Embed Size (px)
Citation preview

Neuropsychologia 84 (2016) 113–126
Contents lists available at ScienceDirect
Neuropsychologia
http://d0028-39
☆ThisCommu(Grant5F31DC
n CorrSargentMA 021
E-m
journal homepage: www.elsevier.com/locate/neuropsychologia
The relationships between the amount of spared tissue, percent signalchange, and accuracy in semantic processing in aphasia$
Jordyn A. Sims a, Kushal Kapse a, Peter Glynn b, Chaleece Sandberg c, Yorghos Tripodis d,Swathi Kiran a,n
a Aphasia Research Laboratory, Boston University, Sargent College of Health and Rehabilitation Sciences, 635 Commonwealth Ave., Boston MA 02215, USAb Northwestern University, Feinberg School of Medicine, 303 Chicago Ave., Chicago, IL 60611, USAc Pennsylvania State University, College of Health and Human Development, Ford Building, State College, PA 16801, USAd Department of Biostatistics, School of Public Health, Boston University, 801 Massachusetts Ave., Boston, MA 02118, USA
a r t i c l e i n f o
Article history:Received 19 November 2014Received in revised form10 September 2015Accepted 12 October 2015Available online 13 January 2016
Keywords:AphasiafMRILanguage recoveryLesion mappingRegions of interest (ROI)
x.doi.org/10.1016/j.neuropsychologia.2015.10.032/& 2016 Elsevier Ltd. All rights reserved.
research was supported by the National Instnication Disorders/National Institute of Heanumber 1K18DC011517-01) and to Chaleec011220).espondence to: Department of Speech LangCollege of Health and Rehabilitation Science14, USA.ail addresses: [email protected] (J.A. Sim
a b s t r a c t
Recovery from aphasia, loss of language following a cerebrovascular incident (stroke), is a complexprocess involving both left and right hemispheric regions. In our study, we analyzed the relationshipsbetween semantic processing behavioral data, lesion size and location, and percent signal change fromfunctional magnetic resonance imaging (fMRI) data. This study included 14 persons with aphasia in thechronic stage of recovery (six or more months post stroke), along with normal controls, who performedsemantic processing tasks of determining whether a written semantic feature matched a picture orwhether two written words were related. Using region of interest (ROI) analysis, we found that leftinferior frontal gyrus pars opercularis and pars triangularis, despite significant damage, were the onlyregions to correlate with behavioral accuracy. Additionally, bilateral frontal regions including superiorfrontal gyrus, middle frontal gyrus, and anterior cingulate appear to serve as an assistive network in thecase of damage to traditional language regions that include inferior frontal gyrus, middle temporal gyrus,supramarginal gyrus, and angular gyrus. Right hemisphere posterior regions including right middletemporal gyrus, right supramarginal gyrus, and right angular gyrus are engaged in the case of extensivedamage to left hemisphere language regions. Additionally, right inferior frontal gyrus pars orbitalis ispresumed to serve a monitoring function. These results reinforce the importance of the left hemispherein language processing in aphasia, and provide a framework for the relative importance of left and rightlanguage regions in the brain.
& 2016 Elsevier Ltd. All rights reserved.
1. Introduction
There is already a significant body of research on the neuro-physiological mechanisms of recovery within each of the phases ofrecovery from aphasia. Multiple studies have emphasized theimportance of reperfusion of damaged tissue in the acute phase ofaphasia recovery (Hillis et al., 2004, 2002 Reineck et al., 2005),while later stages of recovery are likely driven by other mechan-isms, such as the reorganization of structural and functional
19
itute on Deafness and Otherlth grants to Swathi Kirane Sandberg (Grant number
uage and Hearing Sciences,s, Boston University, Boston,
s), [email protected] (S. Kiran).
relationships and learning of compensatory strategies (Hillis andHeidler, 2002).
Saur et al. (2006) studied patients in the sub-acute phase ofrecovery and suggested that reorganization of activation in pa-tients with left hemisphere strokes follows three phases. In theacute phase patients showed significantly reduced left hemisphereactivation. This was followed by a period of increased righthemisphere homologous activation patterns, which correlatedwith improved language function. In the chronic phase, a re-shiftof peak activation to the left hemisphere correlated with evengreater improvements in language function. These results in-dicated that, although the right hemisphere may be engaged as acompensatory region, activation of the left hemisphere is morefacilitatory for language recovery.
Recent qualitative reviews suggest that there is extensivevariability in terms of functional and behavioral characteristicsfrom patient to patient during the chronic phase of recovery.

J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126114
Variables such as lesion location and size influence both activationand task accuracy in the chronic phase. As highlighted above,studies have revealed that while language recovery does occur inboth hemispheres, left hemisphere activation is ultimately moreeffective for long term recovery, and furthermore that the morerestored the left hemisphere, the less the activation in the righthemisphere (Cao et al., 1999; Heiss et al., 1999; Jordan and Hillis,2005; Karbe et al., 1998; Thiel et al., 2013; van Oers et al., 2010;Winhuisen et al., 2007).
More specifically, Fridriksson et al. (2010) found that increasednaming accuracy was associated with greater activation in pre-served left hemisphere tissue, indicating the importance of the lefthemisphere in terms of behavioral accuracy. These results suggestthat post-stroke language function is dependent on the activation ofpreserved tissue in the left hemisphere. Further, Fridriksson et al.(2012) examined activation of the perilesional cortex which wasdefined as tissue directly adjacent to the lesion exhibiting hypo-perfusion. The boundaries to define perilesional cortex within thisspecific study were calculated based on group results examiningcerebral perfusion (up to 15 mm beyond the lesion). Perilesionalactivation, particularly in the frontal lobe, predicted improved ac-curacy following anomia treatment. Modulation of posterior areas,primarily in the temporal lobe, predicted decreased semanticparaphasias, while modulation of the parietal lobe predicted de-creased phonemic paraphasias. Again, activation of left hemisphericnetworks appear to be associated with better recovery.
The importance of activation in residual, undamaged tissue inleft hemisphere language regions is again underscored in a meta-analysis of 12 studies (Turkeltaub et al., 2011), in which the au-thors investigated the influence of lesion location on languagerecovery. The authors conducted a systematic review in whichthey compiled study results to achieve an experimental group of105 patients and a control group of 129 normal control partici-pants, across 16 unique tasks. Patients were divided into twogroups: those with lesions in inferior frontal gyrus (IFG) and thosewithout lesions in IFG. The study found that normal controls wereconsistent in their activations during generalized language tasks;normal controls activated left inferior frontal gyrus (LIFG), withparticular peaks in left inferior gyrus pars opercularis (LIFGop), leftinferior frontal gyrus pars orbitalis (LIFGorb), and left inferiorfrontal gyrus pars triangularis (LIFGtri), and also activated leftmiddle temporal gyrus (LMTG). Across the 16 unique languagetasks, patients with aphasia were consistent in their recruitmentmechanisms, depending upon whether the LIFG was damaged ornot. Patients with damage to the LIFG showed activation inneighboring ipsilesional regions (left anterior insula, left middlefrontal gyrus (LMFG)) as well as right hemisphere homologues(RIFGop, RIFGorb, RIFGtri). Patients without damage to LIFGshowed activation in the left hemisphere (LIFG, LMFG, LMTG), andsome right hemisphere activation (RMTG and RIFGtri). Taken to-gether, these studies highlight the importance of left hemisphereIFG but do not address when and under what circumstances ac-tivation of left hemisphere undamaged regions emerges in pa-tients with aphasia.
The size, or extent, of the lesion also is important in determiningthe pattern of activation (Allendorfer et al., 2012; Crinion et al.,2013). Sebastian and Kiran (2011) found that when examining re-gions of interest (ROIs) that were active during a picture namingand semantic processing task, larger lesions in the left hemispheretended to result in greater right hemisphere activation than didsmaller lesions in the left hemisphere. This positive relationshipbetween larger lesions and more likely right hemisphere compen-sation is supported by Grafman (2000), who suggested that re-cruitment of right-hemisphere homologues is more likely whencortical regions that serve a specific function are entirely destroyed,and that transfer of function is less likely if damage is incomplete.
The relationship between the extent of lesion and languagefunction has also been examined in the literature. One approach,albeit indirect, to understanding the effect of lesion on languagefunction is the Voxel-Based Lesion-Symptom Mapping (VLSM)methodology. VLSM integrates behavioral data and very specificlesion data to identify lesioned regions that most affect specificfunctions (Bates et al., 2003). Multiple studies have used VLSM toexamine data of patients with aphasia (Arévalo et al., 2012; Baldoet al., 2010; Baldo et al., 2006; Baldo et al., 2011; Borovsky et al.,2007; Kim et al., 2010; Magnusdottir et al., 2013; Piras and Mar-angolo, 2007, 2010). Pertinent to the present study, Dronkers et al.(2004) utilized VLSM in a study of language comprehension, andfound that left hemisphere regions including MTG, superior tem-poral gyrus (STG), the superior temporal sulcus (STS) and angulargyrus (AG), and IFG were involved in language comprehension;specifically, patients with aphasia whose lesions did not affectthese areas performed comparable to normal controls in measuresof language comprehension. In another study, Walker et al. (2011)found that damage to Wernicke's area was not correlated withsemantic error production and instead the strongest correlationsbetween semantic errors and lesioned tissue were found in the leftanterior temporal lobe. Likewise, Antonucci et al. (2008) andLambon Ralph et al. (2012) have demonstrated impairments inprocessing of semantic information in patients with damage to leftinferior temporal lobe.
VLSM is an efficient method for mapping behavior onto lesionsin chronic stroke patients (Geva et al., 2012). However, it does notprovide information regarding whether undamaged tissue is ac-tually engaged in the service of a specific language processingfunction. Specifically, while a lesion in a region is correlated withan impairment in language function, the inverse is not necessarilytrue; the lack of a lesion in a region does not necessarily mean thatthis preserved region is accomplishing that language function.Further, simply because damage to a region is linked to impairedlanguage function, it does not mean that regions remote to thelesion are also not affected (i.e., dynamic diaschisis (Price et al.,2001). To answer that question, we need to return to fMRI studiesthat provide structure function mapping and take into account theamount of lesioned tissue in calculating percent BOLD signalchange.
Moreover, while fMRI studies on language recovery broadlysuggest that left hemisphere language regions are important forlanguage recovery, studies from normal individuals have shownthat these same regions are involved in several specific aspects oflanguage processing including semantic processing, the focus ofthe present study. Therefore, the goal of the present study was toexamine how the extent of signal change in preserved left hemi-sphere (LH) regions and homologous right hemisphere (RH) re-gions varied as a function of lesion size in the LH. Within thisstudy, we attempt to build upon our pre-existing knowledge of theprocesses of language recovery following the onset of aphasia bycombining structural, functional and behavioral data to examinethe relationship between lesion location, lesion size, task perfor-mance and percent signal change in left and right hemisphereregions. Studies have not yet examined the relationships betweenlesion location, size, and percent signal change, in particular withregards to task accuracy, which can provide information regardingthe recruitment of specific language regions during successful andunsuccessful language performance.
As noted above, we examined semantic processing in thisproject, which has been an important focus of neuroimaging re-search in aphasia. Recent theories of semantic processing havecombined behavioral and anatomical data to explain how wecreate, manipulate, and utilize linguistic/semantic meaning (Bin-der and Desai, 2011; Jefferies, 2013; Thompson-Schill et al., 1999).Specifically, Binder and Desai (2011) suggest that certain regions

J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126 115
form a semantic network, processing semantic informationthrough the following steps: first, modality-specific stimuli areprocessed and the semantic network is engaged (this process isthought to be driven by higher-level temporal and inferior parietalregions that store increasingly abstract semantic representations);second, appropriate semantic information is retrieved (this pro-cess is thought to employ dorsomedial, inferior prefrontal corticeswhich are accompanied by the posterior cingulate gyrus and ad-jacent precuneus); and finally, any appropriate semantic in-formation is stored (this process is thought to utilize a connectionbetween the semantic network and the hippocampal memorysystem) (Binder and Desai, 2011). The model relies on a meta-analysis completed by Binder et al. (2009), that examined 120functional neuroimaging studies focusing on semantics. Acrossthese studies, participants performed different semantic taskswhich ranged from category decision, to semantic decisions (suchas whether a presented stimulus was living or nonliving), to se-mantic feature verification. Therefore, regardless of the specificstimuli or variations of the task, it appears that the process ofretrieving semantic information engages the same network withsome level of consistency.
The present study examined signal change elicited by proces-sing of semantic attributes during the presentation of writtenwords across two tasks. Following Binder and Desai's (2011) fra-mework, the semantic processing tasks required access to visualwritten input, manipulation of abstract semantic representation,and selection of the appropriate response. Given the task re-quirements, we selected ROIs for our study that have been shownto be involved in semantic processing, as well as adjacent regionsto typical lesions in the LH that result in aphasia. See Table 1 for alist of selected ROIs and their presumed functions. The ROIs in-cluded IFG pars orbitalis (IFGorb), pars opercularis (IFGop), andpars triangularis (IFGtri), the middle frontal gyrus (MFG), superiorfrontal gyrus (SFG), anterior cingulate cortex (ACC), middle
Table 1Regions of interest and their presumed functions. Here presumed functions of this papcolumn.
Region Presumed function
Inferior Frontal Gyrus – Pars Orbitalis(IFGorb)
Semantic processing
Inferior Frontal Gyrus – Pars Opercularis(IFGop)
Semantic processing
Inferior Frontal Gyrus – Pars Triangularis(IFGtri)
Semantic cognition
Inferior Frontal Gyrus – Overall (IFG) Phonological, working memory, and syntprocessesSemantic processing
Nonliteral processing
Superior Frontal Gyrus (SFG) Semantic processingNonliteral processing
Middle Frontal Gyrus (MFG) Semantic processingLanguage processingDomain general activation with increaseddifficultyNonliteral processing
Middle Temporal Gyrus (MTG) Semantic processingLanguage comprehension and semanticprocessing
Angular Gyrus (AG) Semantic processingIntegration of individual concepts into a w
Supramarginal Gyrus (SMG) Semantic processingReading
Anterior Cingulate (ACC) Language controlAttention/Working memory
temporal gyrus (MTG), angular gyrus (AG), and supramarginalgyrus (SMG). In this study, we combined AG and SMG (AG/SMG)given their close proximity and overlapping presumed functions,although there are other reports of these regions being distinct intheir function (Caspers et al., 2011). Of note, we did not separatemiddle temporal gyrus into sub-regions. In the literature, Vigneauet al. (2006) identify two peaks, middle temporal lateral andmiddle temporal posterior, while Price (2012) identifies an ante-rior middle temporal and a posterior middle temporal peak ofactivation. Given this variability in the research, and due to the factthat the anatomical atlas we utilized in this study does not dis-tinguish between subregions within MTG, we retained MTG as oneregion.
The ROIs were utilized to calculate percent signal change in ip-silesional spared tissue and corresponding homologous regions. Wechose the methodological approach of examining anatomicallyconstrained ROI-based percent signal change in apriori regions fortwo reasons. First, relative to the typical, whole-brain GLM analysisthat performs the best fit between canonical HRF and acquired data,percent signal change as calculated in Marsbar (Brett et al., 2002)performs time-locked averaging of data into a condition(s) in a gi-ven voxel over the total duration of experiment (Poldrack, 2007),thus providing more information about activation in a particularregion. Second, we chose anatomically defined ROIs to examinepercent signal change (instead of functional ROIs) because func-tional ROIs can be inherently very variable in the peak activationlocation, making it challenging to relate percent signal change todamage across patients. We return to this issue in the methods.
As discussed above, prior research has suggested the involve-ment of contralesional regions following LH damage, and thereforeright hemisphere homologues of the LH ROIs were selected as well.
To summarize, we examined signal change in specific regions ofinterest including typical language regions, neighboring regions,and contralateral homologues, taking lesion size and location as
er's selected ROIs are provided, based on prior literature as listed in the citations
Citations
(Binder et al., 2009; Bookheimer, 2002; Fiez, 1997; Jeffries, 2013)
(Pillai et al., 2003; Vigneau, et al., 2006)
(Vigneau et al., 2006; Jeffries, 2013)
actic (Binder et al., 2009)
(Bedny et al., 2007; Binder et al., 2009; Cappa, 2012; Novick et al., 2009;Reilly et al., 2011; Ruff et al., 2008)(Benedek et al., 2014; Bohrn et al., 2012; Rapp et al., 2012; Vartanian,2012)(Binder et al., 2009)(Benedek et al., 2014; Bohrn et al., 2012; Rapp et al., 2012; Vartanian,2012)(Binder et al., 2009; Pillai et al., 2003)(Axelrod et al., 2014)(Fedorenko et al., 2013)
(Benedek et al., 2014; Bohrn et al., 2012; Rapp et al., 2012; Vartanian,2012)(Binder et al., 2009; Cappa, 2012)(Chertkow et al., 1997; Dronkers et al., 2004; Gow, 2012; Hillis and Car-amazza, 1991; Kertesz, 1982)(Binder et al., 2009)
hole (Friederici and Kotz, 2003; Newman et al., 2003)(Binder et al., 2009)(Booth et al., 2002; Gow, 2012)(Abutalebi et al., 2008; Abutalebi, Rosa, Tettamanti et al., 2009)(Wang and Holland, 2014)

J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126116
well as task accuracy into account, when participants were per-forming a semantic processing task. The following were the spe-cific questions addressed in the study:
(1) What is the relationship between task accuracy on a semanticprocessing task and percent signal change in left and righthemispheric language regions? Further, what is the relationshipbetween standardized test scores and percent signal change inleft and right hemispheric language regions? This analysis wasintended to demonstrate which regions were related to accu-rate task performance. We expected to see increased signalchange in frontal and temporal regions previously identified asregions of interest related to semantic processing demands, perthe Binder et al. (2009) review. Further, when participantsperformed the tasks accurately, we expected percent signalchange in these regions to be correspondingly higher.
(2) What is the relationship between the amount of damaged tis-sue and percent signal change within left and right hemisphereregions? This analysis intended to show which regions areassociated with greater percent signal change in response tolesioned tissue in the left hemisphere. We expected frontaland temporal regions to be damaged, and hence expected anegative relationship between spared tissue in these regionsand percent signal change in other regions in the left and righthemisphere, such that the greater the damage in frontal andtemporal language regions, the greater the activation in otherleft and right hemisphere regions.
(3) What is the relationship of percent signal change between re-gionswithin the left and right hemisphere for both patients andhealthy controls? In this analysis, we intended to investigatewhich regions show concurrent increased or decreased percentsignal change, indicating their function within a network. Wehypothesized that for normal controls positive relationshipswill emerge between our selected left hemisphere ROIs. Forpatients, specific regions in the frontal, temporal and parietallobe would be engaged as a network in the service of successfulbut residual semantic processing.
2. Materials and methods
2.1. Participants
Participants with aphasia were 14 persons (females¼ 4; agerange¼48�75 years) in the chronic recovery stage of aphasia as aresult of a left middle cerebral artery stroke. Their time post-stroke
Table 2Participant information. Participant demographic and testing information is summarizedscores from the CLQT provide composite severity.
ID Gender Age Time post-stroke Aphasia/stroke description
1 M 60;4 13;6 Wernicke's or Conduction2 M 59;3 2;0 Anomic or Transcortical Motor3 M 55;9 6;5 Conduction4 M 47;6 3;9 Anomic5 M 53;0 9;3 Broca's6 M 66;11 6;7 Broca's7 M 48;5 7;10 Broca's or Conduction8 F 66;9 1;8 Transcortical Motor9 F 57;2 3;7 N/A**10 M 69;2 1;4 Anomic11 M 66;1 2;2 Anomic12 M 74;6 11 months Transcortical Motor13 F 55;1 6 months Anomic14 F 63;1 8;2 ConductionAverages
75% M 59;7 5;11 ––
varied from 6 months to 13 years post-stroke, with an average of6 years' time post-stroke. All participants' native language wasEnglish and all were right-handed.
Each participant with aphasia was administered the WesternAphasia Battery- Revised, WAB-R Kertesz (2007), which assessesauditory comprehension, naming, fluency, repetition, reading, andwriting. From the WAB-R we also calculated each participant'sAphasia Quotient (range¼48–99.2), providing a severity rating andassisting in classification of participants into a range of syndromesincluding Wernicke's, Broca's, Transcortical Motor, Conduction, andAnomic Aphasias. Participants also completed the Boston NamingTest, 2nd edition BNT-2 (Kaplan et al., 2001) the mean score was 40out of 60 (range¼4–57). Additionally, they were administered the3-picture subtest of the Pyramids and Palm Trees, PAPT (Howard andPatterson, 1992), a test that examines non-verbal semantic proces-sing. This test generally suggested that participants' semantic sys-tems were fairly intact with a mean score of 49 out of 52(range¼39–51). In order to assess participants' cognition, they werealso administered the Cognitive Linguistic Quick Test, CLQT (Helm-Estabrooks, 2001), which elicited a composite severity score, asdetermined by combining measures of aspects of cognition per thetest manual; the great majority of participants were within normallimits, though one participant was severely impaired. The criteriafor inclusion were left hemisphere strokes and at least some sparedtissue in the LIFG. Based on these criteria, two additional partici-pants were not included in this data set as one had a right hemi-sphere stroke and another participant had no spared tissue in theLIFG. See Table 2 for a summary of participant data.
A group of healthy normal controls (N¼8, females¼5; agerange¼44–75 years) with no history of brain damage were re-cruited to obtain normative data on task-specific activation for thetwo tasks described below. Exclusionary criteria included neuro-logical disorders such as stroke, transient ischemic attacks, Par-kinson's disease, Alzheimer's disease, psychological illness, learn-ing disability, seizures and attention deficit disorders.
2.2. Tasks
fMRI data were acquired while participants completed in one oftwo semantic language tasks in English; normal controls were splitevenly between the two tasks. Participants 1, 5, 6, 8, 11, and 14performed a semantic feature verification task. Sixty-four picturestimuli, evenly distributed across two categories (birds, vege-tables) and typicality (typical, atypical), were used. Participantswere presented with a picture prime for one second and then thetarget stimulus (written phrase) for 4 s, for a total of 5 s , which
in this table. Aphasia quotient and syndromic diagnosis are provided by WAB. The
Aphasia quotient BNT PAPT CLQT Experiment
71.2 36 (60%) 49 (94.23%) Mild 178.6 50 (66.7%) 49 (94.23%) WNL 277.7 52 (86.7%) 51 (98.08%) WNL 295.5 57 (95%) 51 (98.08%) WNL 248 4 (6.7%) 45 (86.54%) Mild 149.6 9 (15%) 50 (96.15%) Mild 172.5 49 (81.7%) 47 (90.38%) Mild 282.2 50 (83.3%) 39 (75%) Severe 199.2 55 (91.7%) 50 (96.15%) WNL 297.1 57 (95%) 51 (98.1%) Mild 297.2 39 (65%) 48 (92.31%) Mild 167.4 55 (91.7%) 48 (92.31%) Mild 284.7 54 (90%) 51 (98.1%) WNL 253.4 9 (15%) 50 (96.15%) Mild 1
76.6 40 (68%) 49 (90.74%) –– 50-50

1 We initially considered utilizing functional ROIs, and tested functional ROIdefinition with a portion of our data. However, that resulted in great variability inpeak activation location across patients, thereby making it difficult to relate percentsignal change to structural damage defined in anatomical regions.
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126 117
was based on pilot data indicating that this was an adequateamount of time for patients to respond. For the experimentalcondition, these written phrases were comprised of semanticfeatures; through button press, participants indicated whether thefeature matched the picture. For the control condition, participantslooked a scrambled picture that was either black and white orcolor, with the written phrases “black and white” or “color” below;again using button press, participants indicated whether the colorstatement was true or false. All stimuli were balanced betweenbutton presses requiring the index finger and middle finger, andwere randomized, with each stimulus presentation preceded by afixation of a cross for a two or four second inter-stimulus interval(ISI) that was randomized.
Participants 2, 3, 4, 7, 9, 10, 12, and 13 performed a word re-latedness task. Stimuli were 100 written word pairs (experimentalcondition), split evenly between abstract and concrete words, and50 written nonword pairs (control condition). Each stimulus had aduration of 5 s, which was based on pilot data indicating that thiswas an adequate amount of time for patients to respond. For theexperimental condition, participants indicated whether the wordpairs were related or not using a button press. For the controlcondition, participants indicated whether paired nonwords werethe same or not, again by button press. The nonwords were ob-tained from the ARC nonword database (Rastle et al., 2002). Again,all stimuli were balanced between button presses requiring theindex finger and middle finger, and were randomized. Each sti-mulus presentation was preceded by a fixation cross of two, three,or four second duration as a randomized ISI. Stimuli for both taskswere nouns balanced for length, frequency of occurrence (CELEX,(Vanderwouden, 1990)), and familiarity (http://www.psy.uwa.edu.au/mrcdatabase/uwa_mrc.htm) (Coltheart, 1981).
While these tasks are unique, both tasks elicit the same se-mantic processing steps as pointed out by Binder and Desai (2011),Thompson-Schill et al. (1999), and Jefferies (2013). First, in bothtasks, words are read and comprehended. Second, semanticmeaning is extracted. Finally, this semantic meaning is processedand an appropriate decision made. Given the precedent for com-bining analyses of tasks that demand the same language functionsset by recent reviews (Binder and Desai, 2011; Turkeltaub et al.,2011), combining the analysis is valid for testing the hypothesesoutlined above. As a further confirmation, we ran follow-up dataanalyses with a partial correlation accounting for task.
2.3. Neuroimaging data collection
Scans for both tasks were performed at the Boston UniversityCenter for Biomedical Imaging using a 3 T Philips Acheiva MRIscanner. Structural T1 scans were taken with 140 sagittal slices,1 mm3 voxels, 240�240 matrix, FOV of 240 mm, flip angle of 8,fold-over direction of AP, TR of 8.2 ms, and TE of 3.8 ms. BOLD signalinformation was obtained using 31 axial slices (3 mm thick, 0.3 in-terslice gap), 3 mm3 voxels, 80�78 matrix, FOV of 240, a flip angleof 90, fold-over direction of AP, TR of 2000 ms and TE of 35 ms.
2.4. Behavioral data
Behavioral data from the tasks performed within the fMRI scannerwere used to calculate accuracy by dividing the number of correctresponses by the number of total stimulus presentations. Accuracywas calculated for both control and experimental conditions.
2.5. Lesion masking
Using structural T1 scan, lesion masks were manually drawn asvolume-of-interest files (VOIs) slice-by-slice within MRICRON(Rorden, 2012) for each participant. This was done on each slice of
the structural MRI for each participant, generating a binary VOI file.Next, a lesion mask was created by deleting regions covered by theVOI lesion file, generating a version of each participant’s brainwhere the lesion tissue was removed, as in Brett et al. (2002). In thiscase, the area within the lesion was given a binary intensity of 0.Then, a lesion map was created by preserving regions covered bythe VOI lesion file, generating a file containing only the lesionedtissue. In this case the area within the lesion was given a binaryintensity of 1 while the rest of the image was given a binary in-tensity of 0. This lesion map also was used to generate total lesionvolume using the descriptive statistics provided by MRICRON wheneach lesion map was overlaid onto a normalized brain template.
Reliability for lesion mapping was ensured by the authors ofthis study by performing a Dice analysis as suggested by Rehmet al. (2004), as a measure of similarity between lesion mapscreated by two of the authors. A Dice coefficient of 0 indicates nooverlap, while a Dice coefficient of 1 indicates complete overlap. ADice analysis was performed on lesion maps of 5 of the 14 parti-cipants as a confirmation for intra-rater reliability. Each of thesecomparisons revealed Dice indices of greater than 0.8, with anaverage of 0.88, indicating that the lesion maps hand-drawn by theauthors were consistent.
2.6. fMRI preprocessing
SPM8 (Friston et al., 2009) was used to preprocess the images.Slice timing was performed using functional images, which werereferenced to the middle slice. Realign, estimate, and re-slice wasperformed with registration to the mean slice and re-slice inter-polation with 4th degree B-Spline. Structural T1 scans were co-registered to the mean functional image. Segmentation was per-formed based on co-registered structural images into grey matter,white matter and CSF. A masking image (i.e., containing damagedand preserved tissue with assigned values of 0 and 1, respectively)was provided during segmentation so that the regions containinga value of zero would not contribute when estimating the varioussegmentation parameters. The images were then normalized forboth functional and structural scans. Lesion maps were also nor-malized separately with the same normalization parameters.
2.6.1. First level analysisStatistical analysis of functional data was performed by a mass-
univariate approach based on General Linear Models (GLM) inSPM8. Task timings (stimulus onsets and durations) were con-volved with the canonical hemodynamic response function (HRF)and its temporal derivative. The timings entered as onsets in theGLM were locked to the onset of each trial (prime). A high passfilter of 128 s was used. Motion parameters were included in themodel as regressors. The data were not smoothed in order to avoidinterpolation from nearby regions or CSF which might extend intothe boundaries of specific ROIs selected in this study (Meinzeret al., 2013).
2.7. ROI analysis
Given the variance across lesioned brains, we elected to utilizeanatomical ROIs that were based on evidence for ROIs reported forsemantic processing.1 Importantly, anatomically defined ROIs al-lowed for the examination of the relationship between theamount of signal change within a specific region and the amount

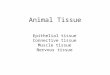
Fig. 1. Lesion overlap (n¼14).
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126118
of damage within that and other regions across patients.
2.7.1. Definition of structural ROIsAnatomical ROIs were selected using the AAL atlas within
Marsbar (Brett et al., 2002), a toolbox in SPM8. ROIs selected in-cluded the IFGorb, IFGtri, IFGop, MFG, SFG, MTG, combined an-gular and supramarginal gyri (AG/SMG), and the ACC. Each ROIwas registered to the template brain during the SPM8 unifiedsegmentation procedure, allowing the warping of each subject'smap from native to MNI space. We manually verified this as wellby overlaying the normalized map onto the normalized T1 to en-sure that the boundaries were precisely defined. The normalizedlesion map was then subtracted from each of these individual ROIsfor each participant. This yielded an ROI containing only thespared tissue for each region for each participant.
2.7.2. Analysis of structural ROIsWe then calculated the percentage of spared tissue within each
of these spared tissue ROIs in MRICRON. This was done by addingindividual, normalized spared tissue ROIs as an overlay to a nor-malized template. By generating the descriptive data for the im-age, we then derived the volume of the voxels in the spared tissueROIs in cubic centimeters. Based on the volume data taken fromtypical anatomical ROIs, the percent spared tissue within each ROIwas calculated by dividing the volume of the spared tissue ROI bythe typical anatomical ROI volume, thus yielding the percentage ofspared tissue in each ROI for each participant.
2.7.3. Extraction of percent signal change from ROIsFor each task, semantic feature t-statistic maps were calculated
in a first level GLM analysis (Section 2.6.1). Utilizing the ROItoolbox within Marsbar, the percent BOLD signal change for aspecified ROI was calculated for the semantic versus control con-dition. The event duration for each condition was taken into ac-count in this calculation. This process was repeated for each ROI,for both patients and controls.
2.8. Statistical analysis
First, a Principal Component Analysis (PCA) was performed as apreliminary tool to explore the structure in the correlationamong the percent spared tissue outcomes. This structure wasthen used to build multivariate models to allow for outcome-specific fixed effects and participant-specific and structure-specificrandom effects. Then, multivariate mixed-effects linear regressionanalyses were used to test for significant associations betweenpercent spared tissue and percent signal changes.
Additionally, to examine the extent to which total lesion vo-lume predicted BOLD signal change in the right hemisphere, linearregressions were performed. Partial Pearson correlations ac-counting for task type examined the relationships between task
accuracy and percent spared tissue/signal change, demographicand testing information and percent spared tissue/signal change,and the relationships between signal change across regions forboth normal controls and patients.
3. Results
3.1. Lesion overlap
Across patient participants, the most damage occurred in LIF-Gop, which was damaged in 13 of 14 participants, with an averageof 38% spared tissue. Anteriorly, LIFGtri also showed extensivedamage in 13 of 14 participants with an average of 55% sparedtissue. Posteriorly, all participants showed damage in LMTG(average 55% spared) and LAG/SMG (average 52% spared). LMFG(average 77% spared) and LIFGorb (average 77% spared) were re-latively spared. LSFG (92% spared) and LACC (average of 98%spared) were not lesioned in most participants. See Table 3 andFig. 1 for a summary of damage within regions for each participant.
3.2. Task accuracy and signal change
Based on a paired t-test across participants, control conditionaccuracy (mean 88% accuracy, SD of 26%) was significantly higherthan experimental, semantic processing task accuracy (mean 75%accuracy, SD of 18%, Task 1 average accuracy 76%, Task 2 averageaccuracy 74%), (t (13)¼�3.62, po0.003), indicating that for pa-tients, semantic processing was more demanding than the controlconditions. Task accuracy significantly correlated with signalchange in LIFGop (r¼0.54, pr0.05) and LIFGtri (r¼0.54, pr0.05),suggesting that LIFGop and LIFGtri were associated with higheraccuracy on the semantic processing task. Additionally, correla-tions between task accuracy and lesion extents were performed;however, they did not yield significant correlations.
3.3. Demographic and testing correlations
To examine the relationship between language impairment (asmeasured by the WAB-R, BNT-2, and PAPT), spared tissue, andpercent signal change, we examined Pearson correlations betweentest scores on the WAB-R, BNT-2, and PAPT and the amount ofspared tissue, BOLD signal change, and experimental task accuracy.We used the Aphasia Quotient (AQ) from the WAB-R, a score re-flecting overall language severity of aphasia across language tasks.This revealed significant positive correlations between the WAB-RAQ and amount of spared tissue in LIFGorb (r¼0.61, pr0.05), inthe LMTG (r¼0.74, pr0.05), and in the LAG/SMG (r¼0.56,pr0.05), indicating that less severe language impairment (thehigher the AQ) was associated with greater sparing of tissue inLIFGorb, LMTG, and LAG/SMG.

Table 3Percent spared tissue in ROIs in the left hemisphere for each participant. The numbers in the following table represent the percent spared tissue within each region for eachparticipant. Darker shading implies greater damage, and thus less percent spared.
Participants1 2 3 4 5 6 7 8 9 10 11 12 13 14 Averages
Regions LIFGop 21 3 46 51 6 94 4 18 6 100 74 21 56 38 38LIFGorb 46 93 85 85 52 81 31 96 88 100 100 90 97 34 77LIFGtri 28 10 85 73 15 99 13 48 48 100 72 42 70 68 55LMFG 78 55 62 99 35 100 66 40 90 100 93 57 99 99 77LSFG 99 98 99 100 72 100 85 83 100 100 95 57 100 100 92LMTG 5 72 13 86 31 1 5 91 96 99 92 93 87 1 55LAG/SMG 14 31 75 78 24 58 1 41 59 88 91 84 73 4 52LACC 96 100 100 100 100 100 99 94 100 100 100 80 100 100 98
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126 119
Using the total number of correctly named pictures from theBNT-2, the amount of spared tissue in LIFGorb correlated positivelywith the number of correctly named pictures (r¼0.53, pr0.05), asdid the amount of spared tissue in LMTG (r¼0.64, pr0.05) and inLAG/SMG (r¼0.51, pr0.05), suggesting that the greater theamount of spared tissue in these regions, the more pictures werenamed correctly.
For the PAPT, a non-verbal semantic processing task, accuracycorrelated positively with the amount of spared tissue in the LMFG(r¼0.72, pr0.05, pr0.05) and LSFG (r¼0.52, pr0.05), suggest-ing that the more spared tissue in this region, the better semanticprocessing. Additionally, PAPT score correlated positively withexperimental accuracy on our semantic processing tasks (r¼0.76,pr0.05).
We calculated correlations between percent BOLD signalchange and standardized test scores; however, these did not yieldsignificant results. We chose not to examine the correlations be-tween age and time post-stroke, as our data were more weightedtowards older adults who were several months post their strokeonset.
3.4. Percent spared tissue and percent signal change
3.4.1. Principal Component Analysis (PCA) resultsA PCA was used as an exploratory analysis to examine the re-
lationship between percent spared tissue and percent signalchange. Moreover, groupings seen within the PCA were utilized inadditional analyses (see Section 3.4.2). A scree plot was used todetermine the possible number of factors underlying these com-ponents as well as the Kaiser criterion of eigenvalues greater than1.00. Based on a varimax normalized matrix, 13 factors wereconsidered factors of interest, the first four of which explained79.6% of the variance in the data (See Table 4). Structures withscores greater than 0.5 were assigned to each factor. The positivecomponents within factor 1 consisted of the amount of sparedtissue in LIFGorb, LMTG, and LAG/SMG. Negative components offactor 1 included percent signal change in LMFG, LSFG, RIFGop,RIFGtri, RMFG, RSFG, RMTG, RAG/SMG, and RACC, along with tis-sue in LACC, LIFGop signal change, and accuracy within the controlcondition. It should be pointed out that all of the RH contralesionalregions' signal change emerged in this factor, except for RIFGorb,which notably did not appear in this factor. Within factor 2, allcomponents were positive and included the amount of sparedtissue in LIFGop, LIFGtri, LMFG, LSFG, and LACC. Factor 3 includedpositive components of percent spared tissue in LIFGorb and signalchange from LIFGop and LIFGtri. Negative components for factor3 included signal change from LACC and RIFGorb. Finally, factor4 positive components included signal change from LIFGorb andLMTG. The only negative component in factor 4 was signal changefrom RAG/SMG.
3.4.2. Multivariate models resultsWe structured our multivariate models based on the results of
our PCA analysis. Outcomes of percent spared for each participantwere correlated using a single between-outcome correlation byapplying a compound-symmetry model for the covariance matrix.Hence, two levels of correlations were modeled in the outcomes: i)correlations of all percent spared tissue from the same patientsand ii) correlations of all percent signal change from the samestructure (e.g., LIFGop % signal, LIFGtri % signal, LMTG % signal,LACC % signal, and RIFGorb % signal are assigned to the same factoras indicated by the PCA). These multivariate analyses are morerealistic models of the outcomes than using independent regres-sion models for each outcome. Since all information within eachparticipant was utilized, we were able to provide more inter-pretable and consistent results than simpler statistical models.Moreover, the problem of multiple comparisons is removed whenusing these models (Gelman et al., 2012). These multivariatemodels provide higher power for detecting small but clinicallyimportant differences compared to independent regression mod-els for each outcome (Goldstein, 2010)
Table 5 indicates t-values for the positive and negative corre-lations. T-values greater than 2.28 are significant after correctionfor multiple comparisons (Benjamini and Hochberg, 1995). Bothnegative and positive correlations were found. Positive correla-tions imply that the greater the amount of spared tissue, thehigher the BOLD signal change (or the lower the amount of da-maged tissue, the lower the BOLD signal change). Positive corre-lations were observed between the amount of spared tissue inLSFG with percent signal change in LIFGop, LIFGorb, LIFGtri, RIF-Gop, and RIFGtri. The amount of spared tissue in LACC was posi-tively correlated with percent signal change in all ROIs that wereexamined.
Conversely, negative correlations imply that the lower theamount of spared tissue, the higher the BOLD signal change (or thehigher the amount of spared tissue, the lower the BOLD signalchange). Negative correlations were observed between (a) theamount of spared tissue in LIFGorb and percent signal change inLACC signal; (b) the amount of spared tissue in LMTG and percentsignal change in LACC and LSFG; and (c) the amount of sparedtissue in LAG/SMG and percent signal change in bilateral anteriorregions including LACC, LMFG, LSFG, RACC, and RSFG. The amountof spared tissue in LIFGop, LIFGtri, and LMFG did not correlate withsignal change in any of the other ROIs in either hemisphere.
3.4.3. Lesion volume and right hemisphere BOLD signal resultsTo examine the extent to which right hemisphere BOLD signal
change was driven by the total lesion volume in the LH, 8 linearregressions were completed. Only two regressions (i.e., ROIs) weresignificant; (a) total lesion volume predicted percent BOLD signalchange in RMTG (R2 ¼0.29, F(1, 12) ¼5.09, po0.05, β¼ 0.54) and(b) total lesion volume predicted percent BOLD signal change in

Table 4Principal components analysis factors. Percentage values for each factor reflect the individual percent variation explained by that factor; scores of interest are marked in boldand shaded boxes.a Together, these factors explain 79.6% of the variance. *supplemental factor.
Factor 1 Positive: Tra-ditional language re-gions Negative: Com-pensatory regions36.5%
Factor 2 Traditionallanguage regions 17.6%
Factor 3 Positive: Pri-mary semantic proces-sing regions Negative:Outliers 13.7%
Factor 4: Secondarysemantic processingregions 11.7%
Amount of sparedtissue
LIFGop percent spared 0.30 0.79 0.23 0.16LIFGorb percent spared 0.59 0.20 0.58 �0.29LIFGtri percent spared 0.41 0.81 0.19 0.21LMFG percent spared 0.07 0.68 0.35 0.27LSFG percent spared �0.49 0.57 0.48 0.17LMTG percent spared 0.60 0.01 0.37 �0.47LAG/SMG percentspared
0.68 0.42 0.33 �0.07
LACC percent spared �0.63 0.59 0.25 �0.05Ipsilesional BOLDsignal change
LIFGop signal change �0.58 �0.23 0.72 0.07LIFGorb signal change �0.33 �0.43 0.15 0.68LIFGtri signal change �0.43 �0.44 0.51 0.49LMFG signal change �0.85 �0.07 0.12 0.24LSFG signal change �0.78 0.12 �0.11 0.40LMTG signal change �0.34 0.19 0.15 0.65LAG/SMG signalchange
�0.32 0.12 0.03 0.39
LACC signal change �0.50 0.49 �0.62 �0.06Contralesional BOLDsignal change
RIFGop signal change �0.85 0.15 0.23 �0.35RIFGorb signal change �0.06 0.68 �0.61 0.03RIFGtri signal change �0.85 0.02 0.30 �0.22RMFG signal change �0.82 0.26 0.22 �0.44RSFG signal change �0.84 0.17 �0.03 �0.31RMTG signal change �0.71 �0.25 �0.08 �0.12RAG/SMG signalchange
�0.63 �0.28 0.03 �0.54
RACC signal change �0.71 0.35 �0.32 �0.25Accuracy Experimental task
accuracy*�0.39 0.23 0.48 0.39
Control conditionaccuracy*
�0.52 0.33 0.28 0.19
a Of note, some structures scored greater than 0.5 in multiple factors. In these cases we assigned structures to the factor for which they had the highest score.
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126120
RAG/SMG (R2¼0.33, F (1, 12) ¼6.06, po0.05, β¼0.57).
3.5. Percent signal change among regions
To understand how percent signal change was affected acrossregions, a Pearson partial correlation matrix was calculated usingthe percent signal change data for both patients and normalcontrols.
3.5.1. Pearson partial correlation matrix results for controlsFor controls, after accounting for task as a covariate, almost all
correlations between regions were positive (see Table 6A, Fig. 3).Specifically, LIFGop, LIFGorb, and LIFGtri were found to be correlatedpositively with one another, suggesting that they work as a unit.Additionally, all LIFG regions were found to correlate positively withLAG/SMG, suggesting anterior to posterior connections within theleft hemisphere. Other LH regions were also correlated with eachother including LSFG and LAG/SMG, LMFG and LIFG, and LACC andLIFG/LMFG. Interestingly, several cross-hemispheric correlationswere also significant: RSFG and LMTG, RIFGorb and LAG/SMG, RMTGand LAG/SMG, LIFG and RIFG, and LMTG and RMTG.
3.5.2. Pearson partial correlation matrix results for patientsThe most striking differences in the correlation matrices be-
tween the controls and the patients is that while correlations forcontrols were mostly all positive, several positive and negativecorrelations emerged for the patients (see Table 6B, Fig. 3). Like thecontrols, LIFGop, LIFGorb, and LIFGtri were found to be correlated
positively with one another for the patient group. Additionally,LIFGorb was found to correlate positively with LMTG, again sug-gesting anterior to posterior connections within the lefthemisphere.
The correlation matrix also revealed many positive correlationswithin right hemisphere regions, including RIFGop, RIFGtri, RMFG,RMTG, and RAG/SMG. Additionally, percent signal change in bothRSFG and RMFG correlated positively with 6 of 8 other RH regionsand RIFGop correlated positively with 5 of the 8 other RH regions.Of interest, RIFGorb stood out as the only region to demonstratenegative correlations, correlating negatively with LIFGop andLIFGtri. Several regions also demonstrated positive cross-hemi-sphere correlations between homologues, including LIFGop andRIFGop, LMFG and RMFG, LSFG and RMFG, and LACC and RACC.
4. Discussion
The overall goal of our study was to examine the contributionof spared tissue in the recovered language network in patientswith aphasia. Specifically, we sought to (1) assess the relationshipbetween task accuracy and percent signal change in left and rightlanguage ROIs, and to examine the relationship between testscores and percent signal change, testing the hypothesis that in-creased signal change in LH frontal and temporal regions would becorrelated with increased task accuracy; (2) analyze the relation-ship between the amount of damaged tissue and percent signalchange in ROIs, testing the hypothesis that greater damage in

Table 5Significant percent spared to percent signal change correlations with task as a covariate. Positive correlations indicate that the less percent spared, the less the signal change(more damage, less signal). Negative correlations indicate that the more percent spared, the less the signal change (more damage, more signal). Numbers bolded aresignificant and reflect t-values for the positive and negative correlations.
Predictor LeftIFGtri % signal
LeftIFGop % signal
RightIFGop % signal
RightIFGtri % signal
LeftIFGorb % signal
RightMTG % signal
RightAngSMG % signal
RightIFGorb % signal
LeftMTG % signal
RightMFG % signal
LeftAngSMG % signal
LeftMFG % signal
RightSFG % signal
RightAntCing % signal
LeftSFG % signal
LeftAntCing % signal
L AntCing% spar
3.65 3.60 3.46 3.42 3.42 3.36 3.28 3.21 3.20 3.25 3.08 3.11 3.10 3.04 3.03 2.89
LSFG % spared 3.43 3.36 3.01 2.93 2.92 2.74 2.57 2.41 2.40 2.55 2.12 2.21 2.17 2.04 2.01 1.69L MFG % spared 1.38 1.18 0.71 0.52 0.48 0.32 0.00 -0.04 -0.14 -0.04 -0.57 -0.54 -0.60 -0.78 -0.84 -1.31L IFGop% spared 1.00 0.72 0.40 0.07 -0.52 -0.51 -0.67 0.05 -0.63 -0.56 -1.25 -1.49 -1.53 -1.52 -1.62 -1.88L IFGtri % spar 0.40 0.26 -0.26 -0.66 -0.88 -0.80 -1.11 -0.71 -1.18 -1.20 -1.91 -1.90 -1.93 -2.00 -2.07 -2.69L IFGorb % spar -0.25 -0.34 -1.09 -1.32 -1.37 -1.43 -1.68 -2.00 -1.99 -1.87 -2.68 -2.51 -2.50 -2.66 -2.83 -3.44L MTG % spared 0.23 0.43 -0.59 -1.05 -1.21 -0.92 -1.18 -1.53 -1.64 -1.68 -2.69 -2.91 -2.51 -2.61 -3.29 -3.71L AngSMG % spar 0.05 -0.31 -1.05 -1.56 -1.62 -1.30 -1.73 -1.59 -1.81 -2.11 -2.70 -2.83 -2.78 -2.78 -3.12 -3.78
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126 121
frontal and temporal regions would be negatively correlated withsignal change in those areas, and that greater damage to theseregions would be correlated with percent signal change in RHhomologues as well as undamaged LH ROIs; and finally, (3) eval-uate the relationship between percent signal change across re-gions, for both patients and controls anticipating that we wouldfind positive correlations between the percent signal change infrontal, temporal, and parietal regions in the left and right hemi-spheres for both groups.
Before providing an interpretation of the patient results, let usfirst examine percent signal change relationships between ROIs forthe healthy controls. The Pearson partial correlation matrix forcontrols revealed that subregions within LIFG (triangularis, oper-cularis and orbitalis) were highly correlated with each other andfunctioned as a unit. Predominantly positive correlations wereobserved between LH ROIs within the same hemisphere (LIFG,LAG, LMFG, and LSFG), RH ROIs within the same hemisphere (RIFG,RMTG, RAG, RSFG) and cross-hemispheric ROIs (LIFG–RIFG;LMTG–RMTG; LMTG–RSFG; LAG/SMG–RIFG, LAG/SMG–RIFG).These controls represent the normal 'optimal’ relationship be-tween ROIs within- and across-hemispheres in the absence of anydamage to the left hemisphere. In contrast, when we examine theeffects of lesion on this language network, several interestingfindings emerge.
In persons with aphasia, we found that while the LIFG andLMTG were the most damaged ROIs in our population, these werealso important regions associated with successful semantic pro-cessing during the fMRI task as well as on standardized languageassessments. First, task accuracy was significantly correlated withpercent signal change in LIFGop and LIFGtri. Second, the moredamage to these regions, the higher the percent signal change inLACC and LSFG. And, the less the damage to LSFG and LACC, themore the percent signal change in LH ROIs and RH ROIs includingRSFG, RMFG, RACC, RIFGtri, and RIFGop.
Third, the negative correlations between percent spared tissueand percent signal change were very informative as they indicatedwhich ROIs exhibited high percent signal change relative to lesionsin specific LH ROIs. As noted above, the amount of spared tissue inLIFGorb and LMTG was positively correlated with the amount ofsignal change in LACC and LSFG; however, the amount of sparedtissue in LAG/SMG was also negatively correlated with the percentsignal change in several LH frontal regions, including LMFG, LSFG,and LACC, as well as RH anterior regions, including RSFG and RACC(see Fig. 2).
Fourth, even though our methods segregated the subregions ofthe inferior frontal gyrus into triangularis, orbitalis and oper-cularis, these regions emerged as a cluster of correlated signalchange in both patients and controls. Other ROIs that exhibitedcorrelated percent signal change included RH ROIs comprising IFG,MTG and AG/SMG (see Fig. 3) and cross-hemispheric homologues
(LIFGop–RIFGop, LMFG–RMFG, LSFG–RMFG, and LACC–RACC) (seeTable 6). Interestingly, RIFGorb appears to be isolated from the restof the right hemisphere, and only correlated positively with LACCand correlated negatively with LIFGop and LIFGtri.
We will discuss each of these results in further detail in thecontext of our research questions.
4.1. Task accuracy and percent signal change
In terms of accuracy correlations, we found that task accuracyis significantly correlated with signal in LIFGop and LIFGtri, sug-gesting that the more accurate participants were on a task, thestronger the signal in LIFGop and LIFGtri. This is intuitive, as theseregions are typically responsible for semantic processing (Ruffet al., 2008), and, thus, should be more effective at completing asemantic processing task (see Table 1 for literature supportingthese regions' involvement in semantic processing).
4.2. Language impairment and spared tissue
We found several notable relationships between language im-pairment and the amount of spared tissue, BOLD signal change,and experimental task accuracy. First, severity of aphasia (asmeasured by AQ from WAB-R) and better picture naming (asmeasured by the BNT-2) were correlated with the amount ofspared tissue in LIFGorb, LMTG, and LAG/SMG, such that less se-vere aphasia was linked with more spared tissue in these tradi-tional language regions. These results are consistent with recentVLSM studies highlighting the role of traditional language regionsin language impairment (Dronkers et al., 2004) and reinforce theimportance of these regions for processing language in generaland for semantic processing in particular.
Furthermore, we found that the amount of spared tissue withinLMFG and LSFG regions was related to non-verbal semantic pro-cessing (as measured by the PAPT). These findings are consistentwith studies that have indicated that SFG and MFG are involved insemantic processing (Binder et al., 2009). Alternately, Fedorenkoet al. (2013) found that in typical brains, a set of regions in thefrontal and parietal lobes, including MFG, are activated acrossdomains and tasks, from arithmetic, to working memory, to fil-tering. Additionally, the more challenging a task, regardless ofdomain, the greater the demand on these regions (Fedorenkoet al., 2013). It is feasible that provided our participants' level ofaphasia, our semantic processing task might be quite challenging,resulting in greater engagement of these frontal and parietal re-gions. This is further supported by a recent meta-analysis studyfrom Geranmayeh et al. (2014), which suggests that there aredomain-general systems that enable cognitive control and atten-tion. These systems would likely be highly necessary given thelevel of difficulty of our task for patients with aphasia; yet those

Table 6Significant correlations of signal change across regions with task as a covariate for (A) controls and (B) patients. Within this table, each region is listed with its significant correlations with other regions, controlling for task. A scale isgiven explaining the heat map design of the table. Numbers bolded are significant.
A LIFGop RIFGop LIFGorb RIFGorb LIFGtri RIFGtri LMFG RMFG LSFG RSFG LMTG RMTG LAG+Supra RAG+Supra LACC RACCLIFGop 1.00 0.66 0.78 0.72 0.89 0.35 0.86 0.47 0.61 0.28 0.33 0.41 0.81 0.25 0.70 0.62RIFGop 0.66 1.00 0.66 0.64 0.77 0.58 0.50 0.42 -0.04 0.05 0.27 0.31 0.47 0.43 0.40 0.17LIFGorb 0.78 0.66 1.00 0.94 0.92 0.49 0.83 0.64 0.57 0.55 0.53 0.64 0.86 0.55 0.92 0.72RIFGorb 0.72 0.64 0.94 1.00 0.84 0.52 0.82 0.68 0.59 0.73 0.75 0.82 0.87 0.77 0.81 0.62LIFGtri 0.89 0.77 0.92 0.84 1.00 0.65 0.91 0.57 0.42 0.35 0.32 0.41 0.73 0.40 0.85 0.72RIFGtri 0.35 0.58 0.49 0.52 0.65 1.00 0.51 0.62 -0.20 0.34 0.07 0.14 0.11 0.41 0.46 0.30LMFG 0.86 0.50 0.83 0.82 0.91 0.51 1.00 0.42 0.63 0.48 0.44 0.45 0.74 0.45 0.86 0.88RMFG 0.47 0.42 0.64 0.68 0.57 0.62 0.42 1.00 0.32 0.71 0.37 0.61 0.56 0.45 0.54 0.19LSFG 0.61 -0.04 0.57 0.59 0.42 -0.20 0.63 0.32 1.00 0.60 0.59 0.64 0.85 0.28 0.62 0.64RSFG 0.28 0.05 0.55 0.73 0.35 0.34 0.48 0.71 0.60 1.00 0.79 0.87 0.61 0.77 0.50 0.36LMTG 0.33 0.27 0.53 0.75 0.32 0.07 0.44 0.37 0.59 0.79 1.00 0.95 0.70 0.91 0.34 0.25RMTG 0.41 0.31 0.64 0.82 0.41 0.14 0.45 0.61 0.64 0.87 0.95 1.00 0.80 0.85 0.45 0.25LAG/SMG 0.81 0.47 0.86 0.87 0.73 0.11 0.74 0.56 0.85 0.61 0.70 0.80 1.00 0.52 0.75 0.60RAG/SMG 0.25 0.43 0.55 0.77 0.40 0.41 0.45 0.45 0.28 0.77 0.91 0.85 0.35 0.22LACC 0.70 0.40 0.92 0.81 0.85 0.46 0.86 0.54 0.62 0.50 0.34 0.45 0.75 0.35 1.00 0.89RACC 0.62 0.17 0.72 0.62 0.72 0.30 0.88 0.19 0.64 0.36 0.25 0.25 0.60 0.22 0.89 1.00
B LIFGop RIFGop LIFGorb RIFGorb LIFGtri RIFGtri LMFG RMFG LSFG RSFG LMTG RMTG LAG+Supra RAG+Supra LACC RACCLIFGop 1 0.55 0.38 -0.51 0.73 0.62 0.6 0.53 0.42 0.44 0.34 0.41 -0.35 0.4 -0.24 0.03RIFGop 0.55 1 0.09 -0.07 0.25 0.92 0.59 0.93 0.44 0.77 0.08 0.52 0.13 0.78 0.4 0.67LIFGorb 0.38 0.09 1 -0.37 0.67 0.27 0.34 -0.12 0.34 -0.13 0.57 0.17 0.36 0.04 -0.11 -0.1RIFGorb -0.51 -0.07 -0.37 1 -0.59 -0.11 -0.07 0.11 0.16 0.18 0.18 0.04 0.33 -0.29 0.73 0.42LIFGtri 0.73 0.25 0.67 -0.59 1 0.43 0.67 0.16 0.4 0.11 0.38 0.3 0.09 0.19 -0.37 -0.11RIFGtri 0.62 0.92 0.27 -0.11 0.43 1 0.61 0.87 0.4 0.61 0.14 0.54 0.12 0.73 0.31 0.52LMFG 0.6 0.59 0.34 -0.07 0.67 0.61 1 0.63 0.86 0.73 0.4 0.61 0.26 0.33 0.23 0.57RMFG 0.53 0.93 -0.12 0.11 0.16 0.87 0.63 1 0.46 0.86 0.08 0.56 0.01 0.67 0.43 0.73LSFG 0.42 0.44 0.34 0.16 0.4 0.4 0.86 0.46 1 0.67 0.49 0.45 0.3 0.14 0.48 0.57RSFG 0.44 0.77 -0.13 0.18 0.11 0.61 0.73 0.86 0.67 1 0.21 0.67 0.1 0.53 0.49 0.81LMTG 0.34 0.08 0.57 0.18 0.38 0.14 0.4 0.08 0.49 0.21 1 0.24 0.32 -0.3 0.16 0.2RMTG 0.41 0.52 0.17 0.04 0.3 0.54 0.61 0.56 0.45 0.67 0.24 1 0.18 0.49 0.29 0.38LAG/SMG -0.35 0.13 0.36 0.33 0.09 0.12 0.26 0.01 0.3 0.1 0.32 0.18 1 0.12 0.56 0.47RAG/SMG 0.4 0.78 0.04 -0.29 0.19 0.73 0.33 0.67 0.14 0.53 -0.3 0.49 0.12 1 0.28 0.41LACC -0.24 0.4 -0.11 0.73 -0.37 0.31 0.23 0.43 0.48 0.49 0.16 0.29 0.56 0.28 1 0.71RACC 0.03 0.67 -0.1 0.42 -0.11 0.52 0.57 0.73 0.57 0.81 0.2 0.38 0.47 0.41 0.71 1
1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 -0.1 -0.2 -0.3 -0.4 -0.5 -0.6 -0.7 -0.8 -0.9 -1
J.A.Sim
set
al./Neuropsychologia
84(2016)
113–126
122

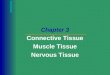
Fig. 2. Correlations between spared tissue and signal change. This diagram summarizes the spared to signal correlations. The region that an arrow originates from is thepercent spared tissue region; the region that the arrow terminates at is the region showing signal change. Note labels for positive versus negative correlations.
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126 123
domain-general systems may in fact be damaged, further com-plicating task accuracy for patients.
4.3. Spared tissue and signal change
Based on the PCA and our combined findings from the multi-variate analysis, two major findings emerge. First, it appears thatwhen the anterior regions of LSFG and LACC were more spared,more bilateral anterior signal change was observed. Additionally,LACC emerged as the sole region to have its percent spared tissuecorrelate positively with signal change in every other region. Thissuggests that LSFG and LACC may perform some sort of co-ordinating or regulatory role within the language network, con-sistent with other work in our laboratory (Kiran et al., 2015;Sandberg et al., 2015).
Second, it appeared that the more damage there was in pos-terior regions including LMTG and LAG/SMG, the more activationthere was in anterior bilateral SFG, ACC regions and LMFG. Al-though not significant, similar trends were observed for LIFGsubregions, indicating that anterior frontal regions were engagedas a supportive/compensatory network as a function of the degreeof damage to the LIFG and MTG and LAG/SMG regions. Taken to-gether with the findings of correlations between task accuracy andspared tissue in LIFG, these results suggest that while compensa-tory activation may occur, these compensatory regions were notnearly as effective as traditional language regions such as LIFG.
4.4. Lesion volume and right hemisphere signal change
Total left hemisphere lesion volume predicted signal change intwo RH ROIs, RMTG and RAG/SMG, such that the greater the lesionvolume in LH, the greater the signal change in these regions. Theseresults are similar to results from Turkeltaub et. al (2011), whichalso showed that greater damage in the left hemisphere wascoupled with more activation in RMTG. This is suggestive of pos-sible RH activation in response to greater LH damage, although theresults of the present study do not provide a confirmatory answeras to whether this mechanism serves a compensatory function or a
reorganization function.
4.5. Signal change relationships across regions
The signal change relationships across regions and groups al-lowed for several important observations. While the normal con-trols showed mostly positive correlations between ROIs, patientsshowed both positive and negative correlations. For both groups,LIFG semantic processing regions (LIFGop, LIFGorb, and LIFGtri)were correlated positively with one another. Additionally, RHhomologues (RIFGop, RIFGtri, RMFG, RMTG, and RAG/SMG) cor-related positively with one another for the patients, but for con-trols these regions were correlated with left hemisphere regions.Finally, cross hemispheric correlations were observed more forcontrols whereas right hemisphere correlations were more forpatients.
The only region that displayed negative correlations was RIF-Gorb with regions such as RIFGtri and LIFGop and positively cor-related with LACC. We see this same isolation of RIFGorb in ourpercent spared to signal change results. Given the ACC’s role inmonitoring language processing, it is possible that RIFGorb workswith LACC in this function. This will be discussed in greater detailbelow.
An interesting observation in the percent signal change corre-lation analysis was that RMFG was the hub of several positivecorrelations only for the patients (but not controls) as it was cor-related with 8 other ROIs ( LIFGop, RIFGop, RIFGtri, LMFG, RSFG,RMTG, RAG/SMG, and RACC). While the precise role of the RMFGin this study is unclear, it is worth pointing out that in a separatestudy examining changes in task-based effective connectivity afterrehabilitation in patients with aphasia, the connections betweenRIFG and MFG were the most modulated across patients (Kiranet al., 2015). These results highlight the potentially regulatory roleof the right frontal regions during language recovery, and futurework needs to explore this possibility in greater detail.

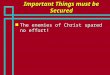
Fig. 3. Signal correlations across regions. This diagram summarizes signal-to-signal correlations across regions, both for normal controls and for patients. Note labels forpositive versus negative correlations.
J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126124
4.6. The isolation of RIFGorb
In the patient data, the question of RIFGorb's role raises inter-esting questions. RIFGorb and LACC are the only two negativecomponents within Factor 3. Within LIFG, the subregions emergedas one unit based on correlation results; however, subregions inthe RIFG do not display this pattern, due to RIFGorb's seemingisolation. RIFG has been implicated in monitoring and attention(Stuss and Alexander, 2007); however, based on recent researchfrom Aron et al. (2014), it appears that RIFG may not be solelyresponsible for monitoring and attention, but is also likely in-volved in inhibitory breaking, both in terms of complete stoppingof an action and of pausing an action. It should be noted, however,that the work of Aron et al. (2014) refers to the RIFG in general,while our research implicates RIFGorb only. The involvement ofRIFGorb in an inhibitory, breaking function could explain our
findings of negative relationships between RIFGorb signal changeand signal change in LIFGop and RIFGtri – perhaps was acting asan inhibitor of these regions.
An alternate, but not opposing view, is that RIFGorb and bi-lateral ACC form a monitoring network that inhibits actions asneeded. Signal change in RIFGorb correlated positively with LACC,which in turn correlated positively in terms of signal change withits contralateral homologue, RACC. Additionally, the percentspared tissue in LACC correlated positively with bilateral signalchange in all regions; it was the only region to correlate with allother regions' signal change, again suggesting a potential reg-ulatory role. Given the regulatory processes that ACC appears toparticipate in, studies on RIFGorb’s participation in monitoring,and our data as summarized here, it is possible that these regionsform a monitoring network. These results are speculative at thispoint, and future work needs to be done to identify the precise

J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126 125
relationships between RIFGorb, ACC, and other language regions inthe brain during language processing tasks.
4.7. Limitations of the study
As discussed in the introduction, we intentionally selected adiverse group of patients and healthy controls that had partici-pated in two semantic processing tasks. Additionally, the correla-tions for the healthy controls were very similar to the patients,with some important differences and lend further support to ourconclusions. Nonetheless, we cannot rule out the possibility thateven though the tasks engaged the same type of semantic pro-cessing abilities, they may not have evoked the same magnitude ofBOLD signal change across the ROIs we examined to the samedegree. Additionally, these subtle differences may have been evenmore pronounced with differing lesion sites and behavioral lan-guage impairment profiles. Future work needs to examine a largerand more homogenous sample of patients (constrained either bylesion site or behavioral profile) to carefully examine the degree ofactivation in specific regions. Such work is currently ongoing inour lab.
5. Conclusions
Taken as a whole, our results concerning task accuracy, sparedtissue, and percent BOLD signal change suggest a nuanced re-lationship between damaged regions and signal change in otherregions. Our findings are in line with previous research that sug-gests that recovery of function in left language regions and acti-vation of ipsilesional, left hemisphere tissue is essential for re-covery, though some recovery may involve recruitment of areas inthe right hemisphere as well. Indeed, these right hemisphere re-gions show extensive positive signal change correlations with eachother, with the exception of RIFGorb. RIFGorb stands out as iso-lated amongst right hemisphere regions, appearing to be part of apotentially regulatory network involving bilateral ACC.
Acknowledgments
This research was supported by the National Institute onDeafness and Other Communication Disorders/National Instituteof Health grants to Swathi Kiran (Grant number 1K18DC011517-01) and to Chaleece Sandberg (Grant number 5F31DC011220).
References
Abutalebi, J., Annoni, J.M., Zimine, I., Pegna, A.J., Seghier, M.L., Lee-Jahnke, H.,Khateb, A., 2008. Language control and lexical competition in bilinguals: anevent-related FMRI study. Cereb. Cortex 18 (7), 1496–1505. http://dx.doi.org/10.1093/cercor/bhm182.
Abutalebi, J., Rosa, P.A., Tettamanti, M., Green, D.W., Cappa, S.F., 2009. Bilingualaphasia and language control: a follow-up fMRI and intrinsic connectivitystudy. Brain Lang. 109 (2–3), 141–156. http://dx.doi.org/10.1016/j.bandl.2009.03.003.
Allendorfer, J.B., Kissela, B.M., Holland, S.K., Szaflarski, J.P., 2012. Different patternsof language activation in post-stroke aphasia are detected by overt and covertversions of the verb generation fMRI task. Med. Sci. Monit. 18 (3),CR135–CR137.
Arévalo, A.L., Baldo, J.V., Dronkers, N.F., 2012. What do brain lesions tell us abouttheories of embodied semantics and the human mirror neuron system? Cortex48 (2), 242–254. http://dx.doi.org/10.1016/j.cortex.2010.06.001.
Aron, A.R., Robbins, T.W., Poldrack, R.A., 2014. Inhibition and the right inferiorfrontal cortex: one decade on. Trends Cogn. Sci. . http://dx.doi.org/10.1016/j.tics.2013.12.003
Axelrod, V., Bar, M., Rees, G., Yovel, G., 2014. Neural correlates of subliminal lan-guage processing. Cereb. Cortex . http://dx.doi.org/10.1093/cercor/bhu022.
Baldo, J.V., Bunge, S.A., Wilson, S.M., Dronkers, N.F., 2010. Is relational reasoning
dependent on language? A voxel-based lesion symptom mapping study. BrainLang. 113 (2), 59–64. http://dx.doi.org/10.1016/j.bandl.2010.01.004.
Baldo, J.V., Schwartz, S., Wilkins, D., Dronkers, N.F., 2006. Role of frontal versustemporal cortex in verbal fluency as revealed by voxel-based lesion symptommapping. J. Int. Neuropsychol. Soc. 12 (6), 896–900. http://dx.doi.org/10.1017/S1355617706061078.
Baldo, J.V., Wilkins, D.P., Ogar, J., Willock, S., Dronkers, N.F., 2011. Role of the pre-central gyrus of the insula in complex articulation. Cortex 47 (7), 800–807.http://dx.doi.org/10.1016/j.cortex.2010.07.001.
Bates, E., Wilson, S.M., Saygin, A.P., Dick, F., Sereno, M.I., Knight, R.T., Dronkers, N.F.,2003. Voxel-based lesion-symptom mapping. Nat. Neurosci. 6 (5), 448–450.http://dx.doi.org/10.1038/nn1050.
Bedny, M., Hulbert, J.C., Thompson-Schill, S.L., 2007. Understanding words in con-text: the role of Broca's area in word comprehension. Brain Res. 1146, 101–114.http://dx.doi.org/10.1016/j.brainres.2006.10.012.
Benedek, M., Beaty, R., Jauk, E., Koschutnig, K., Fink, A., Silvia, P.J., Neubauer, A.C.,2014. Creating metaphors: The neural basis of figurative language production.Neuroimage 90, 99–106. http://dx.doi.org/10.1016/j.neuroimage.2013.12.046.
Benjamini, Y., Hochberg, Y., 1995. Controlling the false discovery rate: a practicaland powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 57(1), 289–300.
Binder, J.R., Desai, R.H., 2011. The neurobiology of semantic memory. Trends Cogn.Sci. 15 (11), 527–536. http://dx.doi.org/10.1016/j.tics.2011.10.001.
Binder, J.R., Desai, R.H., Graves, W.W., Conant, L.L., 2009. Where is the semanticsystem? A critical review and meta-analysis of 120 functional neuroimagingstudies. Cereb. Cortex 19 (12), 2767–2796. http://dx.doi.org/10.1093/cercor/bhp055.
Bohrn, I.C., Altmann, U., Jacobs, A.M., 2012. Looking at the brains behind figurativelanguage–a quantitative meta-analysis of neuroimaging studies on metaphor,idiom, and irony processing. Neuropsychologia 50 (11), 2669–2683. http://dx.doi.org/10.1016/j.neuropsychologia.2012.07.021.
Bookheimer, S., 2002. Functional MRI of language: new approaches to under-standing the cortical organization of semantic processing. Annu. Rev. Neurosci.25, 151–188. http://dx.doi.org/10.1146/annurev.neuro.25.112701.142946.
Booth, J.R., Burman, D.D., Meyer, J.R., Gitelman, D.R., Parrish, T.B., Mesulam, M.M.,2002. Functional anatomy of intra- and cross-modal lexical tasks. Neuroimage16 (1), 7–22. http://dx.doi.org/10.1006/nimg.2002.1081.
Borovsky, A., Saygin, A.P., Bates, E., Dronkers, N., 2007. Lesion correlates of con-versational speech production deficits. Neuropsychologia 45 (11), 2525–2533.http://dx.doi.org/10.1016/j.neuropsychologia.2007.03.023.
Brett, M., Anton, J., Valabregue, R., and Poline, J., 2002. Region of interest analysisusing an SPM toolbox. In: Proceedings of the 8th International Conference onFunctional Mapping of the Human Brain, Sendai, Japan.
Cao, Y., Vikingstad, E.M., George, K.P., Johnson, A.F., Welch, K.M., 1999. Corticallanguage activation in stroke patients recovering from aphasia with functionalMRI. Stroke 30 (11), 2331–2340.
Cappa, S.F., 2012. Imaging semantics and syntax. Neuroimage 61 (2), 427–431. http://dx.doi.org/10.1016/j.neuroimage.2011.10.006.
Chertkow, H., Bub, D., Deaudon, C., Whitehead, V., 1997. On the status of objectconcepts in aphasia. Brain Lang. 58 (2), 203–232. http://dx.doi.org/10.1006/brln.1997.1771.
Coltheart, M., 1981. The MRC psycholinguistic database. Q. J. Exp. Psychol. 33A,497–505.
Crinion, J., Holland, A.L., Copland, D.A., Thompson, C.K., Hillis, A.E., 2013. Neuroi-maging in aphasia treatment research: quantifying brain lesions after stroke.Neuroimage 73, 208–214. http://dx.doi.org/10.1016/j.neuroimage.2012.07.044.
Dronkers, N.F., Wilkins, D.P., Van Valin, R.D., Redfern, B.B., Jaeger, J.J., 2004. Lesionanalysis of the brain areas involved in language comprehension. Cognition 92(1–2), 145–177. http://dx.doi.org/10.1016/j.cognition.2003.11.002.
Fedorenko, E., Duncan, J., Kanwisher, N., 2013. Broad domain generality in focalregions of frontal and parietal cortex. Proc. Natl. Acad. Sci. USA 110 (41),16616–16621. http://dx.doi.org/10.1073/pnas.1315235110.
Fiez, J.A., 1997. Phonology, semantics, and the role of the left inferior prefrontalcortex. Hum. Brain Mapp. 5 (2), 79–83.
Fridriksson, J., Bonilha, L., Baker, J.M., Moser, D., Rorden, C., 2010. Activity in pre-served left hemisphere regions predicts anomia severity in aphasia. Cereb.Cortex 20 (5), 1013–1019. http://dx.doi.org/10.1093/cercor/bhp160.
Fridriksson, J., Richardson, J.D., Fillmore, P., Cai, B., 2012. Left hemisphere plasticityand aphasia recovery. Neuroimage 60 (2), 854–863. http://dx.doi.org/10.1016/j.neuroimage.2011.12.057.
Friederici, A.D., Kotz, S.A., 2003. The brain basis of syntactic processes: functionalimaging and lesion studies. Neuroimage 20 (Suppl 1), S8-17.
Friston, K., Ashburner, J., Heather, J., Holmes, A., & Poline, J., 2009. SPM8: StatisticalParametric Mapping (Version 8).
Gelman, A., Hill, J., Yajima, M., 2012. Why we (usually) don’t have to worry aboutmultiple comparisons. J. Res. Educ. Eff. 5 (2), 189–211.
Geranmayeh, F., Brownsett, S., Wise, R., 2014. Task-induced brian activity in aphasicstroke patients: what is driving recovery? Brain 137 (10), 2632–2648. http://dx.doi.org/10.1093/brain/awu163.
Geva, S., Baron, J.C., Jones, P.S., Price, C.J., Warburton, E.A., 2012. A comparison ofVLSM and VBM in a cohort of patients with post-stroke aphasia. NeuroimageClin. 1 (1), 37–47. http://dx.doi.org/10.1016/j.nicl.2012.08.003.
Goldstein, H., 2010. Multilevel Statistical Models, 4th ed. John Wiley & Sons, Ltd.Gow Jr., D.W., 2012. The cortical organization of lexical knowledge: a dual lexicon
model of spoken language processing. Brain Lang. 121 (3), 273–288. http://dx.doi.org/10.1016/j.bandl.2012.03.005.

J.A. Sims et al. / Neuropsychologia 84 (2016) 113–126126
Grafman, J., 2000. Conceptualizing functional neuroplasticity. J. Commun. Disord.33 (4), 345–355, quiz 355-346.
Heiss, W.D., Kessler, J., Thiel, A., Ghaemi, M., Karbe, H., 1999. Differential capacity ofleft and right hemispheric areas for compensation of poststroke aphasia. Ann.Neurol. 45 (4), 430–438.
Helm-Estabrooks, N., 2001. Cognitive Linguistic Quick Test. The Psychological Cor-poration, San Antonio, TX.
Hillis, A.E., Caramazza, A., 1991. Category-specific naming and comprehensionimpairment: a double dissociation. Brain 114 (Pt 5), 2081–2094.
Hillis, A.E., Barker, P.B., Wityk, R.J., Aldrich, E.M., Restrepo, L., Breese, E.L., Work, M.,2004. Variability in subcortical aphasia is due to variable sites of cortical hy-poperfusion. Brain Lang. 89 (3), 524–530. http://dx.doi.org/10.1016/j.bandl.2004.01.007.
Hillis, A.E., Heidler, J., 2002. Mechanisms of early aphasia recovery. Aphasiology 16,885–895.
Hillis, A.E., Wityk, R.J., Barker, P.B., Beauchamp, N.J., Gailloud, P., Murphy, K., Metter,E.J., 2002. Subcortical aphasia and neglect in acute stroke: the role of corticalhypoperfusion. Brain 125 (Pt (5)), 1094–1104.
Howard, D., & Patterson, K., 1992. The pyramids and palm tees test. Bury St. Ed-munds: Thames Valley Test Company.
Jefferies, E., 2013. The neural basis of semantic cognition: converging evidence fromneuropsychology, neuroimaging and TMS. Cortex 49, 611–625.
Jordan, L.C., Hillis, A.E., 2005. Aphasia and right hemisphere syndromes in stroke.Curr. Neurol. Neurosci. Rep. 5 (6), 458–464.
Kaplan, G., Goodglass, H., Weintraub, S., 2001. Boston Naming Test, 2nd edition. PA:Lippincott Williams & Wilkins, Philadelphia.
Karbe, H., Thiel, A., Weber-Luxenburger, G., Herholz, K., Kessler, J., Heiss, W.D., 1998.Brain plasticity in poststroke aphasia: what is the contribution of the righthemisphere? Brain Lang. 64 (2), 215–230. http://dx.doi.org/10.1006/brln.1998.1961.
Kertesz, A., 1982. The Western Aphasia battery. Grune & Stratton, Philadelphia, PA.Kim, M.J., Jeon, H.A., Lee, K.M., 2010. Impairments of syntactic comprehension in
Korean and the location of ischemic stroke lesions: a voxel-based lesion-symptom mapping study. Behav. Neurol. 22 (1–2), 3–10. http://dx.doi.org/10.3233/BEN-2009-0254.
Kiran, S., Meier, E.L., Kapse, K.J., Glynn, P.A., 2015. Changes in task-based effectiveconnectivity in language networks following rehabilitation in post-stroke pa-tients with aphasia. Front. Hum. Neurosci. 9, 316. http://dx.doi.org/10.3389/fnhum.2015.00316.
Lambon Ralph, M.A., Ehsan, S., Baker, G.A., Rogers, T.T., 2012. Semantic memory isimpaired in patients with unilateral anterior temporal lobe resection for tem-poral lobe epilepsy. Brain: J. Neurol 135 (Pt 1), 242–258. http://dx.doi.org/10.1093/brain/awr325.
Magnusdottir, S., Fillmore, P., den Ouden, D.B., Hjaltason, H., Rorden, C., Kjartansson,O., Fridriksson, J., 2013. Damage to left anterior temporal cortex predicts im-pairment of complex syntactic processing: a lesion-symptom mapping study.Hum. Brain Mapp. 34 (10), 2715–2723. http://dx.doi.org/10.1002/hbm.22096.
Meinzer, M., Beeson, P.M., Cappa, S., Crinion, J., Kiran, S., Saur, D., Parrish, T.,Crosson, B., Thompson, C.K., 2013. Neuroimaging in aphasia treatment re-search: consensus and practical guidelines for data analysis. Neuroimage 73,215–224.
Newman, S.D., Just, M.A., Keller, T.A., Roth, J., Carpenter, P.A., 2003. Differentialeffects of syntactic and semantic processing on the subregions of Broca’s area.Brain Res. Cogn. Brain Res. 16 (2), 297–307.
Novick, J.M., Kan, I.P., Trueswell, J.C., Thompson-Schill, S.L., 2009. A case for conflictacross multiple domains: memory and language impairments following da-mage to ventrolateral prefrontal cortex. Cogn. Neuropsychol. 26 (6), 527–567.http://dx.doi.org/10.1080/02643290903519367.
Pillai, J.J., Araque, J.M., Allison, J.D., Sethuraman, S., Loring, D.W., Thiruvaiyaru, D.,Lavin, T., 2003. Functional MRI study of semantic and phonological languageprocessing in bilingual subjects: preliminary findings. Neuroimage 19 (3) 565–57.
Piras, F., Marangolo, P., 2007. Noun-verb naming in aphasia: a voxel-based lesion-symptom mapping study. Neuroreport 18 (14), 1455–1458. http://dx.doi.org/10.1097/WNR.0b013e3282ef6fc9.
Piras, F., Marangolo, P., 2010. When “Crack walnuts” lies in different brain regions:evidence from a voxel-based lesion-symptom mapping study. J. Int. Neu-ropsychol. Soc. 16 (3), 433–442. http://dx.doi.org/10.1017/S1355617710000068.
Poldrack, R., 2007. Region of interest analysis for fMRI. Soc. Cogn. Affect. Neurosci. 2(1), 67–70. http://dx.doi.org/10.1093/scan/nsm006.
Price, C.J., 2012. A review and syntehsis of the first 20 years of PET and fMRI studiesof heard speech, spoken language and reading. NeuroImage . http://dx.doi.org/10.1016/j.neuroimage.2012.04.062.
Price, C.J., Warburton, E.A., Moore, C.J., Frackowiak, R.S., Friston, K.J., 2001. Dynamicdiaschisis: anatomically remote and context-sensitive human brain lesions. JCognit Neurosci 13 (4), 419–429.
Rapp, A.M., Mutschler, D.E., Erb, M., 2012. Where in the brain is nonliteral lan-guage? A coordinate-based meta-analysis of functional magnetic resonanceimaging studies. NeuroImage 63 (1), 600–610. http://dx.doi.org/10.1016/j.neuroimage.2012.06.022.
Rastle, K., Harrington, J., Coltheart, M., 2002. 358,534 nonwords: the ARC NonwordDatabase. Q. J. Exp. Psychol. A 55 (4), 1339–1362. http://dx.doi.org/10.1080/02724980244000099.
Rehm, K. Schaper, Anderson, J., Woods, R., Stoltzner, S., Rottenberg, D., 2004. Put-ting our heads together: a consensus approach to brain/non-brain segmenta-tion in T1-weighted MR volumes. NeuroImage 22, 1262–1270.
Reilly, J., Rodriguez, A.D., Peelle, J.E., Grossman, M., 2011. Frontal lobe damage im-pairs process and content in semantic memory: evidence from category-spe-cific effects in progressive non-fluent aphasia. Cortex 47 (6), 645–658. http://dx.doi.org/10.1016/j.cortex.2010.05.005.
Reineck, L.A., Agarwal, S., Hillis, A.E., 2005. “Diffusion-clinical mismatch” is asso-ciated with potential for early recovery of aphasia. Neurology 64 (5), 828–833.http://dx.doi.org/10.1212/01.WNL.0000152983.52869.51.
Rorden, C. (2012). MRICron.Ruff, I., Blumstein, S.E., Myers, E.B., & Hutchison, E., 2008. Recruitment of anterior
and posterior structures in lexical-semantic processing: an fMRI study com-paring implicit and explicit tasks. Brain Lang, 105(1), 41–49. doi: S0093-934X(08)00004-7 [pii]10.1016/j.bandl.2008.01.003.
Sandberg, C., Bohland, J., Kiran, S., 2015. Neural plasticity related to direct trainingand generalization effects of word finding treatment in chronic aphasia. BrainLang. 150, 103–116.
Saur, D., Lange, R., Baumgaertner, A., Schraknepper, V., Willmes, K., Rijntjes, M.,Weiller, C., 2006. Dynamics of language reorganization after stroke. Brain 129(Pt 6), 1371–1384. http://dx.doi.org/10.1093/brain/awl090.
Sebastian, R., Kiran, S., 2011. Task-modulated neural activation patterns in chronicstroke patients with aphasia. Aphasiology 25, 927–951.
Stuss, D.T., Alexander, M.P., 2007. Is there a dysexecutive syndrome? Philos. Trans.R. Soc. Lond. B Biol. Sci. 362 (1481), 901–915. http://dx.doi.org/10.1098/rstb.2007.2096.
Thiel, A., Hartmann, A., Rubi-Fessen, I., Anglade, C., Kracht, L., Weiduschat, N., Heiss,W.D., 2013. Effects of noninvasive brain stimulation on language networks andrecovery in early poststroke aphasia. Stroke 44 (8), 2240–2246. http://dx.doi.org/10.1161/STROKEAHA.111.000574.
Thompson-Schill, S.L., Aguirre, G.K., D’Esposito, M., Farah, M.J., 1999. A neural basisfor category and modality specificity of semantic knowledge. Neuropsychologia37 (6), 671–676.
Turkeltaub, P.E., Messing, S., Norise, C., Hamilton, R.H., 2011. Are networks for re-sidual language function and recovery consistent across aphasic patients?Neurology 76 (20), 1726–1734. http://dx.doi.org/10.1212/WNL.0b013e31821a44c1.
van Oers, C.A., Vink, M., van Zandvoort, M.J., van der Worp, H.B., de Haan, E.H.,Kappelle, L.J., Dijkhuizen, R.M., 2010. Contribution of the left and right inferiorfrontal gyrus in recovery from aphasia. A functional MRI study in stroke pa-tients with preserved hemodynamic responsiveness. Neuroimage 49 (1),885–893. http://dx.doi.org/10.1016/j.neuroimage.2009.08.057.
Vanderwouden T., 1990. Celex-building a multifunctional, polytheoretical lexicaldatabase. Budalex'88 Proceedings, pp. 363–373.
Vartanian, O., 2012. Dissociable neural systems for analogy and metaphor: im-plications for the neuroscience of creativity. Br. J. Psychol. 103 (3), 302–316.http://dx.doi.org/10.1111/j.2044-8295.2011.02073.x.
Vigneau, M., Beaucousin, V., Hervé, Duffau, H., Crivello, F., Houdé, O., Mazoyer, B.,Tzourio-Mazoyer, N., 2006. Meta-analyzing left hemisphere language areas:phonology, semantics, and sentence processing. Neuroimage 30, 1414–1432.http://dx.doi.org/10.1016/j.neuroimage.2005.11.002.
Walker, G.M., Schwartz, M.F., Kimberg, D.Y., Faseyitan, O., Brecher, A., Dell, G.S.,Coslett, H.B., 2011. Support for anterior temporal involvement in semantic errorproduction in aphasia: new evidence from VLSM. Brain Lang. 117 (3), 110–122.http://dx.doi.org/10.1016/j.bandl.2010.09.008.
Wang, Y., Holland, S.K., 2014. Comparison of functional network connectivity forpassive-listening and active-response narrative comprehension in adolescents.Brain Connect. . http://dx.doi.org/10.1089/brain.2013.0190
Winhuisen, L., Thiel, A., Schumacher, B., Kessler, J., Rudolf, J., Haupt, W.F., Heiss, W.D., 2007. The right inferior frontal gyrus and poststroke aphasia: a follow-upinvestigation. Stroke 38 (4), 1286–1292. http://dx.doi.org/10.1161/01.STR.0000259632.04324.6c.