Embed Size (px)
Citation preview

J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 5 , N O . 3 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 4 . 1 0 . 0 4 5
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Device-Detected Atrial Fibrillation
What to Do With Asymptomatic Patients?Carol Chen-Scarabelli, PHD,* Tiziano M. Scarabelli, MD, PHD,y Kenneth A. Ellenbogen, MD,zJonathan L. Halperin, MDy
ABSTRACT
Fro
Wi
Co
Bo
Bo
Da
lat
sen
Lis
Yo
Ma
Atrial fibrillation (AF) is the most common clinically significant arrhythmia and conveys an increased risk of stroke,
regardless of whether it is symptomatic. Despite multiple studies supporting an association between subclinical atrial
tachyarrhythmias (ATs) detected by cardiac implantable electronic devices and increased risk of thromboembolic events,
clinical intervention for device-detected AT remains sluggish, with some clinicians delaying treatment and instead opting
for continued surveillance for additional or longer episodes. However, the 2014 updated clinical practice guidelines on AF
recommend use of the CHA2DS2-VASc stroke risk score for nonvalvular AF, with oral anticoagulation recommended for
scores $2, regardless of whether AF is paroxysmal, persistent, or permanent. This paper reviews the epidemiology of AF
and mechanisms of stroke in AF, and discusses device-detected AF and its clinical implications. (J Am Coll Cardiol 2015;
65:281–94) © 2015 by the American College of Cardiology Foundation.
A trial fibrillation (AF) is the most commonclinically significant heart rhythm disorder(1), with an estimated lifetime risk of 22%
to 26% or about a lifetime risk of 1 in 4 (2). It hasbeen diagnosed in >2.5 million people in the UnitedStates alone (3). In 2010, the incidence of diagnosedAF in the United States was 1.2 million, and itsprevalence is projected to increase to >12 millioncases by 2030 (4). In the European Union, therewere 8.8 million adults >55 years of age with AFin 2010, with an expected increase to 17.9 millionby 2060 (5). Globally, AF incidence in 2010 was esti-mated at 33.5 million (20.9 million men and 12.6million women). Despite a higher incidence inmen, mortality associated with AF is greater inwomen, doubling between 1990 and 2010 (6). These
m the *Veterans Affairs Ann Arbor Health Care System, University of Mi
ener Cardiovascular Institute, Mount Sinai Medical Center, New York, Ne
mmonwealth University School of Medicine, Richmond, Virginia. Dr. Ell
ston Scientific and St. Jude Medical, and has received research, honora
ston Scientific. Dr. Halperin has served as a consultant for Bayer Healt
iichi Sankyo, Pfizer, Inc., Biotronik, Boston Scientific, and Medtronic. All
ionships relevant to the contents of this paper to disclose. Drs. Ellenboge
ior authors. Sumeet Chugh, MD, served as Guest Editor for this paper.
ten to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Vale
u can also listen to this issue’s audio summary by JACC Editor-in-Chief D
nuscript received June 29, 2014; revised manuscript received October 14
statistics do not account for silent or undiagnosedAF, which is thought to affect as many as one-third of the U.S. population (3).
MECHANISMS OF AF
The pathophysiology of AF is multifactorial and com-plex, including both genetic and neural mechanisms.The main mechanism by which autonomic activationtriggers AF is activation of the sympathetic and para-sympathetic nervous system, which likely interactwith the pulmonary vein–left atrial (LA) junction totrigger atrial ectopy (7). Genetic mechanisms linked toAF development include alterations in potassium orsodium channels, connexin expression or function (2),and microRNAs (8). Four major mechanisms that
chigan, Ann Arbor, Michigan; yZena and Michael A.
w York; and the zDepartment of Medicine, Virginia
enbogen has served as a consultant for Medtronic,
rium, and fellowship support from Medtronic and
hcare, Boehringer Ingelheim, Bristol-Myers Squibb,
other authors have reported that they have no re-
n and Halperin contributed equally to this work as
ntin Fuster.
r. Valentin Fuster.
, 2014, accepted October 14, 2014.

ABBR EV I A T I ON S
AND ACRONYMS
AF = atrial fibrillation
AHRE = atrial high
rate episodes
AT = atrial tachyarrhythmia
CIED = cardiac implantable
electronic device
CRT = cardiac
resynchronization therapy
CS = cryptogenic stroke
ECG = electrocardiogram
EGM = intracardiac electrogram
ICM = implantable cardiac
monitor
LA = left atrium/atrial
LAA = left atrial appendage
TE = thromboembolic event(s)
Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
282
promote focal ectopic firing and reentry sub-strate formation have been implicated in AF:1) ion channel dysfunction; 2) calciumhandling abnormalities; 3) structural remod-eling (primarily atrial fibrosis); and 4) auto-nomic neural dysregulation (2,8). These 4conditions not only trigger AF, but may alsoresult from episodes of AF, supporting theconcept that “atrial fibrillation begets atrialfibrillation,” first reported in an early animalstudy documenting atrial electrical remodel-ing in AF (9). Further advances in knowledgeof the pathophysiology of AF have revealedthat electrical remodeling in AF is not limitedto the atria. More pronounced remodeling af-ter brief episodes of induced AF has beendocumented in the pulmonary veins (10),thereby extending the concept to “AF begetsAF in the pulmonary veins”.
AF AND STROKE
AF is amajor independent predictor of ischemic stroke,resulting in a 5-fold increase in risk (1). Each year,approximately 795,000 people experience strokes, ofwhich 610,000 are first strokes and approximately 87%are ischemic. In the United States, someone suffers astroke every 40 s (that is, approximately 90 people/h)(1). Among patients with AF, it is estimated that everyhour, 15 will have a stroke (11), and such AF-relatedstrokes impose a higher mortality than strokes unre-lated to AF (12). The prevalence of AF and associatedstroke risk are highest among elderly patients, withstroke risk independent of whether AF is paroxysmal,persistent, or permanent (1). A large number ofearlier clinical trials (13–15) demonstrated that sys-temic anticoagulation is highly efficacious for strokeprevention in patients with AF (16), with a recentmeta-analysis documenting the efficacy of bothdirect thrombin inhibitors and vitamin K antago-nists in stroke prevention in nonvalvular AF (17).
The association between AF and cryptogenicstroke (CS) was recently documented using animplantable cardiac monitor (ICM). The CRYSTAL-AF(CRYptogenic Stroke and underlying Atrial Fibrilla-tion) trial, a prospective, randomized, multicenter,global study, in which long-term cardiac monitoringusing an ICM was compared to conventional elec-trocardiogram (ECG) monitoring (ECG, 24-h Holter, orevent monitor) for detection of AF in 441 patientswith CS, demonstrated that AF was detected in 8.9%of ICM patients (compared to 1.4% in the ECG controlgroup) at 6 months. Furthermore, on long-termfollow-up at 3 years, AF was detected in 30% of
patients by ICM, compared to only 3% in the con-ventional ECG group (18). Although anticoagulantprescription for AF was higher in the ICM groupversus the routine ECG monitoring group (10.1% vs.4.6%) at 6 months, 97.0% of patients with detectedAF were receiving oral anticoagulant agents by the12-month follow-up (18).
A similar study, the EMBRACE (30-Day CardiacEvent Monitor Belt for Recording Atrial FibrillationAfter a Cerebral Ischemic Event) study, compared newAF detection by noninvasive ambulatory ECG moni-toring with either a 30-day event-triggered recorder(intervention group) or a conventional 24-h monitor(control group) in 572 patients with CS within the pre-ceding 6 months, without a history of AF (19). The in-vestigators reported a greater than 5-fold increase(16.1%vs. 3.2%; p<0.001) in AFdetection in the 30-dayevent monitor group, with a subsequent significantincrease in anticoagulation prescription (18.6% vs.11.1%; p ¼ 0.01) among the 30-day event monitorgroup. At the 90-day follow-up, 87% of patients withAF in the event monitor group and 100% of patientswith AF in the control group were on anticoagulanttherapy (19). Thus, both the CRYSTAL-AF andEMBRACE studies documented a significant increasein anticoagulant prescription in CS patients withnewly detected AF. However, anticoagulation treat-ment rates are significantly lower for patientswithout a prior history of stroke with newly detectedAF on cardiac implantable electronic devices (CIEDs).One retrospective study reported a 50% incidence ofpacemaker-detected AF, yet <25% of these patientswith pacemaker-detected AF were treated with anti-coagulant agents (20). The temporal relationship be-tween atrial fibrillation and stroke is not as wellunderstood, and in some patients, episodes of AF arenot detected until months after a stroke.
MECHANISMS OF STROKE IN AF
Although AF-related stroke is commonly attributedto clot formation resulting from blood stasis in thepoorly contracting LA during AF, the mechanismsof thrombogenesis in AF are much more complex,implicating Virchow’s triad reviewed by Watson et al.(21) and Iwasaki et al. (22).
In AF, endothelial and endocardial damage in theleft atrial appendage (LAA), the presence of complexaortic plaque ($4 mm, ulcerated, or mobile) (23), andabnormal extracellular matrix turnover (which caninduce fibrosis) all contribute to vessel wall changes.Abnormal blood stasis in the LA and LAA (whichis promoted by and further worsens LA dilation),along with abnormal hemostasis and coagulation

J A C C V O L . 6 5 , N O . 3 , 2 0 1 5 Chen-Scarabelli et al.J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4 Device-Detected Atrial Fibrillation
283
(activation of platelets and the coagulation cascade),complete Virchow’s triad (21). Virchow’s triad(described by the German physician, RudolfVirchow), identified 3 main factors contributing tothrombosis: alterations in blood flow (stasis), thevessel wall (injury to the vascular endothelium), andblood constituents (hypercoagulability). Whenapplied to thrombogenesis in AF, blood stasis occursin the LA/LAA, atrial structural remodeling (includingendothelial damage) ensues, and there is hypercoag-ulability due to activation of platelets and the coag-ulation cascade. Atrial hypocontractility and loss ofatrial kick, along with LA enlargement, lead to bloodstasis, which promotes endothelial damage and hy-percoagulability. Up-regulation of inflammatory andgrowth factors leads to endothelial damage, which inturn, promotes hypercoagulability with subsequentabnormal fibrinolysis (22).
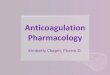
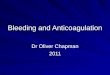
Due to its anatomical morphology, the LAA, avestigial remnant of the original embryonic LA, has apredilection for thrombus formation. In fact, theLAA is the most common site of thrombus formationin patients with nonvalvular AF (24), accountingfor >90% of thrombi (Figure 1). This thrombogenictendency has led to targeted interventions to occludethe LAA in an attempt to reduce stroke risk in AF, asreported in trials such as the PLAATO (PercutaneousLeft Atrial Appendage Transcatheter Occlusion) trialin 2002 (25) and, most recently, the PROTECT AF(Watchman Left Atrial Appendage System for EmbolicProtection in Patients With Atrial Fibrillation) study,which documented noninferiority of LAA occlusion tosystemic anticoagulation (26). In fact, the PROTECTAF trial was credited with being the first trial todemonstrate involvement of the LAA in the patho-genesis of stroke in AF (27).
Significant safety concerns for WATCHMAN im-plantation, including pericardial effusions and deviceembolization, were addressed in a subsequent trial,the PREVAIL (Watchman LAA Closure Device in Pa-tients With Atrial Fibrillation Versus Long TermWarfarin Therapy) trial, which documented a signifi-cantly lower rate of adverse events compared to thePROTECT AF trial (4.2% vs. 8.7%; p ¼ 0.004) (28).Although the third review by the Food and DrugAdministration Circulatory System Devices AdvisoryPanel in October 2014 (29) resulted in a unanimousvote on safety of the device, analysis of the updatedJune 2014 PREVAIL dataset demonstrated newischemic strokes occurring more than 1 year afterWATCHMAN device implant. Furthermore, neitherthe first primary endpoint of the PREVAIL trial(composite 18-month rate of stroke, cardiovascular orunexplained death, and systemic embolism) nor the
second primary endpoint (composite 18-month rate ofstroke and systemic embolism) were met, raisingthe question regarding long-term efficacy, with thecommittee split on the benefit-risk profile. At thepresent time, the fate of the WATCHMAN deviceremains uncertain (29).
Recent studies reported a significant associationbetween the type of LAA morphology and silent ce-rebral ischemia as well as stroke risk, suggesting apotential role for LAA morphology in stroke riskstratification schemes. Among the 4 major types ofLAA morphology (chicken wing, cactus, windsock,and cauliflower), cauliflower LAA morphology carriedthe highest risk of stroke, whereas chicken wing car-ried the lowest in a study of 932 patients undergoingcatheter ablation of AF (30). A significant associationbetween LAA morphology and burden of silent cere-bral ischemia was reported in 348 patients undergo-ing catheter ablation of AF (31). Although LAAexclusion does not prevent AF-related strokes due toother causes (i.e., noncardioembolic origin), becausethe LAA accounts for >90% of thrombi in AF (25), itmay be a significant strategy in stroke preventionin nonvalvular AF.
DEVICE-DETECTED AF
Subclinical atrial tachyarrhythmias (AT) can bedetected by various cardiac monitoring methods,including external surface monitoring (e.g., standard12-lead electrocardiogram, ambulatory Holter moni-tors, event monitors) and by CIEDs (e.g., implantablecardiac monitors, dual-chamber pacemakers, dual-chamber implantable cardioverter-defibrillators, car-diac resynchronization therapy [CRT] devices), manyof which enable remote monitoring. This reviewaddresses only CIEDs, given their continuous moni-toring capability. AT commonly occurs in patientswith CIEDs and is associated with an increased riskof thromboembolism (TE) (1). Several studies havecorrelated TE risk with the total duration or burdenof device-detected AT (32–34). However, there arepresently no published randomized clinical studiesinvestigating treatment of AT detected by CIEDs.
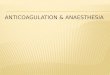
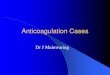
All cardiac rhythm recordings obtained from CIEDsrequire adjudication or review by a qualified clinicianto verify diagnostic accuracy. Retrospective review ofdevice-derived data has confirmed that most of thesetachyarrhythmias represent paroxysmal AF or atrialflutter. However, false detection may occur due tofar-field R-wave (Figure 2) oversensing by the atriallead (35–37) or runs of premature atrial complexes.False negative or missed AF has been reported whenepisodes of AF are very brief (35,37). In addition,

FIGURE 1 Mechani
Cardioembolic sourc
embolic material disl
Lung, and Blood Inst
Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
284
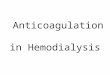
antitachycardia responses of CIEDs are not spe-cific for AF (35,37) and may be triggered by otherforms of AT, including atrial tachycardia or atrialflutter. Thus, intracardiac electrograms (EGMs) mustbe reviewed to verify the accuracy of the device di-agnostics. Device-stored data based solely on markerchannels, without EGMs, cannot be used to verify AFdue to the potential for diagnostic errors caused byoversensing or undersensing by the atrial lead.Furthermore, atrial tachycardia detection rate pro-gramming and the duration of the post-ventricularatrial blanking interval can also influence the num-ber of automatic mode-switching episodes in thesetting of AT (38). Although ICM are also susceptibleto false AF detection due to oversensing or missed AFdetection due to undersensing, 2 ICM with AF algo-rithms (Medtronic Reveal XT, Model 9529, MedtronicInc., Minneapolis, Minnesota, and, SJM ConfirmImplantable Cardiac Monitor Model DM2102, St. JudeMedical, Inc., Sunnyvale, California) are currentlyavailable on the market, with the Medtronic RevealXT reported to have an overall accuracy of 98.5% inAF detection (39) (Figure 3). Although atrial high rateepisodes (AHRE) have been used as a surrogate forAF, the data must be interpreted with caution. In theASSERT (ASymptomatic AF and Stroke Evaluation in
sms of Stroke in Atrial Fibrillation
es, almost exclusively represented by left atrial appendage thrombi, account
odged from thoracic and or carotid plaques, account for the remaining 10% of
itute.
Pacemaker Patients and the AF Reduction AtrialPacing) trial, the positive predictive value of AHREsfor EGM-confirmed AF was examined in 2,850 sub-jects with implanted pacemakers. In 17.3% of cases,AHRE episodes at >190 beats/min lasting >6 minwere found to be falsely positive, due predominantlyto repetitive non–re-entrant ventriculoatrial syn-chrony (40), also known as atrioventricular-desynchronization arrhythmia (Figure 4). Repetitivenon–re-entrant ventriculoatrial synchrony is trig-gered by retrograde ventriculoatrial conduction withfunctional atrial undersensing. It results from retro-grade atrial activation during the post-ventricularatrial refractory period and functional atrial non-capture due to atrial stimulation during the absoluterefractory period, with the potential to trigger modeswitching (41–45).
REVIEW OF PUBLICATIONS ON
DEVICE-DETECTED AF
Because the advent of dual-chamber devices andventricular leads with atrial sensing capability, theclinical implications of device-detected AT have beenconsidered in the context of anticoagulation forstroke prevention (46), but the question of what to
for >90% of embolic events. Noncardioembolic origin, more often
events. Graphics source: National Institutes of Health/National Heart,

FIGURE 2 EGM Representative of AT/AF Due to Far-Field R-Wave Sensing
Far-field R-wavesensing on the atriallead: AR on EGM 1(atrial EGM)correlates with VS onEGM 2 (ventricularEGM). R-wave issensed on the atrialchannel, triggeringfalse AT/AF.
Note: R-R intervalis regular,therefore this isnot AF.
Intracardiac electrogram (EGM) demonstrating sensing of the R-wave on the atrial lead, resulting in false detection of atrial tachycardia
(AT)/atrial fibrillation (AF). AR ¼ atrial refractory event.
J A C C V O L . 6 5 , N O . 3 , 2 0 1 5 Chen-Scarabelli et al.J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4 Device-Detected Atrial Fibrillation
285
do about device-detected AF remains unsettled. TheMOST (MOde Selection) trial in patients with sinusnode dysfunction, the TRENDS study: A ProspectiveStudy of the Clinical Significance of Atrial Arrhyth-mias Detected by Implanted Device Diagnostics, and
FIGURE 3 Implantable Cardiac Monitor Strips Exemplifying True an
False AT/AF triggereddue to PVC
False AT/AF
Examples of true and false detection of atrial tachycardia (AT)/atrial fibril
in a patient with frequent premature ventricular contractions (PVC).
the ASSERT trial are among the more comprehensiveefforts to provide guidance. Although these studiesvaried with regard to rate thresholds for detectionof AT (including AT and AHRE), duration of epi-sodes, and follow-up, an association between these
d False AT/AF
Note: irregularR-R intervals.
True AT/AF
lation (AF) by implantable cardiac monitors. False AT/AF detection due to irregular R-R intervals

Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
286
tachyarrhythmias and risk of ischemic stroke wasconsistently found.
The MOST trial, a 6-year randomized trial of DDDRversus VVIR pacing in patients with sinus nodedysfunction, documented a 50% reduction in newlydiagnosed AF with dual-chamber pacing compared toventricular pacing alone (hazard ratio: 0.50; 95%confidence interval: 0.32 to 0.76; p ¼ 0.001) (47). Asubgroup analysis of 316 patients correlated AHREwith clinical outcomes, but found no significant as-sociation of pacing mode (dual-chamber vs. single-chamber ventricular pacing) on the presence orabsence of AHRE (48). The presence of AHRE (atrialrate >220 beats/min for 10 consecutive beats) was anindependent predictor of mortality (HR: 2.48), deathor nonfatal stroke (HR: 2.79), and AF (HR: 5.93),indicating that pacemaker patients with sinus nodedysfunction and AHRE were more than 2.5 times aslikely to die or have a stroke, and were 6 timesas likely to develop AF than those without AHRE(32). Limitations of this substudy were its retro-spective design, small sample size, and that 81%(129 of 160) of patients with AHRE had prior su-praventricular arrhythmias (32). A prospective studySearch AV Extension and Managed Ventricular Pacingfor Promoting Atrio-Ventricular Conduction (SAVEPACe) measured the time to persistent AF with
FIGURE 4 Example of Automatic Mode-Switching Due to Repetitive
Blue oval: P-wave falls inthe post-ventricular atrialrefractory period and is notsensed [functional atrialundersensing], withsubsequent atrial pacing[in red rectangle] occurringin the absolute refractoryperiod [functional atrialnon-capture].
Electrogram documenting false detection of atrial tachycardia/atrial fibr
falling into the post-ventricular atrial refractory period (functional atria
refractory period (functional noncapture).
dual-chamber minimal ventricular pacing com-pared to conventional dual-chamber pacing (49). Bymeasuring AF with stored diagnostic data fromthe pacemaker, the SAVE PACe trial showed a mod-erate reduction of the risk of persistent AF in patientswith sinus node disease (49). These observationsmotivated a prospective study (TRENDS) to investi-gate the relationship between device-detected AT(including atrial flutter, AF, and atrial tachycardia)and stroke risk (50). The TRENDS study was a pro-spective, observational study of 2,486 patients with1 or more risk factors for stroke who had implanteddevices. Patients with either a low (#5.5 h on anysingle day within a 30-day period) or a high burden ofAT ($5.5 h) had a higher risk of stroke than thosewithout AT (HR: 2.20; 95% CI: 0.96 to 5.05; p ¼ 0.06)(33). However, the difference in hazard ratio betweenthe groups with low and high AHRE burdens wasnot statistically significant (51).
The ASSERT trial evaluated whether detection ofasymptomatic AHRE predicted an increased risk ofstroke and systemic embolism in pacemaker patientswithout a history of AF, as well as whether overdriveatrial pacing would reduce the risk of symptomaticAF (52). Although overdrive atrial pacing failed toreduce the risk of symptomatic AF, subclinical epi-sodes of AT, defined as atrial rates $190 beats/min
Non–Re-Entrant Ventriculoatrial Synchrony
illation due to retrograde ventriculoatrial conduction, with P-wave
l undersensing), with subsequent atrial pacing during the absolute

TABLE 1 CHADS2 and Associated Stroke Risk in the NRAF and ASSERT Trials
NRAF ASSERT
n ¼ 1,733Number ofCVAs (94)
AdjustedStroke Risk n ¼ 259
Number ofCVAs (11)
AdjustedStroke Risk
CHADS2 ¼ 0 120 2 1.9 (1.2–3.0) — — —
CHADS2 ¼ 1 463 17 2.8 (2–3.8) 68 1 2.11 (0.23–18.9)
CHADS2 ¼ 2 523 23 4.0 (3.1–5.1) 119 4 1.83 (0.62–5.4)
Values are n or hazard ratio (95% confidence interval).
ASSERT ¼ ASymptomatic AF and Stroke Evaluation in Pacemaker Patients and the AF Reduction Atrial Pacing;CHADS2 ¼ Congestive heart failure, Hypertension, Age 75 years or older, Diabetes Mellitus, and history of Strokeor transient ischemic attack; CVA ¼ cerebrovascular accident; NRAF ¼ National Registry of Atrial Fibrillation.
TABLE 2 Comparison of Patient Characteristics Between NRAF and ASSERT Trials
NRAF(N ¼ 1,733)
ASSERT (N ¼ 261[With Subclinical AT])
Comparison ofProportions (p Value)
Age, yrs 81 77 � 7
CHF 56% 14.9% <0.0001
HTN 56% —
Male 42% 56.3% <0.0001
Female 58% 43.7% <0.0001
DM 23% 22.6% 0.9487
Prior CVA or TIA 25% 11.9% <0.0001
ASA therapy 31% 61.3% <0.0001
Mean CHADS2 score 2.1 (without aspirin)2.3 (with aspirin)
2.2 � 1.1 0.1711
ASA ¼ acetylsalicylic acid; AT ¼ atrial tachyarrhythmia; CHF ¼ congestive heart failure; DM ¼ diabetes mellitus;HTN ¼ hypertension; TIA ¼ transient ischemic attack; other abbreviations as in Table 1.
J A C C V O L . 6 5 , N O . 3 , 2 0 1 5 Chen-Scarabelli et al.J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4 Device-Detected Atrial Fibrillation
287
lasting >6 min, were associated with an increased riskof ischemic stroke (HR: 1.76; 95% CI: 0.99 to 3.11;p ¼ 0.05). Longer episodes of AT were associated withincremental stroke risk, but AT of 6 to 24 h (HR: 2.00;95% CI: 1.13 to 3.55; p ¼ 0.02) and episodes >24 h(HR: 1.98; 95% CI: 1.11 to 3.51; p ¼ 0.02) carried asimilar risk. Stroke risk increased with the numberof subclinical AT episodes, with annual rates ofTE ranging from 1.20 with a single episode to 1.93with $4 episodes. Subclinical AT was almost 8 timesmore common than clinical AF, which developed in15.7% of patients with subclinical AT. The 2.5-foldgreater risk of TE associated with subclinical AT wasindependent of the appearance of clinical AF andother stroke risk factors (52).
Although the stroke risk on the basis of the CHADS2(Congestive heart failure, Hypertension, Age $ 75years, Diabetes Mellitus, Stroke or transient ischemicattack) score appeared lower in the ASSERT trial thanthat published by Gage et al. (53) (HR of 1.82 in theASSERT trial vs. HR of 4.0 in the NRAF [National Reg-istry of Atrial Fibrillation] trial, for CHADS2 score of 2)(Table 1), the ASSERT trial was a prospective, ran-domized trial with lower-risk patients whereas theNRAF was a registry trial with a higher-risk patientpopulation. Furthermore, the NRAF trial had a greaterpopulation of females, which was not factored intorisk stratification with the CHADS2 score system.However, female sex has been recognized as a riskfactor for cerebrovascular accident and is included inthe currently recommended stroke risk stratificationscheme, CHA2DS2-VASc (54). In addition to a higherproportion of females, the NRAF trial population(in comparison to the ASSERT trial population) hada significantly greater incidence of congestive heartfailure, prior cerebrovascular accident or transientischemic attack, and lower utilization of aspirin ther-apy (all p values <0.0001) (Table 2). Thus, the lowerstroke risk in the ASSERT trial may be due to lower-risk population, despite similar mean CHADS2 scores(2.1 in the NRAF trial vs. 2.2 in the ASSERT trial). Aneditorial accompanying the ASSERT trial contendedthat the hypothesis of causation required AF to pre-cede TE events, along with existence of a time-threshold effect, whereby longer episodes or greaterburden of AT conferred greater risk. Clinical trialswere deemed warranted to determine whether pa-tients with brief, asymptomatic AT had significantstroke risk and whether anticoagulation wouldbenefit this population (55).
The latest clinical trial on device-detected AF isthe IMPACT (Randomized Trial of Anticoagulat-ion Guided by Remote Rhythm Monitoring in Pa-tients With Implanted Cardioverter-Defibrillator and
Resynchronization Devices) trial, which hypothesizedthat remote monitoring for AT with a predefinedanticoagulation plan would prove superior to con-ventional methods for identification of AT withphysician-directed anticoagulation (56). Patients withICDs or CRT defibrillators were randomized 1:1 toeither office visits or remote monitoring for detectionof AT ($200 beats/min for 36 of 48 beats) and, whenAT was detected, an anticoagulation protocol wasinitiated in the intervention group on the basis ofthe CHADS2 risk score. Patients with CHADS2 riskscore #2 were to initiate oral anticoagulation if ATlasted $48 h, with discontinuation if there wereno AT recurrences detected for 30 days. Those withCHADS2 scores of $3 to 4 would initiate anti-coagulation for device-detected AT $24 h in 2 days,with discontinuation if there were no AT recurrencesdetected for 90 days. Those with CHADS2 scores $5to 6, or with a history of TE were prescribed anti-coagulant therapy for any AT, without discontinua-tion, regardless of AT recurrence. Exclusion criteriaincluded a history of stroke, transient ischemicattack, or systemic embolism, and documented AFor atrial flutter. A total of 2,718 patients were

Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
288
enrolled, with no significant differences in baselinedemographics between the 2 groups, except that aslightly higher percent of the intervention arm wastreated with antiplatelet drugs other than aspirin(34.5% vs. 30.7%; p ¼ 0.037). The incidence of AT wassimilar for the 2 groups (33.2%, control vs. 36.3%,interventional group; p ¼ 0.09), and adjudication ofdevice-based atrial EGMs verified 60.5% of AT eventsas AF, 30% as atrial flutter, and the remaining 9.5% asfalse positive, with no significant differences betweengroups. Patients were followed up to 5 years, whenthe Data Monitoring Committee recommended trialtermination on the basis of failure to demonstrate ameaningful difference in outcome with the inter-ventional strategy.
During a median follow-up of 701 days, 225 pa-tients in the control group met criteria for oral anti-coagulation versus 126 in the intervention group.There were no statistically significant differencesbetween groups in the proportion of patients startingor stopping anticoagulant agents, nor in the meanduration of anticoagulant therapy. However, theintervention group started treatment earlier (mean 3vs. 54 days; p < 0.001), indicating that remotemonitoring facilitated earlier intervention for AT.Nonetheless, there was no significant difference be-tween groups in the primary outcome, which was thecomposite of ischemic stroke, systemic embolic, andmajor hemorrhagic events, or in all-cause mortality.Although compliance with the oral anticoagulationprotocol in the interventional group was suboptimal,the overall primary event rate was low. The in-vestigators concluded that initiation of oral antico-agulant therapy on the basis of device-detected AFand subsequent discontinuation of therapy on thebasis of the absence of AT did not improve clinicaloutcomes in these patients with implanted ICD orCRT defibrillators. Despite an association between agreater burden of AT, duration of AT, and TE in thecontrol group, which was attenuated in the inter-vention group, there was no temporal relationshipbetween device-detected AT and clinical TE (56).
TEMPORAL ASSOCIATION BETWEEN
DEVICE-DETECTED AT/AF AND STROKE
Several studies have examined the temporal rela-tionship between device-detected AT and TE events.A subgroup analysis of the TRENDS trial found notemporal association between AHRE and stroke (34)and observations in the ASSERT trial were similar(Figure 5) (57). Among patients with heart failure andCRT devices, those with AHRE (atrial rates >180beats/min lasting $3.8 h/day were 9 times more likely
to develop TE (p ¼ 0.006). However, in the majorityof patients (73%), there was no temporal relationshipbetween AHRE and ischemic events, with a meaninterval of 46.7 � 71.9 days (range 0 to 194 days)before the TE complication (58). Even patients withAHRE #3.8 h/day displayed a trend toward increasedrisk of TE (HR: 4.3; p ¼ 0.11) (48). In studies prior toIMPACT, the use of anticoagulant therapy was un-controlled, potentially attenuating a relationship be-tween AT and clinical TE. In the CRYSTAL-AF trial,implanted cardiac monitoring showed that clinicallymeaningful AF was present in a substantial propor-tion of CS patients (18) and that these AF episodeswould be missed by intermittent rhythm monitoring(18). In contrast, a recent preliminary report from anational cohort of CIED patients with acute strokesuggested that 72% of these patients had either newlydetected or increasing AT/AF burdens just prior tothe stroke event (59).
The absence of a temporal relationship betweensubclinical AF and stroke in studies of patients withCIEDs parallels the relatively infrequent detection ofAF in patients within the 30 days preceding stroke(57). In the AFFIRM (Atrial Fibrillation Follow-upInvestigation of Rhythm Management) study, a mul-ticenter comparison of high-risk patients with AFwho were randomized to sinus rhythm control or arate control strategy, an analysis of the occurrenceand characteristics of stroke events showed a strongrelationship between the presence of AF and the riskof stroke (60).
ANTICOAGULATION FOR AF:
EFFECTS ON STROKE PREVENTION,
STROKE SEVERITY, AND MORTALITY
The benefits of therapeutic anticoagulation in patientswith AF are multifaceted, including not only strokeprevention, but also reduction of stroke severityand mortality (61,62). Anticoagulation with warfarinreduced stroke severity or death in patients with AF bynearly 50% (63). Underutilization of anticoagulationtherapy for stroke prevention in AF is a pervasiveproblem perpetuated by clinician inertia. Analysis ofthe Canadian Stroke Network registry revealed thatamong AF patients admitted with a first ischemicstroke, only 10% were anticoagulated, 60% suffereddisabling strokes, and 20% were fatal (64).
The management of patients with device-detectedAT remains controversial, and uncertainties surroundthe duration of the longest episode of AT, cumula-tive duration of AT, and individual stroke risk, onthe basis of the current stroke risk classificationschemes for nonvalvular AF, the CHADS2 (53,65) or

FIGURE 5 Summary of AT/AF Burden Per Day Relative to Onset of Cerebrovascular Events/Systemic Emboli From the TRENDS Study
101
01
0240
240
240
240
240
240
240
240
240
240
240
240
240
240
2401
0-30 -24 -18 -12 -6 0 6 12 18 24 30
20
1
1
1
1
2
2 None
ASA
None
None
None
None
None
ASA
OAC
OAC
ASA
ASA
ASA
ASA
ASA
ASA
OAC/ASA
OAC/ASA
OAC/ASA
OAC/ASA
2
2
2
2
2
3
3
3
3
3
3
4
4
4
4
5
5
5
6
6
7
8
9
10
11
12
13
14
15
16
18
19
20
17
Patient # CHADS2Score
BaselineAntithrombotic
Therapy
AT/A
F Bu
rden
(Hou
rs/D
ay)
Months From CVE
Each row in the graph represents the data extracted from the implanted device for each of the 20 patients. Reproduced with permission from
Daoud et al. (34). ASA ¼ acetylsalicylic acid (aspirin); AT/AF ¼ atrial tachycardia/atrial fibrillation; CVE ¼ cerebrovascular events; OAC ¼ oral
anticoagulant.
J A C C V O L . 6 5 , N O . 3 , 2 0 1 5 Chen-Scarabelli et al.J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4 Device-Detected Atrial Fibrillation
289
CHA2DS2VASc scores (54,66,67). The 2012 EuropeanSociety of Cardiology guideline update (68) and the2014 American Heart Association/American College ofCardiology/Heart Rhythm Society Guideline forManagement of Patients with Atrial Fibrillation (69)both recommend using the CHA2DS2VASc score toassess stroke risk in patients with nonvalvular AF,whereas the American College of Chest Physicians(70) and the Canadian Cardiovascular Society (71)both recommended the CHADS2 score (Figure 6). Ajoint collaboration between the Atrial FibrillationCompetence NETwork/European Heart Rhythm
Association issued the following consensus state-ment: “It should be considered that AF burden rep-resents a heterogeneous entity; for example, manyshort episodes of AHRE could result in the same AFburden as a single long-standing episode, and mayhave different biological effect on atrial electricaland contractile function, and on remodeling andcoagulation processes” (72).
If patients had incidentally detected asymptomaticAF on office electrocardiograms, Holter monitoring,or event monitors, the decision to anticoagulatefor stroke prevention would be undisputed and on

FIGURE 6 Compar
European SCardiology
oral anticoagu[NOACs preferr
[antiplatelet theraponly for those pat
oral anticoagul
CHA2DS2
CHA2DS2-V
CHA2DS2-Vno antithromb
recomm
Differences among v
compared to CHA2DS
Society (AHA/ACC/H
Diabetes Mellitus, an
and diabetes mellitus
Stroke/Transient Isch
years to 74 years, Se
CKD ¼ chronic kidne
Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
290
the basis of the risk of stroke and bleeding. Moni-toring atrial activity continuously with implanteddevices (which are arguably more accurate than sur-face monitors) inexplicably tends to promote a wait-and-see approach for many clinicians who prefer tocontinue surveillance for additional or longer epi-sodes, even though stroke risk is independent ofsymptoms in patients with AF.
Reasons for a lack of consensus on management ofdevice-detected AT vary, some clinicians justifyinginertia on the basis of the lack of evidence to supportprophylactic anticoagulation. Others, given the lackof temporal association between AT and stroke,
ison of Cardiovascular Society Guidelines for Antithrombotic Therapy in N
ociety of (2012)
lant therapyed over VKA]
y recommendedients who refuseant therapy]
AHA/ACC/HRS (2014)
[no antithrombotic therapy,or treatment with an oral
anticoagulant or aspirin maybe considered]
oral anticoagulant therapyrecommended
[VKA is reasonable in patientswith end-stage CKD (creatinineclearance [CrCl] <15 mL/min)
or are on hemodialysis]
AmerPhysi
no an
combinaand clo
only unsuitab
to take
-VASc CHA2DS2-VASc
ASc ≥1 CHA2DS2-VASc = 1
CHA2DS2-VASc ≥ 2
ASc = 0,otic therapyended
CHA2DS2-VASc = 0,no antithrombotic therapy
recommended
NOAC[dabigapreferr
[oral apreferrerecomm
deemed unto take
arious society guidelines, with use of CHADS2 score by the American College
2VASc score recommended by the European Society of Cardiology and Amer
RS), along with the threshold for anticoagulation recommendation. CHADS2d history of Stroke or transient ischemic attack [TIA] [Scoring: 1 point each for
, 2 points for a history of stroke or TIA]; CHA2DS2VASc ¼ Congestive Heart Fai
emic Attack/Thromboembolism (2 points), Vascular disease (includes prior my
x category (i.e. female sex) (1 point for each risk factor, except 2 points for age
y disease; INRs ¼ international normalized ratio; NOACs ¼ novel oral anticoa
rationalize that the mechanism of stroke in patientswith device-detected AT may not involve cardiogenicembolism and propose that AF may be a markerof a patient population at risk of stroke, rather thanthe proximate cause, possibly related to athero-thrombosis, hypertension, or other sources andetiologies (51,67). Although intriguing, this interpre-tation clashes with the findings of the multicenterPROTECT AF study, which established that the “local”strategy of LAA closure is noninferior to “systemic”anticoagulation with warfarin and, for the first time,implicated the LAA in the pathogenesis of stroke in AF(27). Despite the robust association between AHRE
onvalvular Atrial Fibrillation
ican College of Chestcians [ACCP] (2012)
CHADS2
CHADS2 = 0,tithrombotic therapyrecommended
CHADS2 = 1
CHADS2 ≥ 2
tion therapy with aspirinpidogrel recommendedfor patients deemedle for or who choose not an oral anticoagulant
Canadian CV Society (2014)
CHADS2
Antiplatelet therapy (aspirin)recommended if coronary artery
disease or arterial vascular disease(coronary, aortic, or peripheral
artery disease) and age is < 65 years
oral anticoagulant therapyrecommended if age ≥ 65 yrs, or ifprior stroke or TIA, hypertension,
diabetes, or heart failure
NOACs preferred over VKA
CHADS2 ≥ 1
CHADS2 = 0,no antithrombotic therapy
recommended if no vascular disease
preferred over VKAtran 150 mg twice dailyed over adjusted-doseVKA therapy]
nticoagulant therapyd; antiplatelet therapyended only for patientssuitable for or choose not
an oral anticoagulant]
of Chest Physicians and the Canadian Cardiovascular (CV) Society,
ican Heart Association/American College of Cardiology/Heart Rhythm
¼ Congestive heart failure, Hypertension, Age 75 years or older,
any of the following–recent CHF, hypertension, age 75 years or older,
lure, Hypertension, Age 75 years or older (2 points), Diabetes Mellitus,
ocardial infarction, peripheral artery disease, or aortic plaque), Age 65
75 years or older, and 2 points for stroke, TIA, or thromboembolism);
gulant(s); VKA ¼ vitamin K antagonist.

CENTRAL ILLUSTRATION Device-Detected Atrial Fibrillation
Detection of atrial fibrillation by a cardiac implantable electronic device and potential
risk for stroke.
J A C C V O L . 6 5 , N O . 3 , 2 0 1 5 Chen-Scarabelli et al.J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4 Device-Detected Atrial Fibrillation
291
and stroke, many clinicians renege on the clinicalguidelines for management of AF, citing lack ofknowledge regarding benefit in anticoagulation forsubclinical AT/AF. “The net benefit of antithrombotictreatment is well established in patients with clinicalatrial fibrillation, but there may not be a similar benefitin patients with subclinical atrial tachyarrhythmias;therefore, a randomized trial of anticoagulant therapyin patients with subclinical atrial tachyarrhythmias isdesirable” (52). However, given the current knowl-edge that stroke risk is independent of whether AT/AFis symptomatic or subclinical, a randomized clinicaltrial of anticoagulant therapy in subclinical AT mayfall under ethical scrutiny.
CURRENT CLINICAL PRACTICES IN
SUBCLINICAL AT/AF
Fewer than 25% of patients with stroke riskfactors and device-detected AT are treated withanticoagulation (20). In a retrospective study of 445pacemaker patients from a single academic hospital,there was a 50% incidence of pacemaker-detected AF.However, there was a significantly lower usage ofanticoagulant therapy in patients with subclinicalpacemaker-detected AF than in patients with clinicalAF (23.7% vs. 58.9%; p < 0.001) (20). Similar un-derutilization of anticoagulant therapy was alsoreported in a pacemaker clinic study in which only61.3% of patients with device-detected AF wereanticoagulated, despite a mean CHADS2 score $2 (73).
Analysis of management patterns and clinical out-comes in patients with AF in Canada and the UnitedStates in the AFFIRM trial database (74) revealed that,despite comparable use of warfarin at randomization,Canadians with AF were more often treated withwarfarin to therapeutic intensity during the follow-upperiod. After adjusting for differences in baselinecharacteristics, mortality was lower among Canadianpatients with AF than their counterparts in the UnitedStates (HR: 0.70; p ¼ 0.02) (73). In Europe, an elec-tronic survey of practice in management of patientswith silent AF among European Heart Rhythm Asso-ciation Research Network partners from 33 centers in16 countries revealed a strong consensus for oralanticoagulant therapy in patients with silent AF,including those with pacemaker-detected AF, withmost responders considering device-detected AF assufficient evidence to warrant anticoagulation (75).
CONCLUSIONS
Despite multiple studies (the MOST, TRENDS, andASSERT trials, and the study of AHRE events on
continuous home monitoring and stroke risk) allsupporting an association between device-detectedAT/AF and stroke, and updated guidelines for AFmanagement, specific recommendations for device-detected subclinical AF are lacking, instead deferringto risk stratification on the basis of the CHA2DS2-VAScscoring system (69) to determine whether patientsshould be anticoagulated. Of note, the updatedguidelines for management of AF, developed jointlyby the American Heart Association, the AmericanCollege of Cardiology, and the Heart Rhythm Society,and in collaboration with the Society of ThoracicSurgeons, advocate against the implementation ofbleeding-risk scoring systems, although guidance isprovided for certain high-risk populations, such aspatients with end-stage renal disease. Risks andbenefits of anticoagulation, along with the risk ofstroke, should be extensively discussed with thepatient to enable a knowledgeable decision.
The results of the ASSERT trial (52) and a morerecent study (67) cast doubt on a critical threshold

Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
292
for AHRE burden. Instead, conventional clinical riskfactors may be more important in determining theneed for anticoagulation (48). Hence, the decisionabout prophylactic anticoagulation therapy shouldnot be delayed awaiting further elucidation ofthe mechanisms and relationships between device-detected AF and TE. The most recent clinicalpractice guidelines (69) acknowledge “clinically un-recognized and asymptomatic AF as a potentiallyimportant cause of stroke,” but conclude that “addi-tional studies are needed to further clarify the rela-tionship between stroke risk and atrial high-rateepisodes detected by implanted devices and to definekey characteristics of atrial high-rate episodes in pa-tients who warrant further investigation or potentiallytherapy.” Do we really need to know how much silentAF is too much and what duration is long enoughbefore we can implement stroke-prevention strate-gies? Given the frequency of AF in the population,especially in those with underlying heart diseasewho have pacemakers and other CIEDs, can we affordto withhold treatment for stroke prevention? The goalof anticoagulation in AF is primary prevention ofstroke. Thus, once AF is detected, regardless of themechanism of detection, anticoagulation should beinitiated if indicated on the basis of stroke riskassessment using the CHA2DS2-VASc score. Devicediagnostics from CIEDs provide a unique opportunityfor early intervention and prevention of stroke(Central Illustration). In fact, remote cardiac devicemonitoring, has been shown to lead to improvedclinical outcomes due to earlier detection and in-tervention, with reduced emergency room visits,increased efficiency for healthcare providers, andimproved quality of care for patients with CIEDs(76). As clinicians, we cannot afford to waste thisrare occasion to try to prevent strokes. Clinicianswith access to such device diagnostics have an
inherent responsibility to act on such informationgleaned from device diagnostics, with potentiallegal ramifications for those who fail to act. Anti-coagulation is too often unjustifiably underutilizedin those patients at the greatest risk for stroke: elderlypatients (77).
To the best of our knowledge, there are no pub-lished trials investigating whether AF-related strokerisk varies on the basis of whether AF is detectedby 12-lead ECG, Holter, or event monitor (all ofwhich require clinical adjudication for verificationof accurate arrhythmia diagnosis), nor whether an-ticoagulation efficacy varies on the basis of methodof AF detection. Thus, stroke risk and anticoagula-tion recommendations are not delineated on thebasis of method of AF detection. The reluctance ofclinicians to act on device-detected AF is bewil-dering, as many would not hesitate to act on a singlestandard 12-lead ECG that records 10 s of rhythm.This discrimination against CIED-detected asymp-tomatic AF is unfounded, and the delay by cliniciansto implement anticoagulation in device-detected AFignores the clinical guidelines and is an injustice topatients. Such failure represents a lost opportunityby clinicians to have clinically meaningful discus-sions and shared decision-making with their patientsabout AF, the associated risk of cerebrovascularaccident, and the importance of anticoagulationin stroke prevention. The time is now to preventstroke in patients with asymptomatic AF . . . time isbrain! (3).
RESEARCH REQUESTS AND CORRESPONDENCE: Dr.Tiziano M. Scarabelli, Zena and Michael A. WienerCardiovascular Institute, Mount Sinai Medical Center,One Gustave L. Levy Place, Box 1030, New York,New York 10029-6574. E-mail: [email protected].
RE F E RENCE S
1. Go AS, Mozaffarian D, Roger VL, et al., for theAmerican Heart Association Statistics Committeeand Stroke Statistics Subcommittee. Heart diseaseand stroke statistics–2014 update: a report fromthe American Heart Association. Circulation 2014;129:e28–292.
2. Andrade J, Khairy P, Dobrev D, et al. The clinicalprofile and pathophysiology of atrial fibrillation:relationships among clinical features, epidemi-ology, andmechanisms. Circ Res 2014;114:1453–68.
3. National Stroke Association. NSAFactSheet_Afib_2013. 2013. Available at: http://www.stroke.org/sites/default/files/resources/NSA_FactSheet_Afib_2014.pdf. Accessed November 7, 2014.
4. Colilla S, Crow A, Petkun W, et al. Estimates ofcurrent and future incidence and prevalence of
atrial fibrillation in the U.S. adult population. AmJ Cardiol 2013;112:1142–7.
5. Krijthe BP, Kunst A, Benjamin EJ, et al. Pro-jections on the number of individuals with atrialfibrillation in the European Union, from 2000to 2060. Eur Heart J 2013;34:2746–51.
6. Chugh SS, Havmoeller R, Narayanan K, et al.Worldwide epidemiology of atrial fibrillation: aGlobal Burden of Disease 2010 Study. Circulation2014;129:837–47.
7. Shen MJ, Zipes DP. Role of the autonomicnervous system in modulating cardiac arrhythmias.Circ Res 2014;114:1004–21.
8. Nattel S, Harada M. Atrial remodeling andatrial fibrillation: recent advances and translational
perspectives. J Am Coll Cardiol 2014;63:2335–45.
9. Wijffels MC, Kirchhof CJ, Dorland R, et al. Atrialfibrillation begets atrial fibrillation. A study inawake chronically instrumented goats. Circulation1995;92:1954–68.
10. Rostock T, Steven D, Lutomsky B, et al. Atrialfibrillation begets atrial fibrillation in the pulmo-nary veins: on the impact of atrial fibrillation onthe electrophysiological properties of the pulmo-nary veins in humans. J Am Coll Cardiol 2008;51:2153–60.
11. TeamAFib. What is Atrial Fibrillation? Boeh-ringer Ingelheim Pharmaceuticals Inc. 2013.Available at: https://www.teamafib.com/about-afib/what-is-afib/. Accessed November 7, 2014.

J A C C V O L . 6 5 , N O . 3 , 2 0 1 5 Chen-Scarabelli et al.J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4 Device-Detected Atrial Fibrillation
293
12. Jorgensen HS, Nakayama H, Reith J, et al.Stroke recurrence: predictors, severity, and prog-nosis. The Copenhagen Stroke Study. Neurology1997;48:891–5.
13. The effect of low-dose warfarin on the riskof stroke in patients with nonrheumatic atrialfibrillation. The Boston Area Anticoagulation Trialfor Atrial Fibrillation Investigators. N Engl J Med1990;323:1505–11.
14. Ezekowitz MD, James KE, Nazarian SM, et al.Silent cerebral infarction in patients with non-rheumatic atrial fibrillation. The Veterans AffairsStroke Prevention in Nonrheumatic Atrial Fibrilla-tion Investigators. Circulation 1995;92:2178–82.
15. Connolly SJ, Laupacis A, Gent M, et al.Canadian Atrial Fibrillation Anticoagulation (CAFA)Study. J Am Coll Cardiol 1991;18:349–55.
16. Go AS, Hylek EM, Chang Y, et al. Anti-coagulation therapy for stroke prevention inatrial fibrillation: how well do randomized trialstranslate into clinical practice? JAMA 2003;290:2685–92.
17. Salazar CA, del Aguila D, Cordova EG. Directthrombin inhibitors versus vitamin K antagonistsfor preventing cerebral or systemic embolism inpeople with non-valvular atrial fibrillation.Cochrane Database Syst Rev 2014;3:Cd009893.
18. Sanna T, Diener HC, Passman RS, et al., for theCRYSTAL AF Investigators. Cryptogenic stroke andunderlying atrial fibrillation. N Engl J Med 2014;370:2478–86.
19. Gladstone DJ, Spring M, Dorian P, et al., forthe EMBRACE Investigators and Coordinators.Atrial fibrillation in patients with cryptogenicstroke. N Engl J Med 2014;370:2467–77.
20. Healey JS, Martin JL, Duncan A, et al.Pacemaker-detected atrial fibrillation in patientswith pacemakers: prevalence, predictors, andcurrent use of oral anticoagulation. Can J Cardiol2013;29:224–8.
21. Watson T, Shantsila E, Lip GY. Mechanismsof thrombogenesis in atrial fibrillation: Virchow’striad revisited. Lancet 2009;373:155–66.
22. Iwasaki YK, Nishida K, Kato T, et al. Atrialfibrillation pathophysiology: implications formanagement. Circulation 2011;124:2264–74.
23. Blackshear JL, Pearce LA, Hart RG, et al. Aorticplaque in atrial fibrillation: prevalence, predictors,and thromboembolic implications. Stroke 1999;30:834–40.
24. Al-Saady NM, Obel OA, Camm AJ. Left atrialappendage: structure, function, and role inthromboembolism. Heart 1999;82:547–54.
25. Sievert H, Lesh MD, Trepels T, et al. Percu-taneous left atrial appendage transcatheterocclusion to prevent stroke in high-risk patientswith atrial fibrillation: early clinical experience.Circulation 2002;105:1887–9.
26. Holmes DR, Reddy VY, Turi ZG, et al. Percu-taneous closure of the left atrial appendageversus warfarin therapy for prevention ofstroke in patients with atrial fibrillation: arandomised non-inferiority trial. Lancet 2009;374:534–42.
27. Reddy VY, Doshi SK, Sievert H, et al., for thePROTECT AF Investigators. Percutaneous left
atrial appendage closure for stroke prophylaxis inpatients with atrial fibrillation: 2.3-Year Follow-upof the PROTECT AF (Watchman Left AtrialAppendage System for Embolic Protection inPatients with Atrial Fibrillation) Trial. Circulation2013;127:720–9.
28. Holmes DR Jr., Kar S, Price MJ, et al. Pro-spective randomized evaluation of the WatchmanLeft Atrial Appendage Closure device in patientswith atrial fibrillation versus long-term warfarintherapy: the PREVAIL trial. J Am Coll Cardiol 2014;64:1–12.
29. FDA Executive Summary. Boston ScientificWatchman Left Atrial Appendage ClosureTherapy. Food and Drug Administration. Availableat: http://www.fda.gov/downloads/advisorycommittees/committeesmeetingmaterials/medicaldevices/medicaldevicesadvisorycommittee/circulatorysystemdevicespanel/ucm419373.pdf. AccessedNovember 27, 2014.
30. Di Biase L, Santangeli P, Anselmino M, et al.Does the left atrial appendage morphologycorrelate with the risk of stroke in patients withatrial fibrillation? Results from a multicenterstudy. J Am Coll Cardiol 2012;60:531–8.
31. Anselmino M, Scaglione M, Di Biase L, et al.Left atrial appendage morphology and silentcerebral ischemia in patients with atrial fibrillation.Heart Rhythm 2014;11:2–7.
32. Glotzer TV, Hellkamp AS, Zimmerman J, et al.,for the MOST Investigators. Atrial high rate epi-sodes detected by pacemaker diagnostics predictdeath and stroke: report of the Atrial DiagnosticsAncillary Study of the MOde Selection Trial(MOST). Circulation 2003;107:1614–9.
33. Glotzer TV, Daoud EG, Wyse DG, et al. Therelationship between daily atrial tachyarrhythmiaburden from implantable device diagnostics andstroke risk: the TRENDS study. Circ ArrhythmElectrophysiol 2009;2:474–80.
34. Daoud EG, Glotzer TV, Wyse DG, et al., for theTRENDS Investigators. Temporal relationship ofatrial tachyarrhythmias, cerebrovascular events,and systemic emboli based on stored device data:a subgroup analysis of TRENDS. Heart Rhythm2011;8:1416–23.
35. Plummer CJ, Henderson S, Gardener L, et al.The use of permanent pacemakers in the detectionof cardiac arrhythmias. Europace 2001;3:229–32.
36. Purerfellner H, Gillis AM, Holbrook R, et al.Accuracy of atrial tachyarrhythmia detection inimplantable devices with arrhythmia therapies.Pacing Clin Electrophysiol 2004;27:983–92.
37. Plummer CJ, McComb JM, STOP AF Trial.Detection of atrial fibrillation by permanentpacemakers: observations from the STOP AF trial.Cardiac Electrophysiol Rev 2003;7:333–40.
38. de Voogt WG, van Hemel NM, van de Bos AA,et al. Verification of pacemaker automatic modeswitching for the detection of atrial fibrillation andatrial tachycardia with Holter recording. Europace2006;8:950–61.
39. Hindricks G, Pokushalov E, Urban L, et al.,for the XPECT Trial Investigators. Performanceof a new leadless implantable cardiac monitor indetecting and quantifying atrial fibrillation:
Results of the XPECT trial. Circ Arrhythm Elec-trophysiol 2010;3:141–7.
40. Kaufman ES, Israel CW, Nair GM, et al., for theASSERT Steering Committee and Investigators.Positive predictive value of device-detected atrialhigh-rate episodes at different rates and dura-tions: an analysis from ASSERT. Heart Rhythm2012;9:1241–6.
41. Barold SS, Levine PA. Pacemaker repetitivenonreentrant ventriculoatrial synchronousrhythm. A review. J Interv Card Electrophysiol2001;5:45–58.
42. Francis J. Repetitive Nonreentrant Ven-triculoatrial Synchrony (RNRVAS). Indian PacingElectrophysiol J 2010;10:203–4.
43. Barold SS. Repetitive reentrant and non-reentrant ventriculoatrial synchrony in dualchamber pacing. Clinical Cardiol 1991;14:754–63.
44. Mulpuru SK, Saponieri C. Multiple episodes ofpresyncope in a pacemaker dependent patient:what is the diagnosis? Indian Pacing ElectrophysiolJ 2010;10:233–5.
45. Barold SS, Stroobandt RX, Van Heuverswyn F.Pacemaker repetitive nonreentrant ventriculoatrialsynchrony. Why did automatic mode switchingoccur? J Electrocardiol 2012;45:420–5.
46. Sparks PB, Mond HG, Kalman JM, et al. Atrialfibrillation and anticoagulation in patients withpermanent pacemakers: implications for strokeprevention. Pacing Clin Electrophysiol 1998;21:1258–67.
47. Lamas GA, Lee KL, Sweeney MO, et al., for theMode Selection Trial in Sinus-Node Dysfunction.Ventricular pacing or dual-chamber pacing forsinus-node dysfunction. N Engl J Med 2002;346:1854–62.
48. Healey JS. Device-detected atrial tachyar-rhythmias: what do we know? Europace 2012;14:157–8.
49. Sweeney MO, Bank AJ, Nsah E, et al., for theSearch AV Extension and Managed VentricularPacing for Promoting Atrioventricular Conduction(SAVE PACe) Trial. Minimizing ventricular pacingto reduce atrial fibrillation in sinus-node disease. NEngl J Med 2007;357:1000–8.
50. Glotzer TV, Daoud EG, Wyse DG, et al. Ratio-nale and design of a prospective study of theclinical significance of atrial arrhythmias detectedby implanted device diagnostics: the TRENDSstudy. J Interv Card Electrophysiol 2006;15:9–14.
51. Viles-Gonzalez JF, Halperin JL. Everythingcounts in large amounts: device-detected atrialhigh-rate arrhythmias. Circ Arrhythm Electro-physiol 2009;2:471–3.
52. Healey JS, Connolly SJ, Gold MR, et al., for theASSERT Investigators. Subclinical atrial fibrillationand the risk of stroke. N Engl J Med 2012;366:120–9.
53. Gage BF, Waterman AD, Shannon W, et al.Validation of clinical classification schemes forpredicting stroke: results from the National Reg-istry of Atrial Fibrillation. JAMA 2001;285:2864–70.
54. Lip GY, Nieuwlaat R, Pisters R, et al. Refiningclinical risk stratification for predicting stroke andthromboembolism in atrial fibrillation using a

Chen-Scarabelli et al. J A C C V O L . 6 5 , N O . 3 , 2 0 1 5
Device-Detected Atrial Fibrillation J A N U A R Y 2 7 , 2 0 1 5 : 2 8 1 – 9 4
294
novel risk factor-based approach: the euro heartsurvey on atrial fibrillation. Chest 2010;137:263–72.
55. Lamas G. How much atrial fibrillation is toomuch atrial fibrillation? N Engl J Med 2012;366:178–80.
56. Halperin JL, Waldo A, Ip J, et al., forthe IMPACT Investigators. Randomized trial ofanticoagulation guided by remote rhythm moni-toring in patients with implanted cardioverter-defibrillator and resynchronization devices. Paperpresented at: ACC 63rd Annual Scientific Sessionsand Expo; March 29, 2014; Washington, DC.
57. Brambatti M, Connolly SJ, Gold MR, et al., forthe ASSERT Investigators. Temporal relationshipbetween subclinical atrial fibrillation and embolicevents. Circulation 2014;129:2094–9.
58. Shanmugam N, Boerdlein A, Proff J, et al.Detection of atrial high-rate events by continuoushome monitoring: clinical significance in the heartfailure-cardiac resynchronization therapy popula-tion. Europace 2012;14:230–7.
59. Turakhia MP ZP, Bucksa A, Xu X, et al. Atrialarrhythmia burden increases just proximal tostroke: insights from remote monitoring in anational health care system. Paper presented atHeart Rhythm Society Scientific Sessions; May 8,2014; San Francisco, California.
60. Sherman DG, Kim SG, Boop BS, et al. Occur-rence and characteristics of stroke events in theAtrial Fibrillation Follow-up Investigation of SinusRhythm Management (AFFIRM) study. Arch InternMed 2005;165:1185–91.
61. Hylek EM, Go AS, Chang Y, et al. Effect of in-tensity of oral anticoagulation on stroke severityand mortality in atrial fibrillation. N Engl J Med2003;349:1019–26.
62. Schwammenthal Y, Bornstein N, Schwam-menthalE, et al. Relationof effectiveanticoagulationin patients with atrial fibrillation to stroke severityand survival (from the National Acute Stroke IsraeliSurvey [NASIS]). Am J Cardiol 2010;105:411–6.
63. O’Donnell M, Oczkowski W, Fang J, et al., forthe Investigators of the Registry of the CanadianStroke Network. Preadmission antithrombotictreatment and stroke severity in patients with
atrial fibrillation and acute ischaemic stroke: anobservational study. Lancet Neurol 2006;5:749–54.
64. Gladstone DJ, Bui E, Fang J, et al. Potentiallypreventable strokes in high-risk patients withatrial fibrillation who are not adequately anti-coagulated. Stroke 2009;40:235–40.
65. Gage BF, van Walraven C, Pearce L, et al.Selecting patients with atrial fibrillation for anti-coagulation: stroke risk stratification in patientstaking aspirin. Circulation 2004;110:2287–92.
66. Olesen JB, Lip GY, Hansen ML, et al. Validationof risk stratification schemes for predicting strokeand thromboembolism in patients with atrialfibrillation: nationwide cohort study. BMJ 2011;342:d124.
67. Lip GY, Frison L, Halperin JL, et al. Identifyingpatients at high risk for stroke despite anti-coagulation: a comparison of contemporary strokerisk stratification schemes in an anticoagulatedatrial fibrillation cohort. Stroke 2010;41:2731–8.
68. Camm AJ, Lip GY, De Caterina R, et al. ESCCommittee for Practice Guidelines (CPG). 2012focused update of the ESC Guidelines for themanagement of atrial fibrillation: an update of the2010 ESC Guidelines for the management of atrialfibrillation. Developed with the special contribu-tion of the European Heart Rhythm Association.Eur Heart J 2012;33:2719–47.
69. January CT, Wann LS, Alpert JS, et al. 2014AHA/ACC/HRS Guideline for the Managementof Patients With Atrial Fibrillation: A Report ofthe American College of Cardiology/AmericanHeart Association Task Force on PracticeGuidelines and the Heart Rhythm Society. J AmColl Cardiol 2014;64:e1–76.
70. You JJ, Singer DE, Howard PA, et al., for theAmerican College of Chest Physicians. Antith-rombotic therapy for atrial fibrillation: Antith-rombotic Therapy and Prevention of Thrombosis,9th ed: American College of Chest Physicians Ev-idence-Based Clinical Practice Guidelines. Chest2012;141 Suppl 2:e531S–75S.
71. Verma A, Cairns JA, Mitchell LB, et al., forthe CCS Atrial Fibrillation Guidelines Committee.2014 focused update of the Canadian
cardiovascular society guidelines for the manage-ment of atrial fibrillation. Can J Cardiol 2014;30:1114–30.
72. Kirchhof P, Lip GY, Van Gelder IC, et al.Comprehensive risk reduction in patients withatrial fibrillation: emerging diagnostic and thera-peutic options–a report from the 3rd Atrial Fibril-lation Competence NETwork/European HeartRhythm Association consensus conference.Europace 2012;14:8–27.
73. Cabrera S, Mercé J, de Castro R, et al. Pace-maker clinic: an opportunity to detect silent atrialfibrillation and improve antithrombotic treatment.Europace 2011;13:1574–9.
74. O’Hara GE, Charbonneau L, Chandler M, et al.,for the AFFIRM Investigators. Comparison ofmanagement patterns and clinical outcomes inpatients with atrial fibrillation in Canada and theUnited States (from the analysis of the AtrialFibrillation Follow-up Investigation of RhythmManagement [AFFIRM] database). Am J Cardiol2005;96:815–21.
75. Dobreanu D, Svendsen JH, Lewalter T, et al.,for the Scientific Initiatives Committee, EuropeanHeart Rhythm Association. Current practice fordiagnosis and management of silent atrial fibril-lation: results of the European Heart Rhythm As-sociation survey. Europace 2013;15:1223–5.
76. Landolina M, Perego GB, Lunati M, et al.Remote monitoring reduces healthcare useand improves quality of care in heart failure pa-tients with implantable defibrillators: the evo-lution of management strategies of heartfailure patients with implantable defibrillators(EVOLVO) study. Circulation 2012;125:2985–92.
77. Casciano JP, Dotiwala ZJ, Martin BC, et al.The costs of warfarin underuse and nonadherencein patients with atrial fibrillation: a commercialinsurer perspective. J Manag Care Pharm 2013;19:302–16.
KEY WORDS atrial tachyarrhythmias,cardiac implantable electronic devices,cerebral embolism, defibrillator,implantable cardiac monitor, stroke

![AMARANTHUS SPINOSUS PAST, PRESENT AND FUTUREthe treatment of vomiting, abdominal pain, hysteria, tonsillitis, malaria, dysentery, dysurea, chicken pox, fever, and mania.[23,24] A](https://img.pdfslide.us/doc/110x75/5e3ae9486718b4411c1e311f/amaranthus-spinosus-past-present-and-future-the-treatment-of-vomiting-abdominal.jpg)