-
7/30/2019 The Pediatric Airway 2.pdf
1/41
The Pediatric Airway
Andrew Wackett, MD
-
7/30/2019 The Pediatric Airway 2.pdf
2/41
Objectives1) Demonstrate understanding of the indications
for
intubation2) Perform rapid sequence intubation
3) Learn the pharmacology behind emergency airwaymanagement
4) Demonstrate the ability to manage the pediatric airway5)
Demonstrate the ability to identify the difficult and
failed airway
6) Demonstrate working knowledge of the emergencyairway
algorithms
7) Practice the various techniques of airway mangement
-
7/30/2019 The Pediatric Airway 2.pdf
3/41
Objectives1) Demonstrate understanding of the indications
for
intubation2) Perform rapid sequence intubation
3) Learn the pharmacology behind emergency airwaymanagement
4) Demonstrate the ability to manage the pediatric airway5)
Demonstrate the ability to identify the difficult and
failed airway
6) Demonstrate working knowledge of the emergencyairway
algorithms
7) Practice the various techniques of airway mangement
-
7/30/2019 The Pediatric Airway 2.pdf
4/41
Are children little adults?
-
7/30/2019 The Pediatric Airway 2.pdf
5/41
Are the managementprinciples different?
-
7/30/2019 The Pediatric Airway 2.pdf
6/41
NO, they are not! 95% of the principles are exactlythe
same
Hypoxia is bad!
Indications for intubation are the same Universal algorithm is
the same
RSI, Crash, Difficult and Failedalgorithms are the same
Back up devices (LMA) are the same
-
7/30/2019 The Pediatric Airway 2.pdf
7/41
The Differences. . . Anatomical and physiological variation
which evolves as development proceedsfrom infancy to
adolescence
Age and weight related differences in drugdosing and equipment
sizing
Increased performance anxiety which
accompanies the resuscitation of thecritically ill child
-
7/30/2019 The Pediatric Airway 2.pdf
8/41
Anatomical andPhysiological Differences
-
7/30/2019 The Pediatric Airway 2.pdf
9/41
-
7/30/2019 The Pediatric Airway 2.pdf
10/41
-
7/30/2019 The Pediatric Airway 2.pdf
11/41
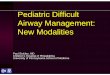
Infant Small Child Older child/Adult
Key to optimal individual patient position-Line traversing
external auditory canal crossing anterior to the shoulders
Support for the occiput in the older child/adult and the
shoulders in the infant
Extension of the head in the infant and small child
Hyperextension of the head in the older child or adult
-
7/30/2019 The Pediatric Airway 2.pdf
12/41
4 yr3 yr
1 yr8 mo6 mo
-
7/30/2019 The Pediatric Airway 2.pdf
13/41
-
7/30/2019 The Pediatric Airway 2.pdf
14/41
-
7/30/2019 The Pediatric Airway 2.pdf
15/41
Normal Anatomy
Vocal Cords
Extra-thoracic trachea
Pleural space
Lung
-
7/30/2019 The Pediatric Airway 2.pdf
16/41
Vocal Cords
Extra-thoracic trachea
Pleural space
Lung
Normal InspirationPrinciples
-
7/30/2019 The Pediatric Airway 2.pdf
17/41
Respiratory arrest is precipitated
without complete obstruction
Obstructed Inspiration
Obstruction
Principles
-
7/30/2019 The Pediatric Airway 2.pdf
18/41
-
7/30/2019 The Pediatric Airway 2.pdf
19/41
-
7/30/2019 The Pediatric Airway 2.pdf
20/41
-
7/30/2019 The Pediatric Airway 2.pdf
21/41
2 Skills required:
1) Starting an IV2) BMV ventilation
Needle Cricothyrotomy
-
7/30/2019 The Pediatric Airway 2.pdf
22/41
-
7/30/2019 The Pediatric Airway 2.pdf
23/41
-
7/30/2019 The Pediatric Airway 2.pdf
24/41
Physiological Differences
-
7/30/2019 The Pediatric Airway 2.pdf
25/41
Drug Dosing and EquipmentSelection
-
7/30/2019 The Pediatric Airway 2.pdf
26/41
ADULT
CHILD
IMPLEMENTATION TIME
Pediatric Resuscitation associated with error and timedelay and
a great dealof discomfort!
-
7/30/2019 The Pediatric Airway 2.pdf
27/41
The Cognitive Load of
Pediatric Resuscitation
Logistical timeAutomatic
Non-automatic activities
Critical thinking time
-
7/30/2019 The Pediatric Airway 2.pdf
28/41
Calculating the correct drug volume
Rechecking the drug volume calculation
Administering the dose correctly,
Administering the dose to the correct patient
Documenting accurately
Patientreceivesintended medication
Communication of dosage (verbal orders, handwritten)
Obtaining a the correct concentration
Estimation of weight
Recall of dose
Calculation of dosage
Decideon a medication
Vs. Automatic Activitynon-automaticactivities
-
7/30/2019 The Pediatric Airway 2.pdf
29/41
Equipment selection equally confusing:
10 different ET tube sizesSuction catheters ET tube size
specificVarious types and sizes of Laryngoscope blades
Various BVM, oral and NP airways
Vs. Automatic Activity
non-automaticactivities
-
7/30/2019 The Pediatric Airway 2.pdf
30/41
1) Weight estimation2) Equipment Selection
3) Recall/referencing doses
4) Calculation of doses5) Calculation of drug volumes
6) Calculation of fluid volumes
7) Calculation of ventilatoryvolumes
Sources of non-automaticactivities,
particular to children:
-
7/30/2019 The Pediatric Airway 2.pdf
31/41
The Broselow Tape
-
7/30/2019 The Pediatric Airway 2.pdf
32/41
-
7/30/2019 The Pediatric Airway 2.pdf
33/41
-
7/30/2019 The Pediatric Airway 2.pdf
34/41
Resuscitation Aids
Transform non-automaticactivities, the age/size
related variables particular to children, into
automaticactivities, thereby accelerating time to
treatment and reducing potential for error.
CHILD
ADULT
ADULT
ADULT
CHILD
NON-AUTOMATIC TIME
CHILD
Time Saved
IMPLM
TIME
Time Eliminated
CHILD
-
7/30/2019 The Pediatric Airway 2.pdf
35/41
Some Specifics ETT size = (16 + age in years)/4
*Cannot be used if < 1 year
Insertion Distance = ETT size x 3
The smallest bag mask is 450 cc*Dont use the 250cc bag
Succinylcholine dose is 2mg/kg
-
7/30/2019 The Pediatric Airway 2.pdf
36/41
RSI Sequence Preparation use the Broselow tape
Preoxygenation be meticulous Pretreatment none necessary
Paralysis with induction
SCh 2 mg/kg or rocuronium 1 mg/kg
Etomidate 0.3 mg/kg or ketamine 1.5 mg/kg
Positioning EAM anterior shoulder
Placement and Proof
Postintubation Management
-
7/30/2019 The Pediatric Airway 2.pdf
37/41
Follow the nose
PostintubationManagement
-
7/30/2019 The Pediatric Airway 2.pdf
38/41
1o
2o
Postintubation
Management
-
7/30/2019 The Pediatric Airway 2.pdf
39/41
Pediatric Induced Anxiety
-
7/30/2019 The Pediatric Airway 2.pdf
40/41
Summary The indications and algorithms are the same
Use the Broselow tape to select your medicationdoses and
equipment sizes
Be prepared to BMV
Intubation is different, but always in the sameway
Secure the tube and the neck
Needle cricothyrotomy is the solution to thefailed airway
-
7/30/2019 The Pediatric Airway 2.pdf
41/41