Embed Size (px)
Citation preview

The Risk of CV Events for Patients Treated The Risk of CV Events for Patients Treated with Clopidogrel or Prasugrel in with Clopidogrel or Prasugrel in
Combination with a Proton Pump Inhibitor Combination with a Proton Pump Inhibitor
Results from the TRITON-TIMI 38 Trial Results from the TRITON-TIMI 38 Trial
M. O’Donoghue, S.D. Wiviott, E.M. Antman,
S.A. Murphy, C.F. Contant, E.R. Bates, Y. Rozenman,
J.L. Mega, M.S. Sabatine and E. Braunwald
Cardiovascular Division, Brigham and Women’s Hospital

DisclosuresDisclosures M. O’Donoghue: M. O’Donoghue: nonenone
S.D. Wiviott: S.D. Wiviott: Grants from Eli Lilly, Daiichi Sankyo, sanofi aventis, Schering Plough. Grants from Eli Lilly, Daiichi Sankyo, sanofi aventis, Schering Plough. Consulting or advisory board fees: Astra Zeneca, sanofi aventis. Honoraria from Eli Lilly, Consulting or advisory board fees: Astra Zeneca, sanofi aventis. Honoraria from Eli Lilly, Daiichi Sankyo, Astra Zeneca, Schering PloughDaiichi Sankyo, Astra Zeneca, Schering Plough
E.M. Antman: E.M. Antman: Grants from Eli Lilly, Daiichi Sankyo, sanofi aventis. Consulting or advisory Grants from Eli Lilly, Daiichi Sankyo, sanofi aventis. Consulting or advisory board feesboard fees from sanofi aventis. Lecture fees from Eli Lilly, sanofi aventisfrom sanofi aventis. Lecture fees from Eli Lilly, sanofi aventis
S.A. Murphy: S.A. Murphy: Research grants from Eli Lilly, Daiichi Sankyo. Consulting fees from Eli Lilly.Research grants from Eli Lilly, Daiichi Sankyo. Consulting fees from Eli Lilly.
E.R. Bates: E.R. Bates: Honoraria from Eli Lilly, Daiichi Sankyo, sanofi aventis, Bristol-Myers SquibbHonoraria from Eli Lilly, Daiichi Sankyo, sanofi aventis, Bristol-Myers Squibb
Y. Rozenman: Y. Rozenman: Consulting or lecture fees from Eli Lilly, sanofi aventis, Medtronic, Boston Consulting or lecture fees from Eli Lilly, sanofi aventis, Medtronic, Boston Scientific, Pfizer, Schering-PloughScientific, Pfizer, Schering-Plough
J.L. Mega: J.L. Mega: Grants from Eli Lilly, Daiichi Sankyo, Johnson & Johnson. Honoraria from Bayer Grants from Eli Lilly, Daiichi Sankyo, Johnson & Johnson. Honoraria from Bayer Healthcare.Healthcare.
M.S. Sabatine: M.S. Sabatine: Research grants from sanofi aventis and Astra Zeneca. Honoraria and/or Research grants from sanofi aventis and Astra Zeneca. Honoraria and/or consulting for sanofi aventis, Bristol-Myers Squibb, Astra Zeneca, Eli Lillyconsulting for sanofi aventis, Bristol-Myers Squibb, Astra Zeneca, Eli Lilly
E. Braunwald: E. Braunwald: Research grants and honoraria from Eli Lilly, Daiichi Sankyo. Research grants and honoraria from Eli Lilly, Daiichi Sankyo.

BackgroundBackground• PPIs are often administered with dual PPIs are often administered with dual
antiplatelet therapy for gastric protectionantiplatelet therapy for gastric protection
1 Gilard et al., J Am Coll Cardiol 2008
2 Sibbing et al., Thromb Haemost 2009
• Ex vivoEx vivo studies have shown diminished studies have shown diminished platelet inhibition in response to clopidogrel platelet inhibition in response to clopidogrel in the presence of a PPI in the presence of a PPI 1,1,2
3 Juurlink et al., CMAJ 2009
4 Ho et al., JAMA 2009
• Recent studies have raised concerns Recent studies have raised concerns that PPIs may attenuate the clinical that PPIs may attenuate the clinical benefit of clopidogrel benefit of clopidogrel 3,43,4

FDA and EMEA StatementsFDA and EMEA Statements
EMEA statement May 29, 2009EMEA statement May 29, 2009::
“The product information for all
clopidogrel-containing medicines
should be amended to discourage
concomitant use of PPIs unless
absolutely necessary”

NNSS
OO
ClCl
OO CHCH33CC
Clopidogrel
Pro-drugs
33
NNSS
OO
CCHHCC
OOFF
OO
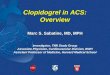
Thienopyridines: Formation of Active MetaboliteThienopyridines: Formation of Active Metabolite
PrasugrelGutGut
Oxidation(Cytochrome P450)
Oxidation(Cytochrome P450)
ActiveMetabolite
HOOCHOOC HSHS
NN
OO
ClCl
OCHOCH33
CYPs:
1A2
2C19
2B6
CYPs:
3A
2C19
2C9
2B6
CHCH33
OONN
SS
OO
ClCl
OOCC
85% Inactive Metabolites
NNSS
OO
FFOO
HOOCHOOC HSHS
NN
OO
FF
CYPs:
3A
2B6
2C9
2C19
ActiveMetabolite
Hydrolysis(Esterases)
-
Proton pump
inhibitors
-
- ?
-

Primary AimPrimary Aim
To examine the association between
PPI use and the risk of CV events for
patients on either clopidogrel or
prasugrel

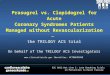
TITAN
ASAn= 13,608
Wiviott et al., NEJM 2007; 357: 2001-5
TRITON-TIMI 38TRITON-TIMI 38

0
5
10
15
0 90 180 270 360 450
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Days
En
dp
oin
t (%
)
12.1
9.9
HR 1.32(1.03-1.68)
P=0.03
Prasugrel
Clopidogrel1.82.4
1o EP: CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
TITAN
Wiviott et al., NEJM 2007; 357: 2001-5
TRITON-TIMI 38TRITON-TIMI 38

MethodsMethods PPI use was at the discretion of the treating
physician and captured on the case-report forms at each patient visit
Propensity scores were constructed to predict PPI use
Cox proportional hazards models included potential confounders and were stratified by propensity score strata

Primary and Secondary AnalysesPrimary and Secondary Analyses
PPI use at randomization
End of follow-up (median 14.5m)
TRITON-TIMI 38 Trial
3 day and 30 day follow-up
Landmark day 3
Landmark month 3
Landmark month 6
* All analyses were stratified by randomized treatment arm
Additional sensitivity analyses “Consistent” use of a PPI
(defined as patients who were taking a PPI at randomization to end of follow-up)
Use of different types of PPIs Use of a PPI or H2 receptor antagonist

PPI Use at RandomizationPPI Use at Randomizationn=4529, 33% of study populationn=4529, 33% of study population
Type of PPI Frequency
Pantoprazole 1844 (40%)
Omeprazole 1675 (37%)
Esomeprazole 613 (14%)
Lansoprazole 441 (9.7%)
Rabeprazole 66 (1.5%)

Baseline CharacteristicsBaseline CharacteristicsPPI usedPPI used
(n=4529)(n=4529)
No PPINo PPI
(n=9079)(n=9079)P valueP value
Age (median)Age (median) 61 y61 y 60 y60 y <0.001<0.001
MaleMale 72%72% 75%75% <0.001<0.001
Caucasian 94%94% 92%92% <0.001<0.001
Western Europe or North America 66%66% 54%54% <0.001<0.001
UA or NSTEMI 75%75% 73%73% 0.0070.007
Diabetes mellitusDiabetes mellitus 24% 23% 0.140.14
HypertensionHypertension 65% 64% 0.080.08
HyperlipidemiaHyperlipidemia 57% 55% 0.070.07
History peptic ulcer diseaseHistory peptic ulcer disease 9.7% 4.1% <0.001<0.001
Hemoglobin (g/dl)Hemoglobin (g/dl) 13.8 14.0 <0.001<0.001

CV
dea
th,
MI
or
stro
ke
Days
CLOPIDOGREL PPI vs no PPI: Adj HR 0.94, 95% CI 0.80-1.11
PPI use at randomization (n= 4529)
Clopidogrel
Primary endpoint stratified by use of a PPI

CV
dea
th,
MI
or
stro
ke
Days
CLOPIDOGREL PPI vs no PPI: Adj HR 0.94, 95% CI 0.80-1.11
PPI use at randomization (n= 4529)
Clopidogrel
Prasugrel
PRASUGREL PPI vs no PPI: Adj HR 1.00, 95% CI 0.84-1.20
Primary endpoint stratified by use of a PPI

Clopidogrel Adj HR (95% CI)
Death, MI or stroke 0.94 (0.80-1.11)
CV death 0.71 (0.47-1.07)
MI 0.98 (0.82-1.17)
Stent thrombosis (ARC def/prob) 1.08 (0.75-1.55)
TIMI major or minor bleeding 1.13 (0.85-1.49)
Prasugrel
Death, MI or stroke 1.00 (0.84-1.20)
CV death 1.06 (0.70-1.62)
MI 1.02 (0.84-1.25)
Stent thrombosis (ARC def/prob) 1.03 (0.60-1.76)
TIMI major or minor bleeding 0.92 (0.71-1.18)
5.01.00.2
PPI use at randomization
Favors PPI PPI worse

Risk of CV events for patients Risk of CV events for patients “consistently” on a PPI“consistently” on a PPI
CV
dea
th,
MI
or
stro
ke
Days
Defined as: PPI used at randomization and end of f/u (n= 2814)
Patients exposed to PPI for shorter durations were censored (n=3882)
CLOPIDOGREL PPI vs no PPI: Adj HR 1.05, 95% CI 0.85-1.30
PRASUGREL PPI vs no PPI: Adj HR 1.10, 95% CI 0.88-1.39
Clopidogrel
Prasugrel

Short-term outcomes stratified by use of a PPIShort-term outcomes stratified by use of a PPIC
V d
eath
, M
I o
r st
roke
Days
Clopi - Adj HR 1.00 (0.80-1.27)
Pras - Adj HR 1.14 (0.88-1.46)
PPI use at randomization (n= 4529)
THROUGH 3 DAY FOLLOW-UP THROUGH 30 DAY FOLLOW-UP
Clopi - Adj HR 0.98 (0.80-1.21)
Pras - Adj HR 1.09 (0.87-1.37)
Clopi
Pras

Type of PPIClopidogrel
HR (95% CI)CV death, MI or stroke
PrasugrelHR (95% CI)
CV death, MI or stroke
Omeprazole
(n=1675)0.91 (0.72-1.15) 1.04 (0.81-1.34)
Pantoprazole
(n=1844)0.94 (0.74-1.18) 1.09 (0.86-1.39)
Esomeprazole
(n=613)1.07 (0.75-1.52) 0.86 (0.55-1.33)
Lansoprazole
(n=441)1.00 (0.63-1.59) 0.98 (0.61-1.57)
Risk of CV events with different types of PPIsRisk of CV events with different types of PPIs
Rabeprazole not included due to small sample size (n=66)

Additional sensitivity analysesAdditional sensitivity analyses
No association seen between PPI use and the risk of CV events for:
Use of a PPI or H2 receptor antagonist at randomization
Landmark analyses that captured PPI use at day 3, month 3 and month 6 after randomization
Landmark analyses to capture PPI use at different timepoints

LimitationsLimitations
Use of a PPI was not randomized, Use of a PPI was not randomized, thus there is the potential for thus there is the potential for residual confoundingresidual confounding
PPIs could be started or stopped PPIs could be started or stopped during the course of follow-upduring the course of follow-up

ConclusionConclusion
In TRITON-TIMI 38, PPI use was not associated with an increased risk of CV events for patients on clopidogrel or prasugrel
The current findings do not support the need to avoid concomitant use of PPIs in patients treated with thienopyridines

Available online at www.thelancet.com on September 1, 2009
THE LANCET