Embed Size (px)
Citation preview
Forensic Science International 198 (2010) 53–57
The post-mortem relationship between beta-hydroxybutyrate (BHB),acetone and ethanol in ketoacidosis
Simon Elliott *, Christopher Smith, Diane Cassidy
ROAR Forensics, Malvern Hills Science Park, Geraldine Road, Malvern WR14 3SZ, UK
A R T I C L E I N F O
Article history:
Received 27 July 2009
Received in revised form 15 October 2009
Accepted 19 October 2009
Available online 1 December 2009
Keywords:
Ketoacidosis
GC–MS
BHB
Alcohol
Diabetes
A B S T R A C T
A reduced blood pH (ketoacidosis) from the production of b-oxidative ketone bodies as a result of
alcoholism (alcoholic ketoacidosis, AKA) or diabetes (diabetic ketoacidosis, DKA) can feature in many
fatalities and analytical evidence can be used to support a pathological diagnosis, or provide a possible
cause of death in the absence of other pathologically significant findings. Existing beliefs concerning the
relationship of BHB concentrations, acetone and ethanol have been re-examined by analysis of BHB,
acetone and ethanol in over 350 fatalities grouped into alcoholics, diabetics, alcoholic diabetics, coupled
with speculative cases and those with an alternative cause of death. Uniquely, the concentrations of BHB
were measured in post-mortem blood, urine and vitreous humour using selective GC–MS. The results
showed that existing beliefs need to be re-evaluated. Ethanol is not always low (<10 mg/dL) or absent in
cases of AKA. Also, the absence of acetone does not preclude a high BHB (>250 mg/L), therefore acetone
can be used as an initial marker pathologically significant ketoacidosis. For blood and urine BHB
concentrations the following interpretative ranges can be used (in mg/L); normal (<50 mg/L), raised
(51–249 mg/L), high and pathologically significant (>250 mg/L). Initial data suggest vitreous humour
BHB could be a useful alternative in the absence of blood (same interpretative ranges may also apply).
Analytical recommendation for investigation of post-mortem ketoacidosis is also presented.
Crown Copyright � 2009 Published by Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Forensic Science International
journal homepage: www.elsev ier .com/ locate / forsc i in t
1. Introduction
Ketoacidosis is a biochemical disturbance in the body. It arisesfrom the body utilizing fatty acids via the b-oxidative process, analternative fuel pathway [1]. Fatty acids are converted to formacetoacetate which undergoes additional reactions, such asdecarboxylation to form acetone and reduction to form beta-hydroxybutyrate (b-hydroxybutyrate, 3-hydroxybutyrate, BHB).These compounds are called ketone bodies. An increasedpresence of ketone bodies in the blood causes a lowering ofthe blood pH (<7.3). A reduced blood pH from ketones(ketoacidosis) can be a result of various medical reasons,particularly alcohol abuse and diabetes. In alcoholism, alcohol(ethanol) intake results in dehydration (via vomiting anddiuresis) and an increase in NADH co-factor which can beutilized to produce BHB from fatty acids. This is coupled withblocking of gluconeogenesis and poor nutrition, leading to a low(or sometimes normal) glucose level. This results in therequirement for lipolysis with increased fatty acid productionand metabolism (causing ketoacidosis). Symptoms can includenausea, vomiting, abdominal pains, loss of appetite, lethargy,
* Corresponding author. Tel.: +44 1684 585282; fax: +44 1684 574276.
E-mail address: [email protected] (S. Elliott).
0379-0738/$ – see front matter . Crown Copyright � 2009 Published by Elsevier Irelan
doi:10.1016/j.forsciint.2009.10.019
weakness and unconsciousness [2]. In diabetics, a reduction ininsulin (especially Type I diabetes), produces a raised glucoselevel which prevents the glucose being transported in certaintissues and with osmotic diuresis can be associated withdehydration. This along with the presence of other hormones(e.g. glucagon) results in the activation of the b-oxidativepathway, consequent breakdown of fatty acids and increasedketone body production. The symptoms are very similar to thoseof alcoholic ketoacidosis [3]. Both alcoholic and diabeticketoacidosis conditions feature in many fatalities and analyticalevidence can be used to support a pathological diagnosis, orprovide a possible cause of death in the absence of otherpathologically significant findings [4–8]. Current testing mayinvolve analysis of the common ketone bodies, BHB and acetone,this is usually coupled with ethanol and glucose determinationfor suspected alcoholic ketoacidosis (AKA) and diabetic ketoa-cidosis (DKA), respectively. It is generally believed and publishedthat (a) ethanol is low or absent (<10 mg/dL) in AKA, (b) theabsence of acetone does not necessarily preclude ketoacidosis(BHB still needs to be measured), (c) BHB concentrations in bloodbelow 500 mmol/L (52 mg/L) are normal and greater than2500 mmol/L (258 mg/L) are pathologically significant [6]. Inorder to re-examine existing beliefs in the analytical investiga-tion of ketoacidosis, the relationship between common ketonebodies (BHB and acetone) and ethanol was studied. Existing
d Ltd. All rights reserved.

Fig. 1. (a) Post-mortem blood BHB concentrations in various fatal groups. (b) Post-
mortem urine BHB concentrations in various fatal groups. (c) Post-mortem vitreous
humour BHB concentrations in various fatal groups.
S. Elliott et al. / Forensic Science International 198 (2010) 53–5754
publications involve enzymatic measurement of BHB which hasbeen suggested to be not appropriate for post-mortem analysisdue to haemolysis and matrix interferences [5,7]. Indirectmeasurement of BHB and acetoacetate has also been publishedvia conversion to acetone with subsequent analysis by headspacegas chromatography with flame ionization detection [9]. Thiswork utilises an adapted previously developed GC–MS metho-dology for specificity to determine if published BHB concentra-tion ranges still apply [10]. The resultant implications for post-mortem interpretation are discussed along with recommenda-tion for an analytical protocol.
2. Materials and methods
2.1. Chromatographic equipment
Gas chromatography with mass spectrometry (GC–MS) analysis was performed
using an Agilent 7890 GC system fitted with a 5795 series mass selective detector.
Phenomenex (Macclesfield, UK) Zebron ZB-5MS capillary column, 30 m � 0.25 mm,
0.25 mm film thickness was used.
2.2. Materials
Sulphuric acid was supplied by Sigma–Fluka–Aldrich Chemicals (Poole, UK).
Ethyl acetate was obtained from Rathburns (Walkerburn, UK). Bis(trimethylsi-
lyl)trifluoroacetamide (BSTFA) containing 1% trimethylchlorosilane (TMCS)
derivatising agent was supplied by Sigma–Fluka–Aldrich Chemicals (Poole,
UK). Pure 1 mg/mL methanolic GHB-D6 sodium salt and blank human serum was
supplied by LGC Standards (Welwyn Garden City, UK). Pure BHB sodium salt was
obtained from Sigma–Fluka–Aldrich Chemicals (Poole, UK) and was used to
prepare reference and calibration standards for the formal identification and
quantitation of BHB in the specimens analysed. BHB calibration standards of
3.125, 6.25, 12.5 and 25 mg/L were prepared in blank human serum. An internal
quality control standard for BHB of 20 mg/L was also produced in blank human
serum.
2.3. Extraction methods for biological specimens
In a 2 mL Eppendorf capped tube, 50 mL of 50 mg/L GHB-D6 internal standard
(in cold 0.05 M H2SO4) was added to 100 mL of calibration standard. For post-
mortem samples, 10 mL aliquots of blood, urine or vitreous humour samples were
diluted into 100 mL of blank human serum and vortexed prior to addition of
internal standard (1 in 10 dilution). A second dilution of 10 mL of sample into
200 mL of blank human serum (1 in 20 dilution) followed by 100 mL aliquot in a
fresh tube for internal standard introduction and extraction. Then 500 mL ethyl
acetate extraction solvent was added and vortex mixed for 30 seconds followed by
centrifugation at 13,000 rpm for 5 min. 500 mL of upper (solvent) layer was
transferred to a 12 mL glass vial and evaporated to dryness at 45 8C under
nitrogen. 75 mL of BSTFA 1% TMCS derivatising agent was added followed by brief
vortex mixing and incubation at 90 8C for 5 min in a heating block. After cooling,
this was transferred to a GC–MS vial insert ready for injection. The injection
volume was 1 mL.
2.4. Chromatography conditions
GC–MS analysis was based on a ZB-5MS capillary column (30 m � 0.25 mm,
0.25 mm film thickness) with a temperature gradient starting at 60 8C and
ramping to 180 8C (20 8C/min) then ramping to 250 8C (50 8C/min) and finally
70 8C post-run. Total run time 9 min with mass spectrometer data acquired in the
full scan mode (50–300 m/z) between 5 and 6.8 min. Derivatised BHB (BHB-
diTMS) and GHB-D6 (GHB-D6-diTMS) were detected using the 233 and 239 ion
fragments, respectively. Identification of BHB was confirmed using mass spectral
matching of a library standard entry. BHB-diTMS eluted at 6.2 min and GHB-D6-
diTMS eluted at 6.8 min.
2.5. Ethanol and acetone analysis
Ethanol and acetone were analysed using the common method of gas
chromatography with flame ionization detection (GC-FID) with a headspace
autosampler (Thermo Fisher Trace GC-FID with Triplus headspace autosampler).
Propan-1-ol was used as the internal standard in water. The limit of detection and
quantitation for ethanol was 10 mg/dL (0.01 g/L). The limit of detection for acetone
was 2 mg/dL (0.002 g/L) – acetone was not measured in the cases.
2.6. Post-mortem cases
BHB has become increasingly requested in alcohol and diabetic fatalities as well
as unascertained deaths, therefore BHB analysis is performed routinely on many
cases received for toxicological analysis. To aid interpretation, where possible, both
blood and urine samples (and sometimes vitreous humour) were analysed.
Furthermore, decedent groups were divided into (a) alcoholics, (b) diabetics, (c)
alcoholics + diabetics and (d) speculative cases. Speculative cases involved fatalities
where there was no obvious pathological or toxicological cause of death and
required more extensive analysis to exclude (or demonstrate) possible ketoacidosis.
BHB analysis was also requested in a small number of cases where there was an
alternative cause of death (e.g. road traffic accident or drug overdose). These were
used as a ‘‘control’’ group. As the post-mortem interval, production and instability
of BHB has been previously found to not be an issue, this did not form part of the
study [6,9].
3. Results
3.1. Method validation
Inter- and intra-analytical accuracy and precision was deter-mined using an internal quality control BHB standard of 20 mg/L. Abetween batch mean concentration of 20.4 mg/L (�0.9 mg/L) wascalculated, with an accuracy of 1.9% and precision of 4.6% (n = 15).
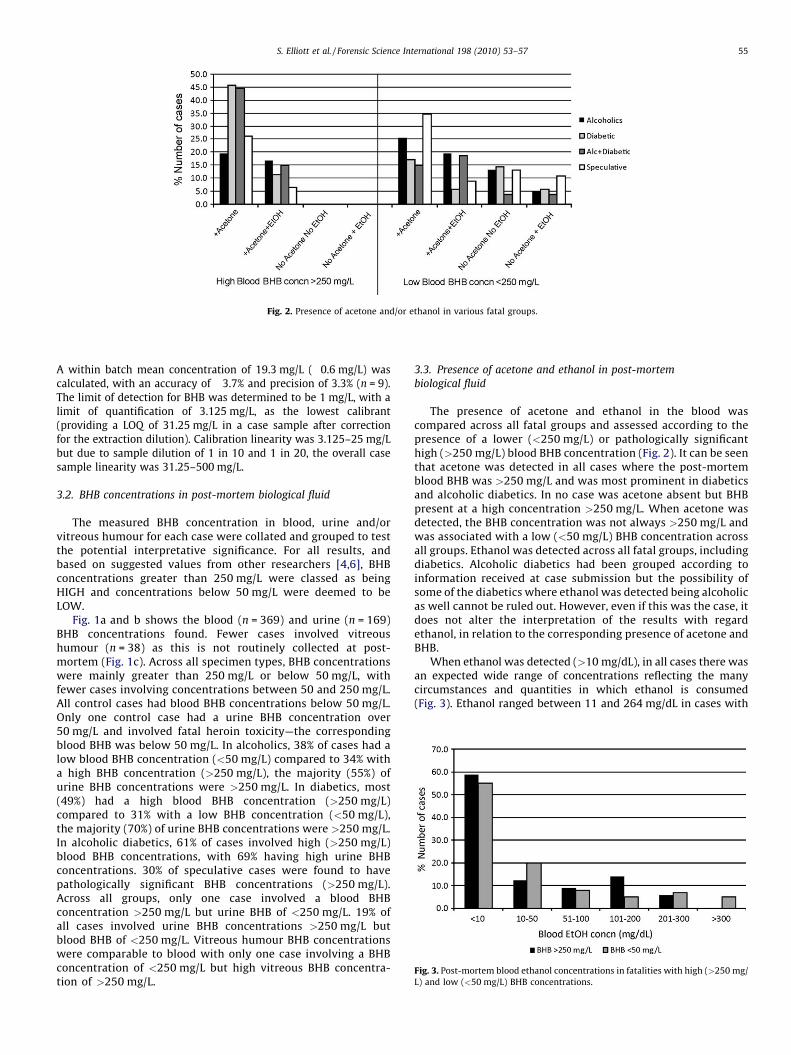
Fig. 2. Presence of acetone and/or ethanol in various fatal groups.
Fig. 3. Post-mortem blood ethanol concentrations in fatalities with high (>250 mg/
L) and low (<50 mg/L) BHB concentrations.
S. Elliott et al. / Forensic Science International 198 (2010) 53–57 55
A within batch mean concentration of 19.3 mg/L (�0.6 mg/L) wascalculated, with an accuracy of �3.7% and precision of 3.3% (n = 9).The limit of detection for BHB was determined to be 1 mg/L, with alimit of quantification of 3.125 mg/L, as the lowest calibrant(providing a LOQ of 31.25 mg/L in a case sample after correctionfor the extraction dilution). Calibration linearity was 3.125–25 mg/Lbut due to sample dilution of 1 in 10 and 1 in 20, the overall casesample linearity was 31.25–500 mg/L.
3.2. BHB concentrations in post-mortem biological fluid
The measured BHB concentration in blood, urine and/orvitreous humour for each case were collated and grouped to testthe potential interpretative significance. For all results, andbased on suggested values from other researchers [4,6], BHBconcentrations greater than 250 mg/L were classed as beingHIGH and concentrations below 50 mg/L were deemed to beLOW.
Fig. 1a and b shows the blood (n = 369) and urine (n = 169)BHB concentrations found. Fewer cases involved vitreoushumour (n = 38) as this is not routinely collected at post-mortem (Fig. 1c). Across all specimen types, BHB concentrationswere mainly greater than 250 mg/L or below 50 mg/L, withfewer cases involving concentrations between 50 and 250 mg/L.All control cases had blood BHB concentrations below 50 mg/L.Only one control case had a urine BHB concentration over50 mg/L and involved fatal heroin toxicity—the correspondingblood BHB was below 50 mg/L. In alcoholics, 38% of cases had alow blood BHB concentration (<50 mg/L) compared to 34% witha high BHB concentration (>250 mg/L), the majority (55%) ofurine BHB concentrations were >250 mg/L. In diabetics, most(49%) had a high blood BHB concentration (>250 mg/L)compared to 31% with a low BHB concentration (<50 mg/L),the majority (70%) of urine BHB concentrations were >250 mg/L.In alcoholic diabetics, 61% of cases involved high (>250 mg/L)blood BHB concentrations, with 69% having high urine BHBconcentrations. 30% of speculative cases were found to havepathologically significant BHB concentrations (>250 mg/L).Across all groups, only one case involved a blood BHBconcentration >250 mg/L but urine BHB of <250 mg/L. 19% ofall cases involved urine BHB concentrations >250 mg/L butblood BHB of <250 mg/L. Vitreous humour BHB concentrationswere comparable to blood with only one case involving a BHBconcentration of <250 mg/L but high vitreous BHB concentra-tion of >250 mg/L.
3.3. Presence of acetone and ethanol in post-mortem
biological fluid
The presence of acetone and ethanol in the blood wascompared across all fatal groups and assessed according to thepresence of a lower (<250 mg/L) or pathologically significanthigh (>250 mg/L) blood BHB concentration (Fig. 2). It can be seenthat acetone was detected in all cases where the post-mortemblood BHB was >250 mg/L and was most prominent in diabeticsand alcoholic diabetics. In no case was acetone absent but BHBpresent at a high concentration >250 mg/L. When acetone wasdetected, the BHB concentration was not always >250 mg/L andwas associated with a low (<50 mg/L) BHB concentration acrossall groups. Ethanol was detected across all fatal groups, includingdiabetics. Alcoholic diabetics had been grouped according toinformation received at case submission but the possibility ofsome of the diabetics where ethanol was detected being alcoholicas well cannot be ruled out. However, even if this was the case, itdoes not alter the interpretation of the results with regardethanol, in relation to the corresponding presence of acetone andBHB.
When ethanol was detected (>10 mg/dL), in all cases there wasan expected wide range of concentrations reflecting the manycircumstances and quantities in which ethanol is consumed(Fig. 3). Ethanol ranged between 11 and 264 mg/dL in cases with

S. Elliott et al. / Forensic Science International 198 (2010) 53–5756
high blood BHB concentrations (>250 mg/L) and between 10 and435 mg/dL in cases with a blood BHB concentration <250 mg/L.Conversely, in cases involving a high blood BHB concentration,ethanol was absent in 59% of cases. This is compared to itsabsence in 55% of cases involving blood BHB concentrations below250 mg/L.
4. Discussion
4.1. Methodology
The use of GC–MS provides a specific and selective techniquefor the detection and measurement of BHB in biological fluid. Itcan be applied quickly and easily to post-mortem samples and assuch is less affected by the viscosity and analytical problems thatmay affect more common enzyme-based assays routinely used inclinical chemistry laboratories [5,7]. Also, the extraction protocolrequires only a very small volume of case material (10 mL ofblood, urine or vitreous humour) which is an additionaladvantage, particularly if BHB analysis is required after routinescreening general drug screening has been performed. This iscompared to a volume requirement of at least 200 mL butpreferably 2 mL for a previously published indirect GC-FIDmethod [9].
4.2. BHB concentrations in post-mortem biological fluid
A previously described interpretative range for BHB by Itenand Meier, was based on mmol/L units [6]. Conversion of theseconcentrations to mg/L equate to <52 mg/L (normal), 52–258 mg/L (raised) and >258 mg/L (pathologically significant). Itis difficult to define any particular range for interpretation oflaboratory findings. As with the approach by Itens et al. (using acut-off of 2500 mmol/L), an interpretative cut-off of 250 mg/L hasbeen used within this study to define a pathologically significantconcentration for BHB in blood. This value proved to be applicablein the cases based on case information provided, pathologicalfindings and outcome, as was a low (normal) cut-off of 50 mg/L.As the vast majority of toxicological results are based on massunits rather than molar units, it seems appropriate that aninterpretative range for blood BHB using mg/L can be defined as<50 mg/L (normal), 51–249 (raised) and >250 (pathologicallysignificant). This range could also largely apply to urine andvitreous humour. In only one case was a high blood BHBconcentration (>250 mg/L) not reflected by a similarly high urineBHB concentration. However, as 19% of all cases showed a urineconcentration >250 mg/L but a blood BHB concentration of lessthan 250 mg/L, then a urine BHB concentration cannot be solelyused to diagnose pathologically significant ketoacidosis. In thesecases the case circumstances and pathological findings did notsuggest a fatal ketoacidosis, which was also supported by a bloodBHB concentration of less than 250 mg/L. Vitreous humour maybe a better indicator in the absence of a blood sample but wouldrequire further assessment using this methodology as only 38vitreous humour specimens were available. Nonetheless, vitr-eous has been suggested to be a suitable alternative by otherresearchers [8,9].
Of additional interest in this study was the subsequentidentification of a potential pathologically significant ketoacido-sis in 30% of ‘‘speculative’’ cases where there was no other cause ofdeath. This was primarily based on the presence of BHB in theblood at a concentration greater than 250 mg/L and wassupported by the presence of acetone in every case. In thesecases, this additional diagnostic tool proved invaluable inassisting the pathologist in determining the likely cause of death.This shows that analysis for ketoacidosis should be considered in
post-mortem investigations even when alcoholism or diabetes isnot suspected.
4.3. Presence of acetone and ethanol in post-mortem
biological fluid
It is clear from the data that acetone is present in every casewhere the blood BHB concentration was pathologically signifi-cant (>250 mg/L). Acetone may also be present in cases where theblood BHB concentration is less than 250 mg/L. Therefore,acetone can be used as an initial indicator of ketoacidosis, withblood BHB measurement required to confirm the diagnosis.However, if no acetone is detected, then BHB analysis is notnecessarily required as the blood concentration is very likely tobe not pathologically significant. It may be raised (i.e. between 50and 249 mg/L) but would be below the high cut-off of 250 mg/L.This also means that the acetone concentration would notnecessarily have to be measured as it is the actual presence orabsence of acetone that is relevant (as an indicator for theultimate diagnosis via BHB measurement). This is an importantfinding and can assist toxicologists in determining the analyticalapproach for post-mortem investigations, especially if ketoaci-dosis is suspected. It is recommended to perform GC-FID ethanolanalysis first (in blood and/or urine) which should also includeacetone detection. If acetone is detected, then BHB should bemeasured in the blood and compared against the interpretativerange described above.
The ethanol data show that in cases with a pathologicallysignificant BHB concentration in the blood, ethanol was absent in59% of cases. Conversely, ethanol was present in 41% of all cases(regardless of the fatal grouping). This is not entirely unexpectedas within the mechanism of ketoacidosis following ethanolintake, the individual case circumstances, quantities consumedand range in metabolism, it is likely that some ethanol would stillbe present in some cases, especially following excessiveconsumption associated with alcoholism. The blood ethanolrange was relatively wide (11–264 mg/dL) but even the highestconcentration would not be considered to constitute fatalethanol toxicity (typically associated with blood ethanol con-centrations greater than 350 mg/dL depending on tolerance).Those cases with a blood BHB concentration less than 250 mg/Lhad a wider blood ethanol range (10–435 mg/dL) and thereforecases at the upper end could have resulted in fatal ethanoltoxicity - thereby providing an alternative cause of death,supported by the non-pathologically significant BHB concentra-tions below 250 mg/L.
5. Conclusions
It is necessary to re-evaluate current beliefs regarding post-mortem analysis for ketoacidosis. Firstly, the study data haveshown ethanol is not always low (<10 mg/dL) or absent in cases ofalcoholic ketoacidosis. Also, the absence of acetone does notpreclude a pathologically significant ketoacidosis (BHB>250 mg/L), therefore acetone can be used as an initial marker. For blood,and to some extent, urine BHB concentrations, the followinginterpretative range can be used (in mg/L); normal (<50 mg/L),raised (51–249 mg/L), high and pathologically significant(>250 mg/L). Initial data suggest vitreous humour BHB couldbe a useful alternative in the absence of blood (same inter-pretative range may also apply). Analytically, it is thereforerecommended to perform GC-FID ethanol analysis first (in bloodand/or urine) which should also include acetone detection. Ifacetone is detected, then BHB should be measured by GC–MS inthe blood and compared against the interpretative rangedescribed above.

S. Elliott et al. / Forensic Science International 198 (2010) 53–57 57
Acknowledgment
The authors would like to thank HM Coroners for theirpermission in publishing the data.
References
[1] P.C. Champe, R.A. Harvey, Ketone bodies: an alternate fuel for cells, in: Biochem-istry, Lippincott Company, Philadelphia, 1987, pp. 176–181.
[2] L.C. McGuire, A.M. Cruickshank, P.T. Munro, Alcoholic ketoacidosis, Emerg. Med. J.23 (6) (2006) 417–420.
[3] A.E. Kitabchi, B.M. Wall, Diabetic ketoacidosis, Med. Clin. North Am. 79 (1) (1995)9–37.
[4] J.L. Thomsen, S. Felby, P. Theilade, E. Nielsen, Alcoholic ketoacidosis as a cause ofdeath in forensic cases, Forensic Sci. Int. 75 (2/3) (1995) 163–171.
[5] D.J. Pounder, R.J. Stevenson, K.K. Taylor, Alcoholic ketoacidosis at autopsy, J.Forensic Sci. 43 (4) (1998) 812–816.
[6] P.X. Iten, M. Meier, Beta-hydroxybutyric acid—an indicator for an alcoholicketoacidosis as cause of death in deceased alcohol abusers, J. Forensic Sci. 45(3) (2000) 624–632.
[7] L.N. Denmark, The investigation of beta-hydroxybutyrate as a marker for suddendeath due to hypoglycemia in alcoholics, Forensic Sci. Int. 62 (33) (1993) 225–232.
[8] E. Osuna, G. Vivero, J. Conejero, J.M. Abenza, P. Martınez, A. Luna, M.D. Perez-Carceles, Postmortem vitreous humor beta-hydroxybutyrate: its utility for thepostmortem interpretation of diabetes mellitus, Forensic Sci. Int. 153 (2-3) (2005)89–95.
[9] S. Felby, E. Nielsen, J.L. Thomsen, The postmortem distribution of ketone bodiesbetween blood, vitreous humor, spinal fluid, and urine, Forensic Sci. Med. Pathol. 4(2) (2008) 100–107.
[10] S.P. Elliott, Further evidence for the presence of GHB in postmortem biologicalfluid: implications for the interpretation of findings, J. Anal. Toxicol. 28 (1) (2004)20–26.