Embed Size (px)
Citation preview

The Risk of Exposure to DiagnosticUltrasound in Postnatal SubjectsNonthermal Mechanisms
Charles C. Church, PhD, Edwin L. Carstensen, PhD,Wesley L. Nyborg, PhD, Paul L. Carson, PhD, Leon A. Frizzell, PhD, Michael R. Bailey, PhD
his review examines the nonthermal physical mecha-nisms by which ultrasound can harm tissue in postnatalpatients. First the physical nature of the more significantinteractions between ultrasound and tissue is described,
followed by an examination of the existing literature with par-ticular emphasis on the pressure thresholds for potentialadverse effects. The interaction of ultrasonic fields with tissuedepends in a fundamental way on whether the tissue naturallycontains undissolved gas under normal physiologic conditions.Examples of gas-containing tissues are lung and intestine.Considerable effort has been devoted to investigating theacoustic parameters relevant to the threshold and extent oflung hemorrhage. Thresholds as low as 0.4 MPa at 1 MHz havebeen reported. The situation for intestinal damage is similar,although the threshold appears to be somewhat higher. Forother tissues, auditory stimulation or tactile perception mayoccur, if rarely, during exposure to diagnostic ultrasound; ultra-sound at similar or lower intensities is used therapeutically toaccelerate the healing of bone fractures. At the exposure levelsused in diagnostic ultrasound, there is no consistent evidencefor adverse effects in tissues that are not known to contain sta-bilized gas bodies. Although modest tissue damage may occurin certain identifiable applications, the risk for induction of anadverse biological effect by a nonthermal mechanism due toexposure to diagnostic ultrasound is extremely small. Keywords: cavitation; intestinal hemorrhage; lung hemorrhage;mechanical effects; nonthermal mechanism.
AbbreviationsALARA, as low as reasonably achievable; CW, continu-ous wave; MI, mechanical index; PRF, pulse repetitionfrequency
© 2008 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 2008; 27:565–592 • 0278-4297/08/$3.50
T
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d
Article includes CME testCME
Received April 12, 2007, from the National Centerfor Physical Acoustics, University of Mississippi,University, Mississippi USA (C.C.C.); Departmentof Electrical Engineering, University of Rochester,Rochester, New York USA (E.L.C.); Department ofPhysics, University of Vermont, Burlington,Vermont USA (W.L.N.); Department of Radiology,University of Michigan, Ann Arbor, Michigan USA(P.L.C.); Department of Electrical and ComputerEngineering, University of Illinois, Urbana, IllinoisUSA (L.A.F.); and Center for Industrial and MedicalUltrasound, Applied Physics Laboratory, Universityof Washington, Seattle, Washington (M.R.B.).Revision requested April 18, 2007. Revisedmanuscript accepted for publication December 4,2007.
Address correspondence to Charles C. Church,PhD, National Center for Physical Acoustics,University of Mississippi, 1 Coliseum Dr, University,MS 38677 USA.
E-mail: [email protected]

Unlike most imaging modalities, diagnosticultrasound necessarily induces mechanicalstrain in tissue. This strain is highest in proximityto gas or vapor bubbles. In the presence of ultra-sound fields like those used in diagnosis, gasbubbles such as those in ultrasound contrastagents as well as naturally occurring gas bodiescan damage adjacent tissue. In the case ofmicrometer-sized bubbles (ie, microbubbles) ingeneral and contrast agents in particular, thedamage is extremely localized, being confined tothe immediate vicinity of the bubble, which isusually in a blood vessel. Sufficient informationis now available concerning effects from contrastmicrobubbles, and they are potentially of suchimportance that they are the topic of a separatearticle in this issue (see Miller et al34). This reviewdeals with potential effects resulting from theinteraction of ultrasound fields with tissues con-taining naturally occurring gas bodies as well astissues not known to contain gas bodies undernormal physiologic conditions.
Fundamentals
As an ultrasound wave travels through a mediumsuch as tissue, the pressure varies above andbelow the ambient value by an amount called theacoustic pressure. If the acoustic pressure isappreciably less than the ambient pressure, thewave propagates under linear conditions.Diagnostic techniques such as harmonicimaging make use of the nonlinear character-istics of propagation of large-amplitude signals.However, there is little evidence that nonlinearpropagation plays a significant role in the non-thermal biological effects of ultrasound. Underlinear conditions, in a continuous wave (CW) ofa single frequency f, the acoustic pressure variessinusoidally in time and space, the distancebetween consecutive maxima being the wave-length λ. When the wave is pulsed, the oscilla-tions occur only during the pulses, the ratio of“on” time to “off” time being the duty factor.Current medical ultrasound uses longitudinalpressure waves. If a longitudinal pressure wavetravels through a medium in the x direction, the“particles” (small-volume elements) that consti-tute the medium oscillate along that direction.Under linear conditions, the particle velocity in
the wave varies sinusoidally in time and spacewith the same frequency and the same spacingas the pressure.
Newton’s second law of motion describes theforward and backward motion of the particlesthat make up the propagating medium. Whenthe mass involved is a part of a continuoussound-propagating medium, the appropriateform for Newton’s second law is
(1)
where FV is the instantaneous force per unit vol-ume; ρ is the density; and Du/Dt is the totalderivative of the particle velocity u. At any instant,the density varies periodically along the directionof sound propagation, and at any position in themedium, the density varies periodically with timeas the wave passes. The total derivative takes intoaccount the fact that the particle velocity dependson both time and the field position of the particleof mass under consideration.
When the shear properties of the propagatingmedium can be neglected, the force FV (per unitvolume) that moves the particle in an acousticwave traveling in the x direction is equal to thenegative gradient of the scalar magnitude ofthe acoustic pressure (–∂p/∂x). This is a goodapproximation for the force per unit volumeeven with the viscous fluids and soft tissuesthat are the propagation paths for most diag-nostic ultrasound.
As the wave (ie, the pattern of oscillating pres-sure and particle velocity) travels, potential andkinetic energy are imparted to the tissue or othermedium through which it passes. It is shown inacoustic theory that the potential and kineticenergy densities for a plane wave are the same,and their sum, the total energy per unit volume Efor a plane wave is equal to ρouo
2, where ρo is theequilibrium density, and uo is the particle veloci-ty amplitude. The wave and its energy movethrough the medium at the speed of sound c. Therate per unit area at which energy is transmittedacross a boundary is called the intensity I and isequal to E c.
In the subsequent discussion, we shall use ter-minology from acoustic theory and refer to suchoscillating quantities as the acoustic pressureand particle velocity as first-order quantities and
Dt
DuF ρV = ,
566 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

to the energy density E and intensity I as second-order quantities. A characteristic of a second-order quantity is that, like the kinetic energydensity, it is proportional to the square of a first-order quantity, or, more generally, to a product oftwo first-order quantities. Quantities of both firstand second order are relevant in discussing pos-sible causes of biological effects. Adverse clinicalimpacts from these effects can be avoided with-out compromising diagnostic information. To doso, however, it is important that practitioners beaware of possible mechanical (as well as ther-mal) effects of ultrasound. Both first- and sec-ond-order phenomena are discussed in detail inNational Council for Radiation Protection andMeasurements report 140, Exposure Criteria forMedical Diagnostic Ultrasound, II: Criteria Basedon All Known Mechanisms.1
Radiation Force
The force in Equation 1 that moves the particlesforward and backward during wave propagationunder typical diagnostic conditions (eg, 1 MPa at2 MHz) is on the order of 1010 N/m3 or about 1million times the force that gravity would exerton the same material. Despite these hugeforces, the particles shift only about 50 nm fromtheir equilibrium positions as the sound passesthrough the medium. If the propagating medi-um is lossless, the time average of the acousticforces is 0.
When some of the energy of the acoustic waveis absorbed by the medium and converted intoheat, the time average of the force per unit vol-ume on the medium has a small net value calledthe radiation body force, which is given by
(2)
Here, α is the absorption coefficient of the medi-um, and c is the sound speed. Because FVR is pro-portional to I, the radiation force is also aquantity of second order.
The intensity in the example above (1 MPa at 2MHz) is approximately 3 ⋅ 105 W/m2 (33 W/cm2).With a typical absorption coefficient for soft tis-sue of 10 nepers/m, this gives a radiation force ofabout 4000 N/m3, about half of the force thatgravity would exert on the same material.
As the wave penetrates the tissue, its amplitudeis reduced exponentially with depth (assuming ahomogeneous path); hence, the radiation bodyforce decreases in the same manner. The totalforce FR exerted on the tissue from the absorp-tion of all of the power W in the beam is
(3)
Notice that Equations 2 and 3 are related by thevolume within which the acoustic power isabsorbed; multiplying a result obtained withEquation 2 by the volume of absorption yieldsthe result given by Equation 3.
Human PerceptionRadiation force has been perceived by humansubjects in a number of instances at differentthresholds. Some of these results are describedhere. For example, with a 1-cm2 transducer cou-pled to the fleshy part of the forearm (avoidingbone in the path), subjects were able to perceive10- to 100-millisecond pulses of 2-MHz ultra-sound in which the power was greater thanapproximately 20 W, or a total radiation force ofabout 13 mN.2 In those experiments, the radia-tion force was distributed over several centime-ters of the sound path.
The fingertips are inherently more sensitive totactile perception than the tissues of the forearm.In addition, anatomic and physical conditionsincrease the radiation forces at the fingertip overthose in the fleshy part of the forearm. Bone has amuch higher absorption coefficient than soft tis-sue, and, in addition, the acoustic impedance ofthe bone is about 3 times that of soft tissue, lead-ing to reflection of a significant fraction of theincoming acoustic wave. The force required toreverse the direction of the wave is twice thatneeded to completely absorb it. Experiments wereperformed in which perfect reflectors of the ultra-sonic wave were fixed to the fingertips of subjects.The material transmitted the radiation forceexerted on it to the finger but reversed the direc-tion of the wave. The highly localized force was
(4)
The results of these studies probably give us thelower limits of the force required for human tac-
c
WF
2R = .
c
WF =r
.
J Ultrasound Med 2008; 27:565–592 567
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

tile perception of acoustic radiation force.Subjects were able to detect 2.2-MHz ultrasoundadministered in a single burst of 10 to 100 mil-liseconds above a threshold force of 3 mN oradministered repetitively in 2.5-millisecondbursts at a repetition frequency of 200 Hz above athreshold radiation force of 0.5 mN (W = 0.4 W,equivalent to ≈0.7 W in the case of completeabsorption).
The temporal characteristics of tactile percep-tion are similar to neural responses to electricalstimuli. For steady-state fields, there is a broadmaximum in tactile sensitivity at about 200 Hz,and for single pulses, thresholds are inverselyrelated to pulse length Δt up to about 1 millisec-ond and relatively independent of pulse length forlonger pulses.2 Thus, the threshold for tactile per-ception is a constant radiation impulse (FR Δt) ≈ 3µN/s for Δt < 1 millisecond and a constant radia-tion force (FR ≈ 3.0 mN) for Δt > 1 millisecond.
Lithotripter patients have no difficulty sensingindividual pulses during their treatments; thissensation is likely the result of radiation forcesgenerated in the body by the lithotripter pulse.However, in almost all diagnostic procedures,subjects are unable to perceive the acoustic radi-ation. Tactile perception presumably arises frommembrane potential changes in specializedperipheral neural receptors. There is no basis forbelieving that radiation forces, even if perceived,are of more concern clinically than any othermild tactile stimulus.
Auditory receptors are the mammalian organ-ism’s most sensitive mechanical detectors.Higher frequencies and shorter pulses can bedetected by the ear than by the finger. There are anumber of reports of the detection of pulsed orsinusoidally modulated megahertz ultrasoundby the human ear. As an example, Tsirulnikov etal3 showed that the threshold ultrasound levelvaried with frequency of modulation in much thesame way that the ear responds to audible air-borne sound, with a broad minimum (maximumsensitivity) of about 1 W/cm2 in the range from200 to 4000 Hz. If the ultrasound in this experi-ment were completely absorbed in the outer ear,a radiation pressure (radiation force per unitarea) on the order of 7 Pa would be generatedthere. Because this is very much greater than thethreshold for hearing of airborne sound (2 ⋅ 10–5
Pa), it is reasonable to assume that the ear inthese experiments was detecting the transmittedaudio frequency radiation force generated by theultrasound, and only a small fraction of the ultra-sound energy was absorbed or back-reflected.
Although it is an interesting example of a bio-logical effect of acoustic radiation force, theabove experiment has little relevance to diagnos-tic ultrasound. Amplitude-modulated CW ultra-sound and temporal-average intensities as highas 1 W/cm2 are rare in diagnosis. There have,however, been reports of auditory sensation dur-ing clinical examinations.4 Patients exposedthrough the foramen magnum at the base of theskull with 2-MHz pulsed ultrasound at temporal-average intensities up to 0.5 W/cm2 heard tonesthat varied in frequency with the pulse repetitionrate and in loudness with the intensity of theultrasound exposure. These observations areconsistent with a radiation force mechanism bywhich the momentum of an ultrasound fieldgenerates low-frequency impulses in the biologi-cal medium. The same mechanism has beencredited with increased fetal movements duringultrasound examination.5–7
BioeffectsBoth tactile and auditory receptors have theirmaximum sensitivities in the audible frequencyrange. Thresholds for detection depend stronglyon the temporal characteristics of the modula-tion of the ultrasound. Bone health requires therepetitive stresses that occur in exercise and dailyactivity. Numerous studies have shown thatultrasound applied with a pulse repetition fre-quency (PRF) of 100 to 1000 Hz and a duty fac-tor of approximately 0.2 accelerates bonefracture healing.8,9 For example, a 1.5-MHz 200-microsecond tone burst repeating at 1 kHz(pulse-average intensity = 150 mW/cm2) acceler-ated the appearance of the fracture callus inhumans,10 and similar exposure conditionsstimulated proteoglycan synthesis in vitro.11
Ultrasound-stimulated synthesis of cell matrixproteoglycan, which is associated with accelerat-ed fracture healing, appears to be mediated byintracellular calcium signaling.12 The pulsed 1.5-MHz signal produces radiation force vibrationsat 1 kHz, and it has been found that a squarewave 1-kHz signal is similar to the pulsed 1.5-
568 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

MHz signal in inducing chondrogenesis in an invitro model.13 Parvizi et al11 quantified the area ofcartilage nodules formed by the chondrocytes,providing a measure of chondrogenesis, andshowed that the pulsed 1.5-MHz waves (PRF = 1kHz) increased the area of nodules more than 3-fold compared with control chondrocytes.Continuous wave ultrasound does not appear tobe effective for bone healing, while shock wavedevices designed similarly to lithotripters, alsohave been shown to accelerate bone growth andhealing.14,15 Because the average intensity foreither pulsed ultrasound or shock wave devicesis usually much less than is typical for physicaltherapy, and the temperature rise is unlikely toexceed 1.5°C, the mechanism appears to be non-thermal.16 Radiation force appears likely to bethe cause of the effect, although further evalua-tion is needed to establish force as the mecha-nism directly responsible for bone healing.
There is also evidence of the detection of veryintense, unmodulated acoustic fields in the brainat frequencies much higher than the traditional-ly defined upper limits of hearing. Divers canhear sounds up to 130 kHz (E. Cudahy, PhD,written and oral communications, 2005). Theperception of the sound as reported by divers isthat of a very high pitch, but the apparent fre-quency changes little above 16 kHz.
Radiation forces induced by ultrasound pulsestimed to coincide with the moment of contrac-tion of the frog heart have been shown to reducethe strength of contraction.17,18 The effectrequired a minimum pulse duration of 5 mil-liseconds, which is orders of magnitude longerthan typical diagnostic pulses. Therefore, there isno reason to assume that the effect will occur inthe human heart under diagnostic conditions.
Radiation forces from short pulses of high-fre-quency, high-intensity focused ultrasound havebeen shown to move detached retinas and causeblanching (reduction of blood flow) of theregion.19,20 The conditions of exposure approachthose that produce irreversible lesions in theeye.21
Radiation forces within standing wave fields,where there is no large-scale transport ofmomentum, are somewhat more complex thanthose described above for traveling waves.22,23
Particles much smaller than the acoustic wave-
length that are denser than the suspending fluidare forced to pressure minima in such a field.Using a specially designed exposure chamber,Dyson et al24 showed that this mechanismcaused banding and stasis of blood cells in chickembryos. This phenomenon is unlikely to havesignificance in typical diagnostic examinationsfor at least 3 reasons related to the physicalaspects of exposure. First, for standing waves toform, there must be a reasonably well-definedspecular reflector. Bone and possibly somelocations on the surface of the lung satisfy thatrequirement to some degree. Second, the stand-ing wave, such as it is, would be confined to theregion of overlap of the incoming and reflectedpulses, effectively somewhat less than half of thelength of the pulse. For the longest pulses used indiagnosis, this would be less than 5 mm. Third,with typical scanning procedures, the beamwould not remain stationary long enough forstasis to occur.
Sustained radiation forces on liquids may resultin macroscopic streaming.25 Investigators havetaken advantage of this phenomenon to differ-entiate between fluid-filled cysts and solidlesions.26–28 Investigators have also used radia-tion force directly in imaging. In this technique,known as acoustic radiation force impulse imag-ing, tissue is “pushed” from its equilibrium posi-tion with a long acoustic pulse. After the pulse,the tissue slowly moves, or “relaxes” back to itsoriginal position. The relaxation movement isdetected by shorter probing pulses, and infor-mation on the elastic properties of the tissue isobtained.29,30
ImplicationsAcoustic radiation forces, which arise whenacoustic waves are absorbed or reflected, canunder certain circumstances be detected. Ineach case, there is a threshold that depends onacoustic pressure, PRF, and pulse duration.However, in normal diagnostic procedures, themagnitudes of the radiation forces are small, andtheir effects, if any, do not impact negatively onthe medical use of ultrasound. One possibleexception to this general conclusion concernsthe interaction of diagnostic ultrasound with thelarge gas bodies present in the lung and intes-tine. This is discussed in detail below.
J Ultrasound Med 2008; 27:565–592 569
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

First-Order Acoustic Phenomena
In contrast with second-order radiation forces,the first-order forces that are used routinely indiagnostic procedures are very large. The 2- to3-MPa pressures that are common in imagingand Doppler ultrasound are greater by 1011
than the threshold for hearing of airbornesound and greater than the threshold for painfor airborne sound by 105. The acoustic pres-sures used in lithotripsy are greater than diag-nostic levels by an order of magnitude ormore.31 Instantaneous first-order body forces,the forces that cause the elements of the tissueto oscillate back and forth along the directionof propagation, are directly proportional to theacoustic pressure and the frequency of theultrasound. For 1 MPa at 1 MHz, these forcesare greater than the forces of gravity on thesame material by 4 · 105.
However, most tissues in the body areexposed routinely to diagnostic ultrasoundwith no apparent adverse biological effects. Itis not the forces per se, of course, but theirphysical effect on the tissue that leads tobiological effects. Ultrasound propagating ina medium, such as tissue, causes the con-stituent molecules to move closer together andfarther apart. These displacements are oscilla-tory and tiny (≈0.1 µm for a 1-MHz pulse at 1MPa); they produce no lasting effect. For high-intensity ultrasound or lithotripter pulses, thedisplacements are greater, 1 to 100 µm, and theaccelerations producing them are very large.These displacements and accelerations, incombination with internal heterogeneity in thecellular structure, have been used to explainthe disruption of cells observed after exposureto high-amplitude pulses.32,33 Inhomogeneities,in particular gaseous inclusions, can amplifyand distort the particle motion. Almost everyadverse biological effect of diagnostically rele-vant ultrasound that has been identified hasbeen associated with some form of includedgas. Before proceeding further with an explo-ration of mechanically produced biologicaleffects, it will be useful to provide some infor-mation about how bubbles respond to acousticfields.
Response of Bubbles to Acoustic Fields
TheoryThere is a large body of theoretical analysis andexperimental data on the interactions of individ-ual gas-filled microbubbles with acoustic fields.These may be present naturally in the body (eg,in the lung or intestine); they may be producedby the passage of an acoustic wave of sufficientintensity (eg, in the kidney during shock wavelithotripsy, either from preexisting cavitationnuclei or spontaneous nucleation in regions oflow interfacial tension); or they may be producedby an external process and subsequently may beintroduced into the body (eg, by intravenousinjection of ultrasound contrast agents).34 In thiswork, the term gas body is sometimes used torepresent any physically contiguous collection ofgas molecules without restriction on size orshape and which may be acted on by the acous-tic field. Thus, both the lung as a whole and theindividual microbubbles constituting an ultra-sound contrast agent, as well as anything inbetween, are considered gas bodies. To differen-tiate between the general term gas body and thespecific term gas bubble, we simply require thatthe latter be completely surrounded by eitherfluid or tissue or both and that it be small in com-parison to the acoustic wavelength.
A bubble in a sound field is acted on byacoustic stress at its surface. Because a bubbleis composed of highly compressible gas, thistime-varying acoustic pressure produces rela-tively large oscillations in the bubble volume. Atlow pressures, the motion of a bubble havingequilibrium radius R0 and suspended in a liquidof density ρ0 is well described by the equation fora damped linear harmonic oscillator:
(5)
where x = R(t) – R0; m is the effective mass (= 4πR0
3ρ0); b is proportional to the damping; ks isthe stiffness (equivalent to a spring constant in aspring bob oscillator); pA is the acoustic pressureamplitude; and ω is the angular frequency (= 2πf). Equation 5 is an expression of Newton’sfirst law: F = ma. The three terms on the left sideof Equation 5 represent the effective mass timesthe net acceleration, the damping force (caused
t ,pRxkxm ωcos�4 A20s −=++ xb
570 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

by several mechanisms), and the outward forceexerted by the gas within the bubble, respective-ly, while the term on the right side gives the forceexerted on the bubble by the surrounding liquid.A solution to Equation 5 is
(6)
where x0 is the amplitude of the radial displace-ment, and β is the phase angle between the driv-ing pressure wave and the displacement. Thesehave the following forms:
(7)
and
(8)
where ω02 = ks/m, and f0 = ω0/2π is the resonance
frequency. Bubbles exhibiting the largest radialresponse for low driving pressures at a particularacoustic frequency (eg, in blood), bubbles ofapproximately 3.9 µm in diameter at 2 MHz, aresaid to be of resonance size. The spherical bub-ble motion is damped (ie, loses energy) becauseof 3 primary mechanisms: viscous damping aris-ing from the viscosity of the liquid that is forcedinto motion by the pulsating bubble, radiationdamping from the acoustic wave emitted by thepulsating bubble itself, and thermal dampingarising from a net transfer of heat out of the bub-ble and into the liquid. More thorough treat-ments of this problem are widely available.1,35–37
For small pressures where Equation 5 is appli-cable, a bubble is said to oscillate “linearly,” anda plot of the radius versus time will be a simplesinusoid centered about the bubble’s equilibri-um radius R0. On the other hand, exposure to asufficiently high acoustic pressure will inducehigher-amplitude, nonlinear oscillations in thebubble volume. These two situations are illus-trated in Figure 1 for a 4-µm-diameter sphericalbubble exposed to 2-MHz acoustic waves havingpressure amplitudes of either 0.01 or 0.5 MPa.While the response to the lower pressure is sinu-soidal as expected, the response to the higherpressure is characterized by high-amplitude,long-duration (ie, greater than half of an acoustic
period) excursions above the equilibrium radiusseparated by relatively brief intervals below it. Asthe bubble contracts from a radial maximum tothe subsequent minimum, the motion of the sur-rounding fluid may attain such a large momen-tum that the rising pressure within the bubble,which easily counteracts this momentum at lowacoustic intensities and thus produces a bal-anced (sinusoidal) oscillation, cannot withstandthe inrushing liquid. The bubble’s radius veryrapidly becomes extremely small; that is, the bub-ble “collapses.” This is termed an inertial collapsebecause the motion is dominated by the inertia ofthe liquid. This concept is used to differentiatetwo classes of cavitation fields: noninertial cavi-tation when bubble motion does not involveinertial collapse and inertial cavitation wheninertial collapse does occur. As might be expect-ed, the mathematical description of bubble activ-ity at higher pressure amplitudes is much morecomplicated, but again several authors havetreated the problem,38–41 while Prosperetti andLezzi42 have shown that these formulations areessentially equivalent.
Cavitation ThresholdsTheoretical results from this research indicatethat there is often a rapid increase in radialresponse with only a very modest increase in theamplitude of the acoustic field; the effect is par-
( )⎥⎦⎤
⎢⎣
⎡
−=
20
2 ωωarctanβ
mωb ,
( ) 222222000
A0
ωωωρ mbR
px
+−=
( )βωcos0 += txx ,
J Ultrasound Med 2008; 27:565–592 571
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d
Figure 1. Predicted radial responses for a bubble having a diam-eter of 4 µm and exposed to a 5-microsecond pulse of 2-MHzultrasound having an acoustic pressure of 0.01 MPa (thick line)or 0.5 MPa (thin line). The former illustrates a harmonic linearresponse, while the latter exhibits strong nonlinearity and sever-al inertial collapses.

ticularly strong for small bubbles (ie, those belowthe linear resonance size).43 The acoustic pressureat which this rapid increase in response occurs isloosely termed the cavitation threshold or, moreprecisely, the threshold for inertial cavitation.44
Theoretical results indicate that inertial cavitationshould be produced quite readily by diagnosticexposures of pure liquids given the presence ofappropriate cavitation nuclei.45–48 The cavitationthreshold is approximately 0.2 MPa at 1 MHz for a1-cycle pulse, decreasing to as little as 0.12 MPa asthe pulse length increases.49 However, it is clearthat pure liquids are rare in the human body.Body tissues are viscoelastic solids, and recentmodeling indicates that the cavitation thresholdsfor soft tissues will be higher, and sometimesmuch higher, than those for liquids even whenoptimally sized nuclei are present50; the differ-ence in response is primarily due to the rigidity ofthe tissue that constrains the bubble motion. Thetheoretical result is consistent with animal studiesof shock wave lithotripsy in which cavitation isobserved first in the collecting system of the kid-ney,51 and tissue injury is seen in vessels andtubules within the tissue.52 In addition, there is lit-tle evidence for the presence in vivo of cavitationnuclei that may be excited by diagnostic ultra-sound, although cavitation can be detectedimmediately in the urine in pig kidneys duringshock wave lithotripsy.51,53,54 In the absence ofpreexisting nuclei, the minimum cavitationthreshold for microsecond-long pulses of 1-MHzultrasound is at least 4.0 MPa, a value obtained bycombining observations of cavitation during clin-ical lithotripsy procedures with theoretical analy-ses of spontaneous nucleation and bubbledynamics in liquids.55 The fact that the experi-mental threshold for tissue damage in a variety oflaboratory animal models exposed to millisec-ond-long pulses of megahertz-frequency ultra-sound is more than an order of magnitude greaterthan the threshold in water is taken as evidencethat preexisting, gas-filled nuclei are not usuallypresent in vivo (see “In Vivo Effects, Soft Tissue:Gas Free” below for a review of this literature).
Potential Mechanisms for Biological EffectsThe mechanisms by which a bubble may affectnearby biological material are dependent on themagnitude of the bubble’s response to the acous-
tic field. Essentially all bubbles produce acousticradiation forces and microstreaming, while onlythe more strongly affected will exhibit the violentresponses (eg, shock wave generation or free rad-ical production) characteristic of inertial cavita-tion. Descriptions of these effects follow.
Radiation ForcesIn the same way that absorption of an acousticwave by tissue causes a decrease in the forwardmomentum of the wave, which is recognized asan “effective force” on the tissue called the radia-tion force (see Equation 1), so too does a bubbleabsorb an acoustic wave and thereby decrease itsforward momentum. This effect is also perceivedas an effective force, a radiation force on the bub-ble. The method for calculating this force is simi-lar to the method for tissue. Equivalent to theabsorption coefficient for tissue is the extinctioncross section σe, which quantifies the ability of abubble to remove energy from a wave (ie, todecrease the wave’s momentum). Multiplying σe
by the incident intensity I gives the rate at whichenergy is removed from the wave, equivalent tothe numerator in Equation 1, 2αI, which is therate at which a unit volume of tissue removesenergy from the wave. Dividing by the speed ofsound c gives the radiation force σeI/c for a bub-ble and 2αI/c for a unit volume of tissue. For low-amplitude acoustic fields, a simple analyticalexpression for σe may be obtained from Equation4. This expression shows that near resonance, theextinction cross section of a bubble is manytimes greater than its physical cross section andthus that the force is much greater than might beimagined. For higher-amplitude pulsations, theextinction cross section and thus the force mustbe computed numerically.
It is found that radiation force can cause a bub-ble to move at high speed (≈10 m/s) in a cell sus-pension exposed to ultrasound under typical invitro experimental conditions. Cells near thepath of a speeding bubble may be damaged byexposure to high shear stresses as it passes.56
There are many predictable phenomena forbubbles and the materials around bubbles. Apulsating bubble itself acts as a source of acous-tic waves, reradiating, or scattering, a part of theacoustic energy that it absorbs. If a second bub-ble happens to be near the first, this scattered
572 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

wave will exert a force on the second bubble; the“second” bubble also exerts a force on the first. Ifthe two bubbles are both smaller or larger thanthe resonance size, the net force will be attrac-tive, and the bubbles will move toward oneanother. This force is responsible for one of thepossible mechanisms whereby bubbles in asound field may grow because if the two bubblestouch, they may coalesce into a single largerbubble. If one of the bubbles is larger than theresonance size and the other is smaller, thesmaller will be attracted to the larger when thetwo are closer together than about 0.8 times theradius of the larger bubble, but it will be repelledfor larger separations.57
The acoustic wave scattered by a bubble mayalso affect small particles (eg, biological cells)that happen to be near the bubble. For particlesdenser than the suspending medium, whichincludes most cases of biological interest, thedirection of the force is toward the bubble, whilethe magnitude of the force decreases as the fifthpower of the distance from the center of the bub-ble.57 Oscillating bubbles will tend to attractnearby particles or cells, thus collecting theminto small, highly concentrated groups wherethey may be more easily damaged or destroyedby the pulsating bubble. However, the oscillationof a bubble may be reduced by material accu-mulating on its surface, thereby reducing theextent of any damage that may occur.58–60
MicrostreamingBubbles oscillating in a sound field, especially ifthey are located on a solid surface, produce a vig-orous small-scale circulatory motion in the sur-rounding fluid.61–64 Such fluid motion is calledmicrostreaming. Oscillating bubbles that arebeing pushed by a traveling wave also may pro-duce shearing flow in the surrounding fluid,although this motion is noncirculatory. In allcases, because the velocity of the fluid flowingaround the bubble is greatest near the bubblesurface, and because the fluid velocity decreasesas the distance from the bubble increases, a gra-dient exists in the fluid flow field around the bub-ble. When a cell is carried by the streaming flowinto a region of strong fluid velocity gradients,the fluid will exert greater force on the side of thecell near the bubble and less force on the side
farther away. This unequal distribution of forceson the exterior of the cell results in shearingstresses (or forces) that tend to distort and tearthe cellular membrane. Because cells have vis-coelasticity, some minimum time is required fora given level of shear stress to disrupt a mem-brane; typical minimum times for hemolysis are1300 microseconds at 0.45 kPa and 25 microsec-onds at 0.1 MPa.62
Shock WavesDuring an inertial collapse, the speed of the gas-liquid interface may be very high, in some casesbecoming supersonic in both the gas (>330 m/s)and the liquid (>1500 m/s). Such supersonicmotion can produce shock waves both withinthe bubble and in the surrounding fluid. Theexternal shock will propagate outwardly as aspherically diverging wave. A biological cell ortissue exposed to the shock will briefly experi-ence very large stresses and spatially varyingbody forces. For a shock wave generated by alithotripter, the shock thickness measured invivo was 150 nm,65 and shock waves generatednear a bubble collapse may be even thinner.Hence, a pressure difference on the order of 10MPa can exist inside a cell, thereby subjectingthe cellular contents at the shock front to a bodyforce of greater than 7 · 1013 N/m3. Because theindividual components of the cell have differentdensities, they may be displaced to differentdegrees by this body force. Forces of this magni-tude can break the cell whether the shock is gen-erated by a bubble collapse or the acousticsource itself. Lokhandwalla and Sturtevant66 pro-posed a mechanism for tissue damage by alithotripter shock wave in which the very narrowshock front was superfocused by inhomo-geneities in tissue (termed wave front folding inthe case of sonic booms propagating in a turbu-lent atmosphere). The focusing creates pressuregradients and shear within cells, tissues, andblood vessels. The authors then expanded thisidea to show that the shock wave source mightbe a cavitation bubble67 and therefore that theeffect might also occur during diagnostic exami-nations. Overpressure experiments in cell sus-pensions confirm a minimal level of lysisattributed to shear when thermal and cavitationeffects are suppressed.68 As with microstream-
J Ultrasound Med 2008; 27:565–592 573
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

ing, creation of a significant pressure gradientacross the cell causes distension of the cell, andat some threshold level, the gradient is strongenough, and the distension great enough, to tearthe cell. In addition, inhomogeneities in the tis-sue (eg, structural fibers or blood vessels) mayfurther concentrate these stresses and thusamplify the effect.
Free RadicalsWhen a bubble undergoes inertial collapse, thereis a brief time (on the order of nanoseconds induration) near the radial minimum during whichthe pressure within the bubble may rise to hun-dreds or thousands of megapascals, and the tem-perature may reach thousands of kelvins. Inaddition to various gases, such as nitrogen, oxy-gen, and argon, and various fluorocarbons in thecase of ultrasound contrast agents,34 the interiorof a bubble contains water vapor. The existenceof high temperatures in such an aqueous medi-um may lead to the formation of chemically reac-tive free radicals, such as •H and •OH, by thedissociation of water.69–71 Although these freeradicals would be very damaging to any biologi-cal tissue they should encounter, they tend tohave extremely short lifetimes in vivo (≈10–9 sec-ond, equivalent to a mean free path of ≈0.5 µm).However, hydrogen peroxide, which may be pro-duced by recombination of the appropriate freeradicals, is another product of cavitation. Thismolecule is long lived and has been shown toinduce single-strand breaks in DNA in vitro.56
One may speculate that any of these chemicalspecies produced by the action of the soundwave (ie, any of these “sonochemicals,” as well asmany of the others produced by inertial cavita-tion) may injure biological cells or tissues in thevicinity of a collapsing bubble, particularly if thebubble collapses inside the cell. This damagemay result from the direct effect of a sonochemi-cal on a biological molecule such as DNA, thusresulting in a potential genetic effect, or theaction may be indirect, involving the productionof potentially toxic secondary chemicals (eg, rad-ical adducts).72 However, intensive investigationsin vitro have shown that it is very difficult toinduce genetic mutations in intact cells even forexposure levels far above those permitted indiagnostic ultrasound examinations.73,74
MicrojetsMost theoretical analyses of bubble-mediatedultrasound bioeffects assume that the bubbleremains spherically symmetrical throughout itsmotion. While this assumption is valuable in thatit allows detailed investigations of variousaspects of cavitational activity, bubbles in the rel-atively strong acoustic fields common tobiomedical ultrasound probably do not remaincompletely spherical. The threshold for the gen-eration of surface waves on the bubbles is muchbelow the intensity of typical biomedical expo-sures,57 and the amplitude of the waves increaseswith the acoustic driving pressure. At high ampli-tudes, surface waves become distorted. Bubblesmay be pierced by liquid jets, ruptured into manydaughter bubbles, or both. The generation ofdaughter bubbles is important because they mayact as nuclei, or “seeds,” from which additionalbiologically damaging cavitation bubbles maydevelop. Small liquid jets, called microjets, mayalso produce significant biological effects.
When a bubble located on or near a solidboundary is exposed to an acoustic wave, itexpands and contracts in response to the time-varying pressure, as would any other bubble. Inthis case, however, while the fluid opposite theboundary is free to flow toward the bubble’s cen-ter, the solid surface restricts the motion of fluidon that side of the bubble. This asymmetry dis-torts the bubble interface in such a way that aninvagination of fluid forms on the side of thebubble opposite the boundary. As the acousticpressure is increased, this distortion is magnifieduntil the liquid flows completely through thebubble and impacts the solid boundary. Suchevents are known to be very violent, being able topit brass plates and pierce aluminum foils.75
Although the relevance of microjet activity toultrasound bioeffects research remains to bedetermined, Kodama and Takayama76 haveshown that microjets will be directed towardnearby compliant surfaces such as vascularepithelia, and considerable tissue damage mayresult.
StrainSeparate from studies showing tissue damagefrom the fluid jet impact of a collapsing bubble,there are several in vitro experiments that have
574 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

measured strain and rupture of tissue or tissuephantoms induced by bubble oscillation. Theoscillations of a bubble within a fluid that is incontact with a tissue surface strain that tissue.Using a polariscopic technique, Delacretaz etal77 measured relative strain induced in apolyacrylamide tissue phantom by an oscil-lating bubble. The highest tensions, displace-ments, and macroscopic damage to the gelwere observed as the bubble collapsed, draw-ing fluid inward and pulling on the tissue.Compression was seen as the bubble expanded.Lokhandwalla and Sturtevant67 and Gracewskiet al78 calculated the elongational and shearstrain induced in a red blood cell by the asym-metric fluid flow field induced by oscillationand shock wave emission of a cavitation bub-ble. Experiments showed that such spatialpressure gradients produced hemolysis,68 sup-porting earlier results from Rooney,61–63 who hadused flow generated by an oscillating bubble tomeasure shear injury to blood cells. In fact, itappears that little fluid between the bubble andthe tissue is necessary to strain or rupture the tis-sue. Zhong et al79 filmed the expansion of acous-tically excited microbubbles and the subsequentdistension of a plastic tube surrounding them.Their design of a lithotripter pulse intended tominimize bubble expansion resulted in fewerruptured vessels in animal studies. Carstensen etal80,81 had earlier proposed that a similar mecha-nism, the ultrasonically induced expansion of apreexisting gas body, could produce the tissueinjury observed in Drosophila larvae. While itmay be difficult to conceive that a nearly emptybubble can push on tissue strongly enough todamage it, the concentration of applied stressnear a void and the resulting strain in the sur-rounding material are generally accepted to behow fractures grow in brittle materials82,83; a sim-ilar mechanism has been proposed for tissue.66
Therefore, the asymmetry of fluid flow or hydro-dynamic pressure created by oscillating bubbleswill certainly stress, and may then shear, biologi-cal tissue.
In Vivo EffectsThere is considerable evidence relating the pres-ence of microbubbles to a variety of biologicaleffects of ultrasound, in many cases under diag-
nostically relevant exposure conditions. However,much of this work was performed in vitro, and itsrelevance to diagnostic exposures of adulthumans is not clear because large numbers ofgaseous microbubbles are not known to be pre-sent under normal conditions. An importantexception occurs with the use of ultrasound con-trast agents, a subject discussed in some detail byMiller et al.34 The relationship between exposuresto diagnostic ultrasound and acoustic cavitationis treated below insofar as it relates to the healthyadult.
BloodIt appears that in normal mammalian tissue andblood, micrometer-sized bubbles are extremelyrare. Cavitation is seen readily and immediatelyin the urine of the kidney collecting system dur-ing shock wave lithotripsy, but it is only detect-ed much later in tissue, after hundreds of shockwaves. If this were not true, certain high-inten-sity diagnostic procedures probably would haveproduced noticeable tissue damage. Blood, inparticular, seems to be largely free of small bub-bles. It is, of course, the body’s transport medi-um for gases, but it appears that most if not allof those gases are dissolved or chemicallybound. Using a resonant-bubble detector locat-ed on the abdominal aortas of dogs, Gross etal84 were unable to detect cavitation bubbles inheart or aortic blood exposed to 0.5- to 1.6-MHz, CW ultrasound up to 16 W/cm2 (0.7 MPa).Using a similar detector, Gross et al84 were alsounsuccessful in attempts to identify cavitationfrom left ventricular blood in dogs exposed to0.75- and 1.45-MHz ultrasound up to 1 kW/cm2
(5.5 MPa). Ivey et al85 recorded images of bubbleboluses produced by a 15-millisecond pulse of1.8-MHz ultrasound at 19 kW/cm2 (23 MPa).Recently, Hwang et al,86 using a passive cavita-tion detector operating at 5 MHz, detected anincrease in the inertial cavitation rate in theauricular veins of rabbits exposed to 500-cycle,1-kHz-PRF pulses of 1.17-MHz ultrasound at ararefactional acoustic pressure pr of 6.5 MPa butno increase at a pr of 3.0 MPa; the threshold wasa pr of less than 1.0 MPa in the presence of themicrobubble contrast agent Optison (GEHealthcare, Princeton, NJ).
J Ultrasound Med 2008; 27:565–592 575
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

Soft Tissue: Gas FreeHigh-intensity focused ultrasound can be usedto necrotize tissue and form thermally coagulat-ed lesions by conversion to heat of absorbedultrasound energy. Short bursts of focused ultra-sound produce negligible heating but can createlesions due to bubble nucleation and subse-quent cavitation. Lesions induced in soft tissuesby heating are characterized by smooth bound-aries, while those produced by cavitation usuallyare irregular. Fry et al87 and Dunn and Fry88
induced cavitation in cat brains with 1-MHz CWexposures of a few milliseconds’ duration at 2kW/cm2 (8 MPa). A sharp, audible “snap” corre-lated with the appearance of irregular lesions,consistent with a cavitational mechanism, andthe lesions did not necessarily appear at thefocus but rather at the interfaces between neuraltissue and fluid-filled spaces such as ventriclesand blood vessels. Frizzell89 reported similarresults for CW exposure of cat livers at 3 MHz,with a threshold intensity for cavitation involve-ment that was less than 2 kW/cm2 (7.7 MPa cal-culated assuming linear propagation, whichoverestimates the rarefactional pressure) for 30-millilsecond pulses. Taylor and Pond90 found dis-ruption of the normal cellular architecturearound the central vein of rat livers after 5-minute exposures to 10-millisecond pulses of1.3-MPa ultrasound at 0.5, 1.0, and 2.0 MHz. Thenumber of lesions decreased with increasing fre-quency, and none were observed at 6.0 MHz; thisfrequency response is indicative of cavitationalactivity. Lee and Frizzell91 reported the thresholdlevel for cavitational involvement in hind limbparalysis of the mouse neonate due to CW expo-sure of the spinal cord to be approximately 1.5MPa at 1 MHz for exposure durations of about 1second at 37°C. However, Frizzell et al92 laterused the same animal model to examine thresh-olds with pulsed ultrasound. Using 1-MHzpulsed ultrasound with a 10-microsecond pulseduration and a 2.4-second exposure duration at10°C, they found that the threshold peak rarefac-tional pressure for cavitational involvement inthe paralysis was greater than 5.1 MPa for a 5-kHz PRF. The threshold decreased as the PRF wasincreased, suggesting that the threshold wouldbe even higher if the PRF were reduced to 1 kHz,more typical of diagnostic ultrasound. In general,
the studies using pulsed exposures are moreindicative of what would be expected from diag-nostic ultrasound because heating associatedwith CW exposures can increase the likelihood ofcavitation by increasing the prevalence of nuclei.
In experimental hyperthermia procedures indog muscle, Hynynen93 noted the sudden onsetof subharmonic emissions (a common indicatorof cavitation) from the focal region and a simul-taneous marked increase in scattering, attenua-tion, and the rate of heating for 1-secondexposures. Thresholds were approximately 300W/cm2 (3 MPa) at 0.5 MHz and 800 W/cm2 (5MPa) at 1 MHz. In addition, a kind of hysteresiswas observed, with higher thresholds beingobserved when the acoustic pressure wasincreasing and lower thresholds when it wasdecreasing from levels above the initial thresh-old. Tissue emulsification has been observedwith pulsing schemes involving a repeatedsequence of one high-amplitude “primary” pulsefollowed at the mid period by one lower-ampli-tude “cavitation-sustaining” pulse.94 Porcinemyocardium exposed to 5 × 104 17-microsecond-long pulses of 750-kHz ultrasound at a PRF of0.33 kHz with primary and cavitation-sustainingamplitudes of 17 and 4.5 MPa, respectively, waseroded completely away by inertial cavitationbut formed solid, apparently thermal lesions forcavitation-sustaining pulse amplitudes above 9.0MPa.95 Cavitation has also been detected in thekidney parenchyma of pigs during lithotripsy butonly after many shock waves.51 Perhaps not coin-cidently, vascular injury to pigs in the DornierHM3 lithotripter (Dornier MedTech, Kennesaw,GA) has only been sufficient to quantify aftermany shock waves.52
While it requires rather substantial acousticpressures to damage biological tissues, simplebubble growth apparently may be induced invivo at much lower levels. ter Haar and Daniels96
and ter Haar et al97 reported that exposing thehind legs of guinea pigs to 0.75-MHz CW ultra-sound caused the appearance of new echoes onan 8-MHz pulse echo imager capable of detect-ing bubbles of 10 µm or more in diameter. Thethreshold was 80 mW/cm2 (0.05 MPa), and thenumber of bubbles detected increased withintensity up to 680 mW/cm2 (0.14 MPa). Thedetection of new echoes (ie, microbubbles) was
576 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

suppressed by the application of hydrostaticpressure, a classic test for cavitational activity.The same authors also reported that the thresh-old for pulsed ultrasound (2-millisecond pulsesand 50% duty cycle) was approximately 240mW/cm2 (0.08 MPa). Although these studies didnot involve tests for biological effects, they areimportant because they provide evidence for theexistence of cavitation nuclei in tissues.
Soft Tissue: Gas ContainingIn contrast to the tissues discussed above, somebody structures contain copious amounts ofundissolved gas. For example, the lung is largelygas. Rather than being the micrometer-sizedspherical bubbles in an infinite fluid medium asidealized in the theory above, most of the gas inthe lung is contained in comparatively large alve-oli, surrounded by other gas-filled alveoli andtherefore not in an environment favorable toinertial cavitation. Bacterial action within thecontents of the intestine produces bubbles witha nearly continuous distribution of sizes. Someof these bubbles are near the walls of the lumenand in an environment that can support inertialcavitation. That nuclei exist in other parts of thebody is attested by the physics of decompressionillness.98,99 However, the concentration and dis-tribution of gaseous micronuclei in the bodyremain somewhat a mystery. Because these tis-sues may be more easily affected by diagnosticexposures than apparently gas-free tissues, theywill be treated more extensively.
Lung Hemorrhage
In the normal healthy subject (absent exogenouscontrast agents), there is little basis for concernabout mechanically induced biological effects ofultrasound in most diagnostic procedures. Theorgan most vulnerable, however, is the lung. Thiswas shown in the initial studies of biologicaleffects on the lung of the mouse.100 As a result ofthe low threshold for hemorrhage in the lung anda desire to determine the responsible mecha-nism, the lung has become one of the most exam-ined organs for biological effects studies. Studieshave been conducted by several different labora-tories using a variety of experimental animalsranging in size from newborn mice to 60-kg pigs.
Studies included monkeys,101 mice,18,100,102–106
rats,106–116 rabbits,105,117 and pigs.118–120
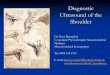
An example of lung hemorrhage is shown inFigure 2, and the penetration into the lung is shownin Figure 3.
Although thresholds for lung hemorrhageappear to be lower than exposure levels extant indiagnostic equipment used on humans, lesionsare small, do not appear to affect function,108 andare repaired by the body within a few weeks.109 Inthe large database of lung hemorrhage studies,there is no clear dependence of threshold on thespecies of the laboratory animal. Within the rangeof interest for most diagnostic examinations, nei-ther is there a clear dependence on frequency ofexposure. Although the superthreshold damageincreases with pulse duration and total exposuretime, the threshold itself is only weakly depen-dent on these parameters.
The body of literature providing thresholds forhemorrhage in lung from exposure to acousticwaves is huge, ranging from audible121 and low122
ultrasonic frequencies to several megahertz. Tosimplify analyses of these data for purposes ofthis document, the frequency range will berestricted to 1 MHz and above. The available datafor the threshold for lung hemorrhage at diag-nostically relevant frequencies are tabulated inTable 1. Even in this frequency range, the varia-tion in exposure parameters is very large. Thedata as a whole contain a range of pulse dura-tions, exposure durations, beamwidths, andPRFs. The threshold results show the followinggeneral trends. Thresholds decrease slightly butconsistently with pulse length and are indepen-
J Ultrasound Med 2008; 27:565–592 577
Church et al
Figure 2. Lateral view of rat lung exposed to pulsed ultrasoundunder superthreshold conditions. Note the circular area of sub-pleural hemorrhage that radiates centripetally from the center ofthe exposure beam (darker red area) to the periphery (lighter redarea). Scale bar indicates 5.5 mm.
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

dent of beamwidth (although the superthresh-old lesion size is dependent on beamwidth). Forall studies, however, once the acoustic pressureexceeds the threshold for lung hemorrhage, theextent of damage depends strongly on pressure.
Some additional insight on thresholds may begained by selecting a subset of the data in thediagnostic frequency range representing twoextremes of exposures that exist in the litera-ture. The first group (labeled A in Figure 4)includes exposures with pulse durations on theorder of 1 microsecond at a 1000-Hz PRF andexposure durations on the order of 10 seconds.The second group (labeled B in Figure 4)includes exposures with pulse durations on theorder of 10 microseconds at a 100-Hz PRF andexposure durations of 3 minutes. Thresholds forthese two sets of experiments are summarizedin Figure 4. Although the total on time (productof pulse duration, PRF, and exposure duration)for sound in group B is roughly 15 times greaterthan for group A, the thresholds for the twogroups differ by only a factor of approximately3. For example, at 3 MHz, the threshold for longexposures may be rounded to approximately 1MPa, while the threshold for short exposurescenters around 3 MPa. It is concluded that thethreshold for damage decreases as the exposureduration or the pulse length increases.
In contrast with thermal damage, hemorrhagecan occur with very short exposures and very lit-tle acoustic energy delivered to the tissue. Thedegree of superthreshold damage depends onacoustic pressure, total exposure time, andbeamwidth. The question of mechanisms is dis-cussed in greater detail below.
Of course, comparable investigations withhuman subjects have not been conducted. Onestudy involving patients that had been exposedto observations of the heart with ultrasound inpreparation for open heart surgery had negativefindings; of 50 subjects, none showed any evi-dence of lesions on the surface of the lung.123 Theupper limits of lung exposure in that study wereestimated to be approximately equal to thethreshold for hemorrhage in laboratory animals.From this, we may conclude that human lungsare not anomalously much more sensitive thanthose of laboratory animals.
Relating Output to ThresholdIf this information is to be useful, we first mustassess the probability that there will be a biologicaleffect, in this case, whether the acoustic pressureat the surface of the lung exceeds the threshold forlung hemorrhage. Then, the magnitude of anyadverse effect must be assessed. Combining theprobability of harm and the magnitude of thatharm provides a measure of the risk to the patientfrom the diagnostic exposure. If the probability isnonzero, the risks or possible risks to the patientmust be balanced against the benefits of theexamination. Evaluation of risk versus benefit islargely a qualitative process involving informedjudgment of the operator. We can, however, relatequantitatively the experimentally determinedthresholds for lung hemorrhage shown in Figure 4to values of output shown on-screen in specificexposure situations. These relationships dependon assumptions for geometry of the tissue pathand sound beam and the attenuation characteris-tics of the tissues through which the sound passes.This must be done in any application; however,the relationship between output and exposure isparticularly contorted in the case of the lung.
Lung exposure in routine practice is confinedalmost exclusively to echocardiography. Withinthis discipline, transdermal and transesophagealexaminations of the heart present different
578 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
Figure 3. Histologic section through hemorrhage induced in ratlung exposed to pulsed ultrasound under superthreshold expo-sure conditions. Scale bar indicates 200 µm. Inset, Enlargementof the pleural surface in the region of damage. Scale bar indi-cates 20 µm. Note the accumulation of red blood cells in thealveoli. Hematoxylin-eosin stain.
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

anatomic pictures. In either case, the lung maybe exposed either in the near field of the trans-ducer or at the distal surface of the heart after thesound beam has passed through heart muscleand blood.
Information on machine output relevant tolung exposure comes to the operator as themechanical index (MI). The MI was formulatedwith a simple homogeneous organ such as theliver in mind. In that application, the MI multi-plied by the square root of the frequency wouldgive a reasonable approximation to the negativeacoustic pressure at the focus of the transducer.Almost nothing that entered into the definitionof MI is relevant to exposure of the lung in
echocardiographic applications. Therefore, onemust “undo” the on-screen MI information toget the original output information and add sev-eral assumptions about the geometry of the fieldand the attenuation of the tissues that are actual-ly in the sound path. Undoing the MI is straight-forward. We simply multiply the on-screennumber by the square root of the frequency andthe attenuation built into the definition of MI.In many cases, this will yield the focal pressureoriginally measured for the instrument inwater.124–126 We can then apply more realisticattenuations that are applicable to the echocar-diographic setting. An idealized transdermalexposure is sketched in Figure 5.
Church et al
Table 1. Summary of Threshold Data for Lung Hemorrhage
Lung Hemorrhage Threshold ResultsFrequency, Beamwidth, PRF, Pulse Exposure pr, In
Nature of Study Animal MHz µm kHz Duration, µs Duration, s Situ, MPa
Threshold1 Mouse 2.8 466 1.0 1.4 10 3.6Mouse 5.6 448 1.0 1.2 10 3.0Rat 2.8 466 1.0 1.4 10 2.3Rat 5.6 448 1.0 1.2 10 2.8
Beamwidth2 Rat 2.8 470 1.0 1.1 10 3.6Rat 2.8 930 1.0 1.1 10 3.5Rat 5.6 310 1.0 1.1 10 3.5Rat 5.6 510 1.0 1.1 10 3.4
Age dependence3 Pig, 5 d 3.1 610 1.0 1.2 10 3.6Pig, 39 d 3.1 610 1.0 1.2 10 5.8Pig, 58 d 3.1 610 1.0 1.2 10 2.9
Threshold4 Rabbit 5.6 510 1.0 1.1 10 3.5Frequency5 Mouse 3.7 NR 0.1 1.0 180 1.4Threshold6 Rat 4.0 NR 1.25 1.0 90 2.0
Rat 4.0 NR 0.4 1.0 90 2.5Pulse length7 Rat 2.8 470 1.0 1.3 10 3.1
Rat 2.8 470 1.0 4.4 10 2.8Rat 2.8 470 1.0 8.2 10 2.3Rat 2.8 470 1.0 11.7 10 2.0
Frequency8 Mouse 1.1, U NR 0.1 10.0 180 0.4Mouse 1.2 NR 0.1 10.0 180 0.7Mouse 2.3, U NR 0.1 10.0 180 0.6Mouse 3.5, U NR 0.1 10.0 180 1.3Mouse 3.7 NR 0.1 10.0 180 1.0
On time9 Mouse 1.2 3500 0.017 10.0 180 1.1Threshold10 Mouse 1.0 1000 0.1 10.0 180 0.4
Mouse 1.0 1000 1.0 10.0 2.4 1.5Exposure Duration11 Mouse 2.3, U NR 0.1 10.0 180 0.7
Mouse 2.3, U NR 0.1 10.0 20 0.8Threshold12 Pig 2.3 3000 0.1 10.0 120 0.9Threshold13 Pig 2.3 3000 0.1 10.0 120 0.7Age dependence14 Mouse, N 1.15 NR 0.1 10.0 180 0.6
Mouse, J 1.15 NR 0.1 10.0 180 0.9Mouse, A 1.15 NR 0.1 10.0 180 0.7
A indicates adult; J, juvenile; N, neonate; NR, not reported; and U, unfocused transducer.1Zachary et al109; 2O’Brien et al111; 3O’Brien et al120; 4O’Brien et al117; 5Child et al100; 6Holland et al107; 7O’Brien et al113;8Child et al100; 9Raeman et al103; 10Frizzell et al92; 11Raeman et al104; 12Baggs et al118; 13Dalecki et al119; 14Dalecki et al.18
J Ultrasound Med 2008; 27:565–592 579
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

Instead of the homogeneous medium envi-sioned in the definition of MI, the echocardio-graphic exposure potentially exposes 5 distinctlydifferent tissues, lung, bone, intercostal muscle,heart muscle, and blood, each with its own atten-uation characteristics. Lung and bone each havevery high attenuation coefficients and acousticimpedances that differ greatly from those of
heart muscle and blood. The attenuation of boneis so high that we can exclude any tissue underly-ing it from consideration. Furthermore, theattenuation of the lung itself is so high that onlyits superficial tissue is involved in threshold con-siderations. The attenuation coefficients of themuscle tissues and blood are to a close approxi-mation linear functions of the frequency. Valuesassumed for these tissues and the attenuationincluded in the definition of the MI are summa-rized in Table 2.
For the acoustic pressure pt in the tissue at thesurface of the lung in a diagnostic examination toequal the threshold pressure, the source transduc-er must be adjusted so that its pressure in water pw
at a corresponding distance from the source isgreater than the threshold pressure by the attenu-ation of the tissues in the path to the lung:
(9)
Ai and zi are the attenuation coefficients (normal-ized to 1 MHz) and path lengths of the tissues inthe path, and f is frequency in MHz. To get thedesired value of pw, we would need a screen valueof the MI of
(10)
or
(11)
The closest practical window to the heart isthrough the intercostal tissue. The initial phase ofan examination of the heart is spent in a searchfor the best possible location for the transducer.During that time, lung tissue near the chest wallwill be exposed to the near field of the source.Selection of the window automatically elimi-nates much of the proximal lung simply becauseit has very high attenuation. While only a verysmall margin of the beam can hit the lung with-out seriously limiting the diagnostic information,in many cases, some proximal lung is exposedthroughout the examination.
In this case, the actual path is through approxi-mately 2 cm of intercostal tissue instead of theliverlike material assumed in the definition of MI.At 3 MHz, the exponential function in Equation
∑ ∑−
=i
iMii )(
2/1t
t
zAzAf I
ef
pMI .
∑−
= iiMI
2/1w
t
zfA
ef
pMI ,
∑= i
ii
tw
zAf
epp .
580 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
Figure 4. In situ negative pressure thresholds for lung hemor-rhage induced by exposure to low–temporal-average intensitypulsed ultrasound in the diagnostic frequency range. Exposureswere to mice, rats, and pigs using pulse durations of 1.4microseconds or less for exposures of 10 seconds (group A) and10 microseconds for exposures of 180 seconds (group B). Dataare culled from Table 1.
Figure 5. Exposure of lung through the chest wall.
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

11 above is 2.3. Referring back to Figure 4, wherethe thresholds are approximately 1 MPa for thelong-pulse exposures (group B) and 3 MPa forthe short-pulse exposures (group A), we see thatthe corresponding values of MIt are 1.3 and 3.9.Comparing this to the MI limit of 1.9 in mostdiagnostic devices, we see that damage to theproximal lung can be ruled out in all but atypi-cally long-pulse exposures.
Figure 4 shows that with long pulses, thethreshold is approximately 0.6 MPa at 1 MHz. Forthe case of exposure of the surface of the lungthrough the intercostal tissue by a transducer incontact with the skin, the MIt would be 0.8. Thisexample is purely hypothetical, of course. Notethat implicit in these computations is theassumption that the focus of the transducer ison the surface of the lung. That would be dif-ficult at frequencies as low as 1 MHz. In fact, it ishighly unlikely to occur in any practicalechocardiographic examination. In other words,the lung under the ribcage would be exposed tothe near field of the transducer. The near field ofa focused transducer has many high-pressureregions, but all are significantly lower than thefocal pressure. Taking all of these factors intoconsideration, it appears extremely unlikely thatthe proximal surface of the lung would be dam-aged in any normal clinical procedure. Thesame general considerations allow us to rule outdamage to the proximal lung surface in trans-esophageal examinations.
Consider next lung tissue on the far side of theheart. Although the focus of the sound beamwould fall within the heart during most of theexamination, it is possible that the focus itselfwould occasionally fall on the surface of the lungon the distal side of the heart. This worst-caseassumption will be used in the calculation. In
addition to the attenuation of 2 cm of the chestwall, this path includes roughly 2 cm of heartmuscle and 8 cm of blood for a total path of 12cm. Using this tissue geometry and the attenu-ation coefficients in Table 2 transforms Figure 4to Figure 6. Again, for clarity only the extremesof clinically realistic exposures are shown, andthe “curve fits” have no great significance but aregiven simply to assist in evaluating the data.
Figure 6 illustrates that the on-screen values ofthe MI required to reach the threshold for lunghemorrhage on the distal side of the heart duringa transdermal exposure are rather sensitive tothe choice of the real tissue path. The solid datapoints are for the original assumption involving2 cm each of heart and intercostal muscle and
J Ultrasound Med 2008; 27:565–592 581
Church et al
Figure 6. Threshold data of Figure 4 expressed in terms of on-screen MI for exposures of the lung at the distal surface of theheart (transdermal application). Path 1 includes 2 cm each ofintercostal and heart muscle. Path 2 includes 1 cm each of inter-costal and heart muscle (see “Lung Hemorrhage, RelatingOutput to Threshold”).
Table 2. Representative Attenuation Values for Thoracic Tissues
Attenuation, Tissue Neper/(cm · MHz) Reference
AMI 0.034 AIUM/NEMA,124,125 IEC126
Intercostal tissue 0.17 Dalecki et al,18 Baggs et al,118 Teotico et al,127 Towa et al,128 Miller et al129
Heart muscle 0.060 O’Donnell et al130
Blood 0.024 Carstensen and Schwan131
AIUM indicates American Institute of Ultrasound in Medicine; AMI, attenuation included in the definition of the MI; IEC,International Electrotechnical Commission; and NEMA, National Electrical Manufacturers Association. A
IUM
Co
nsen
sus R
epo
rt on
Poten
tial Bio
effects of D
iagn
ostic U
ltrasou
nd

8 cm of blood. The open data points are for thesame total distance but with 1 cm each of themuscle tissues replaced by blood.
Because the de facto upper limit for diagnosticultrasound equipment is an MI of 1.9, Figure 6shows that lung hemorrhage, in this transducerconfiguration, is unlikely to occur with the shortpulses used in standard B-mode diagnosticexaminations, but caution should be exercisedwith very long pulses and exposure times.
For the lung on the far side of the heart intransesophageal echocardiography, the analysisis the same as it was for the transdermal exam-ple except for the absence of the ribcage (ie, 8cm of blood and 2 cm of heart muscle for a totalpath length of 10 cm). Here, most of the pathhas a somewhat lower attenuation than thatused in the definition of MI. As a result, it is pos-sible in principle with existing diagnosticmachines to produce superthreshold pressuresat the lung surface on the distal side of the hearteven with the short pulses used in B-modeimaging (Figure 7).
Finally, for an extreme example, consider thefollowing hypothetical scenario. Instead of a spe-cialized short-focus transducer, a pediatric cardi-ologist uses one with a 10-cm focus with awater-filled standoff. In this case, the onlyabsorber in the path is a 1-cm chest wall. In thatcase, a 1-MPa threshold at 2 MHz corresponds toan on-screen indication of an MI of 0.5.
We can conclude the following:
1. There is no single on-screen number thatcorresponds to the threshold for lung hem-orrhage. Each application presents a differ-ent problem.
2. We may know outputs with some precisionand have a reasonably accurate value forhemorrhage threshold, but relating the twoquantities in practical situations involvesvery large assumptions.
3. As noted below, both positive and negativepressures are equally effective in producinglung hemorrhage. Nonlinear propagationenhances the positive pressure relative tothe negative pressure in long-focus soundfields. The MI is defined in terms of the peaknegative pressure. There is no simple way torecover the positive pressure in modern sys-tems. However, because a variety of attenua-tions are involved in possible applications, itis unlikely that any other output indicatorcould be devised that would be a direct indi-cator of the threshold for lung hemorrhage.
4. The values used in the examples above arereasonably conservative. From the results, itis clear that lung hemorrhage can occur dur-ing realistic diagnostic exposures. Whereaslung hemorrhage is highly unlikely to occurduring the bulk of routine diagnostic exami-nations, to be completely certain that hem-orrhage will not occur in all applicationswould require output levels that compro-mise the quality of the diagnostic informa-tion in many kinds of examinations.
Superthreshold DamageBecause lung hemorrhage is theoretically possibleas the result of diagnostic procedures, the natureof the possible damage must be known to balancerisk with benefit. The examples above show thateven in the focal region of the transducer, it isunlikely that acoustic pressures will greatly exceedthe threshold for hemorrhage. In young swineexposed for approximately 4 minutes to 2-MHzfocused ultrasound at twice the threshold level (in10-microsecond pulses with a repetition frequen-cy of 100 Hz), the total area of hemorrhage wasapproximately 0.3 cm2.18 Because of the highattenuation of lung tissue, the region of damage is
582 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
Figure 7. Threshold data of Figure 4 expressed in terms of on-screen MI for exposures of the lung at the distal surface of theheart (transesophageal applications).
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

confined to a depth of a few millimeters. The mostvulnerable tissues are the septa that separate thealveoli. Capillaries there are sufficiently damagedthat blood collects in the alveolar space. There isno basis to expect damage in the human lung tobe significantly greater than in swine under thesame exposure conditions.
The superthreshold lesions that have beenobserved in experimental animals do not appearto present a clinically significant problem. Evenrelatively large lesions in rat lung (eg, 30 mm2)began to resolve within a few days after exposureand by 2 weeks had essentially disappeared,leaving only traces of fibrosis.109
Lung hemorrhage in patients will remain hypo-thetical, supported only by basic biophysical evi-dence. It is unlikely that damage to the lung wouldbe detected in living subjects if it were to occur.
Mechanism of Lung HemorrhageThe temporal characteristics of lung hemor-rhage make it clear that heating is not a factor inthe phenomenon, even taking into considera-tion the possibility of selective heating at thebone-air structure that surrounds the organ.132
Instead, the action of ultrasound is purelymechanical.
Even inertial cavitation, which is responsiblefor many of the biological effects of ultrasound,does not appear to play a significant role in lunghemorrhage. Lung tissue is no more sensitive toultrasound than other tissues until it fills withair.133 This appears to have more to do with thefragility of the alveolar walls than to nonlinearoscillation of air bodies. In fact, lung hemorrhagedoes not appear to have any of the properties thatwe associate with classical inertial cavitation:
1. The capillaries of the septa, the most sensi-tive sites for hemorrhage, do not provide anenvironment conducive to inertial cavita-tion. In inertial cavitation, the violence ofcollapse comes from the inertia of inrushingfluid. The environment of the alveolar capil-laries, however, is air not liquid.
2. If a few bubbles in the pulmonary capillarieswere acting as cavitation sites, adding morebubbles should increase the damage. That isthe case for other tissues.134 However, it doesnot happen in lung tissue.114,135
3. Thresholds for lung hemorrhage are lowerthan those for hemorrhage in tissues such asintestine2 and hemolysis in blood and tissuescontaining exogenous contrast microbub-bles136 where, as discussed below and in thearticle on contrast agents in this issue,34 cav-itation is more obviously the responsiblemechanism. The threshold pressures inFigure 4 and Table 1 are the computed “free-field” pressures at the surface of the lung.Because of the very low impedance of thelung relative to the overlying media, a largefraction of the incident field is reflected andinterferes destructively with the incidentwave. Probably no more than half of the inci-dent field is transmitted into the lung. It wasshown that a deflated lung (having animpedance closer to that of the soft tissueoverlying the lung and therefore a highertransmission coefficient) was more easilydamaged than an inflated lung.112,120
4. Some lung studies show a weak dependenceof the threshold on frequency, whereas oth-ers106,109,115 show no significant dependenceon frequency. Most of the bioeffects that areclearly related to acoustic cavitation34 showa stronger frequency dependence.
5. In theory, microbubbles should respondmore violently to negative than to positivepressures. That behavior is found in hemor-rhage of tissues to which contrast agentshave been added.34,137 In the lung, however,negative pressures cause no greater effectthan positive pressures.116,138
6. In many applications, it is possible to elimi-nate inertial cavitation by applying hydro-static pressures to the medium. The excesspressure acts in two ways: (1) with higherambient pressures, greater acoustic pres-sures are necessary to drive the mediuminto tension; and (2) the application ofhydrostatic pressure can drive small bub-bles into solution and completely eliminatethem as cavitation nuclei. The thresholdsfor lung hemorrhage are not changed byexposing experimental animals underhyperbaric conditions.110 Furthermore, thesizes of the lesions were greater underhyperbaric conditions.
J Ultrasound Med 2008; 27:565–592 583
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

None of these observations taken individuallyclearly rules out inertial cavitation as the mecha-nism for lung hemorrhage, but taken collective-ly, the evidence suggests that direct mechanicalstresses associated with propagation of ultra-sound in the lung are the primary cause of hem-orrhage rather than acoustic cavitation. This issupported by the theoretical analysis providedby Fung et al,139 who modeled the response of agroup of gas-filled alveoli to a tensional or com-pressional wave. The alveoli respond to an inci-dent stress (ie, acoustic pressure) wave bycontracting and expanding. During expansion,a tensile stress is generated in the walls of thealveoli, and it is hypothesized that lung traumais caused by overstretching the alveolar mem-branes.140
Cavitation may become a secondary mecha-nism of damage once blood begins to pool inthe alveoli. Considering the environment, itis possible that this blood would containmicrobubbles that would serve as nuclei forinertial cavitation.103
Although microbubbles within the lung do notappear to play a significant role in lung hem-orrhage, the behavior at audible frequenciesof the whole lung acting as a single bubblepotentially provides information on the non-cavitation damage to the tissues at higher fre-quencies. The radial oscillation of the adultmouse lung can be modeled by the linear theo-ry of a gas bubble with a resonance frequency ofapproximately 300 Hz.141 Exposure of themouse to that frequency at levels greater than 2kPa causes extensive hemorrhaging. This isclearly not inertial cavitation. The amplitude ofradial oscillation of the lung at the threshold fordamage is on the order of 1% of the radius of thelung. The injury does not come from a staticstretching of the tissues because normal breath-ing in the same mode but much below resonanceinvolves somewhat greater amplitudes. Rather,the damage is related to the dynamics of theresponse of the lung to the sound field.Remarkably, the liver adjacent to the lung, andtherefore subject to the same dynamics as thesurface of the lung, is hemorrhaged underapproximately the same exposure conditions asthe lung.
Intestinal Hemorrhage
The intestine appears to be the only organ in thenormal body that contains a large concentrationof microbubbles that act as ideal nuclei for iner-tial cavitation. It would be surprising if exposureto ultrasound did not cause damage to the innerwall of the lumen by this mechanism. That this isthe case has been shown in several studies per-formed using both lithotripter pulses142,143 as wellas both pulsed and CW ultrasound at biomedicalfrequencies.144–148 Miller and Thomas145 haveshown that heating is the primary mechanismfor CW exposures but that a nonthermal mecha-nism is solely responsible for effects observedwith short pulse lengths.
The thresholds for intestinal hemorrhage pro-duced by biomedical ultrasound are shown inFigure 8. It is apparent that the data for hemor-rhage in the intestine are rather limited in com-parison with those for lung. While the exposureparameters for both the lung and intestine are sodiverse that no formal comparison is possible, itis possible to say that thresholds for the intestinetend to be somewhat higher than those for thelung.
584 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
Figure 8. Threshold in situ negative pressures for intestinal hem-orrhage induced by exposure to low–temporal-average intensitypulsed ultrasound. Pulse lengths were 10 and 100 microsecondsat PRFs of 10, 100, and 1000 Hz. Exposures were to mice.Exposure durations were 100 seconds at 400 kHz (▲ and ■),1000 seconds at 1.09 MHz (●●), and 300 seconds at other fre-quencies (■■ ).
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

In contrast to the lung, vascular infusion ofexperimental animals with contrast agentsincreases the cavitation damage in the intes-tine.34,148 In this case, however, the sites of hem-orrhage are the capillaries within the intestinaltissue itself rather than within the mucosal-sub-mucosal layer.
Because of the almost random distribution ofgas within the intestine, attenuation of the beampassing through the abdomen is highly variable.This creates uncertainty in relating on-screenoutput information to actual exposure pressuresat the focus of the transducer. With this reserva-tion in mind, a reasonable estimate of maximumpressure at the intestine is just the on-screenindication of the MI multiplied by the squareroot of the frequency.
An Example of Risk Assessment for theMechanism of Spontaneous Nucleation inGas-Free Tissue
For the purposes of this document, risk isdefined as a combination of the probability ofoccurrence of harm and the severity of thatharm, whereas harm is defined as physical injuryor damage to health.149 Regarding these twocomponents of risk:
1. Probability—Of all of the many nonthermalmechanisms considered here, only one maybe considered to have zero probability ofoccurrence during diagnostic sonography,and even then only at the lowest range ofpotential outputs. That mechanism is iner-tial cavitation. It is physically impossible toinduce inertial bubble collapse at an outputbelow a well-defined level, even in the pres-ence of bubbles of optimal size. However,these same bubbles will respond to theacoustic field to produce noninertial cavita-tion; thus, while the probability of inertialcavitation is zero, the probability of harmfrom all cavitational mechanisms is notzero. Furthermore, while it is true that if nobubbles were present, then the probabilitywould be zero, it is also true that bubbles ofany particular size may arise spontaneouslydue to thermal fluctuations within the tis-sues of the body. Although the probability of
such nucleation events may be vanishinglysmall, the probability of cavitation of somekind can never be zero.55,150
2. Harm—There are many nonthermal mech-anisms by which ultrasound may affectbiological tissue, and some of those interac-tions may even be sensible to the subject ofthe examination. While most of theseappear to produce no harmful effect on thesubject and indeed are not capable of pro-ducing harm, at least one type of exposure atdiagnostic levels provides a therapeutic ben-efit: bone healing. It is possible to conceiveof a course of events stemming from thiseffect leading to harm to a patient, but thereis no evidence to suggest that this hasoccurred or is likely ever to occur. Of all themechanisms considered here, those involv-ing the interaction of ultrasound with gasbodies appear to be the most harmful.Damage to the lung or intestine may occurat gas-tissue interfaces, while inertial cavita-tion can damage cells and tissues at anypoint in the body.
From component 1 above, it is reasonable toconclude that the probability of the occurrenceof harm is not zero, while from component 2, it isreasonable to conclude that harm may occurduring a diagnostic examination. The next stepin a determination of risk is to assess the severityof any harm that may occur to the subject. Twolimiting cases will be considered here, one com-mon but mild and the other rare but severe.
For the first case, consider petechial hemor-rhage in the lung or intestine. Because the in situthreshold rarefactional pressure for an effect iswithin the diagnostic range, it is reasonable toassume that some patients will have modestdamage to their lung during a cardiac examina-tion or to their intestine during an abdominalexamination. However, numerous studies haveshown that the severity of this damage is verylow, and in addition, there is good evidence thatsuch damage heals quickly and completely.Therefore, the risk of permanent harm fromexposure to diagnostic ultrasound is extremelysmall.
For the second case, consider the possibilitythat isolated inertial cavitation events may trans-form cells and tissue. While such events are
J Ultrasound Med 2008; 27:565–592 585
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

much rarer than petechial hemorrhage in thelung or intestine, the preceding analysis of theseverity of any harm also holds true here.
Two lines of evidence provide an approach tothis problem. First, the in vitro results of Doida etal73,74 show that genetic transformation (ie alter-ation of one or more genes within viable cells) isachieved with ultrasound only at output levelsabove the diagnostic range. In contrast, diagnos-tic levels of x rays produce easily quantifiable lev-els of transformation in the same cell line(Chinese hamster V-79). Second, Church55 hasquantified the theoretical probability of inertialcavitation events in the absence of exogenousmicrobubbles in patients under normal condi-tions (ie, in the absence of conditions recognizedto produce artificially high microbubble contentin the tissues and vasculature, such as recoveryfrom a rapid decompression from high pressure,or the presence of gas bubble–producing bacteri-al infections). The results show that the probabil-ity of obtaining at most 1 inertial cavitation eventduring a typical noncontrast ultrasound exami-nation is 1 per 10,000,000,000 examinations,assuming that the acoustic pressure is 4.0 MPa orhigher and the MI is 1.8 or higher (the current USFood and Drug Administration limit is MI = 1.9).Combining these results indicates that the prob-ability of cellular transformation from a diagnos-tic ultrasound examination is very much less (ie,many orders of magnitude less) than is true for adiagnostic x-ray examination. As for the first caseconsidered above, the risk of permanent harmfrom exposure to diagnostic ultrasound isextremely small.
Summary
Except for the intestine, mammalian tissues,absent exogenous contrast agents, appear to beremarkably free of the small bubbles that may actas cavitation nuclei (note that the lung is a specialcase in that while it contains a large volume ofundissolved gas, this gas is not present in theform of small bubbles). That cavitation nuclei arenot completely absent, or may be formed underextraordinary circumstances, is shown bydecompression illness and detection of inertialcavitation events after repeated exposure tolithotripter shock waves. The biophysics of iner-
tial cavitation tells us that isolated microbubblescan be activated by diagnostically relevant ultra-sound but that the effects of inertial collapsewould be highly localized. That is to say, all of theeffects that may arise in the presence of contrastmicrobubbles may in principle also occur inhealthy subjects without the introduction of con-trast agents but to a much smaller extent. In nor-mal mammalian tissues, the effects are unlikelyto be detectable, and the probability of a clinical-ly significant effect at diagnostic levels is verysmall.
Tissues containing stabilized gas bodies, suchas lung, are more susceptible to nonthermaldamage by diagnostic ultrasound than are tis-sues that do not contain undissolved gas. Thethreshold for adverse effects depends strongly onthe in situ acoustic pressure rather than the pres-sure at the body surface. The dependence on sev-eral other parameters (eg, pulse duration andrepetition rate, temporal-average intensity, andexposure duration) is relatively weak. The thresh-old for lung hemorrhage depends on relativeinflation, with fully inflated lungs being moreresistant to damage. In the biomedical frequencyrange (>1 MHz), thresholds appear to be onlyweakly dependent on frequency. Superthresholdexposures produce an extent of nonthermaldamage that is strongly dependent on the vol-ume of tissue exposed and the duration of expo-sure, while the dependence on pulse durationand repetition rate is less. Significantly, there isgood evidence that any damage heals quicklyand completely. Thus, even if these effects wereto occur in some patients, the probability of aclinically significant effect at diagnostic levels isvery small.
For other nonthermal biological effects such asbone healing and auditory or tactile sensation,tissues appear to respond not to the (megahertz)carrier frequencies directly but rather to the (kilo-hertz) PRF of the wave. Regardless of the mecha-nism, however, none of these effects appear topose a risk to the health and well-being of thepatient undergoing examination by diagnosticultrasound.
Therefore, it is concluded that the risk of per-manent harm from any nonthermal mechanismof action due to exposure to diagnostic ultra-sound is extremely small.
586 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

Conclusions
1. Tissues containing stabilized gas bodies aremore susceptible to nonthermal damage bydiagnostic ultrasound than are tissues thatdo not contain undissolved gas. For thesetissues, there are no confirmed reports ofadverse biological effects in animals pro-duced by a nonthermal mechanism fromexposure to pulsed ultrasound when
where pr and f are the in situ values of therarefactional acoustic pressure and frequen-cy, respectively.a. Lung hemorrhage in mouse neonates
has been observed after exposure topulsed ultrasound at in situ peak rarefac-tional pressures as low as 0.4 MPa at 1.0MHz for 3-minute exposures to 10-microsecond pulses.
b. Lung hemorrhage in young pigs has beenobserved after exposure to pulsed ultra-sound at in situ peak rarefactional pres-sures as low as 1.0 MPa at 2.3 MHz for2-minute exposures to 10-microsecondpulses.
c. Lung hemorrhage in adult pigs has beenobserved after exposure to pulsed ultra-sound at in situ peak rarefactional pres-sures as low as 2.9 MPa at 3.1 MHz for10-second exposures to 1.3-microsecondpulses. This frequency, pulse duration,and dwell time are characteristic of B-mode imaging.
d. Intestinal hemorrhage in adult mice hasbeen observed after exposure to pulsedultrasound at in situ peak-rarefactionalpressures as low as 1.5 MPa at 1.1 MHzfor 5-minute exposures to 10-microsec-ond pulses.
2. In tissues that are not known to containwell-defined gas bodies (eg, the spinal cord),there is no evidence of harmful nonthermalbiological effects from exposure to 10-microsecond pulses of 1-MHz ultrasoundup to a peak rarefactional acoustic pressureof 4 MPa.
Recommendations
Clinical Use1. Users of diagnostic ultrasound should apply
the ALARA (as low as reasonably achievable)principle if the tissues to be exposed containstabilized gas bodies (eg, lung) and the MIexceeds 0.4.
2. Users should be aware that for soft tissuesnot known to contain gas bodies, there is nobasis in present knowledge to suggest anadverse nonthermal bioeffect from currentdiagnostic instruments not exceeding theUS Food and Drug Administration outputlimits.
Research (Global)1. The mechanism by which low-amplitude
acoustic fields produce confirmed biologicaleffects, such as accelerated bone healing,should be investigated and, if possible,understood in detail. This informationwould help to determine whether diagnosticprocedures performed at similar levels posea risk to the patient.
Output Indicators1. At a given frequency, the MI provides to the
clinical user of diagnostic ultrasound a use-ful but imperfect indicator of risk to thepatient. Therefore, use of the MI should becontinued, and improvements to the under-lying algorithm should be implemented aspermitted by better understanding of physi-cal mechanisms and biological effects.
2. Diagnostic ultrasound devices should dis-play the MI if the value of the MI can exceed0.4; the display should begin at a minimumof 0.1 to allow application of the ALARAprinciple.
References
1. National Council on Radiation Protection andMeasurements. Exposure Criteria for Medical DiagnosticUltrasound, II: Criteria Based on All Known Mechanisms.Bethesda, MD: National Council on Radiation Protectionand Measurements; 2002. Report 140.
2. Dalecki D, Child SZ, Raeman CH, Carstensen EL. Tactileperception of ultrasound. J Acoust Soc Am 1995; 97:3165–3170.
2/1r MPa / MHz4.0<f
p,
J Ultrasound Med 2008; 27:565–592 587
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

3. Tsirulnikov EM, Vartanyan IA, Gersuni GV, Rosenblyum AS,Pudov VI, Gavrilov LR. Use of amplitude-modulatedfocused ultrasound for diagnosis of hearing disorders.Ultrasound Med Biol 1988; 14:277–285.
4. Magee TR, Davies AH. Auditory phenomena during tran-scranial Doppler insonation of the basilar artery. J Ultrasound Med 1993; 12:747–750.
5. Arulkumaran S, Talbert DG, Nyman M, Westgren M, HsuTS, Ratman SS. Audible in utero sound from ultrasoundscanner [letter]. Lancet 1991; 338:704–705.
6. Fatemi M, Ogburn PL Jr, Greenleaf JF. Fetal stimulation bypulsed diagnostic ultrasound. J Ultrasound Med 2001;20:883–889.
7. Stratmeyer M, Greenleaf J, Dalecki D, Salvesen K. Fetalultrasound: mechanical effects. J Ultrasound Med 2008;27:597–605.
8. Dyson M, Brookes M. Stimulation of bone repair by ultra-sound. In: Lerski A, Morley P (eds). Ultrasound ’82.Elmsford, NY: Pergamon Press; 1983:61–66.
9. Wang SJ, Lewallen DG, Bolander ME, Chao EYS, IlstrupDM, Greenleaf JF. Low-intensity ultrasound treatmentincreases strength in a rat femoral fracture model. J OrthopRes 1994; 12:40–47.
10. Leung K-S, Lee W-S, Tsui H-F, Liu PP-L, Cheung W-H.Complex tibial fracture outcomes following treatment withlow-intensity pulsed ultrasound. Ultrasound Med Biol2004; 30:389–395.
11. Parvizi J, Wu CC, Lewallen DG, Greenleaf JF, Bolander ME.Low-intensity ultrasound stimulates proteoglycan synthesisin rat chondrocytes by increasing aggrecan gene expres-sion. J Orthop Res 1999; 17:488–494.
12. Parvizi J, Parpura JF, Greenleaf JF, Bolander ME. Calcium sig-naling is necessary for ultrasound-stimulated aggrecan syn-thesis by rat chondrocytes. J Orthop Res 2002; 20:51–57.
13. Greenleaf JF, Argadine HM, Bolander ME. 1 kHz vibrationstimulates ATDC5 chondrocytes. In: Hynynen K (ed).Proceedings of the Fifth International Symposium onTherapeutic Ultrasound. New York, NY: American Instituteof Physics; 2006:49–53.
14. Schaden W. Clinical experience with shock wave therapy ofpseudarthrosis, delayed fracture healing, and cement-freeendoprothesis loosening. In: Siebert W, Buch M (eds).Extracorporeal Shock Waves in Orthopaedics. Heidelberg,Germany: Springer-Verlag; 1997:137–148.
15. Wang C, Chen H, Chen C, Yang K. Treatment ofnonunions of long bone fractures with shock waves. ClinOrthop Relat Res 2001; 387:95–101.
16. O’Brien WD Jr, Deng CX, Harris GR, et al. The risk of expo-sure to diagnostic ultrasound in postnatal subjects: thermaleffects. J Ultrasound Med 2008; 27:517–535.
17. Dalecki D, Keller BB, Raeman CH, Carstensen EL. Effects ofultrasound on the frog heart, I: thresholds for changes incardiac rhythm and aortic pressure. Ultrasound Med Biol1993; 19:385–390.
18. Dalecki D, Child SZ, Raeman CH, Cox C, Penney DP,Carstensen EL. Age dependence of ultrasonically inducedlung hemorrhage in mice. Ultrasound Med Biol 1997;23:767–776.
19. Purnell EW, Sokollu A, Torchia R, Tanner N. Focal choriore-tinitis produced by ultrasound. Invest Ophthalmol 1964;3:657–664.
20. Lizzi FL, Coleman DJ, Driller J, Franzen LA, Jakobiec FA.Experimental, ultrasonically induced lesions in the retina,choroid, and sclera. Invest Ophthalmol Vis Sci 1978;17:350–360.
21. Herman BA, Harris GR. Theoretical study of steady-statetemperature rise within the eye due to ultrasoundinsonation. IEEE Trans Ultrason Ferroelectr Freq Control1999; 46:1566–1574.
22. Nyborg WL. Physical principles of ultrasound. In: Fry FJ (ed).Ultrasound: Its Applications in Medicine and Biology. Part I.New York, NY: Elsevier; 1978:1–75.
23. Nyborg WL. Biological effects of sound and ultrasound. In:Trigg GL (ed). Encyclopedia of Applied Physics. New York,NY: VCH Publishers Inc; 1991:403–420.
24. Dyson M, Woodward B, Pond JB. Flow of red blood cellsstopped by ultrasound. Nature 1971; 232:572–573.
25. Nyborg WL. Acoustic streaming due to attenuated planewaves. J Acoust Soc Am 1953; 25:68–75.
26. Stavros AT, Dennis MA. Ultrasound of breast pathology. In:Parker SH, Jobe WE (eds). Percutaneous Breast Biopsy. NewYork, NY: Raven Press; 1993:111–115.
27. Nightingale KR, Kornguth PJ, Walker WF, McDermott BA,Trahey GE. A novel ultrasonic technique for differentiatingcysts from solid lesions: preliminary results in the breast.Ultrasound Med Biol 1995; 21:745–751.
28. Nightingale KR, Kornguth PJ, Trahey GE. The use of acous-tic streaming in breast lesion diagnosis: a clinical study.Ultrasound Med Biol 1999; 25:75–87.
29. Trahey GE, Palmeri ML, Bentley RC, Nightingale KR.Acoustic radiation force impulse imaging of the mechani-cal properties of arteries: in vivo and ex vivo results.Ultrasound Med Biol 2004; 30:1163–1171.
30. Palmeri ML, Frinkley KD, Zhai L, et al. Acoustic radiationforce impulse (ARFI) imaging of the gastrointestinal tract.Ultrason Imaging 2005; 27:75–88.
31. Evan AP, McAteer JA, Williams JC, et al. Shock wavephysics of lithotripsy: mechanisms of shock wave actionand progress toward improved SWL. In: Moore R, BishoffJT, Loening S, Docimo SG (eds). Textbook of MinimallyInvasive Urology. London, England: Martin Dunitz Ltd;2004:425–438.
32. Howard DD, Sturtevant B. In vitro study of the mechanicaleffects of shock-wave lithotripsy. Ultrasound Med Biol1997; 23:1107–1122.
33. Burov VA, Dmitrieva NP, Rudenko OV. Nonthermal impactof high-intensity ultrasound on a malignant tumor. In:Rudenko OV, Sapozhnikov OA (eds). Nonlinear Acoustics at
588 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

the Beginning of the 21st Century. Vol I. Moscow, Russia;Moscow State University; 2002:411–416.
34. Miller DL, Averkiou MA, Brayman AA, et al. Bioeffects con-siderations for diagnostic ultrasound contrast agents. J Ultrasound Med 2008; 27:611–632.
35. Devin C Jr. Survey of thermal, radiation, and viscous damp-ing of pulsating air bubbles in water. J Acoust Soc Am1959; 31:1654–1667.
36. Leighton TG. The Acoustic Bubble. San Diego, CA:Academic Press; 1994.
37. Prosperetti A. Thermal effects and damping mechanisms inthe forced radial oscillations of gas bubbles in liquids. J Acoust Soc Am 1977; 61:17–27.
38. Gilmore FR. The Growth or Collapse of a Spherical Bubblein a Viscous Compressible Liquid. Pasadena, CA: CaliforniaInstitute of Technology; 1952.
39. Flynn HG. Cavitation dynamics, I: a mathematical formula-tion. J Acoust Soc Am 1975; 57:1379–1396.
40. Keller JB, Miksis MJ. Bubble oscillations of large amplitude.J Acoust Soc Am 1980; 68:628–633.
41. Matsumoto Y, Watanabe M. Nonlinear oscillation of gasbubbles with internal phenomena. Jpn Soc Mech Eng Int J1989; 32:157–162.
42. Prosperetti A, Lezzi A. Bubble dynamics in a compressibleliquid, part 1: first-order theory. J Fluid Mech 1986;168:457–478.
43. Flynn HG, Church CC. Transient pulsations of small gasbubbles in water. J Acoust Soc Am 1988; 84:985–998.
44. Flynn HG. Cavitation dynamics, II: free pulsations and mod-els for cavitation bubbles. J Acoust Soc Am 1975;58:1160–1170.
45. Apfel RE. Acoustic cavitation: a possible consequence ofbiomedical uses of ultrasound. Br J Cancer Suppl 1982;5:140–146.
46. Apfel RE. Possibility of microcavitation from diagnosticultrasound. IEEE Trans Ultrason Ferroelectr Freq Control1986; 32:139–142.
47. Flynn HG. Generation of transient cavities in liquids bymicrosecond pulses of ultrasound. J Acoust Soc Am 1982;72:1926–1932.
48. Apfel RE, Holland CK. Gauging the likelihood of cavitationfrom short-pulse, low-duty cycle diagnostic ultrasound.Ultrasound Med Biol 1991; 17:179–185.
49. Church CC. Frequency, pulse length, and the mechanicalindex. Acoust Res Lett Online 2005; 6:162–168.
50. Yang X, Church CC. Nonlinear dynamics of gas bubbles inviscoelastic media. Acoust Res Lett Online 2005;6:151–156.
51. Bailey MR, Pishchalnikov YA, Sapozhnikov OA, et al.Cavitation detection during shock wave lithotripsy.Ultrasound Med Biol 2005; 31:1245–1256.
52. Evan AP, Willis LR, Lingeman J, McAteer J. Renal traumaand the risk of long-term complications in shock wavelithotripsy. Nephron 1998; 78:1–8.
53. Coleman AJ, Kodama T, Choi MJ, Adams T, Saunders JE.The cavitation threshold of human tissue exposed to 0.2-MHz pulsed ultrasound: preliminary measurements basedon a study of clinical lithotripsy. Ultrasound Med Biol 1995;21:405–417.
54. Coleman AJ, Choi MJ, Saunders JE. Detection of acousticemission from cavitation in tissue during clinical extracor-poreal lithotripsy. Ultrasound Med Biol 1996;22:1079–1087.
55. Church CC. Spontaneous, homogeneous nucleation, iner-tial cavitation and the safety of diagnostic ultrasound.Ultrasound Med Biol 2002; 28:1349–1364.
56. Miller DL, Thomas RM, Williams AR. Mechanisms forhemolysis by ultrasonic cavitation in the rotating exposuresystem. Ultrasound Med Biol 1991; 17:171–180.
57. Coakley WT, Nyborg WL. Cavitation, dynamics of gas bub-bles: applications. In: Fry FJ (ed). Ultrasound: Its Applicationin Medicine and Biology. New York, NY: Elsevier;1978:chap II.
58. Nyborg WL, Miller DL. Biophysical implications of bubbledynamics. In: van Wijngaarden L (ed). The Mechanics andPhysics of Bubbles in Liquids. New York, NY: Kluwer;1982:17–24.
59. Nyborg WL, Miller DL. Biophysical implications of bubbledynamics. Appl Sci Res 1982; 38:17–24.
60. Brayman AA, Miller MW. Cell density dependence of theultrasonic degassing of fixed erythrocyte suspensions.Ultrasound Med Biol 1993; 19:243–252.
61. Rooney JA. Hemolysis near an ultrasonically pulsating gasbubble. Science 1970; 169:869–871.
62. Rooney JA. Shear as a mechanism for sonically inducedbiological effects. J Acoust Soc Am 1972; 52:1718–1724.
63. Rooney JA. Hydrodynamic shearing of biological cells. J BiolPhys 1973; 2:26–40.
64. Nyborg WL. Acoustic streaming. In: Hamilton MF,Blackstock DT (eds). Nonlinear Acoustics. San Diego, CA:Academic Press; 1997:chap 7.
65. Cleveland RO, Lifshitz DA, Connors BA, Evan AP, Willis LR,Crum LA. In vivo pressure measurement of lithotripsyshock waves. Ultrasound Med Biol 1998; 24:293–306.
66. Lokhandwalla M, Sturtevant B. Fracture mechanics modelof stone comminution in ESWL and implications for tissuedamage. Phys Med Biol 2000; 45:1923–1940.
67. Lokhandwalla M, Sturtevant B. Mechanical haemolysis inshock wave lithotripsy (SWL), I: analysis of cell deformationdue to SWL flow-fields. Phys Med Biol 2001; 46:413–437.
68. Lokhandwalla M, McAteer JA, Williams JC Jr, Sturtevant B.Mechanical haemolysis in shock wave lithotripsy (SWL), II:In vitro cell lysis due to shear. Phys Med Biol 2001;46:1245–1264.
J Ultrasound Med 2008; 27:565–592 589
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

69. Makino K, Mossoba MM, Riesz P. Chemical effects of ultra-sound on aqueous solutions: evidence for •OH and •H byspin trapping. J Am Chem Soc 1982; 104:3537–3539.
70. Armour EP, Corry PM. Cytotoxic effects of ultrasound: invitro dependence on gas content, frequency, radical scav-engers and attachment. Radiat Res 1982; 89:369–380.
71. Verral RE, Sehgal CM. Sonoluminescence. In: Suslick KS(ed). Ultrasound: Its Chemical, Physical, and BiologicalEffects. New York, NY: VCH Publishers; 1988:chap 6.
72. Edmonds PD, Sancier KM. Evidence for free radical pro-duction by ultrasound cavitation in biological media.Ultrasound Med Biol 1983; 9:635–639.
73. Doida Y, Miller MW, Cox C, Church CC. Confirmation ofan ultrasound-induced mutation in two in-vitro mam-malian cell lines. Ultrasound Med Biol 1990; 16:699–705.
74. Doida Y, Brayman AA, Miller MW. Modest enhancement ofultrasound-induced mutations in V-79 cells in-vitroUltrasound Med Biol 1992; 18:465–469.
75. Coleman AJ, Saunders JE, Crum LA, Dyson M. Acousticcavitation generated by an extracorporeal shockwavelithotripter. Ultrasound Med Biol 1987; 13:69–76.
76. Kodama T, Takayama K. Dynamic behavior of bubbles dur-ing extracorporeal shock-wave lithotripsy. Ultrasound MedBiol 1998; 24:723–738.
77. Delacretaz G, Walsh JT Jr, Asshauer T. Dynamic polariscop-ic imaging of laser-induced strain in a tissue phantom. ApplPhys Lett 1997; 70:3510–3512.
78. Gracewski SM, Miao H, Dalecki D. Ultrasonic excitation ofa bubble near a rigid or deformable sphere: implications forultrasonically induced hemolysis. J Acoust Soc Am 2005;117:1440–1447.
79. Zhong P, Zhou Y, Zhu S. Dynamics of bubble oscillation inconstrained media and mechanisms of vessel rupture inSWL. Ultrasound Med Biol 2001; 27:119–134.
80. Carstensen EL, Child SZ, Lam S, Miller DL, Nyborg WL.Ultrasonic gas-body activation in Drosophila. UltrasoundMed Biol 1983; 9:473–477.
81. Carstensen EL, Campbell DS, Hoffman D, Child SZ, Ayme-Bellegarda EJ. Killing of Drosophila larvae by the fields of anelectrohydraulic lithotripter. Ultrasound Med Biol 1990;16:687–698.
82. Barenblatt GI. The mathematical theory of equilibriumcracks in brittle fracture. Adv Appl Mech 1962; 7:55–129.
83. Ortiz M. Microcrack coalescence and macroscopic crackgrowth initiation in brittle solids. Int J Solids Struct 1988;24:231–250.
84. Gross DR, Miller DL, Williams AR. A search for ultrasoniccavitation within the canine cardiovascular system.Ultrasound Med Biol 1985; 11:85–97.
85. Ivey JA, Gardner EA, Fowlkes JB, Rubin JM, Carson PL.Acoustic generation of intra-arterial contrast boluses.Ultrasound Med Biol 1995; 21:757–767.
86. Hwang JH, Brayman AA, Reidy MA, Matula TJ, KimmeyMB, Crum LA. Vascular effects induced by combined 1-
MHz ultrasound and microbubble contrast agent treat-ments in vivo. Ultrasound Med Biol 2005; 31:553–564.
87. Fry FJ, Kossoff G, Eggleton RC, Dunn F. Threshold ultrason-ic dosages for structural changes in the mammalian brain.J Acoust Soc Am 1970; 48(suppl 2):1413–1417.
88. Dunn F, Fry FJ. Ultrasonic threshold dosages for the mam-malian central nervous system. IEEE Trans Biomed Eng1971; 18:253–256.
89. Frizzell LA. Threshold dosages for damage to mammalianliver by high intensity focused ultrasound. IEEE TransUltrason Ferroelectr Freq Control 1988; 35:578–581.
90. Taylor KJW, Pond J. The effects of ultrasound of varying fre-quencies on rat liver. J Pathol 1970; 100:287–293.
91. Lee CS, Frizzell LA. Exposure levels for ultrasonic cavitationin the mouse neonate. Ultrasound Med Biol 1988;14:735–742.
92. Frizzell LA, Chen E, Lee C. Effects of pulsed ultrasound onthe mouse neonate: hind limb paralysis and lung hemor-rhage. Ultrasound Med Biol 1994; 20:53–63.
93. Hynynen K. The threshold for thermally significant cavita-tion in dog’s thigh muscle in vivo. Ultrasound Med Biol1991; 17:157–169.
94. Fowlkes JB, Parsons JE, Xu Z, et al. The disruption of tissuestructure using high-intensity pulsed ultrasound. J AcoustSoc Am 2005; 117:2371.
95. Parsons JE, Cain CA, Fowlkes JB. Characterizing pulsedultrasound therapy for production of cavitationally inducedlesions. In: ter Haar GR, Rivens E (eds). Proceedings of theFourth International Symposium on TherapeuticUltrasound. Vol 754. Melville, NY: American Institute ofPhysics; 2005:178–180.
96. ter Haar GR, Daniels S. Evidence for ultrasonically inducedcavitation in vivo. Phys Med Biol 1981; 26:1145–1149.
97. ter Haar GR, Daniels S, Eastaugh KC, Hill CR. Ultrasonicallyinduced cavitation in vivo. Br J Cancer Suppl 1982; 45:151–155.
98. Harvey EN. Physical factors in bubble formation. In: FultonJF (ed). Decompression Sickness. Philadelphia, PA: WBSaunders Co; 1951:90–114.
99. Buckles RG. The physics of bubble formation and growth.Aerosp Med 1968; 39:1062–1069.
100. Child SZ, Hartman CL, Schery LA, Carstensen EL. Lungdamage from exposure to pulsed ultrasound. UltrasoundMed Biol 1990; 16:817–825.
101. Tarantal AF, Canfield DR. Ultrasound-induced lung hemor-rhage in the monkey. Ultrasound Med Biol 1994;20:65–72.
102. Penney DP, Schenk EA, Maltby K, Hartman-Raeman C,Child SZ, Carstensen EL. Morphological effects of pulsedultrasound in the lung. Ultrasound Med Biol 1993;19:127–135.
103. Raeman CH, Child SZ, Carstensen EL. Timing of exposuresin ultrasonic hemorrhage of murine lung. Ultrasound MedBiol 1993; 19:507–512.
590 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd

104. Raeman CH, Child SZ, Dalecki D, Cox C, Carstensen EL.Exposure-time dependence of the threshold for ultrasoni-cally induced murine lung hemorrhage. Ultrasound MedBiol 1996; 22:139–141.
105. Zachary JF, O’Brien WD Jr. Lung lesions induced by contin-uous- and pulsed-wave (diagnostic) ultrasound in mice,rabbits and pigs. Vet Pathol 1995; 32:43–54.
106. O’Brien WD Jr, Frizzell LA, Schaeffer DJ, Zachary JF.Superthreshold behavior of ultrasound-induced lung hem-orrhage in adult mice and rats: role of pulse repetition fre-quency and exposure duration. Ultrasound Med Biol 2001;27:267–277.
107. Holland CK, Deng CX, Apfel RE, Alderman JL, FernandezLA, Taylor KJ. Direct evidence of cavitation in vitro fromdiagnostic ultrasound. Ultrasound Med Biol 1996;22:917–925.
108. Kramer JM, Waldrop TG, Frizzell LA, Zachary JF, O’BrienWD Jr. Cardiopulmonary function in rats with lung hemor-rhage induced by exposure to superthreshold pulsed ultra-sound. J Ultrasound Med 2001; 20:1197–1206.
109. Zachary JF, Frizzell LA, Norrell KS, Blue JP, Miller RJ, O’BrienWD Jr. Temporal and spatial evaluation of lesion reparativeresponses following superthreshold exposure of rat lung topulsed ultrasound. Ultrasound Med Biol 2001; 27:829–839.
110. O’Brien WD Jr, Frizzell LA, Weigel RM, Zachary JF.Ultrasound-induced lung hemorrhage is not caused byinertial cavitation. J Acoust Soc Am 2000; 108:1290–1297.
111. O’Brien WD Jr, Simpson DG, Frizzell LA, Zachary JF.Superthreshold behavior and threshold estimation of ultra-sound-induced lung hemorrhage in adult rats: role ofbeamwidth. IEEE Trans Ultrason Ferroelectr Freq Control2001; 48:1695–1705.
112. O’Brien WD Jr, Kramer JM, Waldrop TG, Frizzell LA,Zachary JF. Ultrasound-induced lung hemorrhage: role ofacoustic boundary conditions at the pleural surface. JAcoust Soc Am 2002; 111:1102–1109.
113. O’Brien WD Jr, Simpson DG, Frizzell LA, Zachary JF.Threshold estimates and superthreshold behavior of ultra-sound-induced lung hemorrhage in adult rats: role of pulseduration. Ultrasound Med Biol 2003; 29:1625–1634.
114. O’Brien WD Jr, Simpson DG, Frizzell LA, Zachary JF. Effectof contrast agent on the incidence and magnitude ofultrasound-induced lung hemorrhage in rats.Echocardiography 2004; 21:417–422.
115. O’Brien WD Jr, Simpson DG, Frizzell LA, Zachary JF.Superthreshold behavior of ultrasound-induced lung hem-orrhage in adult rats: role of pulse repetition frequency andexposure duration revisited. J Ultrasound Med 2005;24:339–348.
116. Frizzell LA, O’Brien WD Jr, Zachary JF. Effect of pulse polar-ity and energy on ultrasound-induced lung hemorrhage inadult rats. J Acoust Soc Am 2003; 113:2912–2926.
117. O’Brien WD Jr, Yan Y, Simpson DG, et al. Threshold esti-mation of ultrasound-induced lung hemorrhage in adult
rabbits, and comparison of thresholds in rabbits, rats andmice. Ultrasound Med Biol 2006; 32:1793–1804.
118. Baggs R, Penney DP, Cox C, et al. Thresholds for ultrasoni-cally induced lung hemorrhage in neonatal swine.Ultrasound Med Biol 1996; 22:119–128.
119. Dalecki D, Child SZ, Raeman CH, Cox C, Carstensen EL.Ultrasonically induced lung hemorrhage in young swine.Ultrasound Med Biol 1997; 23:777–781.
120. O’Brien WD Jr, Simpson DG, Ho MH, Miller RJ, Frizzell LA,Zachary JF. Superthreshold behavior and threshold estima-tion of ultrasound-induced lung hemorrhage in pigs: roleof age dependency. IEEE Trans Ultrason Ferroelectr FreqControl 2003; 50:153–169.
121. Dalecki D, Raeman CH, Child SZ, Carstensen EL. Lungresponse to low-frequency underwater sound. J AcoustSoc Am 1999; 106:2165.
122. O’Brien WD, Zachary JF. Mouse lung damage from expo-sure to 30 kHz ultrasound. Ultrasound Med Biol 1994;29:287–297.
123. Meltzer RS, Adsumelli R, Risher W, et al. Lack of lung hem-orrhage in humans after intraoperative transesophagealechocardiography with ultrasound exposure conditionssimilar to those causing lung hemorrhage in laboratory ani-mals. J Am Soc Echocardiogr 1998; 11:57–60.
124. American Institute for Ultrasound in Medicine, NationalElectrical Manufacturers Association. Standard for Real-Time Display of Thermal and Mechanical Indices onDiagnostic Ultrasound Equipment. Laurel, MD: AmericanInstitute of Ultrasound in Medicine; Rosslyn, VA: NationalElectrical Manufacturers Association; 1992.
125. American Institute for Ultrasound in Medicine, NationalElectrical Manufacturers Association. Standard for Real-Time Display of Thermal and Mechanical Acoustic OutputIndices on Diagnostic Ultrasound Equipment. Laurel, MD:American Institute of Ultrasound in Medicine; Rosslyn, VA:National Electrical Manufacturers Association; 1998.
126. International Electrotechnical Commission. MedicalElectrical Equipment, Part 2: Particular Requirements forthe Safety of Ultrasonic Diagnostic and MonitoringEquipment. Ed 1.1. Geneva, Switzerland: InternationalElectrotechnical Commission; 2004. Publication 60601-2-37.
127. Teotico GA, Miller RJ, Frizzell LA, Zachary JF, O’Brien WD Jr.Attenuation coefficient estimates of mouse and rat chestwall. IEEE Trans Ultrason Ferroelectr Freq Control 2001;48:593–601.
128. Towa RT, Miller RJ, Frizzell LA, Zachary JF, O’Brien WD Jr.Attenuation coefficient and propagation speed estimatesof rat and pig intercostal tissue as a function of tempera-ture. IEEE Trans Ultrason Ferrorelectr Freq Control 2002;49:1411–1420.
129. Miller RJ, Frizzell LA, Zachary JF, O’Brien WD Jr. Attenuationcoefficient and propagation speed estimates of intercostaltissue as a function of pig age. IEEE Trans UltrasonFerroelectr Freq Control 2002; 49:1421–1429.
J Ultrasound Med 2008; 27:565–592 591
Church et al
AIU
M C
on
sensu
s Rep
ort o
n Po
tential B
ioeffects o
f Diag
no
stic Ultraso
un
d

130. O’Donnell M, Mimbs JW, Miller JG. The relationshipbetween collagen and ultrasonic attenuation in myocardialtissue. J Acoust Soc Am 1979; 65:512–517.
131. Carstensen EL, Schwan HP. Absorption of sound arisingfrom the presence of intact cells in blood. J Acoust Soc Am1959; 31:185–189.
132. Hartman CL, Child SZ, Penney DP, Carstensen EL. Ultrasonicheating of lung tissue. J Acoust Soc Am 1992; 91:513–516.
133. Hartman CL, Cox CA, Brewer L, Child SZ, Cox CF,Carstensen EL. Effects of lithotripter fields on developmentof chick embryos. Ultrasound Med Biol 1990; 16:581–585.
134. Dalecki D, Raeman CH, Child SZ, Penney DP, Mayer R,Carstensen EL. The influence of contrast agents on hemor-rhage produced by lithotripter fields. Ultrasound Med Biol1997; 23:1435–1439.
135. Raeman CH, Dalecki D, Child SZ, Meltzer RS, CarstensenEL. Albunex does not increase the sensitivity of the lung topulsed ultrasound. Echocardiography 1997; 14:553–558.
136. Dalecki D, Raeman CH, Child SZ, et al. Hemolysis in vivofrom exposure to pulsed ultrasound. Ultrasound Med Biol1997; 23:307–313.
137. Dalecki D, Child SZ, Raeman CH, Xing C, Gracewski S,Carstensen EL. Bioeffects of positive and negative acousticpressures in mice infused with microbubbles. UltrasoundMed Biol 2000; 26:1327–1332.
138. Bailey MR, Dalecki D, Child SZ, et al. Bioeffects of positiveand negative acoustic pressures in vivo. J Acoust Soc Am1996; 100:3941–3946.
139. Fung YC, Yen RT, Tao ZL, Liu SQ. A hypothesis on themechanism of trauma of lung tissue subjected to impactload. J Biomech Eng 1988; 110:50–56.
140. Fung YC. Strengh, trauma, and tolerance. In: BiomechanicsMotion, Flow, Stress, and Growth. New York, NY: Springer-Verlag; 1990:chap 12.
141. Dalecki D, Child SZ, Raeman CH. Thresholds for sound-induced lung hemorrhage for frequencies from 100 Hz to1 MHz. J Acoust Soc Am 2006; 119:3375.
142. Raeman CH, Child SZ, Dalecki D, Mayer R, Parker KJ,Carstensen EL. Damage to murine kidney and intestinefrom exposure to the fields of a piezoelectric lithotripter.Ultrasound Med Biol 1994; 20:589–594.
143. Dalecki D, Raeman CH, Child SZ, Carstensen EL. Thresholdsfor intestinal hemorrhage in mice exposed to a piezoelec-tric lithotripter. Ultrasound Med Biol 1995; 21:1239–1246.
144. Lehmann JF, Herrick JF. Biologic reaction to cavitation, aconsideration for ultrasonic therapy. Arch Phys Med Rehab1953; 39:347–356.
145. Miller DL, Thomas RM. Heating as a mechanism for ultra-sonically induced petechial hemorrhages in mouse intes-tine. Ultrasound Med Biol 1994; 20:493–503.
146. Dalecki D, Raeman CH, Child SZ, Carstensen EL. Intestinalhemorrhage from exposure to pulsed ultrasound.Ultrasound Med Biol 1995; 21:1067–1072.
147. Miller DL, Gies RA. The interaction of ultrasonic heatingand cavitation in vascular bioeffects on mouse intestine.Ultrasound Med Biol 1998; 24:123–128.
148. Miller DL, Gies RA. Gas-body-based contrast agentenhances vascular bioeffects of 1.09 MHz ultrasound onmouse intestine. Ultrasound Med Biol 1998; 24:1201–1208.
149. International Organization for Standardization. MedicalDevices: Application of Risk Management to MedicalDevices. Geneva, Switzerland: International Organizationfor Standardization; 2000. Publication 14971:2000.
150. Herbertz J. Spontaneous cavitation in liquids free of nuclei.In: Fortschritte der Akustik DAGA ’88. Bad Honnef,Germany: DPG GmbH; 1988:439–442.
592 J Ultrasound Med 2008; 27:565–592
Diagnostic Ultrasound in Postnatal Subjects: Nonthermal Mechanisms
AIU
M C
on
sen
sus
Rep
ort
on
Po
ten
tial
Bio
effe
cts
of
Dia
gn
ost
ic U
ltra
sou
nd