Embed Size (px)
Citation preview
434 BRIT. J. SURG., 1973, Vol. 60, No. 6, JUNE
THE REDUCTION OF SURGICAL WOUND INFECTIONS BY PROPHYLACTIC PARENTERAL CEPHALORIDINE
A CONTROLLED CLINICAL TRIAL
BY CHRISTINE EVANS AND A. V. POLLOCK SCARBOROUGH HOSPITAL. YORKSHIRE
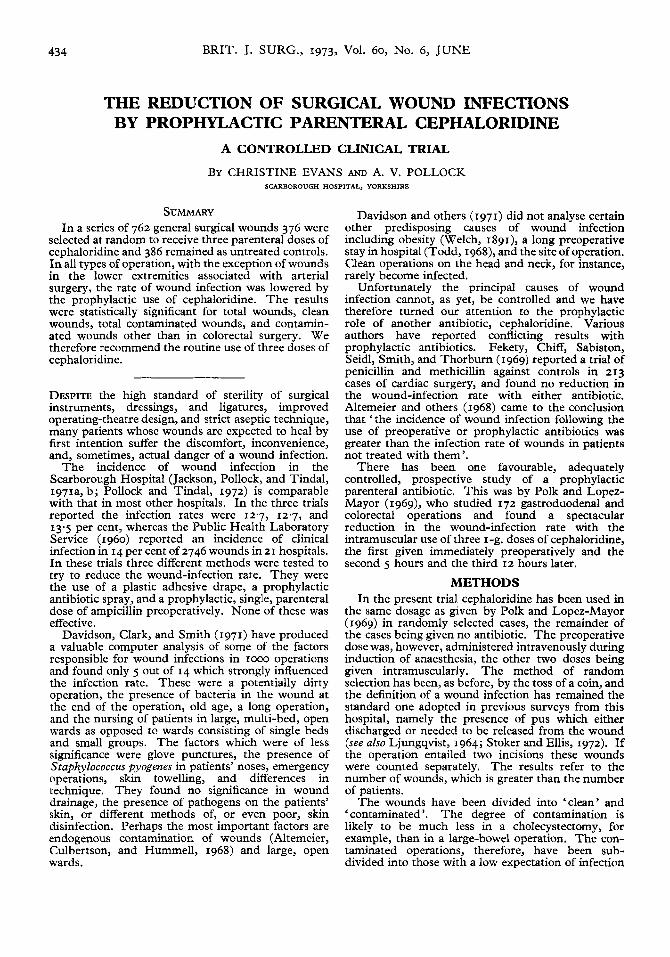
SUMMARY In a series of 762 general surgical wounds 376 were
selected at random to receive three parenteral doses of cephaloridine and 386 remained as untreated controls. In all types of operation, with the exception of wounds in the lower extremities associated with arterial surgery, the rate of wound infection was lowered by the prophylactic use of cephaloridine. The results were statistically significant for total wounds, clean wounds, total contaminated wounds, and contamin- ated wounds other than in colorectal surgery. We therefore recommend the routine use of three doses of cephaloridine.
DESPITE the high standard of sterility of surgical instruments, dressings, and ligatures, improved operating-theatre design, and strict aseptic technique, many patients whose wounds are expected to heal by first intention suffer the discomfort, inconvenience, and, sometimes, actual danger of a wound infection.
The incidence of wound infection in the Scarborough Hospital (Jackson, Pollock, and Tindal, 1971a, b; Pollock and Tindal, 1972) is comparable with that in most other hospitals. In the three trials reported the infection rates were 12.7, 12.7, and 13.5 per cent, whereas the Public Health Laboratory Service (1960) reported an incidence of clinical infection in 14 per cent of 2746 wounds in 21 hospitals. In these trials three different methods were tested to try to reduce the wound-infection rate. They were the use of a plastic adhesive drape, a prophylactic antibiotic spray, and a prophylactic, single, parenteral dose of ampicillin preoperatively. None of these was effective.
Davidson, Clark, and Smith (1971) have produced a valuable computer analysis of some of the factors responsible for wound infections in 1000 operations and found only 5 out of 14 which strongly influenced the infection rate. These were a potentially dirty operation, the presence of bacteria in the wound at the end of the operation, old age, a long operation, and the nursing of patients in large, multi-bed, open wards as opposed to wards consisting of single beds and small groups. The factors which were of less significance were glove punctures, the presence of Staphylococcus pyogenes in patients’ noses, emergency operations, skin towelling, and differences in technique. They found no significance in wound drainage, the presence of pathogens on the patients’ skin, or different methods of, or even poor, skin disinfection. Perhaps the most important factors are endogenous contamination of wounds (Altemeier, Culbertson, and Hummell, 1968) and large, open wards.
Davidson and others (1971) did not analyse certain other predisposing causes of wound infection including obesity (Welch, 1891), a long preoperative stay in hospital (Todd, 1968), and the site of operation. Clean operations on the head and neck, for instance, rarely become infected.
Unfortunately the principal causes of wound infection cannot, as yet, be controlled and we have therefore turned our attention to the prophylactic role of another antibiotic, cephaloridine. Various authors have reported conflicting results with prophylactic antibiotics. Fekety, Chiff, Sabiston, Seidl, Smith, and Thorburn (1969) reported a trial of penicillin and methicillin against controls in 213 cases of cardiac surgery, and found no reduction in the wound-infection rate with either antibiotic. Altemeier and others (1968) came to the conclusion that ‘the incidence of wound infection following the use of preoperative or prophylactic antibiotics was greater than the infection rate of wounds in patients not treated with them’.
There has been one favourable, adequately controlled, prospective study of a prophylactic parenteral antibiotic. This was by Polk and Lopez- Mayor (1969), who studied 172 gastroduodenal and colorectal operations and found a spectacular reduction in the wound-infection rate with the intramuscular use of three I-g. doses of cephaloridine, the first given immediately preoperatively and the second 5 hours and the third 12 hours later.
METHODS In the present trial cephaloridine has been used in
the same dosage as given by Polk and Lopez-Mayor (1969) in randomly selected cases, the remainder of the cases being given no antibiotic. The preoperative dose was, however, administered intravenously during induction of anaesthesia, the other two doses being given intramuscularly. The method of random selection has been, as before, by the toss of a coin, and the definition of a wound infection has remained the standard one adopted in previous surveys from this hospital, namely the presence of pus which either discharged or needed to be released from the wound (see also Ljungqvist, 1964; Stoker and Ellis, 1972). If the operation entailed two incisions these wounds were counted separately. The results refer to the number of wounds, which is greater than the number of patients.
The wounds have been divided into ‘clean’ and ‘contaminated’. The degree of contamination is likely to be much less in a cholecystectomy, for example, than in a large-bowel operation. The con- taminated operations, therefore, have been sub- divided into those with a low expectation of infection
EVANS AND POLLOCK: SURGICAL WOUND INFECTIONS
CEPHALORIDINE No CEPHALORIDINE
No. of Wounds No. Infected Per cent No. of Wounds No. Infected Per cent
6 22'2 46 7 15'2 1.8 171 I1 6.4 3
46 20 43'5 I4 I1 I '$': I I23 I9 15'4
_ _ _ ~ _ - '-7 TYPE OF WOUND
Clean Arterial surgery Other surgery
Contaminated Colorectal Other surgery
435
x 2 p
~ - - ~ - - N.S.
4.43 <0'05
0'79 1 N.S. 4'05 <0'05
~ 5 _ -
TKPE OF OPERATION
Arterial (lower limb)
Total contaminated wounds 1 I85 25 13'5 169 I 39 23'1 1 5'45 I <0'02 Total all types of wound 1 376
-
Wounds
27
TKPE OF OPERATION
Perforated appendices Colorectal Non-arterial
Head and neck Breast and axilla
Wounds
7 34
Hand
Lumbar incisions Scrota1 incisions Groin hernias Varicose veins Other groin incisions
Total
Laparotomy,
Amputations
No. No. of No. [nfected I Wounds I Infected
I 29
8 6
2: 14 9
164
0 0 I I 29 I 0 I4 0 I 0 0 I 2 4 0 8 I
Patients under the age of 16 years were excluded because we do not favour injections in children if they can be avoided. Thirty-two patients who died within 2 weeks of operation in whom the presence or absence of infection was uncertain have been excluded from the study, leaving 762 wounds for analysis out of a total of 794. All patients were seen by one of us for at least 4 weeks. When the infection developed in hospital the pus was cultured and the sensitivity to cephaloridine tested by the Multidisc method. Five late wound infections escaped bacteriological study and 7 pus swabs were sterile. No restriction was placed on the use of therapeutic antibiotics, but no other prophylactic antibiotic was allowed except for the usual oral preparations for colonic surgery.
To avoid bias the details were entered not in the patients' case notes but on punch cards which were kept separately and analysed manually.
RESULTS Seven hundred and sixty-two wounds were studied,
91 of which became infected (11.9 per cent). There were 376 wounds in patients who were given cephaloridine and 386 in patients who were not.
Table III.--CONTAMINATED WOUNDS : TYPES OF OPERATION
Total 41 -___ Stomach
VaEotomv and 1 Gy1oroplasty
Vagotomy and pyloroplasty, and appendicectomy
Gastrotomy Gastrectomy
Gall-bladder and ducts Cholecystectomy Cholecystectomy and
appendicectom y Intestinal resection Appendix
Acute Normal
Cystotomy and prostatectomy
Renal pelvis and ureter Hysterectomy Excision of infected
lesions
9
I 2
I I1
I 2 I9
4
18 15 30
5
7 I
No. No. of Infected I Wounds -- I-
I1 1: I 35
I4 I 46
; I :: 2 5
H I ; 4
No. Infected
5 15
20
2
2
I I
3 3
0
0 0 4
0 0 3
above the abdomen (Table ZZ). On the other hand, incisions for arterial reconstruction in the lower limbs were much more likely to become infected. Most of these infections were probably acquired in the ward postoperatively on the basis of discharging haematomas. Long operating times and the presence of drains in these wounds may also have contributed.
There were 73 clean wounds for arterial disease of the lower extremities; 27 in patients given cephaloridine and 46 in patients who were not. There were 6 infections in the first group (22.2 per cent) and 7 in the second (15.2 per cent). This was the only area in the entire series which showed poorer results
436 BRIT. J. SURG., 1973, Vol. 60, No. 6, JUNE
TYPE OF WOUND
- Clean (non-arterial)
using prophylactic cephaloridine and the difference is not significant.
There were 335 clean wounds apart from those for arterial disease in the lower limbs, with 14 infections (4.2 per cent); 164 in patients given cephaloridine and 171 in patients who were not. In the former there were 3 infections (1.8 per cent) and in the latter
~
YOUNG OLD TREATMENT
-~ 81 79
Cephaloridine 83 No cephaloridine 92
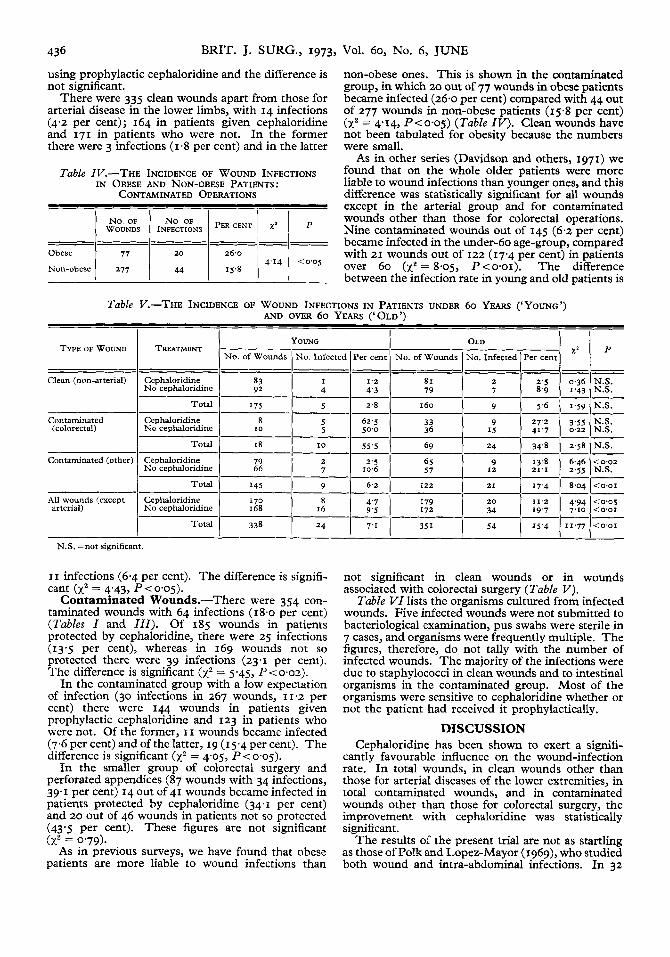
Table IV.-THE INCIDENCE OF WOUND INFECTIONS IN OBESE AND NON-OBESE PATIENTS:
CONTAMINATED OPERATIONS
- Contaminated (colorectal)
non-obese ones. This is shown in the contaminated group, in which 20 out of 77 wounds in obese patients became infected (26.0 per cent) compared with 44 out of 277 wounds in non-obese patients (15.8 per cent) (x2 = 4'14, P<0-05) (Table IV). Clean wounds have not been tabulated for obesity because the numbers were small.
As in other series (Davidson and others, 1971) we found that on the whole older patients were more liable to wound infections than younger ones, and this difference was statistically significant for all wounds except in the arterial group and for contaminated wounds other than those for colorectal operations. Nine contaminated wounds out of 145 ( 6 2 per cent) became infected in the underdo age-group, compared with 21 wounds out of 122 (17.4 per cent) in patients over 60 (xz = 8-05, P<o.oI). The difference between the infection rate in young and old patients is
~ ~~
5.6 1.59 N.S. Total I75 5 2.8 I 60
5 62.5 33 5 50.0 36
Cephaloridine N o cephaloridine
Table V.-THE INCIDENCE OF WOUND INFECTIONS IN PATIENTS UNDER 60 YEARS ('YOUNG') AND OVER 60 YEARS ('OLD')
Contaminated (other) Cephaloridine N o cephaloridine
Total I45 9 6.2
10.02 N.S.
<O'OI
<0'05 <O'OI
<O'OI I
N.S. =not significant.
I I infections (6.4 per cent). The difference is signifi- cant (xz = 4.43, P(0.05).
Contaminated Wounds.-There were 354 con- taminated wounds with 64 infections (18.0 per cent) (Tables I and I I I ) . Of 185 wounds in patients protected by cephaloridine, there were 25 infections (13.5 per cent), whereas in 169 wounds not so protected there were 39 infections (23.1 per cent). The difference is significant (xz = 5.45, P<o.oz).
In the contaminated group with a low expectation of infection (30 infections in 267 wounds, 11.2 per cent) there were I44 wounds in patients given prophylactic cephaloridine and 123 in patients who were not. Of the former, I I wounds became infected (7.6 per cent) and of the latter, 19 (15.4 per cent). The difference is significant (xz = 4'05, Pto.05).
In the smaller group of colorectal surgery and perforated appendices (87 wounds with 34 infections, 39.1 per cent) 14 out of 41 wounds became infected in patients protected by cephaloridine (34.1 per cent) and 20 out of 46 wounds in patients not so protected (43.5 per cent). These figures are not significant
As in previous surveys, we have found that obese patients are more liable to wound infections than
fXZ = 0.79).
not significant in clean wounds or in wounds associated with colorectal surgery (Table V ) .
Table VI lists the organisms cultured from infected wounds. Five infected wounds were not submitted to bacteriological examination, pus swabs were sterile in 7 cases, and organisms were frequently multiple. The figures, therefore, do not tally with the number of infected wounds. The majority of the infections were due to staphylococci in clean wounds and to intestinal organisms in the contaminated group. Most of the organisms were sensitive to cephaloridine whether or not the patient had received it prophylactically.
DISCUSSION Cephaloridine has been shown to exert a signifi-
cantly favourable influence on the wound-infection rate. In total wounds, in clean wounds other than those for arterial diseases of the lower extremities, in total contaminated wounds, and in contaminated wounds other than those for colorectal surgery, the improvement with cephaloridine was statistically significant.
The results of the present trial are not as startling as those of Polk and Lopez-Mayor (1969)~ who studied both wound and intra-abdominal infections. In 32
EVANS AND POLLOCK: SURGICAL WOUND INFECTIONS 437
CEPHALORIDINE
ORGANISMS Clean Wounds Contaminated Wounds -
patients with gastroduodenal operations given cepha- loridine prophylactically they found no infections, whereas in 36 patients given a placebo 11 infections occurred. In 54 colorectal operations protected by cephaloridine there were 4 infections and in 50 without cephaloridine there were 15 infections.
Cephaloridine is a bactericidal antibiotic active against Staphylococcus pyogenes and other Gram- positive cocci (but only some strains of Streptococcus
No CEPHALORIDINE
Clean Wounds Contaminated Wounds -
Jackson and others (1971b) failed to show a significant reduction in the wound-infection rate by the use of a bacitracin-polyrnixin-neomycin spray.
We think it may be more acceptable to staff and patients to instil cephaloridine into the wound before closure rather than to use it parenterally. If its topical use can be shown to have equally satisfactory results we will be prepared to change to this method. This is at present under investigation.
Staphylococcus p y ogenes (coagulase positive)
Staphylococcus epidermidis (coagulase negative)
Intestinal organisms Proteus sp.
Pseudomonas aeruginosa Streptococcus faecalis Klebsiella aerogenes Closrridium welchii Salmonella sp. Enrerobacter aerogenes Acinetobacrer anitratus Micrococcrrs tetragenes
Escherichia coli
5 I 3 0 I 3 0 I 2 0
0 0 2 I 3 0 3 I
I 3 15 4 3 2 32 I 2 0 2 0 I 0 I0 1 I I 0 0 I 13 4
4 8
0 0 0 2 0 I 0 4 0 0 I I 2 0 2 3 0 0 I 0 0 0 4 0 0 0 I 0 0 0 0 0 0 0 0 0 0 0 I 0 0 0 0 0 0 0 I 0 0 0 0 I 0 0 0 0 0 0 0 0 0 0 I 0 --
20 I 6 l Total organisms
T, Organism sensitive to cephaloridine. -, Organism not sensitive to cephaloridine.
5 I9 I 2 47 I 3
faecalis). The Gram-negative organisms which are sensitive to cephaloridine include Proteus mirabilis (but not other species of Proteus), Escherichia coli, and most strains of Klebsiella pneumoniae. It has no activity against Pseudomonas aeruginosa. In the present series wound infections were mainly due to staphylococci and intestinal organisms. The ad- ministration of cephaloridine did not result in any change in the type of organism or, curiously enough, in the emergence of cephaloridine-resistant organisms.
Against the achievement of this drug must be set the inconvenience to the patient of intramuscular injec- tions in the immediate postoperative period, the slight increase in nurses' work, and the cost of the drug. However, assuming a daily cost for in-patient treatment in a non-teaching hospital of approximately LIO per day and keeping in mind the discomfort of any wound infection, the saving due to the use of cephaloridine more than outweighs these disad- vantages.
There have been several favourable reports on the topical use of antibiotics in the prevention of wound infection. Local ampicillin reduced the wound- infection rate after grid-iron appendicectomy (Mountain and Seal, 1970) and after biliary and gastro-intestinal surgery (Stoker and Ellis, 1972). Longland, Gray, Lees, and Garrett (1971) reported benefit from the application of a solution of tetra- cycline to appendicectomy wounds, while Moylan and Brockenbrough (1968) reported improvement with I per cent kanamycin irrigation. On the other hand,
Acknowledgements.-We gratefully acknowledge the assistance of Dr. R. D. Foord of Glaxo Labora- tories Ltd., who also supplied the cephaloridine (Ceporin).
REFERENCES ALTEMEIER, W. A., CULBERTSON, W. R., and HUMMELL,
R. P. (1968), Surg. Clins N. Am., 48, 227. DAVIDSON, A. I. G., CLARK, C., and SMITH, G. (1971),
Br.J . Surg., 58,333. FEKETY, F. R., jun., CHIFF, L. E., SABISTON, D. C., jun.,
SEIDL, L. G., SMITH, J. W., and THORBURN, T. (1969), r. thorac. cardiovasc. Surg., 57, 757. JACKSON, D. W., POLLOCK, A. V., and TINDAL, D. S. (1971a), B r . 3 . Surg., 58, 340. ------ (1971b), Ibid., 58, 565.
LJUNGQVIST, U. (1964)~ Lancet, I , 1095. LONGLAND, C. J., GRAY, J. G., LEES, W., and GARRETT,
J. A. M. (1971), B r . J . Surg., 58, 117. MOUNTAIN, J. C., and SEAL, P. V. (IgO), Br.3 . clin. Pract.,
24. III. I
MOYLAN, J. A., and BROCKENBROUGH, E. C. (1968),
POLK, H. C., jun., and LOPEZ-MAYOR, J. F. (1969), Surg. Forum, 19, 66.
. . . - _ . ~ Surgery, 66, 97.
59. 08. POLLOCK, A. V., and TINDAL, D. S. (I972), Br. J. Surg.,
~ ,,-- PUBLIC HEALTH LABORATORY SERVICE (1960), Lancet, 2,
STOKER, T. A. M., and ELLIS, H. (1972), B r . J . Surg., 59,
TODD, J. C. (1968), Surg. Clins N . Am., 48, 787. WELCH, W. H. (1891), Trans. Cong. Am. Physns Surg.,
659.
184.
2, I.
32




![Research Article The Efficacy of Prophylactic Single Dose … · 2016-12-27 · effect on the prevention of postoperative wound infections in certain high risk foot procedures [2],](https://img.pdfslide.us/doc/110x75/5f42876b4e27494653072563/research-article-the-efficacy-of-prophylactic-single-dose-2016-12-27-effect-on.jpg)