophy, but does not influence myo-cardial function. However, the gradients were signifi-cantly reduced in rats with aortic banding compared with sedentary and exercising rats (P <0.001), which is a model of pathologic hypertrophy occurring as a result of an increase in afterload, and leads to a reduction in systolic function.38
In a comparison of patients with HCM, systemic hypertension and athletes, a decrease in long-axis sys-tolic and early diastolic velocities was seen in patients with pathologic hypertrophy, whereas these parameters were preserved in athletes.41 Athletes with LVH had enhanced global and long-axis diastolic function com-pared with sedentary individuals.41,42 Another study of the regional myocardial function of athletes demon-strated higher systolic and diastolic velocities in several LV regions, whereas deformation parameters (strain and strain rate) showed normal values in athletes compared with the control group.43 Myocardial strain (rate) studied in athletes with LVH demonstrated an overall normal myocardial deforma tion.44 Finally, a supranormal LV velocity pattern, including both systole and diastole as well as supra normal values of systolic strain rate, have
ReviewS
nrcardio_56_JUL10.indd 387 10/6/10 12:07:39
© 20 Macmillan Publishers Limited. All rights reserved10
388 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
been described in athletes with LVH (Table 2).45–47 This observation was supported by 2D strain data demon-strating higher values of transverse and radial strains in athletes than in patients with HCM and normal indivi-duals, whereas in pathologically hypertrophic segments, longitudinal strain was lower in patients with HCM than in athletes.48
Pressure overload hypertrophyHypertensive heart disease and aortic stenosis are charac-terized by pressure overload and increased systolic wall stress, which lead to hypertrophic remodeling. Increased LV mass and wall thickness are associated with reduced global systolic function.49 nevertheless, standard indices of global systolic function, such as ejection fraction and short-axis endocardial shortening, may be supranormal in early stages of the disease owing to increased radial systolic performance.8,50 An increase in circum ferential systolic function and systolic torsion measured by speckle tracking echocardiography were demonstrated in hypertensive patients,51,52 whereas LV radial and circum-ferential systolic impairment was present in patients with heart failure symptoms (nYHA III and IV class).37 Conversely, reduced longitudinal systolic function has been well documented in patients with hypertension at
an early stage, both by measurements of mitral ring dis-placement, velocity and deformation imaging, as well as CMrI tagging.5,41,54
Hypertensive heart diseaseAlthough hypertensive LVH is considered to be a diffuse myocardial disease that results in concentric LVH and overall reduction of deformation parameters, the distri-bution of wall stress on different LV segments is not homogenous, being considerably greater upon the septal wall.55 The basal septal segment is the first region to show changes under the influence of pressure overload as it is under a high level of wall stress owing to an increased local radius of curvature. A reduction in deforma tion parameters, as well as postsystolic deformation and loca lized hypertrophy, occur (Table 2, Figure 3).5,56 The initi ation and localization of functional abnorma lities in the basal septum has also been confirmed by 2D speckle tracking.53
To our knowledge, no prospective study confir ming the expansion of deformation abnormalities from the basal septum across the ventricle currently exists. How-ever, experimental and clinical work on different forms of pressure overload, together with biomechanical know-ledge and insights into the mechanisms of hypertrophy
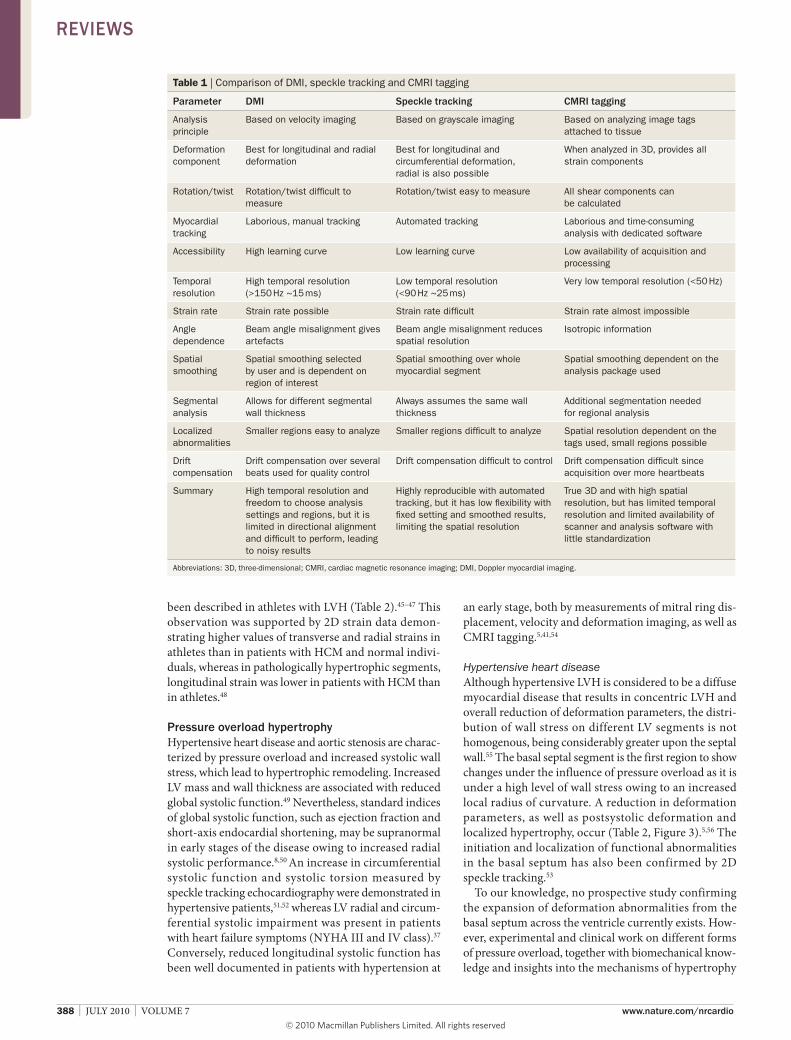
Table 1 | Comparison of DMI, speckle tracking and CMRI tagging
Parameter dMi Speckle tracking CMRi tagging
Analysis principle
Based on velocity imaging Based on grayscale imaging Based on analyzing image tags attached to tissue
Deformation component
Best for longitudinal and radial deformation
Best for longitudinal and circumferential deformation, radial is also possible
When analyzed in 3D, provides all strain components
Rotation/twist Rotation/twist difficult to measure
Rotation/twist easy to measure All shear components can be calculated
Myocardial tracking
Laborious, manual tracking Automated tracking Laborious and time‑consuming analysis with dedicated software
Accessibility High learning curve Low learning curve Low availability of acquisition and processing
Temporal resolution
High temporal resolution (>150 Hz ~15 ms)
Low temporal resolution (<90 Hz ~25 ms)
Very low temporal resolution (<50 Hz)
Strain rate Strain rate possible Strain rate difficult Strain rate almost impossible
Angle dependence
Beam angle misalignment gives artefacts
Beam angle misalignment reduces spatial resolution
Isotropic information
Spatial smoothing
Spatial smoothing selected by user and is dependent on region of interest
Spatial smoothing over whole myocardial segment
Spatial smoothing dependent on the analysis package used
Segmental analysis
Allows for different segmental wall thickness
Always assumes the same wall thickness
Additional segmentation needed for regional analysis
Localized abnormalities
Smaller regions easy to analyze Smaller regions difficult to analyze Spatial resolution dependent on the tags used, small regions possible
Drift compensation
Drift compensation over several beats used for quality control
Drift compensation difficult to control Drift compensation difficult since acquisition over more heartbeats
Summary High temporal resolution and freedom to choose analysis settings and regions, but it is limited in directional alignment and difficult to perform, leading to noisy results
Highly reproducible with automated tracking, but it has low flexibility with fixed setting and smoothed results, limiting the spatial resolution
True 3D and with high spatial resolution, but has limited temporal resolution and limited availability of scanner and analysis software with little standardization
Abbreviations: 3D, three‑dimensional; CMRI, cardiac magnetic resonance imaging; DMI, Doppler myocardial imaging.
ReviewS
nrcardio_56_JUL10.indd 388 10/6/10 12:07:40
© 20 Macmillan Publishers Limited. All rights reserved10

nATure reVIewS | CARdioLoGy VOLuMe 7 | JuLY 2010 | 389
suggest that all other ventricular segments subsequently hypertrophy and show decreased deformation with an increase in pressure overload.
Aortic stenosisPatients with preserved ejection fraction were compared with patients who had the same extent of LVH induced by arterial hypertension or aortic stenosis.57 Generally, the systolic segment of the strain-rate trace was flatter in patients with aortic stenosis. Longitudinal and radial systolic strain rates were reduced in patients with aortic stenosis, compared with patients with arterial hyper-tension and the control group. These reduced rates were attributed to an increase in wall stress secondary to increased LV end-systolic pressure as well as the pres-ence of perimyocytic fibrosis, which had previously been demonstrated in patients with aortic stenosis, but not in patients with hypertension.58 Furthermore, regional differences in deformation parameters were noted in patients with aortic stenosis where longitudinal defor-mation was inhomogeneous between the base and apex, with basal segments having substantially lower strain and strain rate values than apical segments.59
A prospective follow-up study investigated the effect of myocardial fibrosis on myocardial performance in symptomatic severe aortic stenosis.60 results showed that the development of myo cardial replacement fibro-sis was typically located subendo cardially at the basal segments of the left ventricle. This type of fibrosis, demonstrated by both endomyocardial biopsy as well as CMrI late enhancement, had a profound impact on long-term clinical outcome in these patients with aortic stenosis. Measurements of systolic strain and strain rate were markedly reduced in patients with severe fibrosis as determined on biopsy, while mitral ring displace-ment, which was used as a surrogate of overall longitu-dinal septal function, revealed a graded relation with the
degree of myocardial fibrosis, showing the lowest levels in patients with severe fibrosis. nevertheless, such fibro-sis remains undetected by standard echocardio graphy until the terminal disease stages, but its functional con-sequences can be detected by longitudinal mitral ring displacement, which predicts functional improvement after valve replacement.60 remodeling in aortic stenosis may be seen as a continuation of the spectrum of adapta-tion to pressure overload, which governs regional remod-eling in hypertension. Furthermore, a study applying 2D speckle tracking in patients with severe aortic stenosis and preserved ejection fraction demonstrated a pre-operative decrease in longitudinal systolic strain and an increase in radial systolic strain, while normalization of these parameters occurred after aortic valve replace-ment.61 Likewise, an experimental speckle tracking study of aortic banding in pigs showed a decrease in longi-tudinal systolic strain and an increase in radial systolic strain at low increases in LV afterload, whereas a subse-quent increase in LV afterload also led to a considerable decrease in radial systolic strain.62
Pressure overload versus HCMA distinction between hypertensive LVH and non-obstructive HCM has been suggested based on the septum to posterior wall thickness ratio, and average longi tudinal systolic strain for eight myocardial segments.26 A systolic strain cut-off value of –10.6% discrimi nated between HCM and hypertensive LVH with a sensitivity of 85%, a specificity of 100%, and a predictive accuracy of 91.2%, with lower values in the HCM group of patients than in hypertensive patients. Although decreased deformation is present in the basal septum in hypertensive heart disease, it never shows absence of deformation, which is observed in HCM.56 Thus, an average value of systolic strain in several myocardial segments will be lower in HCM. Deformation of the basal septal segment is, therefore,
Table 2 | Biopsy findings and characteristics of hypertrophic remodeling
Parameter Physiological hypertrophy (e.g. in athletes)41–48
Pressure overload5,53,55–61
HCM85,86,91–97 Amyloidosis109–115 Systemic diseases30,31,125–128,134
Biopsy Normal Cellular hypertrophy, replacement fibrosis (AS)
Myocyte disarray Extracellular amyloid deposits
Cellular hypertrophy
Regional or diffuse
Diffuse Regional Regional Diffuse Regional
Affected region
Diffuse Basal septum Predominantly basal/mid septum (patient specific)
Diffuse Basal inferolateral
Ejection fraction
(Supra)normal Normal/reduced (Supra)normal/reduced
Severely reduced Normal/reduced
Diastolic function
Supranormal Impaired Impaired Impaired/restrictive
Impaired
Global deformation
(Supra)normal Reduced + PST Reduced + PST Severely reduced Reduced + PST
Longitudinal function
(Supra)normal Impaired (most in base) Absent in affected regions
Severely impaired Impaired
Radial function
(Supra)normal Maintained/increased Impaired/increased
Mildly impaired Mildly impaired
Abbreviations: AS, aortic stenosis; HCM, hypertrophic cardiomyopathy; PST, postsystolic thickening or shortening.
ReviewS
nrcardio_56_JUL10.indd 389 10/6/10 12:07:41
© 20 Macmillan Publishers Limited. All rights reserved10
390 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
the most sensitive to alterations in pressure overload, which emphasizes the regional nature of initial remodel-ing. Finally, findings suggest that hypertrophy is induced over the entire vent ricle with increasing overload, and this reactive hypertrophy compensates for the elevated afterload until high values of wall stress induce irrevers-ible damage (fibrosis).63
Myocardial torsionrotational mechanics are clearly increased in all pressure overload pathologies.52,64–66 This observation results from the changing interaction between the endocardial and epicardial fibers, which induces LV torsion. endocardial and epicardial fibers are longitudinally oriented, with an oblique angle with regard to the base–apex axis. Contraction of these oblique fibers results, therefore, in rotation of the basal and apical plane in contrary direc-tions. However, endocardial and epicardial fibers have flipped oblique angles and thus induce opposite rotation of the base compared with the apex. In normal LV tissue, epicardial-induced torsion is dominant compared with endocardial-induced torsion. Pressure overload results in proportionally higher loading of the endocardium, together with problems in endocardial perfusion and potential fibrosis. endocardial function is partially lost, therefore, and epicardial torsion becomes even
more dominant, resulting in increased overall torsion.67 However, all processes that influence endocardial func-tion, such as aging68 or Fabry disease,69 induce similar changes. Further development of myo cardial dysfunc-tion, spreading towards the midmyocardial and epicardial layers will consequently reduce torsion again. Currently, no studies have used changes in rotational mechanics to identify specific aspects of cardiac mechanics associated with pressure overload.
Hypertrophic cardiomyopathyHCM is a disease with autosomal dominant transmission that occurs in 1 in 500 individuals of the general popula-tion.70–73 Mutations in the genes that encode cardiac sarcomere proteins, such as myosin-binding protein C, β-myosin heavy chain, and troponin T and I, lead to a disorder of force generation within the myocardium.70 Molecular genetics and clinical research have, however, demonstrated that a mutation in one of these genes is not always associated with increased LV wall thickness.73–75 The combination of these findings, together with age-related penetrance and delayed appearance of LVH on echocardiography in adulthood,73,74 make it no longer possible to exclude the diagnosis of HCM on the basis of a normal echocardiogram in family members of an affected individual.
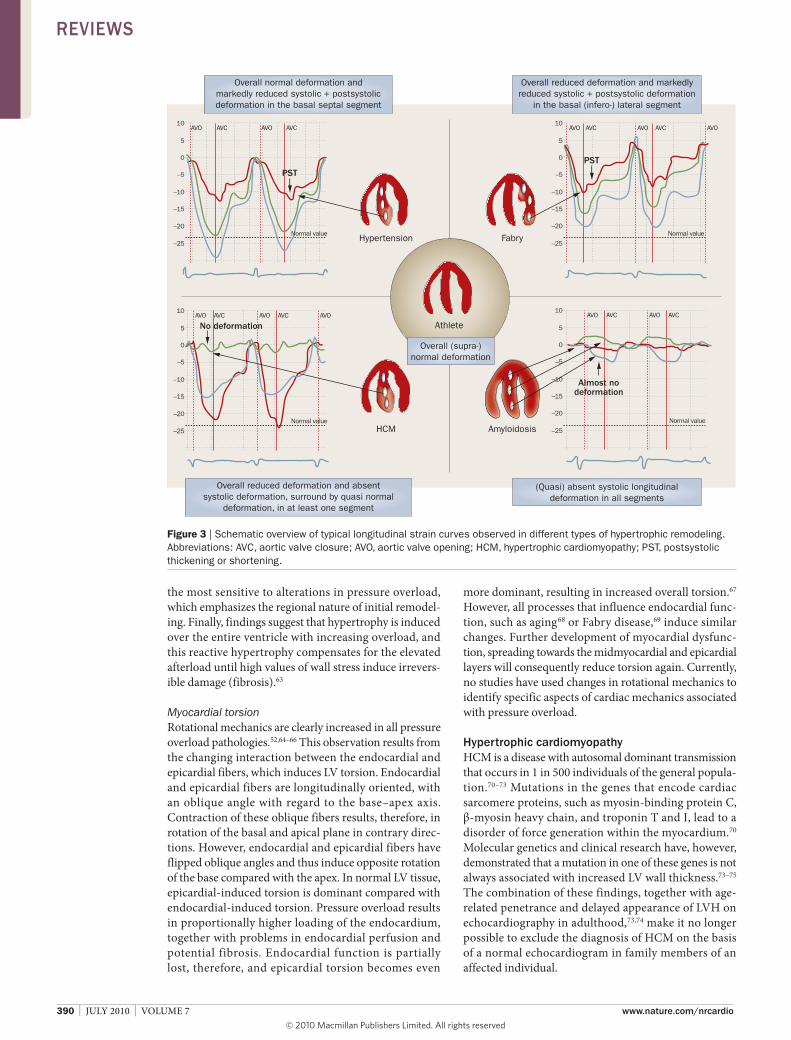
Overall normal deformation andmarkedly reduced systolic + postsystolicdeformation in the basal septal segment
Overall reduced deformation and markedlyreduced systolic + postsystolic deformation
in the basal (infero-) lateral segment
Overall reduced deformation and absentsystolic deformation, surround by quasi normal
deformation, in at least one segment
(Quasi) absent systolic longitudinaldeformation in all segments
Overall (supra-)normal deformation
10
Athlete
Hypertension
PSTPST
Almost nodeformation
No deformation
Fabry
HCM Amyloidosis
AVO AVC AVO AVC
5
0
–5
–10
–15
–25
–20
10AVO AVC AVO AVC AVO
5
0
–5
–10
–15
–20Normal value
–25
10AVO AVC AVO AVC
5
0
–5
–10
–15
–20Normal value
–25
10AVO AVC AVO AVC AVO
5
0
–5
–10
–15
–20Normal value
–25
Normal value
Figure 3 | Schematic overview of typical longitudinal strain curves observed in different types of hypertrophic remodeling. Abbreviations: AVC, aortic valve closure; AVO, aortic valve opening; HCM, hypertrophic cardiomyopathy; PST, postsystolic thickening or shortening.
ReviewS
nrcardio_56_JUL10.indd 390 10/6/10 12:07:43
© 20 Macmillan Publishers Limited. All rights reserved10

nATure reVIewS | CARdioLoGy VOLuMe 7 | JuLY 2010 | 391
Echocardiographic findings in HCMThe clinical diagnosis of HCM is usually established with echocardiography, which traditionally demon-strated nondilated LVH in the absence of hemodynamic stresses (for example, arterial hypertension or aortic stenosis) or systemic disease (for example, amyloidosis or storage diseases), regardless of the presence of LV outflow tract obstruction.71,72,76 However, a substantial overlap is present between echocardiographic findings in patients with HCM and those with hypertensive LVH.77–79 Furthermore, HCM is thought to predominantly affect the heart’s diastolic function, whereas the systolic pro-perties are thought to remain intact, at least in the initial disease period.80–82 Volume-based parameters, such as ejection fraction and fractional shortening often yield supranormal values in hypertrophic ventricles; systolic function was, therefore, assumed preserved until a more advanced stage of the disease.8,9,54,83,84 Moreover, these indices only assess global cardiac function and concen-trate exclusively on radial function, omitting longitu dinal function, which is affected prior to changes in radial indices in most cardiac pathologies.8
Characteristics of HCMHCM is characterized by regions of local fiber disarray. The areas of fiber disarray can vary in size and locali-zation within the hypertrophic areas.85,86 In a mouse model of familial HCM, impaired myocyte defor mation preceded histopathological changes.87 A transgenic mouse model of HCM had decreased sarcomere length, systolic shortening and shear strain in segments with more pronounced hypertrophy.88 Myofiber disarray was associated with reduced septal torsion and reduced surface shortening. Similarly, overall rotational mecha-nics are reduced in patients with HCM and this reduction is dependent on the segmental distribution of hyper-trophic segments.89,90 regional deformation analysis can easily detect hypertrophic, histologically abnormal areas of cardiac muscle that do not demonstrate any systolic deformation, surrounded by hypertrophic regions that still deform (although this deformation is substantially impaired compared with normal regions).15,48,91–93 The absence of deformation usually occurs in the thickest segments of myocardial tissue. A study of children with HCM showed that despite normal echo cardiographic parameters of global systolic function, impaired radial and longitudinal deformation occurred in localized pockets of myocardial tissue that related to the regional hypertrophic pattern. Furthermore, increased post-systolic shortening or lengthening often found in isch-emic myocardium, as well as a delay in mechanical activation and a decrease in peak systolic deformation, were present in the hypertrophic segments, emphasiz-ing the regional nature of myocardial involvement.10,94 A similar pattern of regional deformation was found in a study that described the double peak sign (the second strain-rate peak resulting from post systolic deformation) as a typical deformation pattern seen in hypertrophic segments with fibrosis, which was confirmed by CMrI late enhancement.95
The most typical patterns in HCM are thus the regions where no myocardial deformation is present, sur-rounded by regions of only slightly reduced deforma-tion compared with the same regions in normal hearts. Depending on the individual patient, these regions can be located anywhere within the ventricles, but are usually localized in the interventricular septum, where the basal-mid segment reveals total absence of longi tudinal defor-mation, but radial function is still preserved (Table 2, Figure 3). The detection of non deforming regions using ultrasonic strain rate imaging allows easy and accurate discrimination between patients with HCM, where the nondeforming regions are most often found in the anterior septum and anterior wall, and between patients with HCM and those with other forms of hypertrophy (Figure 3).56 Similar segmental abnormalities were also demonstrated by circumfe rential, radial and longi tudinal 2D strain in the septal, an terior septal and anterior walls.96 regional impairment of systolic deformation indices was also demonstrated in a DMI study employ-ing strain rate imaging. This study showed a correla-tion between regional systolic strain and strain rate and LV wall thickness in patients with HCM in contrast to patients with hypertensive LVH. The result demon-strated that hetero geneity of regional LV systolic function detected by deformation imaging is partly attributable to hetero geneity of LVH, suggesting the link to impaired global LV relaxation in HCM.97
CMRI studies in HCMCMrI studies have confirmed the regional pattern of myocardial involvement in HCM. CMrI tagging data suggest a heterogeneous reduction in shortening and thickening of the myocardium, which is inversely corre-lated with end-diastolic wall thickness. regions of delayed enhancement that correspond to tissue with reduced circum ferential deformation can be found, such that focal nodular enhancement is particularly related to regional dysfunction in patients with HCM.98–100 However, a reduction in strain and strain rate can be detected before the occurrence of apparent LVH or electro cardiography abnormalities and before focal fibrosis can be detected by late gadolinium enhancement CMrI.101
AmyloidosisAmyloid cardiomyopathy can occur in all forms of sys-temic amyloidosis.102 Primary amyloidosis is associated with plasma-cell dyscrasia and is the most common form of amyloidosis. The heart is involved in approximately 50% of primary amyloidosis cases, with rapidly progres-sive signs and symptoms of congestive heart failure, occurrence of which is the worst prognostic factor in this group of patients.103,104 Secondary amyloidosis is associ ated with infection or inflammatory disease, and is becoming increasingly uncommon.102 Hereditary (fami-lial) amyloidosis involves the myocardium, but occurs less frequently than primary amyloidosis. Hereditary amyloidosis is transmitted as an autosomal-dominant disease with onset predominantly after the age of 40, and is usually less aggressive than primary amyloi dosis.102
ReviewS
nrcardio_56_JUL10.indd 391 10/6/10 12:07:46
© 20 Macmillan Publishers Limited. All rights reserved10

392 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
This condition results from a transthyretin protein muta-tion that leads to the production of amyloid;105 the pattern of cardiac involvement varies according to the mutation. Senile systemic amyloidosis results from the deposition of amyloid derived from wild-type trans thyretin, and invariably presents as congestive heart failure with a longer median survival than primary amyloidosis.102,106,107 Isolated atrial amyloidosis is a common finding at autopsy and is the only amyloidosis associated with nonsystemic depositions.102,108,109
Owing to widespread amyloid deposits throughout the heart, endomyocardial biopsy is almost 100% sensi-tive in detecting amyloid cardiomyopathy.109 regardless of the type of amyloidosis, extracellular deposition of amyloid throughout the heart results in biventri-cular wall thicken ing (rather than LVH) associated with a restrictive filling pattern detected by Doppler echocardio graphy.109 Although these findings are typical of end-stage disease, diastolic dysfunction can be mildly impaired in the earlier stages and suggests progressive myocardial infiltration.110
Amyloid deposits induce oxidant stress that depresses myocyte contractile function.111,112 Furthermore, amyloid infiltration of the myocardium disrupts contractile func-tion, which can lead to myocyte necrosis and interstitial fibrosis, resulting in systolic dysfunction. Conversely, LV ejection fraction assessed by conventional echo-cardiography is considered to remain normal until the late stages of the disease. Initial DMI studies were based on pulsed DMI and have demonstrated accuracy in detec ting the presence of diastolic dysfunction as well as the ability to detect impairment in longitudinal systolic function, which occurs prior to abnormal LV ejection fraction.113,114 Studies implementing strain and strain-rate imaging have confirmed the diffuse pattern of the disease primarily affecting longitudinal function, as well as showing superiority of the technique in early detection of impaired LV systolic function (Table 2).29,115 A reduc-tion of longitudinal systolic strain in all 16 myocardial segments was shown in patients with systemic primary amyloidosis without echocardiographic or Doppler evidence of cardiac involvement.29
In line with pathological findings and DMI studies that demonstrate diffuse myocardial involvement in amyloid cardiomyopathy, CMrI studies have shown global subendo cardial late gadolinium enhancement as well as abnormal myocardial and blood pool gado-linium kin etics.116 The subendocardial or subepicardial involvement leads to a severe reduction of the contracti-lity of the longitudinally oriented fibers and results in the virtual absence of longitudinal deformation in amyloid cardiomyopathy (Figure 3), especially in the basal seg-ments. This absence of longitudinal deformation is compensated by radial thickening and circumferential shortening, which is the only deformation generating the cardiac output.
Systemic diseaseAlthough myocardial involvement in systemic diseases is variable, the evaluation of myocardial involvement is
important in the initial diagnosis of the disease as well as for monitoring disease progression. where a specific therapy is available, follow-up data on the impact of treat-ment is of high importance.117–119 However, in sub clinical disease stages, commonly applied echo cardiographic parameters, such as ejection fraction calculations, are often insensitive to subtle functional impairment.30,120,121 Moreover, late onset of diffuse changes detectable by routine echocardiography can be anticipated by detect-ing preceding regional changes. Traditionally, metabolic disorders have been most often linked with concentric hypertrophy.70 research of systemic diseases provides evidence of regional LV involvement, detectable by deformation imaging. even in early stages of disease, signs of remodeling are detectable by reduced systolic deformation in the LV free wall, which may be associated with postsystolic deformation (Table 2, Figure 3).
Fabry diseaseFabry disease is an X-linked recessive lysosomal storage disorder that leads to deficiency of the enzyme α–galactosidase A and an accumulation of the glyco-sphingolipid globotriaosylceramide in various tissues.122 Despite the severity of this disease, its rare occurrence (1 in 40,000–117,000 newborn males) and various manifesta tions often lead to misdiagnosis and inadequate treatment strategies.123 Cardiac symptoms account for 50–60% of the presenting symptoms in these patients, and heart failure is among the leading cause of death at a younger age.124 Myocytes are affected, which leads to LVH (concentric hypertrophy in 50% of the patients, and concentric remodeling in 37% of all patients, mostly in younger patients) with subsequent systolic and dia-stolic dysfunction.125,126 Deformation imaging data have shown a correlation between myocardial wall thickness and radial strain rate, where lower values of strain rate were measured in thick walls.30 Furthermore, functional abnormalities occur prior to morphologic changes, which initially involve the lateral LV wall, with an impairment of longitudinal systolic function preceding radial dys-function. These changes demonstrate a regional rather than a diffuse nature of myocardial involvement.30 CMrI data have demonstrated that fibrosis is initiated in the middle layers of the myocardium of the basal infero-lateral wall, combined with reduced strain and strain rate values in the involved regions, in which the double-peak sign has been described as a marker of postsystolic thickening.95,127,128 In the end stage of heart involvement, Fabry disease is characterized by LVH, myocardial fibro-sis (as seen on myocardial biopsy), and severely reduced regional LV function.30,126
The availability of enzyme-replacement therapy has focused myocardial imaging studies on the follow-up of patients after treatment. Patients have demonstrated a regression of LVH and higher values of strain rate 1 year after therapy was initiated.119,129 nevertheless, myo cardial segments demonstrating late enhancement, as seen by CMrI, showed no functional improvement during enzyme-replacement therapy, which suggests that early disease detection and initiation of treatment is
ReviewS
nrcardio_56_JUL10.indd 392 10/6/10 12:07:48
© 20 Macmillan Publishers Limited. All rights reserved10

nATure reVIewS | CARdioLoGy VOLuMe 7 | JuLY 2010 | 393
crucial within this patient population.130 A 3-year follow-up study of 32 patients receiving enzyme-replacement therapy confirmed these findings; patients with mild or severe myocardial fibrosis, as seen on late enhancement CMrI imaging, showed no improvement in myocardial function quantified by strain-rate imaging, but in patients without fibrosis at baseline, enzyme-replacement therapy resulted in increased systolic strain rate.118
Friedreich ataxiaFriedreich ataxia is a neurodegenerative disease with an autosomal-recessive inheritance. The condition is caused by a GAA triplet repeat expansion in the first intron of FXN—a gene that encodes frataxin—which results in mitochondrial dysfunction.131 Cellular hyper-trophy, focal myocardial necrosis, and diffuse fibrosis all occur as a result of this expansion.132 Myocardial involvement usually includes concentric or asymmetri-cal LVH and does not affect the right ventricle.120,133,134 A DMI study demonstrated reduced systolic and dia-stolic myo cardial velocity gradients in patients with Friedreich ataxia who were free of cardiac symptoms compared with controls.120 An inverse relation between the age-corrected myo cardial velocity gradients and the size of the GAA triple repeat expansion was also seen, suggesting that abnormal myocardial velocity gradients might reflect myocardial involvement as a consequence of the specific genetic defect. These findings were fol-lowed by a study that demon strated marked reduction of myo cardial deformation parameters in patients with Friedreich ataxia.134 Moreover, an impairment of systolic and diastolic deformation parameters was detected in patients with Friedreich ataxia who were free of signs of LVH, as well as in the nonhypertrophied segments of patients with regional LVH, suggesting that regional myo cardial dysfunction precedes changes in LV geo-metry.126,134 Interestingly, the lowest values of systolic deformation properties were noted in the basal ante-rior and lateral LV walls, suggesting a similar pattern of regional abnormalities as seen in other systemic diseases as well.134
The antioxidant drug idebenone protects mito-chondrial respiratory dysfunction; in a study of eight patients undergoing treatment over 1 year, a consider-able reduction in cardiac hypertrophy was seen in six of the eight patients.118 Cardiac strain and strain-rate imaging showed that an improvement in cardiac function preceded the reduction of LVH.
Duchenne muscular dystrophyAnother disorder that is associated with hypertrophy is Duchenne muscular dystrophy. This X-linked, recessive disease is caused by a mutation in the dystrophin gene on chromosome Xp21 that results in a deficiency of the sub-sarcolemmal protein dystrophin, a protein that is critical for muscle membrane stability.136,137 Duchenne muscular dystrophy is clinically associated with skeletal myopathy and dilated cardiomyopathy, leading to congestive heart failure and causing death in 30% of patients.31 One study performed velocity and deformation analysis in young
patients with Duchenne muscular dystrophy who had normal global systolic function.31 This study demon-strated reductions in systolic deformation parameters in the anterolateral and inferolateral LV walls, thus confirm-ing that there is a similar regional distri bution of affected regions in different systemic diseases (Figure 3).31
ConclusionsAlthough all hypertrophic myopathies show thicken-ing of the myocardial walls, they clearly represent a hetero geneous group of diseases with a wide spectrum of myocardial involvement. This heterogeneity can be appreciated at the microscopic level, to specific myo-cardial regions most often affected by the underlying disease. The introduction of deformation imaging in clinical practice has provided insight into regional myo-cardial function. Multiple studies support the regional nature of these myopathies, frequently emphasizing the importance of induced abnormal segmental systolic func-tion. The assessment of longitudinal myocardial function has proved to be of high importance; the assessment of radial function, which is routinely performed, might mask the early onset of functional impairment, which primarily affects the longitudinal myocardial fibers. Moreover, regional phenomena, such as postsystolic thickening and shortening, may occur in several myo-pathies, where the localization of the affected segment might point to the underlying substrate. Assessment of systolic function in hyper trophic myopathies must not be considered secondary to the assessment of diastolic func-tion; rather, these data should be integrated in a compre-hensive approach to hypertrophic remodeling and the early detection of myocardial impairment.
Studies have been carried out to investigate the under-lying pathophysiological substrates in hypertrophic hearts. However, clinical outcome studies and studies on the accuracy and reliability of the methods described in this review have yet to be performed. we have tried to emphasize that it is not the value of the strain in a speci-fic segment, or whether this deviates from the normal range, but rather the pattern and the specific localiza-tion of abnormalities that provides clinical insight in the disease substrate.
Review criteria
Articles were selected from a PubMed search of English language full‑text papers published between 1966 and 2009. The following keywords and their combinations were used: “ventricular hypertrophy”, “hypertrophic myocardium”, “hypertrophic cardiomyopathy”, “hypertensive heart disease”, “aortic stenosis”, “pressure overload”, “amyloid”, “Fabry disease”, “Friedreich ataxia”, and “athlete’s heart”, as well as their combinations with “myocardium”, “hypertrophy”, and “cardiomyopathy”. From the obtained search results, papers that used DMI, speckle tracking or CMRI were further reviewed. In addition, the reference lists of identified papers were searched for further leads. Search words also included the names of known authors in this field.
ReviewS
nrcardio_56_JUL10.indd 393 10/6/10 12:07:49
© 20 Macmillan Publishers Limited. All rights reserved10
394 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
1. Sutherland, G. R., Hatle, L., Claus, P., D’hooge, J. & Bijnens, B. (Eds) Doppler Myocardial Imaging, A Textbook (BSWK bvba, Hasselt, Belgium, 2006).
2. Sengupta, P. P. et al. Left ventricular form and function revisited: applied translational science to cardiovascular ultrasound imaging. J. Am. Soc. Echocardiogr. 20, 539–551 (2007).
3. Grossman, W., Jones, D. & McLaurin, L. P. Wall stress and patterns of hypertrophy in the human left ventricle. J. Clin. Invest. 56, 56–64 (1975).
4. Opie, L. H., Commerford, P. J., Gersh, B. J. & Pfeffer, M. A. Controversies in ventricular remodelling. Lancet 367, 356–367 (2006).
5. Baltabaeva, A. et al. Regional left ventricular deformation and geometry analysis provides insights in myocardial remodelling in mild to moderate hypertension. Eur. J. Echocardiogr. 9, 501–508 (2008).
6. Lang, R. M. et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 7, 79–108 (2006).
7. Bijnens, B., Claus, P., Weidemann, F., Strotmann, J. & Sutherland, G. R. Investigating cardiac function using motion and deformation analysis in the setting of coronary artery disease. Circulation 116, 2453–2464 (2007).
8. Aurigemma, G. P., Silver, K. H., Priest, M. A. & Gaasch, W. H. Geometric changes allow normal ejection fraction despite depressed myocardial shortening in hypertensive left ventricular hypertrophy. J. Am. Coll. Cardiol. 26, 195–202 (1995).
9. Bijnens, B. H., Cikes, M., Claus, P. & Sutherland, G. R. Velocity and deformation imaging for the assessment of myocardial dysfunction. Eur. J. Echocardiogr. 10, 216–226 (2009).
10. Claus, P. et al. Mechanisms of postsystolic thickening in ischemic myocardium: mathematical modelling and comparison with experimental ischemic substrates. Ultrasound Med. Biol. 33, 1963–1970 (2007).
11. Greenbaum, R. A., Ho, S. Y., Gibson, D. G., Becker, A. E. & Anderson, R. H. Left ventricular fibre architecture in man. Br. Heart J. 45, 248–263 (1981).
12. Beyar, R., Yin, F. C., Hausknecht, M., Weisfeldt, M. L. & Kass, D. A. Dependence of left ventricular twist‑radial shortening relations on cardiac cycle phase. Am. J. Physiol. 257, H1119–H1126 (1989).
13. Saito, K. et al. Comprehensive evaluation of left ventricular strain using speckle tracking echocardiography in normal adults: comparison of three‑dimensional and two‑dimensional approaches. J. Am. Soc. Echocardiogr. 22, 1025–1030 (2009).
14. Kowalski, M. et al. Can natural strain and strain rate quantify regional myocardial deformation? A study in healthy subjects. Ultrasound Med. Biol. 27, 1087–1097 (2001).
15. Serri, K. et al. Global and regional myocardial function quantification by two‑dimensional strain: application in hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 47, 1175–1181 (2006).
16. Langeland, S. et al. Experimental assessment of a new research tool for the estimation of two‑dimensional myocardial strain. Ultrasound Med. Biol. 32, 1509–1513 (2006).
17. Korinek, J. et al. Two‑dimensional strain—a Doppler‑independent ultrasound method for quantitation of regional deformation: validation in vitro and in vivo. J. Am. Soc. Echocardiogr. 18, 1247–1253 (2005).
18. Ng, A. C. et al. Comparison of myocardial tissue velocities measured by two‑dimensional speckle
tracking and tissue Doppler imaging. Am. J. Cardiol. 102, 784–789 (2008).
19. Chan, J. et al. Differentiation of subendocardial and transmural infarction using two‑dimensional strain rate imaging to assess short‑axis and long‑axis myocardial function. J. Am. Coll. Cardiol. 48, 2026–2033 (2006).
20. Jamal, F. et al. Noninvasive quantification of the contractile reserve of stunned myocardium by ultrasonic strain rate and strain. Circulation 104, 1059–1065 (2001).
21. Weidemann, F. et al. Myocardial function defined by strain rate and strain during alterations in inotropic states and heart rate. Am. J. Physiol. Heart Circ. Physiol. 283, H792–H799 (2002).
22. Thibault, H. & Derumeaux, G. Assessment of myocardial ischemia and viability using tissue Doppler and deformation imaging: the lessons from the experimental studies. Arch. Cardiovasc. Dis. 101, 61–68 (2008).
23. Voigt, J. U. et al. Comparison of deformation imaging and velocity imaging for detecting regional inducible ischaemia during dobutamine stress echocardiography. Eur. Heart J. 25, 1517–1525 (2004).
24. Marciniak, A. et al. Changes in systolic left ventricular function in isolated mitral regurgitation. A strain rate imaging study. Eur. Heart J. 28, 2627–2636 (2007).
25. Marciniak, A. et al. Myocardial deformation abnormalities in patients with aortic regurgitation: a strain rate imaging study. Eur. J. Echocardiogr. 10, 112–119 (2009).
26. Kato, T. S. et al. Discrimination of nonobstructive hypertrophic cardiomyopathy from hypertensive left ventricular hypertrophy on the basis of strain rate imaging by tissue doppler ultrasonography. Circulation 110, 3808–3814 (2004).
27. Eroglu, E. et al. Quantitative dobutamine stress echocardiography for the early detection of cardiac allograft vasculopathy in heart transplant recipients. Heart 94, e3 (2008).
28. Breithardt, O. A. et al. Cardiac resynchronization therapy can reverse abnormal myocardial strain distribution in patients with heart failure and left bundle branch block. J. Am. Coll. Cardiol. 42, 486–494 (2003).
29. Bellavia, D. et al. Evidence of impaired left ventricular systolic function by Doppler myocardial imaging in patients with systemic amyloidosis and no evidence of cardiac involvement by standard two‑dimensional and Doppler echocardiography. Am. J. Cardiol. 101, 1039–1045 (2008).
30. Weidemann, F. et al. The variation of morphological and functional cardiac manifestation in Fabry disease: potential implications for the time course of the disease. Eur. Heart J. 26, 1221–1227 (2005).
31. Mertens, L. et al. Early regional myocardial dysfunction in young patients with Duchenne muscular dystrophy. J. Am. Soc. Echocardiogr. 21, 1049–1054 (2008).
32. Perseghin, G. et al. Effect of the sporting discipline on the right and left ventricular morphology and function of elite male track runners: a magnetic resonance imaging and phosphorus 31 spectroscopy study. Am. Heart J. 154, 937–942 (2007).
33. Pluim, B. M. et al. Functional and metabolic evaluation of the athlete’s heart by magnetic resonance imaging and dobutamine stress magnetic resonance spectroscopy. Circulation 97, 666–672 (1998).
34. Abergel, E. et al. Serial left ventricular adaptations in world‑class professional cyclists: implications for disease screening and follow‑up. J. Am. Coll. Cardiol. 44, 144–149 (2004).
35. Morganroth, J., Maron, B. J., Henry, W. L. & Epstein, S. E. Comparative left ventricular dimensions in trained athletes. Ann. Intern. Med. 82, 521–524 (1975).
36. D’Andrea, A. et al. Association between left ventricular structure and cardiac performance during effort in two morphological forms of athlete’s heart. Int. J. Cardiol. 86, 177–184 (2002).
37. Blomqvist, C. G. & Saltin, B. Cardiovascular adaptations to physical training. Annu. Rev. Physiol. 45, 169–189 (1983).
38. Derumeaux, G. et al. Tissue Doppler imaging differentiates physiological from pathological pressure‑overload left ventricular hypertrophy in rats. Circulation 105, 1602–1608 (2002).
39. Medugorac, I. Myocardial collagen in different forms of heart hypertrophy in the rat. Res. Exp. Med. 177, 201–211 (1980).
40. Moore, R. L. & Korzick, D. H. Cellular adaptations of the myocardium to chronic exercise. Prog. Cardiovasc. Dis. 37, 371–396 (1995).
41. Vinereanu, D. et al. Differentiation between pathologic and physiologic left ventricular hypertrophy by tissue Doppler assessment of long‑axis function in patients with hypertrophic cardiomyopathy or systemic hypertension and in athletes. Am. J. Cardiol. 88, 53–58 (2001).
42. Caso, P. et al. Pulsed Doppler tissue imaging in endurance athletes: relation between left ventricular preload and myocardial regional diastolic function. Am. J. Cardiol. 85, 1131–1136 (2000).
43. Herbots, L. Assessment of contractile function in endurance trained athletes using strain rate and strain. Thesis, University Hospital Gasthuisberg, Leuven, Belgium (2006).
44. Teske, A. J. et al. Echocardiographic deformation imaging reveals preserved regional systolic function in endurance athletes with left ventricular hypertrophy. Br. J. Sports Med. doi:10.1136/bjsm.2008.054346.
45. Palka, P., Lange, A. & Nihoyannopoulos, P. The effect of long‑term training on age‑related left ventricular changes by Doppler myocardial velocity gradient. Am. J. Cardiol. 84, 1061–1067 (1999).
46. D’Andrea, A. et al. The usefulness of Doppler myocardial imaging in the study of the athlete’s heart and in the differential diagnosis between physiological and pathological ventricular hypertrophy. Echocardiography 23, 149–157 (2006).
47. Poulsen, S. H. et al. Strain rate and tissue tracking imaging in quantitation of left ventricular systolic function in endurance and strength athletes. Scand. J. Med. Sci. Sports 17, 148–155 (2007).
48. Richand, V. et al. An ultrasound speckle tracking (two‑dimensional strain) analysis of myocardial deformation in professional soccer players compared with healthy subjects and hypertrophic cardiomyopathy. Am. J. Cardiol. 100, 128–132 (2007).
49. Ganau, A. et al. Patterns of left ventricular hypertrophy and geometrical remodeling in essential hypertension. J. Am. Coll. Cardiol. 19, 1550–1558 (1992).
50. Hatford, M., Wikstrand, J. C., Wallentin, I., Ljungman, S. M. & Berglund, G. L. Left ventricular wall stress and systolic function in untreated primary hypertension. Hypertension 7, 97–104 (1985).
51. Przewlocka‑Kosmala, M., Kosmala, W. & Mazurek, W. Left ventricular circumferential function in patients with essential hypertension. J. Hum. Hypertens. 20, 666–671 (2006).
ReviewS
nrcardio_56_JUL10.indd 394 10/6/10 12:07:50
© 20 Macmillan Publishers Limited. All rights reserved10
nATure reVIewS | CARdioLoGy VOLuMe 7 | JuLY 2010 | 395
52. Park, S. J. et al. Left ventricular torsion by two‑dimensional speckle tracking echocardiography in patients with diastolic dysfunction and normal ejection fraction. J. Am. Soc. Echocardiogr. 21, 1129–1137 (2008).
53. Kosmala, W. et al. Progression of left ventricular functional abnormalities in hypertensive patients with heart failure: an ultrasonic two‑dimensional speckle tracking study. J. Am. Soc. Echocardiogr. 21, 1309–1317 (2008).
54. Palmon, L. C. et al. Intramural myocardial shortening in hypertensive left ventricular hypertrophy with normal pump function. Circulation 89, 122–131 (1994).
55. Heng, M. K., Janz, R. F. & Jobin, J. Estimation of regional stress in the left ventricular septum and free wall: an echocardiographic study suggesting a mechanism for asymmetric septal hypertrophy. Am. Heart J. 110, 84–90 (1985).
56. Orlando, S. et al. Hypertrophic cardiomyopathy can be effectively discriminated from other forms of hypertrophy by the presence of localised non‑deforming segments—a deformation imaging study [abstract]. Eur. Heart J. 28 (Suppl. 1), 2190 (2007).
57. Strotmann, J. M. et al. Functional differences of left ventricular hypertrophy induced by either arterial hypertension or aortic valve stenosis. Am. J. Cardiol. 101, 1493–1497 (2008).
58. Schwartzkopff, B. et al. Morphometric investigation of human myocardium in arterial hypertension and valvular aortic stenosis. Eur. Heart J. 13 (Suppl. D), 17–23 (1992).
59. Kowalski, M. et al. One‑dimensional ultrasonic strain and strain rate imaging: a new approach to the quantitation of regional myocardial function in patients with aortic stenosis. Ultrasound Med. Biol. 29, 1085–1092 (2003).
60. Weidemann, F. et al. Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 120, 577–584 (2009).
61. Carasso, S. et al. Differential effects of afterload on left ventricular long‑ and short‑axis function: insights from a clinical model of patients with aortic valve stenosis undergoing aortic valve replacement. Am. Heart J. 158, 540–545 (2009).
62. Donal, E. et al. Influence of afterload on left ventricular radial and longitudinal systolic functions: a two‑dimensional strain imaging study. Eur. J. Echocardiogr. 10, 914–921 (2009).
63. Hein, S. et al. Progression from compensated hypertrophy to failure in the pressure‑overloaded human heart: structural deterioration and compensatory mechanisms. Circulation 107, 984–991 (2003).
64. Cappelli, F. et al. Adaptative or maladaptative hypertrophy, different spatial distribution of myocardial contraction. Clin. Physiol. Funct. Imaging 30, 6–12 (2010).
65. Stuber, M. et al. Alterations in the local myocardial motion pattern in patients suffering from pressure overload due to aortic stenosis. Circulation 100, 361–368 (1999).
66. Sandstede, J. J. et al. Cardiac systolic rotation and contraction before and after valve replacement for aortic stenosis: a myocardial tagging study using MR imaging. AJR Am. J. Roentgenol. 178, 953–958 (2002).
67. Van Der Toorn, A. et al. Transmural gradients of cardiac myofiber shortening in aortic valve stenosis patients using MRI tagging. Am. J. Physiol. Heart Circ. Physiol. 283, H1609–H1615 (2002).
68. Lumens, J., Delhaas, T., Arts, T., Cowan, B. R. & Young, A. A. Impaired subendocardial contractile myofiber function in asymptomatic
aged humans, as detected using MRI. Am. J. Physiol. Heart Circ. Physiol. 291, H1573–H1579 (2006).
69. Rutz, A. K. et al. Altered myocardial motion pattern in Fabry patients assessed with CMR‑tagging. J. Cardiovasc. Magn. Reson. 9, 891–898 (2007).
70. Elliott, P. et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 29, 270–276 (2008).
71. Maron, B. J. et al. American College of Cardiology/European Society of Cardiology Clinical Expert Consensus Document on Hypertrophic Cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. Eur. Heart J. 24, 1965–1991 (2003).
72. Elliott, P. & McKenna, W. J. Hypertrophic cardiomyopathy. Lancet 363, 1881–1891 (2004).
73. Niimura, H. et al. Mutations in the gene for cardiac myosin‑binding protein C and late‑onset familial hypertrophic cardiomyopathy. N. Engl. J. Med. 338, 1248–1257 (1998).
74. Maron, B. J. et al. Development of left ventricular hypertrophy in adults in hypertrophic cardiomyopathy caused by cardiac myosin‑binding protein C gene mutations. J. Am. Coll. Cardiol. 38, 315–321 (2001).
75. Charron, P. et al. Diagnostic value of electrocardiography and echocardiography for familial hypertrophic cardiomyopathy in a genotyped adult population. Circulation 96, 214–219 (1997).
76. Richardson, P. et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation 93, 841–842 (1996).
77. Shapiro, L. M. & McKenna, W. J. Distribution of left ventricular hypertrophy in hypertrophic cardiomyopathy: a two‑dimensional echocardiographic study. J. Am. Coll. Cardiol. 2, 437–444 (1983).
78. Charron, P. et al. Accuracy of European diagnostic criteria for familial hypertrophic cardiomyopathy in a genotyped population. Int. J. Cardiol. 90, 33–38 (2003).
79. Conrady, A. O. et al. Prevalence and determinants of left ventricular hypertrophy and remodelling patterns in hypertensive patients: the St. Petersburg study. Blood Press. 13, 101–109 (2004).
80. Nagueh, S. F. et al. Doppler estimation of left ventricular filling pressures in patients with hypertrophic cardiomyopathy. Circulation 99, 254–261 (1999).
81. Severino, S. et al. Use of pulsed Doppler tissue imaging to assess regional left ventricular diastolic dysfunction in hypertrophic cardiomyopathy. Am. J. Cardiol. 82, 1394–1398 (1998).
82. Maron, B. J. et al. Noninvasive assessment of left ventricular diastolic function by pulsed Doppler echocardiography in patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 10, 733–742 (1987).
83. Connelly, K. A. et al. Load sensitive measures may overestimate global systolic function in the presence of left ventricular hypertrophy: a comparison with load‑insensitive measures. Am. J. Physiol. Heart Circ. Physiol. 290, H1699–H1705 (2006).
84. Shimizu, G. et al. Left ventricular midwall mechanics in systemic arterial hypertension: myocardial function is depressed in pressure‑overload hypertrophy. Circulation 83, 1676–1684 (1991).
85. Sengupta, P. P., Mehta, V., Arora, R., Mohan, J. C. & Khandheria, B. K. Quantification of regional nonuniformity and paradoxical intramural mechanics in hypertrophic cardiomyopathy by high frame rate ultrasound myocardial strain mapping. J. Am. Soc. Echocardiogr. 18, 737–742 (2005).
86. Maron, B. J., Anan, T. J. & Roberts, W. C. Quantitative analysis of the distribution of cardiac muscle cell disorganization in the left ventricular wall of patients with hypertrophic cardiomyopathy. Circulation 63, 882–894 (1981).
87. Geisterfer‑Lowrance, A. A. et al. A mouse model of familial hypertrophic cardiomyopathy. Science 272, 731–734 (1996).
88. Karlon, W. J., McCulloch, A. D., Covell, J. W., Hunter, J. J. & Omens, J. H. Regional dysfunction correlates with myofiber disarray in transgenic mice with ventricular expression of ras. Am. J. Physiol. Heart Circ. Physiol. 278, H898–H906 (2000).
89. Chang, S. A. et al. Left ventricular twist mechanics in patients with apical hypertrophic cardiomyopathy: assessment with 2D speckle tracking echocardiography. Heart 96, 49–55 (2010).
90. van Dalen, B. M. et al. Influence of the pattern of hypertrophy on left ventricular twist in hypertrophic cardiomyopathy. Heart 95, 657–661 (2009).
91. Rajiv, C., Vinereanu, D. & Fraser, A. G. Tissue Doppler imaging for the evaluation of patients with hypertrophic cardiomyopathy. Curr. Opin. Cardiol. 19, 430–436 (2004).
92. Ito, T., Suwa, M., Tonari, S., Okuda, N. & Kitaura, Y. Regional postsystolic shortening in patients with hypertrophic cardiomyopathy: its incidence and characteristics assessed by strain imaging. J. Am. Soc. Echocardiogr. 19, 987–993 (2006).
93. Yang, H. et al. Use of strain imaging in detecting segmental dysfunction in patients with hypertrophic cardiomyopathy. J. Am. Soc. Echocardiogr. 16, 233–239 (2003).
94. Ganame, J. et al. Regional myocardial deformation in children with hypertrophic cardiomyopathy: morphological and clinical correlations. Eur. Heart J. 28, 2886–2894 (2007).
95. Weidemann, F. et al. A new echocardiographic approach for the detection of non‑ischaemic fibrosis in hypertrophic myocardium. Eur. Heart J. 28, 3020–3026 (2007).
96. Sun, J. P. et al. Differentiation of hypertrophic cardiomyopathy and cardiac amyloidosis from other causes of ventricular wall thickening by two‑dimensional strain imaging echocardiography. Am. J. Cardiol. 103, 411–415 (2009).
97. Kato, T. S. et al. Heterogeneity of regional systolic function detected by tissue Doppler imaging is linked to impaired global left ventricular relaxation in hypertrophic cardiomyopathy. Heart 94, 1302–1306 (2008).
98. Dong, S. J. et al. Left ventricular wall thickness and regional systolic function in patients with hypertrophic cardiomyopathy. A three‑dimensional tagged magnetic resonance imaging study. Circulation 90, 1200–1209 (1994).
99. Kim, Y. J. et al. Delayed enhancement in hypertrophic cardiomyopathy: comparison with
ReviewS
nrcardio_56_JUL10.indd 395 10/6/10 12:07:52
© 20 Macmillan Publishers Limited. All rights reserved10
396 | JULY 2010 | voLUme 7 www.nature.com/nrcardio
myocardial tagging MRI. J. Magn. Reson. Imaging 27, 1054–1060 (2008).
100. Piella, G. et al. Myocardial deformation from tagged MRI in hypertrophic cardiomyopathy using an efficient registration strategy. Proc. SPIE 7262, 726226 (2009).
101. Moon, J. C. et al. Myocardial late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy caused by mutations in troponin I. Heart 91, 1036–1040 (2005).
102. Falk, R. H. Diagnosis and management of the cardiac amyloidoses. Circulation 112, 2047–2060 (2005).
103. Dubrey, S. W. et al. The clinical features of immunoglobulin light‑chain (AL) amyloidosis with heart involvement. QJM 91, 141–157 (1998).
104. Kyle, R. A. & Gertz, M. A. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin. Hematol. 32, 45–59 (1995).
105. Robbins, M. A., Pizzarello, R. A., Stechel, R. P., Chiaramida, S. A. & Gulotta, S. J. Resting and exercise hemodynamics in constrictive pericarditis and a case of cardiac amyloidosis mimicking constriction. Cathet. Cardiovasc. Diagn. 9, 463–471 (1983).
106. Westermark, P., Sletten, K., Johansson, B. & Cornwell, G. G. 3rd. Fibril in senile systemic amyloidosis is derived from normal transthyretin. Proc. Natl Acad. Sci. USA 87, 2843–2845 (1990).
107. Ng, B., Connors, L. H., Davidoff, R., Skinner, M. & Falk, R. H. Senile systemic amyloidosis presenting with heart failure: a comparison with light chain‑associated (AL) amyloidosis. Arch. Intern. Med. 165, 1425–1429 (2005).
108. Wright, J. R. & Calkins, E. Amyloid in the aged heart: frequency and clinical significance. J. Am. Geriatr. Soc. 23, 97–103 (1975).
109. Ardehali, H. et al. Endomyocardial biopsy plays a role in diagnosing patients with unexplained cardiomyopathy. Am. Heart J. 147, 919–923 (2004).
110. Klein, A. L. et al. Serial Doppler echocardiographic follow‑up of left ventricular diastolic function in cardiac amyloidosis. J. Am. Coll. Cardiol. 16, 1135–1141 (1990).
111. Shah, K. B., Inoue, Y. & Mehra, M. R. Amyloidosis and the heart: a comprehensive review. Arch. Intern. Med. 166, 1805–1813 (2006).
112. Brenner, D. A. et al. Human amyloidogenic light chains directly impair cardiomyocyte function through an increase in cellular oxidant stress. Circ. Res. 94, 1008–1010 (2004).
113. Koyama, J., Ray‑Sequin, P. A., Davidoff, R. & Falk, R. H. Usefulness of pulsed tissue
Doppler imaging for evaluating systolic and diastolic left ventricular function in patients with AL (primary) amyloidosis. Am. J. Cardiol. 89, 1067–1071 (2002).
114. Koyama, J., Davidoff, R. & Falk, R. H. Longitudinal myocardial velocity gradient derived from pulsed Doppler tissue imaging in AL amyloidosis: a sensitive indicator of systolic and diastolic dysfunction. J. Am. Soc. Echocardiogr. 17, 36–44 (2004).
115. Koyama, J., Ray‑Sequin, P. A. & Falk, R. H. Longitudinal myocardial function assessed by tissue velocity, strain, and strain rate tissue Doppler echocardiography in patients with AL (primary) cardiac amyloidosis. Circulation 107, 2446–2452 (2003).
116. Maceira, A. M. et al. Cardiovascular magnetic resonance in cardiac amyloidosis. Circulation 111, 186–193 (2005).
117. Weidemann, F. et al. Long‑term effects of enzyme replacement therapy on fabry cardiomyopathy: evidence for a better outcome with early treatment. Circulation 119, 524–529 (2009).
118. Buyse, G. et al. Idebenone treatment in Friedreich’s ataxia: neurological, cardiac, and biochemical monitoring. Neurology 60, 1679–1681 (2003).
119. Weidemann, F. et al. Improvement of cardiac function during enzyme replacement therapy in patients with Fabry disease: a prospective strain rate imaging study. Circulation 108, 1299–1301 (2003).
120. Dutka, D. P. et al. Echocardiographic characterization of cardiomyopathy in Friedreich’s ataxia with tissue Doppler echocardiographically derived myocardial velocity gradients. Circulation 102, 1276–1282 (2000).
121. Pieroni, M. et al. Early detection of Fabry cardiomyopathy by tissue Doppler imaging. Circulation 107, 1978–1984 (2003).
122. Eng, C. M., Ioannou, Y. A. & Desnick, R. J. in The Metabolic and Molecular Bases of Inherited Disease 8th edn (eds Scriver, C. R. et al.) 3733–3774 (McGraw‑Hill, New York, 2001).
123. Meikle, P. J., Hopwood, J. J., Clague, A. E. & Carey, W. F. Prevalence of lysosomal storage disorders. JAMA 281, 249–254 (1999).
124. Mehta, A. et al. Fabry disease defined: baseline clinical manifestations of 366 patients in the Fabry Outcome Survey. Eur. J. Clin. Invest. 34, 236–242 (2004).
125. Linhart, A. et al. New insights in cardiac structural changes in patients with Fabry’s disease. Am. Heart J. 139, 1101–1108 (2000).
126. Weidemann, F. & Strotmann, J. M. Use of tissue Doppler imaging to identify and manage systemic diseases. Clin. Res. Cardiol. 97, 65–73 (2008).
127. Bogaert, J. & Rademakers, F. E. Regional nonuniformity of normal adult human left ventricle. Am. J. Physiol. Heart Circ. Physiol. 280, H610–H620 (2001).
128. Moon, J. C. et al. Gadolinium enhanced cardiovascular magnetic resonance in Anderson‑Fabry disease. Evidence for a disease specific abnormality of the myocardial interstitium. Eur. Heart J. 24, 2151–2155 (2003).
129. Eng, C. M. et al. Safety and efficacy of recombinant human alpha‑galactosidase A— replacement therapy in Fabry’s disease. N. Engl. J. Med. 345, 9–16 (2001).
130. Beer, M. et al. Impact of enzyme replacement therapy on cardiac morphology and function and late enhancement in Fabry’s cardiomyopathy. Am. J. Cardiol. 97, 1515–1518 (2006).
131. Bradley, J. L. et al. Clinical, biochemical and molecular genetic correlations in Friedreich’s ataxia. Hum. Mol. Genet. 9, 275–282 (2000).
132. Hewer, R. The heart in Friedreich’s ataxia. Br. Heart J. 31, 5–14 (1969).
133. Child, J. S. et al. Cardiac involvement in Friedreich’s ataxia: a clinical study of 75 patients. J. Am. Coll. Cardiol. 7, 1370–1378 (1986).
134. Weidemann, F. et al. Quantification of regional right and left ventricular function by ultrasonic strain rate and strain indexes in Friedreich’s ataxia. Am. J. Cardiol. 91, 622–626 (2003).
135. Rustin, P. et al. Effect of idebenone on cardiomyopathy in Friedreich’s ataxia: a preliminary study. Lancet 354, 477–479 (1999).
136. Biggar, W. D. Duchenne muscular dystrophy. Pediatr. Rev. 27, 83–88 (2006).
137. Hoffman, E. P., Brown, R. H. Jr & Kunkel, L. M. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell 51, 919–928 (1987).
AcknowledgmentsThis work was partially funded by the Ministry of Science, Education and Sports of the Republic of Croatia (project number 108‑1081875‑1991), and the L’Oréal‑UNESCO Scholarship for Women in Science.
Charles P. Vega, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the MedscapeCME‑accredited continuing medical education activity associated with this article.
ReviewS
nrcardio_56_JUL10.indd 396 10/6/10 12:07:53
© 20 Macmillan Publishers Limited. All rights reserved10