Embed Size (px)
Citation preview

The Road to Population Health:
Key Enablers in Implementing Value-Based Models
Webinar January 23, 2013
CONFIDENTIAL AND PROPRIETARY
Any use of this material without specific permission of McKinsey & Company is strictly prohibited
James Stanford, Client Service Executive
Objective Health, a McKinsey Solution for Healthcare Providers
Peter Groves
McKinsey & Company
Will Wright, Luís Almeida Fernandes & Greg Gilbert
McKinsey & Company
What are examples of
implementation at scale?
What is underpinning the move to
population-based models?
What enabling technology or
services are required?
1
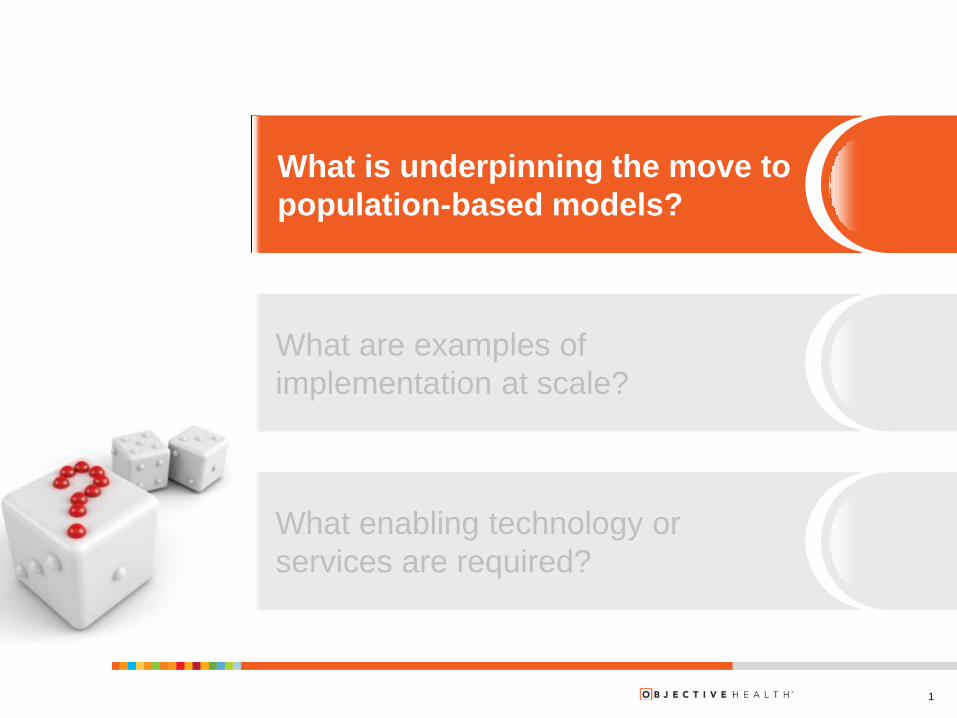
All stakeholders are feeling pressure from the rising costs of healthcare
Sources: Milliman Medical Index; National Health Expenditures; Kaiser Family
Foundation; Interstudy; U.S. Census
1 Including government
Payors1
▪ Payors are increasingly shifting risk to providers given the broader push to quality
and outcomes by CMS
▪ Need for low price products is driving payors to contract on a reduced cost network
▪ Dual eligibles and Medicare Advantage are a rapidly growing segment; both are
high risk causing payors to further consider alternate arrangements with providers
▪ Acute reimbursement pressure leading to health systems and physicians considering
alternate revenue sources and hence value based reimbursements or launching
their own health plan
▪ Increasing number of small solutions providers that are looking to capture value
within this growing market
▪ Cost pressures and scale issues leading to consolidation
Health
systems
▪ Physicians are consolidating, driven by hospital employment
▪ Shortage of PCPs requires change in care delivery models
▪ Going forward, increasing number of physicians see themselves participating in at
least “gain sharing” reimbursement models
Physicians
▪ Growing trend of employers pursuing innovative models of providing care, such as
narrowing their networks to preferred partners or going directly to providers
▪ Employers continue to see opportunity by investing in health management
programs
Employers
2
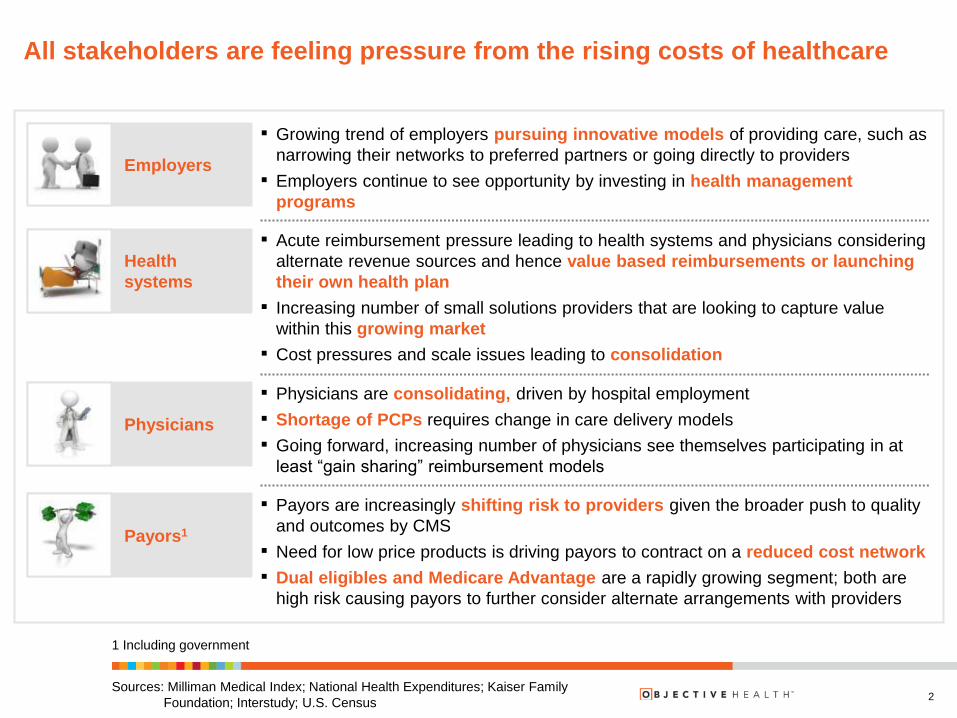
Payors and providers are responding with new approaches to managing
cost and care quality
▪ Focusing on reducing medical cost
trend
▪ Linking reimbursement to value
creation, based on quality, cost
efficiency, and patient experience
▪ Creating product and consumer
strategy that steers members to
highest performing providers
▪ Providing members with reliable
quality and cost information on
providers
Identifying patients at risk and
developing protocols for prevention
Working across the care continuum
Sharing and aggregating
information
Aligning and managing incentives
between healthcare stakeholders
How payors are responding How providers are responding
3
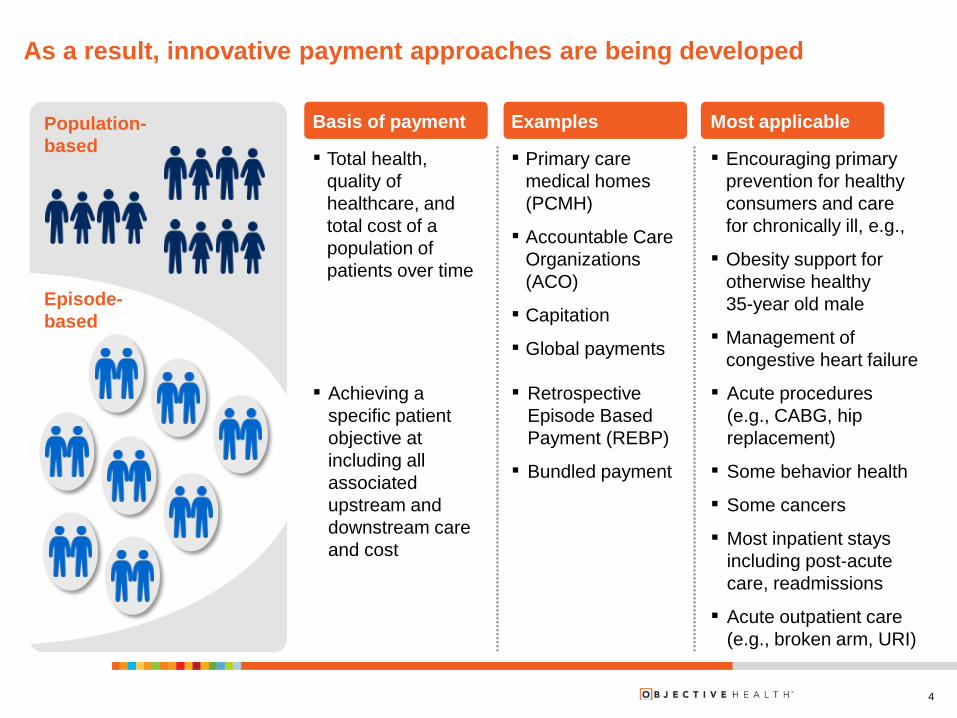
Examples Most applicable Basis of payment Population-
based
Episode-
based
As a result, innovative payment approaches are being developed
▪ Total health,
quality of
healthcare, and
total cost of a
population of
patients over time
▪ Primary care
medical homes
(PCMH)
▪ Accountable Care
Organizations
(ACO)
▪ Capitation
▪ Global payments
▪ Encouraging primary
prevention for healthy
consumers and care
for chronically ill, e.g.,
▪ Obesity support for
otherwise healthy
35-year old male
▪ Management of
congestive heart failure
▪ Achieving a
specific patient
objective at
including all
associated
upstream and
downstream care
and cost
▪ Retrospective
Episode Based
Payment (REBP)
▪ Bundled payment
▪ Acute procedures
(e.g., CABG, hip
replacement)
▪ Some behavior health
▪ Some cancers
▪ Most inpatient stays
including post-acute
care, readmissions
▪ Acute outpatient care
(e.g., broken arm, URI)
4
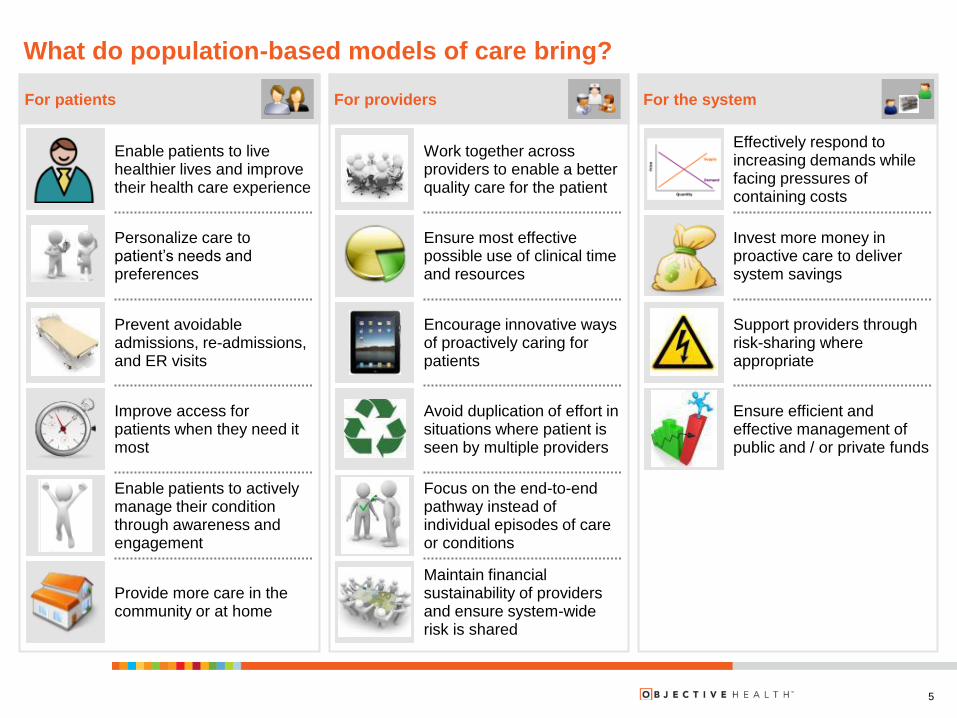
What do population-based models of care bring?
For the system
Ensure efficient and effective management of public and / or private funds
Invest more money in proactive care to deliver system savings
Effectively respond to increasing demands while facing pressures of containing costs
Support providers through risk-sharing where appropriate
For providers
Focus on the end-to-end pathway instead of individual episodes of care or conditions
Avoid duplication of effort in situations where patient is seen by multiple providers
Ensure most effective possible use of clinical time and resources
Work together across providers to enable a better quality care for the patient
Encourage innovative ways of proactively caring for patients
Maintain financial sustainability of providers and ensure system-wide risk is shared
For patients
Enable patients to actively manage their condition through awareness and engagement
Improve access for patients when they need it most
Personalize care to patient’s needs and preferences
Enable patients to live healthier lives and improve their health care experience
Prevent avoidable admissions, re-admissions, and ER visits
Provide more care in the community or at home
5

Payors are aggressively pursuing innovative payment models
6 Source: Team analysis
Ris
k s
hari
ng
F
ull r
isk
“Provider-led”
integrated
network
ACO
“Payor-led”
integrated
network
Episodes of
care
Pay for value
Patient
centered
medical home
“Basic P4P”
▪ Payor - led affiliation or acquisition of health system which seeks
full clinical and operational integration to reduce costs, improve
member experience, and manage referral volume
▪ Provider system builds a health-plan, leveraging brand name to
drive volume to provider system
▪ An organization of health care providers accountable for quality,
cost, and overall care; share cost savings if performance metrics
are met
▪ Covers all aspects of preadmission, inpatient, and follow-up care,
including postoperative complications within a set time period for
procedures, e.g., hip replacement
▪ Team of physicians and extenders, coordinated by a PCP,
coordinate provide high levels of coordinated care; typically tied
to P4P contract
▪ Payment bonus tied to efficiency metrics (e.g., reduction in ER
visits, imaging)
▪ Payment upside based on performance metrics linked to value
creation (e.g. RCSMA Alternative Quality Contract I AQC)
Inc
en
tive
paym
en
t G
ain
sh
ari
ng
Exc
lus
ive
ly u
psid
e
op
po
rtu
nit
y
Bo
th u
psid
e a
nd
do
wn
sid
e r
isk
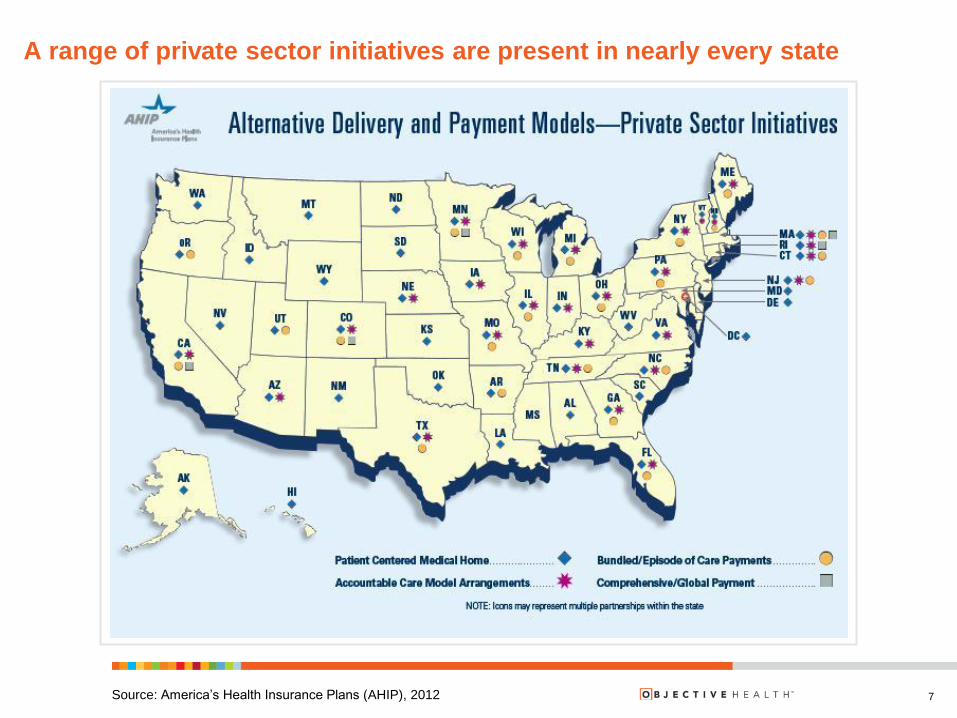
A range of private sector initiatives are present in nearly every state
Source: America’s Health Insurance Plans (AHIP), 2012 7
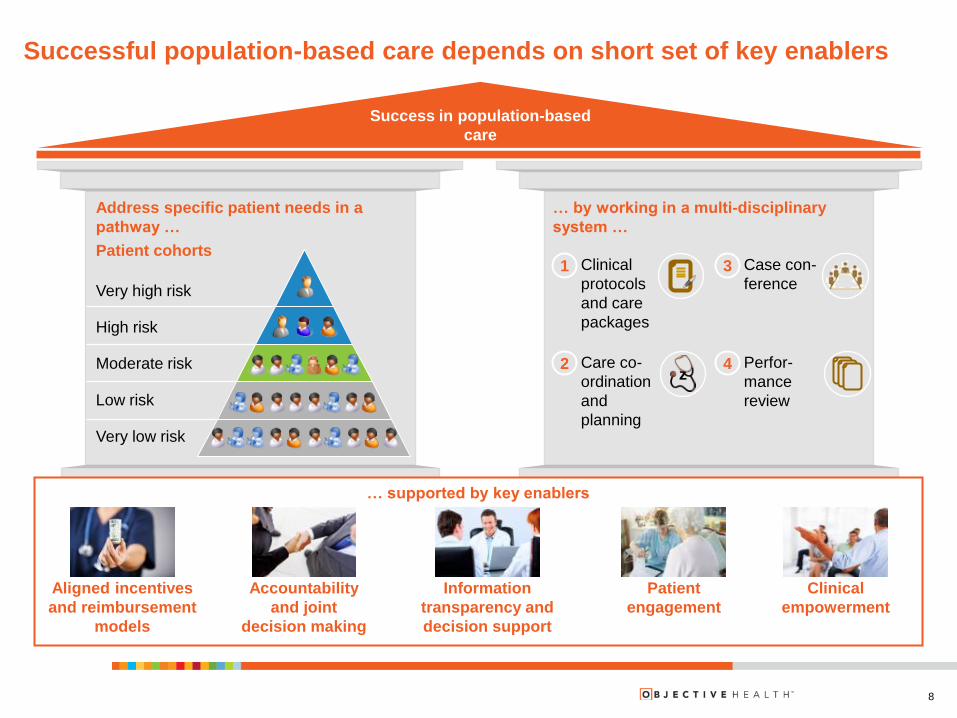
Successful population-based care depends on short set of key enablers
Success in population-based
care
Address specific patient needs in a
pathway …
Patient cohorts
Very high risk
High risk
Moderate risk
Low risk
Very low risk
… by working in a multi-disciplinary
system …
Clinical
protocols
and care
packages
1
z Care co-
ordination
and
planning
2
Case con-
ference 3
Perfor-
mance
review
4
… supported by key enablers
Aligned incentives
and reimbursement
models
Accountability
and joint
decision making
Information
transparency and
decision support
Clinical
empowerment
8
Patient
engagement
What do you see as the most influential lever to implementing population-
based models at scale?
INTERACTIVE POLL
Pick the best answer from the following list
Aligning payor and provider incentives
Accountability & joint decision-making among providers
Information transparency & decision support
9
Establishing direct patient engagement
Clinical empowerment
What is underpinning the move to
population-based models?
10
Q&A Discussion
What are examples of
implementation at scale?
What is underpinning the move to
population-based models?
What enabling technology or
services are required?
11
12
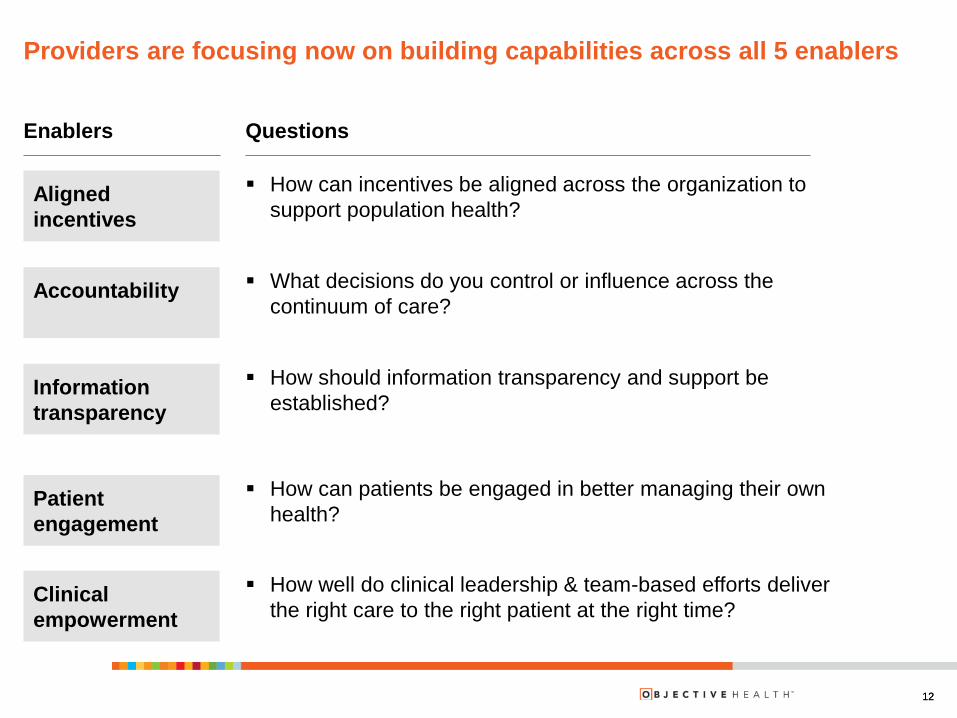
Providers are focusing now on building capabilities across all 5 enablers
Questions
How can incentives be aligned across the organization to
support population health? Aligned
incentives
Accountability
Information
transparency
What decisions do you control or influence across the
continuum of care?
How should information transparency and support be
established?
12
Enablers
Patient
engagement
How can patients be engaged in better managing their own
health?
Clinical
empowerment
How well do clinical leadership & team-based efforts deliver
the right care to the right patient at the right time?
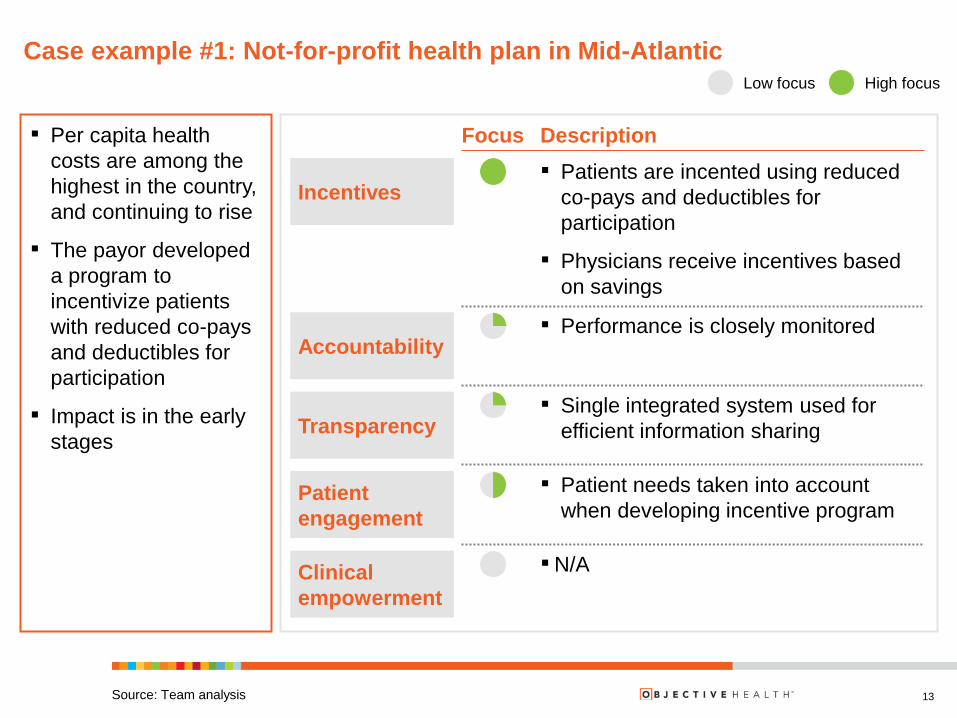
Case example #1: Not-for-profit health plan in Mid-Atlantic
13
Low focus High focus
Description Focus
Incentives ▪ Patients are incented using reduced
co-pays and deductibles for
participation
▪ Physicians receive incentives based
on savings
Accountability ▪ Performance is closely monitored
Transparency ▪ Single integrated system used for
efficient information sharing
Patient
engagement
▪ Patient needs taken into account
when developing incentive program
▪ N/A Clinical
empowerment
▪ Per capita health
costs are among the
highest in the country,
and continuing to rise
▪ The payor developed
a program to
incentivize patients
with reduced co-pays
and deductibles for
participation
▪ Impact is in the early
stages
Source: Team analysis
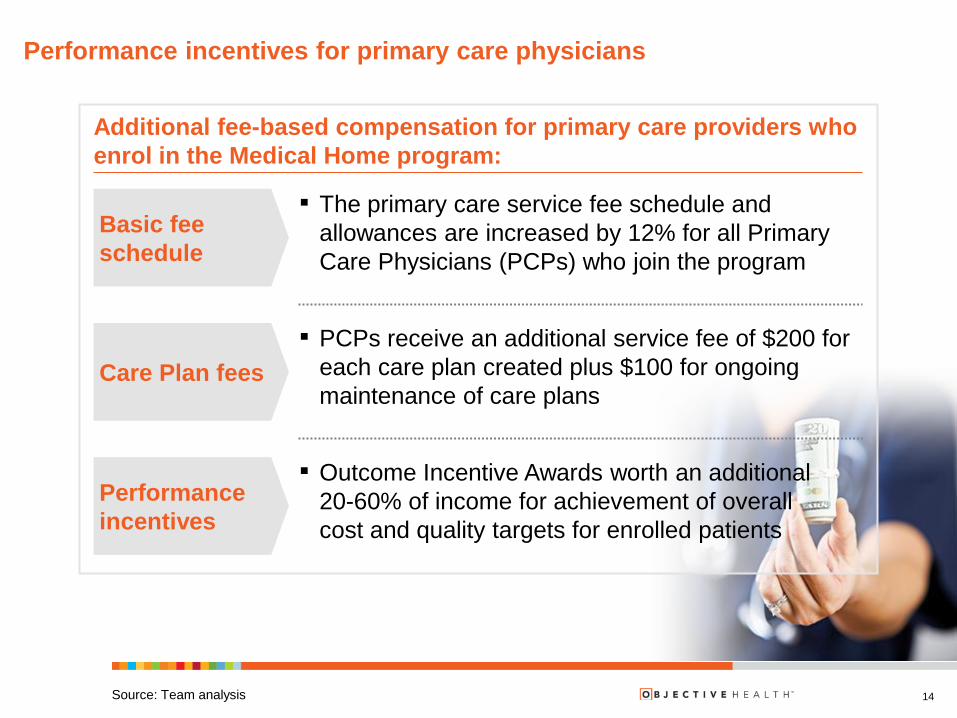
Performance incentives for primary care physicians
14
Additional fee-based compensation for primary care providers who
enrol in the Medical Home program:
Performance
incentives
Basic fee
schedule
▪ The primary care service fee schedule and
allowances are increased by 12% for all Primary
Care Physicians (PCPs) who join the program
Care Plan fees
▪ PCPs receive an additional service fee of $200 for
each care plan created plus $100 for ongoing
maintenance of care plans
▪ Outcome Incentive Awards worth an additional
20-60% of income for achievement of overall
cost and quality targets for enrolled patients
Source: Team analysis
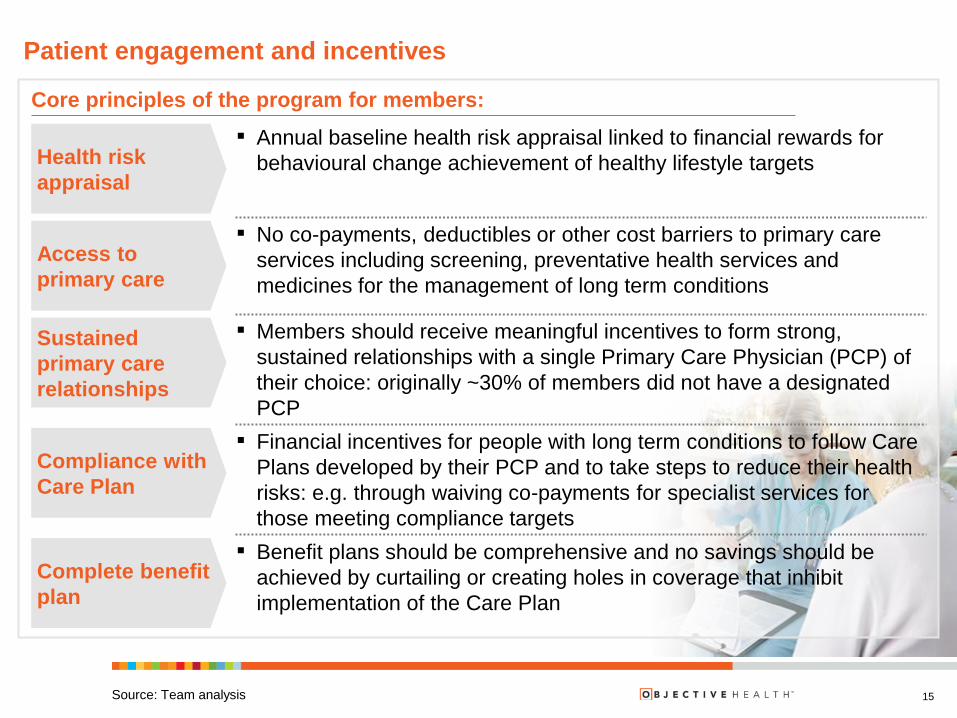
Patient engagement and incentives
15
Core principles of the program for members:
Health risk
appraisal
▪ Annual baseline health risk appraisal linked to financial rewards for
behavioural change achievement of healthy lifestyle targets
Access to
primary care
▪ No co-payments, deductibles or other cost barriers to primary care
services including screening, preventative health services and
medicines for the management of long term conditions
Sustained
primary care
relationships
▪ Members should receive meaningful incentives to form strong,
sustained relationships with a single Primary Care Physician (PCP) of
their choice: originally ~30% of members did not have a designated
PCP
Compliance with
Care Plan
▪ Financial incentives for people with long term conditions to follow Care
Plans developed by their PCP and to take steps to reduce their health
risks: e.g. through waiving co-payments for specialist services for
those meeting compliance targets
Complete benefit
plan
▪ Benefit plans should be comprehensive and no savings should be
achieved by curtailing or creating holes in coverage that inhibit
implementation of the Care Plan
Source: Team analysis
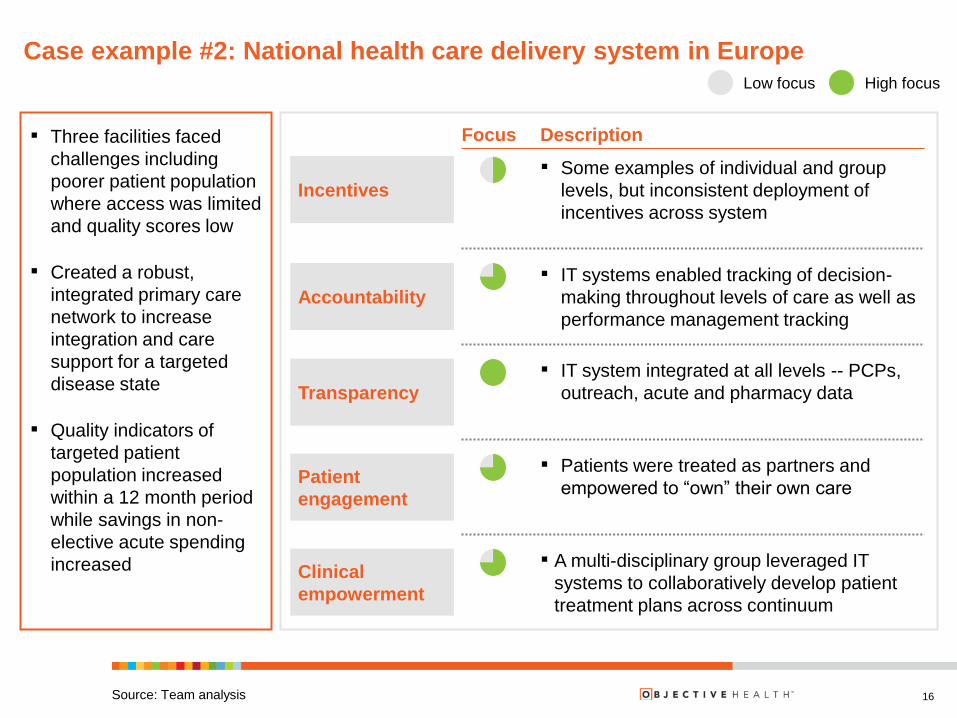
Case example #2: National health care delivery system in Europe
16
Description Focus
Incentives
▪ Some examples of individual and group
levels, but inconsistent deployment of
incentives across system
Accountability
▪ IT systems enabled tracking of decision-
making throughout levels of care as well as
performance management tracking
Transparency
▪ IT system integrated at all levels -- PCPs,
outreach, acute and pharmacy data
Patient
engagement
▪ Patients were treated as partners and
empowered to “own” their own care
▪ A multi-disciplinary group leveraged IT
systems to collaboratively develop patient
treatment plans across continuum
Clinical
empowerment
▪ Three facilities faced
challenges including
poorer patient population
where access was limited
and quality scores low
▪ Created a robust,
integrated primary care
network to increase
integration and care
support for a targeted
disease state
▪ Quality indicators of
targeted patient
population increased
within a 12 month period
while savings in non-
elective acute spending
increased
Source: Team analysis
Low focus High focus
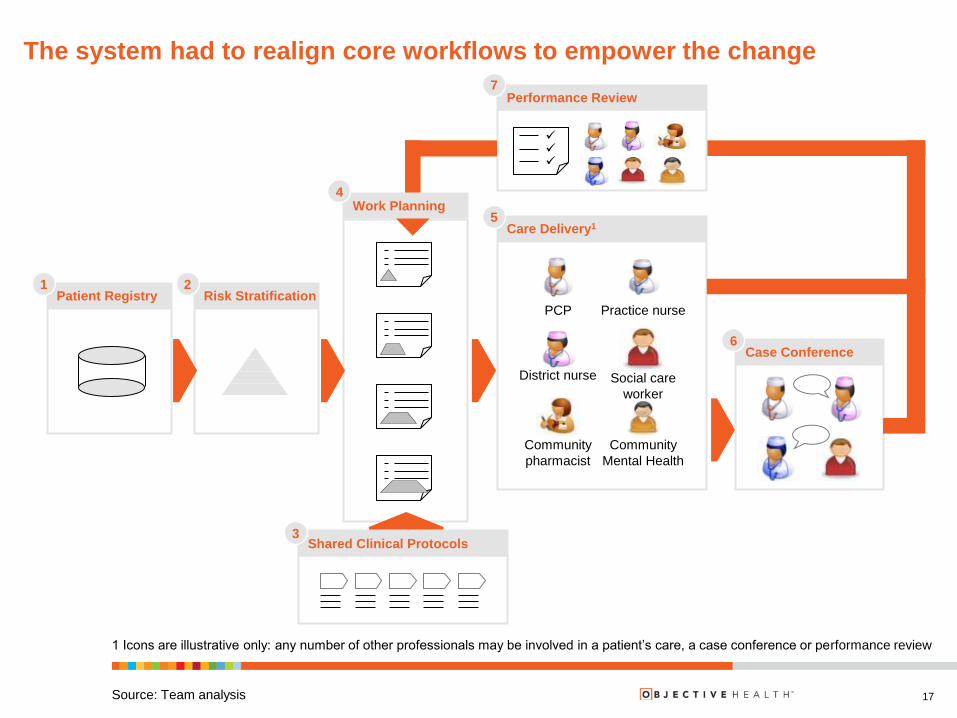
The system had to realign core workflows to empower the change
17
1 Icons are illustrative only: any number of other professionals may be involved in a patient’s care, a case conference or performance review
Community
pharmacist
Practice nurse
Social care
worker
District nurse
PCP
Community
Mental Health
Patient Registry Risk Stratification
Care Delivery1
Case Conference
Performance Review
1 2
5
Shared Clinical Protocols 3
6
7
Work Planning 4
Source: Team analysis
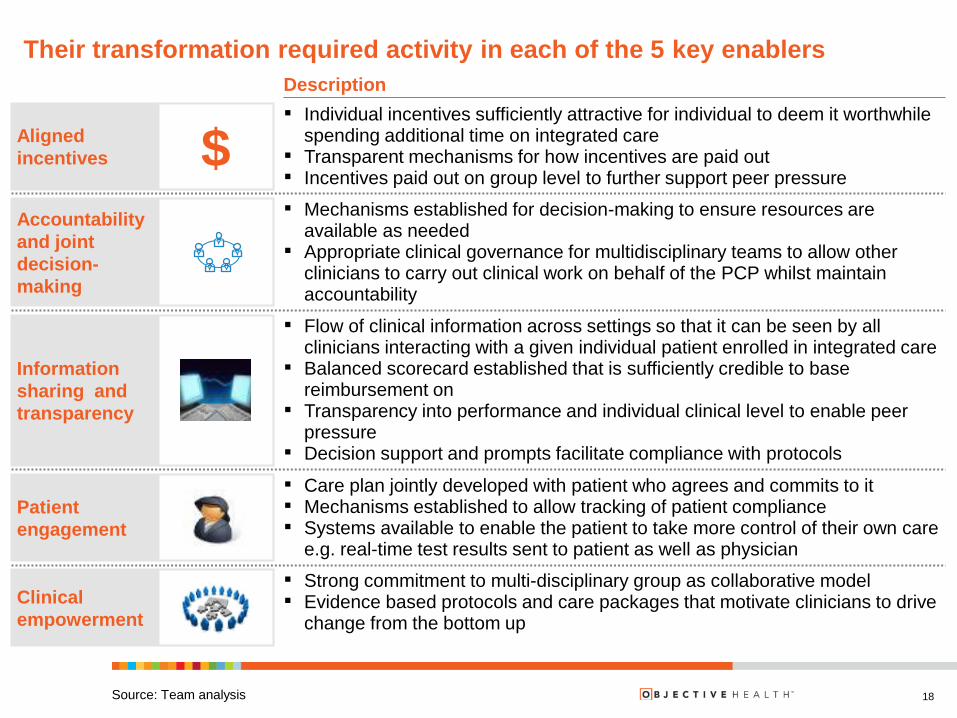
Their transformation required activity in each of the 5 key enablers
18 Source: Team analysis
Description
$ Aligned
incentives
▪ Individual incentives sufficiently attractive for individual to deem it worthwhile spending additional time on integrated care
▪ Transparent mechanisms for how incentives are paid out ▪ Incentives paid out on group level to further support peer pressure
Accountability
and joint
decision-
making
▪ Mechanisms established for decision-making to ensure resources are available as needed
▪ Appropriate clinical governance for multidisciplinary teams to allow other clinicians to carry out clinical work on behalf of the PCP whilst maintain accountability
Information
sharing and
transparency
▪ Flow of clinical information across settings so that it can be seen by all clinicians interacting with a given individual patient enrolled in integrated care
▪ Balanced scorecard established that is sufficiently credible to base reimbursement on
▪ Transparency into performance and individual clinical level to enable peer pressure
▪ Decision support and prompts facilitate compliance with protocols
Patient
engagement
▪ Care plan jointly developed with patient who agrees and commits to it ▪ Mechanisms established to allow tracking of patient compliance ▪ Systems available to enable the patient to take more control of their own care
e.g. real-time test results sent to patient as well as physician
Clinical
empowerment
▪ Strong commitment to multi-disciplinary group as collaborative model ▪ Evidence based protocols and care packages that motivate clinicians to drive
change from the bottom up
How quickly do you see population management models accelerating in the
market over the next 3 years?
INTERACTIVE POLL
Pick the best answer from the following list
Minimal: will take a long time to scale, if at all
Slow but steady: implementation will slow the pace
Selective: some will grow quickly but won’t become majority
Explosive: will rapidly become the “new normal”
19
What are examples of
implementation at scale?
20
Q&A Discussion
What are examples of
implementation at scale?
What is underpinning the move to
population-based models?
What enabling technology or
services are required?
21
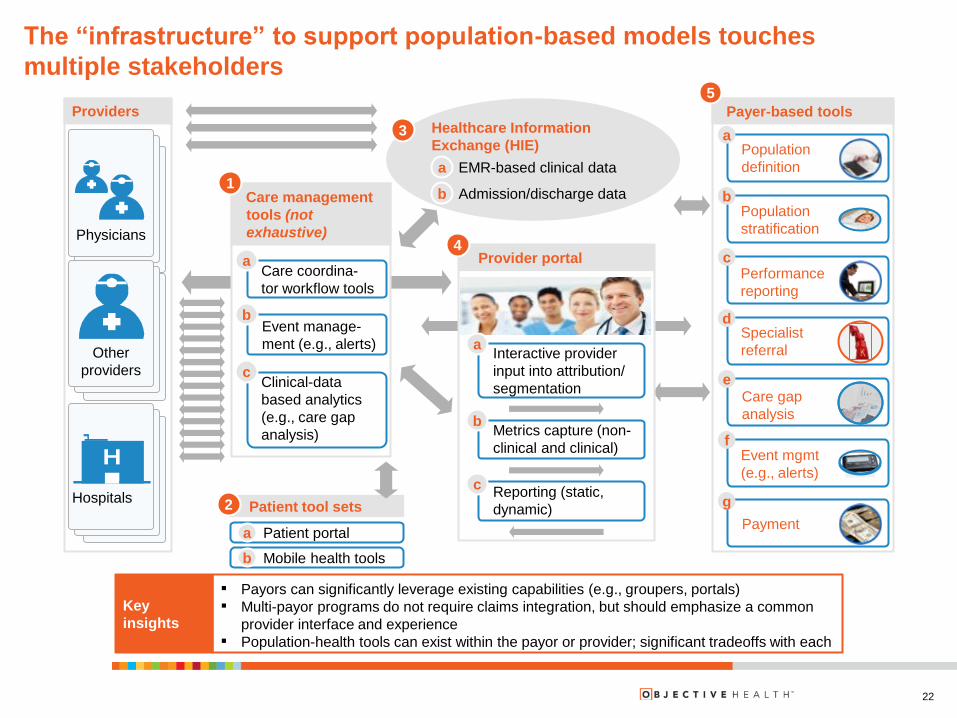
The “infrastructure” to support population-based models touches
multiple stakeholders
Key
insights
▪ Payors can significantly leverage existing capabilities (e.g., groupers, portals)
▪ Multi-payor programs do not require claims integration, but should emphasize a common
provider interface and experience
▪ Population-health tools can exist within the payor or provider; significant tradeoffs with each
Patient tool sets
A Patient portal
B Mobile health tools
3
2
Payer-based tools
5
Providers
Physicians
Hospitals
Other
providers
Care management
tools (not
exhaustive)
1
Care coordina-
tor workflow tools
a
Event manage-
ment (e.g., alerts)
b
Clinical-data
based analytics
(e.g., care gap
analysis)
c
Provider portal
Interactive provider
input into attribution/
segmentation
a
Metrics capture (non-
clinical and clinical)
b
Reporting (static,
dynamic)
c
Population
definition
a
Population
stratification
b
Performance
reporting
c
Specialist
referral
d
Care gap
analysis
e
Event mgmt
(e.g., alerts)
f
Payment
g
Healthcare Information
Exchange (HIE)
EMR-based clinical data a
Admission/discharge data b
4
a
b
22

Technology requirements increase with each stage of population health
maturity
23 Source: Team analysis
Stage 0
Program design
Stage 1
Population analytics
Stage 2
Clinically integrated care
management tool sets
Stage 3
Virtually integrated health system
Description
▪ Required analytics in place to
develop payment model,
attribute patients an pool
providers
▪ Provider enabled with robust
administrative-data based
analytics on relevant sub-
populations and limited
patient-level analysis
▪ Care managers have care
management workflow tools
with real-time access to
clinical (e.g., EMR) data
▪ Optimized, learning ACO
capturing value across all
categories
▪ “Virtual integration” with
mature systems
Admit/
Disch.
Clinical
(partial)
Data
require-
ments
(incre-
mental)
Admin.
Clinical
(system
wide)
Performance improvement
Core technology
capabilities
(incremental)
Population definition
– Patient attribution
– Patient risk adjustment
– Provider pooling
5a
Risk stratification 5b
Payment 5h
Admission/discharge data
exchange 3a
Performance reporting 5c
Specialist referral 5d
Care gap analysis 5e
Event management
(Admission/discharge) 5f
Care management workflow
tools 1a
Clinical data driven event
management (e.g. alerts) 1b
Clinical-data driven analytics
(e.g., care gap analysis) 1c
EMR-based clinical data
exchange 3a
EMR-based clinical data
exchange (all providers) 3a
Mobile health tools 2b
Key
insights
▪ Upgraded payor and provider analytic capabilities are central to creating value
▪ EMR-based data exchange and provider-based tools are not required to achieve short-
term impact, but are critical to maximize value and sustain savings
▪ PCMH program should have basic Stage 1 capabilities at time of launch, though provider-
based tools (e.g., care management workflow) can be deployed post-launch
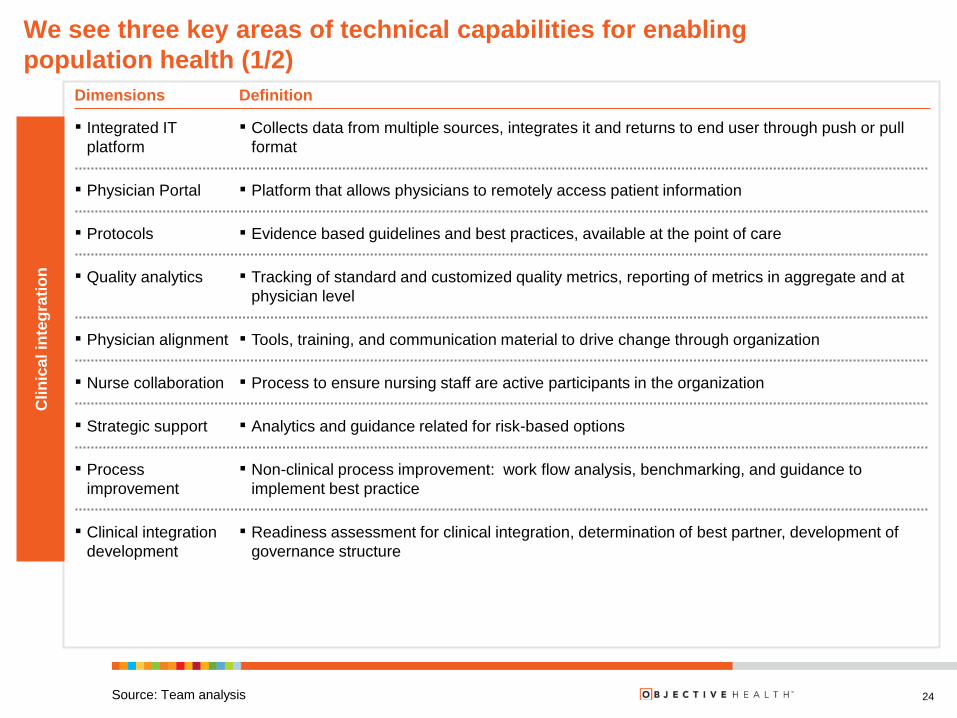
We see three key areas of technical capabilities for enabling
population health (1/2)
Source: Team analysis
Definition Dimensions
▪ Tools, training, and communication material to drive change through organization ▪ Physician alignment
▪ Nurse collaboration ▪ Process to ensure nursing staff are active participants in the organization
▪ Analytics and guidance related for risk-based options ▪ Strategic support
▪ Non-clinical process improvement: work flow analysis, benchmarking, and guidance to
implement best practice
▪ Process
improvement
▪ Readiness assessment for clinical integration, determination of best partner, development of
governance structure
▪ Tracking of standard and customized quality metrics, reporting of metrics in aggregate and at
physician level
▪ Quality analytics
▪ Protocols ▪ Evidence based guidelines and best practices, available at the point of care
▪ Collects data from multiple sources, integrates it and returns to end user through push or pull
format
▪ Clinical integration
development
▪ Integrated IT
platform
▪ Platform that allows physicians to remotely access patient information ▪ Physician Portal
Clin
ica
l in
teg
rati
on
24

We see three key areas of technical capabilities for enabling
population health (2/2)
Source: Team analysis
Definition Dimensions
▪ Chronic disease
management
▪ Coordination of care across settings with standardized protocols and interventions for pre-
chronic patients
▪ Identification of high-risk patients and notification of care providers for steps to take ▪ Predictive analytics
▪ Post-acute care ▪ Identification of partners for post-acute services & contracting
▪ Case management ▪ Care coordination for patient, including non-clinical programs to impact health
▪ Patient portal ▪ Access to health information and comparison of choices for care
▪ Tracking and actions to improve patient adherence
▪ Wellness ▪ Life-style interventions and coaches
▪ Field support ▪ Non-clinical support services to patients at point of care or in home, e.g., ensuring patients have
resources in the community to manage their health post-discharge
▪ Call center for patient’s clinical questions
▪ Claims processing, check cutting, audit support
▪ Identification of sources of variability in cost and utilization & suggest solutions ▪ Cost and utilization
analytics
▪ Financial analytics ▪ Preparation of financial statements, identification of drivers of costs, budgeting support
▪ Call center ▪ Support for customer financial questions
▪ TPA services
▪ Contract
management
▪ Analytics to understand patient population, risk assessment to inform contract negotiations
▪ Patient outreach
▪ Outcomes tracking ▪ Track wellness programs and determine if they work
Hea
lth
ca
re m
an
ag
em
en
t F
ina
ncia
l ri
sk
25
What tech-enabled capabilities do you believe your organization will need to
make a top priority?
INTERACTIVE POLL
Pick the best answer from the following list
Clinical integration
Population health
Financial risk
All areas equally
26
What enabling technology or
services are required?
27
Q&A Discussion

Join us for our next webinar:
28
Topic: New Innovations in Revenue Cycle
Management
Wednesday, April 24, 2013
1pm – 2pm EST
Q & A
The Road to Population Health:
Key Enablers in Implementing Value-Based
Models
CONFIDENTIAL AND PROPRIETARY
Any use of this material without specific permission of McKinsey & Company is strictly prohibited
James Stanford, Client Service Executive
Objective Health, a McKinsey Solution for Healthcare Providers
Peter Groves
McKinsey & Company
Will Wright, Luís Almeida Fernandes & Greg Gilbert
McKinsey & Company
For more information visit: www.objectivehealth.com