Embed Size (px)
Citation preview

1. Wasting in cancer: the cachexia
definition
2. Pathophysiological
mechanisms
3. Cancer cachexia treatment
4. Ghrelin in the treatment of
cancer cachexia
6. Expert opinion
Review
The potential of ghrelin in thetreatment of cancer cachexiaJosep M Argiles† & Britta Stemmler†Cancer Research Group, Departament de Bioquımica i Biologia Molecular, Facultat de Biologia,
Universitat de Barcelona, Barcelona, Spain
Introduction: Cachexia is a multiorgan syndrome associated with cancer,
characterized by body weight loss, muscle and adipose tissue wasting and
inflammation, being often associated with anorexia.
Areas covered: The aim of the present review is to examine the impact of
ghrelin and its agonists in the treatment of cancer cachexia, both at the
biochemical and physiological level a taking into account new clinical and
experimental data related to the effects of ghrelin on food intake and meta-
bolism. The methodology undertaken includes both personal publications
and other obtained by Medline search.
Expert opinion: Based on experimental evidence, it is concluded that ghrelin
strategies are good candidates for muscle wasting treatment because ghrelin
levels are elevated in cancer cachexia and ghrelin controls mediators involved
in the cachectic process. Future clinical studies addressed at the interaction
between the peptide and protein turnover in human skeletal muscle should
be performed.
Keywords: cancer cachexia, ghrelin, skeletal muscle
Expert Opin. Biol. Ther. (2013) 13(1):67-76
1. Wasting in cancer: the cachexia definition
Cachexia -- from the Greek words ‘kakos’ and ‘hexis’, meaning ‘bad condition’ -- is amultiorgan syndrome associated with cancer, characterized by body weight loss(at least 5%), muscle and adipose tissue wasting and inflammation, being oftenassociated with anorexia [1]. The abnormalities associated with cachexia includealterations in carbohydrate, lipid and protein metabolism [1-3]. Cachexia occurs inthe majority of terminal cancer patients, and it is responsible for the deaths ofapproximately 22% of cancer patients [4]. In addition, survival of patients affectedby different types of neoplasias is clearly dependent on the presence of weightloss [5]. Therefore, cachexia represents an important factor in the treatment of acancer patient, affecting not only survival, but also the efficacy of the anticancertreatment, quality of life and, ultimately, hospital costs. It is thus clear that thereis both a medical and a social need for the treatment of cancer cachexia. Accordingto an international consensus [1], ‘cachexia, is a complex metabolic syndromeassociated with underlying illness and characterized by loss of muscle with orwithout loss of fat mass. The prominent clinical feature of cachexia is weight lossin adults (corrected for fluid retention) or growth failure in children (excludingendocrine disorders). Anorexia, inflammation, insulin resistance and increasedmuscle protein breakdown are frequently associated with cachexia. Cachexia isdistinct from starvation, age-related loss of muscle mass, primary depression,malabsorption and hyperthyroidism and is associated with increased morbidity’ [6].Similar definitions have been recently published [7,8]. Fearon et al. [9] describedcancer cachexia as a ‘multifactorial syndrome defined by an ongoing loss of skeletalmuscle mass (with or without loss of fat mass) that cannot be fully reversed byconventional nutritional support and leads to progressive functional impairment.
10.1517/14712598.2013.727390 © 2013 Informa UK, Ltd. ISSN 1471-2598, e-ISSN 1744-7682 67All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

Its pathophysiology is characterised by a negative protein andenergy balance a driven by a variable combination of reducedfood intake and abnormal metabolism’. The diagnostic --provisional -- criterion for cachexia was weight loss greaterthan 5%, or weight loss greater than 2% in individuals alreadyshowing depletion, according to current bodyweight andheight (body mass index (BMI) < 20 kg/m2 or skeletal musclemass (sarcopenia)). The same consensus group reached theconclusion that the cachexia syndrome develops progressivelythrough various stages: precachexia to cachexia to refractorycachexia [9].In spite of the different definitions, the staging of cancer
cachexia patients is not an easy task. Several malnutritionscreening tools are available including the Patient-GeneratedSubjective Global Assessment (PG-SGA) developed byOttery [10]. This tool has two sections: i) a medical historysection that is completed by the patient and ii) a physicalassessment section that is completed by nursing, medical ordietetic staff. The medical history section includes additionalquestions regarding the presence of oncology nutrition impactsymptoms. A simpler assessment tool is the MalnutritionScreening Tool (MST) [11]. However, none of these toolsinclude any biochemical, inflammatory or immunologicalmeasurements. Very recently, the so-called cachexia score(CASCO) has been introduced [12]. The aim of the score isto overcome the problem of patient staging. This scoreconsiders five main different factors: i) body weight and leanbody mass loss, ii) anorexia, iii) inflammatory, immunologicaland metabolic disturbances, iv) physical performance andv) quality of life. The score’s scale goes from 0 to 100: mildcachexia (less than 25), moderate (more than 26 and lessthan 50), severe (more than 51 and less than 75) and terminalphase (more than 76 and up to 100). The score also takes intoconsideration the condition known as precachexia.
2. Pathophysiological mechanisms
In clinical terms, anorexia means decreased appetite resultingin decreased food intake, fatigue, changes in body image andweight loss. In addition to anorexia, cachexia includes asthe-nia, anemia and loss of fat tissue and skeletal muscle, associ-ated with abnormalities in protein, lipid and carbohydratemetabolism (Figure 1) [13-15].Although a recent study involving 1853 cancer patients [16]
did not find common genetic causes in appetite loss in cancerpatients, cytokines, neuroendocrine changes and tumor
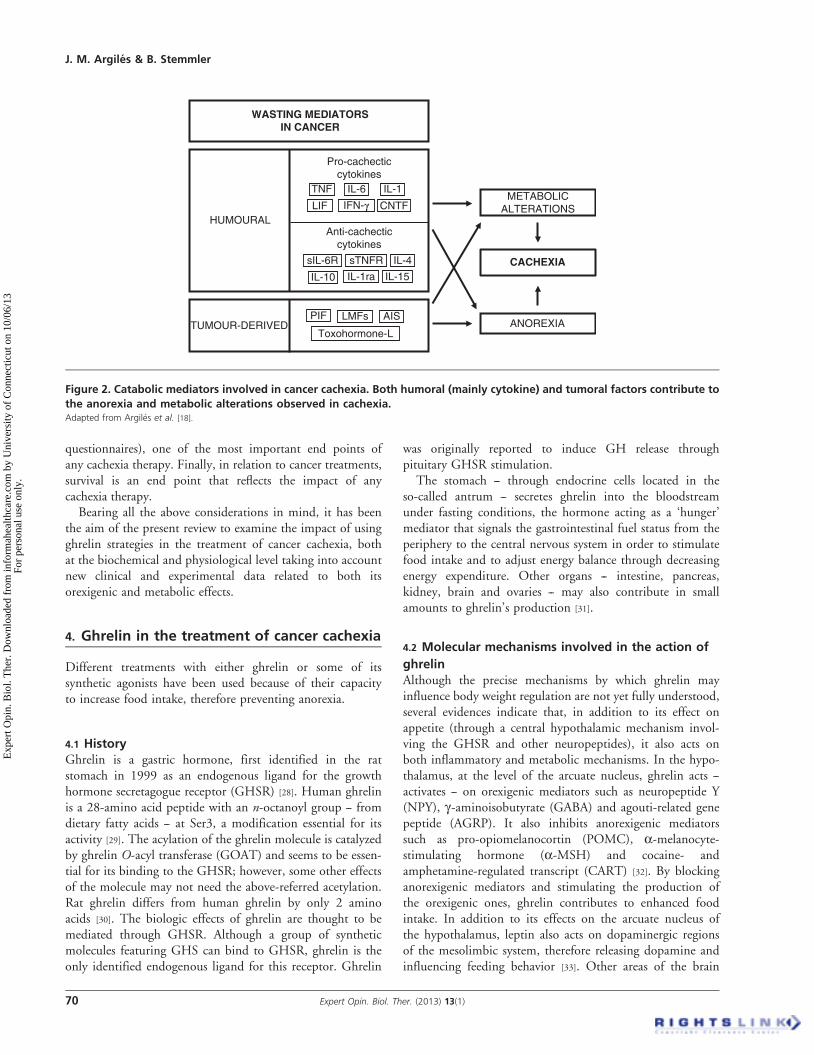
mediators are the main signals involved in appetite depressionin cachexia [17,18]. Additional factors contributing to theanorectic state are: altered taste perception, therapy-induced side effects, depressed motor activity, possiblemechanical interference on the gastrointestinal tract and, ofcourse, psychological factors. Indeed, patients with cachexiaoften experience psychological distress as a result of the uncer-tainties of the disease, its diagnosis, its treatment and its anti-cipated and final outcome. This psychological state, whichoften involves depression, is bound to affect food intake.Although anorexia represents a very important factor in thedevelopment of cachexia, it has to be pointed out that inmany cases the use of total parenteral nutrition does notstop the loss of body weight [19]. It seems, therefore, quiteevident that metabolic disturbances present in the patient(increased energy inefficiency, insulin resistance and abnormalcarbohydrate metabolism, adipose tissue dissolution andhypertriglyceridemia and muscle wasting) have a definitiverole in the development of cachexia (Figure 1) [2]. Differentmediators are involved in the metabolic disturbances,cytokines playing a major role (Figure 2) [6,20].
Although cancer cachexia is a multiorgan syndrome invol-ving many organs and tissues, including liver [21], heart [22]
and fat [23], skeletal muscle tissue is perhaps the most signifi-cant cachexia target, since this tissue alone represents over40% of total body weight. At the level of skeletal muscle,data from the laboratory have clearly shown that duringmuscle wasting three main processes are activated: i) DNAfragmentation or apoptosis, ii) myofibrillar protein degrada-tion (activation of the ubiquitin--proteasome-dependentproteolytic pathway) and iii) increased uncoupling proteins(UCPs) production [24]. Indeed, different pathological condi-tions are associated with increases in muscle UCP2 andUCP3. The UCP3 protein has been related to both energeticinefficiency and protection against oxidative damage [25]. Thethree events are not only interrelated but also coordinated.Lack of muscle regeneration is also involved in muscle wastingduring cancer [26].
3. Cancer cachexia treatment
Although a plethora of treatments for the cachectic syndromehave been proposed, unfortunately, not a single one iscompletely satisfactory in reversing weight loss. Bearing inmind the fact that both anorexia and metabolic disturbancesare involved in the pathophysiology of the cachectic syn-drome, the development of different therapeutic strategieshas focused on these two factors. Several pharmacologicaland nutritional approaches have been used. The ideal candi-date for an anticachectic drug would be a compound able toincrease food intake and also improve muscle weight, whichis the main component of the cachectic syndrome.
Unfortunately, nutritional strategies are not sufficient toreverse the cachectic syndrome. Indeed, patients on totalparenteral nutrition are still subject to significant wasting,
Article highlights.
. Ghrelin
. Cancer
. Cachexia
This box summarizes key points contained in the article.
J. M. Argiles & B. Stemmler
68 Expert Opin. Biol. Ther. (2013) 13(1)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

therefore emphasizing the role of the metabolic abnormalitiesin cachexia. It is perhaps for this reason that any therapeuticapproach based on increasing food intake has to be combinedwith a pharmacological strategy to counteract metabolicchanges. Another important problem associated with thedesign of the ideal therapeutic approach is that no definitemediators of cachexia have yet been identified. Both tumoraland humoral (mainly cytokines) factors seem to be involvedand, therefore, it is doubtful that a simple drug may blockthe complex syndrome. In addition, some of the mediatorsproposed for the wasting syndrome also play a role in theregulation of body weight in absolutely opposite states suchas obesity. For instance, TNF is overexpressed in adiposetissue during obesity [27]. In conclusion, the future treatmentof the cachectic syndrome will no doubt combine differentpharmacological approaches to efficiently revert the metabolicchanges described above and at the same time, ameliorate theanorexia of the patients. Defining this therapeutic combina-tion of drugs is an exciting project that will stimulate manyscientific efforts.
Independent of the treatment, the monitoring of cachexiais a key issue during therapy. Different parameters can be
used but, inevitably, they rely on the targets mentionedbefore. In relation to anorexia, food intake, intestinal absorp-tion, delayed gastric emptying and dysphagia constituteimportant parameters to be monitored. Often, the treatmentof the tumor also causes alterations in both the taste andsmell of foods; therefore, this should also be taken intoconsideration. In addition, metabolic alterations are variedand complex. Assessment of energy expenditure (both restingand total), inflammation (C-reactive protein), glucose intoler-ance, fat mobilization (lipolysis) and protein breakdown areimportant end points and should ideally be monitored.
Although bodyweight is the most important end point ofany cachexia treatment, body composition (lean body mass,fat mass, water) should be analyzed by means of BIA (bodyimpedance analysis), DEXA (dual-energy X-ray absorptio-metry) or CT scanning (computer tomography), since anincrease in body weight based on fat or water -- without anincrease in lean body mass -- may not be relevant (Figure 2). Itis also important to include measurements of physicalperformance (e.g., the monitoring of total activity and gripforce evaluation). Indeed, physical performance is linked withquality of life (that can be estimated through the use of different
CACHEXIA
ANOREXIAMETABOLIC
DISTURBANCES
Food intakeIntestinal absorption
Gastric emptyingDysphagiaHypogeusiaHyposmia
Energy expenditureInflammation
Glucose intoleranceFat mobilization
Protein breakdown
BODY WEIGHT
LEAN BODY MASS
PHYSICAL PERFORMANCE
QoL
FAT MASS
SURVIVAL
Figure 1. Pathophysiology of cachexia: anorexia and metabolic alterations drive body weight loss through both depletion of
fat and lean tissue mass.Adapted from Argiles et al. [77]..
The potential of ghrelin in the treatment of cancer cachexia
Expert Opin. Biol. Ther. (2013) 13(1) 69
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.
questionnaires), one of the most important end points ofany cachexia therapy. Finally, in relation to cancer treatments,survival is an end point that reflects the impact of anycachexia therapy.Bearing all the above considerations in mind, it has been
the aim of the present review to examine the impact of usingghrelin strategies in the treatment of cancer cachexia, bothat the biochemical and physiological level taking into accountnew clinical and experimental data related to both itsorexigenic and metabolic effects.
4. Ghrelin in the treatment of cancer cachexia
Different treatments with either ghrelin or some of itssynthetic agonists have been used because of their capacityto increase food intake, therefore preventing anorexia.
4.1 HistoryGhrelin is a gastric hormone, first identified in the ratstomach in 1999 as an endogenous ligand for the growthhormone secretagogue receptor (GHSR) [28]. Human ghrelinis a 28-amino acid peptide with an n-octanoyl group -- fromdietary fatty acids -- at Ser3, a modification essential for itsactivity [29]. The acylation of the ghrelin molecule is catalyzedby ghrelin O-acyl transferase (GOAT) and seems to be essen-tial for its binding to the GHSR; however, some other effectsof the molecule may not need the above-referred acetylation.Rat ghrelin differs from human ghrelin by only 2 aminoacids [30]. The biologic effects of ghrelin are thought to bemediated through GHSR. Although a group of syntheticmolecules featuring GHS can bind to GHSR, ghrelin is theonly identified endogenous ligand for this receptor. Ghrelin
was originally reported to induce GH release throughpituitary GHSR stimulation.
The stomach -- through endocrine cells located in theso-called antrum -- secretes ghrelin into the bloodstreamunder fasting conditions, the hormone acting as a ‘hunger’mediator that signals the gastrointestinal fuel status from theperiphery to the central nervous system in order to stimulatefood intake and to adjust energy balance through decreasingenergy expenditure. Other organs -- intestine, pancreas,kidney, brain and ovaries -- may also contribute in smallamounts to ghrelin’s production [31].
4.2 Molecular mechanisms involved in the action of
ghrelinAlthough the precise mechanisms by which ghrelin mayinfluence body weight regulation are not yet fully understood,several evidences indicate that, in addition to its effect onappetite (through a central hypothalamic mechanism invol-ving the GHSR and other neuropeptides), it also acts onboth inflammatory and metabolic mechanisms. In the hypo-thalamus, at the level of the arcuate nucleus, ghrelin acts --activates -- on orexigenic mediators such as neuropeptide Y(NPY), g-aminoisobutyrate (GABA) and agouti-related genepeptide (AGRP). It also inhibits anorexigenic mediatorssuch as pro-opiomelanocortin (POMC), a-melanocyte-stimulating hormone (a-MSH) and cocaine- andamphetamine-regulated transcript (CART) [32]. By blockinganorexigenic mediators and stimulating the production ofthe orexigenic ones, ghrelin contributes to enhanced foodintake. In addition to its effects on the arcuate nucleus ofthe hypothalamus, leptin also acts on dopaminergic regionsof the mesolimbic system, therefore releasing dopamine andinfluencing feeding behavior [33]. Other areas of the brain
ANOREXIA
METABOLICALTERATIONS
TUMOUR-DERIVEDPIF LMFs
Toxohormone-L
AIS
HUMOURAL
IL-4
IL-10 IL-15IL-1ra
sIL-6R sTNFR
Anti-cachecticcytokines
Pro-cachecticcytokines
IL-6TNF IL-1
IFN-gLIF CNTF
WASTING MEDIATORSIN CANCER
CACHEXIA
Figure 2. Catabolic mediators involved in cancer cachexia. Both humoral (mainly cytokine) and tumoral factors contribute to
the anorexia and metabolic alterations observed in cachexia.Adapted from Argiles et al. [18].
J. M. Argiles & B. Stemmler
70 Expert Opin. Biol. Ther. (2013) 13(1)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

involved in feeding behavior (amygdala, orbitofrontal cortex,anterior insula and striatum) are also stimulated by ghrelin [34].Ghrelin could also be involved in mediating the appetitesignal from the gut to the brain and vice versa via the vagalsystem [35,36].
Concerning inflammation, ghrelin has been shown toreduce the in vitro production of cytokines (IL-1b, IL-6 andTNF-a) both in vivo [37,38] and in vitro [38]. All of thesehumoral factors have been implicated in the cachec-tic--anorexic response. Interestingly, ghrelin administrationresults in increased circulating IL-10 levels [37,39], an anti-inflammatory cytokine. Ghrelin’s action on pro-inflammatorycytokines seems to be linked to the transcription factor NF-kB(nuclear factor-kappaB), a key molecule involved in inflamma-tory responses [38,40]. However, an implication of the vagusnerve in the action of ghrelin has been postulated [39]. Indeed,one recent study demonstrates the presence of GHSR inafferent neurons of the nodose ganglion, suggesting thatghrelin signals are transmitted to the brain via vagal afferentnerves [41]. Moreover, central administration of ghrelinstimulates the vagal efferent nerve in anesthetized rats [42].
Concerning other metabolic effects of ghrelin, the peptidehas potent effects on fat storage. It activates white adipo-cytes [43] while inactivating brown adipocytes, thereforecontributing to decreased energy expenditure [44]. This isalso interesting because of the connection of white adiposetissue and skeletal muscle associated with cachexia. Indeed,very recent data suggest that adipose tissue fat breakdownprecedes and it is essential for muscle wasting [45]. Theseeffects are related to the capacity of the hormone forstimulating GH release from the anterior pituitary [28]. Inaddition, ghrelin increases IGF-1 (insulin-like growth factor-1) by stimulating its own receptor [46]. These two factors aremajor mediators of metabolism being related to the regulationof energy homeostasis. The effects of ghrelin on GH andIGF-1 may be linked with the capacity of ghrelin to preventincreases in protein degradation -- through different compo-nents of the proteasome such as MuRF1 and MAFbx -- atthe level of skeletal muscle. This is particularly relevant tocancer cachexia since muscle wasting occurs mainly throughan activation of the proteasome [47,48].
Interestingly, ghrelin also seems to stimulate gastricemptying and acid secretion [49]. This is an important effectsince abnormal intestinal function is often observed incancer patients.
Ghrelin also shows important effects at the level of thecardiovascular system, increasing cardiac output and decre-asing blood pressure [50]. Finally, ghrelin improves renalfunction in mice [51].
4.3 Ghrelin levels in cancer: therapeutic potential in
cachexiaIn experimental animals bearing human tumors, a clearupregulation of ghrelin expression is accompanied byincreased circulating levels of the peptide [52]. In a similar
manner, circulating levels of both acyl and des-acyl ghrelinhave been reported to be elevated in cancer cachectic patientswith neuroendocrine [53], gastric [54,55] and lung [56,57] tumors.Garcia et al. [58] reported that the levels of acyl-ghrelinwere 50% higher in cancer patients when they were subjectedto cachexia. These elevated levels could represent a counter-regulatory mechanism to fight anorexia associated with tumorgrowth. It is, in fact, an endocrine response to theso-called ‘ghrelin resistance’ found in cancer patients. Indeed,this is, in part, the reason as to the high doses of ghrelin usedin clinical studies to counteract anorexia in cancer. On theother hand, several types of tumors may actually releaseghrelin [59].
4.4 Clinical trials in cancer cachexiaAnimal studies have revealed that ghrelin administration tocachectic tumor-bearing animals results in an improvementin both appetite and body weight [60-62], improving leanbody mass [62]. Interestingly, ghrelin administration to ratsprevents cisplatin-induced mechanical hyperalgesia -- increasedpain sensitivity -- and cachexia [63]. In fact, cisplatin-induced anorexia is mediated through reduced hypothalamicghrelin secretion [64]. In addition, ghrelin seems to attenuategastrointestinal epithelial damage induced by doxorubicin [65].These results suggest that ghrelin may be a protective factoragainst the toxic effects of chemotherapy.
In clinical practice, the use of ghrelin and ghrelin agonistshas led to promising results in cancer cachectic patients.Different randomized, double-blind placebo-controlled trialshave shown the efficacy and safety of ghrelin in cancerpatients with cachexia. Neary et al. [66] undertook a random-ized, placebo-controlled, crossover clinical trial to determinewhether ghrelin (5 pmole/kg/min i.v. for at least 180 min)could stimulate appetite in seven cancer patients with severeanorexia. Ghrelin infusion resulted in a marked increase inenergy intake in comparison with untreated subjects; allpatients involved in the study showed increased food intake.The meal appreciation score was also higher in ghrelin-treated individuals. Conversely, in another [67] randomized,double-crossover Phase I/II study, involving 21 patients withadvanced cancer (2 or 8 µg/kg i.v. for 4 days, once a day,before lunch), ghrelin did not have any effects on nutritionalintake and eating-related symptoms. More patients, however,preferred ghrelin to placebo at the middle and end of thestudy, although this finding was not dose-dependent.
Garcia and Polvino [68], using the ghrelin (GHSR) agonistRC-1291 (Anamorelin) using oral administration (50 mg/dayfor 12 weeks) found improvements in weight, lean body massand quality of life in subjects with multiple cancer types. Theimprovements were accompanied by increases in circulatingGH and IGF-1 and IGF-binding protein (IGFBP)-3 [69].Lundholm et al. [70] in 31 subjects with unresponsive gastro-intestinal cancer performed a randomized trial using ghrelinadministration for 8 weeks (either 0.7 or 13 µg/kg/day, s.c.once a day, 30 min before main meal) and found a tendency
The potential of ghrelin in the treatment of cancer cachexia
Expert Opin. Biol. Ther. (2013) 13(1) 71
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

toward increased lean body mass. Finally, Adachi et al. [71], ina randomized Phase I study involving 21 patients undergoingtotal gastrectomy found that short-term administration ofghrelin (3 µg/kg for 10 days after starting oral food intakefollowing surgery) resulted in lessened postoperative weighloss and improved appetite and food intake.
4.5 SafetyAkamizu et al. [72] confirmed the safety and hormonal effectsof ghrelin in a randomized, double-blind study involvinghealthy volunteers. No serious adverse effects were found.Ghrelin markedly stimulated GH release, slightly modulatedblood glucose and insulin levels and tended to increase thehunger sensation in a dose-dependent manner. Their resultssuggest that ghrelin may have therapeutic and diagnosticpotential in patients with cachectic disorders.Insignificant side effects have been reported in different
clinical trials involving ghrelin administration to cachecticcancer patients. Tolerability has not represented an importantissue, although one blinded trial showed a trend towardincreased undesirable gastrointestinal effects among subjectsreceiving ghrelin. These gastrointestinal effects includedabdominal pain, dry mouth and an increase in bowel activ-ity [67]. Another aspect that has to be taken into considerationwhen accounting for ghrelin’s safety is the fact of increasedlevels of GH and IGF-1. These hormones may play a role instimulating tumor growth since IGF-1 signaling plays a role
in anchorage-dependent cell growth, which might be impor-tant in tumor cell survival [73]. Additionally, the prospect ofincreased levels of GH rises potential for increased insulinresistance, and ghrelin administration in healthy individualshas been shown to suppress insulin action and worsen glucosetolerance [74]. This may prove problematic in some cachexia-associated conditions, given that insulin resistance is presentin cachectic cancer subjects. However, these concerns havenot been observed in animal models or human application,but longer-term trials will be necessary to clarify safety ofghrelin treatments in cancer.
6. Expert opinion
From the data presented in this review, it can be concludedthat in addition to increasing food intake in both experi-mental animal models and humans, ghrelin exerts metaboliceffects, mainly based on its anti-inflammatory potential.Among these metabolic effects, fat and skeletal muscleaccretion represents essential targets for any state with acatabolic drive that leads to body weight loss: cancer, infec-tions, sarcopenia. The potential anabolic effects on skeletalmuscle are worth underlining since they may contribute toan improvement in lean body mass. Any therapy addressedto cancer cachexia should not only contemplate an anaboliccomponent -- increased food intake, increased fast andprotein synthesis -- but also an anticatabolic one, mainly
Ghrelin
BRAINOREXIGENIC/
ANOREXIGENICMEDIATORS
POMC/MSH/CART
CYTOKINESIL-1, IL-6, TNF-a
FOOD INTAKE
PROTEASOMEACTIVITY
MUSCLEPROTEOLYSIS
PROTEINSYNTHESIS
MUSCLE WASTING
NPY/AGRP/GABA
ANABOLIC ACTION ANTICATABOLIC ACTION
Serotonin
FAT WASTING
QoL
GH/IGF-1
Gastricemptying
Vagal system
GHS-R
nF-kB
Figure 3. Ghrelin treatment involves both an anabolic and an anticatabolic action on the patient.
J. M. Argiles & B. Stemmler
72 Expert Opin. Biol. Ther. (2013) 13(1)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

anti-inflammatory that, in skeletal muscle, is represented byan inhibition of protein catabolism (Figure 3). This type oftherapy -- anabolic and anticatabolic -- is very likely to beeffective in syndromes involving body weight loss. The factthat des-acyl ghrelin has been shown to exhibit pro-anabolic and anticatabolic effects on skeletal muscle cell cul-tures certainly is on this line [75]. Future studies in humans,involving protein turnover in skeletal muscle, are essentialto support the role of ghrelin in the therapy of human cancercachexia. In addition, it is becoming clear that ghrelin treat-ment improves physical performance and muscle force indi-cating that the peptide is the best candidate for musclewasting treatment either alone or in combination with otherdrugs or nutritional strategies. Therefore, future research isneeded to search for the optimal combination. Cancercachexia is a multiorgan syndrome affecting not just skeletalmuscle but also adipose tissues, heart, intestine, kidney andliver. In fact, the final cause of death in cachectic cancerpatients is -- a part from the primary tumor itself -- eithersudden death (heart arrhythmias, hypoventilation), throm-boembolic events (platelet aggregation), cardiorenal altera-tions (kidney dysfunction) or compromised immunefunction (immunosuppression). Ghrelin has a beneficialeffect in all of the referred tissues (Table 1).
The only concern in treating cachectic cancer patientsrelates to the fact that ghrelin may contribute to tumor cellproliferation. Indeed, ghrelin may increase the levels ofgrowth factors, such as GH and IGF-1 that stimulate tumorgrowth. Additionally, ghrelin itself may have mitogenicpotential [76]. As far as is known, no in vivo data haveexamined the differences in tumor growth following ghrelinor GHS treatment. Long-term, large-scale clinical trials arerequired to determine whether ghrelin treatment promotestumor growth.
Declaration of interest
Each author has participated sufficiently, intellectually orpractically, in the work to take public responsibility for thecontent of the article, including the conception, design andfor data interpretation. All authors have read and approvedthe final manuscript. All authors of this research have noconflict of interest related to employment, consultancies,stock ownership, honoraria, paid expert testimony, patentapplications/registrations and grants or other funding. Thiswork was supported by a grant from the Ministerio de Cienciay Tecnologıa (SAF-26091-2011).
Table 1. Beneficial effects of ghrelin in the cancer patient.
Organ Beneficial effect Possible mechanism(s)
Liver Decreased acute-phase response Decreased inflammatory response (IL-6)Skeletal muscle Increased lean body mass Decreased protein degradation/increased protein
synthesis (increased IGF-1)Brain Increased appetite Increased orexigenic/anorexigenic mediators, vagal signalingGut Increased gastric emptying Decreased inflammatory response (IL-1, TNF)White adipose tissue Increased fat deposition Increased LPL and FASBrown adipose tissue Decreased thermogenesis/resting Reduced UCP1 energy expenditure activityKidney Improved renal function Increased IGF-1/nitric oxideHeart Increased cardiac output/reduced Decreased sympathetic blood pressure outflow
FAS: Fatty acid synthase; IGF-1: Insulin-like growth factor-1; LPL: Lipoprotein lipase; UCP: Uncoupling proteins.
The potential of ghrelin in the treatment of cancer cachexia
Expert Opin. Biol. Ther. (2013) 13(1) 73
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Evans W J, Morley J E, Argiles J M,
et al. Cachexia: a new definition.
Clin Nutr 2008;27:793-9. A consensus paper on cachexia
definition and diagnosis
2. Argiles J M, Alvarez B, Lopez-Soriano
F J. The metabolic basis of cancer
cachexia. Med Res Rev 1997;17:477-98
3. Argiles J M, Lopez-Soriano F J. Why do
cancer cells have such a high glycolytic
rate? Med Hypotheses 1990;32:151-5
4. Warren S. The immediate cause of death
in cancer. Am J Med Sci 1932;
184:610-13
5. Dewys WD, Begg C, Lavin PT, et al.
Prognostic effect of weight loss prior to
chemotherapy in cancer patients. Eastern
Cooperative Oncology Group.
Am J Med 1980;69:491-7
6. Llovera M, Garcia-Martinez C,
Lopez-Soriano J, et al. Protein turnover
in skeletal muscle of tumour-bearing
transgenic mice overexpressing the
soluble TNF receptor-1. Cancer Lett
1998;130:19-27
7. Argiles JM, Anker SD, Evans WJ, et al.
Consensus on cachexia definitions. J Am
Med Dir Assoc 2010;11:229-30
8. Muscaritoli M, Anker SD, Argiles JM,
et al. Consensus definition of sarcopenia,
cachexia and pre-cachexia: joint
document elaborated by Special Interest
Groups (SIG) "cachexia-anorexia in
chronic wasting diseases" and "nutrition
in geriatrics". Clin Nutr 2010;29:154-9
9. Fearon K, Strasser F, Anker SD, et al.
Definition and classification of cancer
cachexia: an international consensus.
Lancet Oncol 2011;12:489-95
10. Ottery FD. Definition of standardized
nutritional assessment and interventional
pathways in oncology. Nutrition 1996;
12(1 Suppl):S15-19
11. Isenring E, Cross G, Daniels L, et al.
Validity of the malnutrition screening
tool as an effective predictor of
nutritional risk in oncology outpatients
receiving chemotherapy.
Support Care Cancer 2006;14:1152-6
12. Argiles J M, Lopez-Soriano F J,
Toledo M, et al. The cachexia score
(CASCO): a new tool for staging
cachectic cancer patients. J Cachexia
Sarcopenia Muscle 2011;2:87-93.. New approach for the screening and
staging of cancer cachectic patients.
13. Argiles JM. Cancer-associated
malnutrition. Eur J Oncol Nurs
2005;6:S39-50
14. Argiles J M, Busquets S,
Moore-Carrasco R, Lopez-Soriano F J.
Cancer cachexia and fat metabolism. In:
Mantovani G, editor. Cachexia and
wasting. Springer Milan; 2006.
p. 459-66
15. Argiles JM, Lopez-Soriano FJ,
Busquets S. Novel approaches to the
treatment of cachexia.
Drug Discov Today 2008;13:73-8
16. Solheim TS, Fayers PM, Fladvad T, On
behalf of the European Palliative Care
Research Collaborative (EPCRC) and the
European Pharmacogenetic Study
(EPOS). Is there a genetic cause of
appetite loss? An explorative study in
1,853 cancer patients. J Cachexia
Sarcopenia Muscle 2012;3(3):191-8
17. Argiles JM, Busquets S, Toledo M,
Lopez-Soriano FJ. The role of cytokines
in cancer cachexia. Curr Opin Support
Palliat Care 2009;3:263-8
18. Argiles JM, Busquets S,
Moore-Carrasco R, Lopez-Soriano FJ.
The role of cytokines in cancer cachexia.
In: Mantovani G, editor. Cachexia and
wasting. Springer Milan; 2006.
p. 467-6
19. Ng EH, Lowry SF. Nutritional support
and cancer cachexia. Evolving concepts of
mechanisms and adjunctive therapies.
Hematol Oncol Clin North Am 1991;
5:161-84
20. Argiles JM, Busquets S,
Lopez-Soriano FJ. Metabolic
interrelationships between liver and
skeletal muscle in pathological states.
Life Sci 2001;69:1345-61
21. Fearon KC, Barber MD, Falconer JS,
et al. Pancreatic cancer as a model:
inflammatory mediators, acute-phase
response, and cancer cachexia.
World J Surg 1999;23:584-8
22. Lainscak M, Podbregar M, Anker S D.
How does cachexia influence survival in
cancer, heart failure and other chronic
diseases? Curr Opin Support Palliat Care
2007;1:299-305
23. Das SK, Eder S, Schauer S, et al.
Adipose triglyceride lipase contributes to
cancer-associated cachexia. Science 2011;
333:233-8
24. Argiles JM, Busquets S,
Lopez Soriano FJ. The role of
uncoupling proteins in
pathophysiological states. In:
Magalhaes J, Ascensao A, editors. Muscle
plasticity-advances in physiological
research. Research Signpost; Kerala India
2009. p. 195-207
25. Busquets S, Almendro V, Barreiro E,
et al. Activation of UCPs gene expression
in skeletal muscle can be independent on
both circulating fatty acids and food
intake. Involvement of ROS in a model
of mouse cancer cachexia. FEBS Lett
2005;579:717-22
26. Ametller E, Busquets S, Fuster G, et al.
Effects of formoterol on muscle
regeneration in cancer cachexia.
Insciences J 2011;1:1-17
27. Argiles JM, Lopez-Soriano J, Busquets S,
Lopez-Soriano FJ. Journey from cachexia
to obesity by TNF. FASEB J 1997;
10:743-51
28. Kojima M, Hosoda H, Date Y, et al.
Ghrelin is a growth-hormone-releasing
acylated peptide from stomach. Nature
1999;402:656-60
29. Bednarek MA, Feighner SD, Pong SS,
et al. Structure-function studies on the
new growth hormone-releasing peptide,
ghrelin: minimal sequence of ghrelin
necessary for activation of growth
hormone secretagogue receptor 1a.
J Med Chem 2000;43:4370-6
30. Wang G, Lee HM, Englander E,
Greeley GH Jr. Ghrelin--not just another
stomach hormone. Regul Pept
2002;105:75-81
31. Castaneda TR, Tong J, Datta R, et al.
Ghrelin in the regulation of body weight
and metabolism. Front Neuroendocrinol
2010;31:44-60
32. Shioda S, Takenoya F, Yagi M, et al.
Neural networks of several novel
neuropeptides involved in feeding
regulation. Nutrition 2008;24:848-53
33. Jerlhag E. Systemic administration of
ghrelin induces conditioned place
preference and stimulates accumbal
dopamine. Addict Biol 2008;13:358-63
34. Malik S, McGlone F, Bedrossian D,
Dagher A. Ghrelin modulates brain
J. M. Argiles & B. Stemmler
74 Expert Opin. Biol. Ther. (2013) 13(1)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

activity in areas that control appetitive
behavior. Cell Metab 2008;7:400-9
35. Date Y, Shimbara T, Koda S, et al.
Peripheral ghrelin transmits orexigenic
signals through the noradrenergic
pathway from the hindbrain to the
hypothalamus. Cell Metab 2006;
4:323-31
36. Maier C, Riedl M, Vila G, et al.
Cholinergic regulation of ghrelin and
peptide YY release may be impaired in
obesity. Diabetes 2008;57:2332-40
37. Gonzalez-Rey E, Chorny A, Delgado M.
Therapeutic action of ghrelin in a mouse
model of colitis. Gastroenterology 2006;
130:1707-20
38. Li WG, Gavrila D, Liu X, et al. Ghrelin
inhibits proinflammatory responses and
nuclear factor-kappaB activation in
human endothelial cells. Circulation
2004;109:2221-6
39. Wu R, Dong W, Cui X, et al. Ghrelin
down-regulates proinflammatory
cytokines in sepsis through activation of
the vagus nerve. Ann Surg 2007;
245:480-6
40. Waseem T, Duxbury M, Ito H, et al.
Exogenous ghrelin modulates release of
pro-inflammatory and anti-inflammatory
cytokines in LPS-stimulated macrophages
through distinct signaling pathways.
Surgery 2008;143:334-42
41. Date Y, Murakami N, Toshinai K, et al.
The role of the gastric afferent vagal
nerve in ghrelin-induced feeding and
growth hormone secretion in rats.
Gastroenterology 2002;123:1120-8
42. Sato N, Kanai S, Takano S, et al.
Central administration of ghrelin
stimulates pancreatic exocrine secretion
via the vagus in conscious rats.
Jpn J Physiol 2003;53:443-9
43. Tschop M, Smiley DL, Heiman ML.
Ghrelin induces adiposity in rodents.
Nature 2000;407:908-13.. Leading publication describing the role
of ghrelin in the control of fat mass
44. Mano-Otagiri A, Iwasaki-Sekino A,
Nemoto T, et al. Genetic suppression of
ghrelin receptors activates brown
adipocyte function and decreases fat
storage in rats. Regul Pept
2010;160:81-90
45. Das SK, Eder S, Schauer S, et al.
Adipose triglyceride lipase contributes to
cancer-associated cachexia. Science
2011;333:233-8
46. Nagaya N, Moriya J, Yasumura Y, et al.
Effects of ghrelin administration on left
ventricular function, exercise capacity,
and muscle wasting in patients with
chronic heart failure. Circulation
2004;110:3674-9
47. Argiles JM, Lopez-Soriano FJ. The
ubiquitin-dependent proteolytic pathway
in skeletal muscle: its role in pathological
states. Trends Pharmacol Sci 1996;
17:223-6
48. Pallares-Trujillo J, Agell N,
Garcia-Martinez C, et al. The ubiquitin
system, a role in disease? Med Res Rev
1997;17:139-61
49. Peeters TL. Central and peripheral
mechanisms by which ghrelin regulates
gut motility. J Physiol Pharmacol
2003;54(Suppl 4):95-103
50. Nagaya N, Uematsu M, Kojima M,
et al. Chronic administration of ghrelin
improves left ventricular dysfunction and
attenuates development of cardiac
cachexia in rats with heart failure.
Circulation 2001;104:1430-5
51. Takeda R, Nishimatsu H, Suzuki E,
et al. Ghrelin improves renal function in
mice with ischemic acute renal failure.
J Am Soc Nephrol 2006;17:113-21
52. Hanada T, Toshinai K, Date Y, et al.
Upregulation of ghrelin expression in
cachectic nude mice bearing human
melanoma cells. Metabolism
2004;53:84-8
53. Wang HS, Oh DS, Ohning GV,
Pisegna JR. Elevated serum ghrelin exerts
an orexigenic effect that may maintain
body mass index in patients with
metastatic neuroendocrine tumors.
J Mol Neurosci 2007;33:225-31
54. Kerem M, Ferahkose Z, Yilmaz UT,
et al. Adipokines and ghrelin in gastric
cancer cachexia. World J Gastroenterol
2008;14:3633-41
55. Takahashi M, Terashima M,
Takagane A, et al. Ghrelin and leptin
levels in cachectic patients with cancer of
the digestive organs. Int J Clin Oncol
2009;14:315-20
56. Shimizu Y, Nagaya N, Isobe T, et al.
Increased plasma ghrelin level in lung
cancer cachexia. Clin Cancer Res
2003;9:774-8. Ghrelin levels in cancer patients
57. Karapanagiotou EM, Polyzos A,
Dilana KD, et al. Increased serum levels
of ghrelin at diagnosis mediate body
weight loss in non-small cell lung cancer
(NSCLC) patients. Lung Cancer 2009;
66:393-8
58. Garcia JM, Garcia-Touza M, Hijazi RA,
et al. Active ghrelin levels and active to
total ghrelin ratio in cancer-induced
cachexia. J Clin Endocrinol Metab
2005;90:2920-6
59. Nikolopoulos D, Theocharis S,
Kouraklis G. Ghrelin: a potential
therapeutic target for cancer. Regul Pept
2010;163:7-17
60. Hanada T, Toshinai K, Kajimura N,
et al. Anti-cachectic effect of ghrelin in
nude mice bearing human melanoma
cells. Biochem Biophys Res Commun
2003;301:275-9
61. Wang W, Andersson M, Iresjo BM,
et al. Effects of ghrelin on anorexia in
tumor-bearing mice with eicosanoid-
related cachexia. Int J Oncol 2006;
28:1393-400
62. DeBoer MD, Zhu XX, Levasseur P,
et al. Ghrelin treatment causes increased
food intake and retention of lean body
mass in a rat model of cancer cachexia.
Endocrinology 2007;148:3004-12. Animal study involving ghrelin
administration to animals affected by
cancer cachexia
63. Garcia JM, Cata JP, Dougherty PM,
Smith RG. Ghrelin prevents
cisplatin-induced mechanical hyperalgesia
and cachexia. Endocrinology 2008;
149:455-60
64. Yakabi K, Sadakane C, Noguchi M,
et al. Reduced ghrelin secretion in the
hypothalamus of rats due to
cisplatin-induced anorexia.
Endocrinology 2010;151:3773-82
65. Fahim MA, Kataya H, El-Kharrag R,
et al. Ghrelin attenuates gastrointestinal
epithelial damage induced by
doxorubicin. World J Gastroenterol
2011;17:3836-41
66. Neary NM, Small CJ, Wren AM, et al.
Ghrelin increases energy intake in cancer
patients with impaired appetite: acute,
randomized, placebo-controlled trial.
J Clin Endocrinol Metab 2004;
89:2832-6
67. Strasser F, Lutz TA, Maeder MT, et al.
Safety, tolerability and pharmacokinetics
of intravenous ghrelin for cancer-related
anorexia/cachexia: a randomised,
placebo-controlled, double-blind,
The potential of ghrelin in the treatment of cancer cachexia
Expert Opin. Biol. Ther. (2013) 13(1) 75
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.

double-crossover study. Br J Cancer
2008;98:300-8
68. Garcia JM, Polvino WJ. Effect on body
weight and safety of RC-1291, a novel,
orally available ghrelin mimetic and
growth hormone secretagogue: results of
a phase I, randomized, placebo-
controlled, multiple-dose study in
healthy volunteers. Oncologist
2007;12:594-600
69. Garcia JM, Friend J, Allen S.
Therapeutic potential of anamorelin, a
novel, oral ghrelin mimetic, in patients
with cancer-related cachexia:
a multicenter, randomized, double-blind,
crossover, pilot study.
Support Care Cancer 2012; In press.. A very recent multicenter clinical trial
involving ghrelin mimetics in
cancer patients.
70. Lundholm K, Gunnebo L, Korner U,
et al. Effects by daily long term provision
of ghrelin to unselected weight-losing
cancer patients: a randomized
double-blind study. Cancer
2010;116:2044-52
71. Adachi S, Takiguchi S, Okada K, et al.
Effects of ghrelin administration after
total gastrectomy: a prospective,
randomized, placebo-controlled phase II
study. Gastroenterology
2010;138:1312-20.. Clinical study involving ghrelin
administration in cancer patients.
72. Akamizu T, Takaya K, Irako T, et al.
Pharmacokinetics, safety, and endocrine
and appetite effects of ghrelin
administration in young healthy subjects.
Eur J Endocrinol 2004;150:447-55
73. Maki RG. Small is beautiful: insulin-like
growth factors and their role in growth,
development, and cancer. J Clin Oncol
2010;28:4985-95
74. Tong J, Prigeon RL, Davis HW, et al.
Ghrelin suppresses glucose-stimulated
insulin secretion and deteriorates glucose
tolerance in healthy humans. Diabetes
2010;59:2145-51
75. Sheriff S, Kadeer N, Joshi R, et al.
Des-acyl ghrelin exhibits pro-anabolic
and anti-catabolic effects on
C2C12 myotubes exposed to cytokines
and reduces burn-induced muscle
proteolysis in rats. Mol Cell Endocrinol
2012;351:286-95
76. Majchrzak K, Szyszko K, Pawłowski KM,
et al. A role of ghrelin in cancerogenesis.
Pol J Vet Sci 2012;15:189-97. A possible role of ghrelin influencing
tumor growth.
77. Argiles JM, Olivan M, Busquets S,
Lopez-Soriano FJ. Optimal management
of cancer anorexia-cachexia syndrome.
Cancer Manag Res 2010;2:27-38. A review on the clinical management
of the anorexia--cachexia syndrome.
AffiliationJosep M Argiles†1,2 & Britta Stemmler2
†Author for correspondence1Cancer Research Group, Departament de
Bioquımica i Biologia Molecular,
Facultat de Biologia, Universitat de Barcelona,
Diagonal 645, 08028-Barcelona,
Spain
Tel: +34 934021002;
Fax: +34 934021559;
E-mail: [email protected],
Institut de Biomedicina de la
Universitat de Barcelona, Barcelona,
Spain
J. M. Argiles & B. Stemmler
76 Expert Opin. Biol. Ther. (2013) 13(1)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
onne
ctic
ut o
n 10
/06/
13Fo
r pe
rson
al u
se o
nly.





























![[Cancer-associated cachexia] clean for authors](https://img.pdfslide.us/doc/110x75/61d1ee79118df22edc52f710/cancer-associated-cachexia-clean-for-authors.jpg)